June 2009 - SCTS...35-43 Lincoln's Inn Fields, London WC2A 3PE Tel: +44 (0) 20 7869 6893 Fax: +44...
36
Society for Cardiothoracic Surgery in Great Britain and Ireland The Evolving Role of the Cardiothoracic Dean The Fate of Abstracts The Expanding Role of Nurses The Role of SCTS in Clinical Excellence Awards The Selection Process - A Candidate’s Experience The AF Consensus Statement - A UK Surgeon’s View Intercollegiate Examination Annual Meeting 2009 Bournemouth Review the June 2009
Transcript of June 2009 - SCTS...35-43 Lincoln's Inn Fields, London WC2A 3PE Tel: +44 (0) 20 7869 6893 Fax: +44...

Society for Cardiothoracic Surgeryin Great Britain and Ireland
The Evolving Role of the Cardiothoracic Dean
The Fate of Abstracts
The Expanding Role of Nurses
The Role of SCTS in Clinical Excellence Awards
The Selection Process - A Candidate’s Experience
The AF Consensus Statement - A UK Surgeon’s View
Intercollegiate Examination
Annual Meeting 2009Bournemouth Review
theJune 2009

theBulletin2
Society for Cardiothoracic Surgery in Great Britain and Ireland
The Royal College of Surgeons of England35-43 Lincoln's Inn Fields, London WC2A 3PETel: +44 (0) 20 7869 6893Fax: +44 (0) 20 7869 6890Email: [email protected]
President’s Report 3
Secretary's Report 5
Launch of the 6th Annual Cardiac Database 6
The Evolving Role of the Cardiothoracic Dean 6
The Cardiothoracic Forum at Bournemouth 2009 8
The Expanding Role of Nurses in Cardiothoracic Surgery 10
Notes from the Patient Representative 12
The Intercollegiate Examination in Cardiothoracic Surgery 14
Stepping Down - the Cardiothoracic Tutor 15
The Fate of Abstracts 16
Cardiothoractic Surgery Research Club 17
The Role of the Society in Clinical Excellence Awards 18
Symposium Debates - NCEPOD Report 20
New Administrator 21
Titre 2 Trial Summary 22
Two new SCTS Posts 22
The Trainees’ Newsletter 23
National Selection Process for Cardiothoracic Surgery - A candidate’s view 24
Society Cardiac Scholarship 26
New Appointments 27
Annual Meeting 2009 - Bournemouth Report 28
Forthcoming Events 31
A UK Surgeon’s Perspective on the AF Consensus Statemeent 32
Crossword 34
Contents
bulletinthe
Edited by Sunil Ohri, Communications Secretary Contact: [email protected]
Designed & produced by CPL Associates, London

June 2009 3
President’s Report Leslie Hamilton
By the time you read this the “Blue Book”will have been published. This is anotherlandmark achievement for the Society. Atribute not only to the skills of BenBridgewater as lead Editor and RobinKinsman (of Dendrite) as chief analyst butalso to the professionalism of all thesurgeons who contributed their data witha view to improving the quality of patientcare. A big thank you to all whocontributed and to Dendrite forunderwriting the costs of publication. Wehave always been ahead of the game –not always comfortable but the rightplace to be. I was interested to note thatthe first 3 articles in the May volume ofthe EJCTS were about quality issues inboth cardiac and thoracic surgery.
Our focus on improving the quality of carewe give to our patients has meantchanging the emphasis away frommortality (which ignores the 98.4% ofpatient who survive) to other outcomemeasures – this edition of the Blue book isthe first attempt to look at these in detail.One way we can identify areas forimprovement is to look for variations incare. This analysis has shown two suchareas: referral for aortic valve replacement(an issue for Commissioners) and rates ofmitral valve repair. We would all agree that,where possible, repair is better thanreplacement. I doubt that anyone wouldachieve the 98% reported by David Adams(our guest at our meeting inBournemouth). There will be validexplanations for some of the variation.However we do need to ask questions ofourselves. It is not easy to be self criticaland change is difficult but it is part of ourprofessional responsibility. It is especiallyimportant now with percutaneousmethods of repair being introduced – theone year data from the Everest (using theMitraclip) registry has just been released(the randomised trial data is awaited) andthe ACCESS – Europe registry is recruiting.
It is my dream that we (SCTS) couldproduce a similar “book” for Thoracicsurgery.
Information gives power and influence –power to look at quality of care, to raise thestanding of the specialty and to influencethe development of the service. The issueof data collection has been more difficultfor Thoracic surgeons. No risk stratificationexisted and there was not the samepressure on Trusts to provide theresources. Things have changed –Thoracascore has been accepted andAlessandro Brunelli (another of our guestsin Bournemouth) has published a“performance score” measuring quality ofcare after lung resection (EJCTS 2009;35:769) using the European database. Iwas therefore delighted when this year’s
Thoracic Forum affirmed the decision ofthe previous year to commit to detaileddata collection. At the request of the Forummembers I have written to all ChiefExecutives asking for support andresources. In my letter I set out some of thereasons for detailed data collection: if wedon’t measure quality of care we can’timprove it; benchmarking against otherunits, explanation of variations in mortalitybased on HES data; information forsurgeon’s re-certification ...the list goeson. The dataset to be collected has nowbeen agreed so I hope we can take thisforward. The recent UK Lung cancer auditshowed not only low but also variable ratesof resection around the UK and we need tobe able to address this – we need data! Weare currently working on a positionstatement on this audit with the UK LungCancer Coalition.
Annual Meeting
This is the first Bulletin since the annualmeeting in Bournemouth – see the reportinside. An excellent programme coveringthoracic, congenital and adult surgery andthe Forum going from strength to strength.I have heard nothing but positive reportsso in recognition of the huge amount ofwork involved, I want to record publicly mythanks on your behalf to the organisingteam of Simon Kendall, Ian Wilson, TaraBartley, Isabelle Ferner and Tilly Mitchell (aspecial welcome to Tilly, our new memberof staff in the office) and of course RachelWoolf, now enjoying her new life in Israel.
I have put off mentioning the EuropeanWorking Time Regulations until now! JohnBlack, President of the RCSEng is currentlyleading a response supported by the 4Colleges – his concern is that lack offorward planning by Trusts and specialtieswill mean that implementation will have anegative impact on both training andservice. All the Specialty Associations havesupported him in this concern. However,Our SAC has looked at this is detail andboth we (SCTS) and the British
continued on next page
Our focus on
improving the quality
of care we give to our
patients has meant
changing the
emphasis away from
mortality to other
outcome measures

VASCUTEK, a TERUMO CompanyNewmains Avenue, Inchinnan, Renfrewshire, PA4 9RR, Scotland, UKTel. +44 141 812 5555 Fax. +44 141 812 7170 www.vascutek.com
Conceived, Created and100% Manufactured in the UK
for over 30 years
President’s Report continued
theBulletin4
Orthopaedic Association believe that, with changes in how weprovide the service and a focus on those in training posts, we cantrain in 48 hours under the EWTR. As a Society we began toaddress this in 2003 when a working group put forwardsuggestions for “new ways of working”. My own Trust has recentlyappointed a team of Nurse Practitioners to replace the previoustier of SHOs. We had a vigorous debate on the EWTR at the Boardof Representatives in March and I recognise that the issue ofresident ICU cover is not resolved.
On the question of the Board of Representatives: this wasestablished to act as the forum for discussion / communicationbetween the membership and the Executive. It meets in Marchand November - please use it. Put forward issues for discussion;ask your unit representative for a report afterwards.Communication is important – if there are any pressing issues youcan contact me anytime (0191 2137309 or home: 0191 2850052).
In his report, Pat Magee gives you an insight as to how the Societyprovides support for ACCEA applications. A new feature last year(introduced I think by the NHS Medical Director) was that thesummary statements of successful applicants are available toview on-line. A positive step to transparency – you can now seewhy awards are made.
Surgery or PCI?
Whether patients have surgery or PCI continues to provokedebate. NCEPOD (see article inside) strongly supported MDTmeetings. I have explored this with the President of BCIS and theyhave set up a working group to suggest which patients should bediscussed – Graham Cooper is representing SCTS. Another jointeffort (David Taggart, Ben Bridgewater and I) with BCIS has beenan editorial highlighting the Syntax trial which we have sent to theBMJ. David has also been asked to work on the revascularisationguidelines for the European Society for Cardiology. The Couragestudy was controversial (it questioned the benefits of PCI) buthighlighted the need to have objective evidence of myocardialischaemia before PCI. You may have seen the recent “Fame” studywhich used pressure wires to calculate FFR (fractional flowreserve) in multi-vessel PCI using DES (NEJM 2009; 360:213).Another recent publication which you might find useful indiscussion is one from the AHA/STS/AATS: “AppropriatenessCriteria for Coronary Revascularisation” (JACC 2009; 53)
An example of new technology being introduced rapidly ispercutaneous AVR (TAVI). Neil Moat, elected representative onthe Executive, is leading for us in these discussions. Currentlythere is debate about a UK randomised trial (with pressure toextend to lower risk patients) and a European trial based on theSyntax model. We will keep you posted.
You will be aware of the Department of Health’s intention tointroduce the WHO “Safe Surgery” checklist. Having discussed itwith number of you, thoracic surgeons seem happy with it but itdoesn’t seem to lend itself to cardiac surgery. I have thereforeasked Steve Clark (who recently obtained his pilot’s licence) toadapt it. We will have discussed it at the Executive committee inJune and if it is accepted I will circulate it via the unit reps forcomment. If we can have a nationally accepted / SCTS approved
checklist, I hope that the DoH and Trusts will allow us to use itinstead of the WHO one.
I recognise that it doesn’t affect many of you but the futureconfiguration of paediatric cardiac surgery is an importantpolitical question for our specialty. We have recognised for manyyears that the service with the current number of units wasunsustainable – the one recommendation from both the Kennedyand Monro reports which was not accepted by the politicians wasfor bigger units. The paediatric cardiac community agreed (at ameeting at the DoH in July 2006) that we would provide thehighest quality sustainable service with 5 surgeons in each unit.The DoH has now accepted the need for change – they have askedthe NSCG (National Specialised Commissioning Group) to takethis forward urgently. Again, I will keep you informed.
Sabbaticals
I will finish on a positive note: sabbaticals. I wish I could tell youthat the DoH was going to introduce these into the NHS (like inAustralia and Scandinavia). But, we have the next best thing – theSCTS Ionescu scholarship for Consultants. Originally we restrictedapplications to Consultants within 5 years of appointment butthere is now a feeling that “older” Consultants would benefit froma short sabbatical. Let’s have some applications - seewww.scts.org.

Secretary’s Report Graham Cooper
June 2009 5
The publication of the sixth National Adult Cardiac SurgicalDatabase Report ‘Demonstrating Quality’ represents anothermilestone for SCTS. This latest edition of The Blue Booksignificantly advances the agenda for adult cardiac surgery,showing that our vision extends beyond operative survival intoa broad range of long term outcomes and equality of access totreatment. As members of SCTS we should all be rightly proudof the achievement. I thank you all for making this possible andwe should all join with Leslie in thanking those involved in theBlue Book’s production.
The power of the National Adult Cardiac Surgical Database tocontribute to the quality agenda is evident. Less obvious is itspower to protect members of SCTS. Since the events at Mid-Staffsconcerns about patient safety and service quality have aheightened sensitivity. On several occasions, data from othersources have led the Care QualityCommission to express concern aboutcardiothoracic services. Thanks to ourunique relationship with the Care QualityCommission, developed through thepublic release of cardiac surgicaloutcomes, and the unique resource ofthe database we have been able toeffectively and positively providesupport.
Over the past few months we have beendeveloping our thinking about how wemanage the possibility that a surgeon’soutcomes may cross an alert or an alarmline. There are three key principles; theprocess must not lead to patients whoare at high risk being denied surgery, theresponse must be reasonable andproportionate and that the crossing of aline is a stimulus to interrogate the dataand not the surgeon. This has been debated at The Board ofRepresentatives in November 2008, Annual Business meeting inMarch 2009 and the policy was approved by The Executive on 5thJune 2009. Full details are on the website. In outline; there are twoalert lines at 95% (equivalent to 2SD) and 99% CL and an alarmline at 99.9% CL, this is about 3.5 SD and is the limit used for thepublic portal of the Care Quality Commission. There are threepatterns of crossing the line and this relationship along with theresponse are shown in the table.
The response is proportionate and reasonable. There is a fourstage process to be undertaken to explain any divergence inoutcomes:
• Analysis of the data for accuracy• Analysis of the caseload to ensure that the risk stratification
mechanism in use accurately reflects expected outcomes• Analysis of institutional factors that may contribute to the
divergence in clinical outcomes• Analysis of the surgeon’s performance
We anticipate that it will be anextremely rare event for the processto proceed beyond stage 2. Clearlythe first stage, if there is adivergence in outcomes, is to checkthe data for accuracy. The secondstage is equally important. Theprocess must not lead to patientswho are at high risk being deniedsurgery. We know that for somegroups of patients, especially someof the higher risk patients,EuroSCORE is a poor predictor of risk. Analysis of the caseload ofa surgeon with divergent outcomes is therefore vital, if thesurgeon is operating on more patients in these groups then anydivergence is likely to be simply explained by casemix.
We will be implementing this with immediate effect for the nextupload to the Care Quality Commission website but as always arecontinually looking to improve and so any comments arewelcome; [email protected].
The rapid strides to developing a National Thoracic SurgicalDatabase in the past year are exciting and have the enthusiasticsupport of SCTS Executive. With the experience we have gainedover the past few years we hope to be able to make this a realityquickly. Richard Page has worked hard on this project and withyour support the first National Thoracic Surgical Database reportshould not be too far away.
All in all a time of great optimism, by aligning SCTS with the NHSpriority for quality and leading the delivery of this agenda we havegained respect and can look forward to continuing influence. Anexciting prospect. Enjoy your summer.
Level Frequency
Isolated Recurrent Persistent
First instance in a Second or more instance Second or more instancemonitoring cycle in a monitoring cycle in a monitoring cycle ofof 3 years of 3 years with a gap 3 years with no gap
of at least 1 between monitoringmonitoring period periods
95% CL Letter to Surgeon Letter to Surgeon Letter to Surgeon and Audit lead and Clinical Director
99% CL Letter to Surgeon Letter to Surgeon Letter to Surgeon and Audit lead and Clinical Director Medical Director and CQC
99.9% CL Letter to Surgeon Letter to Surgeon Letter to SurgeonMedical Director Medical Director Medical Directorand CQC and CQC and CQC

