JAMA-1998-Kozyrskyj-1736-42[1]
![download JAMA-1998-Kozyrskyj-1736-42[1]](https://fdocuments.net/public/t1/desktop/images/details/download-thumbnail.png)
of 7
-
Upload
fasika-mekete -
Category
Documents
-
view
218 -
download
0
Transcript of JAMA-1998-Kozyrskyj-1736-42[1]
-
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
1/7
Review
Treatment of Acute Otitis MediaWith a Shortened Course of AntibioticsA Meta-analysisAnita L. Kozyrskyj, BScPhm, MSc; G. Elske Hildes-Ripstein, MD; Sally E. A. Longstaffe, MD;
J. Leigh Wincott, MD; Daniel S. Sitar, BScPhm, PhD; Terry P. Klassen, MD, MSc; Michael E. K. Moffatt, MD, MSc
Objective. To conduct a meta-analysis of randomized controlled trials of an-tibiotic treatment of acute otitis media in children to determine whether outcomeswere comparable in children treated with antibiotics for less than 7 days or at least7 days or more.
Data Sources. MEDLINE (1966-1997), EMBASE (1974-1997), Current Con-tents, and Science Citation Index searches were conducted to identify randomizedcontrolled trials of the treatment of acute otitis media in children with antibiotics ofdifferent durations.
Study Selection. Studies were included if they met the following criteria: sub- jects aged 4 weeks to 18 years, clinical diagnosis of acute otitis media, no antimi-crobial therapy at time of diagnosis, and randomization to less than 7 days of an-tibiotic treatment vs 7 days or more of antibiotic treatment.
Data Extraction. Trial methodological quality was assessed independently by7 reviewers; outcomes were extracted as the number of treatment failures,relapses, or reinfections.
Data Synthesis. Included trials were grouped by antibiotic used in the shortcourse: (1) 15 short-acting oral antibiotic trials (penicillin V potassium, amoxicillin[-clavulanate], cefaclor, cexime, cefuroxime,cefpodoximeproxetil, cefprozil), (2)4intramuscularceftriaxonesodiumtrials,and (3)11 oralazithromycin trials.The sum-maryodds ratiofortreatmentoutcomesat8 to19days inchildren treatedwithshort-acting antibiotics for 5 days vs 8 to 10 days was 1.52 (95% condence interval [CI],
1.17-1.98) but by 20 to 30 days outcomes between treatment groups were com-parable (odds ratio, 1.22; 95% CI, 0.98 to 1.54). The risk difference (2.3%; 95%CI, 0.2% to 4.9%) at 20 to 30 days suggests that 44 children would need to betreated with the long course of short-acting antibiotics to avoid 1 treatment failure.This similarity in lateroutcomes was observed for up to 3 months following therapy(odds ratio, 1.16; 95% CI,0.90-1.50).Comparable outcomeswere shown betweentreatment with ceftriaxone or azithromycin, and at least 7 days of other antibiotics.
Conclusion. This meta-analysis suggests that5 daysof short-acting antibioticuse is effective treatment for uncomplicated acute otitis media in children.
JAMA. 1998;279:1736-1742
ACUTE OTITIS MEDIA (AOM) is oneof the most common reasonsfora childtobebrought to a source ofhealthcare. Be-fore age 7 years, 65% to 95% of childrenwillhave experienced 1 ormoreepisodes
of AOM.1 Acute otitis media is the mostcommon indication for antibiotic pre-scribingintheUnitedStates;over90%of childrenwithAOM will be treatedwitha10-day courseof antibiotics. 2,3 Ithasbeenestimated that more than $3.5 billion isspent annually on managing AOM in theUnited States. 4 The decline in suppura-tivecomplications of otitis media (OM)inNorth America and Europe during the1940s and 1950s has been attributed toantibiotictherapy. 5 Morerecentevidencesuggests that long-term outcomes aresimilar in antibiotic-treated and un-treated children with AOM living indeveloped countries. 2,6-8 Practitioners in
North America, however, may be hesi-tant to discontinue prescribing antibiot-ics altogether. In fact, 2 recent meta-analyses of children with AOM reportedthat compared with placebo, antibiotictreatment did hasten the resolution of acute symptoms. 9,10 In some of the trials,symptoms abated by 2 to 3 days of anti-
biotictreatment,suggestingthatacourseof antibiotics of less than 10 days of therapy may be an effective alterna-tive. 6-8
For editorial comment see p 1748.
The emergence of drug resistance incommunity-acquired infections, such asthat reported in children receiving pro-phylaxis forrecurrentOM, has increasedconcernoverthe indiscriminateprescrib-ing of antibiotics. 11,12 This concern is evi-dent in recent expert opinion which rec-ommends that the duration of antibiotictreatment in uncomplicated AOM be de-creasedto5days;thisrecommendationhasbeen further qualified to exclude youngchildren. 13,14 The quality of scientific evi-dence to support a policy for shortercourses of antibiotic treatment has beenassessed, 15 buta systematic, quantitativeevaluation of this evidence is lacking.Therefore, a meta-analysis of the avail-ableevidence on theantibiotic treatmentof AOM was undertaken, with the pri-mary objective of determining whethertreatmentwitha shortcourseof antibiot-ics was comparable to treatment with alonger course.
METHODSTrial Identication
Randomized controlled trials compar-ingdifferentdurationsofantibiotictreat-ment inchildrenwitha diagnosis ofAOMwere identified from MEDLINE (Janu-ary1966 to July 1997), EMBASE (Janu-ary1974to July 1997), Current Contents(January to July1997), andScience Cita-tion Index searches. There were no lan-
From the Department of Community Health Sciences(Ms Kozyrskyj and Dr Moffatt), Manitoba Centre forHealthPolicy andEvaluation(Ms Kozyrskyj), the Depart-mentof Pediatricsand ChildHealth (DrsHildes-Ripstein,Longstaffe, Wincott, Sitar, and Moffatt), and ClinicalPharmacologySection (DrSitar),Universityof Manitoba,Winnipeg, Manitoba; andDepartmentof Pediatrics,Re-search Institute, Childrens Hospital of Eastern Ontario,University of Ottawa, Ottawa, Ontario (Dr Klassen).
