Laboratory Data in Nutrition Assessment - University of … in Med S… · PPT file · Web...
44
Medical Nutrition Therapy for Anemia
Transcript of Laboratory Data in Nutrition Assessment - University of … in Med S… · PPT file · Web...

Medical Nutrition Therapy for Anemia

Anemia• Definition: deficiency in size or number Definition: deficiency in size or number
of red blood cells or amount of of red blood cells or amount of hemoglobin they containhemoglobin they contain
• Defined as a hemoglobin concentration Defined as a hemoglobin concentration below the 95below the 95thth %ile for healthy reference %ile for healthy reference populationspopulations
• Not a disease but a symptom of Not a disease but a symptom of conditions including extensive blood conditions including extensive blood loss, excessive blood cell destruction, or loss, excessive blood cell destruction, or decreased blood cell formationdecreased blood cell formation

Classification of Anemia
Based on cell size (MCV)Based on cell size (MCV)• Macrocytic (large) MCV 100+ fl Macrocytic (large) MCV 100+ fl
(femtoliters)(femtoliters)• Normocytic (normal) MCV 8-99 flNormocytic (normal) MCV 8-99 fl• Microcytic (small) MCV<80 flMicrocytic (small) MCV<80 flBased on hemoglobin content (MCH)Based on hemoglobin content (MCH)• Hypochromic (pale color)Hypochromic (pale color)• Normochromic (normal color)Normochromic (normal color)
Iron Deficiency Anemia
• Characterized by the production of small Characterized by the production of small (microcytic) erythrocytes and a (microcytic) erythrocytes and a diminished level of circulating diminished level of circulating hemoglobin hemoglobin
• Last stage of iron deficiencyLast stage of iron deficiency• Represents the end point of a long period Represents the end point of a long period
of iron deprivationof iron deprivation

Causes of Iron Deficiency Anemia• Inadequate ingestionInadequate ingestion• Inadequate absorptionInadequate absorption• Defects in release from storesDefects in release from stores• Inadequate utilizationInadequate utilization• Increased blood loss or excretionIncreased blood loss or excretion• Increased requirementIncreased requirement

Stages of Iron Deficiency
• Stage 1: moderate depletion of iron stores; Stage 1: moderate depletion of iron stores; no dysfunctionno dysfunction
• Stage 2: Severe depletion of iron stores; no Stage 2: Severe depletion of iron stores; no dysfunctiondysfunction
• Stage 3: Iron deficiencyStage 3: Iron deficiency• Stage 4: Iron deficiency (dysfunction and Stage 4: Iron deficiency (dysfunction and
anemia)anemia)

Tests for Iron Deficiency• Serum iron: poor indicator, highly variable Serum iron: poor indicator, highly variable
day to day and during the dayday to day and during the day• Ferritin - most sensitive—chief storage form Ferritin - most sensitive—chief storage form
of iron; directly proportional to iron stored of iron; directly proportional to iron stored in cellsin cells

Tests for Iron Deficiency• Zinc protoporphyrin/heme ratio (ZPPH) Zinc protoporphyrin/heme ratio (ZPPH)
protoporphyrin binds iron to form heme protoporphyrin binds iron to form heme or zinc to form zinc protoporphyrinor zinc to form zinc protoporphyrin
• In the presence of iron deficiency, ratio In the presence of iron deficiency, ratio will rise (iron deficiency defined as will rise (iron deficiency defined as ratio>1:12,000) ratio>1:12,000)
• Not affected by hematocrit or other Not affected by hematocrit or other causes of anemia; specific to iron causes of anemia; specific to iron deficiencydeficiency

Tests for Iron Deficiency
• Total iron binding capacity (TIBC)—capacity of Total iron binding capacity (TIBC)—capacity of transferrin to bind irontransferrin to bind iron
• Transferrin—globulin that binds/transports Fe from Transferrin—globulin that binds/transports Fe from gut wall to tissuesgut wall to tissues
• Percent saturation of transferrin (calculate by Percent saturation of transferrin (calculate by dividing serum iron by the TIBC)dividing serum iron by the TIBC)• TIBC increases in iron deficiencyTIBC increases in iron deficiency• As stored iron falls, saturation of transferrin As stored iron falls, saturation of transferrin
decreasesdecreases

Iron Deficiency: Clinical FindingsEarlyEarly• Inadequate muscle Inadequate muscle
functionfunction• Growth abnormalitiesGrowth abnormalities• Epithelial disordersEpithelial disorders• Reduced Reduced
immunocompetenceimmunocompetence
LateLate• Defects in epithelial Defects in epithelial
tissuestissues• GastritisGastritis• Cardiac failureCardiac failure

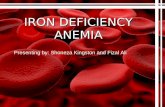
Koilonchia—A Sign of Iron Deficiency
(From Callen JP, Greer KE, Hood AF, Paller AS, Swinyer LJ. Color Atlas of Dermatology. Philadelphia: W.B. Saunders, 1993.)

