
Knowledge for Print
58
ตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตตต Chemistry ตตตตตตตตตต ตตตตตตตตต(Critical values) ตตตตตตต(low) ตตตตตต(high) - Blood gases, ผผผผผผผ - pH <7.20 > 7.58 - pCO2 < 19 mmHg > 61 mmHg - pO2 < 43 mmHg > 350 mmHg - Blood Gases, ผผผผ - pH < 7.25 > 7.50 - pCO2 < 30 mmHg > 50 mmHg - pO2 < 50 mmHg > 90 mmHg - Bilirubin, newborn (under 30 days old) ผผผผผ > 15 mg/dl - BUN ผผผผผ > 100 mg/dl - Calcium, ionized < 0.8 mmol/L > 1.54 mmol/L - Calcium, total < 7.0 mmol/L > 13 mmol/L - Carbon Dioxide < 5 mmol/L > 38 mmol/L - Creatinine ผผผผผ > 7.4 mg/dl - Glucose, ผผผผผผผ < 45 mg/dl > 500 mg/dl - Glucose, ผผผผ < 30 mg/dl > 325mg/dl - Glucose, CSF < 20 mg/dl ผผผผผ - Magnesium < 1.0 mg/dl > 4.9 mg/dl - Osmolality,serum < 240 mOsm/kg > 330 mOsm/kg - Phosphorus < 1.0 mg/dl ผผผผผ - Potassium < 3.0 mmol/L > 6.0 mmol/L - Sodium < 120 mmol/L > 160 mmol/L - Troponin T ผผผผผ > 0.1 ng/ml - Uric acid ผผผผผ > 13 mg/dl Hematology ตตตตตตตตตต ตตตตตตตตต(Critical values)
-
Upload
guitaryada-pyharnvichitnooch -
Category
Documents
-
view
271 -
download
10
Transcript of Knowledge for Print

ตารางแสดงคาวกฤตหองปฏบตการทางการแพทย
Chemistryรายการตรวจ
คาวกฤต(Critical values)คาตำ�า(low) คาสง(high)
- Blood gases, ผใหญ - pH <7.20 > 7.58 - pCO2 < 19 mmHg > 61 mmHg - pO2 < 43 mmHg > 350 mmHg- Blood Gases, ทารก - pH < 7.25 > 7.50 - pCO2 < 30 mmHg > 50 mmHg - pO2 < 50 mmHg > 90 mmHg- Bilirubin, newborn (under 30 days old) ไมม > 15 mg/dl
- BUN ไมม > 100 mg/dl- Calcium, ionized < 0.8 mmol/L > 1.54 mmol/L- Calcium, total < 7.0 mmol/L > 13 mmol/L- Carbon Dioxide < 5 mmol/L > 38 mmol/L- Creatinine ไมม > 7.4 mg/dl- Glucose, ผใหญ < 45 mg/dl > 500 mg/dl- Glucose, ทารก < 30 mg/dl > 325mg/dl- Glucose, CSF < 20 mg/dl ไมม- Magnesium < 1.0 mg/dl > 4.9 mg/dl- Osmolality,serum < 240 mOsm/kg > 330 mOsm/kg- Phosphorus < 1.0 mg/dl ไมม- Potassium < 3.0 mmol/L > 6.0 mmol/L- Sodium < 120 mmol/L > 160 mmol/L- Troponin T ไมม > 0.1 ng/ml- Uric acid ไมม > 13 mg/dl
Hematologyรายการตรวจ
คาวกฤต(Critical values)คาตำ�า(low) คาสง(high)

- Hematrocrit - ผใหญ <18% > 61% - ทารก < 33% > 71%
- Platelet < 20,000/cu.mm>
1,000,000/cu.mm
- Differential พบ blast cell- Malaria smear Positive- WBC - ผใหญ < 1,500/cu.mm > 30,000/cu.mm - ทารก < 5,000/cu.mm > 25,000/cu.mm- Prothrombin Time(PT) ไมม INR > 5- Partial thromboplastin time ไมม > 120- Thromboplastin time (TT) ไมม > 27 sec
- Fibrinogen < 100 mg/dL ไมม
Microbiologyรายการตรวจ คาวกฤต(Critical values)
- Acid fast smear Positive- Blood and CSF cultures Positive- Cryptococcal antigen Positive
1. จากเวบไซต International Federation of Clinical Chemistry and Laboratory Medicine(IFCC),http://www.ifcc.org
2. จากเวบไซต Massachusetts General Hospital, http://mghlabtest.partners.org
3. จากเวบไซต University of Washington, http://www.washington.edu/
การเพาะเชอจากระบบสบพนธ
การเพาะเชอในระบบสบพนธ เชอทเปนสาเหตของการตดเชอในระบบสบพนธ มหลาย

ชนด แตทพบไดคอ Neisseria gonorrhoeae ซงเปนสาเหตของโรค หนองใน โดยทวไปผปวย จะมอาการปสสาวะขด ปวดแสบปวดรอนขณะปสสาวะ ตอมามหนองไหลออกมาจากทอปสสาวะหรอปากมดลก
Specimen
ในผหญง Abscess aspirate Amniotic fluid Amniocentesis fluid Cervical, endocervical swab Cesarean-section swab Ulcer genital aspirate Urethral swab Vagina,vulvar swab
ในผชาย Abcess aspirate Discharge,penile Prostatic secretion Ulcer genital aspirate Urethral
Normal flora ในระบบสบพนธ
- Corynebacterium spp. - Coagulase negative staphylococcus - Various nonphathogenic neisseria - Various enteric gram negative rod - Mycoplasma - Enterococci - Anaerobic streptococci - Anaerobic gram negative rod
แบคทเรยกอโรคในระบบสบพนธ
- Neisseria gonorrhoeae - Treponema pallidum - Staphylococcus aureus- Haemophilus ducreyi - Gardnerella vaginalis - Group B streptococci- Chlamydia trachomatis - Listeria monocytogenes - Mycoplasma hominis Other not bacteria- Candida albicans - Trichomonas vaginalis ( microscopic examination) Microscopic examination
การตร ว จขนตนดวยกลองจลทรรศน
มประโยชนมากในการชวยวนจฉยการตดเชอในระบบสบพนธเชน การยอมแกรมชวยวนจฉยการตดเชอ Neisseria gonorrheae การด wet smear ชวยวนจฉยการตดเชอ Trichomonas

vaginalis และ Budding yeast cells ไดโดยมหลกการวนจฉย สงสงตรวจดวยการดดวยกลองจลทรรศนดงน
- ในผปวยชาย การยอมแกรมมประโยชนมากในการวนจฉย Urethritis โดยถาพบ PMN > 10 cells/ OF และพบ Gram negative diplococci ในเมดเลอดขาว (Gram negative diplococci intracellular) กจะสามารถวนจฉยไดวาผปวยเปนหนองในซงใหความถกตองสงถง 98 % - ในผปวยหญง wet smear หนองจากชองคลอดชวยวนจฉย vaginitis ไดอาจตรวจพบ Trichomonas vaginalis , Budding yeast cells หรอ Clue cells ได Gram stain ชวยวนจฉย Bacterial vaginosis โดยจะพบเมดเลอดขาว > 5 cells/ OF และพบ clue cells จำานวนมาก ในขณะ ท lactobacilli ลดจำานวนลง ถานำาสงสงตรวจจากปากมดลกมายอมแกรมแลวพบเมดเลอดขาว > 10 cells/OF แสดงวาผปวย นาจะเปน cervicitis ซงสาเหตสวนใหญเกดจาก Neisseria gonorrhoeae หรอ Chlamydia trachomatis
เชอท�มกพบเปนสาเหตการตดเชอในระบบสบพนธในเพศชาย
1.gonococcal urethritis - Neisseria gonorrhoeae2. nongonococcal urethritis - Chlamydia trachomatis
- Trichomonas vaginalis
เชอท�มกพบเปนสาเหตการตดเชอในระบบสบพนธในเพศหญง
Vaginitis - Neisseria gonorrhoeae - Chlamydia trachomatisVaginosis - Anaerobic bacteria - Gardnerella vaginaliscervictis - Neisseria gonorrhoeae - Chlamydia trachomatis - Trichomonas vaginalis - Staphylococcus aureus
- Group B streptococci (มความสำาคญใน หญงตงครรภใกลคลอดเพราะเปนสาเหตของneonatal infection)
- Listeria monocytogenes - Clostridium spp. ( สาเหตของ septic abortion)
*** การวนจฉย bacterial vaginosis ตองตรวจพบลกษณะดงน
- Vaginal pH > 4.5

- lactobacilli ลดลง- มการเพมขนของ clue cells ( gram -negative coccobacilli เลกๆตดอยท epithelial cells)- WBC >5 cells/ OF
ขนตอนการเพาะเชอ
1. Streak specimen ลงบน chocolate agar,modified Thayer- Martin,blood agar และ MacCongkey agar
2. Incubate chocolate agar,modified Thayer- Martin,blood agar ท 35-37 ำ C 5% CO2 จนครบ 3 วน ถาไมมเชอขนรายงาน No growth ถามเชอขนแยกชนดของเชอ และรายงานปรมาณเชอ ชนดของเชอ และผลการทดสอบความไวของเชอตอสารตานจลชพ สำาหรบเชอทมความสำาคญ
ไขเลอดออก(Dengue Haemorrhagic Fever)
โดย ทนพ.จรญ ปตตาโน
เชอ Dengue virus มสารพนธกรรมเปน RNA สายเดยว สายบวก มขนาด 40-60 nm อยใน genus Flavivirus, Family Flaviviridae ซงใน Family Flaviviridae ประกอบดวย 3 genus คอ
1. Genus Flavivirus - Dengue virus ทำาใหเกดโรคไขเลอดออก - Japanese Encephalitis(JE) virus ทำาใหเกดโรคไขสมองอกเสบ - Yellow fever(YF) virus ทำาใหเกดโรคไขเหลอง
2. Genus Pestivirus ไดแกเชอ Bovine viral diarrhea virus
3. Genus Hepacivirus ไดแกเชอ Hepatitis C virus
เชอไขเลอดออกประกอบดวย 4 serotype คอ DEN1,DEN2,DEN3 และ DEN4 โดยทง 4 serotype ม antigen บางชนดรวมกน ทำาใหเกด cross-reaction ไดแตไมถาวร เมอตดเชอ serotype หนงแลวจะมภมคมกนตอ serotype

นนตลอดชวต แตจะไมปองกน serotype อนได
นอกจากน antibody ของเชอ Dengue virus ยงมคณสมบตเปน Enhancing antibody คอ เมอเราตดเชอครงแรกแลว การตดเชอครงตอไป antibody ในรางกายเราจะสงเสรมการตดเชอไดมากขนดวย เกดขบวนการ Antibody-dependent enhancement โดย antiody ทจำาเพาะตอเชอไวรสจะจบกบอนภาคของไวรสเขาสเซลลผานตวรบของ antobody(Immunoglobulin receptor/FC receptor)
การตดตอ
ตดตอกนโดยมยงลายบานตวเมย(Aedes spp.) เปนพาหะ โดยผปวยจะถกกดโดยยงลายทมเชอ
อาการ

การตดเชอ dengue virus จะพบอาการทางคลนคไดดงน
1. ตดเชอโดยไมมอาการ
2. มอาการไขแยกจากสาเหตอนไดยาก(undifferentiated viral syndrome) มอาการคลายคลงกบการตดเชอไวรสอนๆ ไมสามารถวนจฉยจากอาการทางคลนคได จะมไข 2-3 วน บางครงอาจมผนแบบ macrolopapula rash
3. ไขแดงก (Dengue fever,DF) มกเกดกบเดกโตหรอผใหญ อาจมเพยงไขหรอ มอาการแดงกชดเจนคอ ปวดศรษะ มไขสงเฉยบพลน ปวดกลานเนอตามตว ปวดขอ ปวดเบาตา บางรายอาจมเลอดออกทผวหนง สวนใหญจะพบเมดเลอดขาวตำา บางรายอาจพบเกลดเลอดตำา เมอทำาการทดสอบ touniquet test จะใหผลบวกทชดเจน
4. ไขเลอดออก(dengue haemorrhagic fever,DHF) ไขเลอดออก(DHF) ตางจากไขแดงก(DF) คอมการรวของพลาสมา(leakage of plasma) อาการเรมจากมไขสงทนท ไขมกสงลอย เบออาหาร อาเจยน ปวดทอง ปวดศรษะ อาการ 2-3 วนแรกจะคลายกบไขแดงก(DF) อาการจะรนแรงทสดในชวงวนท 2-7 พบจดมเลอดออกเลกๆ กระจายตามลำาตว และใบหนา บางรายอาจมเลอดำาเดาออกอาเจยนเปนเลอด หรอปสสาวะเปนเลอด เมอทำา touniquet test จะใหผลบวกทชดเจน ลกษณะอาการทเดนชด 4 ประการ คอ ไขสงเฉยบพลน เลอดออก ตบโต และมอาการชอค(Dengue Shock Syndrome,DSS) ในรายทมอาการชอคเกดจากระบบหมนเวยนโลหตลมเหลว เนองจากมการรวของพลาสมา โดยพบวาผนงของหลอดเลอดฝอยม permeability เพมขน เกดการรวของพลาสมาเขาส serous space พบ albumin ตำา ปรมาตรเลอดของผปวยลดลง เกด hypovolumic shock สามารถดไดจากคา Hct ทสงขน จากการศกษาพบวา DHF สวนใหญจะเปน secondary infection เพราะผปวยจะม antibody จากการตดเชอครงแรก(primary infection) ทำาใหเกดการสงเสรมการตดเชอไดมากขน(antibody-dependent enhancement) สวนการตดเชอครงแรก(primary infection) จะมอาการไมรนแรง สวนใหญจะหายเอง ในทำานองเดยวกนในเดกเลกทอายตำากวา 1 ป จะม antibody IgG ของเชอ dendue virus ทผานรกจากแมมาจำานวนหนง ซงเปน passive dengue IgG antibody แตมปรมาณนอยไมาสามารถปองกนโรคไดแตสามารถทำาใหเกด antibody-dependent enhancement ไดเชนกน

พยาธสภาพของ DHF
จากรปภาพขางบนสามารถสรปพยาธสภาพโดยรวมของ DHF คอ
1. มไขสงลอยตลอดเวลา
2. เมอทำา tourniquet test จะ positive โดยพบเปนจดเลอดออก ตามตว แขนขา และใบหนา
3. มการเพมขนของ permeability ของผนงหลอดเลอด เกดการรวของพลาสมา ทำาใหปรมาตรเลอดลดลงเกด hypovolaemia ซงจะทำาใหอาการชอค และอาจเสยชวตได
4. มตบโต(hepatomegaly) จะคลำาไดในวนท 3-4 ของโรค แตไมพบ jaudice
5. มเกลดเลอดตำา(thrombocytopenia) เกดความผดปกตของการแขงตวของเลอด(coagulopathy) ทำาใหเกดการแขงตวในหลอดเลอด(Dessiminated Intravascular Coaglulation,DIC)

ระดบความรนแรงของ DHF สามารถแบงไดเปน 4 grade คอ
- Grade I มไขและมอาการรวมอนๆแตไมจำาเพาะ แตเมอทำา tourniquet test จะใหผล positive
- Grade II อาการเหมอน grade I แตทเพมเตมคอ พบเลอดออกเปนจดเลอดใตผวหนง
- Grade III ระบบไหลเวยนโลหตเรมลมเหลวเกดอาการชอค ชพจรเรว เบา pulse pressure แคบ ความดนโลหตตำา รมฝปากเขยว ตวเยน กระสบกระสาย
- Grade IV แสดงอาการชอครนแรง ความดนโลหตและชพจรวดไมได
การตรวจทางหองปฏบตการ
1. การตรวจ tourniquet test(TT) คอ วธการวดความดนโลหตดวยเครองวดทมขนาด cuff พอเหมาะ กบขนาดตนแขนสวนบนของผปวย คอครอบคลมประมาณ 2 ใน 3 ของตนแขน บบความดนไว ทกงกลางระหวาง systolic คอ ความดนระยะหวใจบบตว ความดนเลอดในขณะทหวใจบบตวเพอสบฉดโลหตออกไปเลยงรางกาย และ diastolic pressure คอ ความดนระยะหวใจคลายตว ความดนเลอดในขณะทหวใจคลายตว หลงจากทหวใจบบตวเพอสบฉดโลหตออกไปเลยงรางกายแลว ความดนเลอดขณะหวใจคลายตวมคานอยกวาความดนเลอดระยะหวใจบบตว รดคางไวประมาณ 5 นาท หลงจากนนจง คลายดน รอ 1 นาทหลงคลาย ความดนจงอานผลการทดสอบ ถาตรวจพบจดเลอดออก เทากบหรอมากกวา 10 จดตอตารางนวถอวา ใหผลบวก ใหบนทกผลเปนจำานวน จด ตอตารางนว ทงรายทใหผลบวกและรายทมนอยกวา 10 จด
พบวา sensitivity ของ tourniquet test อยท 53%, 91% และ 99% ของวนท 1,2 และ 3 ตามลำาดบ และมความจำาเพาะ specipicity อยทประมาณ 75% ทงน tourniquet test สามารถทำาใหเกดผลบวกปลอม(false positive) ไดเชนกน โดยอาจจะเกดจากการตดเชอไวรสตวอน
2. Complete Blood Count(CBC)
2.1 White Blood Cell(WBC) สวนใหญจะพบเมดเลอดขาวปกตหรอตำาลง ซงเกดจากภาวะ active hemophagocytosis โดยระยะ 1-3 วนแรกจะพบวา lymphocyte ตำาลง ทำาใหเกด

