ITI 1 Immunity, Transplantation and INFECTION Infectious disease are directly responsible for a...
22
1 ITI Immunity, Transplantation and INFECTION • Infectious disease are directly responsible for a major fraction of global mortality. • Microbes now clearly implicated in the etiology of many other, chronic diseases, as well. • Major new diseases have recently emerged. Infectious diseases looming as biological weapons. New tools are in hand. New understanding of host-pathogen systems. Stanford and the U.S. have a responsibility to build partnerships with developing countries. Context:
-
date post
20-Dec-2015 -
Category
Documents
-
view
221 -
download
6
Transcript of ITI 1 Immunity, Transplantation and INFECTION Infectious disease are directly responsible for a...

1
ITIImmunity, Transplantation and INFECTION
• Infectious disease are directly responsible for a major fraction of global mortality.
• Microbes now clearly implicated in the etiology of many other, chronic diseases, as well.
• Major new diseases have recently emerged.
Infectious diseases looming as biological weapons.
New tools are in hand.
New understanding of host-pathogen systems.
Stanford and the U.S. have a responsibility to build partnerships with developing countries.
Context:

2
ITI
1. Infectious disease are directly responsible for a major fraction of global mortality.

3
ITI1.1 Leading causes of death globally, 19991.1 Leading causes of death globally, 1999
• 1 Ischaemic heart disease• 2 Cerebrovascular disease• 3 Acute lower respiratory infections• 4 HIV/AIDS• 5 Chronic obstructive pulmonary disease• 6 Perinatal conditions• 7 Diarrhoeal diseases• 8 Tuberculosis
• 11 Malaria
12.7
9.9
7.1
4.8
4.8
4.2
4.0
3.0
1.9
Source: The World Health Report 2000, WHO
Rank % of total
N~55M

4
ITI1.2 Leading causes of death in Africa, 19991.2 Leading causes of death in Africa, 1999
• 1 HIV/AIDS• 2 Acute lower respiratory infections• 3 Malaria• 4 Diarrhoeal diseases• 5 Perinatal conditions• 6 Measles• 7 Tuberculosis• 8 Cerebrovascular disease• 9 Ischaemic heart disease• 10 Maternal conditions
20.6
10.3
9.1
7.3
5.9
4.9
3.4
3.2
3.0
2.4
Source: The World Health Report 2000, WHO
Rank % of total

5
ITI1.3 Infectious diseases are responsible for a majority of deaths in children, worldwide.

6
ITI
2. Major new diseases have recently emerged.

7
ITI2.1 Many “New” Infectious Agents/Diseases
Have Been Identified Since 1975.
1976 Cryptosporidium parvum (Cryptosporidiosis)
1976 Legionella (Legionnaire’s Disease)
1976 Ebola Virus (Ebola)
1982 E. coli O157 (lethal food poisoning)
1982 Borrelia burgdorferi (Lyme Disease)
1983 HIV (AIDS)
1983 Helicobacter pylori (peptic ulcers)
1989 Hepatitis C (nonA-nonB Hepatitis)
1992 Vibrio cholerae 0139 (new, virulent serotype of Cholera)
1993 Four Corners/Sin Nombre Virus (Hantavirus Pulmonary Syndrome)
1995 Human Herpesvirus 8 (Kaposi’s Sarcoma)
1996 Prions (variant Creutzfeld-Jacob Disease = “Mad Cow” in humans)
1997 H5N1 Influenza virus (Direct bird to human, super-virulent Flu)
1999 West Nile Virus (in N. America - Encephalitis)
2003 SARS coronavirus (SARS)

8
ITI
2.2 HIV is Reversing Hard-Won Improvements in Life Expectancy in many African Countries.
South-Africa
35
40
45
50
55
60
65
1950-55 1955-601960-651965-701970-751975-801980-851985-901990-951995-00
Lif
e e
xp
ecta
ncy
at
bir
th,
in y
ears
Botswana
Uganda
Zambia
Zimbabwe
Source: United Nations Population Division, 1998

9
ITI
3. Microbes now clearly implicated in the etiology of many chronic diseases.

10
ITI3.1 Microbes and Cancer.
•Human papilloma virus and cervical carcinoma.
•Hepatitis B and C viruses and hepatocellular carcinoma.
•Helicobacter and gastric cancer.
•Schistosoma and bladder cancer.

11
ITI3.2 Microbes and Allergy.
Hygiene hypothesis (“idle hands are the devil’s plaything”):
elimination of certain infections leads to inappropriate
immune response to environmental materials.

12
ITI3.3 Microbes and Autoimmunity.
Microbes may be triggers of an immune response to “self”.

13
ITI
4. New tools are in hand.

14
ITI4.1 New tools (many developed here):
•‘omics of the pathogens, vectors and hosts.
•Methods for engineering each.
•HUGE increase in our understanding of the immune system
and pathogen systems.
•High throughput methods for analysis of host and pathogen.
•Major developments in imaging.

15
ITI
5. We have a new understanding of host-pathogen systems.

16
ITI5.1 Microbial ecology in and out of the host.
•We are hosts for a diverse community of microbes.•More microbial cells than human cells in humans.•More microbial genes than human genes in humans.•Much crucial metabolism occurs in the microbes.•Natural keep “unnatural” at bay.•Environmental changes create new opportunities for
infection.