Supplementation for Iron Deficiency Anemia
• Oral iron saltsOral iron salts• Ferrous forms better absorbed than ferric Ferrous forms better absorbed than ferric
(ferrous sulfate, ferrous lactate, ferrous (ferrous sulfate, ferrous lactate, ferrous fumarate)fumarate)
• Best absorbed on an empty stomach but if irritation Best absorbed on an empty stomach but if irritation occurs, give with mealsoccurs, give with meals
• Dosage 50-200 mg of elemental iron for adults; 6 Dosage 50-200 mg of elemental iron for adults; 6 mg/kg body weight for childrenmg/kg body weight for children
• Generally supplement for 3 months (4-5 months if Generally supplement for 3 months (4-5 months if taken with meals)taken with meals)

Nutritional Management of Iron-Deficiency Anemia• Increase absorbable iron in the dietIncrease absorbable iron in the diet• Include vitamin C at every mealInclude vitamin C at every meal• Include meat, fish or poultry at every mealInclude meat, fish or poultry at every meal• Decrease tea and coffee consumptionDecrease tea and coffee consumption

Restoring Iron LevelsFactors to consider:Factors to consider:• Bioavailability of iron—the lower the Fe Bioavailability of iron—the lower the Fe
stores, the greater the rate of absorptionstores, the greater the rate of absorption• Vitamin C—binds iron to form a readily Vitamin C—binds iron to form a readily
absorbed complexabsorbed complex• Heme sources (meat, poultry, fish)—Heme sources (meat, poultry, fish)— about about
15% absorbable15% absorbable• Nonheme iron (grains, vegetables, eggs)—Nonheme iron (grains, vegetables, eggs)—
about 3% to 8% absorbableabout 3% to 8% absorbable
Supplementation for Iron Deficiency AnemiaIf patient fails to respondIf patient fails to respond• May not be taking supplementsMay not be taking supplements• May not be absorbing iron (celiac disease, May not be absorbing iron (celiac disease,
steatorrhea, hemodialysis)steatorrhea, hemodialysis)• May be bleedingMay be bleeding• May need IV iron dextran (can cause May need IV iron dextran (can cause
allergic reactions)allergic reactions)

HemochromatosisA genetically determined form of iron A genetically determined form of iron
overload that results in progressive hepatic, overload that results in progressive hepatic, pancreatic, cardiac, and other organ damagepancreatic, cardiac, and other organ damage

Hemochromatosis• It is one of the most common genetic disorders It is one of the most common genetic disorders
in the U.S.in the U.S.• Present in heterozygous (one gene) form in Present in heterozygous (one gene) form in
12% of nonblacks and 30% of blacks12% of nonblacks and 30% of blacks• Present in homozygous form (2 gene) in 1 in Present in homozygous form (2 gene) in 1 in
200 nonblacks and 1 in 100 blacks200 nonblacks and 1 in 100 blacks• Homozygotes will die of iron overload unless Homozygotes will die of iron overload unless
they give blood frequentlythey give blood frequently• Homozygotes absorb three times more iron Homozygotes absorb three times more iron
from food than other peoplefrom food than other people• Even heterozygotes may be at risk for iron Even heterozygotes may be at risk for iron
overload, increasing risk of heart diseaseoverload, increasing risk of heart disease

Hemochromatosis: Risk Factors• Higher risk in people of northern European Higher risk in people of northern European
descentdescent• Men tend to manifest symptoms earlier because Men tend to manifest symptoms earlier because
they have no way to dispose of excess iron they have no way to dispose of excess iron (menstruation, pregnancy, lactation)(menstruation, pregnancy, lactation)
• Men may develop symptoms in their 30s but Men may develop symptoms in their 30s but may not be diagnosed until their 50smay not be diagnosed until their 50s
• Women often develop symptoms after Women often develop symptoms after menopausemenopause