ภาวะ relative neutrophilia และ absolute lymphopenia แตหลงจากนเมดเลอดขาวชนด granulocyte จะตำาลงในชวงวนท 3-8 จะพบภาวะ relative lymphocytosis และ absolute neutropenia และจะพบ atypical lymphocyte ประมาณรอยละ 15-35%
รปแสดง atyphical lymphocyte
2.2 Hematocite(Hct) และ Hemoglobin(Hb) คา Hct มกสงเกนกวา 40% บางรายอาจพบสงถง 50-60% สวนคา Hb จะพบวาสงมากกวา 14 g/dl ซงคา Hb และ Hct ทสงขนเกดจากการรวของพลาสมา การตรวจ Hct เปนระยะสามารถเฝาตดตามอาการของผปวยได
2.3 Platelet ผปวยจะมเกลดเลอดตำาลงประมาณวนท 3 โดยสวนใหญจะตำากวา 100,000/cu.mm เกลดเลอดจะสงขนหลงจากวนท 7 ไปแลว และจะเขาสภาวะปกตในวนท 9-10 ซงสาเหตททำาใหเกลดเลอดตำาลงคอ - มการกดไขกระดก ทำาใหเซลลในไขกระดกมจำานวนนอยและการเจรญเตบโตหยดอยชวขณะ(maturation arrest) ทสำาคญคอ ม maturation arrest ของ megakaryocyte - ในไขกระดกมการสราง small lymphocyte,monocyte, reticulum cell และ histocyte เพมมากขน ซงอาจเปนไปไดวาเซลลเหลานมการจบกน platelat มากขน - ระบบ immune complex ทเกดขนอยางมากในผปวย DHF อาจทำาให platelet มการ absorb เอา antibody ไวผนงของ platelet ไวมาก ซงทำาให platelet ถกจบกนโดยตบและมาม
3. การตรวจ chemistry
3.1 Albumin ในกระแสเลอดมปรมาณลดลง เนองมาจากมการรวของพลาสมา ในราย

ทรนแรงจะมคา albumin ตำามาก อตราสวน A:G (albumin:globulin) นอยกวา 1
3.3 SGOT,SGPT สงขน และจะสงมากในรายทรายแรง ซงอาจมสาเหตมาจาก anoxia และมการทำาลายเซลลตบ
3.4 ALP, GGT และ bilirubin ปกต
3.5 Electrolyte พบวามภาวะ hyponatremia คอ มระดบ sodium(Na+) และ chloride(Cl-) ตำา และจะมความรนแรงอยางมากในภาวะชอค ซงมสาเหตมาจาก มการอาเจยน เหงอออกมาก และเบออาหาร นอกจากนยงพบวามระดบ ของ CO2 ในกระแสเลอดตำาลงมาก
4. การตรวจหา antibody ตอเชอ dengue virus
4.1 Primary infection ในการตดเชอครงแรกรางกายจะสราง antibody ตอเชอไวรส โดยพบ - IgM จะถกสรางประมาณวนท 5 หลงจากมอาการ และสงนานประมาณ 1-3 สปดาห บางครงอาจจะอยไดนานถง 60 วน - IgG จะตรวจพบประมาณวนท 14 และจะอยนานตลอดชวต
4.2 Secondary infection - IgM จะถกสรางหลงจากตดเชอประมาณ 20 วน จะพบในปรมาณตำา หรอบางครงไมสามารถวดได หรมระยะเวลาทอยในกระแสเลอดนอยกวา primary infection - IgG จะสงขนภายในวนท 1-2 หลงจากทมอาการและจะพบในปรมาณสงกวา primary infection และจะอยสงนาน 30-40 วน
5. การตรวจ Dengue NS1 antigen
Dengue NS1 antigen จะถกสรางตงแตวนแรกหลงจากมอาการไขและจะสงนานประมาณ 9 วน โดยจะพบไดทง primary และ secondary infection ปจจบนเปนทนยมใชตรวจหาเชอ dengue virus ในวนแรกๆ
รปแสดงการเกด immune response ตอเชอ dengue virus

ทมาของรป: www.panbio.com
Laboratory Evaluation of Infectious Disease EmergenciesStephen G. Baum
A6420
The diagnostic work-up of any serious infection constitutes an emergency. The most innocuous-appearing respiratory
infection can proceed to fatal meningitis in a matter of hours, and minor urinary tract symptoms can herald a syndrome
of overwhelming sepsis. Recent publications have emphasized the development of new laboratory culture techniques for
the rapid identification of infectious agents. At best, these techniques require several hours and are susceptible to many
artifacts of specimen collection and storage prior to the time the sample reaches the laboratory.
Accurate assessment of the probable causes of serious infection can be made by the examining clinician within minutes
to an hour after first seeing a febrile patient. This is accomplished by coupling carefully selected history and physical
features with the proper collection of specimens and the use of a few simple staining techniques. The goal of this rapid

diagnostic work-up is elucidation of the causative organism, allowing use of the fewest possible antibiotics that combine
the proper antimicrobial spectrum with the least toxicity to the patient.
The choice of the right therapeutic agent is extremely important for several reasons. First, infections constitute the only
medical conditions that may be susceptible to true cure rather than amelioration. Second, bacteria may develop
resistance to an antibiotic with a frequency roughly proportional to the degree to which the antibiotic is used. Therefore,
injudicious use of broad-spectrum antibiotics may shorten the time during which they remain useful by hastening the
evolution of a new population of resistant microorganisms. Third, use of broad-spectrum antimicrobial therapy perturbs
the normal flora, promoting overgrowth of opportunistic organisms such as fungi. The physician treating a patient with
an infectious disease therefore has the capacity to alter the pathogenesis of diseases not only in the patient but also in
the hospital population and the community at large. The emergent nature of infections, the possibility of bringing about
real cure, and the potential ill effects of antibiotic misuse make it incumbent upon the physician to ascertain the etiology
of the infection rapidly and accurately, and to use the narrowest spectrum of effective drugs.
The prime prerequisite for accurate laboratory work-up of any infectious disease is proper collection of appropriate
specimens. Infectious disease consultants are frequently asked to review "sputum" specimens used in the initial
diagnosis of a patient who has not responded well to therapy, only to find saliva rather than sputum. Whether used for
staining and microscopic examination or for culture, specimens must be collected properly. Following is a discussion of
the laboratory work-up of four commonly analyzed specimens: cerebrospinal fluid, sputum, urine, and blood. Many of the
techniques described for collection and processing of these samples are also valid for specimens such as synovial and
pleural fluid.
Analysis of Cerebrospinal Fluid in Central Nervous System Infection
DefinitionThe physician must have a low threshold for the performance of a lumbar puncture (LP) in cases of suspected
meningitis. In children, the presence of fever, stiff neck, headache, and irritability are obvious justifications for an LP,
while in the aged patient a stiff neck is frequently not found and fever accompanied by confusion or clouded sensorium
may be the only signs of meningitis. If there is clinical evidence for increased intracranial pressure, a CT scan of the
head should be performed before the LP.
Technique

The patient should be placed horizontally on a firm surface with the neck, legs, and back flexed in fetal position. The
back should then be surgically prepared first with 70% alcohol and then with iodine. Start at the point the needle will
enter and swab in a spiral motion, extending laterally to the flanks, cephalad to the midback, and caudad to the coccyx.
This should be repeated twice, using fresh swabs saturated with iodine solution each time. Skin irritation from iodine
may be reduced by thoroughly washing the back with alcohol at the end of the procedure.
After donning gloves, local anesthetic is introduced into the interspace between the second and third lumbar vertebrae.
The exact positioning of the LP needle and method of its introduction are described in neurology or neurosurgery
textbooks.
Several tubes should be available for the collection of cerebrospinal fluid (CSF). These should include a tube collected
first for culture (0.5 to 1 ml) and others for chemical assay of protein and sugar (1 to 2 ml), serologic test for syphilis (1
ml), and, most important, a tube for gross inspection, microscopic cell count, differential cell count, and gram stain (1 to
2 ml). An additional tube of CSF should be saved for future assays.
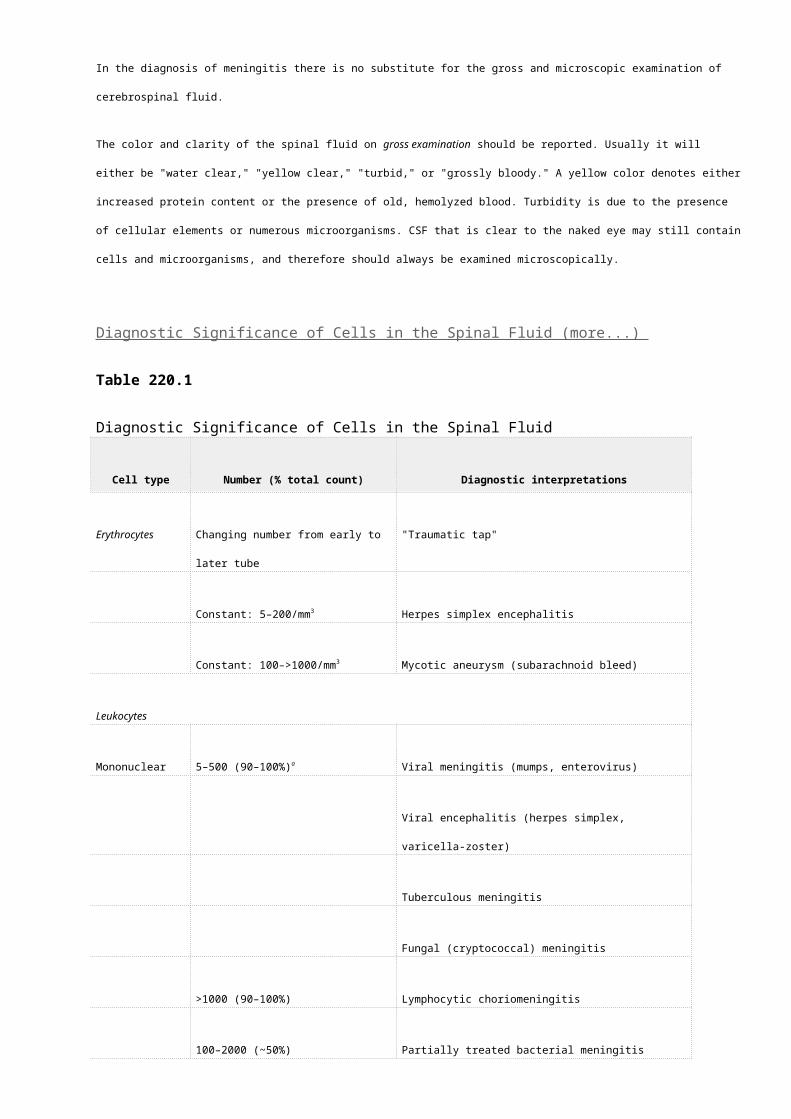
Clinical SignificanceIn the diagnosis of meningitis there is no substitute for the gross and microscopic examination of cerebrospinal fluid.
The color and clarity of the spinal fluid on gross examination should be reported. Usually it will either be "water clear,"
"yellow clear," "turbid," or "grossly bloody." A yellow color denotes either increased protein content or the presence of
old, hemolyzed blood. Turbidity is due to the presence of cellular elements or numerous microorganisms. CSF that is
clear to the naked eye may still contain cells and microorganisms, and therefore should always be examined
microscopically.
Diagnostic Significance of Cells in the Spinal Fluid (more...)
Table 220.1
Diagnostic Significance of Cells in the Spinal Fluid
Cell type Number (% total count) Diagnostic interpretations
Erythrocytes Changing number from early to later
tube
"Traumatic tap"
Constant: 5–200/mm3 Herpes simplex encephalitis

Cell type Number (% total count) Diagnostic interpretations
Constant: 100–>1000/mm3 Mycotic aneurysm (subarachnoid bleed)
Leukocytes
Mononuclear 5–500 (90–100%)a Viral meningitis (mumps, enterovirus)
Viral encephalitis (herpes simplex, varicella-zoster)
Tuberculous meningitis
Fungal (cryptococcal) meningitis
>1000 (90–100%) Lymphocytic choriomeningitis
100–2000 (~50%) Partially treated bacterial meningitis
Brain abscess
Polymorphonucl
ear
5–2000 (>80%) Bacterial meningitis (expect to see organisms on
gram stain)
100–2000 (~50%) Partially treated bacterial meningitis
Very early, polymorphonuclear leukocytes may outnumber mononuclear cells.
On microscopic examination, white blood cells (WBC) should be enumerated in a standard WBC counting chamber using
CSF that is fresh and has not been centrifuged. If cells are seen, no attempt should be made to differentiate cell types in
the counting chamber. Even with the addition of a dye such as methylene blue, this method of differential counting is
fraught with error. The fluid should then be centrifuged and the differential count done as soon as possible on the pellet,
if visible, or on the bottom-most drop of CSF if there is no visible pellet. The drop of sedimented fluid is placed on a clean
slide. It is not smeared, but is allowed to air dry. Two such preparations are made; one is heat fixed for gram stain and
the other Wright stained for the differential count. An accurate differential can often be obtained from the gram-stained
material. Interpretations of the WBC count and differential are given in Table 220.1. These are rough indices, and there
is much overlap in counts and differentials between diseases.
Red blood cells (RBC) may be present in the CSF as a result of infectious or noninfectious processes involving the brain
or subarachnoid space, or may be introduced into the CSF as a result of the lumbar puncture. The latter occurrence is
called a "traumatic tap." This term does not imply that any difficulty was encountered in performing the spinal tap, but
rather that a capillary was entered in the process, thereby carrying blood into the CSF. That this event has occurred is
evidenced by a change in the amount of blood (either an increase or decrease) when a tube collected at the start of the
LP is compared with one collected later in the procedure. If blood is apparent to the naked eye, this comparison can be
made grossly. If blood is visible only under the microscope, counts must be done on an early and later tube. A constant
amount of blood in all tubes indicates that the bleeding occurred before the LP. Infectious implications of blood in the
CSF are given in Table 220.1.
Table 220.2
Microorganisms in the Cerebrospinal Fluid
Table 220.2
Microorganisms in the Cerebrospinal Fluid

Microorganisms may be detected by gram stain or India ink preparations. The etiology of over 80% of cases of bacterial
meningitis can be determined by examining a gram-stained specimen of CSF. This procedure can be performed in 2
minutes and should never be left to a laboratory technician to be done later. The findings from the rapid method of gram
staining are shown in Table 220.2 together with description and interpretation of some of the more common organisms
that cause meningitis. For the India ink test, to one drop of sediment from centrifuged CSF on a slide, add one drop of
ink. Cover the wet preparation with a coverslip and examine under "high dry" magnification. The finding of budding
organisms, visible as bright spots in a "figure-eight" configuration against the dark background of india ink, indicates the
presence of cryptococci (See Table 220.2). In the absence of budding, other visible elements should not be called
cryptococci.
CSF for culture should be taken to the bacteriology laboratory as soon as possible. Pending culture, CSF can be stored in
an incubator to maximize the viability of any organisms present.
Analysis of Sputum in Respiratory Tract Infection
DefinitionGram stain of the sputum is perhaps the most accurate way of diagnosing pulmonary infections. Because there are
always organisms in the nasopharynx, culture of the sputum will often appear positive for some bacterial

microorganism. This culture positivity may be misleading in cases of influenza, mycoplasma, or legionella pneumonia. In
contrast, when anaerobes are the etiologic agents, as in aspiration pneumonia, their presence will not be revealed by
routine sputum culture techniques. Examination of gram-stained sputum will demonstrate whether a bacterium is
present as a predominant species and whether the sputum contains polymorphonuclear leukocytes suggestive of a
bacterial infection. The presence of numerous large squamous cells, even when these are filled with bacteria, indicates
that the specimen has been contaminated with saliva and is therefore inappropriate for diagnostic purposes.
TechniqueSputum can be collected either as a freshly coughed-up specimen or via aspiration through a nasotracheal tube
following rapid instillation of 5 to 10 ml of normal saline. Transtracheal aspiration is only rarely necessary to obtain
sputum.
A sample of sputum is spread on a slide with an applicator stick or by compressing the specimen between two slides.
After the specimen has dried in air, it is heat fixed and gram stained as described for CSF, with one exception. A sputum
specimen will have thick and thin areas. If one attempts to decolorize the thick areas completely, the thin areas may be
over-decolorized. Therefore, one should leave the thickest areas of the sputum blue.
Clinical Significance
Diagnostic Significance of Findings on Sputum Gram (more...)
Table 220.3
Diagnostic Significance of Findings on Sputum Gram Stain
Stain findings Interpretation
Gram-positive diplococci & PMNs Pneumococcal pneumonia
Gram-positive cocci in clusters & PMNs Staphylococcal pneumonia
Gram-negative coccobacilli & PMNs Hemophilus influenzae pneumonia
Gram-negative fat rods with bipolar staining & Klebsiella pneumonia

