Initial Treatment Nov2009 [Autosaved]
47
Initial Treatment of Tuberculosis Makiyatul BBKPM Surakarta International Standards 7, 8, 10, 13,
-
Upload
santifaridkaluku -
Category
Documents
-
view
231 -
download
0
description
treatment
Transcript of Initial Treatment Nov2009 [Autosaved]
PowerPoint Presentation
Initial Treatment of TuberculosisMakiyatul BBKPM SurakartaInternational Standards 7, 8, 10, 13, 17, 21 ISTC TB Training Modules 20091Instructors Guide and Teaching Notes
Module: Initial Treatment of TuberculosisISTC Standards covered: 7, 8, 10, 13, 17, and 21Module Time: Approximately 60 minutes
Alternate slides: Introductory ISTC slidesInteractive options: Ideas for interactive discussions are offered on many of the slides in this module. Participant discussion can enhance active learning, but will add more time to the lecture and must be planned for.Additional Material: Slides containing related material may be found in the following modules: TB and HIV Infection: Treatment, Management of Drug-resistant Tuberculosis. Test Questions: May be attached or inserted within presentation for discussion purposes, or alternatively, combined with questions from other modules to produce evaluation tool.
The full text of the ISTC and all supporting references are available at www.istcweb.orgOther useful Resources/References:Treatment of Tuberculosis: Guidelines for National Programmes, Third Edition. World Health Organization, 2003. www.who.int/tbATS/CDC/IDSA Statement: Treatment of Tuberculosis. American Thoracic Society/Centers for Disease Control/Infectious Diseases Society of America, Am J Respir Crit Care Med 2003; 167(4):603-62. www.thoracic.orgTomans tuberculosis. Case detection, treatment and monitoring, 2nd Edition. Freiden TR ed., World Health Organization, 2004. www.who.int/tbSaukkonen JJ, et al. An official ATS statement: Hepatotoxicity of antituberculosis drugs. Am J Resp Crit Care Med 2006; 174(8): 935-52
[Image Credit: World Lung Foundation/Gary Hampton] ISTC TB Training Modules 2009Initial Treatment of TuberculosisObjectives: At the end of this presentation,participants will have an understanding of:Drug regimens used in the initial treatment of both pulmonary and extrapulmonary tuberculosisThe basis for the public health benefits of treating tuberculosisThe clinical and microbiological effects of treatmentThe rationale for patient monitoring and reportingThe main adverse effects of antituberculosis drugsISTC TB Training Modules 20092It is intended that after completion of this module the student will be able to describe the approach to and rationale for the initial treatment of tuberculosis.
These objectives represent the key points in the presentation. [Review content of slide]
ISTC TB Training Modules 2009Initial Treatment of TuberculosisOverview:Effect of appropriate treatment on public healthFirst-line treatment recommendationsTreatment of extrapulmonary tuberculosisMonitoring of treatmentAdverse reactionsRecording and reportingInternational Standards 7, 8, 10, 13, 17, and 21
ISTC TB Training Modules 20093Initial Treatment of Tuberculosis
Overview: [Review content of slide]
Lecture/module includes International Standards for Tuberculosis Care 7, 8, 10, 13, 17, and 21.
[Image credits: World Lung Foundation/Gary Hampton (top); Erlina Burhan, MD, Persahabatan Hospital (bottom)] ISTC TB Training Modules 2009Standards for TreatmentISTC TB Training Modules 20094This slide emphasizes the fact that treatment for TB is both a matter of individual health and public health and that adherence to treatment must be assured to have confidence that the patient will be cured. Assessing adherence and addressing poor adherence may (likely will) require collaboration between the provider and a program or facility that is capable of ensuring adherence.The main interventions to prevent the spread of TB in the community are the detection of patients with infectious TB and providing them with effective treatment to ensure a rapid and lasting cure. Consequently, treatment for TB is not only a matter of individual health, it is also a matter of public health.
[Image credit: World Lung Foundation/Gary Hampton] ISTC TB Training Modules 2009 Initial Treatment of TuberculosisStandards 7 & 8ISTC TB Training Modules 20095Standards 7 and 8 relate to treatment of the new, previously untreated case of TB.
The information relates to both pulmonary and extrapulmonary TB, although most of the public health issues relate to pulmonary TB. Differences in the treatment of extrapulmonary TB are presented at the end of the discussion.
The photos include a chest radiograph showing extensive bilateral upper lobe opacities consistent with TB and a patient with lymph node TB (swelling and erythema of an anterior cervical node together with a sinus tract from spontaneous rupture of a supraclavicular node).
[Image credits: Francis J. Curry National Tuberculosis Center, University of California, San Francisco (top); Austin Brewin, MD (bottom).]
