INTRAOPERATIVE USE OF HANDHELD SPECTRAL DOMAIN …people.duke.edu/~sf59/dayani.pdf ·...
12
INTRAOPERATIVE USE OF HANDHELD SPECTRAL DOMAIN OPTICAL COHERENCE TOMOGRAPHY IMAGING IN MACULAR SURGERY POUYA N. DAYANI, MD, RAMIRO MALDONADO, MD, SINA FARSIU, PHD, CYNTHIA A. TOTH, MD Purpose: To describe the intraoperative use of handheld spectral domain optical coherence tomography (SDOCT) imaging in macular surgery. Design: Prospective, observational case series. Methods: A handheld SDOCT device was used to obtain preincision optical coherence tomography imaging in patients undergoing vitrectomy for macular diseases. After removal of the internal limiting membrane or the epiretinal membrane, repeat intraop- erative imaging was obtained. Spectral domain optical coherence tomography findings were characterized. Results: An efficient technique was established for obtaining intraoperative SDOCT imaging. A total of eight patients were included in the study. Four patients underwent surgery for macular hole, three patients for epiretinal membrane, and one for vitreomacular traction. Comparison of the preincision and intraoperative SDOCT images demonstrated distinct changes in retinal contour and macular hole configuration. Intraoperative SDOCT imaging identified additional membranes in two patients. Conclusion: The intraoperative use of handheld SDOCT imaging provides an efficient method for visualizing macular pathology. This technology may, in certain cases, help confirm or identify diseases that may be difficult to visualize during surgery. RETINA 29:1457–1468, 2009 O ptical coherence tomography (OCT) is a rapid, noncontact, and noninvasive method of imaging intraocular tissue that has significantly contributed to the understanding, diagnosis, treatment, and follow-up of retinal diseases. 1–5 Spectral domain optical coher- ence tomography (SDOCT) provides a number of advantages over conventional time-domain OCT sys- tems. By eliminating the need for a scanning mirror, SDOCT offers higher acquisition speed and, thus, the ability to obtain significantly more images in a shorter period of time (approximately 20,000 A-scans per second compared with 400 A-scans per second on time-domain OCT). This increased speed minimizes patient movement artifact and improves image reso- lution. Some studies suggest that the higher resolution obtained with SDOCT imaging may improve the de- tection of abnormalities. 6 –10 The ability to obtain vol- ume maps of an entire region and the improved reg- istration with SDOCT allow one to accurately follow changes in the same anatomic area on subsequent imaging. Some units also have added features such as fluorescein angiography, autofluorescence, indocya- nine green angiography, and scanning laser ophthal- moscope capability. An important limitation of typical OCT units is that they are stationary and require a compliant patient who can sit upright. Thus, uncooperative pediatric patients and those with limited mobility (i.e., because From the Department of Ophthalmology, Duke University Eye Center, Durham, North Carolina. Supported by North Carolina Biotechnology Center Collaborative Funding Grant no. 2007-CFG-8005 with Bioptigen Inc., National Institutes of Health R21 EY017393, and the Duke Translational Med- icine Institute Subcontract No. 12 of NIH Grant No. 5ULT- RR024128-03. Supported, in part, by a grant from the Heed Ophthal- mic Foundation (to P.N.D.). Dr. Toth receives other support from the following commercial entities: Alcon Laboratories (honorarium, research support, and royalties), Bioptigen (honorarium, research support, and license agreement), Genentech (honoraria and research grant), and Sirion Therapeutics (research grant). Dr. Dayani received an honorarium as a clinical consultant from OSI Therapeutics. Reprint requests: Cynthia A. Toth, MD, Duke University Eye Center, PO Box 3802, Durham, NC 27710; e-mail: cynthia.toth@ duke.edu 1457
Transcript of INTRAOPERATIVE USE OF HANDHELD SPECTRAL DOMAIN …people.duke.edu/~sf59/dayani.pdf ·...
INTRAOPERATIVE USE OF HANDHELDSPECTRAL DOMAIN OPTICALCOHERENCE TOMOGRAPHY IMAGINGIN MACULAR SURGERYPOUYA N. DAYANI, MD, RAMIRO MALDONADO, MD, SINA FARSIU, PHD,CYNTHIA A. TOTH, MD
Purpose: To describe the intraoperative use of handheld spectral domain opticalcoherence tomography (SDOCT) imaging in macular surgery.
Design: Prospective, observational case series.Methods: A handheld SDOCT device was used to obtain preincision optical coherence
tomography imaging in patients undergoing vitrectomy for macular diseases. Afterremoval of the internal limiting membrane or the epiretinal membrane, repeat intraop-erative imaging was obtained. Spectral domain optical coherence tomography findingswere characterized.
Results: An efficient technique was established for obtaining intraoperative SDOCTimaging. A total of eight patients were included in the study. Four patients underwentsurgery for macular hole, three patients for epiretinal membrane, and one for vitreomaculartraction. Comparison of the preincision and intraoperative SDOCT images demonstrateddistinct changes in retinal contour and macular hole configuration. Intraoperative SDOCTimaging identified additional membranes in two patients.
Conclusion: The intraoperative use of handheld SDOCT imaging provides an efficientmethod for visualizing macular pathology. This technology may, in certain cases, helpconfirm or identify diseases that may be difficult to visualize during surgery.
RETINA 29:1457–1468, 2009
Optical coherence tomography (OCT) is a rapid,noncontact, and noninvasive method of imaging
intraocular tissue that has significantly contributed tothe understanding, diagnosis, treatment, and follow-upof retinal diseases.1–5 Spectral domain optical coher-ence tomography (SDOCT) provides a number ofadvantages over conventional time-domain OCT sys-
tems. By eliminating the need for a scanning mirror,SDOCT offers higher acquisition speed and, thus, theability to obtain significantly more images in a shorterperiod of time (approximately 20,000 A-scans persecond compared with 400 A-scans per second ontime-domain OCT). This increased speed minimizespatient movement artifact and improves image reso-lution. Some studies suggest that the higher resolutionobtained with SDOCT imaging may improve the de-tection of abnormalities.6–10 The ability to obtain vol-ume maps of an entire region and the improved reg-istration with SDOCT allow one to accurately followchanges in the same anatomic area on subsequentimaging. Some units also have added features such asfluorescein angiography, autofluorescence, indocya-nine green angiography, and scanning laser ophthal-moscope capability.
An important limitation of typical OCT units is thatthey are stationary and require a compliant patientwho can sit upright. Thus, uncooperative pediatricpatients and those with limited mobility (i.e., because
From the Department of Ophthalmology, Duke University EyeCenter, Durham, North Carolina.
Supported by North Carolina Biotechnology Center CollaborativeFunding Grant no. 2007-CFG-8005 with Bioptigen Inc., NationalInstitutes of Health R21 EY017393, and the Duke Translational Med-icine Institute Subcontract No. 12 of NIH Grant No. 5ULT-RR024128-03. Supported, in part, by a grant from the Heed Ophthal-mic Foundation (to P.N.D.).
Dr. Toth receives other support from the following commercialentities: Alcon Laboratories (honorarium, research support, androyalties), Bioptigen (honorarium, research support, and licenseagreement), Genentech (honoraria and research grant), and SirionTherapeutics (research grant). Dr. Dayani received an honorariumas a clinical consultant from OSI Therapeutics.