Stain findings Interpretation
PMNs
Gram-negative slender rods & PMNs Enterobacteriacea, pseudomonas pneumonia
Gram-negative diplococci & PMNs Branhamella catarrhalis pneumonia (rarely,
meningococcal)
Mixed gram-positive and -negative cocci and rods
& PMNs
Aspiration pneumonia
Few bacteria seen; many PMNs or mononuclear
cells
Influenza, mycoplasma, or legionella pneumonia
Mixed organisms with squamous cells Specimen contaminated with saliva
PMNs = polymorphonuclear leukocytes.
When examined under the microscope, the best area in which to search for organisms is one where the nuclei of the
leukocytes are pink. In cases of bacterial pneumonia, one should note many polymorphonuclear leukocytes and a
marked preponderance of one morphologic type of organism; that is, in pneumococcal pneumonia, one should see only
gram-positive diplococci to the exclusion of almost all other bacterial forms. An exception occurs in cases of aspiration
pneumonia, in which one sees many different types of organisms indicative of the many types that have been aspirated
from the mouth. The implications of different patterns seen on sputum gram stain are given in Table 220.3.
Analysis of Urine in Urinary Tract Infection
DefinitionExamination of urine for the presence of infection involves the finding of WBCs and/or bacteria. Unlike CSF, the urine
usually contains some WBCs and is easily contaminated with bacteria. Hence, proper assessment requires special steps
in the collection, preparation, and storage of the specimen. Using a few simple techniques, one can show that a urinary
tract infection exists and make an educated guess at the probable offending organism, and therefore at the appropriate
therapy. By repeating these procedures 24 hours after the start of treatment, one may also decide if the chosen therapy

has been effective. In many cases, all of this can be accomplished before the microbiology laboratory has reported the
results of the initial culture.
TechniquePatients from whom urine is to be examined for the presence of infection fall into two groups: those with and without
indwelling urinary catheters. In patients without catheters, a midstream clean-voided specimen is recommended. The
periurethral area should first be cleansed with a soap solution to get rid of contaminating resident flora, then rinsed with
sterile water or saline to avoid the antibacterial effects of the soap when the urine is cultured. To avoid contamination of
the urine by feces in female patients, it is essential that cleansing of the periurethral area be done from the urethral
meatus toward the perineum and never in the reverse direction. In the male, it is important to retract the foreskin, if
present, before cleaning the periurethral area. Cleansing agents other than soap, such as those containing
hexachlorophene (e.g., pHi-so-Hex) and quaternary ammonium compounds (e.g., Zephiran) should be avoided. The
former may dry out the urethra, making it susceptible to infection, and the latter are easily contaminated with
pseudomonas. The importance of a midstream specimen is that the initial voiding washes out bacteria that normally
reside in the distal urethra. In patients who cannot cooperate, urine may have to be obtained by passing a temporary
catheter. This should be done using sterile technique and the cleansing procedures detailed above.
In the patient with an indwelling catheter, the proper method of obtaining urine is to swab the port with alcohol and
aspirate urine using a sterile syringe. If no port is provided, a syringe and small-gauge needle can be used. In this case
the distal rubber part of the closed drainage system should be cleaned with an alcohol pledget, and the rubber tubing
should then be punctured and urine withdrawn. Make sure that the lumen of the tube draining the bladder is entered
rather than the tube lumen that leads to the inflated balloon. To ensure this, the catheter must be punctured distal to
the bifurcation or trifurcation. The tubing system should never be disconnected to obtain urine, as the "closed" modern
urine collection systems play a major role in preventing infection in catheterized patients. The plastic part of the
draining system should not be punctured because it will not self-seal. Urine for diagnosis of infection should never be
obtained from the collection bag. This urine is not fresh and is often contaminated with bacteria, regardless of the
presence or absence of urinary tract infection.
Figure 220.1
Gram-stain technique.

Figure 220.1
Gram-stain technique.
The urine should not be centrifuged before the gram stain. The gram stain is prepared as follows. A drop of unspun urine
is placed on a clean slide and allowed to dry without smearing. The specimen is then heat fixed and stained as described
for CSF (Figure 220.1 ). An approximation of WBCs is
usually made by centrifuging the urine and examining a drop of sediment under the high dry objective of the microscope
without prior staining.
After staining, urine should be sent for culture to confirm the presence, type, and number of bacteria. If the urine is not
cultured immediately, it must be stored in the refrigerator so that high colony counts do not merely reflect bacterial
replication after the urine was collected.
Clinical SignificanceA colony count of more than 100,000 (105) organisms per milliliter correlates well with other evidence of infection. It is
unusual to see bacteria on gram stain of the urine unless the organisms number more than 100,000/ml. Putting these
two facts together, if one sees bacteria in gram-stained urine, one can assume that the organisms exceed 100,000/ml
and therefore the likelihood of infection is high.
The two most common bacterial types are gram-negative rods or gram-positive cocci. The latter may be seen in short
chains, signifying that they are streptococci, most probably enterococci. Gram-positive cocci in clusters are probably

staphylococci, and S. saprophiticus is now recognized as a common lower urinary tract pathogen. Gram-negative rods
are usually not further identifiable by gram stain except by experts. Gram-negative cocci may belong to the genus
Acinetobacter.
Exact enumeration of WBCs in the urine is not very helpful in establishing the presence of urinary tract infection. From 1
to 10 WBCs per high power field may be found in noninfected urine; between 10 and 50 is suggestive of infection. Some
studies have indicated that, as with bacterial enumeration, the presence of any WBCs on unspun urine carries clinical
significance.
The speciation of the organism may be useful in identifying its site of origin and whether it is the result of relapse or
reinfection. Further laboratory work-up will also provide information about the antibiotic sensitivity of the organism.
However, one should not necessarily alter the initial therapy if the patient is doing well and if a repeat urine gram stain
fails to reveal organisms. Many antibiotics are concentrated in the urine and are effective even when in vitro sensitivity
tests would predict failure.
The estimation by gram stain of >105 organisms per milliliter of urine yields a high degree of certainty that the patient
has a urinary tract infection. Conversely, not finding this many organisms cannot be used as proof that a patient is free
of infection. The two groups in whom relatively low bacterial counts occur in the presence of infection are females with
lower tract infections (the so-called urethral syndrome) and patients with indwelling urinary catheters. In catheterized
patients the replication time for the organism is decreased because bladder urine exits immediately via the catheter. In
females with lower urinary tract infections, in whom S. saprophiticus is a common pathogen, frequent voiding may
similarly be responsible for relatively lower colony counts. The physician must use clinical criteria, the presence of
pyuria, and sometimes the recurrent finding of low numbers of the same organism to decide if the patient is infected.
Analysis of Blood in Bacteremia
DefinitionDuring the course of many infections, microorganisms enter the bloodstream. In some infected patients, the blood may
be the only site from which organisms can be cultured. Blood cultures should be taken on all hospitalized patients with
severe infections of the urinary tract, lungs, abdominal viscera, bones, central nervous system, or vascular tree.
TechniqueIn infections other than endocarditis, two or three sets of blood cultures are sufficient. When endocarditis is suspected,
five sets of cultures are recommended. Each set of blood cultures (usually two bottles per set: one for aerobic and one

for anaerobic culture) should be from a different venipuncture. Blood cultures should be drawn over a period of several
hours to a day. The practice of drawing one large syringe of blood and aliquoting it into many blood culture bottles is
inadequate. If contamination occurs before the aliquoting, all blood cultures will be positive for the same organism but
this will not have the same diagnostic significance as multiple positive cultures derived from several sites over different
periods of time.
The arms are the preferred site for the drawing of blood cultures. Either the antecubital fossa or a more distal spot may
be used. The area should be prepared first with 70% alcohol and then with an iodine-containing solution, and allowed to
dry before the venipuncture is performed. If it is necessary to palpate the area to locate a vein, the venipuncturist
should either wear sterile gloves or prepare his or her own fingers so as not to contaminate the area. Once the blood is
drawn, it should be transferred to the appropriate bottles without changing needles or swabbing the tops of the bottles
with disinfectant. The needle used in the venipuncture and the bottle tops should be sterile. Any additional handling
increases the chances for contamination or for the introduction of bactericidal material into the culture bottle. Be sure to
place an adequate volume of blood (5–10 ml) in each culture bottle.
Clinical SignificanceRoutine blood cultures will usually permit a diagnosis to be reached. Two additional techniques may prove rapidly useful
in cases of suspected bacteremia. The first is a search for pustular lesions on the extremities. Pustular or acnei-form
lesions are common on the face and trunk of normal uninfected people. However, they are rare on the extremities,
especially on the hands and feet, and may be a clue to bacteremic disease. If found, these lesions should be gently
swabbed with alcohol, unroofed or aspirated with a syringe and needle, and the contents gram stained. If organisms are
identified, an immediate tentative diagnosis can be made. Material can then be sent for confirmatory culture and
determination of antibiotic sensitivity. This approach is useful in cases of gonococcal, meningococcal, and pneumococcal
sepsis.
A second technique is a gram stain of the "buffy coat." When whole blood is centrifuged, as when determining the
hematocrit, the WBCs are concentrated as a white layer at the interface of plasma and erythrocytes. This layer is called
the buffy coat. In the presence of high-level bacteremia, circulating leukocytes may contain phagocytized organisms.
One can break the microhematocrit tube at the area of the buffy coat, express a drop of WBC-rich blood onto a slide,
smear it, and gram stain it. Although this is a low-yield procedure (i.e., it will be positive in about 5% of bacteremias,
more so staphylococcal and meningococcal bacteremias where blood colony counts may be very high), it is easy to do
and can give immediate diagnostic results.
Copyright © 1990, Butterworth Publishers, a division of Reed Publishing

Overview of Hodgkin lymphoma in children and adolescentsLast literature review version 18.1: January 2010 | This topic last updated: May 6, 2009 (More) EPIDEMIOLOGY — Hodgkin lymphoma (formerly called Hodgkin's disease or HL) is a malignant lymphoma with a characteristic epidemiology. Few risk factors, other than those related to viral exposure and immune function, have been convincingly identified. In addition, variation in the incidence, age and sex distribution of HL occurs in different populations according to geographic location, socioeconomic status, and immunologic status. (See "The role of Epstein-Barr virus in Hodgkin lymphoma".)
The distinguishing epidemiologic feature of HL is its bimodal age distribution curve. In the United States and other economically advantaged countries, two incidence peaks exist: one in young adults and one in older age; most patients are young adults (graph 1) [1]. The bimodal age distribution of HL is different in economically disadvantaged areas. An initial peak occurs in childhood for boys, relatively low rates are found in young adults, and a late peak occurs in older adults [2].
In the United States between 1990 and 1995, the annual incidence of HL among children younger than 20 years of age was 12.1 per million; HL was the most common childhood cancer in the 15- to 19-year age group [3]. The overall incidence of HL in children is greater in females than in males (male to female ratio 0.8); however, the sex distribution is age-dependent, with a male-to-female ratio of 0.8, 1.3, and 5.3 among children aged 15 to 19 years, younger than 15 years, and younger than five years, respectively [3]. The incidence of HL is similar among black and white children younger than 10 years of age, but is increased among white children older than 10 years (white to black ratio of 1.4:1) [3].
Familial disease — Familial HL has been estimated to represent 4.5 percent of all cases of HL [4]. This familial association may include shared environmental factors, exposure to viruses, and genetic influences, including inherited immunodeficiency states. (See "The role of Epstein-Barr virus in Hodgkin lymphoma", section on 'Genetic factors' and "Primary humoral immune deficiencies: An overview", section on 'Hyperimmunoglobulin M syndromes'.)
BIOLOGY — HL is a lymphoid neoplasm defined histopathologically by the presence of clonal malignant Hodgkin/Reed-Sternberg (HRS) cells (picture 1 and picture 2) with a variable cellular infiltrate consisting of lymphocytes, eosinophils, macrophages, plasma cells, and fibroblasts. HRS cells, which usually constitute fewer than 1 percent of the cells in involved lymph nodes, secrete an array of cytokines and chemokines, which are important for HRS cell survival and maintenance of the characteristic cellular infiltrate [5]. The biology of HRS cells and their role in HL are discussed separately. (See "The Reed-Sternberg cell and the pathogenesis of Hodgkin lymphoma".)
Epstein-Barr virus (EBV) infection is associated with HL and can be detected in HRS cells. Twenty-five to 50 percent of cases of classical HL in developed countries are EBV positive; the incidence of EBV varies among histological subtypes. (See "The role of Epstein-Barr virus in Hodgkin lymphoma", section on 'Role of Epstein-Barr virus'.)
HISTOLOGY — The WHO classification of lymphomas divides HL into classical HL and nodular lymphocyte predominant HL [6]. (See "Epidemiology, pathologic features, and diagnosis of classical Hodgkin lymphoma".) Patients with nodular lymphocyte predominant HL seem to have a better outcome [7,8], and their treatment may vary from those with classical HL. (See "Clinical manifestations, pathologic features, and diagnosis of nodular lymphocyte-predominant Hodgkin lymphoma".)

Classical HL — Classical HL occurs more commonly (90 to 95 percent of cases) and is subdivided into four subtypes:
Nodular sclerosis (NS) Mixed cellularity (MC)
Lymphocyte depleted (LD)
Lymphocyte rich (LR)
As in adults, NS is the most common form of pediatric HL, representing 70 to 80 percent of cases in adolescents and 40 to 50 percent of cases in children younger than 10 years of age [3]. The incidence of MC decreases with age, from 30 to 35 percent in younger children to 10 to 15 percent in adolescents. LD and LR are rare events, accounting for fewer than 5 percent of all HL cases.
Nodular lymphocyte predominant HL — Nodular lymphocyte predominant HL (NLPHL) accounts for 5 to 10 percent of cases of HL. The malignant cells seen in NLPHL have distinct characteristics which separate them from the more classic Reed-Sternberg cells of HL (table 1). (See "Clinical manifestations, pathologic features, and diagnosis of nodular lymphocyte-predominant Hodgkin lymphoma".)
PRESENTING SYMPTOMS AND SIGNS — Presenting symptoms and signs of HL in children include lymphadenopathy, systemic complaints, and mediastinal mass. HL almost always presents at a site above the diaphragm, with only approximately 3 percent of cases presenting in a subdiaphragmatic location [9].
Lymphadenopathy — Most children with HL present with painless lymphadenopathy, usually cervical, supraclavicular, axillary, or, less often, inguinal. The affected lymph nodes typically feel rubbery and more firm than inflammatory adenopathy; they may be sensitive to palpation if they have grown rapidly. (See "Approach to the child with peripheral lymphadenopathy", section on 'Lymph nodes'.)
Hepatosplenomegaly — Hepatic and/or splenic enlargement may be present in patients with advanced stage HL. (See "Approach to the child with an enlarged spleen".)
Mediastinal mass — Between 17 and 40 percent of children with HL have a mediastinal mass on chest radiograph at the time of presentation. Mediastinal masses are almost always present in association with low cervical or supraclavicular adenopathy. They are more common occurrences among children older than 12 years of age, in whom approximately 30 percent have masses that are greater than one-third the diameter of the intrathoracic cavity. Such "bulky" mediastinal disease may cause dysphagia, dyspnea, cough, stridor, or the superior vena cava syndrome. (See "Malignancy-related superior vena cava syndrome".)
Children with intrathoracic HL rarely present with hypertrophic osteoarthropathy, a syndrome characterized by abnormal proliferation of the skin and osseous tissue at the distal parts of the extremities [10,11]. Clinical features of hypertrophic osteoarthropathy include digital clubbing and periostosis of tubular bones, which usually is accompanied by pain on palpation of the involved area. (See "Malignancy and rheumatic disorders", section on 'Hypertrophic osteoarthropathy'.)
Systemic symptoms — Patients with HL may present with nonspecific systemic symptoms including fatigue, anorexia, and weight loss. Fewer than 20 percent of children with HL have the classic fever and night sweats that are seen in adults. However, these symptoms along with weight loss (ie, "B" symptoms) have important implications for staging and prognosis (table 2). (See "Staging of Hodgkin lymphoma", section on 'Criteria for B symptoms'.)
As in adults, pruritus and alcohol-induced pain, which typically resolve with treatment, have been described [12-16].
Other — Rarely, patients present with autoimmune disorders such as autoimmune hemolytic anemia, thrombocytopenia, or neutropenia [15].
DIFFERENTIAL DIAGNOSIS — The presenting symptoms and signs of HL in children and adolescents may be caused by a variety of diseases and the differential diagnosis includes other malignant, infectious, and inflammatory diseases. They include non-Hodgkin lymphoma, metastatic adenopathy from other primary tumors (eg, nasopharyngeal carcinoma, soft tissue sarcoma), toxoplasmosis, typical and atypical mycobacterium infections, EBV infection, systemic lupus erythematosus, and disorders causing reactive hyperplasia of lymph nodes [17]. (See appropriate topic reviews).
Chest radiographs should be obtained in all patients in whom a diagnosis of HL is being considered. The diagnostic considerations in patients with mediastinal masses depend upon the anatomic compartment in which the mass is located (figure 1). In children, anterior mediastinal mass must be distinguished from normal thymus, which attains maximal size when the child reaches approximately 10 years of age.