ISTC TB Training Modules 2009
Standard 7: Public Health ResponsibilityAny practitioner treating a patient for tuberculosis is assuming an important public health responsibility to prevent ongoing transmission of the infection and the development of drug resistance. To fulfill this responsibility the practitioner must not only prescribe an appropriate regimen, but also utilize local public health services and other agencies, when necessary, to assess the adherence of the patient and to address poor adherence when it occurs.ISTC TB Training Modules 20096ISTC Training Modules 20086[Read Standard]
Standard 7 emphasizes that treatment for TB is both a matter of individual health and public health and that it is the responsibility of the provider to both prescribe the correct regimen and to ensure adherence to the regimen.
Assessing adherence and addressing poor adherence may (likely will) require collaboration between the provider and a program or facility that is capable of ensuring adherence.
ISTC TB Training Modules 2009Effect of Treatment on Public HealthWhy is TB Treatment a Public Health Measure? Effective treatment rapidly kills organisms, reducing the bacillary population in respiratory secretions, thus reducing the potential for transmission. Effective multiple-drug treatment greatly reduces the risk of resistant organisms emerging.Effective treatment decreases the duration and severity of illness and reduces the risk of death.ISTC TB Training Modules 20097The main interventions to prevent the spread of TB in the community are the detection of patients with infectious TB and providing them with effective treatment to ensure a rapid and lasting cure. Consequently, treatment for TB is not only a matter of individual health, such as is provided by, for example, treatment of hypertension or diabetes mellitus, it is also a matter of public health.All providers, public and private, who undertake to treat a patient with TB, must have the knowledge to prescribe a standard treatment regimen and the means to ensure adherence to the regimen until treatment is completed.National or local TB programs commonly possess mechanisms and tools to ensure adherence with treatment and, when properly organized, can offer these to non-program providers. Failure of a provider to ensure adherence could be equated with, for example, failure to ensure that a child receives the full set of immunizations. Communities and patients deserve to be assured that providers treating TB are doing so in accordance with this principle and are, thereby, meeting this standard. ISTC TB Training Modules 2009Effect of Treatment on Public Health
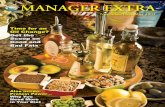
10012014016018020022019801985199019952000Pulmonary TB cases/100,000DOTS 1990PTB falling at 6%/yr case findingEffects of Treatment on the Incidence of Tuberculosis in PeruISTC TB Training Modules 20098This slide shows the effect of an effective drug regimen that was closely supervised to ensure adherence.
Peru began a DOTS program in late 1990. Because of the increased coverage of the program, more cases were found and, initially, case rates increased. However with the continued effectiveness of the program case rates began falling at the rate of approximately 6% per year.
Because of the decrease in case rates, Peru graduated from the list of 22 high-burden TB countries.
[The module Fostering and Assessing Adherence to Treatment describes approaches to enhance patient adherence and treatment supervision.] ISTC TB Training Modules 2009
Standard 8: Initiation of Treatment
All patients (including those with HIV infection) who have not been treated previously should receive an internationally accepted first-line treatment regimen using drugs of known bioavailability. The initial phase should consist of two months of isoniazid (INH), rifampicin (RIF), pyrazinamide (PZA), and ethambutol (EMB).(1 of 2)ISTC TB Training Modules 20099ISTC Training Modules 20089Standard 8 contains several concepts and has been divided into 2 parts. [Read Standard]This part describes the most widely-used and effective initial phase of the initial drug regimen. There are 3 major points to be made with this slide: An accurate history is critical. Patients who have been treated previously have a greater risk of drug resistance and are assessed as described in Standard 11 [Drug-resistant Tuberculosis module]. The drugs used must be quality assured with known bioavailabiity. Poor quality drugs are common and lead to poor outcomes. For maximum efficacy, 4 drugs should be given in the initial phase.A large number of well-designed clinical trials have provided the evidence base for this standard and several sets of treatment recommendations based on these studies have been written in the past few years. All these data indicate that a rifampicin-containing regimen is the backbone of antituberculosis chemotherapy and is highly effective in treating TB caused by drug-susceptible M. tuberculosis. It is also clear from these studies that the minimum duration of treatment for smear and/or culture-positive TB is six months. For the six-month treatment duration to be maximally effective, the regimen must include pyrazinamide during the initial two-month phase and rifampicin must be included throughout the full six months. There are several variations in the frequency of drug administration that have been shown to produce acceptable results.
[Image credit: World Lung Foundation/Gary Hampton]9 ISTC TB Training Modules 2009Mixed population (susceptible and resistant)INH resistant bacilli Emergence of INH resistant strain because of ineffective treatment (INH monotherapy)Effective multi-drug therapyEffect of Treatment on Bacillary PopulationWeeksLog cfu024681012141618202224ISTC TB Training Modules 200910Effective multi-drug treatment rapidly reduces the bacillary population. Within 2 weeks of beginning appropriate chemotherapy the number of organisms in sputum is decreased from ~107 (107 would be a typical number of bacilli to find in the sputum of a person with cavitary pulmonary TB) to 104 (104 is the approximate threshold for detecting acid fast organisms by sputum smear microscopy).
