INTRAOPERATIVE MARGIN ASSESSMENT WITH … Conserving Surgery- More challenging as imaging and...
18
INTRAOPERATIVE MARGIN ASSESSMENT WITH THE MARGINPROBE ® SYSTEM 1
Transcript of INTRAOPERATIVE MARGIN ASSESSMENT WITH … Conserving Surgery- More challenging as imaging and...

INTRAOPERATIVE MARGIN ASSESSMENT WITH THE MARGINPROBE® SYSTEM
1

Breast Conserving Surgery- More challenging as imaging and screening improves
§ Advances in imaging (mammography, ultrasound, MRI, tomosynthesis) mean that most breast cancers are detected in an early stage
§ Early detection means that most breast
cancer patients have the choice between a mastectomy and a lumpectomy
– Lumpectomy followed by radiation offers equivalent survival, while preserving the breast
– 60-70% of women prefer breast conservation
§ Early detection has led to an increase in
the diagnosis of DCIS. – DCIS is not palpable, or visible
macroscopically, during lumpectomy.
2
McCahill, JAMA. 2012;307(5):467-475 US National Cancer Institute, SEER Cancer Statistics Review, 1975 – 2005 Halasz, Int J Rad Oncol Biol Phys (2012) 82(4): 581-6

§ Obtaining negative margins during surgery is a significant challenge: – 20-25% national average re-excision rate (repeat surgery after
lumpectomy). § 35-50% average re-excision rates in DCIS § Recent developments:
Impact of Positive Margins
3
McCahill, JAMA. 2012;307(5):467-475 US National Cancer Institute, SEER Cancer Statistics Review, 1975 – 2005 Halasz, Int J Rad Oncol Biol Phys (2012) 82(4): 581-6
Increased Pressure to reduce positive
margins and repeated lumpectomies
Healthcare reform New SSO Guidelines for Positive margins

Positive Margins- Why are they important?
§ Positive margins are associated with a two-fold risk for recurrence – most patients with positive margins will go back to the OR for additional
surgery1
§ Each year, over 35,000 women have additional surgery for positive or close margins in the US2
§ These procedures lead to over $200 million in added cost to the healthcare system2
4
1) Society of Surgical Oncology consensus guideline on margins for breast-conserving surgery 2) Source: internal estimates

Impact of Re-excisions
§ Added discomfort1 § Increased surgical complications1 § Compromise in cosmetic outcomes1 § Additional unnecessary emotional stress for patients and families1
§ Delay to Adjuvant Therapy2 § Increased Health Care costs1 § Influences preference for conversion to mastectomy2 § Influences patient preference for conversion to prophylactic
contralateral mastectomy3
(1) Moran, Annals of Surgical Oncology (2014) doi 10.1245/s10434-014-3481-4 (2) Morrow, JAMA (2009) October p. 1553 (3) King, Journal of Clinical Oncology (2011) November pgs. 2163-2164