Computed tomography (CT) and/or other imaging studies may be necessary to make this distinction [18]. (See "Evaluation of mediastinal masses".)
DIAGNOSTIC EVALUATION — A complete evaluation of patients with suspected HL is mandatory before beginning treatment. The goal is to evaluate the extent of disease, which, in turn, determines the clinical and pathologic stage, treatment, and to a great extent, prognosis.
The evaluation should be undertaken at a center where a team of pediatric oncologists, pathologists, surgeons, radiotherapists, nurses, and social workers are experienced in the diagnosis and care of children with cancer. The superior results of treating children with malignancies in pediatric oncology centers as opposed to community hospitals is well documented [19].
History — The routine evaluation of a patient with suspected HL should include a complete history, with emphasis on constitutional symptoms such as fever, night sweats, weight loss, previous infections, family exposures to toxins, and parental occupational hazards, as well as evidence of underlying immune deficiencies and familial cancer, including HL.
Physical examination — A complete physical examination includes assessment of general health, measurement of height and weight, and documentation of the size and location of lymphadenopathy, liver and spleen size, skin infiltrations, pulmonary findings, and neurologic signs. The tonsils, base of the tongue, and nasopharynx (ie, Waldeyer's ring) must be included in this evaluation.
Tissue biopsy — The diagnosis of HL is established by histologic examination, usually excisional biopsy of an enlarged lymph node that demonstrates malignant "classic" HRS cells or their variants, which may represent only a minority (usually fewer than 1 percent) of the cellular infiltrates [20]. Subclassification of HL depends upon whether the overall pattern is nodular, diffuse, or both, and whether "classic" or variant Reed-Sternberg cells are present, as well as the composition of the cellular infiltrate (eg, non-neoplastic small lymphocytes, eosinophils, plasma cells, fibroblasts, histiocytes, neutrophils, and collagen fibers). (See "Epidemiology, pathologic features, and diagnosis of classical Hodgkin lymphoma".)
Bone marrow aspirates are recommended only for patients with advanced stage disease (Stage III, IV), B-symptoms, or any abnormality on the complete blood count that is suspicious for bone marrow involvement (see 'Staging' below [21].
Advances in diagnostic imaging and the use of systemic chemotherapy in all pediatric HL treatment protocols have made routine staging laparotomy unnecessary. We would consider a laparotomy in patients with one of the following findings to assure accurate staging before therapy (Pediatric Oncology Group [POG] protocols 9425/9426):
Intraabdominal lymph nodes between one and three centimeters (Lymph nodes >3 centimeters are assumed to be positive unless pathology proves them negative.)
Enlargement of the spleen
Focal abnormalities of the spleen
Focal abnormalities of the liver
Areas of uptake in the abdomen on the gallium scan not explained by other diagnostic studies
Laboratory evaluation — Routine laboratory tests, including complete blood count with white blood cell differential and platelet count, erythrocyte sedimentation rate, renal and liver function tests, lactate dehydrogenase (LDH), and urinalysis, should be obtained. Many of these tests are used to determine the presence or absence of organ involvement, as well as the propensity of the patient to relapse following conventional treatment. (See "Clinical features of and prognostic factors for relapse of Hodgkin lymphoma after initial chemotherapy", section on 'Prognostic factors'.)
Although not routinely studied, patients may have evidence of an impaired cellular immune system, including decreased T-cell and NK-cell function. We suggest that patients who have a past medical history of recurrent infections, autoimmune and inflammatory disorders, or a family history of immune deficiency undergo a detailed immunologic evaluation. (See "Approach to the child with recurrent infections".)
Imaging studies — The goal of imaging is to define the extent of disease. The following studies should be obtained:
Chest radiograph (anteroposterior and lateral) CT of the primary site (with and without intravenous contrast)
CT of thorax, abdomen, and pelvis (with and without intravenous and oral contrast)

Gallium-67 scintigraphy
The chest radiograph provides information about intrathoracic structures, extent of mediastinal involvement, and patency of the airway (which must be ensured in patients with mediastinal masses before they are sedated for diagnostic tests or procedures). The CT provides information about extranodal sites of disease; the most common sites of extranodal disease are the pulmonary parenchyma, chest wall, pleura, and pericardium [22,23].
For initial staging, CT is better than gallium-67 scintigraphy; however, gallium-67 scintigraphy is superior to CT for evaluation of residual (eg, mediastinal) disease after therapy because it may help differentiate between fibrosis (no gallium uptake) and residual active disease (positive gallium uptake) [24,25]. In such cases, it is important to have a pretreatment gallium scan in order to compare the uptake of any residual mass after treatment.
Infradiaphragmatic disease may be evaluated by CT, MRI, or lymphangiography. MRI may provide better contrast resolution and evaluation of retroperitoneal lymph nodes than does CT [26]. Lymphangiography is unique in its ability to differentiate reactive from tumor-containing lymph nodes and to evaluate lymph nodes too small for detection by CT. However, because it is invasive and difficult to interpret, it is recommended only for children who have equivocal infradiaphragmatic CT findings and at centers where expertise in interpretation is available.
STAGING — Subsequent therapy and prognosis are based upon the stage of the disease, as currently defined by the Cotswolds classification used both in children and adults (table 2). (See "Staging of Hodgkin lymphoma".)
PROGNOSIS — A retrospective study evaluated prognostic factors in 328 children who had received combined modality treatment (CMT) for HL [27]. Multivariate analysis revealed the following five adverse pretreatment factors:
Male sex Disease stages IIB, IIIB, or IV
Bulky mediastinal disease
White blood cell count >13,500/microL
Hemoglobin concentration <11.0 g/dL
A scoring system, giving one point for the presence of each of these factors, yielded five-year disease-free survivals as follows [27]:
0 to 1 point: 94 percent 2 points: 85 percent
3 points: 71 percent
4 to 5 points: 49 percent
In a separate report in 195 children and young adults treated with CMT, the cumulative incidence of local failure (LF) was 11 percent at 5 years [28]. Predictors of LF included male sex, low initial hemoglobin level, and bulky mediastinal disease.
The above factors also have been found to predict for disease relapse in adults. (See "Clinical features of and prognostic factors for relapse of Hodgkin lymphoma after initial chemotherapy", section on 'Prognostic factors' and "Staging of Hodgkin lymphoma", section on Prognostic factors.)
TREATMENT — Children with HL should be treated in a comprehensive pediatric oncology center [29]. However, depending upon referral patterns and center-specific policies, adolescents with HL may be treated with either adult or pediatric treatment protocols [30]. Optimal therapy involves a multidisciplinary approach from the time of diagnosis. Assignment of stage and treatment are best determined after the pediatric and radiation oncologist have examined the patient and reviewed the diagnostic images and staging study results.
In prior years, treatment of pediatric HL often involved high-dose radiation therapy, which cured local disease but was associated with numerous adverse effects, including growth impairment of bones and soft tissues, development of second malignancies (eg, breast, thyroid), and decreased lung function. Advanced stage disease was treated successfully with combination chemotherapy programs such as MOPP (mechlorethamine, vincristine, procarbazine, prednisone) (table 3), but long-term side effects included an increased risk of development of second malignancies (eg, acute myeloid leukemia) and gonadal toxicity.

The ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) regimen was developed in an effort to reduce these side effects and remains the standard therapeutic regimen for HL in adults. (See "Staging of Hodgkin lymphoma".) Such chemotherapy-only protocols have been used successfully in pediatric HL; however, concerns about potential ABVD-related toxicities have led to the development of risk-adapted regimens (low versus advanced stage) with reduced chemotherapy and radiation therapy doses [31-33]. Patients with nodular lymphocyte predominant HL seem to have a better outcome [8]. (See "Clinical manifestations, pathologic features, and diagnosis of nodular lymphocyte-predominant Hodgkin lymphoma".)
Early stage disease — Treatment of HL depends upon the extent of disease. Children with Ann Arbor stage IA or IIA are considered to have early stage disease; in some studies, selected stage IIIA patients are also included (table 2).
For children with stage I and IIA (early) HL, the overall five-year survival rate exceeds 90 percent, regardless of the therapeutic program chosen [34,35]. The treatment regimen should consist of combination chemotherapy followed by involved field radiation. The following two studies illustrate the benefits of such a regimen:
In a multicenter trial, 110 children and adolescents with stage I/II disease, only five of whom had systemic symptoms, were treated with four cycles of VAMP (vinblastine, doxorubicin, methotrexate, prednisone) and involved field radiation after the second course of chemotherapy [36]. The radiation dose varied between 15 to 25.5 Gy, depending on the initial response to chemotherapy. At a median follow-up of 9.6 years, ten-year overall and event-free survivals were 96 and 89 percent, respectively.
In another trial, 275 children with stage I/IIA HL were treated with two courses of OEPA (boys: vincristine, etoposide, prednisone, doxorubicin) or OPPA (girls: vincristine, procarbazine, prednisone, doxorubicin) followed by 25 to 35 Gy involved field radiation, depending upon the initial response to chemotherapy [37]. Five-year survival and event-free survival were 99.6 and 94 percent, respectively.
Advanced stage disease — Advanced stage disease is considered present in children with selected Ann Arbor stage IIIA and IIIB, Ann Arbor stage IV, B-symptoms (unexplained fever, night sweats, or unexplained weight loss >10 percent of body weight in the six months before diagnosis) regardless of stage, or a mediastinal mass that is greater than one-third the diameter of the chest.
Advanced stage HL in children has conventionally been treated with a combination of MOPP and ABVD and involved field radiation. The overall five-year survival rate with this regimen is 87 to 93 percent [34]. During the last decade, treatment regimens have been modified in an effort to reduce dose intensity, as illustrated by the following studies:
In one trial, 179 children with advanced stage HL were treated with two courses of OEPA (boys) or OPPA (girls) followed by four courses of COPP (cyclophosphamide, vincristine, procarbazine, prednisone) and 20 to 35 Gy involved field radiation, depending on the initial response to chemotherapy [37]. Five-year survival and event-free survival were 96 and 88 percent, respectively.
In another trial, 216 children were treated with three or five cycles of DBVE-PC (doxorubicin, bleomycin, vincristine, etoposide, prednisone, cyclophosphamide), depending upon the initial response, followed by 21 Gy involved field radiation. Preliminary analysis shows two-year survival and event-free survival of 98 and 88 percent, respectively (unpublished data).
Other regimens that limit doses of alkylating agents, anthracyclines, and/or radiation in children with advanced and unfavorable disease have led to inferior outcomes compared to standard regimens [38,39].
Relapsed disease — The treatment of refractory and relapsed HL depends upon prior therapy. Options include conventional non-cross-resistant combination chemotherapy and hematopoietic cell transplantation [40]. (See "Treatment of relapse of Hodgkin lymphoma after initial chemotherapy" and "Hematopoietic cell transplantation in Hodgkin lymphoma".)
ACUTE EFFECTS OF TREATMENT — Acute effects of treatment for pediatric HL depend upon the specific chemotherapeutic agents used, the total dose of radiation therapy, and the volume irradiated.
Radiation effects — Acute radiation effects are a function of the total dose delivered and the volume irradiated. The low-dose involved field radiation that is used in the treatment of pediatric HL is usually well tolerated. Toxic effects, which are usually self-limited and reversible, include:
Erythema and/or hyperpigmentation of irradiated skin Transient hair thinning in exposed fields
Mild gastrointestinal symptoms (see "Radiotherapy-induced nausea and vomiting: Prophylaxis and treatment")

Dry mouth or alteration in taste
Granulocytopenia
Thrombocytopenia
Chemotherapy effects — Children who receive multiple chemotherapeutic agents for the treatment of HL may develop nausea and vomiting. These effects can be modulated with serotonin receptor antagonist anti-emetics and/or pretreatment with benzodiazepines. (See "Prevention and treatment of chemotherapy-induced nausea and vomiting".)
Reversible alopecia is another acute effect of HL chemotherapy regimens. Other acute effects are related to particular agents. As examples, vincristine is associated with neurotoxicity, bleomycin with pulmonary toxicity, and doxorubicin with cardiac toxicity. (See "Neurologic complications of non-platinum cancer chemotherapy", section on 'Vincristine' and "Bleomycin-induced lung injury" and "Cardiotoxicity of anthracycline-like chemotherapy agents", section on 'Children'.)
Myelosuppression and immunosuppression — Myelosuppression is the most common dose-limiting acute toxicity of multiagent chemotherapy and can be treated with transfusions (red cells, platelets, granulocytes) or the administration of colony-stimulating factors (eg, erythropoietin, granulocyte colony-stimulating factor). Blood products, if given, need to be irradiated to prevent development of fatal transfusion-associated graft-versus-host disease in these immunocompromised subjects. (See "Red cell transfusion in infants and children: Selection of blood products", section on 'Irradiated red cells' and "Transfusion-associated graft-versus-host disease".)
Chemotherapy-induced neutropenia and immunosuppression increase the risk of life-threatening infections with viruses, bacteria, and fungi, which need to be treated quickly and appropriately. (See "Fever in children with chemotherapy-induced neutropenia".)
The cellular immune system, including decreased T-cell and NK-cell function, may be impaired at baseline and further compromised by myelosuppression, increasing the susceptibility to herpes zoster and varicella infections. Postexposure prophylaxis can be used to prevent development of varicella infection in children who did not receive the varicella vaccine before undergoing chemotherapy. Antiviral therapy should be promptly initiated in patients who develop varicella infection or varicella zoster. (See "Post-exposure prophylaxis against varicella-zoster virus infection" and "Treatment of herpes zoster".)
Patients who have undergone splenectomy or splenic irradiation are at particular risk for acquisition of serious bacterial infection and should receive prophylactic antibiotics and guidelines to follow during a febrile illness.
OUTCOME — Most children and adolescents with HL have an excellent prognosis with current therapy. The overall five-year survival for early stage disease exceeds 90 percent, regardless of the therapeutic regimen chosen [34]. The overall five-year survival in patients with advanced stage disease who are treated with MOPP/ABVD and involved field radiation is 93 to 97 percent [34].
Late complications — In addition to the acute effects of chemotherapy and radiation, long-term survivors of HL may suffer from an array of unwanted side effects [41-43]. They include:
Impaired growth of soft tissue and bones Thyroid dysfunction
Gonadal dysfunction
Cardiopulmonary toxicity
Second malignancies
Functional impairment and reduced overall general health [44]
Many of these long-term effects were described initially following treatment regimens that are no longer used in children. The combined modality therapy regimens that are currently given were designed to be less intensive than the early therapies in an effort to decrease the incidence of adverse late effects, which may be a greater cause of delayed mortality than is recurrence of HL (graph 2) [45-47]. (See "Second malignancies after treatment of Hodgkin lymphoma".)
Long-term follow-up of pediatric HL patients should take place in a comprehensive pediatric oncology center, where late complications can best be anticipated, monitored, and treated [29,48]. (See "Monitoring of the patient with Hodgkin lymphoma during and after therapy".)