Launch of the 6th National Adult Cardiac Database Report
theBulletin6
This July will see the release of the next‘Blue Book’ SCTS National Databasereport; ‘Demonstrating quality’. Theprevious edition was published in 2004with data up to the end of March 2003.This latest report has been updated tostudy operations undertaken up to theend of March 2008; the database nowcontains over 400,000 operation records.
The analyses show a continuing increase inthe number of patients having valveoperations, and a stabilisation of thenumber of patients undergoing CABGsurgery each year, at around 23,000operations each year. Over time, thequality of data submitted to the databasehas also improved. The majority ofimportant data fields now have a lowincidence of missing data. This is due tothe enormous work of cardiac surgeryaudit leads and database managersaround the county without whom thereport would not have been possible. Themajority of the analyses and thepublication of the book were kindlyundertaken by Dendrite Clinical Systems.
The major finding of the analyses is thatthe patients coming to surgery arebecoming older and higher risk each year.Despite this trend, the mortality ratescontinue to fall. The degree ofimprovement is marked; between 2001and 2008 the in-hospital mortality ratesdecreased from 2.3% to 1.5% for isolatedCABG, 2.6% to 1.7% for all CABG, 5.2% to3.5% for isolated valves and 8.3% to 6.1%for combined valve and graft operations.We have also been able to gain longer-termoutcomes on these patients by linking theCentral Cardiac Audit Database (CCAD)with data on life status from the Office forNational Statistics (ONS). For example, wehave overall mid-term survival on over88,000 patients who have undergoneCABG which shows a survival rate of over90%. Survival is worse for patients who areolder, female, urgent, diabetic, haveimpaired cardiac function or who are inrenal failure. We have conducted adetailed analysis on patients undergoingCABG as elective operations, which showsexcellent results, with low mortality,morbidity and good long-term survival. The
mortality for patients under 70 years ofage who are admitted to hospital fromhome for their surgery is less than 1%. Wehave also conducted a detailed analysis oncardiac surgery in the elderly.
The database has now evolved to theextent that we can now analyse valveoperations, which have in previous reportsonly been examined from the returns to thecardiac surgical register. Between April2003 & March 2008 we have collected dataon 30,127 aortic valve and 19,545 mitralvalve operations. There has been morethan two-fold increase in the annualnumber of patients who have valve surgeryreplacement between 2001 and 2008.Patients undergoing AVR are becomingmore likely to receive biological valves andthose undergoing mitral surgery are morelikely to undergo a repair rather than areplacement. A detailed study has beenundertaken on patients undergoingsurgery for degenerative mitral valvedisease. We have also analysed outcomeson 4,967 patients who have undergonemajor surgery of the aorta, with 2,245
This is my last article as Dean. TheDean’s role in the SCTS has changedduring my tenure. The Dean no longersits on the executive but sits on theEducation subcommittee. This committeeis chaired by Professor John Pepper (theEducation Secretary) and is working hardto support all education within ourspecialty from medical school toretirement.
With every trainee and consultant havingto undergo annual appraisal I think that itis essential that the SCTS takes the lead instating the educational requirements at alllevels of a cardiothoracic surgeon’s career.This becomes increasingly more relevantas we enter the era of revalidation. TheSCTS annual meeting continues to grow in
attendance and the quality has improvedbeyond recognition especially when I recallsuch infamous venues as Llandudno andNorwich (both in the 1990s). This year Iwas delighted to see a good attendance atthe trainees’ meeting, although sadly notevery NTN attended. The trainees’meetings have become more interactiveover the last five years and I wouldencourage all trainees to give their opinionon training (or lack of it). The annual SCTStrainees meeting is the ideal forum foropen discussion but I would like to remindall trainees that they should contact theirregional SAC liaison member if they havespecific issues.
The Dean sits on the IntercollegiateCardiothoracic Surgery Examination
Board. The last fiveyears have alsoseen many changesin the Examination.The written paperhas been introducednegating the need for a basic science vivaand the scoring system has been reviewedfor the clinicals and vivas. The examinersare now assessed more rigidly byreviewing their marking and by directobservation of their examining skills. TheExamination is an intense experience forthe candidates but it is also quite anexhausting but rewarding 2 days for theexaminers and I would like all consultantsto consider applying to be an examiner andyou can find the details on the websitewww.intercollegiate.org.uk.
The Evolving Role of the Cardiothoracic Dean
Steven Hunter,Cardiothoracic Dean

June 2009 7
having surgery for an aortic aneurysm and 1,288having surgery for an aortic dissection. Themortality for patients undergoing urgent oremergency surgery for dissection was 23%, which isin line with published international registries.
In addition to analysing the changes in patients andtheir associated outcomes, we have also tried touse the database report to respond to some of theexternal influences that act upon our speciality. Wehave examined how developments in cardiacsurgery audit comply with the recommendationsfrom the Bristol Royal Infirmary Inquiry (2001), theShipman Inquiry (2005), the Chief Medical Officersreport Good Doctors, Safer Patients (2006), theWhite Paper Trust, Assurance and Safety (2007) andLord Darzi’s review High Quality Care for All (2008).We have also moved away from mortalitymeasurement to look at other post-operativeoutcomes including new post-operative stroke,renal failure, length of stay, re-explorations forbleeding or infection and 5-year survival rates. Wehave used the power of the database to look atissues surrounding equity of access to aortic valvesurgery by mapping 29,000 AVR operations intotheir PCT of residence and adjusting access rates forthe age and gender structure of the populations.
We have included good practice examples in thecollection and use of cardiac surgery audit datafrom the hospitals around the United Kingdom. Thissection includes examples on data validation,feedback, quality bundles, performance monitoring,disseminating outcomes to patients, servicereconfiguration, clinical leadership developmentand multi-disciplinary process and outcomesbenchmarking. Finally, we have developed aproposed quality account for one hospital,incorporating patient outcomes, patient safety andpatient experience, in line with the planned newlegislation, which will require all hospitals topublish these accounts from 2010.
The latest Blue Book contains an enormous amountof data, which has been diligently andcomprehensively collected in all the unitsundertaking NHS cardiac surgery across the UK,with further contributions from some PrivateHospitals, Hospitals in Ireland, and a guestcontribution from Hong Kong. We hope that thedatabase report will provide useful information tohospitals and surgeons providing cardiac surgicalcare give accurate information to support informedconsent for patients, and contribute towardsimproving quality across the NHS.
Ben Bridgewater, Chair, SCTS Database Committee
‘Demonstrating Quality’
Over the last 5 years the SAC has madehuge strides for training in our specialty.Changing from Calman to MMC coincidedwith a reduction (to zero for a couple ofyears) of trainees admitted to ourspecialty. This was a difficult time butnecessary to restore balance and avoidsubsequent unemployment. Thecurriculum project has been a hugeachievement and now all trainees haveinstant access on line to an array ofassessment tools which can be used bythe training programme directors duringthe ARCP. The establishment of thePostgraduate Medical Education andTraining Board (PMETB) saw the end of thequinquenial training programme reviews.PMETB introduced Deanery (pan-specialty) assessments which areessentially a paper exercise. The SACrecognised the failings of PMETB andinsisted on the training programme liaisonmembers attending all the RegionalTraining Programme meetings and
RITA/ARCPs and producing an annualreport on each programme. This report isdiscussed at he SAC but can also be usedby the Deaneries to trigger PMETB(specialty) visits. I have already mentionedthe liaison members and their relationshipwith trainees but I would like to emphasisethe importance of the pastoral role of theliaison members. Trainees should nothesitate to contact their liaison memberfor advice. The SAC has also taken the leadin national selection. We were the firstspecialty to appoint our ST3s nationally in2008. We had another round this yearappointing 16 trainees (2 were ACFs –Academic Clinical Fellows). The SAC haveorganised the selection but theassessments are performed by the TrainingProgramme Directors (TPD) and many ofthe TPDs are now directly involved with theorganisation of next year’s selection. TheSAC will continue to be involved but with aquality assurance remit. I would like tothank all the TPDs for their commitment to
national selection and I would also like tothank the West Midlands Deanery, and inparticular Denise Harris, for their supportin hosting the last two selections. Theselection process will evolve and time willtell whether it accurately selects the futureleaders of our specialty.
The last 5 years have provided manychallenges but all have been met head onand I believe our specialty has gone fromstrength to strength. Our colleagues whoare involved with the SCTS executive, theSAC and the Exam Board are all to becongratulated for their efforts and it hasbeen a pleasure working along side themfor the last 5 years. My successor is to beelected over the summer and I wishhim/her all the best and I hope they relishthe challenges of the next 5 years.
As always I can be contacted by email [email protected] but only asDean until August.

theBulletin8
The sun shone in Bournemouth, the sealooked fabulous and this yearsCardiothoracic Forum was a huge success.Delegate numbers have increased year onyear with a diverse audience that gave alively buzz to the meeting.
This year’s theme ‘Quality Care: can wedeliver’ was topical within the specialityand the wider NHS agenda. We welcomedMaura Buchanan back to deliver heropening remarks. She captured the moodperfectly linking current health issues withputting patients first. As part of the NHSagenda and SCTS objective for greaterpatient involvement, a patientrepresentative group joined the meetingand feedback would suggest that theyenjoyed Maura’s comments andspecifically the presentation from LisaKetteridge and the clinical team from theQueen Elizabeth Hospital, Birmingham.Lisa’s story hit the national press after shedeveloped cardiomyopathy while pregnantwith her second child in April 2008.Following an emergency caesarean atthirty five weeks gestation she had anLVAD implanted. Her 60 day stay coincidedwith the 60 year celebrations of the NHS.Mr Ian Wilson, Cardiothoracic surgeonpresented the case accompanied in thebackground by Bob Dyans ‘The TimesThere Are A Changing’, while Judith Derby
and Linda Williams, Senior Sisters from theCritical Care unit eloquently express thechallenges of caring for a patient with anLVAD, multi organ failure but not forgettingthat Lisa had just had her second childdelivered. The microphone was then takenby Lisa who told us what it was really like!The impact of hearing the patientperspectives serves to remind us all ofwhat the patient sees as important andshould inform the delivery of care.
Other plenary sessions included the newBTS guidelines on Cancer staging, and areview the impact this will have on surgicaldecision making process, presented by MrEric Lim from Guy’s and St Thomas’. Thissession was clear, concise anddemonstrated the positive effect uponpatients. It also provoked the audience tocontemplate the impact upon surgical units.
Wendy Grey from the Heart ImprovementProgramme shared the work initiated bythe Eighteen Week National ProjectSustaining Cardiac Pathways outlining theproject and giving examples from pilotsites around the UK. Members of theaudience can take the ideas back to theirunits to review the patient pathway andinitiate change. Dr David Foster, Deputy Chief NursingOfficer, DoH, spoke on the impact of
Modernising Nursing Careers onpostgraduate career pathways and AndrewRundle from the Standards & Qualification,Skills for Health discussed the strategicimpact of changing the workforce. Thisprovoked a lively debate around achievinga workforce fit for practice and thedilemma around whether Agenda forChange can meet the challenge of ensuringnurses can have a clinical career structure.Clearly, the way forward is not withouthurdles but the presentations can be usedto inform us in our progress.
Dr Ann Keogh, Birmingham HeartlandsHospital presented on behalf of theNational Patient Safety Project. She gaveus a very practical demonstration howsome of the areas of the work can impactupon practice to underpin the theme ofquality care.
The Cardiothoracic Forum Abstract panelwere able to select thirteen papers forpresentation in addition to the plenarysessions. Speakers were of a very highstandard with sessions encompassingCardiac, Thoracic and Surgical CarePractitioner themes. All thesepresentations can be accessed on thenurses’ page of the SCTS web site;www.scts.org/sections/nurses/index.htmlThe audience selected this years winner ofthe Ethicon £200 prize as:
Postoperative Pulmonary ComplicationsFollowing Thoracic Surgery: Comparison Of Three Scoring Systems P Agostini
Our congratulations go to Paula who willreceive her winners medal during theAnnual dinner at next years SCTS meetingto be held in Liverpool 7th March- 9thMarch 2010. The theme for next year’smeeting will be ‘Excellence in Practice’where we will hope to encompass themessage from the Chief Nursing Officer toengage staff and public involvement thatwill underpin confidence and trust indelivering high quality care for all. So withthis in mind I would encourage you andyour colleagues to consider sharing your
The Cardiothoracic Forum at the Annual Meeting in Bournemouth
Lisa Ketteridge (LVAD recipient, centre), with senior cardiac ITU nurses Linda Williams(left) & Judith Derby (right)

June 2009 9
work and experiences with next year’sCardiothoracic Forum. The call forabstracts will go out early in Septemberand remain open until November. This yearall abstracts will need to be submitted online to enable the abstract committee tocarryout the marking procedure efficientlyand to ensure that the programme can beput together in good time.
Other News from the Speciality
Congratulations to the West of ScotlandHeart and Lung Centre, Golden JubileeHospital who celebrated their firstanniversary with a one-day conference thatlooked at Quality and Innovation within theCardiology and Cardiothoracic Surgicalspeciality. The day was well attended withan audience that represented themultidisciplinary professions. Theprogramme encompassed a varied ofpresentations including ‘How to set up anEuropean Centre of Excellence’ fromProfessor Hetzer from Berlin who alsotalked about their LVAD progamme. MrDalrymple-Hay, Consultant at PlymouthHospital spoke about Minimally InvasiveConduit Harvest; Dr Grube, chair ofCardiology, Seigburg Heart Centre and MrMoat, Consultant at the Royal Bromptonspoke about their hospital’s TAVIprogramme. I was invited to speak on NewWays of Working and Professor Begg,Associate Dean Primary Health Care,School of Health, University of
Wolverhampton presented on thePhysicians Assistants. This is just some ofthe areas covered during what proved tobe an interesting, thought provoking daythat gave all an opportunity to hear aboutdevelopments throughout the UK andEurope.
For those of you who are not aware of theone day ‘Thoracic Surgery Practical Course’that runs twice a year in June and Januaryat the Heartlands Hospital, Birmingham itcombines lectures with clinical wet labsessions enabling delegates to familiarisethemselves with chest anatomy, surgicalprocedures and disease process. Thecourse is open to nurses, doctors,physiotherapists, surgical carepractitioners and other members of the multidisciplinary team. For further information [email protected]
We have updated and tested the data basewhich is working well. There are nowcontacts for all nurses who wish to beincluded; a lead contact in each unit intheir critical care, ward and theatres; andthoracic contacts. If any of your colleagueswould like to add their names so they canreceive the emails then please forwardthere name, address and title to me [email protected]
I would also encourage you to takeadvantage of the greatly reducedAssociate Membership of the SCTS. From2009 the annual fee is £22, with an initialadministration fee of £25. Membershipensures that you receive the Bulletinissues, reduced rate to the Annual meetingand other benefits which are on the SCTSweb site, including the opportunity toapply for a bursary towards professionaldevelopment.
It is now two years since the SCTS benchmarked service provision and it isimportant to follow this work up withcollating information about progress thathas been made. In the December 2008Bulletin I mentioned that we would like toreview role development throughout theCardiothoracic Centres. We have identifiedan online survey tool so will be contactingyou in the near future to seek informationabout how nursing and surgical carepractitioner roles are expanding to meetthe European Working Time Directive andaccounting for the impact of ModernisingMedical and Nursing Careers. If you receivea questionnaire please take the time tocomplete it and return it so we can gatherinformation to inform all about currentservice delivery provision.
Tara BartleyNursing Representative
Maura Buchanan & Tara Bartley at the President’s Dinner
Maura Buchanan
captured the mood of
the Annual Conference
perfectly, linking current
health issues with
putting patients first.