Reprint requests: Cynthia A. Toth, MD, Duke University EyeCenter, PO Box 3802, Durham, NC 27710; e-mail: [email protected]
1457
of musculoskeletal disorders) or access (i.e., hospitalfloor patients or those in isolation) may not be prop-erly imaged. A portable SDOCT unit (Bioptigen Inc.,Research Triangle Park, NC) is now available thatallows imaging of such patients. We have recentlydescribed methods of imaging children with shakenbaby syndrome and those with albinism using thishandheld SDOCT unit and have characterized novelretinal SDOCT findings in these two entities.10,11
An additional value of the handheld SDOCT systemis the capability to obtain noncontact intraoperativeimages in the supine position. In the current study, wereport our experience in using a handheld SDOCTimaging device to obtain high-resolution, cross-sec-tional images in patients undergoing surgery for full-thickness macular hole (FTMH), epiretinal membrane(ERM), or vitreomacular traction. Our objectives areto describe the technique of obtaining reliable intra-operative SDOCT images, to characterize the intraop-erative findings, and to identify how these imagescompare with the preoperative scan and with the sur-geon’s assessment of the macular status.
Materials and Methods
This study was approved by the Institutional Re-view Board of Duke University Medical Center. Con-secutive patients undergoing vitrectomy surgery formacular diseases were enrolled in the study. All pa-tients provided informed consent.
Patients were imaged with a portable SDOCTworkstation consisting of a handheld SDOCT scan-ning head connected, through a flexible fiberopticcable, to a mobile cart housing the computer–spec-trometer unit and viewing screen (Bioptigen Inc.).The handheld scanning head can operate while po-sitioned at any angle, allowing its use in the supinepatient.
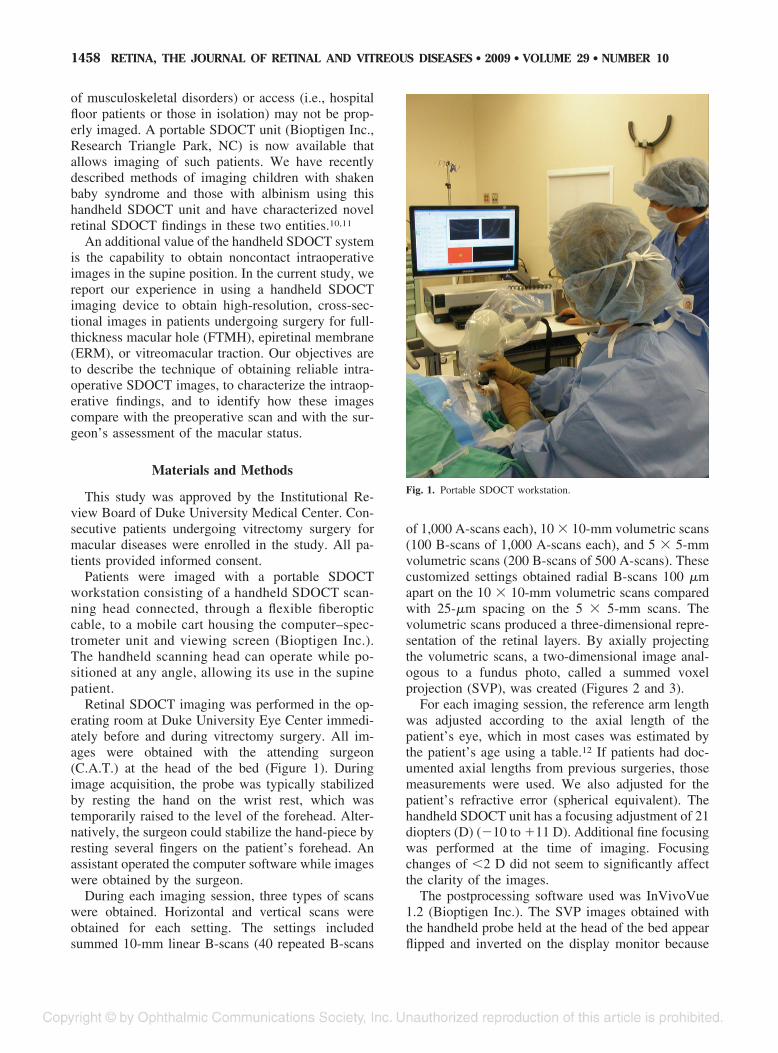
Retinal SDOCT imaging was performed in the op-erating room at Duke University Eye Center immedi-ately before and during vitrectomy surgery. All im-ages were obtained with the attending surgeon(C.A.T.) at the head of the bed (Figure 1). Duringimage acquisition, the probe was typically stabilizedby resting the hand on the wrist rest, which wastemporarily raised to the level of the forehead. Alter-natively, the surgeon could stabilize the hand-piece byresting several fingers on the patient’s forehead. Anassistant operated the computer software while imageswere obtained by the surgeon.
During each imaging session, three types of scanswere obtained. Horizontal and vertical scans wereobtained for each setting. The settings includedsummed 10-mm linear B-scans (40 repeated B-scans
of 1,000 A-scans each), 10 � 10-mm volumetric scans(100 B-scans of 1,000 A-scans each), and 5 � 5-mmvolumetric scans (200 B-scans of 500 A-scans). Thesecustomized settings obtained radial B-scans 100 �mapart on the 10 � 10-mm volumetric scans comparedwith 25-�m spacing on the 5 � 5-mm scans. Thevolumetric scans produced a three-dimensional repre-sentation of the retinal layers. By axially projectingthe volumetric scans, a two-dimensional image anal-ogous to a fundus photo, called a summed voxelprojection (SVP), was created (Figures 2 and 3).
For each imaging session, the reference arm lengthwas adjusted according to the axial length of thepatient’s eye, which in most cases was estimated bythe patient’s age using a table.12 If patients had doc-umented axial lengths from previous surgeries, thosemeasurements were used. We also adjusted for thepatient’s refractive error (spherical equivalent). Thehandheld SDOCT unit has a focusing adjustment of 21diopters (D) (�10 to �11 D). Additional fine focusingwas performed at the time of imaging. Focusingchanges of �2 D did not seem to significantly affectthe clarity of the images.
The postprocessing software used was InVivoVue1.2 (Bioptigen Inc.). The SVP images obtained withthe handheld probe held at the head of the bed appearflipped and inverted on the display monitor because
Fig. 1. Portable SDOCT workstation.