Growth — Long-term effects on bone and soft-tissue growth among survivors of childhood HL are related to the dose and volume of received radiation, as well as the age of the child when the radiation was received. As an example, in one study of 124 children with HL, prepubertal children who received >33 Gy to the entire spine had an average height "loss" of 13 cm (2 SD of the United States population mean), whereas prepubertal children who received <33 Gy and pubertal and postpubertal children who received >33 Gy had little height impairment [49]. High-dose radiation can also cause narrowing of the thoracic apex with symmetric narrowing of the clavicles and atrophy of the soft tissues of the neck.
Thyroid dysfunction — Thyroid dysfunction (usually hypothyroidism) can occur in patients who have received radiation to the head and neck. The incidence varies from 4 to 79 percent, depending upon the radiation dose [31,50,51]. Thyroid dysfunction occurs 20 to 30 months after radiation, and 20 to 30 percent of patients will need thyroid replacement therapy [43,52]; the risk is probably life-long. Accordingly, survivors of childhood HL should be screened annually with a free T4 and TSH. Symptomatic patients should be evaluated sooner. (See "Endocrine surveillance in childhood cancer survivors" and "Acquired hypothyroidism in childhood and adolescence".)
Gonadal dysfunction — Gonadal dysfunction affects female as well as male survivors of childhood HL.
Pelvic radiation carries a high likelihood of ablation of ovarian function. However, moving the ovaries out of the radiation field (oophoropexy) should preserve their function [53-55]. In addition, the successful reimplantation of cryopreserved ovarian cortical strips has been reported [56,57].
The testes are sensitive to radiotherapy and chemotherapy [58]. Thus, in older patients with advanced stage disease, pretreatment storage of sperm should be considered, although decreased sperm quality has been documented before therapy in some cases [59].
Children treated for HL before puberty should have annual ascertainment of Tanner stage to determine whether the pubertal status and tempo of progression are appropriate for age and height. (See "Normal puberty".) Measurement of serum luteinizing hormone (LH), follicle stimulating hormone (FSH), and sex steroid levels (testosterone or estradiol) should be performed in children with delayed or interrupted progression of puberty. (See "Endocrine surveillance in childhood cancer survivors" and "Pubertal development and gonadal function in survivors of childhood cancer".)
Cardiopulmonary and cardiovascular — The long-term cardiopulmonary and cardiovascular complications of childhood HL therapy include cardiomyopathy, pericarditis, pulmonary fibrosis, and accelerated atherosclerosis, with increased risk of stroke [60-64]. In one large study, the relative risk of cardiac death in patients treated with mediastinal radiation was 3.1 in comparison to the general population [65]. The risk of cardiotoxicity may be lessened by reducing the dose of anthracycline chemotherapy and radiation. (See "Cardiotoxicity of anthracycline-like chemotherapy agents", section on 'Children' and "Cardiotoxicity of radiation therapy for malignancy".)
Chronic pulmonary complications of therapy for childhood HL include pulmonary fibrosis and spontaneous pneumothorax [66-68]. (See "Bleomycin-induced lung injury" and "Radiation-induced lung injury" and "Spontaneous pneumothorax in children".)
No guidelines have been established for monitoring cardiopulmonary function in survivors of pediatric HL after completion of therapy. We perform electrocardiogram, echocardiogram, and pulmonary function tests yearly for the first five years after therapy and then every three to five years if no abnormalities are detected.
Second malignancy — Data from the Childhood Cancer Survivor Study indicate that the incidence of second malignancies among survivors of HL and soft-tissue sarcomas is higher than that of other childhood cancers [41]. Twenty years after diagnosis of HL, the cumulative incidence of second malignancies was 7.6 percent. Breast cancer, thyroid cancer, and soft tissue sarcomas were the most common ones. Similar findings have been reported in other studies [48,69-71]. Information concerning the use of chest radiation therapy, age at the time of treatment, family cancer history, and history of thyroid disease may help to determine those most at risk of developing breast cancer [72,73]. (See "Second malignancies after treatment of Hodgkin lymphoma".)
Long-term follow-up — Specific long-term follow-up guidelines after treatment of childhood cancer have been published by the Children's Oncology Group, and are available at www.survivorshipguidelines.org (cccessed January 19, 2010).
ผลตภณฑจากนมววปจจบนแบงออกเปน 2 ประเภทคอ Whole milk และ นมดดแปลง (modified cow’s milk)
1.นมครบสวน(Whole milk) หมายถง นมววท�มไดดดแปลงปรมาณโปรตน, คารโบไฮเดรตและไขมนเม�อนำามาผานกรรมวธทำาใหแหงจะได Whole milk ชนดผง เรยกวานมผงชนดธรรมดา นมดงกลาวมทงชนดท�ไมมการเตสารอ�นลงไปและชนดท�เตมวตามนเอและด ชนดท�เตมวตามนและธาตเหลก นำานมท�ผานกรรมวธและจำาหนายในรปของเหลวแบงออก

เปน 4 ประเภทไดแก นมพาสเจอรไรซ(pasturized), นมยเอชท(UHT), นมสเตอลไรซ(sterirized) และนมขนไมหวาน(evaporated milk) Whole milk ท�ไมผานการดดแปลงทงในรปผงแหงและของเหลวสามารถนำามาใชเลยงทารกและเดกอาย 9-12 เดอนขนไป
2.นมดดแปลง (modified cow’s milk) หมายถงนมววท�ท�มการปรบแตงหรอดดแปลงสวนประกอบของนมววแบงออกเปน 4 ประการคอก. เพ�อใชเลยงทารกปรกต ไดแก นมดดแปลงและอาหารเสรมชนดครบถวนสำาหรบเดกข. เพ�อใชเลยงทารกท�มภาวะดดซมบกพรองไดแก low lactose milkค. เพ�อการควบคมนำาหนก ไดแก นมพรองมนเนยและนมขาดมนเนยจ. เพ�อนำาสวนประกอบบางสวนไปใชประโยชน ไดแก นมแปลงไขมน
ในเดกทารกชวง 6 เดอนแรกนมผงสวนใหญทำามาจากนมวว ทารกไมสามารถยอยและดดซมนมววไดดการใหนมท�ไมมการดดแปลงจงอาจทำาใหเกดอนตรายตอเดกไดจงมการดดแปลงสวนประกอบตางๆในนมววใหใกลเคยงนมแมมากท�สด
การปรบปรมาณสารอาหารตางๆในนมววมแบบแผนการปรบดงน
1. ลดจำานวนโปรตนลงเน�องจากนมววมโปรตนมากกวานมแมถง 3 เทาซ�งมากเกนไปสำาหรบทารก2. เพ�มอตราสวน Casein ตอ Whey โปรตนในนมแมมอตราสวน Casien : Whey เทากบ 40:60 แตในนมววม Casien : Whey เทากบ 80 : 203. ปรบชนดไขมน นมแมมกรดไขมนอ�มตวนอยกวาคร�งสวนนมววมกรดไขมนอ�มตวท�มากกวา4. ลดปรมาณแรธาตไดแก แคลเซยม, ฟอสฟอรส และ โซเดยมซ�งในนมแมมแรธาตเหลานตำ�ากวานมวว5 .เพ�มปรมาณสารอาหารท�จำาเปนเชนธาตเหลกเพราะธาตเลกในนมววมนอยและดดซมไดนอยกวานมแม
กลบดานบน
นมสำาหรบเดกทารกและเดกปกต
ในกรณท�แมตองทำางานนอกบานหรอดวยเหตอ�นใดกตามซ�งมความตองการท�จะใชนมอ�นทดแทนนมแมแกเดกทารกหรอเดกจะตองเลอกใชนมใหถกประเภทมเชนนนจะทำาใหเกดอนตรายแกเดกไดเพราะมสารอาหารไมครบถวนหรอมากเกนไป นอกจากนควรชงนมใหถกตองตามวธตามคำาแนะนำาท�ฉลากขางกระปองเพ�อใหนมมความเขมขนท�พอเหมาะ ถาชงนมขนมากเกนไปจะทำาใหเกดปญหาอจจาระรวงไดแตถาชงนมเจอจางเกนไปกจะทำาใหเดกขาดสารอาหาร อปกรณทกอยางเชนขวดนม, จกยางและฝาครอบภายหลงการใชจะตองตมหรอน�งเพ�อฆาเชอโรค
ผลตภณฑนมสำาหรบเดกทารกและเดกปกตจำาแนกเปน 3 ประเภทตาม ตามปรมาณโปรตนและกลมอายของเดกท�ใชคอนมดดแปลงสำาหรบทารก, นมสตรตอเน�องและนมครบสวน
1.นมดดแปลงสำาหรบทารก(Infant Formula หรอ Modifies milk for infant)
นมประเภทนเปนนมท�ใชสำาหรบทารกตงแตแรกเกดจนถงอายครบ 1 ปในกรณท�ไมสามารถใหนมแมไดและเปนนมเพยงชนดเดยวเทานนท�สามารถใชทดแทนนมแมไดสำาหรบเดกทารกปกตในชวง 6 เดอนแรก แตเม�อทารกอายมากกวา 6 เดอนขนไปสามารถเปล�ยนไปใชนมท�มโปรตนสงกวาไดแก นมสตรตอเน�องหรอนมครบสวนไดเน�องจากไตของเดกปกตอายเกน 6 เดอนสามารถขบของเสยท�เกดขนจากโปรตนไดดขนแลว ในกรณท�ใชนมดดแปลงสำาหรบทารกแทนนมแมควรใหนมประเภทนเปนอาหารอยางเดยวแกทารกไปจนถงอายประมาณ 3 เดอน เม�อทารกอาย 3-4 เดอนขนไปควรไดรบอาหารเสรมเชนเดยวกนกบทารกท�เลยงดวยนมแมเพ�อฝกการใหเดกทารกยอมรบอาหารอ�นนอกจากนมตามวยท�เหมาะสมเดกจะไดมนสยการกนท�ดตอไป
นมดดแปลงสำาหรบทารกผลตขนมาใหมสารอาหารตางๆใหใกลเคยงกบนมแมทงดานคณภาพและปรมาณ ผลตภณฑของแตละบรษทมขอแตกตางกนในดานสวนประกอบและราคาโดยแตละบรษทไดมการพฒนาคณภาพผลตภณฑของตนตลอด

เวลา ดงนนผท�เก�ยวของกบผลตภณฑนมเหลานและผซอจงควรมความรพนฐานเก�ยวกบนมแมและตดตามขอมลใหมๆเพ�อนำามาพจารณาประกอบการเลอกใชผลตภณฑท�เหมาะสม
2.นมสตรตอเน�องหรออาหารเสรมชนดครบถวนสำาหรบเดก(Follow Up formula หรอ complete supplementary food)
นมประเภทนสามารถใชเลยงเดกทารกอายตงแต 6 เดอนขนไปถง 3 ป ในกรณท�เดกอาย 1 ปขนไปและไดรบสารอาหารหลก 3 มอท�ครบ 5 หมสามารถเปล�ยนมาใชนมครบสวน(Whole Cow's milk)ซ�งมราคาถกกวาส�งสำาคญท�ควรทราบคอถงแมฉลากของนมประเภท Follow-up formula วาเปนอาหารเสรมชนดครบถวนสำาหรบเดกแตความจรงแลวกเปนนม มารดาบางคนเขาใจผดวาใชนมประเภทนแลวไมตองใหอาหารเสรม ซ�งเปนความเขาใจผดท�ตองแกไข ทารกท�เลยงดวยนมประเภทนยงจำาเปนตองไดรบอาหารเสรมซ�งเปนอาหารก�งเหลว(Semisolid) ท�เหมาะสมกบวยดวย ผลตภำณฑนมสตรตอเน�องมการดดแปลงโปรตนใหตำ�าลงแตยงสงกวาโปรตนในนมแมและนมดดแปลงสำาหรบเดก คารโบไฮเดรตมแลคโตสเปนหลก ผลตภณฑแทบทงหมดมการผสมวตามนครบถวนและแรธาตเชนเดยวกบนมดดแปลงสำาหรบทารก
3.นมครบสวน( Whole cows milk หรอ whole milk)
นมประเภทนหมายถงนมววท�มไดดดแปลงปรมาณโปรตน คารโบไฮเดรตและไขมนแตอาจจะมการเตมวตามนและธาตเหลกเพ�อคณคาทางโภชนาการเพ�มขนแบงเปนนมผงครบสวน(Whole Milk powder)และนำานมครบสวน(liquid whole milk)
3.1 นมผงครบสวน(Whole milk powder)
นมชนดนควรใชเลยงทารกปกตอายตงแต 1 ปขนไปผลตภณฑสวนใหญไมไดเสรมวตามนครบถวนและไมไดเสรมธาตเหลก ดงนนเดกโตท�ด�มนมเปนอาหารสวนใหญโดยไมคอยรบประทานอาหารใหครบ 5 หมจะเกดปญหาการขาดสารอาหารได จงตองฝกนสยการกนและไมควรใหกนนมเกนวนละ 32 ออนซเพราะเดกจะไมยอมรบประทานอาหารหลกถาใหด�มนมมากกวาน
3.2 นำานมครบสวน(liquid Cow's milk)
ผลตภณฑประเภทนอยในรปนำานมซ�งอาจเปนนมคนรปหรอนมสดกได นมคนรป(recombines Milk) คอนำานมท�ไดมาจากการนำานมผงขาดมนเนยมาเตมมนเนยและนำาแลวนำามาผานกรรมวธฆาเชอดวยความรอน
สวนนมสด(fresh Milk) คอการนำาเอานำานมดบมาฆาเชอดวยความรอนสำาหรบนมสดสามารถใหไดในเดกอายประมาณ 1 ปขนไป มรายงานวาการใหนมสดแกเดกทารกท�อายนอยกวา 1 ปจะเกดปยหาเลอดออกจากระบบอาหารจงไมแนะนำาใหชนมสดเลยงเดกทารก
หลกเกณฑการเลอกใชนมสำาหรบทารกและเดกปรกต
1.นมแมเปนนมท�ดท�สดสำาหรบเลยงเดกทารกถาเปนไปไดควรใหนมแมแกลกนาน 1-2 ป2.ในกรณท�ไมสามารถใหนมแมไดตองพจารณาเลอกนมท�เหมาะสมกบวยของทารกและเดกปจจยในการเลอกซอนมไดแก อาย, สวนประกอบของนม, ภาวะโภชนาการและอาหารอ�นๆท�เดกไดรบ, ราคา และการยอมรบของเดกขอสำาคญอยางย�งคอไมควรตดสนคณภาพของนมจากราคาเพราะนมท�มราคาแพงไมจำาเปนจะตองเปนนมท�มคณภาพดท�สด 2.1 ทารกแรกเกดถง 6 เดอน ใชนมดดแปลงสำาหรบทารกชนดท�เสรมธาตเหลกถาราคาเทากนควรเลอกชนดท�มอตราสวนของ casein:whey ใกลเคยงกบนมแม(40:60) การเตมทอรนและอ�นๆ 2.2 ทารกอาย 6 เดอนถง 1 ปถาไดอาหารเสรมท�ถกตองใชนมดดแปลงสำาหรบทารกหรอนมสตรตอเน�องได ถาการยอมรบอาหารเสรมไมคอยดควรใชนมสตรตอเน�องท�มวตามนและเกลอแรครบถวน ถามปญหาทางเศรษฐกจสามารถใชนมครบสวนซ�งมราคาถกกวาไดโดยตองใหอาหารเสรมท�มคณคาทางโภชนาการดแกเดก กลาวคอประกอบดวยอาหารครบ 5 หม มฉะนนจะเกดปญหาการขาดเหลกและวตามนบางตวได