Reprints:Michael E.K. Moffatt, MD,MSc, UniversityofManitoba, Department of Community Health Sciences,andPediatrics andChildHealth, Faculty ofMedicine,750Bannatyne Ave, Winnipeg, Manitoba, Canada R3E 0W3.
1736 JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/ -
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
2/7
guage restrictions. 16 In MEDLINE,searchtermsemployedwere otitismediain medical subject headings, modified byacute in thetitleorabstract.These termswere combined with the terms of ran-domized controlled trials , random allo-cation ,double-blindmethod ,single-blindmethod , or with the term randomizedcontrolled trial in publication type. Thisstrategy, which was approximated fortheEMBASE search, was an adaptationof one deemed optimally sensitive foridentifying randomized controlled trialsin MEDLINE. 17 Reference lists of rel-evant publications were reviewed toidentify further trials. Where abstractswere referenced, attemptswere madetoobtain the published version.
Trial Selection and QualityClinical trials of the antibiotic treat-
ment of AOM were independently as-sessed for inclusion by the 7 authors, ac-cordingtothefollowingcriteria:(1)patientsbetween theagesof 4 weeksand 18years,
(2) clinical diagnosis of AOM and no anti-microbial therapy at time of diagnosis,(3) random assignment toantibiotictreat-mentoffewerthan7daysvsatleast7days,and (4) an assessment of clinical resolu-tionofAOM. 18Trialswereexcludediftherewas planned surgical cointervention, butnot if myringotomy subsequent to treat-mentfailure or tympanocentesis wasper-formed. Concurrent use of a second anti-bioticwasnota criterionfor trialexclusion,but children given additional antibioticswere counted as treatment failures.
The internal validity of included trialswas assessed by the same authors using
the Jadad scale.19
The scale assignedscores from 0 to 5 (best-quality trial),based on the following criteria: (1) studyparticipants were randomly allocated totreatment using an appropriate methodsuch as a random numbers table, (2) theintervention wasdouble-blindedusinganidentical lookingand tasting placebo, and(3)an accounting anddescriptionof studywithdrawals weredone. 20 Concealmentof treatment allocation was also evaluatedfor adequacy. 21,22 Rater assessment wasblindedinthemajorityoftrialsbyremov-ing all identifying features of the pub-lished trial, such as author names, affilia-tions,andsources offinancialsupportandbyrandomorderingof trials. 20 Interrateragreementon trial inclusionand thequal-ity score was assessed by the statisticusing PC Agree software (Stephen Wal-ter,McMasterUniversity,Hamilton,On-tario). Agreement was categorized usingLandis and Koch guidelines. 23
Data Abstraction andDenition of Terms
The primary outcome of interest wastreatment failure, which included lack of
clinical resolution or relapse or recur-renceofAOM, duringa 31-dayperiodfol-lowing the initiation of therapy. Clinicalresolution meant that the presentingsignsorsymptomsofAOMhadimprovedor resolved. A secondary outcome wasthecumulativenumberof treatment fail-ures, relapses, and recurrences reportedfrom time of diagnosisuntil a final evalu-ationpointbetween1to3months.Middleeareffusionwas not classified as a treat-ment failure because of its documentedpersistence during the course of the dis-ease, regardless of treatment. 9
Twoauthors independentlyabstractedprimary and secondary outcome datafrom each blinded trial, using a standard-izeddataextractionform.Wherepossible,outcome datawereextractedfor childrenboth older and younger than 2 years, andfor children with perforated and nonper-forated tympanic membranes. 8,24-26 De-scriptive data were also collected on thetreatment site, patient baseline charac-teristics, cointerventions, and inclusion,
exclusion,andoutcomecriteria.Thenum-berofwithdrawalsineachtreatmentarm,including those lost to follow-up, thosewith adverse drug effects, and those notcomplying with the study protocol, wasrecorded.
Data AnalysisMeta-analyses were performed on
trials grouped by the pharmacokineticbehavior of the antibiotic used inthe short-treatment arm, as follows:(1)short-actingoralantibiotics,eg,peni-cillin V potassium, amoxicillin, cefaclor,cefuroxime; (2) oral azithromycin; or
(3) intramuscular ceftriaxone. Addi-tional meta-analyses were conducted inthe short-acting antibiotic group fortreatment duration of 48 hours or lessand greater than 48 hours.
Themeta-analyseswerecarriedoutus-ingtheCochraneCollaborationsRevman3.0program(CochraneCollaboration,Ox-ford, England. The risk of treatment fail-ure with a short course of antibiotics, incomparison to a longer course, was ex-pressed as an odds ratio (OR). An ORgreater than 1 indicated a greater num-berof failures with theshortcourseofan-tibioticsandsuperiorityofthelongcourseof antibiotics. The ORs were calculatedfor individual trial outcomes and, usingthe Peto fixed-effects model, a summaryOR was determined for trials pooled byantibiotic type. Statistical heterogeneityamong trials was assessed, 27,28 and trialswith outlying ORs were further investi-gated. 29 In addition, summary ORs werecalculated using the DerSimonian andLairdrandom-effectsmodel. 30 Toprovideadditional clinical meaning, results werealso expressed as a summary risk differ-ence in the failure rate and the number
needed to treat to experience an addi-tionalfailureintheshorttreatmentarm. 28
Sensitivity analyses were conductedto assess the robustness of the meta-analysis by comparing summary ORsamong groupsredefined by (1)excludingtrials of a lower methodological quality(quality 2), (2) excluding trials that in-cludedchildrenwithrecurrentor chronicOM, and (3) excluding trials of compari-sonsbetweendifferentantibiotics. 27Asen-sitivity analysis of outcome criteria wasalsoconductedby redefiningclinicalreso-lution to include cure, but not improvedsymptoms. A funnelgraphof the samplesize vs the OR was plotted to determinewhether publication bias existed. 27