1458 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10

the InvivoVue postprocessing software did not allowus to correct for the orientation of the handheld probeat the time of imaging. A more detailed description ofthe image-processing algorithm used to enhance im-age quality is described in our previous publication.10
Preincision SDOCT images were obtained after ad-ministration of retrobulbar anesthesia with the patientsin the supine position without a lid speculum. Bal-anced salt solution or artificial tears was used to main-tain corneal surface integrity and to improve the clar-ity of the images. Three-port pars plana vitrectomysurgery was performed in all patients. The Alcon25-gauge vitrectomy system (Alcon Laboratories, Inc.,Fort Worth, TX) was used in five patients and the 20-gauge system in the remainder. The posterior hyaloidwas separated in eyes without a complete posterior vit-reous detachment. Indocyanine green angiography wasadded over the posterior pole in the fluid-filled eye in
patients undergoing macular hole (MH) surgery. Preser-vative-free triamcinolone was used to visualize the hya-loid in some patients with ERM. The Tano diamond-dusted membrane scraper and forceps were used to peelthe internal limiting membrane (ILM) along with anymembranes off the fovea. Cannulas were then plugged,and repeat intraoperative SDOCT images were obtainedin all patients. An additional sterile drape was placedfrom the patient’s upper lid, over the forehead, and offthe field to protect from inadvertent contact with thehandheld probe cord. The handheld probe was placedinto a sterile plastic bag, adjusted in such a way that thelens surface of the probe was aligned with a hole in thebag (created earlier by the surgeon), and suspended overthe eye for noncontact imaging. Methylcellulose wasplaced over the ocular surface. After acquisition of theimages, the additional drape was removed and thesurgeon resumed the surgery.
Fig. 2. Preoperative SDOCT of Case 1 captured immediately before surgery. A, SVP from a 10 � 10-mm volumetric scan outlining the areas scannedin B–D. B, Vertical 10 � 10-mm scan showing a FTMH, cystic thickening of the retina at the hole margin (white arrow), and partial posterior vitreousseparation. C, Vertical scan demonstrating partial vitreous separation (red arrow), cystic thickening of the parafoveal region, and normal hyperre-flectivity of the ILM before removal. D, Vertical scan demonstrating normal juxtafoveal retinal contour and ILM hyperreflectivity before surgery.
1459INTRAOPERATIVE SDOCT IMAGING ● DAYANI ET AL

Macular hole measurements were obtained withMatLab software (Version 7.0, Mathworks Inc.,Natick, MA) and verified with ImageJ (freeware, Na-tional Institutes of Health, Bethesda, MD). The scanselected for measurements was the one with the larg-est hole diameter. Four measurements were calculatedfrom each SDOCT image corresponding to the centerof the hole. These included the base diameter, mea-sured at the level of the retinal pigment epithelium; theminimum diameter, defined as the minimal extent ofthe hole; the maximum diameter, defined as the max-imum distance between hole edges; and the holeheight, measured as the distance between the retinalpigment epithelium and the inner most aspect of thehole (greatest height).
Results
A total of eight adult patients (eight eyes) wereenrolled and successfully imaged. There were fourwomen and four men with a mean age of 63.5 years(range, 45–81 years; Table 1). Four patients werephakic and four were pseudophakic. Four patientsunderwent vitrectomy for MH repair, three for ERM,and one for VMT. The MH was idiopathic in allpatients.
There was a learning curve in localizing the area ofinterest and obtaining reliable, high-quality scans.
Manual alignment was challenging because of severalfactors. The most important of these was motion arti-fact associated with stabilization of the handheldprobe because small horizontal or angular movementsof the imager’s hand would shift alignment off thepupil. Other challenges included the lack of real-timefundus image correlation and occasional poor SVPimage quality. Orientation during scanning was morechallenging because the SVP image and scans wereinverted on the viewing screen because of the hand-held scanner location over the patient’s forehead.
Despite such challenges, our ability to image im-proved significantly over the course of the study. TheSVPs were particularly helpful in identifying land-marks such as retinal vessels and the optic nerve,which could be used for orientation during imaging.We, thus, found that the wider field of view on theSVP obtained with the 10 � 10-mm scans, comparedwith the 5 � 5-mm scans, was advantageous in aidingorientation. The vessel pattern on the SVP was alsouseful in assessing image quality. Motion artifact dur-ing volumetric scans typically resulted in a brokenvascular pattern on the SVP (Figure 4). We also foundthat operating the Bioptigen system in “free run”mode allowed the selection of an optimal SDOCTvolume set to capture and save. With experience, eachimaging session lasted 4 minutes to 5 minutes, andindividual scans were acquired in 5.8 seconds. We
Fig. 3. Intraoperative SDOCT of Case 1 obtained immediately after ILM removal. A, SVP of the areas scanned. The dark spot in the lower rightcorner is a preretinal hemorrhage. Asterisks show corresponding location on B-scans of B–D. B, Retinal distortion, residual adherent ILM (whitearrow), and decreased reflectivity of the outer retina and shadowing (blue arrow) corresponding to a focal hemorrhage at the margin of ILM peeling.This site had a normal retinal contour before surgery. C and D, Note the hyperreflective areas along the inner retinal surface that correspond to theremaining ILM (yellow star). In contrast, there is a less intense hyperreflectivity in the areas in which the ILM was peeled corresponding to the nervefiber layer.
1460 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10
instilled Systane artificial tears (Alcon Laboratories)every two or three scans as needed to maintain ocularsurface integrity during preoperative imaging. Wefound that images obtained with artificial tears lubri-cating the cornea produced higher quality imagescompared with balanced salt solution. During surgery,Methocel 2% (Omnivision GmbH, Puchheim, Ger-many) gel over the cornea did not seem to impairimage quality.
Preincision SDOCT images confirmed the diseaseof interest in all cases. Comparison of the preoperativeand intraoperative SDOCT images yielded a numberof observations (Tables 2 and 3). These included fo-cal, iatrogenic traumatic changes (Figure 3), ILM de-fects, and distinction between areas with remainingand removed ILM (Figures 3 and 5). Residual ERMsor ILM (Figure 6) and the absence of a previouslyvisualized operculum or posterior hyaloid face werealso observed (Figures 2 and 3). In addition, alter-ations in the retinal contour and MH configurationwere observed in all cases.
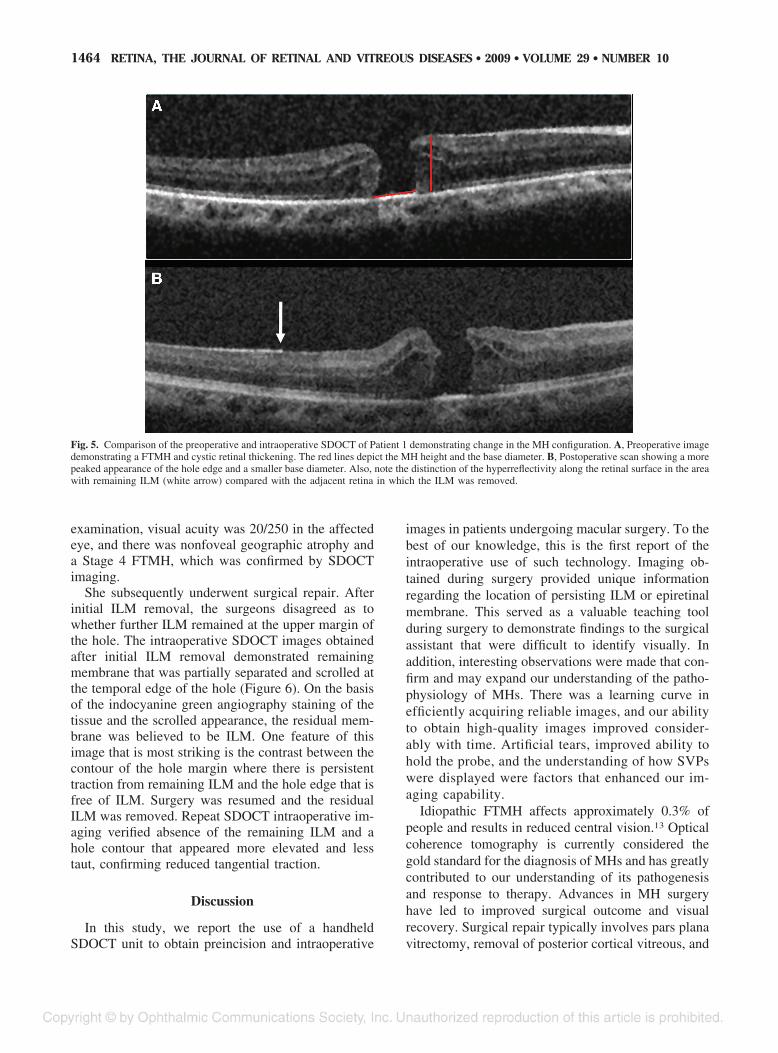
Among the patients undergoing MH surgery, thereseemed to be a reduction in the mean size of the holediameter (Table 4). This change was observed withthe base diameter and with the minimum and maxi-mum diameter (Figures 5 and 6). The MH heightremained relatively stable, and there was only moder-ate change in most cases. In 3 of the 4 patients withFTMH (Patients 1–3), the retina at the edges of thehole seemed to move centrally (toward the center ofthe MH) after ILM removal, suggesting decreasedtangential traction (Figures 5 and 6). In 2 of thesepatients (Patients 1 and 3), there was an increasedvertical retinal elevation at the edges of the hole(Figure 5).