17
ITI6. Questions to be addressed
on the Infection side of ITI:
•What factors lead to the emergence of new infectious diseases in humans?•How do microbial infections lead to chronic disease?•How does the interplay of complex microbial populations contribute to this? •What is the interplay of host and microbial genetics?•How can immunity be down-modulated to accept a transplanted organ but not infection?•How can vaccines and immune therapy be made more effective; e.g., for complex diseases? •How can immunity be stimulated in the very young or old?

18
ITI
• Many world leaders in component areas. Many more studying diseases with infectious
etiologies. A Vaccine Center has already been established. Stanford is a major power in genetics, ‘omics,
imaging, immune monitoring, etc.
7. Why Stanford?

19
ITI
• Development of novel vaccines in and for developing countries (e.g., rotavirus); Harry Greenberg, Gastroenterology.
• Helicobacter and its association with gastric (up) and esophageal (down) cancer. Julie Parsonnet, Infectious Diseases and Stanley Falkow, Microbiology and Immunology.
• Cytomegalovirus association with cardiovascular disease; Ed Mocarski, Microbiology and Immunology, Hannah Valantine & John Cooke, Medicine and Dave Lewis, Pediatrics.
• Development of model host-pathogen systems; Man Wah Tan, Genetics and Brendan Bohannan, Biological Sciences.
• Infection signatures (including smallpox); David Relman, Infectious Diseases and Pat Brown, Biochemistry.
• Molecular mimicry of immune modulators by pathogens (e.g., viral IL6). Chris Garcia, Microbiology and Immunology.
And, finally, some examples of what’s happening now at Stanford.

20
ITI

21
ITI
Slide 2Slide 2Slide 2
36-54k
120-180k
30-40k180-280k
0.7-1k
43-67k
3000-3400k
610-1100k
150-270k
New infections with HIV in 2003.Total: 4.2 - 5.8M
Source: WHO
22
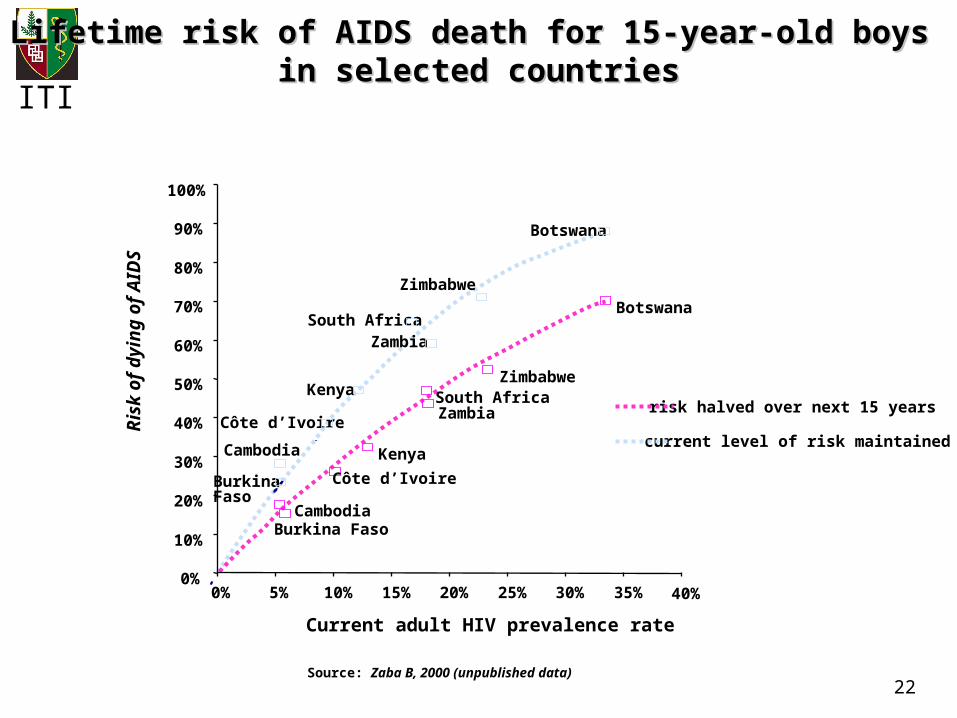
ITI
Lifetime risk of AIDS death for 15-year-old boys Lifetime risk of AIDS death for 15-year-old boys in selected countriesin selected countries
Source: Zaba B, 2000 (unpublished data)
Current adult HIV prevalence rate
Burkina Faso
Cambodia
Côte d’Ivoire
Kenya
South AfricaZambia
Zimbabwe
Botswana
Burkina FasoCambodia
Côte d’Ivoire
Kenya
South AfricaZambia
Zimbabwe
Botswana
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0% 5% 10% 15% 20% 25% 30% 35% 40%
Ris
k o
f d
yin
g o
f A
IDS
current level of risk maintained
risk halved over next 15 years

![Bioactive Powerpoint Microbes fighting microbes [Read-Only]](https://static.fdocuments.net/doc/165x107/625e85126147534db333a997/bioactive-powerpoint-microbes-fighting-microbes-read-only.jpg)