
Last Patient on Friday 2 Joan F. Addington-White MD.
36
Last Patient on Friday 2 Joan F. Addington-White MD
-
Upload
lorin-hardy -
Category
Documents
-
view
217 -
download
0
Transcript of Last Patient on Friday 2 Joan F. Addington-White MD.

Last Patient on Friday2
Joan F. Addington-White MD

Friday March 9, 2007
• 54 year old male cc diarrhea for 10 weeks.
• Treated with Cipro and twice for documented C. Difficile colitis.
• Severe, abdominal pain with bloody stools.
• Orthostatic, cachectic appearing with diffuse abdominal tenderness without rebound.

Admission to UW Hospital
• HGB 8.9 albumin 2.9• WBC 5.9 with normal diff• Colonoscopy Moderately severe
diffuse colitis present throughout colon. No pseudomembrane present.



Diagnosis: Ulcerative Colitis
• Discharged after transfusion and bowel rest on Prednisone 40 mg a day and Rowasa enemas. Seven day admission.
• Much improved clinically and symptomatically.

Friday March 30, 2007• Called into clinic with cc of leg cramps.• Several days after discharge right calf
cramps which extended down to top of his right foot.
• On exam R lower extremity just below the calf cool and extreme pain. Mottling of the plantar surface. Decreased cap refill.
• Unable to detect a pulse in his dorsalis pedis or posterior tibialis.

Called ER and Vascular surgery
• 20 minutes after ER arrival seen by vasc surgery.
• MRA of right lower extremity lack of filling of distal anterior tibial and posterior tibial arteries.

MRA

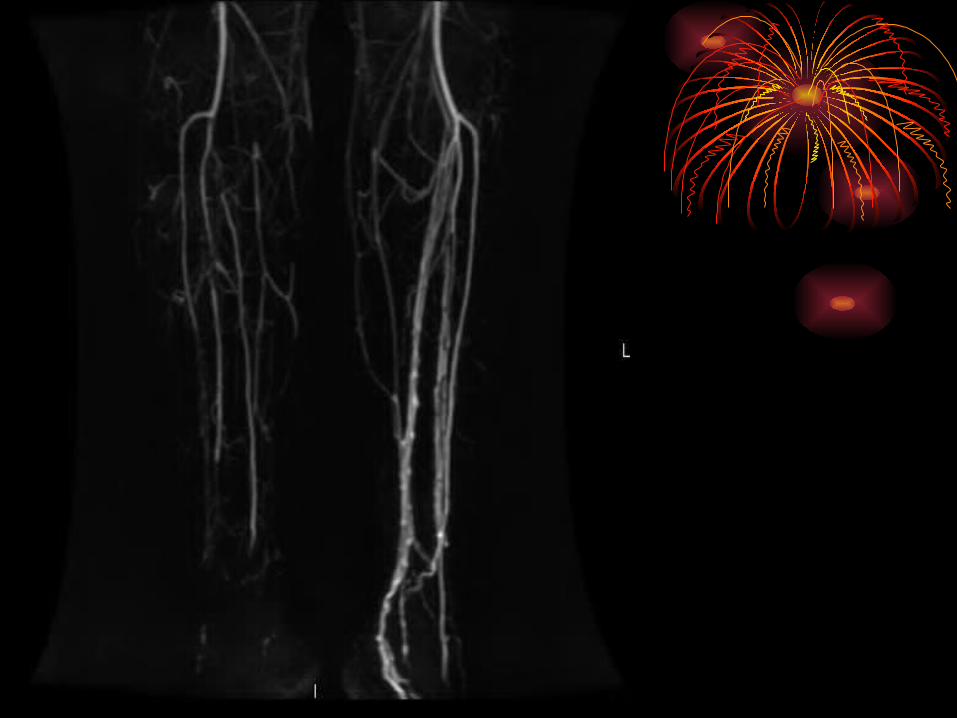

• Taken to surgery and had embolectomy of politial, post tibial, and dorsalis pedis artery with injection of dilute TPA.
• Good dorsalis pedis and post tibial pulse in recovery room.

Post op day 3
• Worsening abdominal pain
• Flex Sig
• Decrease prednisone, start oral Vanco and IV metronidazole.