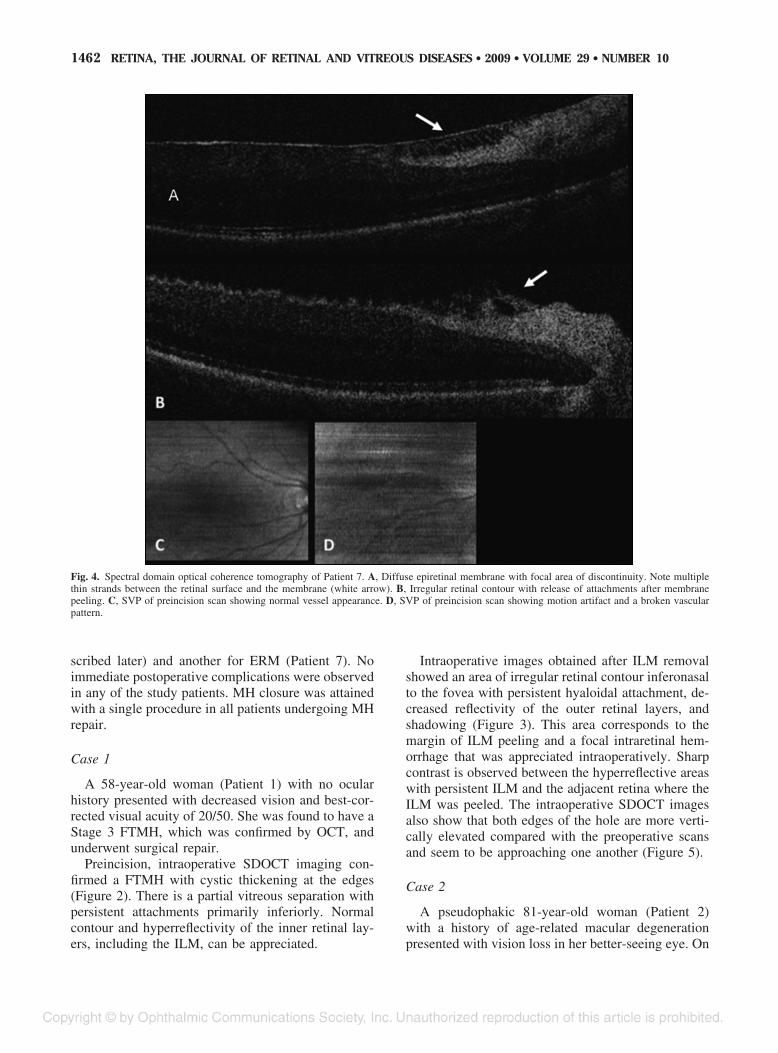
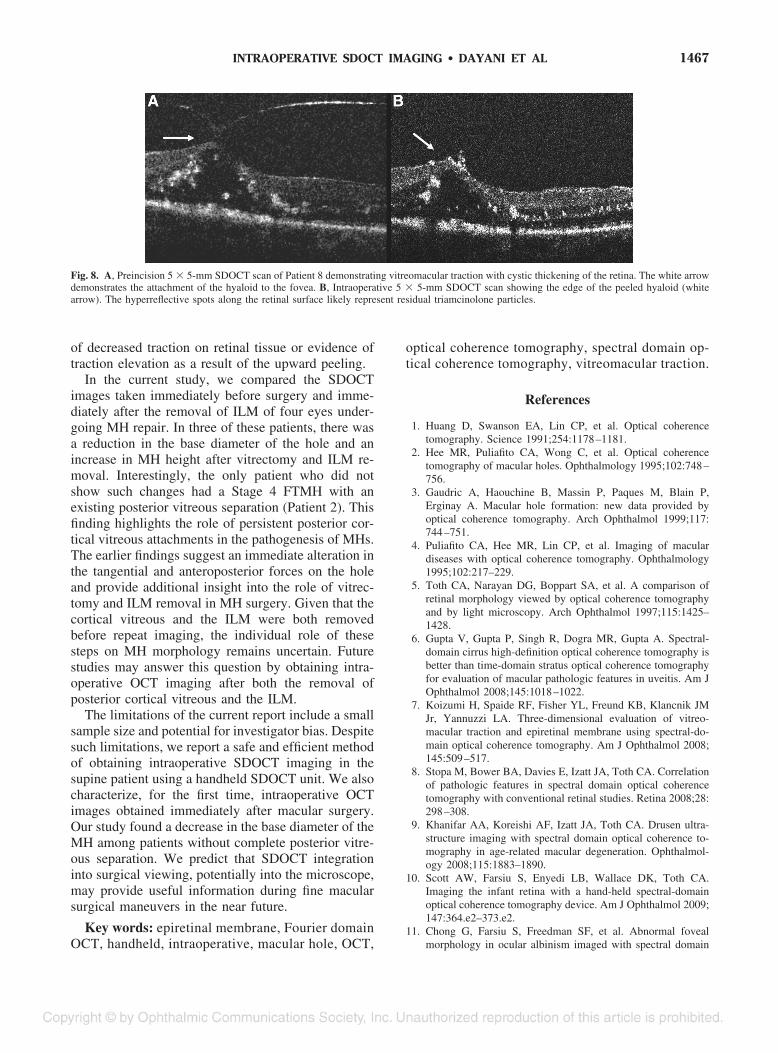
Among those undergoing surgery for ERM andVMT, definite alterations in the retinal contour wereseen after ERM/ILM peeling (Figures 4 and 7). In onepatient with ERM (Patient 6, Figure 7) and anotherwith VMT (Patient 8, Figure 8), an immediate nor-malization of the retinal contour was seen. In Patient7, there were multiple thin attachments between theretinal surface and the ERM (Figure 4A). Aftermembrane peeling, there was persistence of an ir-regular and corrugated retinal contour (Figure 4B).This appearance improved significantly on subsequentSDOCT imaging over the ensuing 4 weeks. In anotherpatient, an increased distortion of the retinal layerswas observed. Interestingly, the intraoperative imagesidentified residual membranes not visualized by theassistant surgeon during surgery in 2 patients, oneundergoing surgery for MH (Patient 2; Case 2, de-
Tab
le1.
