INTRODUCTION - HuffPostbig.assets.huffingtonpost.com/clayotn.pdf · He is sentenced to death, ......
20
1 IN THE UNITED STATES DISTRICT COURT EASTERN DISTRICT OF MISSOURI Cecil Clayton, ) ) Plaintiff, ) ) v. ) ) No. ____________ ) GEORGE A. LOMBARDI, ) Director, Missouri Department of ) Corrections, ) ) TROY STEELE, ) Warden, Eastern Reception Diagnostic ) And Correctional Center ) ) Defendants. ) COMPLAINT UNDER 42 U.S.C. §1983 Plaintiff Cecil Clayton, scheduled to be executed on March 17, 2015, seeks both emergency and permanent relief, requesting this Court declare and enforce his rights under the Eighth and Fourteenth Amendments to the United States Constitution and issue an injunction under 42 U.S.C. §1983 commanding defendants not to carry out any lethal injection on Mr. Clayton because Missouri’s execution protocol and procedures will lead to a prolonged and excruciating execution because of substantial risks unique to Mr. Clayton. INTRODUCTION Cecil Clayton is seventy-four years old and is missing a large portion of his frontal lobe as a result of a sawmill accident. He has dementia, major depression, and a history of psychosis. Three experts have opined that Mr. Clayton is legally incompetent. His IQ Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 1 of 20 PageID #: 1
-
Upload
nguyenkiet -
Category
Documents
-
view
219 -
download
0
Transcript of INTRODUCTION - HuffPostbig.assets.huffingtonpost.com/clayotn.pdf · He is sentenced to death, ......

1
IN THE UNITED STATES DISTRICT COURT EASTERN DISTRICT OF MISSOURI
Cecil Clayton, )
) Plaintiff, )
) v. )
) No. ____________ )
GEORGE A. LOMBARDI, ) Director, Missouri Department of ) Corrections, ) ) TROY STEELE, ) Warden, Eastern Reception Diagnostic ) And Correctional Center )
) Defendants. )
COMPLAINT UNDER 42 U.S.C. §1983
Plaintiff Cecil Clayton, scheduled to be executed on March 17, 2015, seeks both
emergency and permanent relief, requesting this Court declare and enforce his rights
under the Eighth and Fourteenth Amendments to the United States Constitution and issue
an injunction under 42 U.S.C. §1983 commanding defendants not to carry out any lethal
injection on Mr. Clayton because Missouri’s execution protocol and procedures will lead
to a prolonged and excruciating execution because of substantial risks unique to Mr.
Clayton.
INTRODUCTION
Cecil Clayton is seventy-four years old and is missing a large portion of his frontal
lobe as a result of a sawmill accident. He has dementia, major depression, and a history
of psychosis. Three experts have opined that Mr. Clayton is legally incompetent. His IQ
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 1 of 20 PageID #: 1

2
and adaptive deficits meet the standards for a finding of intellectual disability, formerly
known as mental retardation. The issue of his competence to be executed is currently
before the Missouri Supreme Court in a separate action under Rule 91. State ex rel.
Clayton v. Griffith, No. SC94841. This action addresses the issue that even if Mr. Clayton
were to be found competent to be executed, he is still subject to cruel and unusual
punishment because his brain injury and resulting confusion will subject him to unusual
and unnecessary pain and suffering during the execution process.
Under the current practice of the Missouri Department of Corrections, the drug
used to cause death is pentobarbital. However, prior to the administration of the
pentobarbital, it has been the practice of the Missouri Department of Corrections to offer
and administer midazolam and valium to the prisoner, ostensibly to mitigate the pain and
anxiety of the execution process. According to Board Certified Anesthesiologist Dr.
Mark Heath, whose affidavit is attached as Exhibit 30, beginning at Appendix p. A98,
Mr. Clayton’s extensive brain damage renders him unable to competently decide whether
to accept the corrections department’s ostensible offer of midazolam and valium as a
precursor to its protocol. These impairments make it impossible for him to rationally
choose whether to accept midazolam prior to his execution.
Mr. Clayton’s brain damage also significantly elevates the risk of an atypical
reaction to the midazolam and valium, causing Mr. Clayton to become agitated and
confused and to decompensate. In such a state, there is a heightened likelihood that
obtaining intravenous access will be very difficult. However, withholding from Mr.
Clayton the choice of accepting a sedative as he faces his death simply because of his
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 2 of 20 PageID #: 2