theBulletin10
The nursing profession is currentlyresponding to the review ModernisingNursing Careers (MNC) and one of thechallenges that nursing must overcome isthe preverbal question of to how sustaina ‘clinical’ career pathway.
It would be fair to say that traditionalnursing career progression often results ina move away from clinical practice toassume a greater managerial role. Theadvent of the ‘Modern Matron’ role was toaddress the issue of sustaining qualitycare and standards of excellence. In realitythe Modern Matron often assumesleadership for large clinical areas and thedemands draw away from direct practice.There has however, been a plethora ofClinical Nurse Specialists which havedeveloped in clinical roles, which it couldbe argued have come to fruition inresponse to the wider NHS agenda andexpanding skills. Specifically the impact ofthe European Working Time Directive(EWTD) and Modernising Medical Careers(MMC) has reduced the service deliveryaspects of doctors in training, creating avoid in the delivery of care, which isincreasingly being carried out by nurses.Titles include Nurse Consultant, NursePractitioner, Clinical Nurse Specialist,Advanced Nurse Practitioner, PerioperativeSpecialist Practitioner (The area of SurgicalCare Practitioners is covered in detail bySamer Nashef in his article). To date theprofession has failed to formalise thesetitles and while the specialist practitionerqualification has become recognised onthe NMC register, the debate aboutprocess of registering the Advance NursePractitioner qualification remains
unresolved. It follows then that linkingsuch roles with the Key Skill Framework isnot always simple.
Not withstanding the ongoing issues manyof us would like to progress in our nursingcareers while remaining in the clinical fielddelivering direct clinical care. In responseto the EWTD & MMC the ModernisationAgency Changing Workforce Programmeran a pilot project between April 2003 andApril 2004. The outcome laid thefoundations of the career pathway thatwould enable further training in clinicalexpertise along with an academicframework. In response there has been anumber of pre and postgraduate coursesthat have been developed within theuniversity setting, the premise of which isto underpin a clinical role that has relevantclinical competency package and clinicalsupervision.
The National Survey of CardiothoracicService Provision (Bartley & Livesey 2007)concluded that the service would becomeincreasingly reliant upon nurses who couldundertake care of the patient throughoutthe patient pathway and perform many of
the roles traditionally undertaken bydoctors.
Within the speciality there is a move toembrace these roles providing the trainingand academic pursuit that will produceexpert practitioners to meet the needs of ahigh quality service delivery from acollaborative team approach.
The following is guidance on how to pursuesuch a career:
Initially the individual will need to access aspecialist role, one where they will beperforming the day to day care.
The position should be linked with anacademic course at a recognisedinstitution. Recommendations from thePerioperative Specialist Practitionerprogramme are:
• Access a Health Care Trainingprogramme at a higher educationinstitution with formal lectures andclinical labs training.
• Secure employment in a clinical rolewhich is a recognised training positionin an NHS trust.
• Subsequent completion of theacademic course and clinicalcompetencies will result in a highereducation qualification that underpinsa practitioner with advanced skills andthe critical analysis to perform incollaboration with the multidisciplinaryteam.
Alternatively the individual can access apost basic course to undertake the generic
How to Become a Cardiothoracic Nurse Practitioner
The Expanding Roles of Nurseswithin Cardiothoracic SurgeryWith the advent of increasing pressures on our workforce from regulatory changes, the opportunities for nurses(and allied healthcare professionals) to diversify from their traditional roles within our specilaity has expandedenormously in the last 5 years. These new roles are here to stay as they will undoubtedly underpin our collectiveambition to continuously improve the quality of care that we can deliver our patients. I am therefore grateful toTara Bartley and Samer Nashef for writing these 2 articles, which outline how nurses who may be interested inevolving from their current roles may pursue their goals. These articles will also be posted on our new websitewww.SCTSLTD.co.uk. The Editor
Tara BartleyNursing Representative
In reality the Modern
Matron often assumes
leadership for large
clinical areas and the
demands draw away from
direct practice.

June 2009 11
Surgical care practitioners or SCPs(previously called surgical assistants)play an active role in the delivery ofcardiothoracic surgical care in the UnitedKingdom, and their careers and roles areprobably at a more advanced stage ofdevelopment than similar roles in manyother specialties.
Most SCPs are recruited from the ranks ofnurses and operating departmentpractitioners and have a background ofexperience in cardiothoracic surgery. Thiscan be either in the operating theatre orintensive care setting, but some come fromother related specialties and a few join theservice de novo from totally unrelatedbackgrounds.
The existing training system is usually byappointment to a training post and on-the-job training under the supervision of anamed consultant surgeon. Units withestablished SCP programmes have a moreformal training and mentoring structureoften led by trained SCPs themselves, andPapworth Hospital offers a reasonablyopen-access training programme fortrainees from other units who are usuallyseconded for basic or more advancedtraining at Papworth. Other units havelinked their training to higher educationalestablishments so that training cancontribute to the award of a Universitydegree.
There are plans for national certificationand registration for all such roles in allsurgical specialties, but until that happens,cardiothoracic SCPs are currently assessedby the joint Royal College of Surgeons ofEngland and Society for CardiothoracicSurgery examination. This takes place oncea year in November at Papworth. Theexamination can be taken any time afterthe first year of training, although the
diploma is only awarded to successfulcandidates after evidence of two years ofsatisfactory training. The format is one ofmodified essay questions followed by aviva examination.
The syllabus has slowly moved from theoriginal “Cardiac Surgeon’s AssistantOrange Book” to the existing core andspecialty curriculum as published bythe Department of Health (DoH) and theRoyal College of Surgeons andobtainable from the DoH website:www.dh.gov.uk/en/Consultations/Closedconsultations/DH_4113605
SCPs assist in all aspects of surgical care,from the operating room (conduit harvest,first and second assistance) toinvestigations, ward care, outpatientclinics communications within the surgicalfirm. The extent of involvement in thevarious aspects of care varies according tothe hospital and local needs, and in someinstitutions the role also involves audit,research and training of junior doctors insurgical techniques. In general, the morevaried the job and the more it involvespatient interaction, the greater the sense ofjob satisfaction that is obtained.
With the restrictions on junior doctor hoursand the curtailment of time the juniordoctors spend in service as opposed toprotected training, it is almost certain thatSCPS are here to stay. It is difficult topredict the final form of this youngprofession, but it is likely that in duecourse SCPs will have a properly organisedregister with national certification and aformal higher education connection. Whenthis will happen will depend on nationalinitiatives, but in the meantime thecardiothoracic surgery programme with itsexisting training and diploma will continueto thrive.
Surgical CarePractitioners inCardiothoracicSurgery
Samer Nashef, Consultant
CardiacSurgeon,PapworthHospital
aspects of advanced practice thennegotiate completing the clinicalcompetencies within their role. Thisis demanding and difficult optionwhich will take a great dealdedication and time management,although it should be recognisedthat even those amongst us whohave excellent time managementskills, may struggle in a role whereday to day workload isunpredictable. There is a dichotomywith service delivery and timeconstraints of achieving the clinicalobjectives. Before undertaking therole there must be the infrastructureto support the practitioner.Moreover, without the support of anexperienced mentor, themultidisciplinary team and theorganisation this route is unlikely tosucceed.
Once qualified the individual mustensure that they practice inaccordance with their NMC Code ofConduct and in line with theemploying Trust Policy. They have aresponsibility to maintain theirclinical competencies and to keepup to date with the changesimpacting upon their general andspecialist practice. The role needsto reflect the service demands andrequires timely evaluation to createchange in line with the need forprogress. It may also be that theoriginal course studied didn’tencompass further skills or theadditional non medical prescribingqualification that the role requiresto practice. The practitioner and theorganisation must ensure that thenecessary training, qualifications,supervision and framework are inplace to practice within safeboundaries. Moreover, theorganisation and the practitionerhave a responsibility to ensure thatthe role is supported by themultidisciplinary team and theduties are manageable.
In essence the roles are evolvingand those practising would suggestthat one of the challenges is to beall things to all people. It is then forthe individual to know theirlimitations, communicateeffectively and secure the supportthey need to undertake the roleeffectively.

It is only eight months since I took myseat with the Executive Committee, but alot seems to have happened since then.It cannot be easy for a group ofprofessionals to have a layperson jointhem, but I have been warmly receivedand my perceptions are that my presencedoes not seem to have inhibiteddiscussion or debate. In fact they musttrust my discretion, for there havebeen some distinctly controversialtopics under consideration.
This concept of representation notonly relates to the internalbusiness of the Society but also tohow it relates to the current andprospective patients out in thecommunity, and to whatcardiothoracic patients have tosay about matters relating tothem. Two issues have beenquestioned by us during the lastfew months, one being pooradvice concerning post-operativecardiac rehabilitation emanatingfrom the RCS (England) which wasonly rectified following strongintervention from our President,and the other where theDepartment of Health in anadvisory note excused our postoperative ICU’s from the implementationof same sex accommodation. The patientsabsolutely agreed with this advice, butneither the SCTS nor we can recall beingconsulted.
Most cardiac surgery patientrepresentatives have come to be involvedthrough their ongoing engagement withlocal support groups who tend to fosterlively rehabilitation programmes. That iswhy we take cardiac rehabilitation soseriously. There is no agreed tariff forrehabilitation at present and so there isno comprehensive roll out post-discharge. That is why the BHF decided totake on its first ever political challengeand to sponsor the current CardiacRehabilitation Campaign. This campaignhas been rolling for just over two years,
we haven’t won the day yet, but theprofile of rehab is certainly moreprominent. Please don’t forget to instructyour patients to get involved, in rehabthat is, not necessarily the campaign. Youhave saved or certainly improved theirlives with your surgery, now assist themto extend those same lives with ongoingrehabilitation.
Talking about the British HeartFoundation, again this is a charity fondlyembraced by patients, it is their leafletsthat are prominent in providing broadadvice and guidance about ourconditions, and it is the BHF who oftenprovide the pump-priming funds to
establish rehab programmes. However,BHF is also a major supporter of researchand I have been surprised at the smallnumber of surgical professorshipssponsored by them. Does this also reflecton the take-up of doctoral sponsorshipsamongst our trainee surgeon cohorts?It’s the patients and their families whofund the charity and perhaps this is a
question that would benefitfrom a dose of investigation.
By the time these notes appearthe Blue Book will have beenpublished. You surgeons andyour teams must take greatcheer and comfort from thisdocument. In fact you shouldall throw Unit parties tocelebrate your achievements,take photographs, placereports in your Trust journals,invite the Press. In fact have aball!
It is a significant andcomprehensive record of yourcommitment to patients, manyrun of the mill procedures toyou, but to your patients fromtheir perspective it’s life ordeath. The record also
demonstrates that you are getting braver;you are regularly accepting more difficultcases, older people, more women,patients with other debilitatingconditions and still your successes rise.My understanding is that this Blue Bookalso challenges the other surgicalspecialities to look to their laurels and tostart to push back their own boundariesstill further. It is a call to action to thewhole profession. Ben Bridgewater hasled up the writing team on your behalf, heand they have done a great job, butremember, what they are doing isdisplaying your wares. Really well doneeveryone.
As in life, so in medicine, women are aconundrum. In regard to cardiovasculardisease women are under-presented,
theBulletin12
Notes from the Patient Representative
The Mayor of Rochdale, Councillor Jean Hornby, andher Consort, with David Geldard, President of TransPennine Cycling Club, starting on one of his club's
eleven annual Over The Edge sponsored cycle rides inaid of the British Heart Foundation that so far have
raised £130,000 in aid of the charity
This concept of representation
not only relates to the internal
business of the Society but
also to how it relates to the
current and prospective
patients out in the community.

13June 2009
David Geldard MBE,SCTS Patient
Representative
under-diagnosed, under-treated, and under-represented; theseare the findings of the National Joint Working Group forWomen’s Heart Health. It’s not just in the Home Waters; it’s aninternational problem. The World Health Organisation statisticsshow that not only is cardiovascular disease (CVD) the leadingcause of mortality, but more women than men die from thiscause The Blue Book mirrors some of these issues, whichmeans that here is supportable evidence and we need tocapitalise on this opportunity to make our contribution toWomen’s Heart Health (WHH). Would anyone be interested ingiving WHH a good dose of looking at?
At the Annual Meeting in Bournemouth, which to me was athrilling experience, we welcomed our first group of patientsfrom the local cardiac network. Next year we are consideringinvolving patients from the cardiac and the cancer networks ofMerseyside and North Wales, Greater Manchester and Cheshire,Lancashire and Cumbria, West Yorkshire and possibly Ireland.That would be a huge population base to have represented at
our conference. We are thinking of asking the patients toidentify their interests and their concerns so that we can tailortheir experience at conference to match their queries. Patientswill go back to their regions and report what is going on in ourworld. It’s a great opportunity.
It’s only in this previous paragraph that we have touched onthoracic surgery. We are mindful of the need to providebalanced representation in every way possible, and, again, ifanyone has any specific suggestions please do have a word. It’sa two way, open ended process, and please remember we haveonly been going eight months.
So, my sincere thanks to our hardworking President and hisExecutive Committee, and Isabelle and Tilly, for making me sowarmly welcome. Comments and feedback are welcome. Enjoyyour parties, you deserve them!
half page ad to come