Pat
ient
Dem
ogra
phi
csan
dS
urgi
calF
ind
ings
Pat
ient
Dem
ogra
phi
csS
urgi
calF
ind
ings
Cas
eG
end
erA
geE
tiolo
gyfo
rS
urge
ryP
ast
Ocu
lar
His
tory
Vis
ual
Acu
ityP
haki
cS
tatu
sP
VD
Gau
geof
Vitr
ecto
my
Com
ple
teP
VD
Vis
ualiz
atio
nA
id
Suc
cess
ful
Clo
sure
ofM
H
1F
58S
tage
3FT
MH
Non
e20
/50
Pha
kic
No
20N
oIC
GY
es2
F81
Sta
ge4
FTM
HA
MD
,C
E/I
OL
20/2
50–1
Pse
udop
haki
cY
es25
Yes
ICG
Yes
3M
68S
tage
3FT
MH
Fuch
sco
rnea
ld
ystr
ophy
20/3
00P
seud
opha
kic
No
20N
oIC
GY
es4
F69
Sta
ge3
FTM
HE
RM
,C
E/I
OL
HM
Pse
udop
haki
cN
o25
No
ICG
Yes
5M
70E
RM
BR
VO
,C
ME
20/8
0P
haki
cY
es25
Yes
PF
Ken
alog
N/A
6M
45E
RM
PD
R,
CM
E20
0E
Pha
kic
No
20N
oN
/AN
/A7
F55
ER
MN
one
20/6
4�P
haki
cY
es25
Yes
N/A
N/A
8M
62V
MT
PD
R,
CM
E,
CE
/IO
L20
/400
Pse
udop
haki
cY
es25
Yes
PF
Ken
alog
N/A
AM
D,
age-
rela
ted
mac
ular
deg
ener
atio
n;B
RV
O,
bra
nch
retin
alve
inoc
clus
ion;
CE
/IO
L,ca
tara
ctex
trac
tion
with
intr
aocu
lar
lens
;C
ME
,cy
stoi
dm
acul
ared
ema;
ER
M,
epire
tinal
mem
bra
ne;
F,fe
mal
e;FT
MH
,fu
llth
ickn
ess
mac
ular
hole
;M
,M
ale;
PD
R,
pro
lifer
ativ
ed
iab
etic
retin
opat
hy;
PF,
pre
serv
ativ
efr
ee;
PV
D,
pos
terio
rvi
treo
usd
etac
hmen
t;S
F6,
sulfu
rhe
xaflu
orid
e.
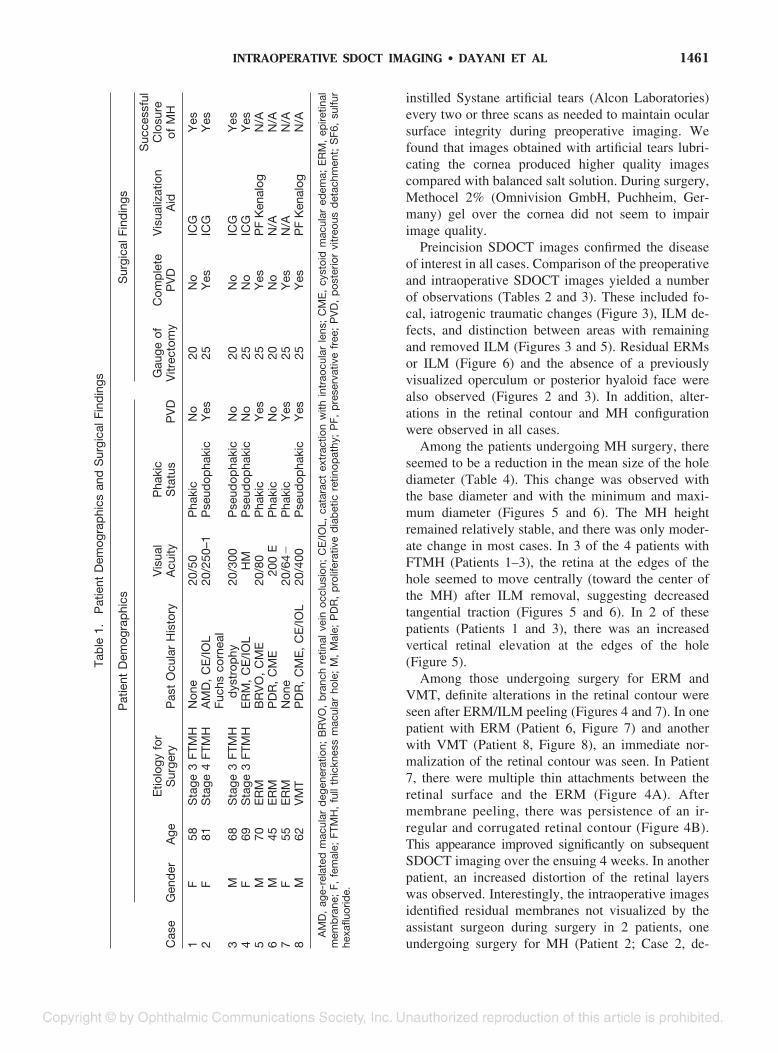
1461INTRAOPERATIVE SDOCT IMAGING ● DAYANI ET AL
scribed later) and another for ERM (Patient 7). Noimmediate postoperative complications were observedin any of the study patients. MH closure was attainedwith a single procedure in all patients undergoing MHrepair.
Case 1
A 58-year-old woman (Patient 1) with no ocularhistory presented with decreased vision and best-cor-rected visual acuity of 20/50. She was found to have aStage 3 FTMH, which was confirmed by OCT, andunderwent surgical repair.
Preincision, intraoperative SDOCT imaging con-firmed a FTMH with cystic thickening at the edges(Figure 2). There is a partial vitreous separation withpersistent attachments primarily inferiorly. Normalcontour and hyperreflectivity of the inner retinal lay-ers, including the ILM, can be appreciated.
Intraoperative images obtained after ILM removalshowed an area of irregular retinal contour inferonasalto the fovea with persistent hyaloidal attachment, de-creased reflectivity of the outer retinal layers, andshadowing (Figure 3). This area corresponds to themargin of ILM peeling and a focal intraretinal hem-orrhage that was appreciated intraoperatively. Sharpcontrast is observed between the hyperreflective areaswith persistent ILM and the adjacent retina where theILM was peeled. The intraoperative SDOCT imagesalso show that both edges of the hole are more verti-cally elevated compared with the preoperative scansand seem to be approaching one another (Figure 5).
Case 2
A pseudophakic 81-year-old woman (Patient 2)with a history of age-related macular degenerationpresented with vision loss in her better-seeing eye. On
Fig. 4. Spectral domain optical coherence tomography of Patient 7. A, Diffuse epiretinal membrane with focal area of discontinuity. Note multiplethin strands between the retinal surface and the membrane (white arrow). B, Irregular retinal contour with release of attachments after membranepeeling. C, SVP of preincision scan showing normal vessel appearance. D, SVP of preincision scan showing motion artifact and a broken vascularpattern.