3
disability would violate Mr. Clayton’s right equal protection of the law as well as his
right to be free from cruel and unusual punishment.
Moreover, given Mr. Clayton’s brain damage, an underdose of pentobarbital—
made more likely by Missouri’s use of compounding pharmacies instead of FDA-
approved drugs—heightens the risk that Mr. Clayton will survive the execution, but only
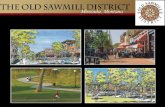
exist in a permanent vegetative state. In sum, Mr. Clayton’s severe brain damage, where
he is missing one fifth of his frontal lobe, is undisputable.
Image of Mr. Clayton’s Brain, Ex. 16.
Mr. Clayton’s brain damage and resultant dementia also render his execution cruel
and unusual punishment. Mr. Clayton’s claims rest not on the inherent dangers of
Missouri’s execution protocol, or on the inherent risks in the use of compounded drugs
generally, but on the unique facts of Mr. Clayton’s medical condition.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 3 of 20 PageID #: 3

4
JURISDICTION AND VENUE
1. Jurisdiction is conferred by 28 U.S.C. §1331 and §1343, which provide for
original jurisdiction of this Court in suits based respectively on federal questions and
authorized by 42 U.S.C. §1983, which provides a cause of action for the protection of
rights, privileges or immunities secured by the Constitution of the United States.
Jurisdiction is further conferred by 28 U.S.C. §2201 and §2202, which authorize actions
for declaratory and injunction relief.
2. Venue is proper in the Eastern District of Missouri under 18 U.S.C.
§1391(b)(1)-(3) in that defendant Steele resides in the territorial jurisdiction of this
district, and defendant Steele’s decisions regarding Missouri’s execution protocol are
made within this Court’s territorial jurisdiction, and Mr. Clayton’s execution, if it occurs,
will occur in this Court’s territorial jurisdiction.
PARTIES
3. Plaintiff Cecil Clayton is a resident of the State of Missouri and presently
resides at Eastern Reception Diagnostic and Correctional Center, Bonne Terre, Missouri.
He is sentenced to death, and is scheduled to die by lethal injection on March 17, 2015.
Mr. Clayton is presently incompetent to utilize the Department of Corrections grievance
procedure.
4. Defendant George Lombardi is the director of the Missouri Department of
Corrections. His office is located at 2729 Plaza Drive, Jefferson City, Missouri. Mr.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 4 of 20 PageID #: 4

5
Lombardi is sued in his official capacity. Mr. Lombardi, by Mo. Rev. Stat. §536.720, has
overall responsibility for carrying out the execution of Mr. Clayton.
5. Defendant Troy Steele is the warden of Eastern Reception Diagnostic and
Correctional Center (ERDCC), Bonne Terre, Missouri. He is sued in his official capacity.
Because Mr. Clayton’s execution is scheduled to occur at ERDCC, Mr. Steele has
immediate responsibility for the execution.
6. All actions of defendants Lombardi and Steele are taken under color of state
law.
FACTUAL BACKGROUND
A. A Sawmill Injury Caused Mr. Clayton Severe Brain Damage and Related Impairments, Including dementia. 7. Mr. Clayton suffered a head injury as a result of a sawmill accident in 1972
when he was 32 years old. Clayton v. State, 63 S.W.3d 201, 204 (Mo. banc 2001). A
piece of wood broke off the log he was working on and pierced his head. The piece
became imbedded inside his skull and could only be removed surgically. Due to his brain
injury, Mr. Clayton lost 7.7 percent of the brain, which equaled 20 percent of the frontal
lobe. As a result, a defense expert testified at trial that Mr. Clayton was incapable of
deliberating or otherwise coolly reflecting on a murder when agitated. Although Mr.
Clayton spent a considerable amount of time recuperating in the hospital after the
accident, he did not receive any long-term therapy.
8. Mr. Clayton desperately sought help. Medical and mental health records
document Mr. Clayton’s attempts to obtain help for his psychiatric issues resulting from
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 5 of 20 PageID #: 5