theBulletin14
This examination currently has two dietsper annum with two sections. The firstsection is a multiple-choice examination,which is held in January and July andconsists of two, 2-hour papers. Paperone is of the single best answer type with110 questions and paper two has 135extended matching items. Following thesection one examination, a standardmeeting is held and the pass markdetermined. Those who pass section oneare then eligible to sit section two, theclinical part of the exam. This takesplace in May and October.
Section two of the exam is divided into sixportions. There is a long cardiac case, along thoracic case, short cardiac caseswhich include an investigation stationwhere candidates may be shownangiograms, echo’s, or CT scans. There is ashort thoracic case section, which againwill include an investigation station, whichmay include identification of instruments,CT scans etc. There are two orals, one incardiac surgery and one in thoracicsurgery. Section two of the examinationemploys a close marking system withmarks ranging from 4 to 8. Six is the passmark and there are six marking areas withsix portions and two examiners markingindependently. Accordingly, the candidateneeds to achieve 432 marks in section twoto be successful.
There have been no recent changes in theregulations to sit the exam and these areavailable on the Intercollegiate website,www.intercollegiate.org.uk. On openingthis website, one follows the link to thespecialties and all regulations areavailable online. An application form,structured reference form and guidancenotes are also available at this site, withthe calendar including the examinationdates and the closing dates forapplication.
I would draw candidates’ attention for theinstructions to the structured referees. For
applicants in approved training posts, allthree referees must be on the UK/Irishspecialist register. One referee must bethe current program director and the othertwo must be consultant trainers/supervising consultants or seniorcolleagues in the specialty with directexperience of the applicant’s currentpractice. For those not in training, all threereferees must again be on the UK/Irishspecialist register and one referee must bethe applicant’s current lead clinician, headof department/medical director, and theother two must be senior colleagues withdirect experience of the applicant withinthe last three years.
The level of theexamination is set at thatwhich one would expect ofa first day consultantcardiothoracic surgeon.The examination is a testof the knowledge base ofsuch an individual andcovers the generality of the specialty. It isimportant to point out that passing theexam does not guarantee attaining a CCT.The examination is only one aspect in theassessment of cardiothoracic surgicaltraining.
I think it is important to dispel some of themyths and misconceptions that may havearisen in the recent past. I have expressedthis view on many occasions and it isimportant that candidates realise thatthere is no understanding that only acertain percentage of those who sit theexamination will pass. Further, there is nosubstance to the rumour that candidateswho are not NTN’s or those resitting theexamination are treated differently. Theexaminers are unaware of a candidate’sbackground. Finally, I repeat, passing theexamination does not guarantee acertificate of completion of training.
Candidates are always keen to know theresults of the examination and these areusually posted within 48 hours ofcompletion of section two. The examinersare also informed of the candidate’s
performance. During section two of theexam the examiners are observed by oneof the assessors of the panel of assessorsfor cardiothoracic surgery and theexaminers receive feedback on theirperformance at that diet of the exam.
In the table below, I attach the results ofthe examination since May 2007. Asrequested, I have split the candidates intothree groups. NTN refer to those withnational training numbers and FTTA referto those who do not possess trainingnumbers but are in training programs. OTrefers to those candidates who are out oftraining.
You will see that the overall pass ratevaries from 57 to 75% over the fiveexaminations since May 2007. As a group,those with national training numbers dobetter than the other two groups. It isinteresting to note that the pass rate ofthose out of training has steadilyimproved.
The examination continues to develop andsection one of the exam is under tensescrutiny by the educationalists andpsychometricians who provide reportsfollowing each diet of this section of theexam. Changes will take place to theconduct of section two, particularly theclinical portion, and program directors willbe advised of these changes before theirimplementation. Similarly, any changeswill be published promptly in the guidancenotes issued to candidates prior to sittingthe examination.
I hope this brief resume of the currentstatus of the examination has been ofsome benefit, and should candidates haveany questions I am happy to be contactedthrough the Intercollegiate Board.
The IntercollegiateExamination in Cardiothoracic Surgery
Robert Jeffrey,Chairman ISB for
Cardiothoracic Surgery
NTN (%) FTTA (%) OT (%) Overall (%)
May 07 82 50 14 61
Oct 07 88 67 33 65
May 08 100 40 33 65
Oct 08 77 36 50 57
May 09 90 57 71 75

15June 2009
Stepping Down: The Cardiothoracic Tutor
Jonathan Hyde
I’m sorry to say that this will be my finalreport as Cardiothoracic Tutor, as I amabout to stand down after over 5 years inthe post. I have very much enjoyed therole and have stayed on much longer thanI originally planned. There have been anumber of challenges during my tenure,including the ‘trainee crisis’ and theadoption of the new curriculum and MMC,but these storms have been weatheredand, hopefully, things seem to be movingin a positive direction again.
First of all, a little bit of background: Thepost of Cardiothoracic Tutor was originallyset up with a commitment of approximatelyone day a week (or two sessions), but thetime could be used flexibly. For thiscommitment, the Trust for whom theincumbent worked would be remuneratedon a basis of 2PAs, to allow them to coverthe absent consultant, if necessary. TheRoyal College of Surgeons of England wereresponsible for this payment, but the fundswere originally generated by sponsorship.The network of sponsors covered thepayments for Tutors of all surgicalspecialties, and different sponsorshipdeals were made for each Tutor.Sponsorship in our specialty was originallyfrom The Freemason’s Grand Charity butafter their term expired, the funding wastaken on in its entirety by the Society. Thetime commitment varies, but one day a
week at The College, as well as attendingall the courses within the portfoliogenerally exceeds the two sessionsallocated, and the Trust needs to be awareof the amount of special leave that will berequired. This is something that needs to
be negotiated between the post-holder andtheir management. Recently, however,there have been a number of changes withrespect to the post, and I shall try tosummarise them now. MMC and the newcurriculum necessitated deconstructionand reconstitution of the entire portfolio ofcourses, which was a huge task over a twoyear period. In addition, following a periodof drought a couple of years ago, where thenumber of trainees massively exceeded thenumbers of potential consultant jobsavailable, entry to the specialty wastemporarily closed and morale amongsttrainees was at an all-time low. As aconsequence, there was a significant fall-off in applications for courses nationally,and several of our courses were eitherdiscontinued or rationalised. The situationwas not helped by the almost universalreduction in the amount of remunerationallowed for Study Leave. However, sincethe specialty has ‘re-opened’ and moralehas risen, the interest in education seemsto be improving and many moreapplications are being received.
The situation at present is moreencouraging and the portfolio is now at anappropriate level. The climate has notallowed the creation of any new courses forthe past couple of years, when the priorityhas been to sustain the existing ones andnot allow them to fail. There is now scope
to resurrect certaincourses that are currently‘on hold’, and evendevelop new ones toreflect evolvingtechnologies. Cost isalways an issue, but thereis a plan to regionalisecertain courses, therebyeliminating the overheadshaving to be paid forbasing them all at TheCollege. Another veryimportant developmentwhich was finalised at The
Education Sub-committee meeting inBournemouth, is that the post will nowbecome Intercollegiate, representing theeducational interests of all four SurgicalRoyal Colleges equally. The job descriptionhas also changed slightly in that it is now a
n o n - E x e c u t i v eposition and isfunded toa level ofapproximately halfa day a week (or 1PA), and reports directlyto the Education Secretary, currently JohnPepper, as well as the Director of Educationat the College. The reduced level of timereflects the fact that the portfolio iscurrently complete, but should things getbusier and more time be needed in thefuture, these things can, I am sure, benegotiated.
The courses currently on offer can be foundon the Royal College of Surgeons ofEngland website www.rcseng.ac.uk/education/courses/specialty/cardiosurgery.html, and suit a range of training levels.The ‘masterclasses’ previously run forsenior trainees and junior consultants havelargely been disbanded as many similaropportunities are now being run byIndustry, and are also fully funded. A list ofcourses currently available is shown in thetable opposite.
One of my aims has been to abolishlectures in their classical form and to makeall the courses either practical orinteractive in their format. This has beensuccessful, and any ‘lectures’ are now usedonly as a link between hands-on sessionsor seminar based workgroups, and are onlypermitted to be 20 minutes long at most.
I firmly believe that the role of Tutor is avery important one, and that it is essentialto maintain and continuously adapteducational courses. The Intercollegiatestatus will, I hope, help to forgeeducational links between all four Colleges,and will help to maximise efficiency byeliminating competition between similarcourses. I hope that my successor will beas enthusiastic and committed toeducation as I have been, and I am surethat in injection of new blood into the postis a positive move forwards. I should like tothank the Society for all their support, bothfinancially and spiritually, in what has beena very rewarding time for me, and hopefullyfor the trainees.
Courses AvailableTitle Target level
Specialty Skills in Cardiothoracic Surgery ST 1-2
Intermediate Cardiac Surgery ST 3-6
Intermediate Thoracic Surgery ST 3-6
Applied Basic Science for Cardiothoracic Intercollegiatesurgical trainees examination
candidates
Advanced Thoracic Surgery ST 7-8
Bypass, Balloons and Circulatory Support ST 1-8
Surgical approaches to Atrial Fibrillation ST 4-8

theBulletin16
Introduction
The Society’s annual meeting fulfils manyroles: invited educational lectures, traineeand business meetings, and ofcourse, spirited socialgatherings. However, most ofthe programme is dedicated tothe presentation of originalresearch and audit. These oralpresentations and postershave an important role insupporting academicproductivity, scientificdiscovery and the careerdevelopment of younginvestigators and trainees inGreat Britain and Ireland.
Whilst presentation to learnedsocieties is valuable, the target of originalresearch should be publication in a peer-reviewed journal. The strength of ameeting may therefore be assessed by therate of subsequent publication. Weconducted an analysis of abstractspresented at three consecutive SCTSannual meetings to assess the rate ofpublication, associated factors andreasons for non-publication.
Methods
Abstract books and meeting reports fromthe Society’s 2003 (Edinburgh), 2004(Guernsey) and 2005 (London) meetingswere reviewed. This period was selected toallow sufficient time for presented work tobe published; studies have shown thatfollowing academic meetings, more than95% of resulting papers are published
within the next four years. Medline wassearched to identify peer-reviewedpublication arising from each work. Factorspotentially associated with publication
were assessed: type (oral v interactive),origin (GB&I or foreign), category (cardiac,thoracic, transplant, congenital,technical/miscellaneous), study design,projection (prospective v retrospective),subjects (human v animal) and whetherthe abstract won a prize at the meeting. Ifno publications directly relating to thepresented abstract were identified,authors were contacted by emailquestionnaire toascertain its status andreasons for non-publication.
Results
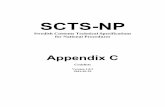
826 abstracts weresubmitted to the threemeetings, of which 156(18.9%) were acceptedfor oral presentation.Of these, 99 (63.4%)had been published orwere in press: 31 of 48(64.6%) from 2003, 34of 54 (63.0%) from2004, and 34 of 54(63.0%) from 2005. Succeeding papershave appeared in 36 peer-reviewedjournals: 58 (58.6%) in cardiothoracicsurgery journals, 19 (19.2%) incardiopulmonary medicine journals, 5(5.1%) in general medical journals, 5(5.1%) in basic science journals and 12(12.1%) in other journals (Figure 1). The
median time to publication was 16 months(range -7 to 66 months) with 8 papersmischievously published prior to theirmeeting (Figure 2). The only factor
associated with publication wasstudy design: randomisedcontrolled trials (84.1%) versusobservational studies (51.3%).
Of 57 unpublished abstracts, 28(49.1%) authors replied to anemail questionnaire. 3 (10.7%)papers were under consideration,5 (17.9%) had been submitted andrejected, and 20 (71.4%) werenever submitted. The mostcommon reason given was lowpriority (42.0%), followed by studyongoing, similar results reportedby others and low likelihood of
acceptance (each 12.9%).
Discussion
So 63% of presented abstracts went on tobe published but is this a good return? Thiscan be assessed in two ways: comparisonwith SCTS meetings from previous yearsand with meetings of similar societies inother specialties.
Looking back at the ten years leading up tothe 2005 meeting (Figure 3), there hasbeen a steady rise in the publication ratefrom under 30% in 1996 to consistentlyover 60% in recent years. Potentialexplanations include better selection ofabstracts for presentation, an increased
The Fate of Abstracts presented at SCTS Annual Meetings 2003-2005
Figure 1. Abstracts were published in a widerange of biomedical journals
Figure 2. Cumulative publication of abstracts from each meeting
Figure 3. Publication rate of abstracts presented at SCTSmeetings 1996-2005

June 2009 17
Cardiothoracic SurgeryResearch ClubSaturday, 19th September, 2009The Hilton Hotel, SheffieldThe Cardiothoracic Surgery Research Club was founded over twentyyears ago. Very quickly it became an important event in theeducational calendar, particularly, but by no means exclusively, forjunior cardiothoracic surgeons in training. Consultants have alwaysbeen involved, not just in terms of selecting the abstracts, chairing thesessions, and sometimes even presenting themselves, but also insupporting their research fellows/registrars. There are fewconsultants in post today, who have not, at some stage in their career,presented both original scientific and clinical work in this forum.
History shows that most winners of the awards have gone on topresent their work in the international arena. The strength of the Clublies in its convivial and relatively informal setting. Importantly, it is notjust a forum in which to make highly polished presentations ofcompleted research. Pilot studies, and research in progress is equallywelcome, and presenters can make full use of the meeting in which toask for, and receive constructive advice from experienced colleagues.The meeting is not exclusive to those with research to present. Allgrades of juniors will derive educational benefit, in terms of learningabout statistical and scientific methodology. In addition, it is anenjoyable social and networking event.
It was agreed at the inauguration of the club that presentation in thisforum does not preclude submission (and presentation) of the samework at our Society Annual Meeting. This year’s date has been chosenin the knowledge that autumn is a busy time of year for submission ofabstracts to the Society and some North American meetings, andtherefore I have little doubt there will be some competition to presentat this meeting. As evidenced by the ever-increasing number ofabstracts submitted to our Society meeting, it is clear that research inour specialty is very much alive and well in the UK.
I am grateful to our colleagues in Industry for their support of themeeting, which will enable three awards of £500, £300, and £200 forthe top three abstracts/presentations. Abstracts will be reviewedusing the same criteria as those used in the Society for the AnnualMeeting. Consultants from several units will be involved in theselection process, chairing the sessions, and scoring thepresentations. It is expected that these educational grants will be awelcome contribution to travel expenses incurred in presenting orattending another meeting.
This year’s venue is the Hilton Hotel in Sheffield. Sheffield is readilyaccessible by road and train from all parts of the UK, and the hotel isjust 5 minutes walk from the station. There is abundant parkingavailable adjacent to the hotel.
Those wishing to submit an abstract for consideration should contactme by e-mail for further details and the deadline date. There will be amodest delegate fee which includes all refreshments throughout theday, and the three-course Awards Dinner, at which the winners willreceive their cheques. The dinner will be held in the hotel. Those wishingto enjoy the evening to the full can book rooms at the Hilton, thoughthere are several (cheaper) hotels within easy walking distance.
David Hopkinson [email protected]
number of target journals and more high-qualitycardiothoracic research being produced in Great Britain &Ireland; it is likely that all three have contributed to thisimprovement.
The publication rates of other national surgical societymeetings are shown in the table but are difficult to interpret.Some meetings have an affiliated journal, follow-up periodswere variable and most studies relate to an era when theSCTS rate was considerably lower than at present; thenagain, our results are the highest reported for such meetings.This may be a time-related phenomenon – it is unknownwhether the publication rates for these meetings have alsoincreased in recent years. In addition, direct comparison withother cardiothoracic surgery meetings is not valid as manyhave an affiliated journal in which most accepted abstractsare subsequently published.
It was disappointing to discover from respondents that over70% of papers that remain unpublished have never beensubmitted. These abstracts had withstood peer-review for themeeting but have not been given the opportunity to reach awider audience. The successful abstracts appeared in 36different clinical or scientific journals, suggesting a broadrange of potential targets for submission; none of these weretested by most of those remaining unpublished. Perhaps thisraises ethical considerations, particularly if the studies hadutilised prospective patient or animal participation?
In conclusion, in recent years, the SCTS annual meeting hasbecome a forum for the presentation of high-quality researchand compares favourably with the national meetings of othersurgical societies. Subsequent papers usually withstandpeer-review, most commonly in a specialty journal, althoughthose that remain unpublished are generally neversubmitted.
Table: Publication rates of abstracts from other nationalsurgical meetings in Great Britain & Ireland.
Specialty Meeting(s) % published
Plastic surgery (BAPS) 1995-9 31.9Orthopaedic surgery (BOA) 1997-8 35.3Colorectal surgery (ACPGBI) 2001 24.3General surgery (ASGBI) 2001 34.6Transplantation (BTS) 2001 35.6Emergency Medicine (BAEM/FAEM) 2001-2 30.7Urology (BAUS) 2001-2 42Vascular surgery (VSGBI) 2001-2 59.4
Acknowledgements: We thank Antonio Martin-Ucar, Leicesterfor providing historical data on abstracts presented at the1996-2002 meetings (Figure 3). We also thank Isabelle Ferner,Domenico Pagano and all abstract authors who responded toour email questionnaire.
Nigel Drury, VanessaRogers and Lynne
Williams, UniversityHospital Birmingham