2.3 เดกอายประมาณ 1 ปขนไปถาภาวะโภชนาการปรกตและรบประทานอาหารหลก 3 มอท�มคณคาทางโภชนาการครบ 5 หมใหใชนมครบสวนแตถารบประทานอาหารหลกไดนอยควรเลอนมท�เสรมวตามนรวมและธาตเหลก
กลบดานบน
นมและอาหารทางการแพทย
อาหารทางการแพทยคออาหารท�มการพฒนาสตรขนมาเพ�อใหใชรบประทานหรอใหทางระบบทางเดนอาหารภายใตการดแลของแพทย โดยมวตถประสงคเพ�อท�จะใหโภชนบำาบดสำาหรบโรคหรอภาวะท�มความตองการสารอาหารแบบพเศษโดยมขอบงใชคอผปวยปฏเสธการรบประทานอาหารหรอมความลำาบากในการใหอาหารทางระบบทางเดนอาหารสวนบนหรอผปวยไมสามารถรบอาหารทางปากไดอยางเพยงพอและการใหอาหารทางระบบทางเดนอาหารตอผปวยนนสามารถทำาไดอยางปลอดภยและมประสทธภาพอาหารทางการแพทย
ผลตภณฑนมท�เปนอาหารทางการแพทย
ผลตภณฑสตรสำาเรจ(define formula diet) คอกลมท�เปนช�อการคาตางๆซ�งเปนสตรสำาเรจมองคประกอบของสารอาหารตางๆท�แนนอนและเปนสตรท�มสารอาหารตางๆครบถวนยกเวนพวกสตรพเศษบางสตร
1. สตรดดแปลงคารโบไฮเดรต การดดแปลงขนพนฐานท�สดของอาหารทางการแพทยทกสตรคอการลดปรมาณแลคโตสซ�งเปนคารโบไฮเดรตหลกของนมสำาหรบทารกปกต สตรนสามารถนำาไปใชในผปวยท�มปญหาการขาดนำายอยแลคเตสเชนอจจาระรวงหรอขาดโปรตนหรอพลงงานท�ท�มอาการอจจาระรวง ผลตภณฑท�มใชไดแกก.สตรแลคโตสตำ�า(Low lactose formular) ช�อการคา อลมรอนข.สตรปราศจากแลคโตส (No lactose formula) ช�อการคา โอแลค
2. สตรดดแปลงคารโบไฮเดรตและโปรตน ใชสำาหรบผปวยท�มปญหาการยอยและดดซมหรอแพโปรตนเชนทารกท�มการแพนมวว การดดแปลงมสองระดบคอ2.1 เปล�ยนเปนโปรตนอ�นท�ไมใชนมววท�นยมใชคอโปรตนจากถ�วเหลอง(Soy-base formula) ช�อการคาคอ ไอโซมล , นวตร-โซยา และโปรโซบ2.2 ปล�ยนเปนโปรตนท�มขนาดโมเลกลเลกลงคอสารยอยสลายจากโปรตนสายยาวเปนสายสน(Protien hydrolysate formula) เน�องจากผปวยท�แพนมววอาจแพนมถ�วเหลองไดการใชนมชนดนซ�งไมเปนแอนตเจนจงปลอดภยกวา ช�อการคาคอ นตรามเยน
3. สตรดดแปลงคารโบไฮเดรตและไขมน ใชสำาหรบผปวยม�มภาวะยอยและดดซมไขมนบกพรองเปนสตรท�ไมมแลคโตสจงใชไดดในเดกท�มภาวะขาดแลกเตสและมสวนผสมของไขมนชนดไตรกลเซอไรดสายปานกลางท�รางกายสามารถนำาไปใชไดเลย ช�อทางการคา แพนเอนเทอราล
4. สตรดดแปลงคารโบไฮเดรต , โปรตนและไขมน ใชสำาหรบผปวยท�มปญหาในการยอยและดดซมคารโบไฮเดรต,โปรตนและไขมนบกพรองเปนสตรท�ไมมแลคโตสมการเตมไตรกลเซอไรดสายปานกลางและโปรตนมการยอยสลายใหเปนสายเลกเหมาะสำาหรบผปวยท�แพโปรตนจากทงนมววและนมถ�วเหลอง ช�อทางการคา พรเจสตมล
5. สตรพเศษ 5.1 สตรสำาหรบทารกคลอดกอนกำาหนดหรอทารกท�มนำาหนกแรกคลอดตำ�ากวา 1,800 กรม( Premature formula) ช�อการคา เอนฟาแลค พรมาชวร และ พรแนน
5.2 สตรสำาหรบทารกท�มความผดปกตทางพนธกรรม เชนสตรสำาหรบภาวะฟนลคโตนสงในปสสาวะ ช�อการคา โลนาฟฟแลค ซ�งเปนสตรท�มฟนลอะลานนตำ�า

ประวต
ประวตทดจะไดมาจากการซกกถามอยางมความร มความเหนอกเหนใจ พยายามทำาความเขาใจในตวเดกและผปกครอง และทสำาคญจะตองไมเรงรบจนเกนไป ใหโอกาสและเวลาแกเดกและผปกครองใหมากทสดเทาทจะสามารถทำาได ในกรณรบดวนอาจจำาเปนตองรบซกแตสวนสำาคญกอน จากนนเมอพนชวงวกฤต จงมาซกโดยละเอยดอกครง
การซกประวตกเชนเดยวกบในโรคทวไปทควรถามถงอาการสำาคญทนำาผปวยมากอน บอยครงทผปกครองนำาเดกมาเนองจากมการตรวจมากอนแลว พบวาเสยงหวใจผดปกต การถามตอใหละเอยดจะมประโยชนมาก เสยง murmur ทยงไมไดยนในวนแรกๆของชวต แตพอไมกวนถดมาฟงไดชดเจน ชวยบอกเราวานาจะเกดจาก L to R shunt ทเรมไดยนเมอ pulmonary vascular resistance ลดลง หรอกรณแพทยคนเดมทเคยดแลเดกมากอนตงแตเลกมาเรมฟงเสยงหวใจไดผดปกตหลงเกดหลายป หรอ เพงจะฟงไดในชวงมไขสง ชวยบอกเราวา เสยงนนอาจเกดจาก acquired heart disease หรอ functional murmur เปนตน

อาการหอบเหนอยเปนอาการสำาคญอนหนงทนำาผปวยมาหา ผปกครองเดกเลกอาจใหประวตหายใจแรงแมในขณะนอนหลบ เดกเหลานถาเปนการหอบเหนอยจรงจะไดประวตการเหนอยขณะดดนมดวยอยางชดเจน การเหนอยขณะดดนมอาจแสดงไดเปน 2 ลกษณะ คอดดไดทละนอย ตองพก หรอใชเวลาในการดดนาน โดยทวไปสำาหรบทารกทดดนมมารดา การสงเกตดวยตนเองของมารดาจะบอกไดเปนอยางดวา เดกดดไดแรงดหรอไม เหนอยหรอไม เมอเปรยบเทยบกบลกคนแรก เดกเลกทดดนมมารดาไดด ไมเหนอย จะใชเวลาประมาณมอละ 20-30 นาท หรออาจถามไดวาหลงดดแตละมอเดกอมหลบไดถง 2-3 ชวโมงหรอไม กรณดดนมผสมเดกตำากวา 6 เดอนทสามารถดดนมไดรวดเดยว 4 ออนซโดยไมตองพกเรยกไดวาไมเหนอย โดยการดดดงกลาวนนประมาณรอยละ 80 ของปรมาณนมในมอนนตองดดไดหมดภายใน 10 นาท ไมมอาการจมกบาน และ/หรอชายโครงบมทแสดงถงการหายใจลำาบาก ไมมเหงอออกทวมทแสดงถงภาวะ sympathetic over-activity
อาการเหนอยหอบในเดกโตอาจบอกไดยากขน เดกเองอาจกลวการนอนโรงพยาบาลไมยอมรบวาเหนอย ยกเวนวาเหนอยมากแลว หรอในทางกลบกนเดกโตหลายคนบนเหนอยโดยไมไดมพยาธสภาพจรงกมาก จงจำาเปนตองถามดใหละเอยดทวา เหนอย เกดตอนไหน อยางไร พยายามถามกจวตรประจำาวน เชน เดนไปโรงเรยนเหนอยหรอไม ไกลเทาไร เดนขนบนไดกชนจงเหนอย เปนตน
อาการตวเขยวเกดเพราะม reduced hemoglobin ในเลอดสง อาการเขยวในชวงแรกเกดทเกดจากสาเหตทางปอด หรอ ระบบประสาท มกมประวตชวยอยางอยางชดเจน เชน ประวตคลอดลำาบาก ม meconium stained amniotic fluid ในทารกทหายใจลำาบากจากเรอง asphyxia หรอ meconium aspiration syndrome ประวตคลอดกอนกำาหนดในทารกทหายใจลำาบากจาก respiratory distress syndrome เปนตน ในทางกลบกนทารกทเขยวจากสาเหตทางหวใจมกไมมประวตชดเจนถงสาเหตของการเขยว การเขยวทมสาเหตจากปอดเดกอาจจะเขยวนอยลงเมอรองไห และเขยวนอยลงไดเมอไดรบออกซเจน ในพวก right ventricular outflow tract obstruction เชน tetralogy of Fallot อาจจะมประวตเดกเลกลงไปนอนควำางอตวเองไว หรอเดกโตนงยองๆ เพอลด oxygen consumption และเพม systemic vascular resistance แลวเดกเขยวนอยลง เหนอยนอยลง
ประวต precordial pain ขณะออกกำาลง พบใน severe aortic stenosis หรอ coronary insufficiency ได อาการปวดแมในขณะอยเฉยๆอาจเปน pericarditis อาการเจบแบบ nonspecific ไมสมพนธกบการออกกำาลงกายอาจพบใน mitral valve prolapse syndrome แตในเดกพบโรคเหลานนอย และ ถาเปนมกมอาการแสดงอนรวมดวยอยางชดเจน ประวตเจบหนาอกอยางเดยวมกไมเกยวกบโรคหวใจในเดก

ประวตการปวดศรษะทชดเจนอาจเนองจากม hypertension ถารวมกบอาการปวดขาเวลาเดน อาจเกดจาก hypotension ในสวนลางของรางกายใน coarctation of aorta
ประวตอดตทสำาคญทควรถามเสมอใน congenital heart disease คอประวตการใชยา ประวต rubella ระหวางตงครรภ นอกจากนนประวตครอบครวอาจมความสำาคญในบางโรค เชน hypertrophic cardiomyopathy
การตรวจรางกาย
การด
การดเปนสงงายทสามารถชวยประเมนผปวยไดดสด โดยเฉพาะอยางยงผปวยทยงฟงไดไมชำานาญ การดแลผปวยอยางละเอยดจะชวยใหขอมลไดมาก ใหสงเกตลกษณะเดกทว ๆ ไป ไดแก
1. cyanosis ตองพยายามมองหาวาม cyanosis หรอไม ถามตองพยายามแยกวาเปน peripheral cyanosis คอ เขยวเฉพาะบรเวณทม circulation ไมด เชน acrocyanosis ในทารกแรกเกด หรอเปน central cyanosis ทเขยวแมแตในบรเวณทม circulation ดดวย ม differential cyanosis คอการเขยวแตกตางกนระหวางแขน และขาหรอไม นอกจากนนตองพยายามบอกความรนแรงของการเขยวดวย วาเปน mild, moderate หรอ severe
2. clubbing of the fingers and toes แมจะพบไดในโรคอนดวย แตการพบ clubbing fingers มกบองถง central cyanosis ทเปนมานานอยางนอยหลายเดอน
3. growth failure พบใน large L to R shunt และ severe cyanotic congenital heart disease
4. respiratory distress ถาหายใจเรว และ ลำาบาก ใหคดถงโรคปอด หรอม congestive heart failure แตถามการการหายใจเรวไมสมดลกบการออกกำาลงกายใหคดถง cardiac dysfunction หรอเปน compensation ในกรณมเขยวรวมดวย ถาหายใจหอบลก เปน metabolic acidosis
5. precordial bulge ใหคดถง ventricular hypertrophy ทเปนมานาน
6. apical activity ถาพบวา apical activity กระจายไปกวาง (เสนผาศนยกลางเกน 2-3 ซม. หรอเกดกวา 1 ICS) แปลวาหวใจโต หรอถาเหน point of
maximal impulse อยเกนกวาแนว midclavicular line หรอ 5th ICS กแปลวาหวใจโต
7. visible pulsation of arterial neck vessels พบไดในรายทม cardiac output มาก หรอ severe aortic diseases เชน PDA, AR, A-V fistula, thyrotoxicosis, severe anemia, SH และ CA
8. engorgement of neck vein พบใน CHF, PA, TA หรอใน TR
9. บวม เกดเนองจากมการรวของ intravascular fluid ออกมาส tissue ในเดกสวนมากพบ puffiness of eyelids และ face
การดเปนสงทมประโยชนมากและตองการเพยงความละเอยดถถวนกจะชวยบอกภาวะของเดกไดอยางมาก จำาไวเสมอวาการตรวจโรคหวใจควรเรมตนดวยการดกอนเสมอใหละเอยดทวทงตว
การเคาะ
ในเดกการเคาะมประโยชนนอยมาก เทาทจะใชกนกมกเคาะดขนาดทแทจรงของตบ เนองจากในภาวะทเดกหอบ ตบอาจถกดนลงมามากๆไดทำาใหรสกวาตบโตกวาทควร นอกจากนนกอาจมการเคาะปอดด consolidation หรอ effusion เปนตน
การคลำา
เปนการตรวจทมประโยชนมากทสดอกอนหนง โดยเฉพาะอยางยงสำาหรบผทยงฟงไดไมชำานาญ การคลำาทควรทำาเสมอในผปวยทกราย ม
1. peripheral pulse
การคลำาชพจรเปนสงสำาคญมากเพราะการใชเพยงนวมออาจวนจฉยโรคไดดกวาการใชเครองมอราคาแพงเสยอก การคลำาตองคลำาทง 4 extremities แนะนำาใหคลำา pulse ทขากอนใหเปนนสย การคลำา pulse ไดแตกตางชดเจนทำาใหตองพยายามตรวจหาซำา คลำาได pulse แรงท upper extremities และคอยท lower extremities ใหคดถง coarctation of aorta หรอถากลบกนคลำา pulse ไดแรงท lower extremities และคอยท upper extremities หรอคลำาไดแรงบาง เบาบางเปนแหงๆนกถง Takayasu disease
Bounding pulse พบใน high output stage เชน ไขสง hyperthyroidism หรอม aortic run off เชน aortic regurgitation, PDA คลำาได
weak pulse พบใน low cardiac output, AS, myocarditis, cardiac tamponade, shock
ในผปวยอาการหนก การคลำาเปรยบเทยบ distal กบ peripheral pulse จะชวยในการบอกระดบการม sympathetic compensation
2. precordial activity
RV impulse คลำาโดยใชฝามอทงสองขางวางขนานกบ sternum ทดานซาย sternum ถาม right ventricular hypertrophy จะพบมลกษณะเปนแบบเตะฝามอแรง lifting หรอ นาน heaving
LV impulse คลำาโดยใชฝามอทงสองขางวางขนานตงฉากกบแนว sternum บรเวณ apex ถาม left ventricular hypertrophy จะมลกษณะเปนแบบ lifting
ในเดกทมทง RV และ LV โต บางทจะสงเกตเหนวา precordial activity เปนแบบ rocking คอ LV impulse เกดทางซาย และหายใจไปพรอมกบทม RV impulse เกด ขนตรงใกลกระดก sternum
apical activity เชนเดยวกบการด คอถาพบ apical activity กระจายไปกวาง หรอ point of maximal impulse อยเกนกวาแนว midclavicular line หรอ 4th ICS แปลวาหวใจโต
precordial thrill จะเกดไดกตองม turbulent blood flow การคลำาจะรสกไดดดวยการใชสวนของ bass of metacarpal area ฉะนนถาคลำาพบม thrill ตองไดยนเสยง murmur แน
3. hepatomegaly
สวนมากพบในราย CHF แตยงพบใน TS, TR และอาจไดแบบ expansile pulsaion, hepato-jugular reflux
การฟง
เปนสวนสำาคญทสดในการตรวจหวใจ stethoscope เปนอปกรณสำาคญทชวยในการวนจฉยทแพทยทกคน ควรมใชเปนของตนเอง จะทำาใหไดยนเสยงทชดเจนขนจาก ear piece ขนาดทเหมาะและเคยชน ทงจำาทำาใหคนกบเสยงทฟงจาก stethoscope ของตนเอง stethoscope ทใชควรจะม bell และ diaphragm bell ใชฟงเสยงทมความถตำาเชน MS, S3, S4 สวน diaphragm เหมาะในการฟงเสยงทมความถสง เชน AR การฟงนนควรจะฟงใหละเอยดหองทใชตรวจควรเปนหองทเงยบปราศจากเสยบรบกวน การฟงอยางนอยตองฟงใน 4 บรเวณทสำาคญ คอ apex, lower LSB, upper sternal
border ทง L และ R การฟงทงดานหนาและดานหลงของทรวงอก หรอบางครงท หว คอ ทอง และ แขนขา เปนสงทชวยในการวนจฉยในผปวยหลายๆรายดวย
การฟงในเดกเลกบอยครงทตองใชจตวทยาชวยเบนความสนใจเดกออกไปจาก stethoscope ดวยเสยง หรอวตถสสดตางๆเวลาฟงใหเดกอยในทาทสบายทสด บอยครงทตองฟงขณะอยบนตกแม ดดนมแมอย หรอดดนมขวดอย ในเดกอายประมาณ 6 เดอนถง 3 ปเรมตนอาจตองทำาเปนฟงทตวแพทยเอง ตวแม แขนแม มอเดกเพอไมใหเดกกลว และใหเดกทราบวาไมมอนตรายจากนนจงตรวจเดกจรง โดยเรมตรวจในขณะทใสเสออยกอน แลวจงคอยเปดเสอเขาไปตรวจ กอนทจะฟงควรทำาใหสวนทวางบนหนาอกของเครองฟง (chest piece) อนขนโดยกำา chest piece ของ stethoscope ไวในองมอกอน การตรวจอยางไมเรงรอน ตลอดจนตรวจดวยความนมนวลมกจะทำาใหเดกไมตอตาน และฟงเสยงไดด และตองไมวาง stethoscope ทเดยวบนหนาอกเดกเลกนานเกนไป เพราะเดกทกคนจะตอตาน รอง ทำาใหฟงตอไดลำาบากขน
ในการฟงเสยงหวใจ และ murmur ควรใชทงสวน diaphragm และสวน bell แรงทใชกดบนสวน chest piece ขณะฟงเสยงหวใจมความสำาคญ ในการใชสวน bell ไมควรออกแรงกด เพยงวางสวน bell ใหแตะกบหนาคนไขดวยแรงเพยงพอทจะไมใหมการรวของอากาศเพราะถากดแรงเกนไป ผวหนงบรเวณทถกกดจะตงออกทำาหนาทคลาย diaphragm ทำาใหไมสามารถไดยนเสยงทควรจะไดยน ในทางตรงกนขาม การใชสวน diaphragm ในการฟงจะตองใชแรงกดมากพอสมควรเพอใหแผน diaphragm แนบชดกบผวหนง เพอทำาใหฟงเสยงทมความถสงไดด
หลกทจะชวยในการฟงเสยงหวใจใหไดด คอ การเจาะจงฟงเฉพาะเสยงใดเสยงหนงในเวลาเดยวจนเปนทพอใจแลวจงตงใจเจาะจงฟงเสยงอนตอไป การทจะบอกวาเสยงทฟงไดนนอยในชวงไหนของ cardiac cycle วธทใชไดผลดคอการคอยๆ ขยบ stethoscope โดยไมยก จาก apex มา lower sternal border แลวไปท upper sternal border ฟงไปพรอมกบความรทวา ปกตเสยง first heart sound จะไดยนชดกวา second heart sound แถวบรเวณ apex ถาเรมฟงจากบรเวณนนจนบอกไดวาเสยงไหนเปน first heart sound ตอไปเมอคอย ๆ เลอนสวน chest piece ไปบรเวณอนกจะพบวา first heart sound จะคอยๆเบาลง ในขณะท second heart sound จะคอย ๆดงขน เมอรวมกบการคลำา pulse พรอมกนไปดวยกจะบอกไดวา เสยงตาง ๆ ทเกดขนนนอยในระยะ systole หรอ diastole โดย pulse ทเตนจะอยในชวง systole ระหวางเสยง first heart sound กบ second heart sound
การหดฟงเสยงหวใจกเชนเดยวกบศาสตรอน ๆ ทมหลกวา “Practice makes perfect” ตองพยายามหดฟงซำาแลวซำาอก เปรยบเทยบใหรจรงวาถกตองจากผทฟงไดด