Hemochromatosis: Symptoms• Joint painJoint pain• FatigueFatigue• Lack of energyLack of energy• Abdominal painAbdominal pain• Loss of sex driveLoss of sex drive• Heart problemsHeart problems• Abnormal pigmentation of the skin, Abnormal pigmentation of the skin,
making it look gray or bronzemaking it look gray or bronze

Hemochromatosis: if untreated, may result in
• ArthritisArthritis• Liver disease: cirrhosis, cancer, Liver disease: cirrhosis, cancer,
liver failureliver failure• Damage to the pancreas, leading Damage to the pancreas, leading
to diabetesto diabetes• Heart abnormalities, including Heart abnormalities, including
arrhythmias and heart failurearrhythmias and heart failure• Impotence or early menopauseImpotence or early menopause• Thyroid or adrenal problemsThyroid or adrenal problems

Hemochromatosis: Diagnosis and Treatment• Testing: serum ferritin and transferrin saturation Testing: serum ferritin and transferrin saturation
can reveal excess stores of iron; followed by HFE can reveal excess stores of iron; followed by HFE (genetic) test and possible liver biopsy(genetic) test and possible liver biopsy
• Treatment: regular phlebotomy to remove excess Treatment: regular phlebotomy to remove excess ironiron
• Avoidance of iron supplements and sources of Avoidance of iron supplements and sources of iron in the diet, especially heme ironiron in the diet, especially heme iron
• Awareness of iron cooking vesselsAwareness of iron cooking vessels

Disorders Associated with Iron Toxicity• ThalassemiasThalassemias• Sideroblastic anemiasSideroblastic anemias• Chronic hemolytic anemiaChronic hemolytic anemia• Aplastic anemiaAplastic anemia• Ineffective erythropoiesisIneffective erythropoiesis• Transfusional iron overloadTransfusional iron overload• Alcoholic cirrhosisAlcoholic cirrhosis

Megaloblastic Anemias• A form of anemia characterized by the presence A form of anemia characterized by the presence
of large, immature, abnormal red blood cell of large, immature, abnormal red blood cell progenitors in the bone marrowprogenitors in the bone marrow
• 95% of cases are attributable to folic acid or 95% of cases are attributable to folic acid or vitamin Bvitamin B12 12 deficiencydeficiency

Static Test for Folate/B12 Status
FolateFolate• Measured in whole blood (plasma and Measured in whole blood (plasma and
cells) and then in the serum alonecells) and then in the serum alone• Difference is used to calculate the red Difference is used to calculate the red
blood cell folate concentration (may blood cell folate concentration (may better reflect the whole folate pool)better reflect the whole folate pool)
• Can also test serum in fasting patientCan also test serum in fasting patientB12B12• Measured in serumMeasured in serum
Functional Tests for Macrocytic Anemias
• Homocysteine: Folate and B12 are Homocysteine: Folate and B12 are needed to convert homocysteine to needed to convert homocysteine to methionine; high homocysteine may methionine; high homocysteine may mean deficiencies of folate, B12 or B6mean deficiencies of folate, B12 or B6
• Methylmalonic acid measurements can be Methylmalonic acid measurements can be used along with homocysteine to used along with homocysteine to distinguish between B12 and folate distinguish between B12 and folate deficiencies (deficiencies (↑ in B12 deficiency)↑ in B12 deficiency)
• Schilling test: radiolabeled cobalamin is Schilling test: radiolabeled cobalamin is used to test for B12 malabsorptionused to test for B12 malabsorption

Pernicious AnemiaA macrocytic, megaloblastic anemia caused by a deficiency of vitamin BA macrocytic, megaloblastic anemia caused by a deficiency of vitamin B12. 12.
• Usually secondary to lack of intrinsic factor (IF)Usually secondary to lack of intrinsic factor (IF)• May be caused by strict vegan diet May be caused by strict vegan diet • Also can be caused by ↓gastric acid secretion, gastric atrophy, H-pylori, gastrectomy, disorders of the Also can be caused by ↓gastric acid secretion, gastric atrophy, H-pylori, gastrectomy, disorders of the
small intestine (celiac disease, regional enteritis, resections), drugs that inhibit B12 absorption including small intestine (celiac disease, regional enteritis, resections), drugs that inhibit B12 absorption including neomycin, alcohol, colchicine, metformin, pancreatic diseaseneomycin, alcohol, colchicine, metformin, pancreatic disease