The Role of the Societyin Clinical Excellence Awards
theBulletin18
The Advisory Committee on ClinicalExcellence Awards (ACCEA) website statesthat Clinical Excellence Awards are givento recognise and reward the exceptionalcontribution of NHS Consultants, over andabove that normally expected in the job,to the value and goals of the NHS andpatient care. ACCEA operates thearrangements which replaceddiscretionary points and distinctionawards with a single more graduatedscheme comprising both local andnational elements.
National AwardsThe Society for Cardiothoracic Surgery is arecognised nominating body for nationalawards, and as such can nominate directlythrough ACCEA and SACDA (the equivalentin Scotland) as well as via the RoyalColleges. The Society’s Committee forClinical Excellence Awards is made up of:Graham CooperLeslie HamiltonRichard PageJohn PepperPatrick Magee (Chairman)Lady Irvine (the wife of Sir DonaldIrvine and herself much experienced inNHS matters, as a Lay Member)
We plan to recruit an extra member fromthose Consultants who does not hold anational award, and we now are invitinganyone interested in taking on this role tocontact either Graham Cooper or myself.
The Society invites those who are eligibleand are applying for a national award, andwould like SCTS support, to submit anapplication. All the applications are scoredby the Committee using the followingsystem, up to a maximum of 21 points:
Contribution to SCTS 0 – 5
SAC Training/Education 0 – 5
Intercollegiate Examination 0 – 1
Science/Innovation 0 – 3
Service 0 – 2
Impact 0 – 5
A cross-check of the scoring is done usingthe ACCEA scoring system, whereby eachof the five domains in the application formis scored separately with a score of 10, 6, 2or 0.
Following the scoring process, SCTSnominates directly to ACCEA. The numberof nominations allowed is determined bythe number of Consultant members of theSociety, and currently with the ACCEA wecan nominate up to 6 for Bronze awards, 3for Silver awards, and 2 for Gold awards.The ACCEA does not invite nominations forPlatinum awards from specialist societies.The situation with SACDA, althoughslightly different, is essentially similar. Wehave no official role in the process inNorthern Ireland, but for the highest levelof award we can submit citations insupport. In addition to submitting ranklists for each level of award, we alsoprovide citations for those beingsupported. It is most important to stressthat the individual submits his or her ownapplication to ACCEA, and SACDA. We, as aSociety, only submit rankings andcitations.
In addition to direct nomination to ACCEA,SCTS also gathers support for members viathe Royal College of Surgeons, especiallythat of England and Edinburgh. TheGlasgow College does not seeknominations from the specialist societies,although we of course provide support forFellows of the Glasgow College. In the caseof the Royal College of Surgeons ofEngland, any surgeon working in Englandor Wales is eligible to apply to them forsupport, whilst in the case of RCSEd, anyEdinburgh Fellow, regardless of where heor she is working, can apply to them forsupport. We, as a Society, provide rankedlists to them for Bronze, Silver and Goldawards, and in addition are usually askedto provide citations for those the Collegedecides to support. The Colleges may alsoof course decide to support Fellows who,for whatever reason, are not on our list,and we of course provide citations forthose applicants also. Citation writing
involves quite a lot of hard work for thecommittee, as the timeframe is often short,and several different citations may benecessary for the same applicant.Identical citations signed by severaldifferent people on behalf of severaldifferent organisations does not scoremany points with ACCEA! As a Society wedo not score Platinum applications, unlessasked to by the Colleges. We submit thenames, and if the College decides tosupport them, they may ask us for acitation. The Colleges then nominatethose they support for Platinum to theAcademy of Royal Colleges, who thendecide which to support and put forward tothe ACCEA Main Committee.
Timetable for 2010 Round
The proposed timetable for theforthcoming round is as follows, althoughexperience would suggest slippage iscommon. I believe, however, that this isgoing to require considerable effort toavoid that this year:
2010 Guide available on ACCEA websiteby end of July 2009
Letter to be sent to successful candidatesin the 2009 roundby end of July 2009
Full results for 2009 posted on ACCEAwebsiteby beginning of August 2009
Submission to SCTS4th September 2009 (to be finalised)
Online system for 2010 round available on ACCEA websiteby end of September 2009
Closing date for receipt of all applications,ranked lists and citationsFriday 11th December 2009
The deadline for those seeking RCSEng support for Platinum applicants14th September 2009
Bronze, Silver and Gold28th September 2009

June 2009 19
Patrick Magee, Chairman, SCTS Clinical Excellence Awards Committee
We, as a Society have to score and then provide the College withrankings by these dates, and therefore the deadline forapplications to the Society will probably be 4th September 2009,although Isabelle and Graham will be advising all members ofthis shortly.
As the online system for 2010 will not be available by that date,we can provide copies in Word of the application forms whichmembers can use for admission to SCTS and Royal Colleges. Inaddition to the main application, there are three optionalsupplementary forms, for management, education and training,and research. These are optional and applicants for Bronze andSilver awards may submit one only; applicants for Gold maysubmit two, and those applying for Platinum can submit up tothree!!
Regional Sub-Committees
All national applicants are discussed and scored by regional sub-committee. All ACCEA regional sub-committees are co-terminousof the whole or part of a Governmental Office of the Regions.There are 13 of these in England and 1 in Wales, and each of theseis made up of professional (medical), employer and laymembers, with a Lay Chairman and a Medical Vice-chairman. We,as a specialty, are represented on some of these committees,including Simon Kendall on the North East Sub-Committee, BSethia on the London North West, and me on the London NorthEast Sub-Committee. Bob Jeffrey is currently on the CentralSACDA Committee. Each of the sub-committees meets at the endof the process with the Chairman (Professor JonathanMontgomery) and the Medical Director (Professor HamidGhodse) of ACCEA, and agree the rankings for Bronze, Silver andGold, which is then confirmed at the main committee. Platinumis discussed briefly, but the main ranking is done by the CentralCommittee.
Filling Out the Form
Members of the Regional Committee have to score a very largenumber of applicants, often within a very short timeframe. A welllaid-out form is more likely to ensure that important points arerecognised, and it is important to follow certain guidelines:
1. Keep within the prescribed size limits and the number ofcharacters used
2. Avoid completely filling in the given space, leave somespaces and consider the use of bullet-points
3. Highlight achievements since the last award. No credit willbe given for something that has previously been rewarded
4. Use dates frequently to show that entries are current5. Avoid repeated use of the same achievement in each domain
Local Awards
There is no formal role forspecialist societies in the localawards system. However,SCTS will provide citationssupporting any member who isapplying for a local CEA award.Any member seeking SCTSsupport should send the Honorary Secretary a brief summaryhighlighting the reasons why they feel they warrant a newClinical Excellence Award. These points will be used to helpprepare the citation, which will then be signed by the Presidentof SCTS in support of the application.
Finally, remember that applications for national and local awardsmust be submitted by the applicant. SCTS offers support,nominations and citations, but does not, and cannot, makeapplications. Further detailed information on the whole processis available at: www.dh.gov.uk/ab/ACCEA/index.htm

theBulletin20
At the Annual Meeting inBournemouth the Society helda symposium to debate someof the most important issuesraised by the recent NCEPODstudy. NCEPOD published itsfinal report - CABG – The Heartof the Matter - in the summerof 2008 so delegates hadplenty of opportunity to absorbits recommendations and thisresulted in excellent debate.The report made ten principlerecommendations and fourwere chosen for debate –Multi-disciplinary CasePlanning, Consent, Morbidityand Mortality meetings and theManagement of Urgent Cases. Thesymposium was chaired jointly by me, onbehalf of the Society and Marisa Mason –the Chief Executive of NCEPOD.
After a general introduction and reminderabout the major findings of the study,Russell Smith, Consultant Cardiologist atGood Hope Hospital, Sutton Coldfielddescribed the structure of theirmultidisciplinary meetings – held withsurgeon visiting from the Queen ElizabethHospital, Birmingham. He described howcases were selected for discussion andsome of the advantages he felt came out ofthe meetings: in addition to fostering goodrelations with surgical centres, the meetingprovides transparency in how cases areselected for CABG or PCI aswell as excellent trainingfor junior doctors and otherhealth professionals. Hispresentation was very wellreceived. The debatefocussed on such issues ashow cases are selected fordiscussion, particularly incentres where PCI is readilyavailable. The impact ofthe changing environmentwith the advent of primary PCI and theincreasing proportion of CABG being forurgent cases was recognised but it wasstill felt that the MDT had an important roleto play in the management of borderlineand complex cases. From a show of hands
it seems that MDT meetings were held inabout two-thirds of surgical centres.
The symposium then moved on to discussthe issue of how consent was obtained forsurgery. The topic was introduced byDavid Richens, Consultant CardiacSurgeon in Nottingham, who described thefindings of the study and outlined theapproach recommended by the HealthService Ombudsman, Ann Abraham, in herpublication “Consent in Cardiac Surgery. Agood practice guide to agreeing andrecording consent”. Cardiac surgeons hadbeen criticised in the NCEPOD report forboth the number of consent forms signedby SHO’s and for the fact that when thiswas the case it was unusual for SHO’s toquote hard figures for mortality andsignificant morbidity (such as stroke) on
the consent form. However, whenconsultants signed the consent form withpatients, quoting hard figures for suchevents was the norm. The general tenor ofthe debate was that this area of practicecould and should be improved upon, but
many speakers pointed out that thesigning of the form was the end-point of a long process ofexplanation and that there weremany examples of good practice tobe found. There then followed adiscussion about NCEPOD’srecommendation that local data isused when advising patients of therisks they face - most speakers feltthat this was appropriate but theopinion was voiced that this wasnot necessarily realistic orappropriate for more complex andrarely performed procedures.
The third topic discussed was theuse of Morbidity and Mortality meetings inthe quality assurance process. The debatewas led by Domenico Pagano, ConsultantSurgeon and Reader in Cardiac Surgery atthe University of Birmingham. Hedescribed the process used at the QueenElizabeth Hospital. They grade the carereceived by patients who died followingcardiac surgery according to the NCEPODclassification.
NCEPOD Grades of Quality of Care
• Good practice – a standard that youwould accept for yourself, yourtrainees and your institution
• Room for improvement – aspects ofclinical care could have been better
• Room for improvement – aspects oforganisational care could have beenbetter
• Room for improvement – aspects ofboth clinical and organisational carecould have been better
• Less than satisfactory – severalaspects of clinical and/or organisationalcare that were well below satisfactory
He showed how using this system canfocus the teams caring for patients onareas where changes need to be made.There was praise for the open andtransparent way the Birmingham team rantheir M&M meetings but concerns wereraised about the difficulties some feltabout discussing cases in a full and frank
Symposium Debates NCEPOD Report

June 2009 21
New AdministratorThe Society Welcomes Tilly Mitchell
way in front of a mixed audience containing all grades ofhealthcare staff comprising the wider multi-disciplinaryteam. Whilst it was recognised that transparency wasimportant the feeling was widespread that thediscussion would be more rigorous if the audience waslimited to medical senior nursing staff only. At this pointSir Terence English spoke from the floor. Although hehas been a regular attender at Society meetings heexplained that since his retirement he preferred to listenrather than contribute from the floor. He described theway in which Dr John Kirklin ran M&M meetings at theUniversity of Alabama forty years ago. He describedhow, as head of department, Dr Kirklin always chairedthe meetings and that cases were analysed in detail in anon-confrontational way so that the team could learnfrom adverse events and improve care for patients in thefuture.
The final area discussed was the care given to patientsrequiring urgent coronary surgery. The mortalityamongst this group of patients was higher than forpatients having elective surgery. They also form anincreasing proportion of most units’ workload. Manypatients have faced long in-hospital waits for surgery asresources have been targeted on waiting times forelective surgery as these are centrally monitored. Thisresults in wasted resources and may be responsible forsome of the increased morbidity experienced by thesepatients. There was general agreement that thesepatients should be operated on within a week of referraland that unit managers should adopt this as a target tobe supported locally.
The NCEPOD study focussed in detail on coronarysurgery in the UK for a period of three years.Interestingly the mortality rate fell through this periodand the results from coronary artery surgery in the UKare the envy of the world. Our willingness to participatein such studies will help maintain these high standardsfor our patients.
I would like to take thisopportunity to introduce myself. Ijoined STCS in March 2009,replacing Rachel Woolf as PA tothe Meeting Secretary andTreasurer.
Originally studying Fashion atLondon College of fashion. I thenturned my interest to Finance andcompleted a BA honours inAccounting and Finance atGreenwich University in 2006. For the last few years I have beenworking in accounts and PA roles until appointment to the roleat the Society.
My role is very dynamic and covers many areas. One aspect is tomaintain the Society’s finances. This involves up keeping ofledgers, accounts payable, credit control, preparing VAT returnsand general accounts duties. I have always had a passion forfigures so I have quickly got to grips with procedures andinitiated my own accounting system. I have also been involved inidentifying ways of reducing costs of the Annual Meetings.
The other part of my role is to provide secretarial support to theMeeting Secretary. I am involved with the planning of the nextAnnual Meeting. This includes site visits, designing the schemefloor plan, securing exhibitors and sponsors, maintaining theannual budget and preparing for registration. I had the pleasureof attending the March Annual Meeting in Bournemouth. Thiswas my first scientific meeting so it was great to see what isexpected of me for in the next meeting in Liverpool 2010.
We have also launched a new website www.sctsltd.co.uk formore of our commercial needs. The website will be used for arecruitment job centre and advertisements. I have been helpingto sell advertising space on this website as well as space in theSociety’s Bulletin. Having never worked in sales or marketing Ifind this a challenge, which I am keen to tackle.
I have so much to learn but also so much to give. I am thankfulfor being giving this opportunity to work for such an establishedand reputable organization and I hope my career can developwith the Society. I also look forward to working with the newTreasurer Malcolm Dalrymple-Hay, who will be taken over from BSethia this Autumn.
Tilly Mitchell, SCTS [email protected]
Steven Livesey, SCTSNCEPOD Lead
The report made ten principle
recommendations and four were
chosen for debate – Multi-disciplinary
Case Planning, Consent, Morbidity and
Mortality meetings and the
Management of Urgent Cases