6
the accident, which included: anxiety and nervousness, depression, irritability and
agitation, hallucinations and delusions, difficulty with impulse control, paranoia, and
confusion. (Ex. 6, 7, 8, 10, 11, 12, 13, 14). The records list various medications
prescribed to Mr. Clayton (including Phenobarbital, Triavil, Dilantin, Thorazine) . (Ex.
10, 11, 13, 15).
9. Five years after the accident, in 1978, a doctor treating Mr. Clayton found that
his “basic neurologic problem is stable and would not be expected to improve.” (Ex. 9).
Another doctor who saw Mr. Clayton in 1979 noted that “He has severe ideas of
reference and borderline paranoid delusions. At present he is disabled for any type of
gainful employment and is just barely making it outside of an institution.” (Ex. 8,
emphasis added). In 1983, testing completed in connection with social security disability
placed Mr. Clayton in the range of Intellectual Disability, revealing a full scale score of
76 and a memory quotient of 62. His 1983 testing put him at a fourth grade reading level
and a third grade spelling level. (Ex. 12, emphasis added). In 1984, yet another doctor
opined that Mr. Clayton was “totally disabled.” (Ex. 14).
B. Mr. Clayton’s mental impairments increasingly disable him.
10. Since his arrest and sentencing, Mr. Clayton’s mental capacity has continued
to deteriorate. In 2004, IQ tests administered by a clinical psychologist for the Bureau of
Prisons revealed a full scale score of 71. Testing further revealed that Mr. Clayton’s
reading level was that of a fourth grade child. The psychologist who performed the
testing believed, “His current WAIS-III score of 71 likely reflects a decrease in
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 6 of 20 PageID #: 6

7
intellectual efficiency secondary to the traumatic brain injury.” Ex. 20, p. 20.
Neuropsychological testing “results indicate severe executive dysfunction.” Specifically,
“During a simpler test of concept formation, the Wisconsin Card Sorting Test. He was
unable to complete even one category correctly. Rather, he perseverated on an incorrect
response 125 times in a row, despite feedback that his responses were incorrect. This
score is considered severely impaired.” Ex. 20, pp. 22-23. (Emphasis added.)
11. Tasked by the district court with administering a competency evaluation,
government psychologists observed Mr. Clayton over the course of months at the United
States Medical Center for Federal Prisoners in Springfield, Missouri. Dr. Lea Ann
Preston presented a report to the district court in which she concluded that Mr. Clayton
was not competent to proceed in habeas. (Ex. 20). Dr. Preston found that “Mr. Clayton’s
tangential speech, impaired judgment, and impaired reasoning abilities, will negatively
affect his ability to communicate effectively with his counsel, testify relevantly, and make
rational decisions regarding his habeas proceedings.” (Ex. 20, p. 32, emphasis added).
Dr. Preston noted that, since the accident, Mr. Clayton had auditory and visual
hallucinations and believed that sometimes Satan spoke to him. On the Mac-CAT-CA, a
test that measures understanding relevant to competence to stand trial, the result:
was indicative of impaired reasoning abilities. Two types of items comprise the Reasoning measure: recognizing relevance and evaluating alternatives. Mr. Clayton’s performance on these items indicated that he was able to recognize relevant information. However, he displayed significant difficulty in being able to reason between two legal options. Mr. Clayton obtained a score of 3 out of a possible 12 on items which assessed the concept of Appreciation. This score is indicative of significant impairment.
(Ex. 20 p. 27.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 7 of 20 PageID #: 7