กวา ตลอดจนพยายามทำาความเขาใจวา เสยงทเกดขนนน ๆ เกดจากพยาธสภาพอะไร จงจะฟงไดดขนเรอยๆ
ปกตเสยงทเกดจากลนทง 4 ของหวใจไดยนชดในตำาแหนงตางๆกนของทรวงอกสวนหนา
1. เสยงทเกดจาก PV ไดยนชดท ICS ชองท 2 หรอ 3 left parasternal border (PVA)
2. เสยงทเกดจาก AV ไดยนชดท ICS ชวงท 2 right parasternal border (AVA)
3. เสยงทเกดจาก MV ไดยนชดทบรเวณ apex (MVA)
4. เสยงทเกดจาก TV ไดยนชดท ICS ชอง 4 บรเวณใกลกบ RSB (TVA)
First heart sound (S1)
เสยงทไดยนเกดจาก 2 components คอ จากการปดของ MV และการปดของ TV การเปลยนแปลงของ S1 ทพบไดบอยและมความสำาคญในเดกกม increased S1 ใน ASD และ decreased S1 ใน myocardial diseases หรอ pericardial effusion
Second heart sound (S2)
การเปลยนแปลงของ S2 เปนสวนทสำาคญมากในการตรวจโรคหวใจเดกจนมผกลาววา การตรวจ S2 เปนเสมอนหวใจของการฟงในการตรวจโรคหวใจเดกทเดยว
เสยงทไดยนเกดจาก 2 components ไดแก เสยงซงเกดจากการปดของ AV และ PV ตามลำาดบ ปกต AV จะปดกอน PV ประมาณ 0.03 วนาท แลว หผฟงกไมสามารถบอกไดวามการ split เกดขนเมอฟงดวย stethoscope เวลาหายใจเขา A2 และ P2 จงจะแยกออกจากกนทำาใหฟงไดยนเปน 2 components บอกไดวาม splitting ของ S2 เมอฟงดวย stethoscope แตเมอหายใจออกทง 2 components นจะเขามาอยชดกนจนฟงไดเสยงเดยวทงนเนองจาก
1. เมอหายใจเขา intrathoracic negative pressure เพมขน intra-abdominal pressure เพมขนและ tone ของ small peripheral veins เพมขนสงตาง ๆ เหลานทำาใหเพม systemic venous return เพม RV filling และเกด prolonged RV emptying time จงทำาใหเกด delayed closure ของ PV ทำาให P2 หางออกไปจาก A2

2. เมอหายใจเขา ทำาใหมการเพม pulmonary vascular capacity เกดการคงของเลอดทปอด ทำาให venous return มาส LA นอยลง LV กไดรบเลอดนอยลง ทำาให LV emptying time สนลง AV closure เกดเรวขนกวาเมอหายใจออกทำาให A2 หางออกไปจาก P2
การเปล�ยนแปลงของ S2
1. Intensity
1.1 Intensity เพมขนในคนไขทม chest wall บาง นอกจากน intensity ยงเพมขน เมอม dilatation หรอมการเพมความดนใน AO หรอ PA เชนใน systemic hypertension, pulmonary hypertension
1.2 Intensity ลดลงในคนไขทม chest wall หนา หรอในพวกทมการแขงตวของลน AV หรอ PV เชน ใน AS, PS หรอพวกทใน AO หรอ PA มความดนตำา
2. Single second heart sound
2.1 เมอ component หนงคอยลงมากจนฟงไมไดยนไดแกใน severe AS, severe PS, TOF
2.2 murmur กลบเสยง A2 ไดแก ใน VSD, PDA, PS, rupture sinus of Valsalva
2.3 ม functioning valve ทออกจากหวใจเพยงอนเดยวไดแกใน persistent truncus arteriosus, pulmonary atresia
2.4 pressure ใน ventricle ทงสองขางเทากนไดแกใน Eisenmenger syndrome, single ventricle
2.5 aortic valve อยหนาตอ pulmonic valve ทำาใหไมไดยนเสยง P2 ไดแก TGA, corrected TGA
3. Abnormally wide splitting พบใน RBBB, PS, TOF (mild), PAPVR เพราะม prolong RV ejection นอกจากนยงพบใน VSD, MR เพราะม shorten LV ejection
4. Abnormally wide and relatively fixed splitting
4.1 ASD A2 split กวางขนเพราะม prolong RV ejection เนองจาก L to R shunt ผาน ASD เขาส RA ลงส RV เกด RV volume overload การหายใจเขาออกไมทำาให volume overload ของ RV ซงมเตมทอยแลวเปลยนแปลงไป เพราะเมอม ASD ขนาดใหญผลการเปลยนแปลงใน intrathoracic pressure จะมตอ atria

ทงสองเสมอนหนงวาเปน atrium ใหญเพยงอนเดยว คอเมอหายใจเขา เลอดกลบเขาส RA มากขน ทำาให L to R shunt ผานทาง ASD จะเพมขน ทำาใหเลอดนผานจาก RA เขาส RV ทงเวลาหายใจเขาและเวลาหายใจออกมประมาณคอนขางคงท RV ejection time จงคงท แตนานขน ทำาให S2 ม abnormally wide and fixed splitting ใน TAPVR กพบการตรวจนไดเชนกน
4.2 RV failure ทำาใหเกด fixed splitting ของ S2 ไดแตไม widely split ทงนอธบายได โดยทในภาวะทม RV failure นน RV ejection จะคงทเพราะ RV ไมสามารถเพม stroke volume ใหมากขนอกขณะทหายใจเขา
5. Paradoxical splitting
เปนการ split ของ S2 ทตรงกนขามกบในภาวะปกต คอ เมอหายใจเขา S2 จะ split แคบกวาเวลาหายใจออก เกดไดเนองจาก delayed aortic closure เชนใน LBBB, AS (severe), SH, COAT, coronary heart disease, acute coronary insufficiency, PDA นอกจากนยงเกดไดใน Wolff-Parkinson-White syndrome เพราะม early electrical activation ของ RV หรออาจเกดจาก early pulmonic closure ซงพบไดใน RA myxoma, TR
Valve opening sound (opening snap, OS)
พบใน MS และ TS เกดใน early diastole เกดเนองจากการทลนทตบแตยงไมแขงพยายามทเปดออก แตตองหยดทนท เพราะเปดไมไดเตมท ทำาใหเกด tension ขนและเกดเสยง OS ขน ถา MS หรอ TS นอย หรอตวลนม calcification กจะไมมเสยง OS, OS ของ MV ฟงไดชดบรเวณ low LSB หรอท apex ในทานอนตะแคงซาย OS ของ TV ฟงไดชดบรเวณ lower RSB หรอบรเวณดานซายตอ xiphoid area ลกษณะของเสยงของ OS intensity, pitch และ duration คลาย S2 OS แยกจาก P2 ไดคอ OS มก radiate ไดกวางกวา P2 ไมเปลยนแปลงตามการหายใจ และ OS หางจาก A2 มากกกวา P2
Third heart sound (S3)
S3 เปนเสยง low-pitched เกดจาก tension ของ chordae tendineae และ mitral valve leaflets ขณะท ventricle ขยายตวและยาวขนอยางรวดเรว เมอมการไหลของเลอดจาก atrium ใน early diastole ถาเปน S3 ทเกดจาก LV ฟงไดแถว apex สวน S3 ทเกดจาก RV ฟงไดแถว left sternal border S3 พบไดใน
1. เดกปรกต S3 อาจหายไปเมอเดกนงหรอยน ถาเดกอยในทายนยงไดยน S3 อยใหนกถงวา ไมนาจะเปน physiologic S3, S3 นพบไดจนถงผใหญในบางคน

2. high cardiac output เชน hyperthyroidism, anemia
3. increased LV filling ใน early diastole เชนใน complete heart block, mitral insufficiency
4. cardiac dilatation เชนใน CHF จาก coronary heart disease, systemic hypertension, aortic valvular disease, cardiomyopathy, pulmonary hypertension, pulmonary embolus
สงทชวยทำาใหฟง S3 ไดดขน ไดแก เดกทม chest wall บาง ฟงในหองทเงยบในทานอนหงาย หรอ นอนตะแคงซาย ใชสวน bell ของ chest piece ของ stethoscope แตะเบา ๆ บนหนาอกคนไข และเจาะจงฟงในระยะ early diastole S3 มกฟงไดชดบรเวณ apex, S3 มกฟงไดชดเมอหายใจออก S3 อาจหายไปถาคนไขหายใจเขาเตมทแลวกลนไว S3 จะดงขนเมอออกกำาลง กดหนาทองคนไข หรอคนนอนยกขา
Fourth heart sound (S4)
S4 กเปนเสยง low-pitch เชนเดยวกบ S3 เพราะฉะนนในการฟง S4 กตองฟงดวยสวน bell ของ chest piece ของ stethoscope ดวยวธการอยางเดยวกบการฟง S3 ดงกลาวแลวขางตน S4 จากขางซายฟงไดชดบรเวณ apex สวน S4 จากขางขวาฟงไดชดแถว left sternal border
S4 เกดจาก sudden upward movement ของ atrioventricular valve ใน ventricular chamber เนองจากการท atrium บบตวอยางแรงเพอไลเลอดใหผานลงไปใน ventricle ทยดไมออกเพราะม hypertrophy, fibrosis, inflammation หรอโรคของ myocardium
S4 ในเดกพบไดใน cardiomyopathy, aortic stenosis (severe), pulmonary stenosis (severe), pulmonary hypertension
Gallop rhythm
คอ การทม S3 และ/หรอ S4 รวมกบ tachycardia หรอ cardiac pathology พบบอยใน advanced myocardial failure ถามทง S3, S4 เวลาฟงเสยงหวใจกจะไดเปน quadruple rhythm คอฟงไดเปน 4 เสยง ไดแก S1, S2, S3, และ S4
Systolic ejection click (SEC)
เปนเสยงทเกดตามหลง S1 แตหางจากเสยงทเกดจาก splitting ของ S1, systolic ejection click เกดจาก

1. การเปดของ semilunar valve (AV หรอ PV) ทตบยงไมแขง แลวหยดทนท เพราะเปดไดไมเตมทเมอ ventricle เรมบบตว
2. เกดเนองจาก sudden distention ของผนง aorta หรอ pulmonary artery เนองจาก impact อยางแรงของกระแสเลอดตอผนงเสนเลอด
pulmonary systolic ejection click ฟงไดชดแถว PVA เสยง click จะคอยลงหรอหายไปเมอหายใจเขา พบไดใน mild and moderate PS, idiopathic dilatation of PA, Eisenmenger syndrome
aortic systolic ejection click ฟงไดชดแถว apex บางครงฟงไดแถว AVA และ TVA เสยงนจะคงอยไมวาจะหายใจเขาหรอหายใจออก พบไดใน congenital AS (ไมคอยพบใน acquired AS เพราะตวลนมกม calcification), truncus arteriosus, TOF บางครงอาจฟงไดใน AR และ aortic aneurysm
Pericardial friction rub
เกดจากการขยบ visceral และ parietal pericardium ทมการอกเสบ เปนเสยง high pitch, superficial scratchy sound ทคลายกบเสยงทเกดจากการเอากระดาษสองแผนมาถกน มกฟงไดทงในระยะ systole และ diastole แตในระยะ systole เสยงมกดงกวาใน diastole และฟงไดชดมากขนถากดสวน chest piece ของ stethoscope ใหแนบแนนกบหนาอก บรเวณทฟงไดชดมกเปนบรเวณ upper sternum กบ apex บางครงถาสงสยวาจะม pericardial friction rub หรอไมอาจตองฟงโดยใหคนไขอยในทาตางๆ เชน นง นอนตะแคงซาย หรอทา knee chest จงไดยนเสยงทผดปกตน แมจะม pericardial effusion จำานวนมากกยงสามารถฟง rub นได
การแยก pericardial friction rub จาก pleural rub นนแยกโดยทถาใหคนไขกลนหายใจ pericardial friction rub จะยงคงไดยนอย สวน pleural rub จะไดยนเฉพาะชวงหายใจ นอกจากน pericardial friction rub มกไดยนบรเวณ precordium สวน pleural rub มกไดยนบรเวณถดจาก apex ออกไปทาง axilla
Heart murmur
Murmur เปนเสยงทเกดจาก turbulent flow ของเลอด การเกด turbulent flow นขนโดยตรงกบขนาดของชองทเลอดไหลผาน ความเรวของการไหลของเลอด ความหนด และความหนาแนนของเลอด เพราะฉะนน murmur จะเกดขนไดเมอมการตบหรอ รวของลนหวใจ หรอเสนเลอดมชองตดตอทผดปกตในหวใจหรอทเสนเลอด เสนเลอดมการพองตวหรอโปงออก หวใจเตนเรวขน เลอดไหลเรวขนหรอในภาวะทความหนดนอยลงเชนในภาวะทคนไขเปนโรคโลหตจางมากๆ

ในการบรรยายถงลกษณะของ murmur ควรบรรยายสงตอไปนคอ
1. Timing คอเปน systolic, diastolic หรอ continuous โดย systolic murmur คอ murmur ทเกดพรอมกบ S1 หรอตามหลง S1 และสนสดลงกอน S2 หรอท S2, diastolic murmur คอ murmur ทเกดพรอมกบ S2 หรอตามหลง S2 และสนสดลงกอน S1 หรอท S1 สวน continuous murmur คอ murmur ทเรมท S1 แลวผาน S2 ไปสนสดกอน S1 ใน stroke ตอไปหรอท S1 ใน stroke ตอไป
2. Nature เปนการบอกถงลกษณะของ murmur ซงอาจจะเปนแบบ ejection, regurgitant, rough, musical, blowing, rumbling, crescendo-decrescendo, machinery, etc.
3. Grade of maximal intensity อาศยความเบาดงของ murmur แบงเปน 6 grade ดงน
grade I เบามาก มกไมคอยไดยนในระยะแรกของการฟง ตองตงใจฟงมากจงจะไดยน
grade II เบา แตไดยนทนททเรมฟง
grade III ดงปานกลาง ไดยนชดเจน
grade IV ดง รวมกบการม thrill
grade V ดงมากฟงไดแมกระทงใชขอบใดขอบหนงของสวน chest piece ของ stethoscope แตะกบ chest wall
grade VI ดงมาก ๆ ไดยนแมกระทงเมอเอาสวน chest piece ของ stethoscope ใหหางจาก chest wall เลกนอย
4. Duration หมายถงความยาวของ murmur เชน ถา murmur ยาวตลอดระยะ systole กบรรยายวาเปน holosystolic หรอ pansystolic
5. Pitch หรอ frequency เชน murmur ของ AR เปนพวก high frequency พวกนตองฟงดวยสวน diaphragm ของ chest piece จงจะไดยนชด สวน murmur ของ MS เปนพวก low หรอ frequency ซงตองใชสวน bell ของ chest piece ในการฟงจงจะไดยนชด
6. Point of maximal intensity คอตำาแหนงทไดยนเสยง murmur ดงทสด เชน murmur ของ AS มกไดยนดงทสดบรเวณ LSB หรอ ICS ท 2 ดาน R