TITRe TrialSummary
theBulletin22
A multi-centre randomised controlled trial of TransfusionIndication Threshold Reduction on transfusion rates,morbidity and healthcare resource use following cardiacsurgery – the TITRe 2 Trial.
Cardiac surgery centres transfuse over 10% of all units of redblood cell (RBC) used in the UK. Although RBC transfusion isessential in some patients for the management of life-threatening haemorrhage, in most cases decisions totransfuse are made because the haemoglobin (Hb)concentration has fallen to a level or threshold at which thephysician is uncomfortable. The transfusion threshold variesbetween units and physicians, contributing to wide variationin the percentage of cardiac surgery patients who aretransfused with RBC (25% to 95%). The threshold variationstems from a lack of evidence as to what constitutes a safelevel of anaemia following cardiac surgery.
Unnecessary blood transfusions increase healthcare costsboth directly, because blood is an increasingly scarce andexpensive resource, and indirectly, due to complicationsassociated with transfusion. Transfusion may causecomplications by reducing patients' ability to fight offinfection and respond to the stress that surgery puts on thebody, as well as the better known, but rare complication ofinfection transmission.
Randomised trials have suggested that, in other patientgroups, only transfusing when the Hb level drops below7.0g/dL reduces transfusion rates as well as complications.However, to date there has been no large high qualityrandomised trial of different transfusion thresholds in apopulation of cardiac surgery patients. We propose to testthe hypothesis that lowering the RBC transfusion thresholdfrom a haemoglobin (Hb) level of 9.0g/dL (“liberal” controlgroup, similar to current practice at most centres) to 7.5g/dL(“restrictive”) reduces postoperative complications and NHScosts in cardiac surgery patients. The study is a UK multi-centre, randomised controlled trial that aims to assign 2000patients to a restrictive or liberal post-operative transfusionthreshold. The primary outcome will be a composite ofinfectious and ischaemic events in the first three monthsafter randomisation.
For further information, contact Gavin Murphy at:[email protected]
GavinMurphy
Applications are invited for 2 newly created posts. This is aresult of the expansion in both the publishing and web-basedaspects of the Society’s activities.
1. Publishing Secretary
The individual will be responsible for commissioning,designing and editing the Society’s Bulletin. The Bulletin hasundergone significant changes over the last 5 years. It requiresan individual who is committed to progressing this evolution sothat the Bulletin continues to meet the demands of themembership. Marketing through the Society’s office, to ensurethat advertising revenues continue to support the publishingcosts, will also be part of this role. In addition, the individualwill be responsible for final proof reading of all the Society’spublished literature and the generation of Society flyers for theAnnual Meeting, including the on-site Bulletin and the AnnualMeeting Programme. Individuals with a vision as how theseelements may be improved and changed in the future arewelcome.
2. Web Secretary
This post is for those who are IT literate. This is an exciting timeat the SCTS with 2 websites, which are undergoingdevelopment/ restructuring. The SCTSLTD.CO.UK website aimsto serve the professional needs of the members and but alsofor generating income for the Society through advertising andthe job centre. It will also host discussion fora for variousmember interests. The SCTS.ORG website will remain as the‘home’ site with it’s emphasis on education, news andresearch. Both sites require a dedicated individual to ensurethat they remain up to date, relevant and focused on membersinterests and needs. Again, an individual with vision for thefuture direction of these sites would be a welcome member ofthe team. The Web Secretary will also have support from theSociety office and a commercially based IT engineer.
It is anticipated that both individuals when appointed will workclosely with the existing Communications Secretary of theSociety who will have overall responsibility for the delivery ofhigh quality paper and web-based publications. The futurestrategic direction and goals will be agreed and set within theteam and subsequently ratified by the Executive Committee.The tenure is initially for 3 years and renewable thereafter; theposts are open to Consultant members of the Society.
Please send an abbreviated CV with your qualifications forthese posts and your development goals. Applications shouldbe sent by mail to the Isabelle Ferner at the Society office or byemail: [email protected]. Closing date is 30th August 2009.
Two new SCTS Posts

June 2009 23
I have been the Trainee Representative foralmost 18 months. During this time I haveseen positive changes pertaining to trainingand general outlook for cardiothoracictrainees. I am proud to be a cardiothoracictrainee and feel privileged to berepresenting the trainees during thisexciting time.
The Trainee Forum at the Society meeting inBournemouth was a great success. Over 100trainees attended the session, almost doublethe number from previous year. This is anindication of increasing involvement oftrainees to forge a brighter future incardiothoracic surgery. The Forum wassupported by a panel consisting of Mr TGraham, Dr Vicky Osgood, Mr C Munsch, Mr SLivesey, Mr P Rajesh, Mr B Jeffrey, Mr SHunter, and Mr S Barnard. They entertainedquestions ranging from entry into specialty,to FRCS(CTh) examinations, to quality oftraining, to the thorny issue of EuropeanWorking Time Directive (EWTD). RegardingEWTD, it is approaching fast and will be herein August 2009. General consensus is toexamine various methods of training within48 hour per week time constraint.Suggestions put forward include, trainees tobecome supernumerary to eliminating night-time duties for trainees.
We need to forge ahead with findingsolutions to optimize our training within thetime constraints imposed by the EWTD. Acontribution to this endeavour is theintroduction of procedure basedassessments. Another aspect to push for istrainee-trainer matching. There are manyideas floating around but the onus is on us,the trainees, to take responsibility of our
training. We are the future and weneed to take an active role indefining our future.
Recruitment into the specialty atspecialist level was done via thenational selection process fromJanuary to March 2009. This wassecond year such a process wasundertaken and 16 candidates wereselected. I was invited as anobserver during the 3-day interviewprocess and I felt that it is a robustand fair process. On the first day,each candidate was interviewed by2 separate panels of 2 interviewers.First interview involved 6 specificquestions asked to all. Secondinterview was review of portfolio.On the second day, each wentthrough 3 practical stations testingsurgical skills and hand-eyecoordination. On the final day, alldid a presentation on a topic givenfollowing short listing. Candidates who wereshortlisted for the Academic Clinical Fellow(ACF) posts, in addition to above, on the firstday had two further rounds of academiarelated interviews by the academic team.Each candidate was scored at each stationand the scores were collated on the final day.Each was ranked and the first 16 wereselected of which 2 were ACF posts. Oneimportant requirement for the ACFappointment was that they should have beenranked among the top 16 on the generalinterview section. Successful candidateswere then matched to respective deanery asper their choice. Candidate number one gotthe first pick, second ranked candidate wasthen matched, and so forth. It is a very wellthought out and comprehensive process.
Tremendous amount of thought and effortare being ploughed into raising theawareness of cardiothoracic surgeryamongst medical students through to coretrainees in surgery. We have embarked on amission to get medical students involved incardiothoracic surgery by experiencing thespecialty in some form during clinicalattachments. We are also exploring avenuesto provide bursaries to medical students toundertake electives in the specialty, either inthe UK or abroad.
Sunil Bhudia, Trainee Representative
& Tim Graham, SAC Chair
The TraineesNewsletter
Over 100 trainees
attended the Forum at
Bournemouth - almost
double the number
from previous year.
But as always, we can only moveforward together…

Throughout our medical training we are exposedto challenging and stressful situations which trialand strengthen our communication andpresentation skills. No amount of rehearsals,examinations or interviews can prepare one for alife-changing interview.
The 2009 interviews for the National Recruitment forST3 in Cardiothoracic Surgery were held over 3 daysin Birmingham in March 2009. Fourteen clinicalNTNs and two Academic Clinical Fellowships wereadvertised and a total of 45 candidates wereshortlisted. The interview form requested an orderof job preference and successful candidates weresubsequently ranked and matched to their choiceaccordingly.
The interview process: The first day was divided intotwo parts, with structured questions in the morningand portfolio based questions in the afternoon.Both sessions lasted 30 minutes, with twointerviewers present at each session. The structuredquestions were based on factual knowledge ofcardiothoracic surgery concentrating on clinicalmanagement, case prioritization, probity and goodclinical practice. I found the questions fair, relevant,and appropriate to our daily clinical practice. Theportfolio session consisted of questions based onour individual portfolios, giving us the opportunityto discuss our career progression and achievementsin depth.
On the second day we were assessed on ourpractical abilities and surgical skills using OSATS(objective structured assessment tools). There werethree OSAT stations lasting 20 minutes each, withtwo examiners at each session. The knot tyingstation measured each candidate’s efficiency viaspecial gloves linked to a computer program. TheVATS station comprised of specific tasks performed
with laparoscopic instruments, and the dissectionstation involved exposing the sapheno-femoraljunction in a groin model using commonly usedsurgical instruments. We were also filmed whilstperforming the dissection and knot tying andthough this was initially slightly daunting, it wasgood practice as we are increasingly expected tooperate in front of other colleagues, and inparticular this is quite common in training courses.
The last day involved a five-minute auditpresentation assessed by a group of consultantsurgeons who then questioned us for a further fiveminutes. This was fairly stressful to start with, butagain a good test of our skills and practice for futurepresentations. At the end of the day we were askedto participate in a virtual reality VATs exercise wherewe were asked to perform certain tasks usinglaparoscopic tools on a computer program. This wasto help evaluate the usefulness of this as a futureassessment tool. I enjoyed this session and thinkthis was an efficient way of measuring hand-eyecoordination and will be helpful in future interviews.Successful candidates were informed of theoutcome by telephone the next morning
An interview is always a stressful experience andthis was no different. Throughout the three dayshowever, we were very well looked after by MrSteven Hunter, the Cardiothoracic Dean, Mr TimGraham the chairman of the SAC and of course theWest Midlands Deanery staff, who were always athand to answer questions and direct us as required.Overall although the three days were grueling,intense and not particularly enjoyable at times, thequestions and the process as a whole were fair andobjective.
National Selection Process The Candidate’s Experience
theBulletin24
There has been considerable interest (and anxiety) fromtrainees about the National Selection Process forCardiothoracic Surgery. We thought it might be helpful tohave the account of 2 trainees who went through the processthis year to inform those who may be considering applying
for the next round. As editor, I have not taken my editorialknife to any of the reports, and I make no apology for theduplication in the two accounts, as they remain intact as twounique perspectives on the process. I thank Alia & Melaniefor their submissions and congratulate them on their success!
Alia Noorani ST3 Cardiothoracic Surgery, East of England Rotation

December 2008 25
for Cardiothoracic Surgery
The 2009 application process for the nationaltraining numbers in cardiothoracic surgeryopened in January. The process was organisedby West Midlands Deanery and gave us 10 daysto complete an online application (I:CAMS) form.There were 16 posts: 14 clinical ST3 trainingposts and 2 academic clinical fellow (ACF)positions.
Initially the I:CAMS application form looked like anightmare, but after navigating through thedifferent sections, it did actually make sense andwas fairly intuitive to use, if a little slow at times.The application required a mixture of details fromyour CV and portfolio, including logbook andextra-curricular activities, along with soundquestions that were appropriate to our field ofcardiothoracic surgery.
Short-listing for interviews was released in midFebruary, with 47 applicants competing for the 16training posts. Of these, only a handful ofcandidates were being considered for the ACFposts.
The interviews were held over 3 days in March atBirmingham City Football Club and werestructured in a way to test the candidaterigorously, but fairly. The first day consisted oftwo 30-minute interviews. There was a structuredinterview in the morning designed to test yourclinical acumen; coping skills in certain situationsand also your views on your own careerprogression. In the afternoon, there was a reviewof your portfolio. A panel of 2 consultantsconducted both interviews.
The second day was OSATS (Objective StructuredAssessment of Technical Skills) day! Thisconsisted of 3 skills stations used to assess
manual dexterity, movement economy, tissue andinstrument handling. The skills stations lasted 20minutes each and included knot tying, dissectionand a thoracoscopic skills station.
The final day of interviews was reserved for auditpresentations. Each candidate had 5 minutes topresent an audit project, which included time forquestions from the panel.
The process was very similar to the 2008interviews, with improvements. This year, wewere given excellent information and the days ranvery smoothly, which was a huge achievementgiven the number of candidates and also thenumber of consultants involved in assessing us.Lady Cynthia was the Lay Chairwoman and wasalways on hand to check that the process wasbeing conducted appropriately and fairly.
Obviously, given the number of candidates short-listed, the interviews had to run over 3 days. Mostof the candidates stayed in the same hotel, whichmade the evenings more sociable, but also attimes, created an air of mass panic, as peoplewent off for the next assessment or interview!
Overall, although this was undoubtedly the mostimportant and nerve-wracking interview of mycareer so far, I rather enjoyed the 3 days and wasable to share a couple of laughs with the panelwhen discussing things. I believe the processtested us thoroughly and in a non-discriminatoryway. Every candidate at the interviews had greatpotential, and the three-day process wasdesigned to give us the opportunity to shine. Thehardest part was waiting 24 hours for the results!
Melanie Jenkins SpR Cardiothoracic Surgery, St Thomas’ Hospital