8
12. Over the past seven years, other psychologists have evaluated Mr. Clayton. Dr.
William Logan, M.D., evaluated Mr. Clayton in 2008, 2013 and 2015. Dr. Logan
concluded each time that Mr. Clayton is incompetent. He found that Mr. Clayton suffers
from dementia and brain damage resulting in significant memory impairment, decreased
judgment, decreased ability to process information or to grasp abstract concepts, a
disorganized thought process, and delusions. (Ex. 1). Dr. Daniel Foster, Psy.D., also
examined Mr. Clayton in 2008, 2013 and 2015. Like Dr. Logan, Dr. Foster found Mr.
Clayton incompetent each time he saw him. He also found that Mr. Clayton suffered from
significant frontal lobe damage, which caused subsequent cognitive impairment with
significant deficits in judgment, problem solving, mental flexibility, processing speed,
and verbal disinhibition. Additionally, he noted that Mr. Clayton suffered from
depressive episodes, insomnia, visual and auditory hallucinations, delusions, and
paranoia. (Ex. 2). Both doctors found Mr. Clayton’s delusions surrounding his execution
to be noteworthy. Specifically, Mr. Clayton believes that he was convicted because of a
conspiracy against him and that he will be spared the death penalty when God intervenes
on his behalf, after which time he will travel the country playing the piano and preaching
the gospel. (Ex. 21, 22, 24, 25).
13. The doctors’ findings are corroborated by other prisoners incarcerated with
Mr. Clayton who observe him daily. Two former cellmates of Mr. Clayton, John Johnson,
149663, and Brandon Swallow, 1140694, both have witnessed Mr. Clayton’s repeated
inability to follow simple directions in the prison. For example, both have observed Mr.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 8 of 20 PageID #: 8

9
Clayton’s inability to order commissary from a kiosk on his own. Mr. Clayton needed to
remember to enter his DOC number, hit “okay,” then enter a four-digit PIN number, but
he could not follow the prompts and complete these steps. Mr. Johnson showed Mr.
Clayton several times how to use the system, however, Mr. Clayton remains unable to
use the system. Both prisoners also noted that Mr. Clayton had severe memory problems.
He was very impulsive and would change subjects frequently when he spoke. He would
forget they were watching a movie and would change the television channel.
15. Both men also observed Mr. Clayton’s delusions. When they talked about
other inmates who had been executed, Mr. Clayton would tell Mr. Johnston that God
would free him. Mr. Clayton would sit and think daily about how God would get him out
of prison. Mr. Clayton told Mr. Johnston that he planned to come back to the prison and
minister and sing to the inmates.
C. Missouri’s Lethal Injection Procedure
16. Missouri’s written lethal injection protocol calls for the administration of 5
grams of pentobarbital, administered through an IV line into the execution chamber,
where the prisoner is alone and strapped to a gurney. No medical personnel are close at
hand, and the prisoner is monitored remotely from the “execution support room.”
Although medical personnel insert the IV lines at the outset, the lethal drug itself is
injected by non-medical personnel pushing syringes into the IV line at a pre-determined
flow rate.
17. Prior to the insertion of the IV lines, the prisoner may be offered oral Valium
as a sedative.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 9 of 20 PageID #: 9

10
18. The procedure itself begins with the insertion of the IV lines – one in each arm
(or a central line in the femoral, jugular or subclavian vein if venous access in the arms is
limited). The gurney is positioned so medical personnel can remotely observe the
prisoner’s face, directly, “or with the aid of a mirror.” Medical personnel “monitor” the
prisoner remotely during the execution.
19. After the IV lines are inserted, according to prison officials, the prisoner, at the
discretion of the medical doctor supervising the execution, is offered midazolam as a
sedative. Since the execution of Earl Ringo on September 10, 2014, the department of
corrections has maintained that the midazolam injection is voluntary and may be rejected
by the prisoner. If accepted, the midazolam is administered intravenously, in dosages far
higher than normally given for sedation.
20. Non-medical personnel administer the lethal drug through syringes into the IV
lines. After the administration of the initial 5 grams of pentobarbital, the non-medical
personnel flush the IV lines with saline and Methylene Blue. Shortly thereafter, the
execution chamber’s curtains are closed and medical personnel check the prisoner to see
if he is dead.
21. If the prisoner is not dead, the non-medical personnel then inject an additional
5 grams of pentobarbital through two additional syringes.
22. As a result of his severe brain damage, Mr. Clayton is not competent to
comply with Missouri’s execution protocol and make a rational decision on whether to
accept midazolam and valium. His intellectual disability makes it likely that he will not
cognitively understand the ramifications of his decision. The severe impairments in
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 10 of 20 PageID #: 10

11
speech and disorganization of thought, resulting from his brain damage, strip him of the
ability to effectively understand and communicate about the decision. His delusional
disorder further complicates the issue. Mr. Clayton may believe that he should not take
the drug because divine intervention is going to rescue him at the last minute. On the
other hand, he could be directed by an auditory hallucination to take the midazolam.
Regardless, he would not be making a competent, rational, and informed decision.
23. Dr. Mark Heath, a board-certified anesthesiologist, explains that the altered
structure of Mr. Clayton’s brain complicates this further. Exhibit 26, Affidavit of Dr.
Mark Heath with Curriculum Vitae, at ¶12, p. A98. Leading up to the execution, the
prison will offer Mr. Clayton valium and midazolam. These drugs are of a similar class,
benzodiazepine. This class of drugs produces “axiolytic, sedative, and amnestic effects.
Because [valium and midazolam] are both benzodiazepines and because they bind to the
same receptors of the brain, [valium, also known as] diazepam and midazolam are
additive in their effects.” (Ex. 26 ¶14.).
24. Moreover, both midazolam and valium act on the very part of the brain where
Mr. Clayton has severe damage. That is, they will cause Mr. Clayton’s frontal lobe to be
“depressed or completely silenced.” Ex. 26 ¶16. Because Mr. Clayton’s abnormalities are
focused in the area where these drugs act, Mr. Clayton is likely to experience an atypical
response to the midazolam. He is likely to experience effects associated with frontal lobe
decompensation. Such a response, coupled with his facing his imminent death, “could
produce extreme psychological—disarray, disinhibition, and behavioral
decompensation.” (Ex. 26 ¶17.)
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 11 of 20 PageID #: 11

12
25. The use of midazolam and valium also increases the risk of difficulty
establishing access to Mr. Clayton’s veins, “If Mr. Clayton is unable to maintain self-
control during the process, it is likely that he will not be able to cooperate and remain still
during the attempted insertion of intravenous catheters. It is foreseeable that the process
of obtaining intravenous access may become an arduous battle requiring extreme restraint
and multiple painful failed attempts.” (Ex. 26 ¶22.)
26. There are common clinical responses to mitigate the risks associated with
sedating a person with injuries like Mr. Clayton’s; however, the Department of
Corrections will not take any of these readily available steps. In “the clinical setting . . .
prior to inducing anesthesia, the anesthesiologist has the option of administering
intramuscular sedatives and/or relaxants to sedate the patient and provide conditions that
are amenable to obtaining IV access.” (Ex. 26 ¶23.) Even if the Department of
Corrections had such drugs at their disposal, “intramuscular sedation is not included as an
option in the current protocol. Further, if Mr. Clayton was to require sedation in order to
obtain IV access, it would render him into a state in which he would not be competent to
be executed, assuming that he currently is.” (Ex. 26 ¶23.)
27. Likewise, in the clinical setting, “the presence of a parent or friend or familiar
caregiver in the operating room prior to and during the induction of anesthesia can be
extremely valuable in assuaging fear and agitation in these patient groups.” (Ex. 26 ¶20.)
The Department of Corrections, by contrast, will cut Mr. Clayton off from such
caregivers, and he “will be surrounded by people who are organized to harm him, who
are restraining him, and who are inserting needles into his arms or legs or groin or neck.”
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 12 of 20 PageID #: 12

13
(Ex. 26 ¶21.) This stress “will likely inflame his documented paranoid and delusional
ideation, and will further increase the risk that he will enter into a cruelly terrified state of
psychological disintegration.” (Ex. 26 ¶21.)
28. Given Mr. Clayton’s significant deficits already present, his potential
decompensation makes it impossible for him to meaningfully assess the risks associated
with accepting or rejecting the valium and midazolam. Fundamentally, it is unfair that
Mr. Clayton, saddled with a crippling brain injury, should be required to make the
difficult choice of whether to face his death fully lucid, and experience the full extent of
the suffering associated with it, or, to opt for midazolam and valium, drugs that could
cause him to psychologically decompensate and expose him to extreme suffering. Other
drugs and clinical techniques are readily available that would not create such risk, and
Mr. Clayton’s execution would violate the Eighth Amendment. See U.S. Const. amend.
VIII; Baze v. Rees, 553 U.S. 35 (2008).
29. Depriving Mr. Clayton the option of midazolam or valium would not alleviate
these problems. To do so would deprive Mr. Clayton of the option of a sedative because
of his disability, something our constitution does not tolerate. U.S. Const. amend. XIV;
New York City Transit Authority v. Beazer, 440 U.S. 568 (1979). Mr. Clayton’s very low
intellectual functioning, together with his profound brain damage makes Missouri’s
current method of execution unconstitutional, as applied to him.
30. Mr. Clayton’s brain damage makes him uniquely susceptible to an atypical
response to valium and midazolam. Even if the Department of Corrections’
administration of midazolam would not render a person with a normal brain
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 13 of 20 PageID #: 13

14
incompetent—and assuming for sake of argument Mr. Clayton is currently competent—
Mr. Clayton’s adverse reaction to the midazolam would render him incompetent to be
executed. Midazolam and valium are both benzodiazepines. They act on the same
receptors in the brain. (Ex. 26 ¶14.) For this reason, if both are administered, they will
have an additive effect. (Ex. 26 ¶14.)
31. Benzodiazepines “can demonstrate atypical effects when administered to
patients with a history of brain damage.” (Ex. 26 ¶15.) Because of Mr. Clayton’s damage
to his frontal lobe, the parts of that portion of his brain that are “partially functional will
likely be depressed or completely silenced by benzodiazepine administration.” (Ex. 26
¶16.) “In combination with his impaired and abnormal cognitive processing of his
imminent death, any derangement caused by [benzodiazepines] could produce extreme
psychological disarray, disinhibition, and behavioral decompensation.” (Ex. 26 ¶17.) He
would “not understand why he is being executed or even that he is being executed.” (Ex.
26 ¶17.)
32. The Eighth Amendment bars executing a person who does not know that he is
being executed or does not rationally understand why he is being executed. See Panetti v.
Quarterman, 551 U.S. 930, 959 (2007). Missouri law prohibits the execution of a person
who “lacks capacity to understand the nature and purpose of punishment about to be
imposed upon him or matters in extenuation.” Mo. Rev. Stat. §552.060.1. Mr. Clayton’s
brain damage, together with the benzodiazepines, would render him unable to
“understand why he is being executed or even that he is being executed.” (Ex. 26 ¶17.)
Thus, his execution under such circumstances would violate state and federal law.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 14 of 20 PageID #: 14