7. Respiratory variation คอการเปลยนแปลงตามการหายใจ เชน murmur ของ TR จะดงข
Heart Murmur ในทารกแรกเกด Heart murmur ในทารกแรกเกดกวารอยละ 50 เปน pathological murmur
การฟงเสยงหวใจเปนสวนหนงของการตรวจรางกายของทารกแรกคลอดทกรายเพอตรวจหา congenital heart disease ไดแตเนนๆ ในยคกอนทจะมการใช echocardiogram อยางแพรหลายเคยมผรายงานไววาทารกแรกเกดม heart murmur ไดถงรอยละ 60-77 แตในยคปจจบนทมการหาสาเหตของ heart murmur ไดแนนอนโดยการตรวจ echocardiogram พบวาอบตการณของ heart murmur ในทารกแรกเกดมประมาณรอยละ 1 การฟงไดยนหรอไมนขนอยกบประสบการณ ชวงเวลาทฟง และสภาพทงในตวทารกเองตลอดจนสภาพแวดลอม แม heart murmur ในเดกสวนใหญจะเปน 'innocent' murmur แตถานบเฉพาะ heart murmur ในทารกแรกเกดแลวสดสวนของ'pathological' murmur จะเพมขนมากเปนประมาณกวารอยละ 50 การแยก'innocent' murmur จาก 'pathological' murmur สามารถทำาไดดวยการประเมนทารกอยางละเอยด โดยภาพรงสทรวงอกหรอ คลนไฟฟาหวใจมสวนชวยนอย จดมงหมายสำาคญของบทความนเพอใหแพทยสามารถใชเปนแนวทางการวนจฉย และปฏบตเมอฟงไดเสยง heart murmur ในทารกแรกเกด
Innocent Heart Murmur ในทารกแรกเกด
ทารกแรกเกดปกตมการเปลยนแปลงทางสรรวทยาหลายอยาง ทอาจทำาใหเกด turbulent flow และ heart murmur ได ลกษณะของ innocent murmur เหลาน มกเปน mid systolic ejection murmur เบาๆ (grade 1-2/6) ฟงไดบรเวณ pulmonic area อาจ radiate ไปท axilla และ ทหลงได murmur เหลานมกหายไปเองเมออายประมาณ 3-6 เดอน นอกจากลกษณะของ murmur แลว การจะบอกไดวาเปน innocent murmur นนการตรวจรางกายอนๆตองปกตดวย
สาเหตทสำาคญ ของ innocent heart murmur ในทารกแรกเกด ประกอบดวย
1. Peripheral pulmonic branch stenosis (PBS)
เปนสาเหตทมหลกฐานสนบสนนมากทสดของ innocent murmur ในทารกแรกเกด เชอกนวา การทปรมาณเลอดทไหลผาน main pulmonary artery เพมขนทนทหลงคลอด ทำาใหเกด relative hypoplasia ของ pulmonary artery branch และม angulation ทตำาแหนง pulmonary bifurcation ทำาใหเกด turbulent flow เกด
เปนเสยง murmur ในทารกคลอดกอนกำาหนด PBS จะสมพนธกบการปดของ Ductus arteriosus(DA) มาก ทำาใหไมไดยนเสยง murmur ในชวงแรกหลงคลอด แตมาไดยนหลง DA ปดแลว ทำาใหตองแยกจากการเปดใหมของ DA
2. Patent ductus arteriosus (PDA)
PDA เลกๆทกำาลงจะปดเปนสาเหตทพบบอยมากอนหนงของ innocent murmur แมวาจะมผพยายามอธบายวา ความผดปกตของหวใจในกลม left-to-right shunt จะไมคอยไดยน heart murmur เรวตงแตเกดกตาม แตในความเปนจรง จำานวนทารกทม VSD และ PDA มสงมากเมอเทยบกบโรคหวใจชนดอนๆทำาให VSD และ PDA ยงเปนสาเหตของ heart murmur ทตองคดถงไวเสมอ ไมวาจะฟงไดเมอใด รวมทงวนแรกคลอด อยางไรกตาม ธรรมชาตของ DA ทจะปดเองในไมกวนแรก ในทารกแรกเกดปกต หากยงฟงไดหลายวนหลงคลอดกไมนานกถงสาเหตน นอกจากนนผเชยวชาญบางทานไมเชอวา PDA จะมสวนสำาคญนกในการเกด murmur แบบน
3. Patent foramen ovale (PFO)
ผเชยวชาญหลายทานเชอวาเลอดทไหลผาน PFO เปนสาเหตสำาคญอนหนงของ innocent murmur โดยพบวา ทารกทกรายทม murmur แบบนจะม high velocity ของ flow ผาน PFO อย สวนมากจะไมมอาการใดๆ และปดเองได
Pathological Heart Murmur ในทารกแรกเกด
Heart murmur ในทารกแรกเกดกวารอยละ 50 เปน pathological murmur บางรายงานใหถงรอยละ 84 ชงสาเหตตางกนไปบางในการศกษาแตละแหง ทสำาคญกคอ ในทารกทมแต heart murmur เหลาน ประมาณรอยละ 10 ควรไดรบการแกไขโดยเรวกอนเกดอาการ จะกลาวถงเฉพาะสาเหตทพบบอยและสาเหตทจำาเปนตองรบแกไขเทานน
1. Ventricular septal defect (VSD)
VSD เปนโรคหวใจพการแตกำาเนดทพบบอยทสด และเปนสาเหตของ heart murmur ในทารกแรกเกดทพบบอยทสดดวย Typical murmur จะเปน pansystolic murmur ทคอนขางดง โดยฟงชดทสดท lower left sternal border เสยง murmur ทดงและมลกษณะเปน pansystolic ทำาใหแยกจาก innocent murmur งาย แตแยกจาก tricuspid valve regurgitation (TR)ไดยาก แตแม murmur จาก VSD อาจฟงไดตงแตวนแรกหลงคลอด การท shunt ผาน VSD ขนอยกบการลดลงของ pulmonary vascular resistance แต flow ของ TR ททำาใหเกด murmur นไมเกยวกบ pulmonary vascular resistance ทำาใหเวลาทไดยน murmur อาจแตก

ตางกน โดย pansystolic murmur ทไดยนตงแตวนแรกคลอดมแนวโนมทจะเกดจาก TR มากกวา VSD ในทางกลบกนถามาเรมไดยนในวนหลงๆยงสนบสนน VSD มากกวา TR VSD ทม murmur เรวแบบนสวนมากจะเปน VSD ขนาดเลก ซงไมมอาการของ congestive heart failure
Muscular VSD ขนาดเลกอาจได heart murmur ทใกลเคยงกบ innocent murmur ได
2. Patent Ductus Arteriosus (PDA)
PDA เปนสาเหตของ pathological murmur ทพบบอยเปนอนดบ 2 ผอานอาจสบสนบางจากการทอานใน innocent murmur มาแลวแบงสาเหตกม PDA เชนกน ตองเขาใจวาธรรมชาตของ DA จะปดเองในทารกคลอดครบกำาหนดไมกวนแรก ระหวางทยงไมปดในชวงนนอาจทำาใหเกด murmur แบบ innocent ทกลาวขางตนได และเมอ DA ปดลงในเวลาตอมาเสยง murmur นกจะหายไป แต DA ทยงคงเปดอยหลายวนหลงคลอด หรอ DA ทมขนาดใหญ ซงพบบอยในทารกคลอดกอนกำาหนดจะทำาใหเกด murmur ทไมเปนแบบ innocent ทกลาวขางตน แตจะดงกวา ฟงไดหลงอาย 2-3 วนไปแลว และบางรายสามารถฟงไดเสยง continuous murmur ชดเจน(ซงพบไดนอย) การทสวนใหญเปน systolic murmur นเอง ถาเปนทารกคลอดกอนกำาหนดจะแยกยากจาก PBS มากจำาเปนตองใชการตรวจอนมาสนบสนน PDA เชน bounding pulses, hyperactive precordium, wide pulse pressure, respirator dependent, ภาพรงสทรวงอก หรอ echocardiogram
3. Tricuspid regurgitation (TR)
TR กคลาย PDA ตรงทมผชำานาญหลายทานแบงไปอยในกลม innocent murmur ทงนเพราะไมม structural defect และหายเองได แตในทนเหนวาทจรงแลว murmur จาก TR นมพยาธสภาพจรง โดยสมพนธกบ myocardial ischemia และ perinatal asphyxia ลกษณะ murmur เปน pansystolic ทแยกไดยากจาก murmur ของ VSD แตถาฟงไดทนทหลงคลอด และสมพนธกบ perinatal asphyxia ทำาใหนกถง TR มากกวา สวนมากแลว TR ทเกดจาก perinatal asphyxia นหายเองได แตบางรายกมปญหาหลงเหลออยนานได ขนกบความรนแรงของ myocardial ischemia และ perinatal asphyxia ดวย
4. Right ventricular outfow obstruction
Right ventricular outfow obstruction เปนสาเหตทพบบอยเปนอนดบตนๆของ pathological murmur โดย Pulmonic valve stenosis (PS) และ Tetralogy of Fallot(TOF) เปนโรคทพบบอยทสดในกลมน ลกษณะ murmur เปน

systolic ejection ฟงไดทนทหลงคลอด แยกจาก PBS ไดตรงท murmur จาก right ventricular outfow obstruction จะมเสยงดงมากกวา บางทานอาจคดวา ใน TOF นาจะม cyanosis ใหเหน แตจรงๆแลว TOF ในทารกแรกเกดมอาการ อาการแสดงแตกตางกนไดมาก ในรายทม right ventricular outfow obstruction ไมมากนอาจไมเหน cyanosis เลยในระยะแรกเกด
5. Left ventricular outfow obstruction
Left ventricular outfow obstruction เปนสาเหตของ pathological murmur ทพบไมบอย โดย Aortic valve stenosis(AS) เปนโรคทพบบอยทสด ถงแมจะพบไมบอย แตมความสำาคญเพราะกวารอยละ 50 จะมาดวยเรองของ heart murmur ทไมมอาการอะไร ทารกกลมนจำานวนไมนอยทตองการการแกไขโดยเรวกอนเกดอาการ ลกษณะ murmur เปน systolic ejection ทดง ฟงไดทนทหลงคลอดเชนเดยวกบ murmur ของ right ventricular outfow obstruction ดงกลาวขางตน แยกไดยากจากการตรวจรางกายอยางเดยว มกตองอาศย echocardiogram ในการวนจฉย
6. Atrial septal defect
Atrial septal defect เปนสาเหตของ pathological murmur ทพบไมบอย สวนมากจะไมมอาการใดๆ และปดเองได ลกษณะ murmur เปน systolic ejection ทฟงไดทนทหลงคลอด ถา murmur เบากแยกไดยาก PBS และถาดงกแยกไดยากจาก left หรอ right ventricular outfow obstruction จากการตรวจรางกายอยางเดยว มกตองอาศย echocardiogram ในการวนจฉย
แนวการปฏบตเม�อฟงได heart murmur ในทารกแรกเกด
จะเหนไดวา แม innocent heart murmur จะมลกษณะทคอนขางจำาเพาะ แตบางครงกแยกไดยากจาก pathological murmur นอกจากนนในรายทเปน pathological murmur นนการใหการวนจฉยทแมนยำาทำาไดยาก เมอฟงได heart murmur ในทารกแรกเกดจงมขอแนะนำา ดงน คอ
1. พงระลกไวเสมอวา heart murmur สวนใหญของทารกแรกคลอดเปน pathological murmur ไมใช innocent murmur
2. ตรวจใหแนวาทารกนนไมม cyanosis, heart failure หรอ คลำาชพจรไดเบากวาปกต หากมอนใดอนหนงตองรบรบไวในโรงพยาบาล สงตอกมารแพทยโรคหวใจโดยดวนทสด

3. Heart murmur ทดง(เกน grade 2/6 ขนไป) หรอทฟงไดหลง 24 ชวโมงแรก มกเปน pathological murmur ควรสงตอกมารแพทยโรคหวใจ แตถาไมมอาการอนใด การสงตอกไมรบดวนนก
4. Heart murmur ทมลกษณะทไมใช systolic ejection เปน pathological murmur เสมอ ควรสงตอกมารแพทยโรคหวใจ
5. Heart murmur ทม systolic ejection click หรอตรวจได hyperactive precordium ดวย เปน pathological murmur เสมอ ควรสงตอกมารแพทยโรคหวใจ
6. การไมสงตอมเฉพาะกรณฟงได typical heart murmur ของ PBS อนไดแก systolic ejection murmur เบาๆ (grade 1-2/6) ฟงไดบรเวณ pulmonic area อาจ radiate ไปท axilla และ ทหลงได พงสงวรณไววา ทารกเหลานตองดปกต ดดนมไดด ตรวจรางกายไมพบความผดปกตอนใด และ murmur ของ PBS
เหลานมกหายไปเอง กรณยงฟงไดเรอยๆแมจะตดตามมาแลวระยะหนง กควรสงตอเชนกน
7. กรณทารกคลอดกอนกำาหนดทจรงแลวยากมากทจะแยก murmur ของ PBS จาก PDA of prematurity หรอ congenital heart disease อน คำาแนะนำาในตางประเทศมกใหทำา echocardiogram เพอชวยวนจฉยเสมอ แตสถานการณในประเทศไทยทมผชำานาญนอยคงทำาแบบนนไดยาก ความเหนของผเขยนเองคดวา ตองใชสงประกอบหลายอยางมาชวยตดสนใจทงอาการ, ลกษณะ murmur, ชพจร, pulse pressure, precordial activity, ภาพรงสทรวงอก มาชวยวนจฉย หากมขอสงสยวาจะไมใช PDA of prematurity กควรสงตอกมารแพทยโรคหวใจเชนกน
TABLE 422-4 -- Pulse Rates at Rest
AGELOWER LIMITS OF NORMAL
AVERAGE
UPPER LIMITS OF NORMAL
Newborn
70/min 125/min
190/min
1–11 mo
80 120 160
2 yr 80 110 1304 yr 80 100 1206 yr 75 100 115

AGELOWER LIMITS OF NORMAL
AVERAGE
UPPER LIMITS OF NORMAL
8 yr 70 90 11010 yr 70 90 110
GIRLS BOYS GIRLS BOYS GIRLS BOYS12 yr 70 65 90 85 110 10514 yr 65 60 85 80 105 10016 yr 60 55 80 75 100 9518 yr 55 50 75 70 95 90
เขยนเองหวะ
ปกตแลว PDA สามารถปดเองไดภายในอาย 1 ป แตเนองจากผปวยรายนมอาการของ heart failure เชน ชพจรคอนขางเรว มapnea ปอดมลกษณะของ pulmonary edema มภาวะหวใจโต ดงนนจงควรพจารณาผาตดปด PDA ทนท แตผปวยเปนทารกคลอดกอนกำาหนดและมอาการในชวง 10 วนแรกเกด ดงนน จงสามารถทดลองใชยา indomethacin ได (แตมขอหามใชในผปวยทม renal dysfunction, bleeding tendency, NEC หรอ shock)
โดยใหยา dose แรก คอ 0.38 mg , dose ท2 คอ 0.47 mg, dose ท3 คอ 0.47 mg ใหทางหลอดเลอดดำา drip over 30 minute ในแตละ dose และใหยาหางกน 12-24 ชวโมง โดยทงหมดนถอเปน 1 course
ในระหวางทผปวยไดรบยาน ตอง monitor urine output ดวย หากผปวยปสสาวะนอยลง ควรเวนระยะเวลาระหวางการใหยาแตละ dose ใหนานขน
หาก PDA ยงไมปด จงใหซำาอก 1 course (maximum 2 courses)
หาก PDA ยงไมปด จงพจารณาผาตดดวยวธ double ligation or division PDA or coil embolization ซงตองดตามความเหมาะสมตอไป


