1462 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10

Tab
le2.
Pre
-an
dIn
trao
per
ativ
eO
CT
Find
ings
inP
atie
nts
Und
ergo
ing
MH
Sur
gery
Pre
oper
ativ
eO
CT
Find
ings
Intr
aop
erat
ive
OC
TFi
ndin
gs
Cas
eN
o.E
RM
Vis
ualiz
eIL
MC
ME
SR
FO
per
culu
m/P
reho
leO
pac
ityA
dd
ition
alP
reop
erat
ive
Find
ings
Res
idua
lFo
veal
ILM
Res
idua
lE
RM
Cha
nge
inS
RF
Cha
nge
inC
ME
Cha
nge
inR
eflec
tivity
Iatr
ogen
icC
hang
es
1N
YY
NN
N/A
NN
/AN
YIn
crea
sed
ILM
RR
thic
keni
ngw
ithad
here
ntst
rand
(ILM
)at
edge
2N
YY
NN
N/A
YN
/AN
NN
N3
NY
YN
Y—
pos
terio
rhy
aloi
dfa
ceN
/AN
N/A
NN
NFo
cals
had
owin
gfr
omhe
me
atIL
Med
ge4
NY
YY
Y—
pos
terio
rhy
aloi
dfa
ceFo
calh
yper
Rat
RP
Ele
vel,
opac
ities
inm
id-l
evel
ofho
le
NN
NY
NN
CM
E,
cyst
oid
mac
ular
edem
a;N
,no
;N
/A,
not
app
licab
le;
R,
refle
ctiv
ity;
RP
E,
retin
alp
igm
ent
epith
eliu
m;
SR
F,su
bre
tinal
fluid
;Y
,ye
s.
Tab
le3.
Pre
inci
sion
and
Intr
aop
erat
ive
OC
TFi
ndin
gsin
Pat
ient
sU
nder
goin
gE
RM
Sur
gery
Cas
eN
o.E
RM
Cha
ract
eris
tics
Ret
inal
Con
tour
Cha
ract
eris
tics
ofH
yalo
idR
esid
ualC
entr
alE
RM
Ret
inal
Con
tour
Iatr
ogen
icFi
ndin
gs
5D
iffus
ew
ithou
tfo
cal
trac
tion
Irre
gula
rw
ithm
oder
ate
thic
keni
ngN
/AN
oIr
regu
lar
thic
keni
ngw
ithin
crea
sein
ragg
edap
pea
ranc
e;in
crea
sed
hyp
erre
flect
ivity
ofin
ner
retin
alla
yers
;fa
int
mem
bra
ne/
stra
nds
atfo
veal
edge
s
Foca
lexc
resc
ence
sw
ithsh
adow
ing;
edge
ofm
emb
rane
/ILM
dire
cted
ante
riorly
6D
iffus
ew
ithm
ultip
lefir
mat
tach
men
ts;
dou
ble
laye
rof
ER
M/s
chis
is
Rag
ged
cont
our;
diff
use
CM
Ew
ithla
rge
cyst
sH
yper
refle
ctiv
ityan
terio
rto
hyal
oid
face
No
Nor
mal
izat
ion
ofre
tinal
cont
our
with
red
uced
ragg
edap
pea
ranc
eTw
ofo
cale
xcre
scen
ces
with
shad
owin
g
7D
iffus
eE
RM
with
mul
tiple
,fo
cal,
firm
atta
chm
ents
;ar
eaof
dis
cont
inui
ty
Irre
gula
rth
icke
ning
;m
ultip
leat
tach
men
tto
ER
M
N/A
Res
idua
lper
ifove
alE
RM
Irre
gula
rw
ithp
ersi
sten
ttr
actio
nfr
omE
RM
and
per
sist
ence
ofra
gged
app
eara
nce
Foca
lret
inal
elev
atio
nw
ithsh
adow
ing
8D
iffus
ew
ithou
tfo
cal
trac
tion
Cys
ticed
ema
with
fove
altr
actio
nel
evat
ion;
hyp
erre
flect
ivity
ofou
ter
laye
rs
Foca
l,fir
mat
tach
men
tto
fove
alce
nter
No
Ab
senc
eof
foca
lele
vatio
n;d
iffus
eth
icke
ning
with
hyp
erre
flect
ivity
ofou
ter
laye
rs;
foca
lhyp
erre
flect
ive
dot
sal
ong
retin
alsu
rfac
e(p
ossi
bly
tria
mci
nolo
nep
artic
les)
Foca
lret
inal
elev
atio
n
CM
E,
cyst
oid
mac
ular
edem
a;N
/A,
not
app
licab
le.
1463INTRAOPERATIVE SDOCT IMAGING ● DAYANI ET AL
examination, visual acuity was 20/250 in the affectedeye, and there was nonfoveal geographic atrophy anda Stage 4 FTMH, which was confirmed by SDOCTimaging.
She subsequently underwent surgical repair. Afterinitial ILM removal, the surgeons disagreed as towhether further ILM remained at the upper margin ofthe hole. The intraoperative SDOCT images obtainedafter initial ILM removal demonstrated remainingmembrane that was partially separated and scrolled atthe temporal edge of the hole (Figure 6). On the basisof the indocyanine green angiography staining of thetissue and the scrolled appearance, the residual mem-brane was believed to be ILM. One feature of thisimage that is most striking is the contrast between thecontour of the hole margin where there is persistenttraction from remaining ILM and the hole edge that isfree of ILM. Surgery was resumed and the residualILM was removed. Repeat SDOCT intraoperative im-aging verified absence of the remaining ILM and ahole contour that appeared more elevated and lesstaut, confirming reduced tangential traction.
Discussion
In this study, we report the use of a handheldSDOCT unit to obtain preincision and intraoperative
images in patients undergoing macular surgery. To thebest of our knowledge, this is the first report of theintraoperative use of such technology. Imaging ob-tained during surgery provided unique informationregarding the location of persisting ILM or epiretinalmembrane. This served as a valuable teaching toolduring surgery to demonstrate findings to the surgicalassistant that were difficult to identify visually. Inaddition, interesting observations were made that con-firm and may expand our understanding of the patho-physiology of MHs. There was a learning curve inefficiently acquiring reliable images, and our abilityto obtain high-quality images improved consider-ably with time. Artificial tears, improved ability tohold the probe, and the understanding of how SVPswere displayed were factors that enhanced our im-aging capability.
Idiopathic FTMH affects approximately 0.3% ofpeople and results in reduced central vision.13 Opticalcoherence tomography is currently considered thegold standard for the diagnosis of MHs and has greatlycontributed to our understanding of its pathogenesisand response to therapy. Advances in MH surgeryhave led to improved surgical outcome and visualrecovery. Surgical repair typically involves pars planavitrectomy, removal of posterior cortical vitreous, and
Fig. 5. Comparison of the preoperative and intraoperative SDOCT of Patient 1 demonstrating change in the MH configuration. A, Preoperative imagedemonstrating a FTMH and cystic retinal thickening. The red lines depict the MH height and the base diameter. B, Postoperative scan showing a morepeaked appearance of the hole edge and a smaller base diameter. Also, note the distinction of the hyperreflectivity along the retinal surface in the areawith remaining ILM (white arrow) compared with the adjacent retina in which the ILM was removed.