15
33. Missouri is not using FDA approved pentobarbital, instead using pentobarbital
from a secret compounding pharmacy. “Because of this provenance, this pentobarbital is
more likely than FDA-approved pentobarbital to be defective.” (Ex. 26 ¶25.) “Because
of existing damage to [Mr. Clayton’s] brain, he is particularly vulnerable and sensitive
effects” of the risks of using compounded pentobarbital. (Ex. 26 27.)
34. Defective pentobarbital is a growing problem. “Defective pentobarbital,
obtained from a cryptic compounding source, has caused a postponed execution in
Georgia.” (Ex. 26 ¶26.) There, the Department of Corrections described their
compounded pentobarbital “cloudy” and “announced it was postponing [all] the
executions . . . ‘while an analysis is conducted of the drugs.’” Mark Berman, Georgia
Postpones Executions Indefinitely So It Can Examine Lethal Injection Drugs,
Washington Post (Mar. 3, 2015) available at http://www.washingtonpost.com/news/post-
nation/wp/2015/03/03/georgia-postpones-executions-indefinitely-so-it-can-examine-
lethal-injection-drugs/. “The exact nature of the problem with the pentobarbital and its
preparation has not yet been divulged.” (Ex. 26 ¶24.) Missouri has no known plans to
review its compounded pentobarbital following the problems in Georgia. Using FDA
approved pentobarbital is a readily available alternative to Missouri’s current protocol
that would avoid this problem.
35.“If defective pentobarbital fails to kill [Mr. Clayton,] but instead exposes him
to a period of reduced or absent breathing, the resulting further damage to his brain could
leave him in a profoundly neurologically damaged or destroyed state.” (Ex. 26 ¶ 27.) Dr.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 15 of 20 PageID #: 15

16
Heath is familiar with Missouri’s protocol and regularly administers the drugs it uses. He
says,
Mr. Clayton, by dint of the traumatic injury to his frontal lobe, presents unique challenges and risks to the Missouri DOC and its process for executing him. His impaired faculties increase the risk of him requiring pre-procedure sedation, but the only drugs available to the anesthesiologist (midazolam and diazepam) hold a high risk of causing atypical agitation and confusion. . . . There is a high likelihood that agitation and fear will render him unable to cooperate with the IV insertion process, and this will foreseeably result in a spiraling cycle of failed access, repeated needling, and uncontrolled struggling, panic, and disarray. The use of non-FDA-approved pentobarbital amplifies this risk of further injury to his already vulnerable and fragile brain.
(Ex. 26 ¶28.)
36. Mr. Clayton’s impairments, and the well-known medical reactions to these
drugs Missouri will use, makes it “foreseeable that deploying the current rigid and
inadequate procedures and protocol will, in Mr. Clayton’s case, lead inexorably to a
cruelly botched debacle of an execution.” (Ex. 26 ¶29.) This debacle will likely result in
extreme pain. As such, it violates the Eighth Amendment for Missouri to use its current
lethal injection protocol to execute Mr. Clayton. See U.S. Const. amend. VIII; Baze v.
Rees, 553 U.S. 35 (2008).
37. Missouri could significantly reduce the risk of unreasonable pain and suffering
to Mr. Clayton by making the following alterations to its protocol:
a. Disallow the use of compounded pentobarbital, and instead require
pharmaceutical grade pentobarbital from an FDA-approved manufacturer.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 16 of 20 PageID #: 16

17
b. Permit a friend or family member of Mr. Clayton to be present with him in the
execution chamber.
c. Amend the execution procedures to include a treating physician, who can
determine the correct medications to be administered in the event that Mr. Clayton
becomes agitated after the administration of midazolam.
COUNT I
VIOLATION OF CRUEL AND UNUSUAL PUNISHMENT CLAUSE
Mr. Clayton realleges the foregoing facts and further states as follows:
38. Defendants’ flawed execution protocol, its use of secret, unregulated drugs,
and its failure to provide for steps for evaluating whether or how Mr. Clayton can be
constitutionally executed will cause extreme and needless suffering to Mr. Clayton,
including but not limited to extreme anxiety and fear, pain from attempts to start IV lines
when he is struggling, and assaults by prison personnel in an effort to complete the
execution protocol.
39. If Missouri proceeds with its scheduled execution of Mr. Clayton, it will be
conducting an unregulated experiment on a human subject, as there are no studies that
support Defendants’ use of Missouri’s lethal injection protocol on an individual suffering
from severe brain damage.
40. Missouri’s lethal injection procedures, as applied to Mr. Clayton, are sure or
very likely to cause excruciating or tortuous pain and needless suffering.
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 17 of 20 PageID #: 17