EnochAkowuah
The Society Cardiac Scholarship at the Royal Melbourne Hospital, Melbourne Australia
theBulletin26
I have always wondered why more UKcardiac surgical trainees do not undertakeoverseas fellowships – that is until I had tomove my family to Melbourne, Australia!The move was challenging for us all but therewards have been immeasurable.
I had always planned to do a fellowshipabroad and I was quite clear about what Iwanted to achieve. I wanted to avoid thetrap of following the well-trodden path tothe large North American centres with ‘thebig names’, which, whilst great for the CV,may not guarantee sufficient hands onexperience. I certainly wanted to go to a‘well known unit’, with a history ofinnovation, a high proportion of high-riskcases and the likelihood of extensivehands on experience. Essentially I wanteda fellowship that would prepare me toperform my day-to-day work as aconsultant in the NHS to a very highstandard. The Royal Melbourne Hospitalseemed to fit the bill.
The philosophy of healthcare delivery inAustralia lies somewhere between the UKand the USA approach. About 40% ofAustralians have private healthcare andthe public hospitals in essence competewith the private sector for this population.This arrangement drives standards in the
public sector, encouraging innovation anduptake of the latest techniques andtechnologies. Public hospitals are very wellfunded. Some standard features in a publiccardiac surgical unit include having twoconsultant anaesthetists for every cardiaccase, routine intra-operativetranoesophageal echocardiography andcardiology consultants on hand to giveintra operative opinions. These areluxuries that I will miss. The other obviouseffect of the private sector is that itencourages intervention and I neverceased to be amazed by the age and/or thelist of co-morbidities of patients referredfor cardiac surgery. For instance, beingover 90 years of age is no barrier to redosurgery or major aortic arch surgery.
The Royal Melbourne Hospital (RMH) is thelargest teaching hospital in Victoria,performing over 1200 cardiac cases peryear. It is consistently the best performingunit amongst units submitting data to theASCATS (Australian Society of Cardiac AndThoracic Surgery) database. Last year’s 30-day mortality for all comers was 1.4% andthe re-exploration rate for bleeding was0.6%. The unit is best known for being oneof the world’s leading proponents of totalarterial revascularisation and they reallypractice what they preach. Vein graftharvesting is a very rare occurrence at theRMH whilst bilateral radial harvesting in80+ years olds is the norm. There is a largethoracic aortic practice and endovascularthoracic surgery is well established. TheRMH was the first unit in the world toreport EVAR for traumatic aortic rupture.The unit has a large GUCH practice and hasone of the world’s largest experiences withthe Ross procedure. The RMH is one of twotrauma centres in Victoria. Trauma casesfrom the entire state (an area the size ofthe UK!) are flown in daily. There wastherefore an excellent opportunity to dealwith a large volume of cardiac and thoracictrauma and this accounted for over 80% ofour out of hours activity.
My Experience
A highlight of my time here has been theextensive level of independent operating
that I have been able to undertake. As afellow I was in theatre five days a weekwith minimal commitment to ward oroutpatient care. In the first six months ofthe fellowship, I was allocated three all-day operating sessions per week, duringwhich I performed a range of operations,
with minimal consultant supervision. Thepatients were selected from the jointcardiac waiting list. They included mediumto high-risk patients undergoing CABG,AVR and aortic surgery. I routinelyperformed CABG with bilateral internalmammary and bilateral radial arteryconduits. Sequential, T-graft, and Y-grafttechniques were the norm. This was a keybenefit of the fellowship. The opportunityto select my own patients, perform surgeryand be in charge of the post-operative carewas fantastic. I also had the opportunity totrain Australian trainees to performcoronary and valve surgery.
During the second half of my fellowship,the emphasis was on performing morecomplicated procedures, particularlyaortic surgery. Most of this attachment wasspent with the three senior surgeons in theunit; Mr J Goldblatt (aortic surgeon),Professor Tatoulis (mitral valve surgeon)and Mr P Skillington (GUCH surgeon). Iperformed complex aortic surgeryincluding the ‘David’ aortic rootremodelling procedures, The ‘Floridasleeve’, warm aortic arch surgery, the Rossprocedure, aortic valve repair, homograftaortic valve replacement and thoracicaortic endovascular stenting. I have alsoperformed complex mitral valve repairFranz Josef glacier in NZ
A day’s fishing of the West Coast ofAustralia

June 2009 27
surgery, multiple valve replacementsurgery; redo surgery, and other GUCHprocedures. No case was considered toohigh risk for teaching. Independentlyperforming an emergency Redo CABGadmitted straight from the catheter suitewith IABP support and aortic valvereplacement surgery in a ventilated patientwith decompensated aortic stenosis onmultiple ionotropes are two examples,which come readily to mind.
One day a week was spent performingthoracic surgery. I performed several majorlung resections and gained experience inVATS lobectomy, which is routinelyperformed here. The thoracic traumaworkload is huge and includes proceduresrarely performed in the UK, like rib fixationfor trauma which is being investigated in a
large randomised trial. Overall, in less than12 months I performed 152 cardiacprocedures and 50 major thoracicsurgical/trauma procedures. There is a significant amount of researchactivity in the unit mostly centred onarterial grafting. I co-authored fiveseparate original articles as well as avariety of case reports and review articles,which will be published in the JTCVS, theATS and JACC. This work has beenpresented at the 2009 SCTS meeting inBournemouth and the Annual meeting ofthe Australian Society of Cardiac andThoracic Surgery in Queensland (2008).
Living and working in Melbourne
I was lucky to undertake my fellowship in acity as beautiful as Melbourne. It isconsistently regarded as one of the bestcities in the world in which to live. It has avibrant cosmopolitan feel with aninteresting mix of new and olderarchitecture: cubic style Millenniumbuildings juxtapose 18th century Anglicancathedrals. My wife and 2-year-olddaughter have really enjoyed Melbourne’slaidback friendly approach, café cultureand extensive facilities for children. Wehave been very privileged, as a family, tovisit some particularly beautiful parts ofthe Southern hemisphere includingTasmania and the South Island of NewZealand.
Working in Australia has been a delight.The ‘can do’ attitude for which Aussies arefamous makes working in a team very easy.My experience overall has been excellent.The heavy operative commitment providedan excellent opportunity to developindependent practice. I have acquiredskills, which will be widely applicable tomy day-to-day work as a consultant in theNHS and will enable me to deliver a highquality service. Furthermore, thisfellowship has allowed me to practicecardiac surgery in an entirely differentenvironment from the one I am used to. Ithas been an excellent training experienceand my family and I are grateful to theSociety for its generous support that madethis fellowship possible.
The pre-race procession (A fire engine foreach driver) at the Melbourne grand prix
Opening match of the rugby league worldcup (Australia 54 England 4)
New AppointmentsName Hospital Specialty Starting Date
Ranjit Deshpande Kings College Hospital, London Cardiothoracic August 2008
Maciej Matuszewski New Cross Hospital Cardiac October 2008
Malgorzata Kornaszewska University Hospital of Wales Thoracic January 2009
Apostolos Nakas Thoracic January 2009
Pedro Catarino Papworth Hospital Cardiothoracic February 2009
Mahmoud Loubani Castle Hill Hospital Cardiothoracic April 2009
Ian Hunt St George’s Hospital Thoracic May 2009
Ira Goldsmith Morriston Hospital Thoracic May 2009
Theo Velissaris Manchester University Hospital Cardiac May 2009
Antonio Martin-Ucar Nottingham City Hospital Thoracic July 2009

Annual Meeting Report -Bournemouth 2009
theBulletin28
In the last Bulletin I stated thatBournemouth was easy to getto... and as I sat in the coachreplacing the train fromSouthampton airport to thetown centre I suspected thatsome delegates might contestmy claim.
Despite the challenges of travel anamazing 480 delegates registeredthis year making it another recordattendance, and in general thefeedback has been very positive –hopefully indicating that the meetingis becoming more and more relevantto our professional lives.
Sunday afternoon started with thebest attended Trainees Meeting todate. Sunil Bhudia had created atopical and interesting agendaranging from National Selection tothe Specialty Exam with speakersincluding the SAC chair, Tim Graham,the Postgraduate Dean, Steve Hunterand the Chairman of IntercollegiateExam Board, Bob Jeffrey.
Also on Sunday afternoon theAssociation of CardiothoracicSurgical Practitioners (ACSA) heldtheir AGM. This is the second timethey have decided to hold theirmeeting in conjunction with the SCTSand included a presentation fromPapworth on how surgicalpractitioners are now performingsternotomies and harvesting the IMA.After an impressive term of office asPresident, Tony Jessop (Hull) is beingsucceeded by Toby Rankin(Plymouth).
Symposium
After the Hunterian lecture by PatrickTansley, ‘Reversal of Heart Failure’,we gathered in the main auditoriumfor the symposium ‘Choice of conduitfor CABG’. David Taggart reviewed thecurrent evidence, Philip Heyward
presented the Melbourne arterialexperience and Malcolm Dalrymple-Hay presented the evidence forendoscopic vein harvesting.
The Mayor of Bournemouthgenerously hosted the WelcomeReception, where delegates relaxedand caught up with friends andcolleagues.
More blue sky and sunshine greetedus on Monday, which started earlywith a well attended scientificsession. The plenary sessioncombined the surgeons, ACSA andthe Cardiothoracic Forum and wasconcluded by Professor AlainCarpentier presenting his insight intothe recent developments of the totalartificial heart.
Database Managers
The Database Managers’ Meetingheld their fourth annual meeting, andCCAD have generously supportedthem all. Tracey Smailes(Middlesbrough) had arranged aninteresting agenda includingpresentations by Phillip Kimberley,Royal Brompton /Harefield andSheila Jamieson from Freeman RoadHospital. After lunch the mainauditorium was packed to hearpresentations regarding UKcardiothoracic activity in its entirety,chaired by Ben Bridgewater. Thisincluded challenging presentationson the past, present and future of UKtransplant activity (Professor Dark)and congenital surgery (Mr LeslieHamilton). This session wasconcluded by an outstanding talk bySir Bruce Keogh on quality indicatorsin the NHS. His presentationcaptivated the audience, whichincluded 12 patient representativesfrom the Bournemouth andSouthampton area.
This was the first time that patientrepresentatives had been invited toour annual meeting, all of whom were
The Commercial Exhibition
The Commercial Exhibition
The Meeting Dinner
Patients visiting the Meeting

June 2009 29
leaders in their respective patientgroups. Our executive patientrepresentative, David Geldard MBE,hosted them throughout the day andwe enjoyed receiving their feedbackon their experience. This is adevelopment that we want continue inour future meetings and there arealready plans for the Liverpoolmeeting.
The Forum
The Cardiothoracic Forum wasprivileged again to welcome MauraBuchanan, President of the RCN togive the opening remarks and thiswas followed by a very touching andprovocative session where the groupshared the experiences of patient LisaKitteridge, who had spent manyweeks in hospital undercardiothoracic care being treated withan LVAD. There were presentationsfrom the lead professionals involvedin her care, reminding everyone of thegreat service that we provide, but alsohow we should always remember toput the patient at the fore front of ourthoughts.
Dr David Adams, Mount SinaiHospital, New York gave the HeartResearch UK lecture on mitral valverepair and on the following day hewas involved in the very popularcardiac workshop with the help ofFrank Wells (tricuspid) and ProfessorMark Redmond (aortic).
After tea on the Monday the ThoracicSurgical content started inabundance. In the CardiothoracicForum, Eric Lim gave an update onlung cancer staging, followed by asymposium that included RichardBerrisford in his current role asSecretary of the European Thoracic
Surgical Society and AlessandroBrunelli (Ancona) who presented theEuropean perspective on auditingquality of care in thoracic surgery.
The day concluded with a symposiumon TAVI organised and chaired by NeilMoat. The audience could only beimpressed how this new technique isbeing applied so effectively. DrMartyn Thomas (St Thomas’)presented the cardiology views ofsuccess and we enjoyed ProfessorFriedrich Mohr’s (Leipzig)presentation on his outstandingprogramme and his vision for thefuture.
Perfusion Scientists
We were delighted to welcome backthe Society for Clinical PerfusionScientists, Great Britain and Ireland,who had elected to continue theirassociation with our annual meetingby holding their workshop on unitaccreditation as well as theircommittee meeting. Although, it isnot possible for us to fully merge ourannual meetings, it is hoped that wecan continue this association foryears to come.
On Tuesday we welcomed thecongenital surgeons, who hadrequested an additional sessioncompared to their two previousmeetings. Dr Andrew Cook,Morphologist brought specimens todemonstrate the anatomy forAtrioventricular septal defects and inthe afternoon we also welcomed DrNicholas Doll from Stuttgart todiscuss atrial fibrillation.
The thoracic surgeons adopted anoesophageal theme, and followingpresentations on the subject we were
Simon KendallMeeting Secretary
Professor Alain Carpentier
Rachel Woolf & Isabelle Ferner
Terrence English

theBulletin30
honoured to welcome Dr Tom DeMeesterto present the thoracic surgical lecture onthe history of en-bloc oesophagectomy.
In total 111 papers were presentedthroughout the Annual Meeting and alsodisplayed as posters in the exhibition area.I am greatly indebted to Ian Wilson whohas been very innovative with the contentand guests. The lead reviewers werepivotal in creating the scientific content -they organised their co-reviewers and theselection process, going on to constructthemed sessions that appear to be morepopular than our previous format.
Each paper is scored by two chairman andtwo assessors – over 60 individuals whoare vital to the smooth running of thesessions, to encourage good discussionand to score the presentations.
The support from Industry continues to beoutstanding despite the current economicrecession. Rachel Woolf has nowemigrated to Israel and this was to be herlast meeting since joining in 2004 – shehas nurtured excellent relations withestablished and new companies and hasleft us in a much more secure setting thanwhen she started. The meeting could notcontinue in its present format withoutindustry’s close involvement, not only interms of the exhibition area, but also theirsponsorship of scientific sessions. We tryvery hard to give each of them value fortheir money and hope we can maintain therelationship to our mutual benefit.
The Cardiothoracic Forum continued to bevery well attended on the Tuesday withpapers sharing best practice, as well as asession discussing the modernisation ofnursing careers and the strategic impact ofchanging our workforce. The Forumcontributes immense added value to theAnnual Meeting – Tara Bartley has beenthe nursing representative since 2006 andhas developed the forum out of allrecognition. The content has expanded butnot at the expense of the quality, and shehas attracted outstanding speakers to talkto a carefully considered agenda.
After lunch on Tuesday Steve Liveseyorganised an NCEPOD symposium to sharebest practice in MDTs for coronaryrevascularisation chaired by Marisa
Mason, who is herselfchairman of NCEPOD.
Prizes
For the second year in a rowall the tickets for the annualdinner had been sold, whichincluded a seaside themebefore and after the meal.We were delighted thatIsabelle Ferner’s father wasable to entertain us on thepiano throughout the meal,during which the prizes andthe scholarships wereannounced –
Ronald Edwards Medal forBest Scientific Paper – H Fallouh – King’s CollegeHospital London
John Parker Medal for BestClinical Paper – S Attaran – King’s CollegeHospital London
Society Thoracic Medal forBest Thoracic Paper – K Sarraf – Royal BromptonHospital London
Society CT Forum Medal for Best ForumPaper – Author / Unit P Agostini
The Society Cardiac Scholarship – Paul Modi
The Society Thoracic Scholarship – Carol Tan
At the conclusion of the meal Sir TerenceEnglish was awarded his lifetimeachievement award for his outstandingcontribution to cardiothoracic surgery andin particular transplant surgery. His careerwas beautifully summarised andpresented by Frank Wells.
The Annual Meeting continues to evolveand tries to adjust to current trends in ourclinical lives as well as the NHS in itsentirety. Prior to 2002 the Annual Meetingwas organised by Concorde Services andin some respects it was a duty rather thanan enjoyment to attend. As a society webenefited from Rob Lamb’s personal
circumstances that allowed him to work sohard to restructure the meeting and allowit to develop as it has. In recognition of hisachievement he was presented with anhonorary lifetime membership of thesociety.
Finally I must acknowledge thesuperhuman contribution by IsabelleFerner – she is fundamental to so verymany aspects of the meeting and we arevery fortunate as a Society to enjoy theexcellence that she continually delivers.
We hope we can continue to develop themeeting in Liverpool next year. The newconference centre is magnificent, situatednext to the city centre on the banks of theMersey and I hope you will be putting thedates in your diary: 7th - 9th March 2010.
We hope to see you there!
Annual Meeting Report - Bournemouth 2009
The President with the Mayor of Bournemouth