1464 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10

infusion of expansile gas with postoperative pronepositioning. A meta-analysis on 1,654 eyes treatedusing different techniques reported an 87.5% ana-tomic success rate.14 Data suggest that removal of theILM may improve the anatomic success of MH repairby relieving tangential traction and by preventing pro-liferation of epiretinal tissue.15–20 Accordingly, amongeyes in which the ILM was not removed at the time ofsurgery, recurring ERMs seem to be the main cause ofMH reopening.21 In our series, residual ILM not vi-sualized by the assistant surgeon at the time of surgerywas identified on the intraoperative SDOCT imagingin one of four patients undergoing MH repair. Afterremoval of the residual ILM segment, there was adefinite change in the MH morphology (Figure 6).Given the apparent role of ILM in MH pathogenesis,and the difficulty in visualizing this structure duringsurgery, intraoperative SDOCT may prove to be auseful adjunct in select cases. This may provide analternative to the current technique of indocyaninegreen angiography staining, which has been associ-ated with ocular toxicity and vision loss.17,22–25 Intra-
operative SDOCT imaging also identified persistenttraction and distortion from residual membranes in apatient undergoing vitrectomy for ERM (Patient 7).Surgery was resumed and additional peeling was per-formed with relief of traction. In a previous publica-tion, we reported on a 6-month infant undergoingvitrectomy for a double layer of ERM.10 One monthafter the initial procedure, a deeper layer of remainingmembrane was identified on SDOCT, and a secondvitrectomy was performed. Intraoperative SDOCTmay, therefore, also be valuable in the managementof ERMs, in particular in cases with limited intra-operative visualization or double-layer (schisis)membranes.
In addition to clinical factors affecting surgical out-come, several studies have assessed the correlationbetween preoperative OCT findings and the anatomicand visual success of MH surgery. For example, OCTstudies suggest that the base and minimum diametersof MHs are predictive of postoperative success andthat visual results are adversely affected by increasinghole size.26,27 The significance of MH height and base
Fig. 6. Spectral domain optical coherence tomography of Patient 2 captured preoperatively and after initial and complete ILM removal. A, SVP froma 5 � 5-mm volumetric scan. B, Preoperative image showing a FTMH in an area of perifoveal geographic atrophy. C, Intraoperative images obtainedafter initial ILM removal show a “scrolled,” partially separated ILM at the margin of the MH. Note the difference in retinal contour at the right sideof the hole where the ILM is now absent compared with the left margin where the ILM persists. The red line depicts the maximum hole diameter.D, OCT scan after complete ILM removal shows a more elevated and less taut retinal morphology compared with previous scans with the MHapproaching closure.
1465INTRAOPERATIVE SDOCT IMAGING ● DAYANI ET AL

diameter was addressed by Kusuhara et al,28 usingOCT imaging, to calculate the MH index. The MHindex, defined as the greatest height of the hole (fromthe retinal pigment epithelium to the vitreoretinal in-terface) divided by its base diameter, was the onlyfactor identified in the study that significantly corre-lated with postoperative vision. This study found thata larger hole height and a smaller base diameter wereassociated with better visual outcome.28 These find-ings are supported by a study that showed a positivecorrelation between both the MH index and the trac-tional hole index (ratio of the maximal height to theminimum diameter) and visual outcome.29 On thecontrary, a study by Haritoglou et al30 found a nega-tive correlation between visual outcome and MHheight.
The success of repeat vitrectomy surgery for pa-tients with persistent FTMH has also been correlatedwith OCT configuration. Hillenkamp et al31 found thatthose with a cuff of subretinal fluid at the hole marginon OCT imaging had a higher success rate for ana-tomic closure and visual outcome. The size, type oftamponade, or duration of the hole before the initialsurgery did not seem to correlate with surgical out-come. The authors explain that the elevated configu-ration may facilitate the centripetal movement of ret-inal tissue over the fovea that is presumably necessaryfor hole closure. As opposed to the “stuck down”appearance, the increased height may be an indicator
Fig. 7. Spectral domain optical coherence tomography of Patient 6. A,Epiretinal membrane with multiple attachments (white arrows) andtraction. Note the corrugated retinal appearance between the attach-ments and the hyperreflective opacities anterior to the membrane. B,Decreased retinal traction after membrane peel (white arrows) withnormalization of the retinal contour.
Tab
le4.
Mea
sure
men
tof
Pre
inci
sion
and
Intr
aop
erat
ive
Hol
eD
imen
sion
s(in
mic
rons
)
Bas
eD
iam
eter
Max
imum
Dia
met
erM
inim
umD
iam
eter
Mac
ular
Hol
eH
eigh
tM
acul
arH
ole
Ind
ex
Cas
eP
rein
cisi
onIn
trao
pC
hang
eP
rein
cisi
onIn
trao
pC
hang
eP
rein
cisi
onIn
trao
pC
hang
eP
rein
cisi
onIn
trao
pC
hang
eP
rein
cisi
onIn
trao
p
184
067
0�
170
960
800
�16
070
051
1�
189
485
584
990.
580.
872
920
960
4093
087
1�
5991
879
0�
128
451
413
�38
0.49
0.43
311
1010
80�
3012
7111
57�
114
590
650
6075
884
183
0.68
0.78
410
9010
50�
4095
210
6010
833
048
015
069
971
415
0.64
0.68
Mea
n99
094
0�
5010
2897
2�
5663
560
8�
2759
863
840
Med
ian
1005
1005
095
696
610
645
581
�64
592
649
57S
.D.
131
187
162
165
245
142
153
183
Intr
aop
,In
trao
per
ativ
e.
1466 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10
of decreased traction on retinal tissue or evidence oftraction elevation as a result of the upward peeling.
In the current study, we compared the SDOCTimages taken immediately before surgery and imme-diately after the removal of ILM of four eyes under-going MH repair. In three of these patients, there wasa reduction in the base diameter of the hole and anincrease in MH height after vitrectomy and ILM re-moval. Interestingly, the only patient who did notshow such changes had a Stage 4 FTMH with anexisting posterior vitreous separation (Patient 2). Thisfinding highlights the role of persistent posterior cor-tical vitreous attachments in the pathogenesis of MHs.The earlier findings suggest an immediate alteration inthe tangential and anteroposterior forces on the holeand provide additional insight into the role of vitrec-tomy and ILM removal in MH surgery. Given that thecortical vitreous and the ILM were both removedbefore repeat imaging, the individual role of thesesteps on MH morphology remains uncertain. Futurestudies may answer this question by obtaining intra-operative OCT imaging after both the removal ofposterior cortical vitreous and the ILM.
The limitations of the current report include a smallsample size and potential for investigator bias. Despitesuch limitations, we report a safe and efficient methodof obtaining intraoperative SDOCT imaging in thesupine patient using a handheld SDOCT unit. We alsocharacterize, for the first time, intraoperative OCTimages obtained immediately after macular surgery.Our study found a decrease in the base diameter of theMH among patients without complete posterior vitre-ous separation. We predict that SDOCT integrationinto surgical viewing, potentially into the microscope,may provide useful information during fine macularsurgical maneuvers in the near future.