Novel Therapies- In all of them the ramification of a positive margin are even more pronounced
Newer therapeutic techniques in breast cancer treatment rely even more heavily on achieving negative margins § Oncoplastic Surgery
§ Partial Breast Irradiation
§ Intraoperative Radiation Therapy
6
Articles
92 www.thelancet.com Vol 376 July 10, 2010
Oncology (M Roncadin MD), Centro di Riferimento
Oncologia, Aviano, Italy; Department of Gynecology and
Obstetrics, Red Cross Hospital, Munich, Germany
(W Eiermann MD); Department of Radiation Oncology,
Technical University of Munich, Munich, Germany
(S Pigorsch MD); Royal Free Hospital, London, UK
(M Keshtgar PhD); Department of Radiation Oncology,
Ninewells Hospital, Dundee, UK (J Dewar FRCR); and
Psychosocial Oncology Clinical Studies Group, National Cancer Research Institute, London, UK
(A Matthews BSc)
Correspondence to:Dr Jayant S Vaidya, Research
Department of Surgery, Division of Surgery and Interventional
Science, University College London, 2nd Floor Clerkenwell
Building, Highgate Hill, London N19 5LW, UK
cancer is common, the absolute number of women with complications and side-eff ects is large. More importantly, the 3–7 weeks of a typical postoperative radiotherapy schedule is at best inconvenient for working women or exhausting and often untenable for elderly women. Although many studies2–4 have failed to identify a subgroup of patients in whom radiotherapy can be completely avoided, whether irradiation of the whole breast is necessary in all or a subgroup of patients remains unclear.
Many observational studies and randomised clinical trials have shown that more than 90% of recurrent disease occurring in the breast is within the index quadrant,5–13 which is by contrast with the fi ndings of three-dimensional analysis of mastectomy specimens that show that 63% of breasts harbour occult cancer foci, with 80% of these situated remote from the index quadrant.14–16 These widespread and occult multifocal or multicentric cancers in other quadrants of the breast therefore appear to remain dormant for many years or even decades, and have a low risk of causing clinical tumours. Thus, irradiation of the immediate vicinity of the primary tumour might be adequate for achieving local control of cancer.14–16
The TARGIT-A trial was designed to test the hypothesis that in selected patients, substituting the policy of whole breast radiotherapy after breast-conserving surgery with a policy of targeted intraoperative radiotherapy (also known as TARGIT) to the tumour bed with additional whole breast radiotherapy in a subgroup of patients (around 15%) with poor features on fi nal pathology would not lead to inferior local control of breast cancer.
MethodsStudy design and participantsTARGIT-A was a pragmatic, prospective, international, multicentre, randomised, phase 3 trial that compared targeted intraoperative radiotherapy with the conventional policy of whole breast external beam
radiotherapy. An outline of the protocol and the full protocol are available online. Women with early breast cancer were eligible for enrolment if they were aged 45 years or older and were suitable for wide local excision for invasive ductal carcinoma that was unifocal on conventional examination and imaging (MRI was not necessary for confi rming unifocality). Preoperative diagnosis of lobular carcinoma was an exclusion criterion. Patients gave written informed consent to join the trial. The protocol was approved by the appropriate regulatory and ethics authorities for each centre before enrolment could begin.The initial trial plan was developed in University College London (UCL), London, UK. Management of the trial was coordinated and supervised by the international steering committee (ISC) with advice from the data monitoring committee (DMC). Representatives from the manufacturer of the Intrabeam equipment (Carl Zeiss, Oberkochen, Germany) attended the ISC meetings as observers. The trial statistician supervised all data analyses. The interpretation of the analyses, presentation of data at meetings, and preparation of manuscripts for publication are all responsibilities of the ISC. The TARGIT Trials Operations Offi ce is located at UCL and is responsible for randomisations, data collection, data management, and servicing of the ISC and DMC. No changes were made to the methods after commencement of the trial.
Before centres were allowed to participate, the team was trained and audited by a member of the ISC. Each centre was allowed to restrict the inclusion criteria beyond the core protocol, and to stipulate local policy for giving external beam radiotherapy (typically 40–56 Gy with or without a boost of 10–16 Gy, standard tangents, etc) both in the external beam radiotherapy group and as an additional dose in the targeted intraoperative radiotherapy group, in a site-specifi c treatment policy document that was reviewed and signed off by the ISC before randomisation could begin.
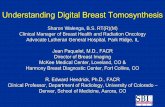
BA
Figure 1: Targeted intraoperative radiotherapy technique with the Intrabeam system(A) The applicator being placed in the tumour bed. (B) The x-ray source is delivered to the tumour bed by use of a surgical support stand. The sterile applicator is joined with a sterile drape that is used to cover the stand during treatment delivery.
For an outline of the protocol for this trial see http://www.
thelancet.com/protocol-reviews/99PRT-47
For the full protocol for this trial see http://www.hta.ac.uk/
project/1981.asp

The Patient’s Lumpectomy Experience
Diagnosis
• 2-4 week process
Surgery
• Visual inspection and palpation
• Specimen imaging
Pathology Results
• Available 2-5 days after surgery
Adjuvant Therapy
• Radiation and/or Chemotherapy
7
A positive margin puts the patient back to where they were after diagnosis – Confidence in the treatment course is shaken, and often leads to second
opinion meetings, possibly at second provider – Most patients with a positive margin undergo a 2nd lumpectomy surgery – 10-36% of patients convert to a mastectomy – Some patients do not comply with additional surgery, proceeding with radiation
(and a 2x higher risk of recurrence)

The Challenge of Intraoperative Detection
§ Current methods are inadequate – Pathology techniques (frozen section,
touch prep) are difficult due to fatty nature of breast tissue and have high sampling error. In addition they add up to 40 minutes of OR time.
– Specimen X-ray (including intraoperative x-ray like Faxitron) cannot identify the small amounts of tumor
– These techniques have very little sensitivity to DCIS at the margin
§ There have been no innovations in helping the surgeon to identify positive margins in 20 years
8

MARGINPROBE
§ MARGINPROBE System consists of a single-use probe attached to a portable console
§ Adjunctive tool to standard of care (SOC) § Identifies positive margins for immediate resection
• Probe applies a localized RF field and captures reflected signals from tissue
• These signals contain information that allows the tissue to be characterized as cancer or non-malignant
• Console performs signal analysis, and displays results to surgeon
9

How it works
10
Membrane de-polarization
Alterations in nuclear
morphology
Increased vascularity
-70mV -20mV
Cell to cell connectivity
The MarginProbe System detects the bioelectric differences in cancerous cells, using a techinque called RF Spectroscopy
Applying a localized RF field and measuring the tissue response
The MarginProbe can measure the electrical signature of the tissue

GROWING BODY OF CLINICAL STUDIES

Clinical Study Data
12
Device + SOC SOC P-value % change
MAST Study
Re-excision rate 5.6% (8/143)
12.7% (19/150)
0.0027 56%
FDA Pivotal Study
Positive margins on the main specimen which were not addressed [positive defined as 0-1mm]
15.4% (46/298)
38.3% (114/298)
<0.0001 60%
DCIS Study
Re-excision rate 17% (7/42)
39% (26/67)
historical
0.018 56%
Post-market Studies
Blohmer – re-excision rate Sebastian – re-excision rate Hareufa – re-excision rate Sebastian – re-excision rate
14.6%
9.7% (16/165)
6% (4/64)
10.7% (31/290)
29.7% 25.8% (48/186) Historical not reported 25.8% (48/186)
0.0014 <0.0001 <0.0001
51%
62% 59%
Consistent >50% reduction in positive margin and re-excision rates

High Patient Satisfaction
§ Patients growing awareness to risk for positive Margins and possible additional surgery leads to patients seeking MarginProbe sites
§ Cosmetic outcome is known to correlate to patient satisfaction in breast conserving surgery
• Re-excisions adversely affect cosemtic outcomes (Wazer et al, 1992) • Lower re-excision rate improves patient satisfaction (Rizzo et al, 2009)
§ Studies with MarginProbe use have shown cosmesis scores of: • Allweis
– 70% good/excellent (all patients) – 78% good/excellent (screening patients)
• Thill – 80% good/excellent (surgeons) – 92% good/excellent (patient reported)
13

Reimbursement
§ Medicare recognizes intraoperative margin assessment as a covered service
– 88331/88332 – Frozen Section analysis of margins – 88333/88334 – Touch Prep analysis of margins – Frozen Section can add over $1000 per patient
§ Intraoperative assessment using RF Spectroscopy – 19499 – breast unlisted code – Medicare national average facility payment of $987 – Commercial payments will vary based on contracting
§ Comprehensive coding and reimbursement support provided by Dune – Coding, Coverage and Payment guide – Hotline support
14

Value to the Hospital
§ More lumpectomies + radiation therapy – ~70% of patients prefer breast conservation – The possibility of multiple surgeries is a significant deterrent
§ Fewer conversions to mastectomy – Negative margins the first time keep a patient headed to radiation instead of
mastectomy § Improved OR efficiency
– Fewer add-on cases – Increased OR availability – Reduction in frozen section wait time (where relevant)
§ More patients – Surgeons can accept more new patients – Marketing benefits increase patient draw radius (frequent local TV and Web
pickup, for early in market) § More satisfied Patients
§ Looking ahead towards the healthcare reform emphasis on payment to providers per quality (vs per procedure): the MarginProbe is perfectly positioned
15

Thank you!
Questions?
16

Pro-forma analysis
§ Many centers find that their MarginProbe program is a net breakeven financially
17

Lumpectomy Processing in Pathology
18
Sectioning the specimen
Microscopic review: 1. Tumor cells 2. Distance to ink
Tissue samples from each margin
Orientation Specimen Inking (OR or pathology)
1. 2. 3.
4.
A. B.
5.