Infections Caused by HRSV A ON1 Are Predominant...
8
Research Article Infections Caused by HRSV A ON1 Are Predominant among Hospitalized Infants with Bronchiolitis in São Paulo City Sandra E. Vieira, 1 Luciano M. Thomazelli, 2 Milena de Paulis, 3 Angela E. Ferronato, 3 Daniele B. Oliveira, 2 Marina Baquerizo Martinez, 4 and Edison L. Durigon 2 1 Faculdade de Medicina da Universidade de S˜ ao Paulo, S˜ ao Paulo, SP, Brazil 2 Instituto de Ciˆ encias Biom´ edicas da Universidade de S˜ ao Paulo, S˜ ao Paulo, SP, Brazil 3 Hospital Universit´ ario da Universidade de S˜ ao Paulo, S˜ ao Paulo, SP, Brazil 4 Faculdade de Ciˆ encias Farmacˆ euticas da Universidade de S˜ ao Paulo, S˜ ao Paulo, SP, Brazil Correspondence should be addressed to Sandra E. Vieira; [email protected] Received 5 January 2017; Revised 10 April 2017; Accepted 2 May 2017; Published 24 May 2017 Academic Editor: Elena Pariani Copyright © 2017 Sandra E. Vieira et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Human respiratory syncytial virus is the main cause of respiratory infections in infants. Several HRSV genotypes have been described. Goals. To describe the main genotypes that caused infections in S˜ ao Paulo (2013–2015) and to analyze their clinical/epidemiological features. Methods. 94 infants (0–6 months) with bronchiolitis were studied. Clinical/epidemiological information was collected; a search for 16 viruses in nasopharyngeal secretion (PCR-real-time and conventional, sequencing, and phylogenetic analyses) was performed. Results. e mean age was 2.4 m; 48% were male. e mean length of hospital stay was 4.4 d (14% in the Intensive Care Unit). e positive rate of respiratory virus was 98.9%; 73 cases (77.6%) were HRSV (76,7% HRSVA). HRSVA formed three clusters: ON1 ( = 34), NA1 (=1), and NA2 (=4). All HRSVB were found to cluster in the BA genotype (BA9- = 10; BA10-=3). Clinical analyses showed no significant differences between the genotype AON1 and other genotypes. Conclusion. is study showed a high rate of HRSV detection in bronchiolitis. HRSVA ON1, which has recently been described in other countries and has not been identified in previous studies in the southeast region of Brazil, was predominant. e clinical characteristics of the infants that were infected with AON1 were similar to infants with infections by other genotypes. 1. Introduction HRSV infections are frequent worldwide, and the most severe cases mainly affect children during the first year of life, elderly and immunocompromised individuals. HRSV is the most common causal agent of respiratory infections in infants, which occur at predictable annual seasons [1, 2]. HRSV is an enveloped virus (genus Orthopneumovirus, family Pneumoviridae) [3]. Its genome consists of a nonseg- mented single-stranded RNA that encodes 11 proteins. e surface proteins F and G are important antigenic targets of neutralizing antibodies. Variations in the G protein and in the gene regions that encode this protein allowed for the classification of HRSV into two subgroups (A and B) and into many genotypes. Different HRSV genotypes of the two subgroups generally cocirculate during a season in the same region, and the predominant genotypes are replaced by others in subsequent years [4, 5]. Such antigenic and genetic variability allows the virus to escape immunity acquired by the population of patients that have been subjected to previous infections. Several genotypes have been described in subgroups A (GA1 to GA7, SAA1 and NA1, NA2) and B (URU1, URU2, and GB1 to GB4, SAB1 to SAB3, and BA1 to BA13). e recently described genotype HRSV A ON1 is characterized by the duplication of 72 nucleotides in gene G. Aſter being reported in Canada, HRSVA ON1 has also been identified in Europe, India, Africa, South America, and Asia [6–11]. Knowledge on the molecular epidemiology of HRSV infections is important to assess the clinical implications of infections by different genotypes. e clinical presenta- tion, severity, response to treatment, and prophylaxis are Hindawi BioMed Research International Volume 2017, Article ID 3459785, 7 pages https://doi.org/10.1155/2017/3459785
Transcript of Infections Caused by HRSV A ON1 Are Predominant...

Research ArticleInfections Caused by HRSV A ON1 Are Predominant amongHospitalized Infants with Bronchiolitis in Satildeo Paulo City
Sandra E Vieira1 LucianoM Thomazelli2 Milena de Paulis3 Angela E Ferronato3
Daniele B Oliveira2 Marina Baquerizo Martinez4 and Edison L Durigon2
1Faculdade de Medicina da Universidade de Sao Paulo Sao Paulo SP Brazil2Instituto de Ciencias Biomedicas da Universidade de Sao Paulo Sao Paulo SP Brazil3Hospital Universitario da Universidade de Sao Paulo Sao Paulo SP Brazil4Faculdade de Ciencias Farmaceuticas da Universidade de Sao Paulo Sao Paulo SP Brazil
Correspondence should be addressed to Sandra E Vieira sandrahuuspbr
Received 5 January 2017 Revised 10 April 2017 Accepted 2 May 2017 Published 24 May 2017
Academic Editor Elena Pariani
Copyright copy 2017 Sandra E Vieira et alThis is an open access article distributed under theCreative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Human respiratory syncytial virus is the main cause of respiratory infections in infants Several HRSV genotypes have beendescribed Goals To describe the main genotypes that caused infections in Sao Paulo (2013ndash2015) and to analyze theirclinicalepidemiological features Methods 94 infants (0ndash6 months) with bronchiolitis were studied Clinicalepidemiologicalinformation was collected a search for 16 viruses in nasopharyngeal secretion (PCR-real-time and conventional sequencing andphylogenetic analyses) was performed Results Themean age was 24m 48 were maleThemean length of hospital stay was 44 d(14 in the Intensive Care Unit) The positive rate of respiratory virus was 989 73 cases (776) were HRSV (767 HRSVA)HRSVA formed three clusters ON1 (119899 = 34) NA1 (119899 = 1) and NA2 (119899 = 4) All HRSVB were found to cluster in the BA genotype(BA9-119899 = 10 BA10-119899 = 3) Clinical analyses showed no significant differences between the genotype AON1 and other genotypesConclusion This study showed a high rate of HRSV detection in bronchiolitis HRSVA ON1 which has recently been describedin other countries and has not been identified in previous studies in the southeast region of Brazil was predominant The clinicalcharacteristics of the infants that were infected with AON1 were similar to infants with infections by other genotypes
1 Introduction
HRSV infections are frequent worldwide and themost severecasesmainly affect children during the first year of life elderlyand immunocompromised individuals HRSV is the mostcommon causal agent of respiratory infections in infantswhich occur at predictable annual seasons [1 2]
HRSV is an enveloped virus (genus Orthopneumovirusfamily Pneumoviridae) [3] Its genome consists of a nonseg-mented single-stranded RNA that encodes 11 proteins Thesurface proteins F and G are important antigenic targets ofneutralizing antibodies Variations in the G protein and inthe gene regions that encode this protein allowed for theclassification of HRSV into two subgroups (A and B) andinto many genotypes Different HRSV genotypes of the twosubgroups generally cocirculate during a season in the same
region and the predominant genotypes are replaced by othersin subsequent years [4 5]
Such antigenic and genetic variability allows the virus toescape immunity acquired by the population of patients thathave been subjected to previous infections Several genotypeshave been described in subgroups A (GA1 to GA7 SAA1and NA1 NA2) and B (URU1 URU2 and GB1 to GB4SAB1 to SAB3 and BA1 to BA13) The recently describedgenotype HRSV A ON1 is characterized by the duplicationof 72 nucleotides in gene G After being reported in CanadaHRSVAON1 has also been identified in Europe India AfricaSouth America and Asia [6ndash11]
Knowledge on the molecular epidemiology of HRSVinfections is important to assess the clinical implicationsof infections by different genotypes The clinical presenta-tion severity response to treatment and prophylaxis are
HindawiBioMed Research InternationalVolume 2017 Article ID 3459785 7 pageshttpsdoiorg10115520173459785