Key words: epiretinal membrane, Fourier domainOCT, handheld, intraoperative, macular hole, OCT,
optical coherence tomography, spectral domain op-tical coherence tomography, vitreomacular traction.
References
1. Huang D, Swanson EA, Lin CP, et al. Optical coherencetomography. Science 1991;254:1178–1181.
2. Hee MR, Puliafito CA, Wong C, et al. Optical coherencetomography of macular holes. Ophthalmology 1995;102:748–756.
3. Gaudric A, Haouchine B, Massin P, Paques M, Blain P,Erginay A. Macular hole formation: new data provided byoptical coherence tomography. Arch Ophthalmol 1999;117:744–751.
4. Puliafito CA, Hee MR, Lin CP, et al. Imaging of maculardiseases with optical coherence tomography. Ophthalmology1995;102:217–229.
5. Toth CA, Narayan DG, Boppart SA, et al. A comparison ofretinal morphology viewed by optical coherence tomographyand by light microscopy. Arch Ophthalmol 1997;115:1425–1428.
6. Gupta V, Gupta P, Singh R, Dogra MR, Gupta A. Spectral-domain cirrus high-definition optical coherence tomography isbetter than time-domain stratus optical coherence tomographyfor evaluation of macular pathologic features in uveitis. Am JOphthalmol 2008;145:1018–1022.
7. Koizumi H, Spaide RF, Fisher YL, Freund KB, Klancnik JMJr, Yannuzzi LA. Three-dimensional evaluation of vitreo-macular traction and epiretinal membrane using spectral-do-main optical coherence tomography. Am J Ophthalmol 2008;145:509–517.
8. Stopa M, Bower BA, Davies E, Izatt JA, Toth CA. Correlationof pathologic features in spectral domain optical coherencetomography with conventional retinal studies. Retina 2008;28:298–308.
9. Khanifar AA, Koreishi AF, Izatt JA, Toth CA. Drusen ultra-structure imaging with spectral domain optical coherence to-mography in age-related macular degeneration. Ophthalmol-ogy 2008;115:1883–1890.
10. Scott AW, Farsiu S, Enyedi LB, Wallace DK, Toth CA.Imaging the infant retina with a hand-held spectral-domainoptical coherence tomography device. Am J Ophthalmol 2009;147:364.e2–373.e2.
11. Chong G, Farsiu S, Freedman SF, et al. Abnormal fovealmorphology in ocular albinism imaged with spectral domain
Fig. 8. A, Preincision 5 � 5-mm SDOCT scan of Patient 8 demonstrating vitreomacular traction with cystic thickening of the retina. The white arrowdemonstrates the attachment of the hyaloid to the fovea. B, Intraoperative 5 � 5-mm SDOCT scan showing the edge of the peeled hyaloid (whitearrow). The hyperreflective spots along the retinal surface likely represent residual triamcinolone particles.
1467INTRAOPERATIVE SDOCT IMAGING ● DAYANI ET AL

optical coherence tomography. Arch Ophthalmol 2009;127:37–44.
12. Gordon RA, Donzis PB. Refractive development of the humaneye. Arch Ophthalmol 1985;103:785–789.
13. la Cour M, Friis J. Macular holes: classification, epidemiology,natural history and treatment. Acta Ophthalmol Scand 2002;80:579–587.
14. Mester V, Kuhn F. Internal limiting membrane removal in themanagement of full-thickness macular holes. Am J Ophthal-mol 2000;129:769–777.
15. Kwok AK, Lai TY, Yuen KS, Tam BS, Wong VW. Macularhole surgery with or without indocyanine green stained inter-nal limiting membrane peeling. Clin Experiment Ophthalmol2003;31:470–475.
16. Smiddy WE, Feuer W, Cordahi G. Internal limiting membranepeeling in macular hole surgery. Ophthalmology 2001;108:1471–1476; discussion 1477–1478.
17. Tognetto D, Grandin R, Sanguinetti G, et al. Internal limitingmembrane removal during macular hole surgery: results of amulticenter retrospective study. Ophthalmology 2006;113:1401–1410.
18. Uemoto R, Yamamoto S, Aoki T, Tsukahara I, Yamamoto T,Takeuchi S. Macular configuration determined by optical co-herence tomography after idiopathic macular hole surgery withor without internal limiting membrane peeling. Br J Ophthal-mol 2002;86:1240–1242.
19. Ando F, Sasano K, Ohba N, Hirose H, Yasui O. Anatomic andvisual outcomes after indocyanine green-assisted peeling ofthe retinal internal limiting membrane in idiopathic macularhole surgery. Am J Ophthalmol 2004;137:609–614.
20. Brooks HL Jr. Macular hole surgery with and without internallimiting membrane peeling. Ophthalmology 2000;107:1939–1948; discussion 1948–1949.
21. Yoshida M, Kishi S. Pathogenesis of macular hole recurrenceand its prevention by internal limiting membrane peeling.Retina 2007;27:169–173.
22. Engelbrecht NE, Freeman J, Sternberg P Jr, et al. Retinalpigment epithelial changes after macular hole surgery withindocyanine green-assisted internal limiting membrane peel-ing. Am J Ophthalmol 2002;133:89–94.
23. Gass CA, Haritoglou C, Schaumberger M, Kampik A. Func-tional outcome of macular hole surgery with and withoutindocyanine green-assisted peeling of the internal limitingmembrane. Graefes Arch Clin Exp Ophthalmol 2003;241:716–720.
24. Kanda S, Uemura A, Yamashita T, Kita H, Yamakiri K,Sakamoto T. Visual field defects after intravitreous adminis-tration of indocyanine green in macular hole surgery. ArchOphthalmol 2004;122:1447–1451.
25. Miura M, Elsner AE, Osako M, Iwasaki T, Okano T, Usui M.Dissociated optic nerve fiber layer appearance after internallimiting membrane peeling for idiopathic macular hole. Retina2003;23:561–563.
26. Ip MS, Baker BJ, Duker JS, et al. Anatomical outcomes ofsurgery for idiopathic macular hole as determined by opticalcoherence tomography. Arch Ophthalmol 2002;120:29–35.
27. Ullrich S, Haritoglou C, Gass C, Schaumberger M, Ulbig MW,Kampik A. Macular hole size as a prognostic factor in macularhole surgery. Br J Ophthalmol 2002;86:390–393.
28. Kusuhara S, Teraoka Escano MF, Fujii S, et al. Prediction ofpostoperative visual outcome based on hole configuration byoptical coherence tomography in eyes with idiopathic macularholes. Am J Ophthalmol 2004;138:709–716.
29. Ruiz-Moreno JM, Staicu C, Pinero DP, Montero J, Lugo F,Amat P. Optical coherence tomography predictive factors for mac-ular hole surgery outcome. Br J Ophthalmol 2008;92:640–644.
30. Haritoglou C, Neubauer AS, Reiniger IW, Priglinger SG, GassCA, Kampik A. Long-term functional outcome of macularhole surgery correlated to optical coherence tomography mea-surements. Clin Experiment Ophthalmol 2007;35:208–213.
31. Hillenkamp J, Kraus J, Framme C, et al. Retreatment offull-thickness macular hole: predictive value of optical coher-ence tomography. Br J Ophthalmol 2007;91:1445–1449.
1468 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 10