Symptoms of Pernicious Anemia• Paresthesia (especially numbness and Paresthesia (especially numbness and
tingling in hands and feet)tingling in hands and feet)• Poor muscular coordinationPoor muscular coordination• Impaired memory and hallucinationsImpaired memory and hallucinations• Damage can be permanentDamage can be permanent

Vitamin B12 Depletion• Stage I—early negative vitamin BStage I—early negative vitamin B1212 balance balance• Stage II—vitamin BStage II—vitamin B1212 depletion depletion• Stage III—damaged metabolism: vitamin BStage III—damaged metabolism: vitamin B1212
deficient erythropoiesisdeficient erythropoiesis• Stage IV—clinical damage including vitamin BStage IV—clinical damage including vitamin B12 12
anemiaanemia• Pernicious anemia—numbness in hands and feet; Pernicious anemia—numbness in hands and feet;
poor muscular coordination; poor memory; poor muscular coordination; poor memory; hallucinationshallucinations

Causes of Vitamin B12 Deficiency
• Inadequate ingestionInadequate ingestion• Inadequate absorptionInadequate absorption• Inadequate utilizationInadequate utilization• Increased requirementIncreased requirement• Increased excretionIncreased excretion• Increased destruction by antioxidantsIncreased destruction by antioxidants

Treatment of B12 Deficiency• Before 1926 was incurable; until 1948 was treated Before 1926 was incurable; until 1948 was treated
with liver extractwith liver extract• Now treatment consists of injection of 100 mcg of Now treatment consists of injection of 100 mcg of
vitamin B12 once per week until resolved, then as vitamin B12 once per week until resolved, then as often as necessaryoften as necessary
• Also can use very large oral doses or nasal gelAlso can use very large oral doses or nasal gel• MNT: high protein diet (1.5 g/kg) with meat, liver, MNT: high protein diet (1.5 g/kg) with meat, liver,
eggs, milk, milk products, green leafy vegetables eggs, milk, milk products, green leafy vegetables

Folic Acid Deficiency• Tropical sprue; pregnancy; infants born to Tropical sprue; pregnancy; infants born to
deficient mothersdeficient mothers• AlcoholicsAlcoholics• People taking medications chronically that affect People taking medications chronically that affect
folic acid absorptionfolic acid absorption• Malabsorption syndromesMalabsorption syndromes

Causes of Folate Deficiency• Inadequate ingestionInadequate ingestion• Inadequate absorptionInadequate absorption• Inadequate utilizationInadequate utilization• Increased requirementIncreased requirement• Increased excretionIncreased excretion• Increased destructionIncreased destruction• Vitamin B12 deficiency can cause folate Vitamin B12 deficiency can cause folate
deficiency due to the methylfolate trapdeficiency due to the methylfolate trap

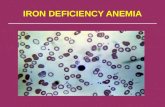
Methylfolate Trap• In the absence of B12, In the absence of B12,
folate in the body folate in the body exists as 5-exists as 5-methyltetrahydro-methyltetrahydro-folate (an inactive folate (an inactive form)form)
• B12 allows the B12 allows the removal of the 5-removal of the 5-methyl group to form methyl group to form THFATHFA

Stages of Folate Depletion and Deficiency
• Stage I—early negative folate balance (serum Stage I—early negative folate balance (serum depletion)depletion)
• Stage II—negative folate balance (cell Stage II—negative folate balance (cell depletion)depletion)
• Stage III—damaged folate metabolism with Stage III—damaged folate metabolism with folate-deficient erythropoiesisfolate-deficient erythropoiesis
• Stage IV—clinical folate deficiency anemiaStage IV—clinical folate deficiency anemia

Diagnosis of Folate Deficiency• Folate stores are depleted after 2-4 Folate stores are depleted after 2-4
months on deficient dietmonths on deficient diet• Megaloblastic anemia, low leukocytes Megaloblastic anemia, low leukocytes
and plateletsand platelets• To differentiate from B12, measure To differentiate from B12, measure
serum folate, RBC folate (more reflective serum folate, RBC folate (more reflective of body stores) serum B12of body stores) serum B12
• High formiminoglutamic acid (FIGLU) in High formiminoglutamic acid (FIGLU) in the urine also diagnosticthe urine also diagnostic