2 BioMed Research International
among these implications The occurrence of genotypesthat have not been previously identified leads to concernsabout the severity of new cases or an increased number ofinfected individuals when considering the possible absenceof immunological memory in the affected population
In this study the authors describe the main genotypesof HRSV A and B which caused infections in infantshospitalized in the University Hospital of Universidade deSao Paulo in Sao Paulo city from 2013 to 2015 The genotypecharacteristics and clinical and epidemiological features ofHRSV are analyzed and the infections caused by the newgenotype HRSV AON1 are compared to other genotypes thatwere circulating during the study period To our knowledgethis is the first report to perform an analysis of the associationbetween clinical features and genotypes in infections causedby HRSV A ON1 in the southeast region of Brazil
2 Methods
This study included 124 infants aged between zero and sixmonths with diagnoses of bronchiolitis that were admittedto the Pediatric Clinic Division of the University Hospitalof the University of Sao Paulo between 2013 and 2015 Theinfants were enrolled in the study by one of the authors(MP) who collected nasopharyngeal secretions after writtenconsent was obtained from the childrsquos parents On exami-nation the clinical and socioeconomic backgrounds clinicalsignssymptoms and diagnosis at admission were recordedon a standard form Diagnosis of bronchiolitis was definedas the first wheezing crisis beginning no more than 3 daysbefore hospital admission
For clinical analysis infants diagnosed with or suspectedof having bacterial or fungal infections and those whoreceived antibiotics macrolides or antifungals prior to orduring hospitalization were excluded Infants with code-tection of respiratory viruses were also excluded from theclinical analysis
The project was approved by the Research Ethics Com-mittee of the University Hospital of the University of SaoPaulo (101110) and was funded by Fundacao de Amparo aPesquisa do Estado de Sao Paulo (1222854-9)
Nasal wash fluid was obtained after washing the nostrilswith 3ml of a saline solution and collecting the suctionedspecimen in a cup within a maximum of 24 hours afteradmission The samples were shipped within 48 hours underrefrigeration and analyzed at the Laboratory of Clinicaland Molecular Virology of Institute of Biomedical SciencesUniversity of Sao Paulo by in-house singleplex real-timeRT-PCR assays for the detection of 16 common respiratoryviruses (HRSV A and B human rhinovirus enterovirushuman metapneumovirus parainfluenza virus 1 2 3 and4 adenovirus influenza virus A and B bocavirus andcoronavirus OC43 NL63 HKU1 and 229E) Viral RNA wasextracted with an automatic NucliSens easyMAG extractor(Biomerieux Inc Durham NC USA) according to themanufacturerrsquos instructions The one-step qPCR was carriedout with the AgPath-ID one-step RT-PCR kit in the 7300Real-Time PCR System (Applied Biosystems Foster CityCA USA) with primers previously described by Sakthivel etal 2012
HRSV-positive samples were amplified by traditionalPCR in two steps for DNA sequencing cDNA was synthe-sized using the Super Script III kit (Applied BiosystemsFoster City CA USA) according to the manufacturerrsquosinstructions The second hypervariable region of the G pro-tein gene PCR was carried out with the primers Gr5_fwd (51015840-CTGGCAATGATAATCTCAACTTC-31015840) and FV_rev (51015840-GTTATGACACTGGTATACCAACC-31015840) in a 10 120583L mixturethat contained 5 120583L of 10x PCR buffer 25mM of eachdNTP 25 pmol of each primer and 15U of Platinum TaqDNA Polymerase (Invitrogen Carlsbad CA USA) for afinal volume of 50 120583L The amplification was performedin a GeneAmp PCR System 9700 thermocycler (AppliedBiosystems Foster City CA USA) A second step withSeminested PCR was carried out using the F1AB_rev (51015840-CAACTCCATTGTTATTTGCC-31015840) primer correspondingto bases 3ndash22 of the F gene The traditional PCR assayswere performed with the following program 95∘C for 5minutes followed by 35 cycles each composed of 30 secat 95∘C 30 sec at 55∘C and 45 sec at 72∘C and finally 7minutes of extension at 72∘C The amplified products wereanalyzed by agarose gel electrophoresis and visualized underUV light after staining with ethidium bromideThe amplifiedproducts of gene G were asymp490 bp were purified by ExoSap-IT (Affymetrix Inc USA) and were submitted to a cyclesequencing reaction (Sanger) using the Bigdye terminatorkit (Applied Biosystems Foster City CA USA) and GR5FV or F1AB primers in a 3100 DNA Sequencer (AppliedBiosystems Foster City CA USA) Both strands of eachamplicon were sequenced at least twice Sequence editingalignments and phylogenetic analyses were performed withMegAlign 503 v software (DNAStar Inc Madison Wiscon-sin USA) Standard published sequences from subgroupsA (accession numbers from KY828387 to KY828428) andB (accession numbers from KY828374 to KY828386) weredownloaded fromGenBank as references of different lineagesand genotypes
21 Statistical Analysis The results of the analyses of the clin-ical and demographic characteristics as well as the categoricalvariables are presented as absolute numbers and percentagesand the continuous variables are presented as the means andstandard deviations For studies of the associations betweenthe categorical variables the chi-square test and Fisherrsquosexact test were used For associations between the continuousvariables Studentrsquos 119905-test was used The null hypothesis wasrejected when the probability was less than 5 (119875 lt 005)We used IBM SPSS Statistic software version 23
3 Results
Of the 124 infants selected 94 were studied after the exclusionof 30 cases (infants with clinical diagnoses or suspicion ofinfection by bacteria or other agents as well as those whoreceived antibiotics)
The mean age of the infants was 24 months (SD = 16)and 48 were male The mean length of hospital stay was 44days (SD = 36) and 14 were admitted to the Intensive CareUnit The positivity of respiratory virus detection was 989
BioMed Research International 3
500
9643
21112111 287
11
HRSVHRVPV
FLU AHKUHMPV
OC43CodetectionRV neg
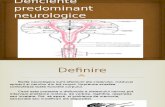
Figure 1 Etiological analysis of the 94 cases of bronchiolitisin infants younger than 6 months HRSV = human respiratorysyncytial virus HRV= human rhinovirus PV= parainfluenza virusFlu A = influenza virus A HKU = coronavirus HKU HMPV =human metapneumovirus OC43 = coronavirus OC43 RV neg =result was negative for respiratory viruses
73 (776) samples were positive for HRSV 47 were single-agent and 26 showed codetection with other respiratoryviruses Cocirculation of HRSV A and B was observed witha predominance of HRSVA (767) The results of the viralagent searches in the studied 94 cases of HRSV are shown inFigures 1 and 2
Fifty-two samples of HRSV were sequenced (34 A ON110 BA9 4 NA2 3 BA10 and 1 NA1) Genotype trees arepresented in Figures 3 and 4 The HRSV A isolates formedthree clusters (NA1 NA2 and ON1 genotypes) most of theHRSVA isolates were found to cluster in the ON1 genotypeTheON1 cluster included 40 isolates theNA1 cluster included2 isolates and the NA2 cluster included 4 isolates Theyshowed a 0004ndash0113 sequence p-distance at the nucleotidelevel but there was a 0000ndash0175 p-distance at the aminoacid level compared to the ON1 prototype strain (JN257694)The sequenced HRSVB isolates were found to cluster in theBA genotype The HRSV B isolates formed two subclustersidentified as the BA-9 and BA-10 genotypes The BA-9cluster included 10 isolates and the BA-10 cluster included3 isolates They showed a 0026ndash0052 sequence p-distance atthe nucleotide level but there was a 0045ndash0084 p-distanceat the amino acid level compared to the BA prototype strain(AY333362)
The comparative clinical analyses included 32 infantswitha HRSV single infection (22 AON1 and 10 other genotypes)and showed no significant differences between these sub-groups (Table 1)
4 Discussion
The present study showed the strong predominance of HRSVinfections in infants hospitalized with bronchiolitis predom-inance of the HRSVA ON1 genotype and occurrence of theNA1 andNA2 genotypes previously unidentified in southeastregion of Brazil