18
41. Defendants’ intended actions as set forth in this Complaint will inflict extreme,
tortuous and unnecessary pain and therefore violate the Cruel and Unusual Punishments
Clause of the Eighth Amendment of the United States Constitution.
PRAYER FOR RELIEF
Mr. Clayton requests the following relief:
1. That this Court issue a declaratory judgment declaring and enforcing the rights
of Mr. Clayton, as alleged above, and further issue a temporary restraining order or
preliminary or permanent injunction to enforce Mr. Clayton’s rights under the Eighth and
Fourteenth Amendments to the United States Constitution, directing the defendants not to
carry out any lethal injection on Mr. Clayton until such time as adequate procedures are
in place to prevent a violation of Mr. Clayton’s Eighth Amendment rights as alleged
above.
2. That this Court award Mr. Clayton a reasonable attorney’s fee and costs
pursuant to 42 U.S.C. §1988.
3. For such other relief as this Court deems just and proper.
Respectfully submitted, /s Elizabeth Unger Carlyle Elizabeth Unger Carlyle 41930MO 6320 Brookside Plaza #516 Kansas City, MO 64113 (816)525-6540 FAX (866) 764-1249 e-mail: [email protected] ATTORNEY FOR CECIL CLAYTON
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 18 of 20 PageID #: 18

19
LIST OF EXHIBITS
Ex. 1, 2009 report of William S. Logan, M.D. Ex. 2, 2009 report of Dr. Daniel V. Foster Ex. 3, Report of Dr. John Tsang, January 24, 1972 Ex. 4, Report of Dr. John Tsang, January 26, 1972 Ex. 5, St. John’s Hospital Discharge Summary, Feb. 3, 1972 Ex. 6, Letter from Dr. George Klinkerfuss, Jan. 30, 1978 Ex. 7, Statement of Dr. Klinkerfuss, April 24, 1978 Ex. 8, Psychiatric Evaluation, Ozark Psych. Clinic, Jan. 24, 1979 Ex. 9, Letter from Dr. Klinkerfuss, January 31, 1980 Ex. 10, Letter from Dr. Klinkerfuss, July 16, 1980 Ex. 11, Letter from Dr. Klinkerfuss, Sept. 1, 1983 Ex. 12, Letter from Dr. Douglas A. Stevens, Oct. 31, 1983 Ex. 13, Psychiatric Evaluation, February 9, 1984 Ex. 14, Letter from Dr. James A. Bright, March 20, 1984 Ex. 15, US DHS determination, April 6, 1984 Ex. 16, copy of MRI scan Ex. 17, Affidavit of Julie Eilers, Investigator Ex. 18, Affidavit of Attorney Laura Martin Ex. 19, Affidavit of Rebecca Kurz, Attorney Ex. 20, Forensic evaluation, Dr. Lea Ann Preston Ex. 21, Updated findings by William S. Logan, M.D., Aug. 28, 2013
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 19 of 20 PageID #: 19

20
Ex. 22, Updated findings by Daniel V. Foster, Psy. D., Nov. 24, 2013 Ex. 23, Purdy School Records Ex. 24, Updated findings by William S. Logan, M.D., Jan. 7, 2015 Ex. 25, Updated findings by Daniel v. Foster, Psy.D, Jan. 7, 2015 Ex. 26, Declaration and CV of Dr. Mark Heath
Case: 4:15-cv-00470-AGF Doc. #: 1 Filed: 03/13/15 Page: 20 of 20 PageID #: 20