Other Nutritional Anemias• Copper deficiency anemiaCopper deficiency anemia• Anemia of protein-energy malnutritionAnemia of protein-energy malnutrition• Sideroblastic (pyridoxine-responsive) anemiaSideroblastic (pyridoxine-responsive) anemia• Vitamin E–responsive (hemolytic) anemiaVitamin E–responsive (hemolytic) anemia
Copper Deficiency• Copper is required for mobilization of iron Copper is required for mobilization of iron
from storage sitesfrom storage sites• In copper deficient state, result is low serum In copper deficient state, result is low serum
iron and hemoglobin, even when iron stores are iron and hemoglobin, even when iron stores are normalnormal
• Copper is widespread in foods and needed in Copper is widespread in foods and needed in tiny amountstiny amounts
• Sometimes occurs in infants fed deficient Sometimes occurs in infants fed deficient formula or cow’s milk, adults and children with formula or cow’s milk, adults and children with malabsorption or on TPN without coppermalabsorption or on TPN without copper
• Diagnosis is important, since more iron won’t Diagnosis is important, since more iron won’t help and may interfere with copper absorptionhelp and may interfere with copper absorption

Sideroblastic Anemia• Microcytic, hypochromic formMicrocytic, hypochromic form• Inherited defect of heme synthesis enzymeInherited defect of heme synthesis enzyme• High serum and tissue iron levelsHigh serum and tissue iron levels• Buildup of immature sideroblasts—hence the Buildup of immature sideroblasts—hence the
namename• BB66 is essential—must replace 25 to 100 times is essential—must replace 25 to 100 times
the RDA; may need lifelong replacementthe RDA; may need lifelong replacement• Pyridoxine-responsive anemia, distinguished Pyridoxine-responsive anemia, distinguished
from anemia caused by pyridoxine deficiencyfrom anemia caused by pyridoxine deficiency

Hemolytic Anemia• Oxidative damage to cells—lysis occursOxidative damage to cells—lysis occurs• Vitamin E is an antioxidant that seems to Vitamin E is an antioxidant that seems to be be
protective.protective.• This anemia can occur in newborns, This anemia can occur in newborns, especially especially
preemies.preemies.

Nonnutritional Anemias• Sports anemia (hypochromic microcytic Sports anemia (hypochromic microcytic
transient anemia)transient anemia)• Anemia of pregnancy: dilutionalAnemia of pregnancy: dilutional• Anemia of inflammation, infection, or Anemia of inflammation, infection, or
malignancy (anemia of chronic disease)malignancy (anemia of chronic disease)• Sickle cell anemiaSickle cell anemia• ThalassemiasThalassemias

Sports Anemia• Transient—usually in athletes who are runners; Transient—usually in athletes who are runners;
from compression of RBCs in feet until they from compression of RBCs in feet until they burst, releasing hemoglobinburst, releasing hemoglobin
• Check lab valuesCheck lab values• Counsel about a proper dietCounsel about a proper diet

Sickle Cell Anemia• Protein-energy malnutrition common; may have poor intake and increased Protein-energy malnutrition common; may have poor intake and increased
energy needsenergy needs• Be careful not to overdo iron in diet or supplements; iron stores are often Be careful not to overdo iron in diet or supplements; iron stores are often
high due to frequent transfusions; avoid iron rich foods, alcohol, and high due to frequent transfusions; avoid iron rich foods, alcohol, and ascorbic acid which enhance iron absorptionascorbic acid which enhance iron absorption
• Promote foods high in copper, zinc and folate as needs are increased due to Promote foods high in copper, zinc and folate as needs are increased due to constant replacement of erythrocytesconstant replacement of erythrocytes
• Zinc supplements may be usefulZinc supplements may be useful

Thalassemia• Severe inherited anemia affecting mostly people of Mediterranean extractionSevere inherited anemia affecting mostly people of Mediterranean extraction• Defective globin formation in hemoglobin leads to increased blood volume, Defective globin formation in hemoglobin leads to increased blood volume,
splenomegaly, bone marrow expansion, facial deformities, osteomalacia, bone splenomegaly, bone marrow expansion, facial deformities, osteomalacia, bone changeschanges
• Iron buildup due to transfusions requires chelation therapy to remove excess ironIron buildup due to transfusions requires chelation therapy to remove excess iron

Medical and Nutritional Management of Anemia• It is important to be familiar with the It is important to be familiar with the
etiology and treatment of nutritional and etiology and treatment of nutritional and non-nutritional anemiasnon-nutritional anemias
• Many non-nutritional anemias have Many non-nutritional anemias have nutritional implicationsnutritional implications
• It is critical to DIAGNOSE before treating It is critical to DIAGNOSE before treating anemias with nutritional or non-nutritional anemias with nutritional or non-nutritional therapiestherapies