The high occurrence of HRSV among infants wasexpected due to the inclusion criteria that selected children
259
22274
74
37
74
185
37 37
HRSV + HRVHRSV + PVHRSV + FLU AHRSV + HMPVHRSV + OC43
HRSV + NL63HRSV + ADVHRSV + EnteroHRV + PV
Figure 2 Etiological analysis of 27 cases with respiratory viruscodetection HRSV = human respiratory syncytial virus HRV =human rhinovirus PV= parainfluenza virus FluA= influenza virusA HKU = coronavirus HKU HMPV = human metapneumovirusOC43 = coronavirus OC43 NL63 = coronavirus NL63 ADV =adenovirus Entero = enterovirus
under 6 months old and the exclusion of those who haddiagnoses or suspicion of infection by nonviral agents In factHRSV is recognized as the most frequent etiologic agent inbronchiolitis during the first year of life [1]
The use of molecular methods for conducting viralresearch in the selected cases showed low occurrences of 6other respiratory viruses and a high prevalence of respiratoryvirus codetections most of which involved HRSV whichwas the main viral agent in both single infections and incodetection
Cocirculation of HRSV A and B was observed with apredominance ofHRSVA (767) as reported inmost studiesconducted in other countries [5 7 12] Previous studiesperformed by this group of researchers in the same serviceshowed the cocirculation of different genotypes of HRSV Aand B during the same viral season An analysis from 1995 to2006 showed the predominance of group B only in 1999 inthe State of Sao Paulo [13]
After genotype HRSV A ON1 BA9 was the secondmost frequent genotype identified in the present studyThe genotypes that predominated in previous seasons werenot detected such as GB1 GB3 GA2 and GA5 In aprevious study the authors included HRSV samples thatwere collected from hospitalized children in the State ofSao Paulo until seven years before this study They showedimportant nucleotide substitutions in the GA2 genotype thatare genetically close to the NA1 andNA2 genotypes identifiedhere between 2013 and 2015 [14]
Since the first year of the study (2013) the genotypeHRSVA ON1 was predominant but the genotypes NA1 andNA2 and genotypes BA9 and BA10 also circulated In sub-sequent years (2014 and 2015) the genotype ON1 remainedpredominant and a unique representative of HRSV A butthere was cocirculation with the BA9 and BA10 genotypeswith predominance of the BA9 genotype among HRSV B
4 BioMed Research International
PEG52PEG15
PEG57
PEG55
PEG56 PEG23
FJ210830_NA1
HQ731741_NA1 JF920053_NA2
PEG105 PEG79 PEG80 PEG82
PEG6 PEG100
PEG16 PEG8
newONl PEG10 PEG45 PEG13 PEG44
PEG35 PEG40
PEG31 PEG32 PEG18
PEG63 PEG24 PEG29
PEG38 PEG92
PEG51 PEG2 PEG19 PEG12 PEG1 PEG36
PEG39 PEG61
PEG90 PEG27 PEG54
M74568_GA1 AF065250_GB1_out
AF065410_GA6AF193327_GA7
JF920065_GA7 DQ171791_SAA1
AF065255_GA5JF920058_GA5
AF065406_GA5AF065254_GA4
AF233921_GA3 CN2395_GA3
Z33416_GA3AF233915_GA2
TX69554_GA2 AY344660_GA2
HQ731737_GA2 AF065257_GA1
50
ON1
NA2
NA1
Figure 3 Genotype tree the topology of the HRSV A tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype ON1 Clades in blue show samples thatbelong to genotype NA2 and clades in green show samples that belong to genotype NA1
In molecular analysis most of the sequenced HRSVAisolates were found to cluster in the ON1 genotype withprototype reference strain JN257694 whichwas first reportedin Ontario Canada [6] The sequenced isolates had thesignature 72-bp duplication in the G protein when alignedwith representative sequences from all of the A subgroup(GA1 to GA7 NA1 NA2 and ON1) from GenBank TheBrazilianHRSVA isolatesweremost closely related to isolatesfrom the United States Kenya and New Zealand
All of the sequenced HRSVB isolates were found tocluster in the BA genotype with prototype BA referencestrain AY333362 which was first reported in Buenos AiresArgentina [15] The sequenced isolates had the signature 60-bp duplication in the G protein when aligned with represen-tative sequences from all of the B subgroup (GB1 to GB4SAB1 to SAB4 URU1 and URU2 and BA-1 to BA-13) fromGenBank The Brazilian HRSV B isolates were most closelyrelated to isolates from the United States New Zealand andVietnam
Some authors suggest the occurrence of a greater numberof cases during seasons inwhich new genotypes predominateThis could be a result of the absence of immunity acquired bythe population against the new genotypes [4 15] GenotypeA ON1 shows a duplication of 72 nucleotides in the C-terminal third of the G gene The region of the G proteinencoded by this gene sequence is targeted by specific geno-type neutralizing antibodies which may contribute to theescape of the virus from the population immunity induced byprevious contact with other genotypes However accordingto the National Registry of Hospitalization Cases there wasno increase in the frequency of hospitalizations of infantsdiagnosed with bronchiolitis between 2013 and 2015 in Braziland the State of Sao Paulo compared to the previous five years[16] It is possible that acting as a controller the immunity ofthe population only contributes to the selection of genotypesthat replace each other without necessarily increasing thenumber of cases when genotypes without recent incidencesappear
BioMed Research International 5
PEG11PEG4PEG7PEG9
PEG108PEG118
PEG115PEG83
PEG42DQ227395_BA9
PEG62PEG84
PEG98 PEG22
JF714708_BA10 DQ985142_BA7 DQ227396_BA4
DQ227370_BA3 DQ227387_BA3 DQ227389_BA2
AY751108_BA5 AY751117_BA6
AY333362_BA1 DQ227380_BA1
AY488805_URU1 AF065252_GB3
DQ270231_SAB4AY327815_SAB2
DQ171866_SAB3 AY333361_URU2
JF704213_SAB1 AF065250_GB1
AF065251_GB2DQ171853_GB4
AF065257_RSVA_out
40
BA9
BA10
Figure 4 Genotype tree the topology of the HRSV B tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype BA10 Clades in blue show samples thatbelong to genotype BA9
The demographic and clinical characteristics of theinfants that were infected with genotype AON1 were similarto the characteristics of the other genotypes Exclusionof infants with viral codetection and those who receivedantimicrobials during hospitalization made it possible toavoid confounding factors in the comparative analysis of theseverity between the genotypes
A mean age at 2 months showed the precocity of theinfection which was independent of the infecting genotypeClinical characteristics that could differentiate the initialpresentation such as the presence of cough fever dyspneaand apnea crises also showed similar prevalence among thegenotypes Some prognostic factors that are relevant in respi-ratory infections in infants were also similar such as exposureto tobacco smoke and breastfeeding Severity as analyzedby the hospitalization time need and duration of oxygentherapy and mechanical ventilation and hospitalization inthe Intensive Care Unit was also similar regardless of theinfecting genotype
Despite the limited number of cases the results suggestthat the HRSV A ON1 genotype was not associated withspecific clinical characteristics and was therefore clinicallyindistinguishable from the other genotypes These resultsneed to be confirmed by more extensive analyses but areconsistent with a previous German study that found no clin-ical differences between infections by other HRSV genotypes[17] Althoughnucleotide variation in this region is importantfor viral antigenicity other regions may be more relevantdeterminants of infection severity In addition other factorsinherent to the host and the environmentmust be considered[18]
On the other hand an epidemiological study carriedout in Vietnam compared community-acquired infectionsand nosocomially acquired infections and showed a greaterseverity of the respiratory condition in children infectedwith HRSV ON1 compared to those infected with NA1with consideration of the clinical severity and occurrenceof pneumonia In that study all children used antibiotics
6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

2 BioMed Research International
among these implications The occurrence of genotypesthat have not been previously identified leads to concernsabout the severity of new cases or an increased number ofinfected individuals when considering the possible absenceof immunological memory in the affected population