RESULTSLiterature Search and Trial Inclusion
TheMEDLINEsearchyielded 209ci-tations of randomized controlled trials inAOM, of which 36 were assessments of theantibiotictreatmentdurationofAOMin children. An additional 4 trials werefound among 236 clinical trials of AOMidentifiedby theEMBASEsearch.Fourtrials not identified by MEDLINE orEMBASEwereretrieved from theCur-rent Contents index search and refer-ence listings. Three clinical trials of an-tibiotics no longer used today wereexcluded, 31-33 leaving41 citationsfor fur-ther assessment according to inclusioncriteria. Substantial interrater agree-ment for trial inclusion into the meta-analysis for theremainingtrials ( score,0.89; 95% CI, 0.86-0.92) was attained.Twelveof these trials wereexcludedfromthe meta-analysis for the following rea-
sons: duration of antibiotic therapy wasequivalentin bothtreatment arms 34-39;du-ration of antibiotic therapy in both treat-mentarmswaseitherfewerthan7days 40,41or 7 days or greater 42; there was no com-parison ofdifferentdurations ofantibiotictherapy 43; trialparticipantswerepredomi-nantlyadults 44;orinsufficientdatawerere-portedinabstract. 45 Thisleft32trials,con-tainedin29publishedreports,forinclusionin the meta-analysis. The 32 trials weredistributedinantibioticgroupsas follows:17 were short-acting antibiotics, 26,46-58 4were ceftriaxone sodium, 59-62 and 11 wereazithromycin. 63-73 Two of the trials were
in a language other than English.53,57
Methodologic QualityThemeanqualityscoreforallofthetri-
alswas2.66(SD,0.97)of a maximum scoreof 5 (Table 1). Ceftriaxone trials scoredhighest (mean, 3.50;SD, 0.58),followedbyshort-acting antibiotic trials (mean, 2.71;SD, 1.07) and azithromycin trials (mean,2.27; SD, 0.79). Substantial interrateragreementwas reached(weighted ,0.82;95% CI, 0.79-0.85). Only 9 trials in 8 pub-lications reported adequate concealment
JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al 1737
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/ -
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
3/7
Table 1.Methodologic Quality of Included Trials
QualityScore
Concealment ofTreatment Allocation
No. inArm Antibiotic Duration, d
1-MonthDropouts, %
SubgroupData *
ReferenceNo.
Short-Acting Antibiotic4 Unclear 42 Amoxicillin 3 9.5
No 4642 Amoxicillin 10 2.32 Unclear 82 Penicillin V potassium 5 0
2 y 4781 Penicillin V potassium 10 02 Unclear 66 Penicillin V potassium 5 0
2 y 4768 Penicillin V potassium 10 02 Adequate 47 Penicillin V potassium 2 2.1
No 4856 Penicillin V potassium 7 1.93 Inadequate 30 Cefaclor 5 10
2 y 4930 Amoxicillin 10 3.33 Inadequate 131 Amoxicillin 2 9.9
No 50143 Amoxicillin 7 12.64 Unclear 47 Cefaclor 3 . . .
No 5153 Cefaclor 7 . . .3 Unclear 7 Amoxicillin 1 0
No 5210 Amoxicillin 10 05 Unclear 74 Cefaclor 5 26.2
Perforat ed eardrum 2677 Cefaclor 10 27.52 Adequate 125 Cefpodoxime proxetil 5 0.8
No 53122 Cexime 8 0.82 Adequate 242 Cefuroxime 5 39.2
No 54242 Amoxicillin 10 26.92 Adequate 242 Cefuroxime 5 39.2
No 54235 Cefuroxime 10 26.4
1 Unclear 50 Cefpodoxime proxetil 5 4 No 5550 Cefaclor 10 42 Unclear 359 Cefprozil 5 20.3
No 56349 Cefprozil 10 21.63 Adequate 200 Cefpodoxime proxetil 5 17.9
No 57200 Amoxicillin 8 162 Unclear 293 Amoxicillin 5 67.2
No# 58287 Amoxicillin 10 622 Unclear 293 Amoxicillin 5 67.2
No# 58288 Amoxicillin 10 65.6
Ceftriaxone4 Unclear 27 Ceftriaxone sodium 1 18.5
No 5935 Amoxicillin 7 124 Adequate 128 Ceftriaxone sodium 1 9.3
No 60133 Amoxicillin 10 123 Inadequate 41 Ceftriaxone sodium 1 24.3 **
No 6132 Cefaclor 10 28.13 Unclear 241 Ceftriaxone sodium 1 19.9
No 62243 Trimethoprim-sulfamethoxazole 10 15.6
Azithromycin2 Inadequate 15 Azithromycin 3 0
No 6315 Amoxicillin 10 01 Unclear 77 Azithromycin 3 0
No 6477 Amoxicillin 10 02 Unclear 105 Azithromycin 3 1.9
No 6554 Amoxicillin 10 02 Unclear 197 Azithromycin 3 2.5
2 y 66192 Amoxicillin 10 1.62 Unclear 243 Azithromycin 3 11.5
2 y 67240 Amoxicillin 10 17.52 Unclear 263 Azithromycin 5 11.4
No 68263 Amoxicillin 10 19.84 Adequate 341 Azithromycin 5 22.6
No 69336 Amoxicillin 10 23.53 Adequate 51 Azithromycin 3 7.8
No 7049 Amoxicillin 10 8.22 Unclear 125 Azithromycin 3 8.8
No 71134 Cefaclor 10 10.42 Inadequate 85 Azithromycin 5 41.2
No 7284 Amoxicillin 10 58.33 Adequate 51 Azithromycin 3 2
No 7349 Clarithromycin 10 4.1
*Subgroup data can be extracted.High dose must be taken of this antibiotic in this situation.Ellipses represent unknown.Only 1 dose was taken.
Clavulanic acid form of antibiotic.New formulation that requires twice-daily dosing.#Age group analysis, but data not present.**Three month or less dropouts.
1738 JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/ -
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
4/7
-
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
5/7
However,among1031 children treatedwith anantibioticfor 5 days and1084chil-dren treated for8 to10days,primaryout-
comes at 20 to 30 days were not signifi-cantlydifferentbetweenthe2 groups(OR,1.22; 95% CI, 0.98-1.54). The weightedmeanfailurerateat20to30dayswas15.7%(SE, 13.3%) with 5 days of treatment and12.5% (SE, 12.4%) in the long-treatmentarm. The weighted summary risk differ-ence was 2.3% (95% CI, 0.2% to 4.9%).There were no differences in secondaryoutcomes (failures, relapses, and recur-rencesduring a 3-month period)between539childrenintheshort-treatmentand515children in thelong-treatmentarms (OR,1.16;95%CI,0.90-1.50). 26,46,53,58 Similarsum-maryORswereobtainedinchildrenevalu-ated at 30 to 40 days (OR, 1.16; 95% CI,0.87-1.55) orat90days (OR, 1.16;95% CI,0.65-2.06) (Figure 1).