This greatly decreases (but does not completely eliminate) the potential for transmission. Further treatment beyond the initial period is intended to kill the remaining organisms that persist through the initial period.
In all populations of M.tb there is a small number of organisms that are resistant to each of the drugs used. If treatment does not contain at least two drugs to which the organisms are susceptible, a bacillary population that is resistant to one or more of the first line drugs emerges.
ISTC TB Training Modules 2009Months of Rx0579INHRIFEMBSmear++++Culture++++SusceptibilityINHR*RRRRIFS*RRREMBS*SSR* Results not known to clinicianUnintended Monotherapy and ResistanceISTC TB Training Modules 200911In this hypothetical example a patient is begun on treatment with an initial 2 drug regimen, a clear mistake. The organisms were initially resistant to isoniazid, although the treating provider was unaware of this. After 5 months of treatment, the smear was still positive and the organisms had become resistant to rifampicin because the resistance to isoniazid prevented the eradication of the few organisms that were rifampicin resistant and the rifampicin resistant strain proliferated. Again the provider was not aware of the resistance that had occurred. Because the smear was still positive, the provider added ethambutol. This is also a clear mistake. A single drug should never be added to a failing regimen. A sputum specimen, after 9 months of treatment, was still positive. In effect the patient had been treated with ethambutol alone for the last 4 months of the regimen and the organisms that were resistant to ethambutol proliferated. This result would have been prevented if a regimen of isoniazid, rifampicin, ethambutol and pyrazinamide had been used in the initial 2 months of treatment. [Interactive option: This is a very important concept in the management of TB treatment. Stop to ask if there are any questions or clarifications needed.] ISTC TB Training Modules 2009Treatment GoalsMicrobiological Goals of Antituberculosis Chemotherapy Kill tubercle bacilli rapidly (early bactericidal effect)Prevent the emergence of drug resistanceEliminate persistent bacilli to prevent relapse (sterilizing effect)ISTC TB Training Modules 200912The previous slides presented the individual and public health goals of treatment for TB.
This slide defines the microbiological goals of treatment. [Review content of slide]
Antituberculosis drugs operate in a complimentary way to accomplish these goals as shown in the next slide.
ISTC TB Training Modules 2009Activities of Antituberculosis Drugs Highest ++++ High +++ Intermediate ++ Low + DrugEarly bactericidal activityPreventing drug resistanceSterilizing activityIsoniazid+++++++++Rifampicin+++++++++Pyrazinamide+++++Streptomycin++++++Ethambutol++ - ++++++ISTC TB Training Modules 200913This table shows the relative activities of the first line antituberculosis drugs.
Isoniazid has the most potent early bactericidal effect and is also effective in preventing resistance, but has less sterilizing effect. Rifampicin has a weaker early effect but is more potent than isoniazid in its sterilizing activity. Pyrazinamide is only effective as a sterilizing agent. [Note: relatively poor agent for prevention of drug resistance]Streptomycin has an intermediate effect in all three activities as does ethambutol. ISTC TB Training Modules 2009
Standard 8: Continuation of TreatmentThe continuation phase should consist of isoniazid and rifampicin given for four monthsThe doses of antituberculosis drugs used should conform to international recommendations
Fixed-dose combinations (FDCs) of two (INH and RIF), three (INH, RIF, and PZA), and four (INH, RIF, PZA, and EMB) drugs are highly recommended(2 of 2)ISTC TB Training Modules 20091414Standard 8 continued: [Read Standard]The second part of Standard 8 describes the continuation phase regimen. First, the major point is that it is preferable to use rifampicin throughout the continuation phase. [Previous recommendations for a continuation phase of six months of isoniazid and ethambutol is no longer recommended (WHO 2009 pending publication).]A review of the outcomes of treatment of TB in patients with HIV infection clearly shows that TB relapse is minimized by the use of a regimen containing rifampicin throughout a six-month course. Thus, the 6 month regimen containing rifampicin throughout the entire course is preferable in patients with HIV infection to minimize the risk of relapse; however, the patients HIV stage, the need for, and availability of, antiretroviral drugs, and the quality of treatment supervision/support must be considered in choosing an appropriate continuation phase of therapy.Second, the shortest total duration of treatment is 6 months. Although regimens of less than 6 months have been evaluated in clinical trials, a Cochrane systematic review on this topic, and a more recent review found that regimens

![1. initial plans [autosaved]](https://static.fdocuments.net/doc/165x107/58cfca3e1a28ab7c6e8b5641/1-initial-plans-autosaved.jpg)