In this study the authors describe the main genotypesof HRSV A and B which caused infections in infantshospitalized in the University Hospital of Universidade deSao Paulo in Sao Paulo city from 2013 to 2015 The genotypecharacteristics and clinical and epidemiological features ofHRSV are analyzed and the infections caused by the newgenotype HRSV AON1 are compared to other genotypes thatwere circulating during the study period To our knowledgethis is the first report to perform an analysis of the associationbetween clinical features and genotypes in infections causedby HRSV A ON1 in the southeast region of Brazil
2 Methods
This study included 124 infants aged between zero and sixmonths with diagnoses of bronchiolitis that were admittedto the Pediatric Clinic Division of the University Hospitalof the University of Sao Paulo between 2013 and 2015 Theinfants were enrolled in the study by one of the authors(MP) who collected nasopharyngeal secretions after writtenconsent was obtained from the childrsquos parents On exami-nation the clinical and socioeconomic backgrounds clinicalsignssymptoms and diagnosis at admission were recordedon a standard form Diagnosis of bronchiolitis was definedas the first wheezing crisis beginning no more than 3 daysbefore hospital admission
For clinical analysis infants diagnosed with or suspectedof having bacterial or fungal infections and those whoreceived antibiotics macrolides or antifungals prior to orduring hospitalization were excluded Infants with code-tection of respiratory viruses were also excluded from theclinical analysis
The project was approved by the Research Ethics Com-mittee of the University Hospital of the University of SaoPaulo (101110) and was funded by Fundacao de Amparo aPesquisa do Estado de Sao Paulo (1222854-9)
Nasal wash fluid was obtained after washing the nostrilswith 3ml of a saline solution and collecting the suctionedspecimen in a cup within a maximum of 24 hours afteradmission The samples were shipped within 48 hours underrefrigeration and analyzed at the Laboratory of Clinicaland Molecular Virology of Institute of Biomedical SciencesUniversity of Sao Paulo by in-house singleplex real-timeRT-PCR assays for the detection of 16 common respiratoryviruses (HRSV A and B human rhinovirus enterovirushuman metapneumovirus parainfluenza virus 1 2 3 and4 adenovirus influenza virus A and B bocavirus andcoronavirus OC43 NL63 HKU1 and 229E) Viral RNA wasextracted with an automatic NucliSens easyMAG extractor(Biomerieux Inc Durham NC USA) according to themanufacturerrsquos instructions The one-step qPCR was carriedout with the AgPath-ID one-step RT-PCR kit in the 7300Real-Time PCR System (Applied Biosystems Foster CityCA USA) with primers previously described by Sakthivel etal 2012
HRSV-positive samples were amplified by traditionalPCR in two steps for DNA sequencing cDNA was synthe-sized using the Super Script III kit (Applied BiosystemsFoster City CA USA) according to the manufacturerrsquosinstructions The second hypervariable region of the G pro-tein gene PCR was carried out with the primers Gr5_fwd (51015840-CTGGCAATGATAATCTCAACTTC-31015840) and FV_rev (51015840-GTTATGACACTGGTATACCAACC-31015840) in a 10 120583L mixturethat contained 5 120583L of 10x PCR buffer 25mM of eachdNTP 25 pmol of each primer and 15U of Platinum TaqDNA Polymerase (Invitrogen Carlsbad CA USA) for afinal volume of 50 120583L The amplification was performedin a GeneAmp PCR System 9700 thermocycler (AppliedBiosystems Foster City CA USA) A second step withSeminested PCR was carried out using the F1AB_rev (51015840-CAACTCCATTGTTATTTGCC-31015840) primer correspondingto bases 3ndash22 of the F gene The traditional PCR assayswere performed with the following program 95∘C for 5minutes followed by 35 cycles each composed of 30 secat 95∘C 30 sec at 55∘C and 45 sec at 72∘C and finally 7minutes of extension at 72∘C The amplified products wereanalyzed by agarose gel electrophoresis and visualized underUV light after staining with ethidium bromideThe amplifiedproducts of gene G were asymp490 bp were purified by ExoSap-IT (Affymetrix Inc USA) and were submitted to a cyclesequencing reaction (Sanger) using the Bigdye terminatorkit (Applied Biosystems Foster City CA USA) and GR5FV or F1AB primers in a 3100 DNA Sequencer (AppliedBiosystems Foster City CA USA) Both strands of eachamplicon were sequenced at least twice Sequence editingalignments and phylogenetic analyses were performed withMegAlign 503 v software (DNAStar Inc Madison Wiscon-sin USA) Standard published sequences from subgroupsA (accession numbers from KY828387 to KY828428) andB (accession numbers from KY828374 to KY828386) weredownloaded fromGenBank as references of different lineagesand genotypes
21 Statistical Analysis The results of the analyses of the clin-ical and demographic characteristics as well as the categoricalvariables are presented as absolute numbers and percentagesand the continuous variables are presented as the means andstandard deviations For studies of the associations betweenthe categorical variables the chi-square test and Fisherrsquosexact test were used For associations between the continuousvariables Studentrsquos 119905-test was used The null hypothesis wasrejected when the probability was less than 5 (119875 lt 005)We used IBM SPSS Statistic software version 23
3 Results
Of the 124 infants selected 94 were studied after the exclusionof 30 cases (infants with clinical diagnoses or suspicion ofinfection by bacteria or other agents as well as those whoreceived antibiotics)
The mean age of the infants was 24 months (SD = 16)and 48 were male The mean length of hospital stay was 44days (SD = 36) and 14 were admitted to the Intensive CareUnit The positivity of respiratory virus detection was 989
BioMed Research International 3
500
9643
21112111 287
11
HRSVHRVPV
FLU AHKUHMPV
OC43CodetectionRV neg
Figure 1 Etiological analysis of the 94 cases of bronchiolitisin infants younger than 6 months HRSV = human respiratorysyncytial virus HRV= human rhinovirus PV= parainfluenza virusFlu A = influenza virus A HKU = coronavirus HKU HMPV =human metapneumovirus OC43 = coronavirus OC43 RV neg =result was negative for respiratory viruses
73 (776) samples were positive for HRSV 47 were single-agent and 26 showed codetection with other respiratoryviruses Cocirculation of HRSV A and B was observed witha predominance of HRSVA (767) The results of the viralagent searches in the studied 94 cases of HRSV are shown inFigures 1 and 2
Fifty-two samples of HRSV were sequenced (34 A ON110 BA9 4 NA2 3 BA10 and 1 NA1) Genotype trees arepresented in Figures 3 and 4 The HRSV A isolates formedthree clusters (NA1 NA2 and ON1 genotypes) most of theHRSVA isolates were found to cluster in the ON1 genotypeTheON1 cluster included 40 isolates theNA1 cluster included2 isolates and the NA2 cluster included 4 isolates Theyshowed a 0004ndash0113 sequence p-distance at the nucleotidelevel but there was a 0000ndash0175 p-distance at the aminoacid level compared to the ON1 prototype strain (JN257694)The sequenced HRSVB isolates were found to cluster in theBA genotype The HRSV B isolates formed two subclustersidentified as the BA-9 and BA-10 genotypes The BA-9cluster included 10 isolates and the BA-10 cluster included3 isolates They showed a 0026ndash0052 sequence p-distance atthe nucleotide level but there was a 0045ndash0084 p-distanceat the amino acid level compared to the BA prototype strain(AY333362)
The comparative clinical analyses included 32 infantswitha HRSV single infection (22 AON1 and 10 other genotypes)and showed no significant differences between these sub-groups (Table 1)
4 Discussion
The present study showed the strong predominance of HRSVinfections in infants hospitalized with bronchiolitis predom-inance of the HRSVA ON1 genotype and occurrence of theNA1 andNA2 genotypes previously unidentified in southeastregion of Brazil
The high occurrence of HRSV among infants wasexpected due to the inclusion criteria that selected children
259
22274
74
37
74
185
37 37
HRSV + HRVHRSV + PVHRSV + FLU AHRSV + HMPVHRSV + OC43
HRSV + NL63HRSV + ADVHRSV + EnteroHRV + PV