The summary OR for antibiotic failureat30days or less inchildrenyoungerthan2 years (n = 118) and those who were atleast2yearsold(n = 235)was0.71(95%CI,0.3-1.64) and 1.01 (95% CI, 0.53-1.94), re-spectively. 47,49 Significant differences inoutcome between5-dayand 10-day treat-mentamongchildrenyoungerthan2yearsold, but not in older children, were re-portedin anadditional trial,butnoextract-
ablesubgroupdatawerepresented. 58Inthesingle trial thatreportedoutcomedataforperforated and nonperforated ear-drums, 26 the OR for treatment failure inchildrenwithperforatedeardrums(n = 27)was3.62(95%CI,0.81-16.06)and1.06(95%CI, 0.40-2.75) in children with nonperfo-rated eardrums (n = 101).
Outcome of Ceftriaxone in the
Short-Treatment Arm. Meta-analyseswere conducted on 3 trials for primary(n = 671)59,60,62 and 2 trials for secondaryoutcomes (n = 312). 60,61 The outcomes of treatmentwithceftriaxonefor1monthorless and for 3 monthsor lesswerenot sig-nificantly different from those of treat-ment with a longer course of oral antibi-otics,withsummary ORsof 1.25 (95%CI,0.90-1.72) and of 0.91 (95% CI, 0.57-1.47),respectively.
Outcome of Azithromycin in theShort-Treatment Arm. The summaryOR for primary outcomes following 3 or5 days of treatment with azithromycin(n = 1347) in comparison to 10 days of treatment with another antibiotic(n = 1246)was1.09 (95%CI,0.86-1.38).Thesummary ORs did not change when chil-dren were treated for 3 days only (OR,1.17; 95% CI, 0.71-1.92), when childrenwereevaluatedat10to14days(OR,1.11;95%CI, 0.82-1.51),or when childrenwereevaluated at 30 days (OR, 1.02; 95% CI,0.78-1.34). The odds of treatment failurewith azithromycinwas1.92(95% CI,0.73-5.04) in children younger than 2 years(n = 138; 17.4%) and 1.34 (95% CI, 0.61-2.94) in older children (n = 656). 66,67
Sensitivity Analysis and PublicationBias. Sensitivity analyses were con-ducted for all primary outcomes up until30 days following trial entry, and sepa-rately for outcomes at a 20- to 30-dayevaluation in the 5-day short-acting anti-biotic group. Treatment failures at 30days or less were not significantly morelikely in the short- than long-treatmentarm among short-acting antibiotic trialsgrouped as (1) high-quality trials, (2) tri-als with adequate treatment allocation,and (3) trials that excluded children withrecurrent or chronic OM (Table 2). The
majority of summary ORs for primaryoutcomes at 20 to 30 days did not changeduring any of the sensitivity analyses.
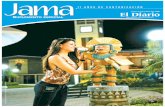
The symmetrical, inverted funnel-shaped plot of the ORs vs sample size, asshownbythewidescatteringofORsfromsmall studiesnarrowing to a peak amonglarger trials, suggested no evidence of apublication bias in the meta-analysis tri-
als (Figure 2). Using a random-effectsmodel, which accounts for trial heteroge-neity, only 1 of the summary ORs waschanged. The random-effects model wid-ened the 95% CI for the summary OR intheshort-actingantibioticgroupat8to19days, so that a 5-day course of antibioticswasnolongerstatisticallysignificantlyas-sociated withpoorer treatmentoutcomesthan a longer course.
Adverse Effects. The summary ORfor gastrointestinal side effects in theshort-acting antibiotics trials was 0.54(95%CI,0.43-0.66).AnORlessthan1wasobserved only in trials in which the shortcourse of antibiotics was compared witha 10-day course of the standard formula-tion of amoxicillin-clavulanate. 54,57,58 Oncethese were excluded,therewasno differ-ence in the likelihood of gastrointestinalside effects following a short or longcourse of antibiotics (OR, 1.13; 95% CI,0.81-1.57). Children treated with azithro-mycin were also less likely to experiencegastrointestinalside effects thanchildrentreated with a long course of antibiotics(OR, 0.26; 95% CI, 0.19-0.37), which wasmost often amoxicillin-clavulanate.
COMMENTOurmeta-analysis results indicate that
at an early evaluation point (8 to 19 days)a reductionin treatmentfrom10 to5 daysof short-actingantibioticsmay slightlyin-crease the risk of a child experiencingsignsand symptomsor relapse orreinfec-tion (OR, 1.52; 95% CI, 1.17-1.98). How-ever, by 30 days following initiation of therapy, a longer course of short-actingantibiotics was comparable to a 5-daycourse in terms of these outcomes (OR,1.22; 95% CI, 0.98-1.54). We do note thatthe latter finding is based on a summary
Table 2.Sensitivity Analyses of Primary Outcomes at 30 Days or Less and at 20 to 30 Days for Short-Acting Antibiotic Group *
DescriptionReference Nos.
of Included Trials
8- to 30-d SummaryOdds Ratio
(95% Condence Interval)Reference Nos.
of Included Trials
20- to 30-d SummaryOdds Ratio
(95% Condence Interval)All trials 26, 47, 49, 53-58 1.38 (1.15-1.66) 26, 47, 49, 54-57 1.22 (0.98-1.54)Quality score 2 26, 49, 57 1.20 (0.83-1.75) 26, 49, 57 1.20 (0.83-1.75)Quality score 2 47, 53-56, 58 1.44 (1.17-1.78) 47, 54-56 1.24 (0.93-1.64)Adequate concealment 53, 54, 57 1.14 (0.88-1.47) 54, 57 1.16 (0.88-1.52)Inadequate concealment 26, 47, 49, 55, 56, 58 1.68 (1.39-2.19) 26, 47, 49, 55, 56 1.40 (0.92-2.11)Chronic otitis media excluded 53, 55, 56 1.29 (0.76-2.20) 55, 56 1.55 (0.79-3.04)
Chronic otitis media included 26, 47, 49, 54, 57, 58 1.39 (1.15-1.70) 26, 47, 49, 54, 57 1.19 (0.93-1.51)Improved outcomes counted as failures 26, 47, 53-58 1.35 (1.14-1.59) 26, 47, 54-57 1.24 (1.01-1.54)Same antibiotic per arm 26, 47, 53, 56, 58 1.54 (1.21-1.95) 26, 47, 54, 56 1.25 (0.90-1.74)
*Five days vs 8 or 10 days or therapy.Concealment of treatment allocation.