June 2009 31
Diary of Forthcoming Events
Date: 16 January 2009 Meeting: Yorkshire Advanced Chest Imaging CourseTown: LEEDS UNITED KINGDOM Venue: Radiology Academy, Leeds General Infirmary, Leeds
LS1 3EXContact: Dr R J H Roberson, Consultant RadiologistEmail: [email protected]
Date: 31 JULY - 4 AUGUST 2009 Meeting: 13th World Conference on Lung Cancer (WCLC
2009)Town: SAN FRANCISCO, CA UNITED STATES Contact: Khara RobertsonPhone: +1-604-681-2153Email: [email protected] Web: www.2009worldlungcancer.org
Date: 10 - 11 SEPTEMBER 2009 Meeting: 3rd David Sharpe Memorial SymposiumTown: BLACKPOOL UNITED KINGDOM Venue: Lancashire Cardiac Centre, Blackpool Victoria
HospitalContact: Lorraine Richardson, L R AssociatesPhone: +44 (0)1296 733 823Fax: +44 (0)1296 733 823Email: [email protected]
Date: 14 - 16 SEPTEMBER 2009 Meeting: BACCN Conference 2009 Town: BELFAST UNITED KINGDOM Venue: Waterfront HallContact: Conference Office
Benchmark Communications LtdPhone: +44 (0)191 241 4523Fax: +44 (0)191 245 3802Email: [email protected]: www.baccnconference.org.uk
Date: 24 - 27 SEPTEMBER 2009 Meeting: BIRMINGHAM REVIEW COURSE IN
CARDIOTHORACIC SURGERYTown: BIRMINGHAM UNITED KINGDOM
Education Centre, Birmingham Heartlands HospitalContact: Lorraine Richardson L R AssociatesPhone: 01296 733 823Fax: 01296 733 823Email: [email protected]: www.birminghamreviewcourse.com
Date: 29 SEPTEMBER – 1 OCTOBER 2009 Meeting: First International Meeting of the Jordanian
Association of Thoracic and Cardio VascularSurgeons
Town: AMMAN, JORDANContact: Dr. AbdullahAl-Qudah Fawz ShocairPhone: +962 79 5557838Email: [email protected]
Date: 23 - 24 OCTOBER 2009 Meeting: Society of Clinical Perfusion Scientists of GB &
Ireland Congress 2009Town: LEICESTER UNITED KINGDOMVenue: The Marriott HotelContact: Simon Philips
St George's Healtchard NHS TrustEmail: [email protected]: www.sopgbi.org
Date: 5 - 6 NOVEMBER 2009 Meeting: Advances in Thoracic SurgeryTown: LONDON UNITED KINGDOM Venue: National Heart and Lung InstituteContact: Maria Leung (PA to Eric Lim)Fax: +44 207 351 8560Email: [email protected]
Date: 6 NOVEMBER 2009 Meeting: Yorkshire Chest Imaging CourseTown: LEEDS UNITED KINGDOM

A UK Surgeon’s Perspective on theAF Consensus Statement… But What Do you Think?
theBulletin32
With last year’s publication of theConsensus Statement on catheter andsurgical ablation for atrial fibrillation (AF)(Hugh, Josep et al. 2007;www.heartrhythmjournal.com/article/S1547-5271(07)00498-5/fulltext), therenow exists some guidance towardstreating and managing patients with bothparoxysmal and persistent AF. Over thepast few years the management of AF incardiac surgical patients has beenexpanding but there has been little in theway of advice to those staring out. TheConsensus Statement provides aframework that an individual and/or unitcan use to embark and develop aprogramme for the management of AF. Thestatement consists of thirteen sections,the bulk of them relating to catheter basedinterventions. The statement alsoacknowledges the limitations of consensusagreement, i.e. there was not completeagreement by all authors on all theconsensus statements. In common withprevious reports, representation from thecardiac surgery was limited. In this articlethe application of the statement to cardiacsurgical practice in the UK will bediscussed.
The definition of AF has been addressedand it is recommended that the followingterms be used: Paroxysmal, Persistent,Longstanding Persistent and Permanent(Table 1). This classification does awaywith Cox’s (Cox 2003) simpler classificationof AF being intermittent or continuous. Thecurrent classification appears to be moretreatment orientated.
The origin and mechanism of AF isoutlined. This should be read inconjunction with excellent articles byNattel (Nattel 2002) and Wyse (Wyse andGersh 2004). These papers review thecurrent theories of the development of AFand explain the evolution from focaltriggers in paroxysmal AF (PAF) tosubstrate change (atrial remodelling) inpersistent AF. In this way one can view theclinical picture of a patient as a continuous
process that starts as episodes of PAF dueto predominately focal triggers ofarrhythmic activity and over time becomespersistent due to atrial remodelling.
Currently it is rare in the UK for patients toundergo surgical treatment for lone AF. Thevast majority of patients presenting to thesurgeon are those with concomitant AF.The management of these patients ishighly variable in the UK. The Statementshould help to develop a more uniformapproach to patients with AF and hopefully
more consistent results. The rationale forestablishing sinus rhythm (SR) is clearlyoutlined, and although contentious indetails, there appears to be agreementthat SR confers a better outcome than AF.Equally, it is made clear that ablationprocedures should be performed in thepresence of symptomatic AF or in thoseasymptomatic patients undergoing cardiacsurgery in whom ablation would addminimal risk. This casts doubt on practiceswhere concomitant AF has been treatedregardless of symptoms and/or complexityof the operative procedure in all patientscoming to cardiac surgery.
The environment in which patientsundergo ablation for AF is of paramountimportance, particularly for the catheterbased procedures. The statement providesprinciples on how training and competenceshould be achieved. This ranges frompatient selection, anatomical knowledge,conceptual knowledge, technical ability,
management of complications and follow-up. Catheter based AF treatment is timeconsuming and in these situations, theprocedure is technically demanding andrequires a skilled operator. In contrast,concomitant ablation in the operatingtheatre requires skill and knowledge that iseasily taught and reproducible. Themodern ablation devices are relatively userfriendly and quick to use andcomplications are now rare. All majordevice manufacturers provide training inthe UK with either visits to centres or
bringing proctors to a surgeon’s own unit.The technical expertise required toperform an ablation in concomitantprocedures is well within the ability ofcardiothoracic surgeons.
Although the technical aspects of surgeryfor AF are easy to master, the extent of thelesion set has been variable betweenindividual operators. The Statement doesnot set out to define a specific lesion set,but does provide two generalobservations. Firstly, that more extensiveleft atrial lesion sets provide better long-term freedom form AF and secondly,results are significantly better with biatriallesions sets when compared to left atriallesion sets alone (up to one third ofpatients have triggers outside of thepulmonary veins). This is more relevant tosurgical practice as most patients with AFcoming to surgery have either persistent orlongstanding AF. In these patients thelikelihood or return to SR will be poor with
Table 1Paroxysmal AF Recurrent AF (≥ 2 episodes) that terminate spontaneously
within 7 days.
Persistent AF AF sustained beyond 7 days or less than 7 days but requiringpharmacological/electrical cardioversion.
Longstanding Continuous AF 1 year durationPersistent AF
Permanent AF Patients with AF in whom a decision has been made not toattempt restoration of sinus rhythm by any means.

June 2009 33
PV ablation alone. It will be necessary inthese patients to perform extra lesions inthe LA and for maximal success rates totreat the RA. This should be taken intoconsideration when the patient is beingconsented for this procedure. It would notbe acceptable to quote success ratesobtained from studies using biatrialablations to be quoted to a patient havingPV isolation alone for longstanding AF.
Although not stated in the ConsensusStatement, researchers have been awareof the impact of LA size on the success rateof ablation for AF. No specific size ismentioned, but previous studies havesuggested that LA sizes greater than 50-55mm have lower success rates(Grubitzsch, Beholz et al. 2008),(Geidel,Ostermeyer et al. 2005). A large number ofpatients undergoing cardiac surgery haveatria similar or larger than this and this willimpact on long-term results of ablation.The Statement is light on how to managethe left atrial appendage and the Ligamentof Marshall. Both these are easily dealtwith during concomitant procedures, butpose challenges for the catheter andminimally invasive approaches. The lack ofany consensus on this matter is probablymore a reflection of the preponderance ofcardiologists on the panel. Both thesestructures should be dealt with in patientsundergoing an open surgical procedure.The ligament is easily divided and theappendage can be dealt with by a numberof recognised ways. The Ligament ofMarshall has been implicated by a numberof authors as a site for triggers andrecurrence.
It is no longer sufficient to perform a lesionwithout demonstrating conduction block.This has been common practice in thecatheter lab, but not in the operatingtheatre. With the new ablation kitsavailable, pacing and sensing probes arenow sufficiently developed to allow intra-operative testing of conduction block. Thenewer tools also permit the localisation ofautonomic ganglionic plexi, the ablation of
which has been shown to increase the rateof success.
Surgical treatment for lone AF has beendone within the UK but it has been limitedby logistical and economical factors. Theconsensus recommends that patients onlyundergo stand alone AF treatment insymptomatic patients who prefer asurgical approach, have failed catheterablation or in whom catheter ablation iscontraindicated. Such patients will onlycome through via electro-physiologists,and in such instances there needs to bemore of a multi-disciplinary approach.Proper documentation of the type of AF. LAsize, planned lesion set, management ofthe LA appendage, ablation of ganglionicplexi, documentation of conduction block(see below) needs to be done. With such aplan it will then be possible to consent thepatients in a more informed manner. Insuch circumstances the success rates andrisks quoted to the patient should be thosebased on the units owns experience.
The measurement of success followingablation now has a specific meaning. Theprimary endpoint is ‘Freedom fromAF/flutter/tachycardia off anti-arrhythmictherapy’. The aim of such a strict definitionappears to be to provide an ideal stateform the patient’s perspective. If widelyadopted it will also permit easiercomparisons between the various ablationtechnologies. The follow-up of patientsfollowing ablation will impact on standardcardiac surgical practice. Units carrying outablations should ensure that there areadequate follow facilities and thatreferring physicians are aware of the needfor detailed follow up. It is recommendedthat patients are seen for two yearsfollowing ablation and that spot ECGs as ameans of confirming success are notsatisfactory. Using standardiseddefinitions of success and monitoring itwill make it easier in the future to comparethe results from different studies.
Surgery has a major role in the treatmentof AF. The initial work by Cox has set themethodological approach that surgeonsshould still adhere to. The aim of suchprocedures is to cure the patient of AF,relief of symptoms and abolition of long-term problems of AF. In the current era it iseasy to be lured into a false sense ofsecurity that one is doing the right thing.Surgeons should not limit themselves toinappropriate lesion sets just becausecertain lesions are not done in the catheterlab. Equally they must resist beingrestricted by the limitations of technology.The consensus statement provides thegroundwork upon which we can build ascientific approach to the varioustreatments being offered in the treatmentof AF. For surgeons this entails treatingsymptomatic patients or patients in whomthe procedure will not incur undue risk.Patients with paroxysmal AF will do wellwith a left sided ablation alone, but forpersistent and longstanding AF a biatrialablation is strongly recommended.
Ablation patients require long-term followup. It is not practical for all patients toreturn to the tertiary centre for such followup. Using the Consensus Statement,cardiac networks should be able to drawup local protocols for selecting, treatingand following up patients. There are anumber of unresolved issues, but usingsuch a network approach will permit unitsto find answers and work in the patients’best interest.
Please submit your views either directly to:[email protected], or register your support/criticism/ ideas at theConsultant Forum at www.SCTSLTD.co.uk
Uday Trivedi,Royal Sussex County
Hospital, Brighton

Society for Cardiothoracic Surgeryin Great Britain and Ireland
by Samer Nashef
Across 9 Breathed his last (7)10 More temperamental in low, dire trouble (7)11 Trail skis, at no regular addresses (5,2)12 Sticky or humid metal (7)13 They share same motor? (4-5)15/25 Ride lumpy, so built a divine home (5,7)16 Boat and bed form part of the story (7)19 Freedom in the morning unknown at home
(7)20 Heads rolling in the underworld (5)21 We hear hairdo and crash diet will lead to
beauty (9)25 See 1526 I’m queer about hymn (7)28 Apply within: it’s open for certain (7)29 Allows football manager to lose his head (7)
Down 1 15/25 drink: source of wild trance (6)2 A vote on love god (6)3 Love is painful when rejected (4)4 These days, riot can be handy (6)5 15/25 food: I’m so Arab! (8)6 Order soldier to avoid bloomers (2,8)7 Little mother’s baselines (8)8 Readily provide around frolic with model (8)14 Different smile and a role that’s very
different (5,5)16 Half train in dog transport: that’s trained (8)17 Seriously turned poor (5,3)18 Move faster, Royal Navy, move (8)22 Messenger brings no end to woman’s
trouble (6)23 Two 99s: lick end at first, it’s frozen! (6)24 Tangle with headless chicken wire (6)27 Essential sounding dock (4)
Send your solution to: Samer Nashef, PapworthHospital, Cambridge CB23 3RE or fax to 01480 364744by 31 July 2009. Solutions from areas over 10 milesfrom Cambridge will be given priority.
Last issue’s winner:The winner of the last crossword is Mr Mark Miller,Chief ODP, Department of Cardiac Surgery, RoyalSussex County Hospital, Brighton BN2 5BE
bulletinthe
crosswordthe

INNOVATIVE PRODUCTS FOR LESSINVASIVE SURGERY
VASOVIEW™ ENDOSCOPIC VESSELHARVESTING SYSTEMS
MAQUET LIMITED14 - 15 Burford WayBoldon Business ParkSunderlandTyne and WearNE35 9PZtel: 0191 519 6200fax: 0191 519 6201email: [email protected]
MEMBER OF THEGETINGE GROUP
Endoscopic Vessel Harvesting, also
known as EVH, is a minimal invasive
technique used to obtain healthy blood
vessels for coronary bypass surgery.
It was pioneered in America, where it
is now used in over 80% of cardiac
bypass procedures.
Following its acquisition of Boston
Scientific's cardiac and vascular
business, Maquet is now making this
innovative system available in Britain.
Efficient harvesting of saphenous vein orradial artery A less-invasive 2cm incision
Significantly less risk of infection andwound complications
More rapid recovery
Less postoperative pain
Minimal scarring for improved cosmesis
Excellent conduit quality and haemostasisresults
MAQUET - The Gold Standard