Figure 2 Etiological analysis of 27 cases with respiratory viruscodetection HRSV = human respiratory syncytial virus HRV =human rhinovirus PV= parainfluenza virus FluA= influenza virusA HKU = coronavirus HKU HMPV = human metapneumovirusOC43 = coronavirus OC43 NL63 = coronavirus NL63 ADV =adenovirus Entero = enterovirus
under 6 months old and the exclusion of those who haddiagnoses or suspicion of infection by nonviral agents In factHRSV is recognized as the most frequent etiologic agent inbronchiolitis during the first year of life [1]
The use of molecular methods for conducting viralresearch in the selected cases showed low occurrences of 6other respiratory viruses and a high prevalence of respiratoryvirus codetections most of which involved HRSV whichwas the main viral agent in both single infections and incodetection
Cocirculation of HRSV A and B was observed with apredominance ofHRSVA (767) as reported inmost studiesconducted in other countries [5 7 12] Previous studiesperformed by this group of researchers in the same serviceshowed the cocirculation of different genotypes of HRSV Aand B during the same viral season An analysis from 1995 to2006 showed the predominance of group B only in 1999 inthe State of Sao Paulo [13]
After genotype HRSV A ON1 BA9 was the secondmost frequent genotype identified in the present studyThe genotypes that predominated in previous seasons werenot detected such as GB1 GB3 GA2 and GA5 In aprevious study the authors included HRSV samples thatwere collected from hospitalized children in the State ofSao Paulo until seven years before this study They showedimportant nucleotide substitutions in the GA2 genotype thatare genetically close to the NA1 andNA2 genotypes identifiedhere between 2013 and 2015 [14]
Since the first year of the study (2013) the genotypeHRSVA ON1 was predominant but the genotypes NA1 andNA2 and genotypes BA9 and BA10 also circulated In sub-sequent years (2014 and 2015) the genotype ON1 remainedpredominant and a unique representative of HRSV A butthere was cocirculation with the BA9 and BA10 genotypeswith predominance of the BA9 genotype among HRSV B
4 BioMed Research International
PEG52PEG15
PEG57
PEG55
PEG56 PEG23
FJ210830_NA1
HQ731741_NA1 JF920053_NA2
PEG105 PEG79 PEG80 PEG82
PEG6 PEG100
PEG16 PEG8
newONl PEG10 PEG45 PEG13 PEG44
PEG35 PEG40
PEG31 PEG32 PEG18
PEG63 PEG24 PEG29
PEG38 PEG92
PEG51 PEG2 PEG19 PEG12 PEG1 PEG36
PEG39 PEG61
PEG90 PEG27 PEG54
M74568_GA1 AF065250_GB1_out
AF065410_GA6AF193327_GA7
JF920065_GA7 DQ171791_SAA1
AF065255_GA5JF920058_GA5
AF065406_GA5AF065254_GA4
AF233921_GA3 CN2395_GA3
Z33416_GA3AF233915_GA2
TX69554_GA2 AY344660_GA2
HQ731737_GA2 AF065257_GA1
50
ON1
NA2
NA1
Figure 3 Genotype tree the topology of the HRSV A tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype ON1 Clades in blue show samples thatbelong to genotype NA2 and clades in green show samples that belong to genotype NA1
In molecular analysis most of the sequenced HRSVAisolates were found to cluster in the ON1 genotype withprototype reference strain JN257694 whichwas first reportedin Ontario Canada [6] The sequenced isolates had thesignature 72-bp duplication in the G protein when alignedwith representative sequences from all of the A subgroup(GA1 to GA7 NA1 NA2 and ON1) from GenBank TheBrazilianHRSVA isolatesweremost closely related to isolatesfrom the United States Kenya and New Zealand
All of the sequenced HRSVB isolates were found tocluster in the BA genotype with prototype BA referencestrain AY333362 which was first reported in Buenos AiresArgentina [15] The sequenced isolates had the signature 60-bp duplication in the G protein when aligned with represen-tative sequences from all of the B subgroup (GB1 to GB4SAB1 to SAB4 URU1 and URU2 and BA-1 to BA-13) fromGenBank The Brazilian HRSV B isolates were most closelyrelated to isolates from the United States New Zealand andVietnam
Some authors suggest the occurrence of a greater numberof cases during seasons inwhich new genotypes predominateThis could be a result of the absence of immunity acquired bythe population against the new genotypes [4 15] GenotypeA ON1 shows a duplication of 72 nucleotides in the C-terminal third of the G gene The region of the G proteinencoded by this gene sequence is targeted by specific geno-type neutralizing antibodies which may contribute to theescape of the virus from the population immunity induced byprevious contact with other genotypes However accordingto the National Registry of Hospitalization Cases there wasno increase in the frequency of hospitalizations of infantsdiagnosed with bronchiolitis between 2013 and 2015 in Braziland the State of Sao Paulo compared to the previous five years[16] It is possible that acting as a controller the immunity ofthe population only contributes to the selection of genotypesthat replace each other without necessarily increasing thenumber of cases when genotypes without recent incidencesappear
BioMed Research International 5
PEG11PEG4PEG7PEG9
PEG108PEG118
PEG115PEG83
PEG42DQ227395_BA9
PEG62PEG84
PEG98 PEG22
JF714708_BA10 DQ985142_BA7 DQ227396_BA4
DQ227370_BA3 DQ227387_BA3 DQ227389_BA2
AY751108_BA5 AY751117_BA6
AY333362_BA1 DQ227380_BA1
AY488805_URU1 AF065252_GB3
DQ270231_SAB4AY327815_SAB2
DQ171866_SAB3 AY333361_URU2
JF704213_SAB1 AF065250_GB1
AF065251_GB2DQ171853_GB4
AF065257_RSVA_out
40
BA9
BA10
Figure 4 Genotype tree the topology of the HRSV B tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype BA10 Clades in blue show samples thatbelong to genotype BA9
The demographic and clinical characteristics of theinfants that were infected with genotype AON1 were similarto the characteristics of the other genotypes Exclusionof infants with viral codetection and those who receivedantimicrobials during hospitalization made it possible toavoid confounding factors in the comparative analysis of theseverity between the genotypes
A mean age at 2 months showed the precocity of theinfection which was independent of the infecting genotypeClinical characteristics that could differentiate the initialpresentation such as the presence of cough fever dyspneaand apnea crises also showed similar prevalence among thegenotypes Some prognostic factors that are relevant in respi-ratory infections in infants were also similar such as exposureto tobacco smoke and breastfeeding Severity as analyzedby the hospitalization time need and duration of oxygentherapy and mechanical ventilation and hospitalization inthe Intensive Care Unit was also similar regardless of theinfecting genotype
Despite the limited number of cases the results suggestthat the HRSV A ON1 genotype was not associated withspecific clinical characteristics and was therefore clinicallyindistinguishable from the other genotypes These resultsneed to be confirmed by more extensive analyses but areconsistent with a previous German study that found no clin-ical differences between infections by other HRSV genotypes[17] Althoughnucleotide variation in this region is importantfor viral antigenicity other regions may be more relevantdeterminants of infection severity In addition other factorsinherent to the host and the environmentmust be considered[18]
On the other hand an epidemiological study carriedout in Vietnam compared community-acquired infectionsand nosocomially acquired infections and showed a greaterseverity of the respiratory condition in children infectedwith HRSV ON1 compared to those infected with NA1with consideration of the clinical severity and occurrenceof pneumonia In that study all children used antibiotics
6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 3
500
9643
21112111 287
11
HRSVHRVPV
FLU AHKUHMPV
OC43CodetectionRV neg
Figure 1 Etiological analysis of the 94 cases of bronchiolitisin infants younger than 6 months HRSV = human respiratorysyncytial virus HRV= human rhinovirus PV= parainfluenza virusFlu A = influenza virus A HKU = coronavirus HKU HMPV =human metapneumovirus OC43 = coronavirus OC43 RV neg =result was negative for respiratory viruses
73 (776) samples were positive for HRSV 47 were single-agent and 26 showed codetection with other respiratoryviruses Cocirculation of HRSV A and B was observed witha predominance of HRSVA (767) The results of the viralagent searches in the studied 94 cases of HRSV are shown inFigures 1 and 2