Transferred toGeneral Surgery
• WBC 17.4, platelet 420, albumin 1.9
• Pos. C Difficile toxin
• Abdominal film


Treatment
• Subtotal abdominal colectomy with end ilestomy for perforated colon at splenic flexion secondary to fulminant UC and C. diff.
Objectives
• Discuss the increase risk of thrombosis in patients with inflammatory bowel disease.
• Explore pathophysiology of this phenomenon.
• Look at treatment options and outcome.
Incidence
• 1936 Mayo clinic 1500 patients with IBD. 18 extensive thrombosis.
• 1970 Mayo clinic 7,199 patients over 11 years 92 (1.3%) developed thrombosis.
• Other studies have shown incidence of 6.4%.
• Thrombosis, venous and arterial occurs in young people, in unusual sitesUpper extremityCarotidRetinalMesentaricRenalSubclavian

• 49 Crohn’s and 43 UC.
• Additional 4 vasculitis and 17 arteritis-related diagnosis.
• Patients excluded who had other risks for vascular dz.i.e. atherosclerosis, diabetes, obesity.

• Risk of thrombotic complications increases with disease activity and thrombosis may reoccur with a flare of disease.

• Of 113 patients with thrombosis
72 (64%) active disease30 (26%) disease controlled with
steroids or sulfasalazine or both.11 (10%) in remission.

• 9 patients had cerebral thrombotic events (mean age 38) and all had active IBS.
• 10 additional patients CV events were excluded because of other factor.

Mortality
• 23 patients died concurrent with vascular complication in the acute episode.
9 died of PE1 MI13 were also associated with sepsis
• Autopsy series PE and DVT ranked 3rd as cause of death behind peritonitis and neoplasm.

Pathogenesis
• Mechanism of thrombosis not clear, but appears to be acquired.
• Sorting out cause from effect.
• Changes indicative of thrombosis vs. those accompanying.
Platelets, factor V, factor VIII, and fribrinogen all acute phase reactants.

Antithrombin III
• Deficiency has been demonstrated in IBD.
• In combination with other factors will predispose to thrombosis.
• ie. Alpha-2 macroglobulin deficiency.
• GI protein loss and inc catabolism.

• Hypoalbuminemia normally binding arachidonic acid.
• Endotoxins cause a release of clotting factors from monocytes.
• ? if local activation in inflamed bowel leads to systemic thrombosis.
• Decrease Vit K dependent Protein C and S both of which inhibit coagulation.

Treatment
• Prevention Anticoagulation for adm related to IBD or other
illness Risk of catheter-induced DVT
• Conventional anticoagulation
• Surgical thrombectomy
• Thrombolytic therapy for extensive thrombosis. With or without active GI bleeding

Colectomy
• Stable patients15 at Mayo had resection after
episode of DVT or PE.– No postop deaths– 12 free of recurrent clot 2 to 9 years later.– 1 died PE from migration of VC umbrella.

Our patient:
• In acutely ill colectomy may increase risk of thombosis and mortality.
Same Mayo study 7 of 8 who developed portal or mensenteric thrombosis. (50% mortality)
Case reports of CVA in young patients after colectomy.

Friday April 20, 2007
• First patient afternoon sessionNo weight gain, but feeling better. Full
sensation in his foot.Questions if he should keep coming to our
clinic as he is admitted after each visit.
• Further proof of the interaction between thombosis and inflammation. ? Whether thrombosis may initiate inflammation in IBD.


Bibliography
• Talbot RW, Heppell J, Dozois RR, Beart RW Jr. Vascular complications of inflammatory bowel disease. Mayo Clin Proc 61(2):140-45, 1986.
• Koenigs KP, McPhedran P, Spiro, HM. Thrombosis in inflammatory bowel disease. J Clin Gastroenterol 9(6):627-631, 1987.

• Van Woert JH, Thompson RC, Cangemi JR, Streptokinase Therapy for extensive venous thromboses in a patient with severe ulcerative colitis. Mayo Clinic Proc, 65(8):1144-49, 1990.
• Szychta P, Reix T, Sevestre MA, Brazier F, Pietri J. Aortic thrombosis and ulcerative colitis. Ann Vasc Surg 15(3):402-4, 2001.

• Braverman D, Bogoch A. Arterial Thrombosis in Ulcerative Colitis. Am J Dig Dis 23(12):1148-50, 1978.
• Solem CA, Loftus EV, Tremaine WJ, Sanborn WJ. Venous thromboembolism in inflammatory bowel disease. Am J Gastroenterol 2004 Jan;99(1):97-101.


