500
101Odds Ratio
0.1
400
300
200
100
0
S a m p
l e S i z e
Figure 2.Funnel plot of the odds ratios vs samplesize for studies included in the meta-analysis of pri-maryoutcomes( 1 month), excluding1 trialwith17children and an odds ratio of 13.34.
1740 JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/ -
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
6/7
OR for which the lower limit of the CI isclose to 1. At the 8- to 19-day evaluation,the difference in risk of failure betweentreatment with 5 days vs 10 days of ashort-acting antibiotic was 7.8%. Theclinical significance of thisrisk difference,expressedas thenumberneededto treatto experience an additional failure in theshort-treatment arm (or1 dividedby theriskdifference), indicatesthat13 childrenwould require treatment with a longcourse of antibiotics to prevent 1 excessfailurefollowingtreatmentwithashortercourse.However,arecentstudysuggeststhat a 6-week evaluation period, 74 ratherthan the traditional 2-week evaluation, 75decreases the necessity of retreatingAOM without increasing complications.In our study, the risk difference at 1month following treatment dropped to2.3%,whichtranslatesinto 44children re-quiring treatmentwith a longer courseof antibiotics to prevent 1 failure followingshorter treatment. This is not likely aclinically important difference because
the 44th child with persistent symptomswill generally returnto a sourceof healthcare. Moreover,a shortenedcourseof an-tibioticsmayprotectthechildfromdevel-oping resistant microorganisms, 11,12,76-79which in our opinion outweighs the mini-mal risk of increased treatment failure, if such a risk exists at all.
Differences in outcome between theevaluations at 8 to 19 days and 20 to 30days likely reflect bias in the timing of evaluation. Children treated with a longcourse ofantibioticshadfewer days toex-perience an outcome than those treatedwith 5 days when the time to evaluation
was 8 to 19 days, as opposed to 30 days.15
Comparisonsoftreatmentoutcomeovera3-month period, although based on asmaller number of children, revealed nosignificant differences between the 2treatment regimens. The long-term com-parabilitybetweenashortandlongcourseof antibiotics is biologically plausible, onthe basis of (1) spontaneous resolution of untreatedAOM, 9,10 (2)earlyeradicationof pathogensafter 3 to5 days of treatment, 80(3)poorerpenetrationoftheantibioticintothe ear with continued administration asinflammation decreases, 81 and (4) treat-ment ofchildren without AOMbecauseof diagnostic uncertainty. 2
Potential weaknessesof meta-analysistechniques are that they incorporate ex-isting biases and introduce new biases,someofwhichhavepredicteddiscordanceof results between meta-analyses andsingle, large randomized controlled tri-als. 82,83 To minimize bias during study se-lection, we used predetermined inclusioncriteria, and most trials were assessed ina blinded fashion, although recent evi-dence suggests that blinded evaluationsare not necessary. 84 Publication bias was
assessed in our funnel plot of sample sizevs theORs andnonewasevident. 27 Usingthe validated Jadad scale to assess for bi-ases within individual trials, 19,20 the ma- jority of short-acting antibiotic trialsscored less than 3 because they were notdouble-blinded. Lack of double-blindingin trials has yielded larger estimates of treatmenteffects. 21 InAOMtrials,theab-senceofblinding maybias outcomes in fa-vor of longer treatment with antibioticsbecause parents and physicians may bemore vigilant in detecting failures in achild receiving a shorter course. 46 An in-creasedriskof treatmentfailure with a 5-daycourseof antibioticswas indeeddocu-mented among poor-quality trials in oursensitivity analyses. Less favorable out-comesin theshorter-treatment armwerealsolimited to trialswith inadequatecon-cealment of treatment allocation, consis-tent with evidence that poor conceal-ment of treatment allocation results inbiased treatment effects. 21,22 The issue of trial heterogeneity was addressed in our
groupingofantibioticsaccording tophar-macokineticprofile. 85Inaddition,thefixed-effectsmodel,which assumestrialhomo-geneity, and the random-effects model,whichincorporatesbetween-studyvaria-tion, 82 producedsimilarORsinmostoftheantibioticsubgroups.Specificinclusioncri-teria for the diagnosis of AOM were notused,butdiagnostic criteria were compa-rableacrosstrials.However,outcomecri-teria did vary among trials and changesto the definition of a successful outcomealtered the 20- to 30-day summary OR.
Most of the short-acting antibiotics inthis study are commonly prescribed in
primary practice and our sensitivityanalyses indicate that comparisons be-tween different short-acting antibioticsdid not alter treatment outcomes. Simi-lar outcomes were observed between a3- or 5-day course of azithromycin and a10-day courseof other antibiotics. Com-parability was also demonstrated be-tween ceftriaxone anda longercourseof antibiotics, although the sample size of theconsolidated trials wassmall.It is dif-ficult to support the useof azithromycinorceftriaxonebasedontheircostandcon-cern over indiscriminate use of broad-spectrum antibiotics. 86 Ceftriaxones in-tramuscularmodeof administrationmayfurtherlimititsrole. 87 While antibioticusein children with AOM may increase theincidenceof diarrhea andvomiting, 10 wedid not find that a shortened course of antibiotics decreased the likelihood of gastrointestinal effects, except whencompared with a longercourseof amoxi-cillin-clavulanate.
Our findings can be safely applied tochildren who present to ambulatory caresettings with uncomplicated AOM, withsomenoteworthyexceptions.These find-
ings do not apply to children with under-lyingdiseaseandpotentiallychildrenwithrecurrentor chronic OM. Treatment fail-ure at less than 1 month was not morelikely with a 5-day course of antibioticsonce children with chronic or recurrentOM were excluded. Subgroup samplesizes were too small to provide a reliableestimate of the risk of treatment failurewith a shortened course of antibiotics inchildren younger than 2 yearsorchildrenwith perforated eardrums. In addition,while our meta-analysis included data onchildren from various populations, it re-mainsunprovenwhetherour findingscanbe extrapolated to other high-risk chil-dren. 5,88
The meta-analysis results support theuseof 5 days ofa short-actingantibiotic inuncomplicatedAOM in theevent that cli-nicians and parents decide to use antibi-otics. Treatmentwith a shortenedcourseof antibiotics has the potential to greatlyreduceantibioticuse in regionswhere 10days of treatment is considered the stan-
dard, with anticipated cost savings, im-provedcompliance, anddecreasedantibi-otic resistance. 15
Support for this work was provided by the Cana-dian Cochrane Network and by the Department of Community Health Sciences at the University of Manitoba. Thanksto Mary Cheang, MSc,for statisti-cal assistance.
References
1. Klein JO,Teele DW,Rosner BA,et al.Epidemi-ology of acute otitis media in Boston children frombirth to seven years of age. In: Lim DJ, BluestoneCD, Klein JO, Nelson JD, eds. Recent Advances inOtitis Media With Effusion: Proceedings of theFourth International Symposium. Toronto,Canada: BC Decker; 1988:6-8.2. Froom J, Culpepper L, Grob P, et al. Diagnosis
andantibiotictreatment of acuteotitismedia. BMJ.1990;300:582-586.3. McCaigLF, Hughes JM. Trends in antimicrobialdrug prescribing among office-based physicians.JAMA. 1995;273:214-219.4. Stool SE, Field MJ. The impact of otitis media.Pediatr Infect Dis J. 1989;8:S11-S14.5. Berman S. Otitis media in developing countries.Pediatrics. 1995;96:126-131.6. Mygind N, Meistrup-Larsen KI, Thomsen J,Thomsem VF, Josefsson K, Sorensen H. Penicillinin acute otitismedia. Clin Otolaryngol. 1981;6:5-13.7. Burke P, BainJ, Robinson D, Dunleavey J. Acutered ear in children. BMJ. 1991;303:558-562.8. Van Buchem FL, Dunk JHM, Vant Hof MA.Therapy of acute otitis media: myringotomy, anti-biotic or neither? Lancet. 1981;2:883-887.9. RosenfeldRM,VertreesJE, CarrJ, etal. Clinicalefficacy of antimicrobial drugs for acute otitis me-dia. J Pediatr. 1994;124:355-367.
10. DelMar C, Glazziou P, Hayem M. Areantibiot-ics indicated as initial treatment for children withacute otitis media. BMJ. 1997;314:1526-1529.11. Cohen ML. Epidemiology of drug resistance.Science. 1992;257:1050-1055.12. Murray BE. Can antibiotic resistance be con-trolled? N Engl J Med. 1994;330:1229-1230.13. Paradise JL. Managing otitis media: a time forchange. Pediatrics. 1995;96:712-715.14. Paradise JL. Short-course antimicrobial treat-ment foracuteotitismedia: notbest forinfants andyoung children. JAMA. 1997;278:1640-1642.15. Pichichero ME, Cohen R. Shortened course of antibiotic therapy for acute otitis media, sinusitis,and tonsillopharyngitis. Pediatr Infect Dis J. 1997;16:680-695.
JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al 1741
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/ -
8/6/2019 JAMA-1998-Kozyrskyj-1736-42[1]
7/7
16. GregoireG, DerderianF, Le LorierJ. Selectingthelanguageof thepublications included in a meta-analysis. J Clin Epidemiol. 1995;48:159-163.17. Dickersin K, Scherer R, Lefebvre C. Identify-ing relevant studies for systematic reviews. BMJ.1994;309:1286-1291.18. Cook DJ, Sackett DL, Spitzer WO. Methodo-logic guidelines for systematic review of random-ized control trials in health care from the PotsdamConsulation. J Clin Epidemiol. 1995;48:161-171.19. Moher D, Jadad AR, Nichol G, Penman M, Tug-well P, Walsh S. Assessingthe qualityof randomizedcontrolled trials. Control Clin Trials. 1995;16:62-73.20. JadadAR,MooreR,CarrollD,etal.Assessingthequalityof reportsof randomizedclinicaltrials:is blind-ing necessary? Control Clin Trials. 1996;17:1-12.21. SchulzKF,ChalmersI,HayesR,AltmanDG.Em-pirical evidence of bias. JAMA. 1995;273:408-412.22. Chalmers TC, CelanoP, Sacks HS,Smith H Jr.Bias in treatment assignment in controlled clinicaltrials. N Engl J Med. 1983;309:1358-1361.23. Landis B, Koch GG. The measurement of ob-server agreement for categorical data. Biometrics.1977;3:159-174.24. Kaleida PH, Casselbrant ML, Rockette HE, etal. Amoxicillin or myringotomy or both for acuteotitis media. Pediatrics. 1991;87:466-474.25. Appelman CLM, Claessen QPL, Touw-OttenFWMM, Hordijk GJ, de Melker RE. Co-amoxiclavin recurrent acute otitis media: placebo controlledstudy. BMJ. 1991;303:1450-1452.26. Hendrickse WA, Kusmiesz H, Shelton S, Nel-son JD. Five vs ten days of therapy for acute otitismedia. Pediatr Infect Dis J. 1988;7:14-23.27. OxmanA. Preparing andmaintainingsystematicreviews. In: Cochrane CollaborationHandbook. Ox-ford, England: The Cochrane Collaboration; 1995.28. Laupacis A, SackettDL, RobertsRS. An assess-mentofclinicallyusefulmeasuresoftheconsequencesof treatment. N EnglJ Med. 1988;318:1728-1733.29. ThompsonSG. Why sources of heterogeneity inmeta-analysis should be investigated? BMJ. 1994;309:1351-1355.30. DerSimonianR, LairdN. Meta-analysis in clini-cal trials. Control Clin Trials. 1986;7:177-188.31. SticklerGB,McBeanJB.Thetreatmentofacuteotitis media in children. JAMA. 1964;187:85-89.32. Rubenstein MM, McBean JB, Hedgecock LD,SticklerGB.Thetreatmentofacuteotitismediainchil-dren,III:athirdclinicaltrial. AJDC. 1965;100:308-313.33. Stickler GB, Rubenstein MM, McBean JB,Hedgecock LD, Hugstad A, Griffing T. Treatmentofacuteotitis mediain children,IV:a fourthclinicaltrial. AJDC. 1967;114:123-130.34. Jacobson JA, Metcalf TJ, Parkin JL, Wener-stromLG. Evaluationof cefaclor and amoxycillininthetreatmentofacuteotitismedia. PostgradMedJ.1979;55(suppl 4):39-41.35. HarrisonCJ,ChartrandSA,PichicheroME.Mi-crobiologicandclinicalaspectsof a trialof oncedailycefixime compared with twice daily cefaclor fortreatment of acute otitis media in infants and chil-dren. Pediatr Infect Dis J. 1993;12:62-69.36. Johnson CE,Carlin SA,SuperDM, et al.Cefix-ime compared with amoxicillin for treatment of acute otitis media. J Pediatr. 1991;119:117-122.37. MurphJR,DusdiekerLB, BoothB, MurphWE.Is treatment of acute otitis media with once-a-dayamoxicillin feasible? Clin Pediatr. 1993;32:528-534.38. Spencer RC, Hannington J, Fraser S, Mason T.Cefpodoxime proxetil vs co-amoxiclav in the treat-ment of acute infections of theear, nose andthroat in
children-amulticentrerandomizedstudy.In:Programand abstracts of the 18th International Congress of Chemotherapy; June 27-July 2, 1993; Stockholm,Sweden. Abstract 851.39. MacLoughlin GJF, Barreto DG, de la Torre C,Pinetta EA, del Castilllo F, Palma L. Cefpodoximeproxetilsuspension comparedwith cefaclor suspen-sionfor treatmentof acuteotitismedia in paediatricpatients. JAntimicrobChemother. 1996;37:565-573.40. Jenner PN, Tierney HE, Carle WK. A generalpractice study ofa new approachto the use ofantibi-oticsin thetreatment ofacuteotitismediain childrenagedthreeandover. BrJClinPract. 1987;41:820-826.41. Gehanno P, Taillebe M, Denis P, et al. Short-course cefotaxime compared with five-day co-amoxyclavin acute otitismedia in children. J Anti-
microb Chemother. 1990;26(suppl A):29-36.42. Mandel EM, Casselbrant ML, Rockette HE,Bluestone CD, Kurs-Lasky M. Efficacy of 20- ver-sus 10-day antimicrobial treatment for acute otitismedia. Pediatrics. 1995;96:5-13.43. Scott HV, Pannowitz D, Ketelbey JW. Cefix-ime: clinical trialagainst otitismedia and tonsillitis.N Z Med J. 1990;103:25-26.44. ODoherty B. An open comparative study of azithromycinversuscefaclorin thetreatmentof pa-tientswith upper respiratorytractinfections. JAn-timicrob Chemother. 1996;37(suppl C):71-81.45. Varsano I, Volovitz B,HorevZ, et al.Single IMdose of ceftriaxone (CRO) compared to 10 daysamoxicillin-clavulanate augmentin (AUG) fortherapy ofacuteotitis media(AOM)in children.Pa-per presented at: Sixth International Congress forInfectiousDisease,Session117; April1994; Prague,Czech Republic. Abstract 1059.46. Chaputde SaintongueDM, LevineDF, TempleSavage I, et al. Trial of three-day and ten-daycourses of amoxycillin in otitis media. BMJ. 1982;284:1078-1081.47. IngvarssonL, LundgrenK. Penicillintreatmentof acute otitis media in children. Acta Otolaryngol.1982;94:283-287.48. Meistrup-Larsen KI, Sorensen H, Johnsen NJ,ThomsenJ, Mygind N,Sederberg-OlsenJ. Twover-sus seven days penicillin treatment for acute otitismedia. Acta Otolaryngol. 1983;96:99-104.49. Ploussard JH. Evaluation of five days of cefa-clor vsten days ofamoxicillintherapyin acuteotitismedia. Curr Ther Res. 1984;36:641-645.50. Bain J, Murphy E, Ross F. Acute otitis media.Br Med J Clin Res Ed. 1985;291:1243-1246.51. JonesR,BainJ.Three-dayandseven-daytreat-ment in acute otitismedia: a double-blindantibiotictrial. J R Coll Gen Pract. 1986;36:356-358.52. Puczynski MS, Stankiewicz JA, OKeefe JP.Single dose amoxicillin treatment of acute otitismedia. Laryngoscope. 1987;97:16-18.53. Boulesteix J, Dubreuil C, Moutot M, Rezvani Y,Rosembaum.Cefpodoximeproxetil 5 joursversusce-fixime8 jours,dansle traitementdes otitesmoyennesaigues de lenfant. Med Mal Infect. 1995;25:534-539.54. GoochWM, Blair E,Puopolo A, etal. Effective-ness of five days of therapy with cefuroxime axetilsuspension for treatment of acute otitis media. Pe-diatr Infect Dis J. 1996;15:157-164.55. Adam D. Five-day therapy with cefpodoximeversus ten-day treatment with cefaclor in infantswith acute otitis media. Infection. 1995;23:398-399.
56. Kafetzis DA, Astra H, Mitropoulos L. Five-dayversusten-daytreatmentofacuteotitismediawithce-fprozil. EurJ ClinMicrobInfectDis. 1997;16:283-286.57. Cohen R, de La Rocque F, Boucherat M et al.Etuderandomiseecefpodoximeproxetil5joursver-sus amoxicilline-acide calvulanique 8 jours dans letraitment de lotite moyenne aiguede lenfant. MedMal Infect. 1997;27:596-602.58. Hoberman A, Paradise JL, Burch DJ, et al.Equivalent efficacy and reduced occurrence of di-arrhea froma new formulationof amoxicillin/clavu-lanate potassium (Augmentin) for treatment of acute otitis media in children. Pediatr Infect Dis J.1997;16:463-470.59. VarsanoI,FrydmanM,AmirJ,AlpertG.Singleintramuscular dose of ceftriaxone as compared to7-day amoxicillin therapy for acute otitis media inchildren. Chemotherapy. 1988;34(suppl 1):39-46.60. GreenSM, RothrockSG. Single-doseintramus-cular ceftriaxone for acute otitis media in children.
Pediatrics. 1993;91:23-30.61. Chamberlain JM, Boenning DA, Waisman Y,Ochsenschlager DW, Klein BL. Single-dose ceftri-axone versus 10 days of cefaclor for otitis media.Clin Pediatr. 1994;33:642-646.62. Barnett ED, Teele DW, Klein JO, Cabral HJ,Kharasch SJ. Comparison of ceftriaxone and tri-methoprim-sulfamethoxazoleforacute otitismedia.Pediatrics. 1997;99:23-28.63. PetalozzaG, CioceC, Facchini M. Azithromycinin upper respiratory tract infections clinical trial inchildren withotitis media. ScandJ InfectDis. 1992;83:22-25.64. Mohs E, Rodriguez-Solares A, Rivas E, HoshyZE.Acomparativestudyofazithromycinandamoxy-cillin in paediatric patients with acute otitis media.
J Antimicrob Chemother. 1993;31(suppl E):73-79.65. Daniel RR. Comparison of azithromycin and co-amoxiclavin thetreatment ofotitismediainchildren.J Antimicrob Chemother. 1993;31(suppl E):65-71.66. Schaad UB. Multicentre evaluation of azithro-mycinincomparisonwithco-amoxiclavforthetreat-ment ofacuteotitis mediain children. J AntimicrobChemother. 1993;31(suppl E):81-88.67. Principi N. Multicentre comparative study of the efficacy and safety of azithromycin comparedwith amoxicillin/clavulanic acid in the treatment of paediatric patients with otitis media. Eur J ClinMicrobiol Infect Dis. 1995;14:669-676.68. Khurana CM. A multicenter, randomized, openlabel comparison of azithromycin and amoxicillin/ clavulanate in acuteotitis mediaamong children at-tending day care or school. Pediatr Infect Dis J.1996;15(suppl):S24-S29.69. McLinn S. A multicenter, double blindcompari-son of azithromycin and amoxicillin/clavulanate forthe treatment of acute otitis media in children. Pe-diatr Infect Dis J. 1996;15(suppl):S20-S23.70. Arguedas A, Loaiza C, Herrara M, Mohs E.Comparative trial of 3-dayazithromycin versus 10-day amoxycillin/clavulante potassium in the treat-ment of children with acute otitis media with effu-sion. Int J Antimicrob Agents. 1996;6:233-238.71. RodriguezA. An open study to compare azithro-mycin withcefaclorin thetreatmentof children withacute otitis media. J Antimicrob Chemother. 1996;37(suppl C):63-69.72. Aronovitz G. A multicenter, open label trial of azithromycinvsamoxicillin/clavulanatefortheman-agement of acute otitis media in children. Pediatr Infect Dis J. 1996;15(suppl):S15-S19.73. Arguedas A, Loaiza C, Rodriguez F, HerreraML et al. Comparative trial of 3 days of azithromy-cin versus 10 days of clarithromycin in the treat-ment of children with acute otitis media with effu-sion. J Chemother. 1997;9:44-50.74. Kurbasci M, Jones VF, Badgett JT, Thomas A.Two-weekvssix-week followupforacuteotitismedia[abstract]. ArchPediatr Adolesc Med. 1996;150:19.75. BermanS,ByrnsPJ,BondyJ,etal.Otitismedia-related antibiotic prescribing patterns, outcomes,and expenditures in a pediatric medicaid popula-tion. Pediatrics. 1997;100:585-592.76. Harrison CJ, Marks MI, Welch DF. Microbiol-ogyof recently treated acuteotitis mediacomparedwith previouslyuntreatedacute otitismedia. Pedi-atr Infect Dis J. 1985;4:641-646.77. Faden H,BernsteinJ, BrodskyL, etal. Effect of
prior antibiotic treatment on middle ear disease inchildren. AnnOtol Rhinol Laryngol. 1992;101:87-91.78. MillsR, UttleyA, McIntyreM. Relationship be-tween acute suppurative otitis media and chronicsecretory otitis media: role of antibiotics. J R SocMed. 1984;77:754-757.79. Guillemot D, Carbon C, Balkau B, et al. Lowdosage and long treatment duration of -lactam.JAMA. 1997;279:365-370.80. Howie VM,PloussardJH. TheIn Vitro Sensi-tivity Testbacteriology of middle ear exudate.Pediatrics. 1969;44:940-944.81. Canafax DM,Giebink GS. Clinical andpharma-cokinetic basis for the antimicrobial treament of acute otitis media. Otolaryngol Clin North Am.1991;24:859-874.82. Borzak S, Ridker PM. Discordance betweenmeta-analyses and large-scale randomized, con-trolled trials. Ann Intern Med. 1995;123:873-877.83. Egger M,Smith GD, Schneider M,et al. Bias in
meta-analysis detected by a simple, graphical test.BMJ. 1997;315:629-634.84. Berlin JA. Does blinding of readers affect theresults of meta-analyses? Lancet. 1997;350:185-186.85. SchentagJJ. Antibiotictreatmentof acuteotitismediainchildren:dosingconsiderations. PediatrIn- fect Dis J. 1995;14:S30-S33.86. Rosenfeld RM. An evidence-based approach toapproach to treating otitis media. Pediatr ClinNorth Am. 1996;43:1165-1181.87. EppesSC, Klein JD,LewisLL.Ceftriaxoneforacute otitis media. Pediatrics. 1997;100:157.88. Boswell JB, Nienhuys TG. Patterns of persis-tent otitismediain thefirstyearof lifein aboriginalandnon-aboriginalinfants. AnnOtolRhinolLaryn- gol. 1996;105:893-900.
1742 JAMA, June 3, 1998Vol 279, No. 21 Treatment of Acute Otitis MediaKozyrskyj et al
1998 American Medical Association. All rights reserved.at University of Greenwich on July 20, 2011 jama.ama-assn.orgDownloaded from
http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/http://jama.ama-assn.org/