Fifty-two samples of HRSV were sequenced (34 A ON110 BA9 4 NA2 3 BA10 and 1 NA1) Genotype trees arepresented in Figures 3 and 4 The HRSV A isolates formedthree clusters (NA1 NA2 and ON1 genotypes) most of theHRSVA isolates were found to cluster in the ON1 genotypeTheON1 cluster included 40 isolates theNA1 cluster included2 isolates and the NA2 cluster included 4 isolates Theyshowed a 0004ndash0113 sequence p-distance at the nucleotidelevel but there was a 0000ndash0175 p-distance at the aminoacid level compared to the ON1 prototype strain (JN257694)The sequenced HRSVB isolates were found to cluster in theBA genotype The HRSV B isolates formed two subclustersidentified as the BA-9 and BA-10 genotypes The BA-9cluster included 10 isolates and the BA-10 cluster included3 isolates They showed a 0026ndash0052 sequence p-distance atthe nucleotide level but there was a 0045ndash0084 p-distanceat the amino acid level compared to the BA prototype strain(AY333362)
The comparative clinical analyses included 32 infantswitha HRSV single infection (22 AON1 and 10 other genotypes)and showed no significant differences between these sub-groups (Table 1)
4 Discussion
The present study showed the strong predominance of HRSVinfections in infants hospitalized with bronchiolitis predom-inance of the HRSVA ON1 genotype and occurrence of theNA1 andNA2 genotypes previously unidentified in southeastregion of Brazil
The high occurrence of HRSV among infants wasexpected due to the inclusion criteria that selected children
259
22274
74
37
74
185
37 37
HRSV + HRVHRSV + PVHRSV + FLU AHRSV + HMPVHRSV + OC43
HRSV + NL63HRSV + ADVHRSV + EnteroHRV + PV
Figure 2 Etiological analysis of 27 cases with respiratory viruscodetection HRSV = human respiratory syncytial virus HRV =human rhinovirus PV= parainfluenza virus FluA= influenza virusA HKU = coronavirus HKU HMPV = human metapneumovirusOC43 = coronavirus OC43 NL63 = coronavirus NL63 ADV =adenovirus Entero = enterovirus
under 6 months old and the exclusion of those who haddiagnoses or suspicion of infection by nonviral agents In factHRSV is recognized as the most frequent etiologic agent inbronchiolitis during the first year of life [1]
The use of molecular methods for conducting viralresearch in the selected cases showed low occurrences of 6other respiratory viruses and a high prevalence of respiratoryvirus codetections most of which involved HRSV whichwas the main viral agent in both single infections and incodetection
Cocirculation of HRSV A and B was observed with apredominance ofHRSVA (767) as reported inmost studiesconducted in other countries [5 7 12] Previous studiesperformed by this group of researchers in the same serviceshowed the cocirculation of different genotypes of HRSV Aand B during the same viral season An analysis from 1995 to2006 showed the predominance of group B only in 1999 inthe State of Sao Paulo [13]
After genotype HRSV A ON1 BA9 was the secondmost frequent genotype identified in the present studyThe genotypes that predominated in previous seasons werenot detected such as GB1 GB3 GA2 and GA5 In aprevious study the authors included HRSV samples thatwere collected from hospitalized children in the State ofSao Paulo until seven years before this study They showedimportant nucleotide substitutions in the GA2 genotype thatare genetically close to the NA1 andNA2 genotypes identifiedhere between 2013 and 2015 [14]
Since the first year of the study (2013) the genotypeHRSVA ON1 was predominant but the genotypes NA1 andNA2 and genotypes BA9 and BA10 also circulated In sub-sequent years (2014 and 2015) the genotype ON1 remainedpredominant and a unique representative of HRSV A butthere was cocirculation with the BA9 and BA10 genotypeswith predominance of the BA9 genotype among HRSV B
4 BioMed Research International
PEG52PEG15
PEG57
PEG55
PEG56 PEG23
FJ210830_NA1
HQ731741_NA1 JF920053_NA2
PEG105 PEG79 PEG80 PEG82
PEG6 PEG100
PEG16 PEG8
newONl PEG10 PEG45 PEG13 PEG44
PEG35 PEG40
PEG31 PEG32 PEG18
PEG63 PEG24 PEG29
PEG38 PEG92
PEG51 PEG2 PEG19 PEG12 PEG1 PEG36
PEG39 PEG61
PEG90 PEG27 PEG54
M74568_GA1 AF065250_GB1_out
AF065410_GA6AF193327_GA7
JF920065_GA7 DQ171791_SAA1
AF065255_GA5JF920058_GA5
AF065406_GA5AF065254_GA4
AF233921_GA3 CN2395_GA3
Z33416_GA3AF233915_GA2
TX69554_GA2 AY344660_GA2
HQ731737_GA2 AF065257_GA1
50
ON1
NA2
NA1
Figure 3 Genotype tree the topology of the HRSV A tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype ON1 Clades in blue show samples thatbelong to genotype NA2 and clades in green show samples that belong to genotype NA1
In molecular analysis most of the sequenced HRSVAisolates were found to cluster in the ON1 genotype withprototype reference strain JN257694 whichwas first reportedin Ontario Canada [6] The sequenced isolates had thesignature 72-bp duplication in the G protein when alignedwith representative sequences from all of the A subgroup(GA1 to GA7 NA1 NA2 and ON1) from GenBank TheBrazilianHRSVA isolatesweremost closely related to isolatesfrom the United States Kenya and New Zealand
All of the sequenced HRSVB isolates were found tocluster in the BA genotype with prototype BA referencestrain AY333362 which was first reported in Buenos AiresArgentina [15] The sequenced isolates had the signature 60-bp duplication in the G protein when aligned with represen-tative sequences from all of the B subgroup (GB1 to GB4SAB1 to SAB4 URU1 and URU2 and BA-1 to BA-13) fromGenBank The Brazilian HRSV B isolates were most closelyrelated to isolates from the United States New Zealand andVietnam
Some authors suggest the occurrence of a greater numberof cases during seasons inwhich new genotypes predominateThis could be a result of the absence of immunity acquired bythe population against the new genotypes [4 15] GenotypeA ON1 shows a duplication of 72 nucleotides in the C-terminal third of the G gene The region of the G proteinencoded by this gene sequence is targeted by specific geno-type neutralizing antibodies which may contribute to theescape of the virus from the population immunity induced byprevious contact with other genotypes However accordingto the National Registry of Hospitalization Cases there wasno increase in the frequency of hospitalizations of infantsdiagnosed with bronchiolitis between 2013 and 2015 in Braziland the State of Sao Paulo compared to the previous five years[16] It is possible that acting as a controller the immunity ofthe population only contributes to the selection of genotypesthat replace each other without necessarily increasing thenumber of cases when genotypes without recent incidencesappear
BioMed Research International 5
PEG11PEG4PEG7PEG9
PEG108PEG118
PEG115PEG83
PEG42DQ227395_BA9
PEG62PEG84
PEG98 PEG22
JF714708_BA10 DQ985142_BA7 DQ227396_BA4
DQ227370_BA3 DQ227387_BA3 DQ227389_BA2
AY751108_BA5 AY751117_BA6
AY333362_BA1 DQ227380_BA1
AY488805_URU1 AF065252_GB3
DQ270231_SAB4AY327815_SAB2
DQ171866_SAB3 AY333361_URU2
JF704213_SAB1 AF065250_GB1
AF065251_GB2DQ171853_GB4
AF065257_RSVA_out
40
BA9
BA10
Figure 4 Genotype tree the topology of the HRSV B tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype BA10 Clades in blue show samples thatbelong to genotype BA9
The demographic and clinical characteristics of theinfants that were infected with genotype AON1 were similarto the characteristics of the other genotypes Exclusionof infants with viral codetection and those who receivedantimicrobials during hospitalization made it possible toavoid confounding factors in the comparative analysis of theseverity between the genotypes
A mean age at 2 months showed the precocity of theinfection which was independent of the infecting genotypeClinical characteristics that could differentiate the initialpresentation such as the presence of cough fever dyspneaand apnea crises also showed similar prevalence among thegenotypes Some prognostic factors that are relevant in respi-ratory infections in infants were also similar such as exposureto tobacco smoke and breastfeeding Severity as analyzedby the hospitalization time need and duration of oxygentherapy and mechanical ventilation and hospitalization inthe Intensive Care Unit was also similar regardless of theinfecting genotype
Despite the limited number of cases the results suggestthat the HRSV A ON1 genotype was not associated withspecific clinical characteristics and was therefore clinicallyindistinguishable from the other genotypes These resultsneed to be confirmed by more extensive analyses but areconsistent with a previous German study that found no clin-ical differences between infections by other HRSV genotypes[17] Althoughnucleotide variation in this region is importantfor viral antigenicity other regions may be more relevantdeterminants of infection severity In addition other factorsinherent to the host and the environmentmust be considered[18]
On the other hand an epidemiological study carriedout in Vietnam compared community-acquired infectionsand nosocomially acquired infections and showed a greaterseverity of the respiratory condition in children infectedwith HRSV ON1 compared to those infected with NA1with consideration of the clinical severity and occurrenceof pneumonia In that study all children used antibiotics
6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

4 BioMed Research International
PEG52PEG15
PEG57
PEG55
PEG56 PEG23
FJ210830_NA1
HQ731741_NA1 JF920053_NA2
PEG105 PEG79 PEG80 PEG82
PEG6 PEG100
PEG16 PEG8
newONl PEG10 PEG45 PEG13 PEG44
PEG35 PEG40
PEG31 PEG32 PEG18
PEG63 PEG24 PEG29
PEG38 PEG92
PEG51 PEG2 PEG19 PEG12 PEG1 PEG36
PEG39 PEG61
PEG90 PEG27 PEG54
M74568_GA1 AF065250_GB1_out
AF065410_GA6AF193327_GA7
JF920065_GA7 DQ171791_SAA1
AF065255_GA5JF920058_GA5
AF065406_GA5AF065254_GA4
AF233921_GA3 CN2395_GA3
Z33416_GA3AF233915_GA2
TX69554_GA2 AY344660_GA2
HQ731737_GA2 AF065257_GA1
50
ON1
NA2
NA1
Figure 3 Genotype tree the topology of the HRSV A tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype ON1 Clades in blue show samples thatbelong to genotype NA2 and clades in green show samples that belong to genotype NA1
In molecular analysis most of the sequenced HRSVAisolates were found to cluster in the ON1 genotype withprototype reference strain JN257694 whichwas first reportedin Ontario Canada [6] The sequenced isolates had thesignature 72-bp duplication in the G protein when alignedwith representative sequences from all of the A subgroup(GA1 to GA7 NA1 NA2 and ON1) from GenBank TheBrazilianHRSVA isolatesweremost closely related to isolatesfrom the United States Kenya and New Zealand
All of the sequenced HRSVB isolates were found tocluster in the BA genotype with prototype BA referencestrain AY333362 which was first reported in Buenos AiresArgentina [15] The sequenced isolates had the signature 60-bp duplication in the G protein when aligned with represen-tative sequences from all of the B subgroup (GB1 to GB4SAB1 to SAB4 URU1 and URU2 and BA-1 to BA-13) fromGenBank The Brazilian HRSV B isolates were most closelyrelated to isolates from the United States New Zealand andVietnam
Some authors suggest the occurrence of a greater numberof cases during seasons inwhich new genotypes predominateThis could be a result of the absence of immunity acquired bythe population against the new genotypes [4 15] GenotypeA ON1 shows a duplication of 72 nucleotides in the C-terminal third of the G gene The region of the G proteinencoded by this gene sequence is targeted by specific geno-type neutralizing antibodies which may contribute to theescape of the virus from the population immunity induced byprevious contact with other genotypes However accordingto the National Registry of Hospitalization Cases there wasno increase in the frequency of hospitalizations of infantsdiagnosed with bronchiolitis between 2013 and 2015 in Braziland the State of Sao Paulo compared to the previous five years[16] It is possible that acting as a controller the immunity ofthe population only contributes to the selection of genotypesthat replace each other without necessarily increasing thenumber of cases when genotypes without recent incidencesappear
BioMed Research International 5
PEG11PEG4PEG7PEG9
PEG108PEG118
PEG115PEG83
PEG42DQ227395_BA9
PEG62PEG84
PEG98 PEG22
JF714708_BA10 DQ985142_BA7 DQ227396_BA4
DQ227370_BA3 DQ227387_BA3 DQ227389_BA2
AY751108_BA5 AY751117_BA6
AY333362_BA1 DQ227380_BA1
AY488805_URU1 AF065252_GB3
DQ270231_SAB4AY327815_SAB2
DQ171866_SAB3 AY333361_URU2
JF704213_SAB1 AF065250_GB1
AF065251_GB2DQ171853_GB4
AF065257_RSVA_out
40
BA9
BA10
Figure 4 Genotype tree the topology of the HRSV B tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype BA10 Clades in blue show samples thatbelong to genotype BA9
The demographic and clinical characteristics of theinfants that were infected with genotype AON1 were similarto the characteristics of the other genotypes Exclusionof infants with viral codetection and those who receivedantimicrobials during hospitalization made it possible toavoid confounding factors in the comparative analysis of theseverity between the genotypes
A mean age at 2 months showed the precocity of theinfection which was independent of the infecting genotypeClinical characteristics that could differentiate the initialpresentation such as the presence of cough fever dyspneaand apnea crises also showed similar prevalence among thegenotypes Some prognostic factors that are relevant in respi-ratory infections in infants were also similar such as exposureto tobacco smoke and breastfeeding Severity as analyzedby the hospitalization time need and duration of oxygentherapy and mechanical ventilation and hospitalization inthe Intensive Care Unit was also similar regardless of theinfecting genotype
Despite the limited number of cases the results suggestthat the HRSV A ON1 genotype was not associated withspecific clinical characteristics and was therefore clinicallyindistinguishable from the other genotypes These resultsneed to be confirmed by more extensive analyses but areconsistent with a previous German study that found no clin-ical differences between infections by other HRSV genotypes[17] Althoughnucleotide variation in this region is importantfor viral antigenicity other regions may be more relevantdeterminants of infection severity In addition other factorsinherent to the host and the environmentmust be considered[18]
On the other hand an epidemiological study carriedout in Vietnam compared community-acquired infectionsand nosocomially acquired infections and showed a greaterseverity of the respiratory condition in children infectedwith HRSV ON1 compared to those infected with NA1with consideration of the clinical severity and occurrenceof pneumonia In that study all children used antibiotics
6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 5
PEG11PEG4PEG7PEG9
PEG108PEG118
PEG115PEG83
PEG42DQ227395_BA9
PEG62PEG84
PEG98 PEG22
JF714708_BA10 DQ985142_BA7 DQ227396_BA4
DQ227370_BA3 DQ227387_BA3 DQ227389_BA2
AY751108_BA5 AY751117_BA6
AY333362_BA1 DQ227380_BA1
AY488805_URU1 AF065252_GB3
DQ270231_SAB4AY327815_SAB2
DQ171866_SAB3 AY333361_URU2
JF704213_SAB1 AF065250_GB1
AF065251_GB2DQ171853_GB4
AF065257_RSVA_out
40
BA9
BA10
Figure 4 Genotype tree the topology of the HRSV B tree shows the study samples identified (PEG) compared to the specimens fromGeneBank identified by their access number Clades in red show samples that belong to genotype BA10 Clades in blue show samples thatbelong to genotype BA9
The demographic and clinical characteristics of theinfants that were infected with genotype AON1 were similarto the characteristics of the other genotypes Exclusionof infants with viral codetection and those who receivedantimicrobials during hospitalization made it possible toavoid confounding factors in the comparative analysis of theseverity between the genotypes
A mean age at 2 months showed the precocity of theinfection which was independent of the infecting genotypeClinical characteristics that could differentiate the initialpresentation such as the presence of cough fever dyspneaand apnea crises also showed similar prevalence among thegenotypes Some prognostic factors that are relevant in respi-ratory infections in infants were also similar such as exposureto tobacco smoke and breastfeeding Severity as analyzedby the hospitalization time need and duration of oxygentherapy and mechanical ventilation and hospitalization inthe Intensive Care Unit was also similar regardless of theinfecting genotype
Despite the limited number of cases the results suggestthat the HRSV A ON1 genotype was not associated withspecific clinical characteristics and was therefore clinicallyindistinguishable from the other genotypes These resultsneed to be confirmed by more extensive analyses but areconsistent with a previous German study that found no clin-ical differences between infections by other HRSV genotypes[17] Althoughnucleotide variation in this region is importantfor viral antigenicity other regions may be more relevantdeterminants of infection severity In addition other factorsinherent to the host and the environmentmust be considered[18]
On the other hand an epidemiological study carriedout in Vietnam compared community-acquired infectionsand nosocomially acquired infections and showed a greaterseverity of the respiratory condition in children infectedwith HRSV ON1 compared to those infected with NA1with consideration of the clinical severity and occurrenceof pneumonia In that study all children used antibiotics
6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

6 BioMed Research International
Table 1 Comparative analysis between the demographic and clinical characteristics of infants with HRSV infection caused by ON1 and byother genotypes
All genotypes119873 = 32
HRSV A ON1119873 = 22
Other HRSV genotypes119873 = 10
119875lowast
Demographiccharacteristics 119873 () 119873 () 119873 ()
GenderM 21 (656) 16 (727) 05 (500) 021F 11 (344) 06 (273) 05 (500)
Mean (sd) Mean (sd) Mean (sd)Age in months 245 (144) 233 (142) 271 (157) 051
Clinicalcharacteristics 119873 () 119873 () 119873 ()
Cough 31 (100) 21 (100) 10 (100) nsaFever 12 (375) 08 (381) 04 (400) 100lowastlowast
Dyspnea 23 (852) 17 (944) 06 (667) 009lowastlowast
Apnea 02 (063) 01 (909) 01 (250) 045lowastlowast
Complete Immunization forage 24 (960) 18 (100) 06 (851) 028lowastlowast
CurrentBreastfeeding 26 (896) 18 (947) 8 (800) 027lowastlowast
Second-handsmoking 06 (188) 05 (333) 01 (143) 062lowastlowast
Admission in Critical Care Unit 05 (156) 03 (158) 02 (200) 064lowastlowast
Oxygen therapy 27 (871) 20 (952) 07 (700) 009lowastlowast
Mechanicventilation 02 (645) 02 (091) 00 (000) 100lowastlowast
Mean (sd) Mean (sd) Mean (sd)Duration of stay 513 (438) 591 (484) 340 (259) 014Percentages are relative to the number of cases with complete information lowastcomparison of ON1 times other genotypes lowastlowastFisher exact test Studentrsquos t-testaccording to Brazilian National Program of Immunization
which may have created a bias since nonexcluded bacterialcoinfections could impact clinical evolutionAdditionally theage group was a differential factor since children up to 5 yearsof age were included including infants with bronchiolitis andalso cases of posterior HRSV infections [19] Other authorsfound fewer signs of severity in children infected by HRSVAON1 compared to other HRSV genotypes such as NA1 [7]GA2 and BA [20]
Another important aspect is the need for clinical follow-up studies that can assess the possible impacts of infectionsby different genotypes on the development of recurrentwheezing and asthma in the years following infections
5 Conclusion
The present study showed a high rate of HRSV detection ininfants hospitalized with bronchiolitis Five genotypes werefound with a predominance of genotype A ON1 whichwas recently described in other countries and not identifiedin previous studies in the southeast region of Brazil Theclinical and epidemiological characteristics of infants thatwere infected with HRSV A ON1 were similar to infants withinfections by other genotypes identified in the study
Conflicts of Interest
The authors declare no conflicts of interest
References
[1] C B Hall G A Weinberg A K Blumkin et al ldquoRespiratorysyncytial virus-associated hospitalizations among children lessthan 24 months of agerdquo Pediatrics vol 132 no 2 pp e341-e3482013
[2] A R Falsey P A Hennessey M A Formica C Cox and EE Walsh ldquoRespiratory syncytial virus infection in elderly andhigh-risk adultsrdquoTheNew England Journal ofMedicine vol 352no 17 pp 1749ndash1759 2005
[3] International Committee on Taxonomy of VirusesmdashICTVhttpwwwictvonlineorgvirustaxonomyasp
[4] T C T Peret C B Hall K C Schnabel J A Golub and LJ Anderson ldquoCirculation patterns of genetically distinct groupA and B strains of human respiratory syncytial virus in acommunityrdquo Journal of General Virology vol 79 no 9 pp 2221ndash2229 1998
[5] S E Vieira A E Gilio E L Durigon and B Ejzenberg ldquoLowerrespiratory tract infection caused by respiratory syncytial virus
BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

BioMed Research International 7
in infants the role played by specific antibodiesrdquoClinics vol 62no 6 pp 709ndash716 2007
[6] A Eshaghi V R Duvvuri R Lai et al ldquoGenetic variabilityof human respiratory syncytial virus a strains circulating inOntario a novel genotype with a 72 nucleotide G gene dupli-cationrdquo PLoS ONE vol 7 no 3 Article ID e32807 2012
[7] S Esposito A Piralla A Zampiero et al ldquoCharacteristicsand their clinical relevance of respiratory syncytial virus typesand genotypes circulating in Northern Italy in five consecutivewinter seasonsrdquo PLoS ONE vol 10 no 6 Article ID e01293692015
[8] M L Choudhary S P Anand B SWadhwa andM S ChadhaldquoGenetic variability of human respiratory syncytial virus inPune Western Indiardquo Infection Genetics and Evolution vol 20pp 369ndash377 2013
[9] A Fall N Dia E H A K Cisse et al ldquoEpidemiologyand molecular characterization of human respiratory syncytialvirus in Senegal after four consecutive years of surveillance2012ndash2015rdquo PLoS ONE vol 11 no 6 Article ID e0157163 2016
[10] M Viegas S Goya and A S Mistchenko ldquoSixteen years ofevolution of human respiratory syncytial virus subgroup A inBuenos Aires Argentina GA2 the prevalent genotype throughthe yearsrdquo Infection Genetics and Evolution vol 43 pp 213ndash2212016
[11] P Hu T Zheng J Chen et al ldquoAlternate circulation and geneticvariation of human respiratory syncytial virus genotypes inChengdu West China 2009ndash2014rdquo Journal of Medical Virologyvol 89 no 1 pp 32ndash40 2017
[12] J AMelero andM LMoore ldquoInfluence of respiratory syncytialvirus strain differences on pathogenesis and immunityrdquo CurrTop Microbiol Immunol vol 372 pp 59ndash82 2013
[13] H Katzov-Eckert V F Botosso E A Neto and P M D AZanotto ldquoPhylodynamics and Dispersal of HRSV Entails ItsPermanence in the General Population in between YearlyOutbreaks in Childrenrdquo PLoS ONE vol 7 no 10 Article IDe41953 2012
[14] V F Botosso PMD ZanottoMUeda et al ldquoPositive selectionresults in frequent reversible amino acid replacements in theG protein gene of human respiratory syncytial virusrdquo PLoSPathogens vol 5 no 1 Article ID e1000254 2009
[15] A Trento M Galiano C Videla et al ldquoMajor changes in the Gprotein of human respiratory syncytial virus isolates introducedby a duplication of 60 nucleotidesrdquo Journal of General Virologyvol 84 no 11 pp 3115ndash3120 2003
[16] httpwwwtabnetdatasusgovbr[17] J Tabatabai C Prifert J Pfeil J Grulich-Henn and P Schnit-
zler ldquoNovel respiratory syncytial virus (RSV) genotype ON1predominates in germany during winter season 2012ndash2013rdquoPLoS ONE vol 9 no 10 Article ID e109191 2014
[18] L Lambert A M Sagfors P J M Openshaw and F J CulleyldquoImmunity to RSV in early-liferdquo Frontiers in Immunology vol5 article 466 2014
[19] K Yoshihara M N Le M Okamoto et al ldquoAssociation ofRSV-A ON1 genotype with Increased Pediatric Acute LowerRespiratory Tract Infection in Vietnamrdquo Scientific Reports vol6 article 27856 2016
[20] C Panayiotou J Richter M Koliou N Kalogirou E Georgiouand C Christodoulou ldquoEpidemiology of respiratory syncy-tial virus in children in Cyprus during three consecutivewinter seasons (2010ndash2013) age distribution seasonality andassociation between prevalent genotypes and disease severityrdquoEpidemiology and Infection vol 142 no 11 pp 2406ndash2411 2014
Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Submit your manuscripts athttpswwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 201
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology