
INCIDENCE OF PREECLAMPSIA IN 200 ANTENATAL ANAEMIC …
118
1 INCIDENCE OF PREECLAMPSIA IN 200 ANTENATAL ANAEMIC MOTHERS ATTENDING A TERTIARY CARE REFFERAL CENTRE AT THE TIME OF ADMISSION AND MATERNAL MORTALITY IN ANAEMIA ASSOCIATED PRE ECLAMPSIA Dissertation submitted to THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY In partial fulfillment of the regulations For the award of the degree of M.D. BRANCH-II OBSTETRICS AND GYNAECOLOGY MADRAS MEDICAL COLLEGE CHENNAI APRIL 2014 CERTIFICATE
Transcript of INCIDENCE OF PREECLAMPSIA IN 200 ANTENATAL ANAEMIC …

1
INCIDENCE OF PREECLAMPSIA IN 200 ANTENATAL ANAEMIC MOTHERS
ATTENDING A TERTIARY CARE REFFERAL CENTRE AT THE TI ME OF
ADMISSION AND MATERNAL MORTALITY IN ANAEMIA ASSOCI ATED
PRE ECLAMPSIA
Dissertation submitted to
THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY
In partial fulfillment of the regulations
For the award of the degree of
M.D. BRANCH-II
OBSTETRICS AND GYNAECOLOGY
MADRAS MEDICAL COLLEGE
CHENNAI
APRIL 2014
CERTIFICATE
2
This is to certify that the dissertation entitled INCIDENCE OF PREECLAMPSIA IN
200 ANTENATAL ANAEMIC MOTHERS ATTENDING A TERTIARY CARE
REFFERAL CENTRE AT THE TIME OF ADMISSION AND MATERNAL
MORTALITY IN ANAEMIA ASSOCIATED PRE ECLAMPSIA is a bonafide work
done by DR. V. POORANA DEVI in the Institute of Social Obstetrics, Govt. Kasturba
Gandhi hospital ( Madras Medical College ) Triplicane, Chennai in partial fulfillment
of the university rules and regulations for award of MS degree in Obstetrics and
Gynecology under my guidance and supervision during the academic year 2011 to 2014.
Prof.DR.V.KANAGASABAI M.D. Prof.DR.S.DILSHATH MD.DGO,
DEAN, Director
Madras Medical College, Institute of Social Obstetrics,
Rajiv Gandhi Govt. General Hospital Govt. Kasturba Gandhi Hospital
Chennai -3 for women and children,
Madras medical college,
Chennai-3
Prof.DR.RAMANI RAJENDRAN MD.DGO.,
GUIDE Institute of Social Obstetrics,
Govt. Kasturba Gandhi Hospital
Madras medical college Chennai
-

3
DECLARATION
I solemnly declare that this dissertation entitled “ INCIDENCE OF
PREECLAMPSIA IN 200 ANTENATAL ANAEMIC MOTHERS ATTENDING A
TERTIARY CARE REFFERAL CENTRE AT THE TIME OF ADMISSION AND
MATERNAL MORTALITY IN ANAEMIA ASSOCIATED PRE ECLAMPSIA was
done by me at The Institute Of Social Obstetrics, Govt. Kasturba Gandhi Hospital,
Madras Medical College during 2011-2014 under the guidance and supervision of
Prof.Dr. RAMANI RAJENDRAN MD,DGO. This dissertation is submitted to the
Tamil Nadu Dr. M.G.R. Medical University towards the partial fulfillment of
requirements for the award of M.D. Degree in Obstetrics and Gynaecology (Branch-II).
Place: Chennai-3 Signature of Candidate
Date: Dr.V.POORANA DEVI M.B.B.S,
MS Post Graduate
Institute of SocialObstetrics,
Government Kastuurba Gandhi Hospital
Chennai.

4
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “INCIDENCE OF PREECLAMPSIA IN
200 ANTENATAL ANAEMIC MOTHERS ATTENDING A TERTIARY CARE
REFFERAL CENTRE AT THE TIME OF ADMISSION AND MATERNAL
MORTALITY IN ANAEMIA ASSOCIATED PRE ECLAMPSIA is a bonafide
research work done by Dr. V.Poorana devi in partial fulfillment of the requirement for
the degree of Master of Surgery in Obstetrics and Gynaecology.
Prof.DR.RAMANIRAJENDRANMD.DGO
GUIDE Institute of Social Obstetrics,
Government Kasturba Gandhi hospital
Madras medical college
Chennai
Place;
Date;
5
ACKNOWLEDGEMENT
I sincerely thank Prof. Dr. V.KANAGA SABAI MD., Dean,Madras medical college, Chennai, for
granting me permission to use the facilities of the Institution and Hospital for this study.
I expess my gratitude and thanks to Prof.Dr.S. DILSATHM.D.,DGO., Director , Institute of social
obstetrics Government Kasturba Gandhi Hospital for women and children for her guidance.
I am greatly indepted to Prof.Dr.RAMANI RAJENDRAN, M.D.,DGO.,Deputy Superindendent ,
Government Kasturba Gandhi Hospital for women and children, for her meticulous
commitment, constant support, and encouragement throughout this dissertation.
Iam extremely grateful to Dr. Sampath kumarai M.D.,D.G.O., Registrar, Govt. Kasturba Gandhi
Hospital for women and children for giving me inspirations, wise directions at every stage in
bringing out this dissertation.
I also thank Mr. Ravanan , who helped me in completing the statistical work.
I also thank all the unit Chiefs, Assistants, Lab Technicians and all my colleagues for their
continuous support.
I also thank all the patients for their kind cooperation.

6
ABSTRACT
OBJECTIVES AND BACKGROUND
Anemia during pregnancy is a major public health problem especially in
developing countries like India. This prospective study is aimed to find out the
incidence of preeclampsia in mild, moderate, and severe anemia and to analyse the
synergistic effect of anemia with preeclampsia in pregnancy associated Morbidity and
Mortality .
METHODS;
This prospective observational study was carried out at
Govt.KasturbaGandhi Hospital for women and children,Madras medical college,
Chennai,during the period of December 2012 to December 2013 on 200 patients
.Pregnant women attending the antenatal out patient department and labour ward in
Govt.Kasturba Gandhi Hospital with hemoglobin value less than 11gms and after 20
weeks of gestation were selected for the study. After recording the base line data,
patients with moderate and severe anemia were advised admission for anemia evaluation
and treatment .In these patients the incidence of preeclampsia at the time of admission
were calculated. The patients with preeclampsia were admitted for preeclampsia
evaluation The selected patients were monitored and followed till delivery
RESULTS;
In this study 83% of the patients were in the moderate anemia with Hb 7.to 10
gms. 11% of the patients were in the severe anemia with Hb less than7grams and 6% of
the cases were in the mild anemia (Hb 10-11gms). This study was showed the

7
association between anemia and the preeclampsia, anemic patients were more prone to
develop preeclampsia due to associated hypo proteinemia. More severe the anemia,
greater the chance to get preeclampsia. Incidence of preeclampsia in the study was
18.5%, the p value shows .000 highly significant Incidence of severe preeclampsia was
11.5% and incidence of mild preeclampsia was 7%.Maternal outcome of the study
showed that AtonicPPH -6%.Pulmonary edema -1.5%, Death occurred in one case in
the studypopulation.Both HELLP and DIVC occurred in one case 0.5%.Abruptio
placenta occurred in 1%.Eclampsia occurred in 2% of the cases.
CONCLUSION
Anemia during pregnancy is still continues to be a major problem in developing
countries with maternal and fetal complications The coexistence of preeclampsia in
anemic women’s worsening the situation. In preeclampsia, there was already
intravascular volume depletion hence anemia gets masked the patients are not able to
cope up even with mild blood loss during delivery .Correct diagnosis and treatment of
the underlying cause can improve the maternal outcome
.We have to counsel the pregnant mothers during their antenatal checkup regarding the
importance of blood pressure monitoring, screening and correction of anemia prior to
pregnancy and Iron and folic acid supplementation. The Tenth plan strategies has to be
effectively implemented to all pregnant women with anemia to reduce the maternal
mortality and morbidity and long term consequences of anemia.
8
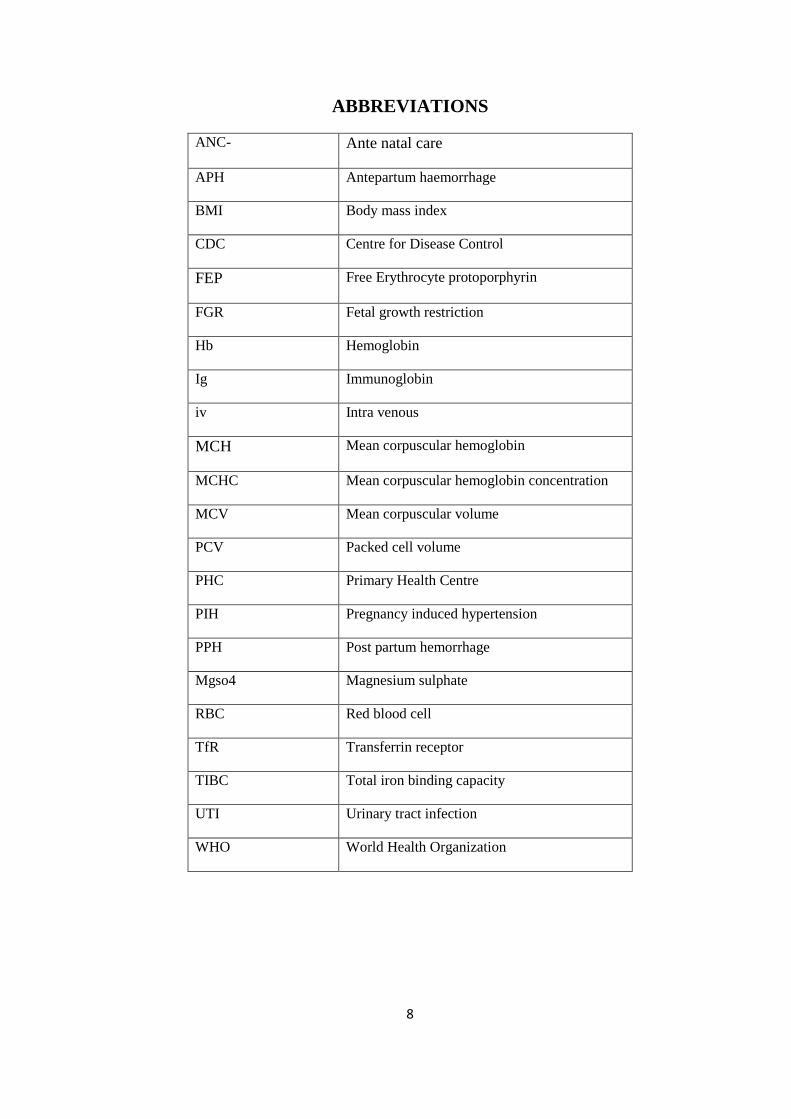
ABBREVIATIONS
ANC- Ante natal care
APH Antepartum haemorrhage
BMI Body mass index
CDC Centre for Disease Control
FEP Free Erythrocyte protoporphyrin
FGR Fetal growth restriction
Hb Hemoglobin
Ig Immunoglobin
iv Intra venous
MCH Mean corpuscular hemoglobin
MCHC Mean corpuscular hemoglobin concentration
MCV Mean corpuscular volume
PCV Packed cell volume
PHC Primary Health Centre
PIH Pregnancy induced hypertension
PPH Post partum hemorrhage
Mgso4 Magnesium sulphate
RBC Red blood cell
TfR Transferrin receptor
TIBC Total iron binding capacity
UTI Urinary tract infection
WHO World Health Organization

9
CONTENTS
SERIAL NUMBER
TITLE PAGE NUMBER
1 INTRODUCTION 1
2 REVIEW OF LITERATURE 3
3 H ISTORICAL ASPECTS OF ANEMIA 8
4 HISTORICAL ASPECTS OF PRE ECLAMPSIA 9
5 ANEMIA IN PREGNANCY 11
5.1 DEFINITION 11
5.2 SEVERITY OF ANEMIA 11
5.3 HAEMATOLOGICAL CHANGES DURING PREGNANCY 12
5.4 CHANGES IN BLOOD CONSTITUENTS 13
5.5 CHANGES IN BLOOD COAGULATION 14
5.6 CLASSIFICATION OF ANEMIA 15
5.7 ERYTROPOIESIS 18
5.8 IRON METABOLISM 18
5.9 IRON DISTRIBUTIONIN THE BODY 19
5.10 IRON DEFICIENCY ANEMIA 20
5.10.1 AETIOLOGY 20
5.10.2 FACTORS AFFECTING IRON ABSORPTION 21
5.10.3 IRON REQUIREMENT DURING PREGNANCY 22
5.10.4 CLINICAL FEATURES 23
5.10.5 HAEMATOLOGICAL INDICES 24
5.10.6 SPECIFIC INVESTIGATIONS FOR IRON DEFICIENCY 26
5.11 EFFECT OF ANEMIA ON PREGNANCY 28

10
5.12 CARE OF ANTENATAL WOMEN WITH ANEMIA 29
5.13 PHARMACOLOGICAL THERAPY OF ANEMIA 30
5.14 BLOOD TRANSFUSION 31
5.15 INTRAPARTUM MANAGEMENT 32
5.16 POSTPARTUM MANAGEMENT 32
6 PRE ECLAMPSIA 33
6.1 DEFINITION 33
6.2 CLASSIFICATION OF HYPERTENSIVE DISORDERS OF PREGNANCY
33
6.3 ETIOLOGY 35
6.4 RISK FACTORS FOR PREECLAMPSIA 36

11
SERIAL NUMBER
TITLE PAGE NUMBER
6.5 PATHOGENESIS 38
6.6 PATHOLOGICAL CHANGES IN ORGANS 39
6.7 CLINICAL FEATURES 41
6.8 INVESTIGATIONS 42
6.9 MANAGEMENT 43
6.10 MILD PREECLAMPSIA 47
6.11 SEVERE PREECLAMPSIA 47
6.11.1 MATERNAL MONITORING 47
6.11.2 FETAL MONITORING 48
6.11.3 INDICATIONS FOR DELIVERY 48
6.11.4 COMPLICATIONS OF SEVERE PREECLAMPSIA 50
7 AIM OF THE STUDY 51
8 MATERIALS AND METHODS 51
8.1 INCLUSION CRITERIA 51
8.2 EXCLUSION CRITERIA 51
8.3 METHODS 52
8.4 STATISTICAL METHODS 43
9 RESULTS AND ANALYSIS 55
10 DISCUSSION 80
10.1 NEAR MISS CASES IN THE STUDY 89
11 SUMMARY 91
12 CONCLUSION 93
13 BIBILIOGRAPHY
14 PROFORMA
15 MASTER CHART

12
LIST OF TABLES
S.NO TITLE PAGE
NO
1 AGEDISTRIBUTION 56
2 DISTRIBUTION OF GRAVIDITY 57
3 DISTRIBUTION OF SOCIO ECONOMIC CLASS 58
4 DISTRIBUTION OF BOOKING STATUS 59
5 REFERRAL STATUS 60
6 LITERACY STATUS 61
7 DISTRIBUTION OF MATERNAL WEIGHT 62
8 DISTRIBUTION OF GESTATIONAL AGE TABLE 63
9 DISTRIBUTION OF SEVERITY OF ANEMIA 64
10 DISTRIBUTION OF PERIPHERAL SMEAR 65
11
DISTRIBUTION OF PLATELET COUNT 66
12 DISTRIBUTION OF SEVERITY OF BLOOD PRESSURE
67
13 DISTRIBUTION OF URINE ALBUMIN 68
14 DISTRIBUTION OF 24 HOURS URINARY PROTIEN 70
15 ONSET OF LABOUR 71
16 MODE OF DELIVERY 72
17 MATERNAL OUTCOME 73

13
18 FETAL OUTCOME 74
19 BIRTH WEIGHT 75
20 BLOOD TRANSUSION 76
21 CROSS TABLE HEMOGLOBIN AND BLOOPRESSURE
77
22 CROSS TABLE MATERNAL OUTCOME AND BP 79

14
LIST OF FIGURES
S.NO TITLE PAGE NO
1 PIE DIAGRAM SHOWING AGE DISTRIBUTION 56
2 PIE DIAGRAM SHOWING DISTRIBUTION
OFGRAVIDITY
57
3 PIE DIAGRAM SHOWING DISTRIBUTION OF
SOCIOECONOMIC CLASS
58
4 PIE DIAGRAM SHOWING BOOKED STATUS 59
5 PIE DIAGRAM SHOWING REFERRAL STATUS 60
6 PIE DIAGRAM SHOWING LITERACY STATUS 61
7 PIE DIAGRAM SHOWING DISTRIBUTION OF MATERNAL WEIGHT
62
8 PIE DIAGRAM SHOWING DISTRIBUTION OF GESTATIONAL AGE
63
9 PIE DIAGRAM SHOWING SEVERITY OF ANEMIA 64
10 PIE DIAGRAM SHOWING DISTRIBUTION OF PERIPHERAL SMEAR
65
11 PIE DIAGRAM SHOWING DISTRIBUTION OF PLATELET COUNT
66
12 PIE DIAGRAM SHOWING SEVERITY OF BLOOD PRESSURE
67
13 PIE DIAGRAM SHOWING DISTRIBUTION OF URINE ALBUMIN
69
14 PIE DIAGRAM SHOWING ONSET OF LABOUR 71

15
15 PIE DIAGRAM SHOWING MODE OF DELIVERY 72
16 PIE DIAGRAM SHOWING MATERNAL OUTCOME 73
17 PIE DIAGRAM SHOWING FETAL OUTCOME 74
18 PIE DIAGRAM SHOWING BIRTH WEIGHT 75
19 PIE DIAGRAM SHOWING BLOOD TRANSUSION 76
20 CHART SHOWING HEMOGLOBIN AND BLOOD PRESSURE
78

16
I .INTRODUCTION
Anaemia in pregnancy is one of the most important public health
problems. Anemia is the most common medical disorder in pregnancy especially in
developing countries. It is responsible for 20% of direct cause of Maternal Mortality in
developing countries. In recent years, worldwide an estimated five lakh women die as a
result of pregnancy each year. Approximately one quarter of all pregnancy and delivery
related maternal deaths Worldwide occur in India.
The current estimated Maternal Mortality Ratio in India is 301 per 100,000
live births. This translates in to about 80,000 pregnant women dying annually. Most
maternal deaths are preventable% In Asia .more than 70% of maternal deaths are due to
direct complications .Hemorrhage 31%. Sepsis/infection 12% unsafe abortion 6%
.Eclampsia 9% obstructed labour 9%. Severe anemia is a critical underlying factor and
important indirect cause of maternal deaths in India. Most maternal deaths occur
between the third trimester and the first week after delivery
Prevalence of anemia in India is about 60% which is increased to 80%
during pregnancy. Most of the pregnant mothers attending a Antenatal outpatient
department are anemic. During pregnancy the nutritional requirement of iron and folic
acid is increased, pregnancy induced hypervolemia also causes physiological anemia
.The increase in blood volume varies among different women. The increase in blood
volume is mainly affected by an increase in plasma volume 40% much more than the red
cell volume 20%resulting in relative hemodilution of pregnancy. This brings the
haemoglobin decrease to almost by2 gms .This along with the increased demand for iron
leads to physiological anemia of pregnancy.

17
The women in the developing countries enter the pregnancy with depleted
iron stores.because most women are not able to develop adequate iron stores during the
growth period due to poverty ,inadequate intake of nutrients recurrent infections
,menstrual blood loss,and WHO defined anemia of pregnancy as a hemogolobin level of
less than 11g/dl ,or hematocrit less than 33% at any point during pregnancy.
Preeclampsia is a multisystem disorder of unknown etiology and is unique to
pregnant women after 20 weeks of gestation. It is a progressive disease with variable
mode of presentation and rate of progression . Preeclampsia is a clinical diagnosis
consisting of 1)new onset hypertension systolic blood pressure >140,diastolic blood
pressure >90mmHg recorded on two occasions at least 6 hours apart in a previously
normotensive women 2) new onset proteinuria (defined as >300mg/24hour .or >2+ on a
clean catch dipstick in the absence of urinary infection; and new onset significant
nondependent edema. Preeclampsia is classified as either mild or severe ‘’ Preeclampsia
complicates 6-8% of all pregnancies . Preeclampsia and eclampsia contributes to 12% of
all maternal deaths in the developing countries( WHO1999) Perinatal outcomes were
significantly higher in preeclampsia
The present study was undertaken to find out the incidence of Preeclampsia in
mild./ moderate/ severe anemia . and to analyse the synergistic effect of anemia with
preeclampsia in pregnancy associated Morbidity and Mortality
Early detection and treatment of anemia in pregnant women significantly
reduces the Mortality andMorbidity

18
2 .REVIEW OF LITERATURE
Early detection of preeclampsia in anemia complicating pregnancy
significantly reduces the maternal mortality .In preeclampsia patients anemia is usually
masked because of hemoconcentration. If they manifest anemia, it is usually of severe
degree
Abdel Aziem A Ali had done a retrospective case control study at Eastern
Sudan Kassala hospital.. Pregnant women with severe anemia Hb <7gms/dl who
delivered between the period of Jan 2008 to Dec2010 ,medical files of them were
reviewed out of these 41.8% women had anemia and 3.2% had severe anemia .The
corrected risk for preeclampsia was increased only in patients with severe
anemia(OR=3.6,p=0.007) .When compared with women who were not anemic ,the risk
of LBW was 2.5 times more in women with mild/moderate anemia and 8.0 times
increased in women with severe anemia . The risk of preterm delivery proportionately
increased with the severity of anemia. More severe the anemia during pregnancy, the risk
of preeclampsia was increased.1
Fernandez G Diez EM, VelaquezN,Oberto J had done a case control study In
48 middle class pregnant women who were given placebo during gestation were
compared with 88 women who were all given iron and folic acid tablets. 23 women
were found to be having anemia, preeclampsia coexisted in 10 of these women.. The
anemic women associated with preeclampsia had lower transferrin saturation than the
anemic patients. 2
Masoomeh Goodarzi Khoigani had done a prospective cohort study with ,520 Iranian
pregnant women aged 15-45 years, hemoglobin and haematocrit was measured in them

19
during the 6th -11thweeks and 26-30th weeks of pregnancy . The cases who were all
having low levels of hemoglobin during the first half of pregnancy were more chance to
get preeclampsia ,p=0.024, The patients with low levels of hemoglobin during the
second half of pregnancy were associated with increased risk of preterm premature
1rupture of membranes (p=0.01) 3.
Ugur Keshin. Emre Karasahin.Seyit Temel Ceyhan,Ahkara had done a
retrospective study included 162 pregnant women with second trimester Hb levels <
8gms/dl(G1) and they were compared to 160 women with second trimester Hb levels
10gms/dl (G2) at Gulhane Military Medical Academy between Jan 2003 to Dec 2006
Preeclampsia rates of women with Hb <8gs were 8.6% n:14, and women with Hb 10
gms were 3.2%(n:5) respectively p(0.05)4
Vitthal G Kuchake, Sunny G Kolhe, had done a prospective observational study
with 971 pregnant women between July 2009 to Feb 2010 . A total 73 (7.51%)
preeclamptic pregnancy was found in the age group of 18-22 years of age . HELLP
Syndrome was found to be 8% and the women with eclampsia were 10% . 48%
incidence of caesarean mode of delivery was observed in that study..This study stated
that in preeclampsia syndrome ,maternal mortality and morbidity rate was high .5
Patra S et al had done the maternal and perinatal outcomes of 130 severely anemic
pregnant women who had 5 gm/dl or less hemoglobin ,the hemoglobin values were
found at the third trimester and 81% of their population were multiparas ,preterm birth
rate was 69.2%, preeclampsia 17% eclampsia 4% , placental abruption 3% fetal distress
23% low birth weight 24.6% neonatal death 35% (6)

20
Pankaj kumar Prasad pore , Usha patil had studied Maternal anemia and its impact
on the perinatal outcome at Maharastra in a tertiary care Hospital of Pune .The study
group was 126 pregnant women . 46% of the cases were anemic during the time of
delivery.and the ,peripheral smear showed that 78% of cases were normochromic
normocytic , 44% pregnant women were microcytic hypochromic and 2% of the study
group had megaloblastic anemia .Anemia was observed in the women with less than
three antenatal follow up visits , with history of early marriage before 18 years of age
and also women who were not taken Iron and folic acid tablets 7
M A Brown ,C Mackenaie , W Dunmuir, L Roberts, had done a retrospective cohort
study . with 1515 women who were diagnosed as preeclampsia or gestational
hypertension between the period of 1988- 1998 the data was collected from the hospital
records.. 1354 women were followed up,and compared with 333 normal pregnancy
women as per the records were selected randomly as controls during the same period.
All most all cases with normal pregnancy outcome previously were found to be having
normotensive pregnancy . One in 50 women was found hypertensive in their past
pregnancy was developed essential hypertension in next pregnancy . Women with
preeclampsia in their previous pregnancy equally chance to develop either preeclampsia
or gestational hypertension (approximately 14% of each) .while women with gestational
hypertension were more chance to get gestational hypertension (26%) when compared to
preeclampsia(6%) in their next pregnancy. When compared with primiparous women
,multiparous women with gestational hypertension were more chance to develop
preeclampsia (11versus 4%) or gestational hypertension (45 versus 22%) in their
subsequent pregnancies. (8

21
James .N.Martin , Jr ,MD, Brian .K. Rinehart,MD,Warren L .May had conducted a
retrospective analytic study , 777 pregnant patients with class1,2,or3 HELLP syndrome
had compared with 193 women with severe pre eclampsia but with the absence of
HELLP syndrome.About 50% of the cases complicated by class 1 HELLP syndrome
showed significant maternal morbidity. When compared with cases complicated by
severe preeclampsia with the absence of HELLPsyndrome(9)
Attiya Ayaz .TajMuhammad, Shaheryar A Hussain.Sadia Habib,had done a cross
sectional comparative study , to find out the neonatal outcome in babies born of
preeclampsia pregnant women. The study was conducted in Ayub Teaching hospital ,
Abbottabad during the period of Janauary 2007 to June 2007. Study population was 73
cases of preeclampsia ,they had matched with controls for the following variables like
age , gestational age ,and parity.Neonatal outcome report showed that the perinatal
mortality of 328 neonates per 1000 total births. Main cause of death was still births and
intra uterine death..Preeclampsia pregnant patient had more of adverse neonatal
outcome.(10)
Mohammad A Salahat and Abdallah I. Ibrahim was ,conducted a cross sectional study
with 1030 pregnant women in the age group of 16 to 40 years for the assessment of
their hemoglobin .The results of the study showed that anemia was more common
among pregnant women of age group16- 19years, Incidence of anemia was more
common in multiparas than primiparas .Prevalence of anemia was increased during the
third trimester,. The significant increase in alkaline phospatase activity was associated
with increased complications like diabetes mellitus,preeclampsia, proteinuria,and
diabetes with hypertension.(11)

22
JamaiyahHaniff et al had done a multicenter cross sectional observational study at
Malaysia to find out the epidemiological parameters of anemia complicating pregnancies
during the period of February to March 2005.The study population was 1072 pregnant
women. The results showed the prevalence was 35%,most of the study population had
mild anemia.12
J.J.Zhang, J. Grewal,J.P.souza, they used the data from WHO Global Survey for
maternal and perinatal health collected in hospitals from2007-2008 to analyse whether
the several types of anemia were risk factors for developing hypertensive disorders
during pregnancy in the developing countries,the results showed that multiparous women
who had severe anemia were increased chance to get gestational hypertension( ODDS
RATIO 1.58)confidence interval of( 1.15-2.19).
Nulliparous women with severe anemia were having significant correlation with
preeclampsia(OR)3.55; 95% CI2.87-4.41, Multiparous women with severe anemia were
having risk of developing preeclampsia (OR;3.94;95% CI 3.05-5.09).13

23
3.H ISTORICAL ASPECTS OF ANEMIA
Iron deficiency has been described as the most common nutritional deficiency across the
world.William Harvey (1628) was the one who postulated the circulation of blood.
German biochemist Felix Hoppe Seyler (1825-1895) showed that hemoglobin was a
complex of haematin and protein by absorption spectrometry.
Paul ehrlich (1854-1915)was discovered aniline dyes to stain blood films ,which was
used in the study of red blood cell, and the birth of Modern Haematology.-
Wintobe(1985).
In Seventeenth century, Chlorosis was used to denote anemia Most of the features of
chlorosis were similar to that of severe iron deficiency anemia in adolescent girls and
young women.(21)
Gabriel Andril (1797-1876) had noticed and stated that the size of red blood cells in
chlorosis which were very small in size.
In 19 th century the term anemia was coined to denote the clinical condition which was
associated with pallor of the mucous membranes and nails. Davis and Witts (1931)
were found the role of iron therapy in hypochromic anemia in adults. The accurate
measurement of haemoglobin levels was a Twentieth century developmentNow we were
using various modalities to treat anemia like injectable forms of iron therapy, blood
transfusions particularly specific components like packed cells.platelets. fresh frozen
plasma.cryoprecipitate.

24
4.HISTORICAL ASPECTS OF PRE ECLAMPSIA 15
Around 400BC, Hippocrates who stated that the headache accompanied by heaviness
and convulsions during pregnancy was considered bad.In the early years of 18th
century,when only the end stage of toxemia ,eclampsia was known they believed that it
was a special form of epilepsy associated with pregnancy.
In 1739.Bossier de sauvages, differentiated the seizures of eclampsia from epilepsy,
Eclampsia was acute in onset, and it was resolved after removal of the precipitating
factor. Prior to 18th century, the term eclampsia was used to refer the visual phenomena
occurring in neurological diseases, as flashes of light.
Rayer’s (1839-1841) stated that the evidence of renal involvement in eclampsia, he
found that the presence of protein in the urine of pregnant edematous women. Lever
(1843) in London also found that eclampsia was associated with albuminuria. He also
demonstrated that eclampsia was more common in first pregnancies than subsequent
pregnancies, and disappearance of protein in the urine of pregnant women after child
birth.
The term toxemia was used previously to denote eclampsia, when it was believed t o be
caused by toxic substances in the blood, the term is a misnomer.After the invention of
Scipione Riva –Rocci’s mercury manometer (1896) to measure the blood pressure, they
recognized that the preeclampsia was a hyper tensive disorder associated with
pregnancy.
In 1959 Farughar demonstrated renal pathology glomerular endotheliosis in
preeclampsia patients using Electron microscopy

25
In the last two decades ,because of advance reasearches in molecular level,and biological
level the pathophysiological changes associated with preeclampsia like examination of
the placenta, role of spiral arterioles, endothelial cells, antioxidants, antiangiogenic
proteins, and other systemic dysfunction were made out. Still the etiopathogenesis of
preeclampsia is not well understood.

26
5.ANEMIA IN PREGNANCY
5.1.DEFINITION :
Anemia is defined as a hemoglobin value that is lower than the threshold
of two standard deviations below the median value for a healthy matched population.
WHO CRITERIA:
WHO defined anemia of pregnancy as hemoglobin level of less than
11gm/dl, or hematocrit less than 33%, at any point during pregnancy.
CDC CRITERIA
The US Centers for Disease control and Prevention defines anemia of
pregnancy as a hemoglobin level less than 11gms/dl, or hematocrit less than 33% in the
first or third trimester or hemoglobin less than 10.5 g/dl or haematocrit less than 32% in
the second trimester.
5.2 SEVERITY OF ANEMIA
According to ICMR the severity of anemia is graded as follows;
Mild degree :10-10.9gms%
Moderate degree :7- 10gms%
Severe degree:less than 7gms%
Very severe degree: less than 4gms%
Prevalence of anemia is higher in India when compared to other South Asian
Countries. 80% of maternal deaths in South Asia due to anemia occurring in India.

27
5.3HAEMATOLOGICAL CHANGES DURING PREGNANCY
The hematological changes in pregnancy include increases in plasma volume and total
red cell mass and hemoglobin changes thorough out the gestation.
True anemia denotes that the decrease in hemoglobin concentration and fall in the
oxygen carrying capacity of blood. But during pregnancy the oxygen carrying capacity
of the blood is increased than in the non pregnant mothers. This was reflected by
increased oxygen saturation in the venous blood of pregnant women.
The increase in the plasma volume was greater when compared to red cell mass , which
leads to physiological dilution .In the first six weeks of pregnancy ,the plasma volume
decreases ,it begins to raise from sixth week .and reaches plateau after 34-36 weeks. The
maximum rise is about 50% of the base line value.
The blood volume starts to increase from sixth week of gestation, reaches the maximum
of 50-% above the base line value at 30- 32 weeks. In the first 12 weeks of gestation, red
cell mass decreases, then it increases till third trimester which was about 20-30% above
the base line value. Both the plasma volume and redcell mass reaches the prepregnant
value after six weeks of post partum. Because of both physiological anemia during
pregnancy and increased iron demand, anemia is more prevalent among pregnant
women.
The increased maternal circulatory volume.plasma volume, and redcell mass in
association with decreased peripheral resistance leads to increase uteroplacental
circulation , the above mentioned changes are mediated thorough various hormones like
rennin, angiotensin II, aldosterone,thromboxane A2,cortisol,
prostacylin,estrogens,progesterone,anti diuretic hormone, antinatiuretic hormones.
28
The hydremia of pregnancy favours the followings;
1) The hemodilution leads to decrease in blood viscosity which helps in better oxygen
and co2 transport between the maternal and fetal circulation
2) It protects the mother against the blood loss during third stage of labour,
3) The increased blood volume leads to increased glomerular filtration rate; thereby it
regulates the fetal amniotic fluid production,
4) It protects the pregnant women against supine hypotension.
In normal pregnancy
The serum iron concentration decreased.
The absorption of iron from the small intestine increased.
The iron binding capacity also increased.
There is increased synthesis of the beta1 globulin and transferrin.
The plasma folate concentration decreased to 50% at term because of renal clearance of
folate is increased during pregnancy, but red cell folate concentration is minimally
affected.
5.4 CHANGES IN BLOOD CONSTITUENTS
Bone marrow showed erythroid hyper plasia and increased production of reticulocytes
The total white cell count increased particularly poly morpho leucocytes, T and B
lymphocyte count do not change much, but their functional ability is decreased, so that
pregnant women are more prone for getting infections

29
Platelets may show a small reduction in number because of increased thrombaxane levels
in mid trimester, which causes increased platelet consumption. But platelet production is
increased during pregnancy.
Plasma proteins increased during pregnancy, but because of hemodilution, the total
protein value is 6gm/dl (normal 7gm/dl) Albumin also falls to 3gm/dl (normal 4gm/dl)
Globulin is marginally increased. It leads to decrease in colloid osmotic pressure .The
albumin globulin ratio in pregnancy is altered to 1:1, (normal 2:1).
5.5 CHANGES IN BLOOD COAGULATION
In pregnancy, there is increase in all the coagulation factors except factor 10 and factor
12. There is reduction in the concentration of anticoagulation factors like antithrombin
III, protein C, and protein S The activity of the fibrinolytic system is inhibited.Thus
pregnancy is a hyper coagulable state, it helps to prevent hemorrhage during delivery but
it increases the risk of venous thrombosis and pulmonary embolism.
The level of coagulation factors becomes normal in 2weeks after delivery. As a result of
increased fibrinogen level, globulin level and decreased blood viscosity ESR is four fold
increased. Hence ESR value is little significance.

30
5.6 CLASSIFICATION OF ANEMIA
PHYSIOLOGICAL ANEMIA & PATHOLOGICAL ANEMIA
DEFICIENCY ANEMIA
Iron deficiency
Folic acid deficiency
Vitamin B12 deficiency
Protein deficiency
HEMORRHAGIC ANEMIA
Antepartum hemorrhage
Hook worm infestations
Bleeding piles
HEMOLYTIC ANEMIA
Hemoglobinopathies
Thalassemia,Sickle cell anemia,
Hereditary Sperocytosis
Malaria
MISCELLANEOUS CAUSES
Bone marrow insufficiency –Aplastic anemia,Drug induced
Neoplasm
Chronic renal disease Tuberculosis
31
MORPHOLOGICAL CLASSIFICATION
Normocytic MCV: 80-100fl
Microcytic MCV :< 80 fl
Macrocytic MCV :> 100
NORMOCYTIC ANEMIA CAUSES
Aplastic anemia
Acute post hemorrhagic anemia
Hemolytic anemia(except thalassemia)
Pure red cell aplasia
Endocrine diseases
Bone marrow infiltration
Renal failure
Protein malnutrition
MICROCYTIC ANEMIA
Iron deficiency
Sideroblastic anemia
Thalassemia
Lead poisoning
Anemia of chronic diseases

32
MACROCYTIC ANEMIA
Megaloblastic anemia
Non megaloblastic anemia
MEGALOBLASTIC MACROCYTIC ANEMIAS
Folic acid deficiency, Vitamin B12 deficiency
NON MEGALOBLASTIC MACROCYTIC ANEMIAS
Anemia of acute bleeding
Leukemias(acute)
Liver disease
Hemolytic anemias
Myleodysplasic syndrome
Hypothyroidism
Alcoholism
Aplastic anemia
PATHOGENIC CLASSIFICATION
DECREASED HEMOGLOBIN PRODUCTION
Iron deficiency anemia
Sideroblastic anemia
Thalassemia
DEFECTIVE DNA SYNTHESIS
VitaminB12 deficiency , Folic acid deficiency

33
5.7 ERYTROPOIESIS
Red blood cells are formed from Colony forming unit of elytroid
precursors – pronormoblasts- normoblasts- reticulocytes- to mature nucleated
erythrocytes. The red blood cell life span is about 120 days. Under normal conditions,
average weight human destroys 1-2X108 erythrocytes per hour, which was corresponds
to 6 gm hemoglobin turnover. When the hemoglobin is destroyed it produces globin and
heameglobin is again degraded into its constituents amino acids iron content of heme
enters in to the iron pool. The catabolism of heme occurs mainly in the
reticuloendothelial system of the body (liver, spleen .bone marrow).
Adequate nutrients are essential for erythropoiesis, inadequate reserve, or increased
demand, or deficient supply of vitamins and minerals are interfering with normal
erythropoiesis.
5.8 IRON METABOLISM
Iron is present in many of the hemoproteins like hemoglobin, myoglobin,and
cytochromes.It is ingested in the diet either as heme or non heme iron.Absorption of
haem iron is two to three times more than than nonhaemiron.Absorption of iron occurs in
the proximal duodenum by enterocyte .Ferric iron in the food is reduced to ferrous form
by the ferric reductase present on the surface of the enterocyte The transfer of iron from
the apical surface of the enterocyte to the interior is brought by the proton coupled
divalent metal transporter . A newly discovered peptide named as hepcidin plays an
important role in iron metabolism . It down regulates the intestinal absorption and
placental transfer of iron and also release of iron from the macrophages. When the
plasma level of iron is low, the synthesis of hepcidin decreases

34
Once the iron enters in to the enterocyte, it can be stored as ferritin or transferred across
the basement membrane in to the plasma and carried by the transferrin , ferric iron is
taken up by the transferrin One transferrin molecule binds with the two atoms of iron.
The regulation of iron absorption is complex and not well understood. Regulation occurs
at the level of enterocyte ( mucosal block) The concentration of transferrin in the plasma
is 300mg/dl, it binds with the 300mcg of iron per deciliter.it denotes the total iron
binding capacity of the plasma
The amount of ferritin in the plasma can be measured by sensitive and specific radio
immunoassay ,it reflects the body iron stores
Ferritin aggregates to form hemosiderin,ferritin is a water soluble form but hemosiderrin
is water insoluble. When there is a need the stores are first mobilized to provide iron.
5.9 IRON DISTRIBUTIONIN THE BODY
(ref;harper27th edi)
Transferrin 3-4mg
Hemoglobin in red blood cells 2500mg
Myoglobin and other enzymes 300mg
Storage iron 100-400mg
Absoption 1mg/day
Losses 1.5-2mg/day

35
5.10 IRON DEFICIENCY ANEMIA
5.10.1 AETIOLOGY
Deficient intake and absorption
1. Inadequate diet
2. . Presence of phosphates and phytates in the food
3. Hyperemesis
4. Achlorhydria and vitamin C deficiency
INCREASED DEMAND
Multiple pregnancy
Excessive loss of blood
1. Repeated pregnancies and inadequate spacing between pregnancies
2. Hookworm infestation
3.History of menorrhagia
4. Malaria
CHRONIC ILLNESS affecting the general condition of the patients.
36
5.10.2 FACTORS AFFECTING IRON ABSORPTION
DIETARY SOURCES WITH RICH IRON CONTENT;
VEGETARIAN DIET
Green leafy vegetables, spinach, mustard and, fenugreek. In cereals like whole wheat,
bajra, jowar. In pulses like ground nuts, green peas, beans, and other foods like jaggry,
dates.
NON VEGETARIAN DIET
Liver and meat are the good sources of haem iron among non vegetarian foods.
Fish and eggs are containing medium iron content.
FACTORS FAVORING ABSORPTION FACTORS INHIBITING
ABSORPTION
I n organic iron
Organic iron phosphates in egg
yolk, phytates in cereals
Ferrous iron(ironsalts, haem iron)
Ferric iron( non haemiron)
Acids like Hcl, ,citric acid .ascorbic acid
Alkalies, antacids.calcium salts

37
5.10.3 IRON REQUIREMENT DURING PREGNANCY
Requirements Amount (mg)
Expansion of RBC 500
Fetus 200
Placenta & Cord 100
Basal losses 200
Blood loss at delivery 200
Total Need 1200
Amount of iron saved due to amenorrhoea 300 mg. Finally iron requirement during
pregnancy is about 1000mg.
Iron deficiency occurs in three stages:
Stage I: Iron Stores depletion
Stage II: Deficient erythropoiesis
Stage III: Iron deficiency anemia

38
5.10.4 Clinical features
Symptoms
Mildly anemic patients are asymptomatic
• Patients complains of difficulty in breathing, Chest pain,palpitation in severe
anemia.
• Weakness, fatigue, impaired work capacity,
• Giddiness , headache,
• Decreased appetite
• Dyspepsia , anorexia
Signs
• Pallor of skin and mucus membrane.
• Glossitis, Stomatitis
• Koilonychia –Initially there will be brittleness and dryness in the nails later
on, there will be flattening and finally concavity (spoon shaped nails).
• Tachycardia
Investigations
Investigations has to be done to find out
(i) Degree and diagnosis of anemia
(ii) The type of anemia
(iii) Cause of anemia

39
Degree and diagnosis of anemia
Heamoglobin estimation by using acid hematin method (sahli’s heamoglobino meter )
Type of anemia
Peripheral bloods smear using leishmann stain to study the morphology of red blood
cells. Presence of small pale staining cells with variations in size (anisocytosis) and
shape (poikilocytosis) suggestive of microcytic hypochromic anemia. This is the most
common blood picture in iron deficiency.
5.10.5 Haematological indices
(i) Mean corpuscular Volume ( MCV)
= Volumes of packed cells per 1000 milliliters RBC in millions per cmm Normal MCV is 68 cubic microns. If it is more than 90, it indicates macrocytosis
(ii) Mean corpuscular Hb .(MCH)
= HB. in gm per 1000 millimeters of blood RBC in millions per c mm Normal value of MCH is 29.5 picograms in iron deficiency anemia; it will be less than 25 pg.
(iii) Mean Corpuscular Haemoglobin concentration (MCHC) = Hb. In gm per 100ml X 100
Volume of packed cell per 100ml It is normally about 34 %. It denotes the actual heamoglobin concentration in the blood.
It is the most common indices affected in iron deficiency anemia.

40
(iv) Packed cell volume (Haematocrit= Volume of packed cells per 100 milliliters of
blood.
The normal value of PCV is about 40% .
(v) Colour index
= Hb. (percentage of normal )
RBC ( percentage of normal)
The normal value is one. If it is less than, the anemia is hypochromic, and if it is more
than one, then it is hyperchromic.
The typical iron deficiency anemia shows the following blood picture
Hemoglobin is less than 10gms%
PCV less than 30%
Red blood cells –less than 4 millions/cubic mm
MCHC less than 30%
MCH less than 25 pico grams.
MCV less than 70 cubic microns.

41
5.10.6 SPECIFIC INVESTIGATIONS FOR IRON DEFICIENCY
INVESTIGATIONS NORMAL VALUES IRON DEFICIENCY ANEMIA
IN PREGNANCY
Serum iron 60-120 microgram/dl <60 microgram/dl
Total iron binding capacity 300-350microgram/dl >400 microgram/dl
Serum ferritin 15-20microgram/lite <i2 microgram/liter
Saturation percentage of
iron
20-45% <16%
Transferrin receptors 2-4mg/litre Increased
Freeerythrocyte
protoporphyrin
0-35microgram/dl I ncreased
Bone marrow stainable
iron (hemosidderin)
Present Absent
Decrease in the concentration of hemoglobin is relatively late in iron deficiency,before
that iron stores get depleted . Serum iron and total iron binding capacity combined to
give the value of transferrin saturation.Transferrin saturation gets reduced when ever
there is deficient iron supply to the tissues,impairment of erythropoiesis, and iron
dependent tissue enzymes are affected.In the development of iron deficiency serum
ferritin is reduced first .it was the first abnormal laboratory finding.

42
TRANSFERRIN RECEPTOR
It is a relatively new method to assess the cellular iron status. There will be no change in
the serum transferrin receptor concentration in early stages of iron store depletion.
Whenever there is tissue iron deficiency. The serum transferrin receptor concentration
increases in direct propotion to the severity of iron deficiency. This change in transferrin
receptor concentration is first change to appear before the reduction in MCV.When
combined with serum ferritin it will give a complete picture of iron status,Serum ferritin
value denotes iron stores ,and transferrin receptor level depicts tissue iron status.
CAUSES OF ANEMIA
To find out the cause of anemia, history taking will be helpful.
Dietary history regarding Total calorie intake, iron content of the food,presence of
haem iron in the diet, patients knowledge about inhibitors and enhancers of food items in
iron absorption, daily protein content in the diet .Obstetric history birth spacing of short
intervals, multiparous women.
Menstrual history regaring menorrhagia
H/O passing worms in the stools
H/O Malarial fever
H/O Recurrent urinary tract infections
URINE EXAMINATION
Urine routine and Microscopy Urine culture and sensitivity

43
STOOL EXAMINATION
Motion ova cyst and occult blood
HOOK WORM ANEMIA
The worm is a habitual blood sucker,it inhabits in the small intestine particularly jejunum
by attaching to the mucous membrane.The average blood loss per day per worm by the
host,for Ancylostoma duonenale is o-2ml, Nector Americans is 0.03ml.
SERUM PROTEINS
It may show hypo proteinemia
5.11 EFFECT OF ANEMIA ON PREGNANCY
The daily iron requirement during pregnancy is approximately 4mgm which will be
increased to6-8 mgm/day from the 32 weeks of gestation.
ANTEPARTUM PERIOD
Cardiac failure may occur at 30-34 weeks of gestation
Pre term labour risk is increased to 3 fold.
Increased susceptibility to infections
Preeclampsia
DURING LABOUR
Incoordinate Uterine contractions.
Postpartum hemorrhage
Cardiac failure

44
Shock
DURING PUERPERIUM
• Cardiac failure
• Puerperal infection.
• Subinvolution
• Lactational failure
• Chronic ill health
FETAL PROBLEMS
• Small for gestational age
• Preterm babies
• Intra uterine growth restriction
LONG TERM SEQULAE
• Short statured and thin built
• Delayed menarche because of poor iron stores.
• GDM in later life
• H.T. atherosclerosis in later life
5.12 CARE OF ANTENATAL WOMEN WITH ANEMIA
All antenatal women with moderate and severe anemia should be admitted in
the hospital for anemia evaluation and further management. Women with severe anemia
Hb is less than7 gms/dl should be evaluated for cardiac failure and anemia should be
treated according to the gestational age
Ante natal management of anemia depends on the degree ,severity of anemia
,and the gestational age

45
5.13 PHARMACOLOGICAL THERAPY OF ANEMIA
Prophylactic iron supplementation
It can be given as selective prophylaxis or routine basis. In the developed countries,
selective administration of iron is given to women with low or depleted iron stores .A
serum level of ferritin is less than 50gm/l is an indication for selective prophylaxis.
WHO Recommends universal iron supplementation with 60 gm elemental iron daily for
6 months in areas, where the prevalence of iron deficiency is less than 40%,.in areas
where the prevalence is more than 40% the recommendation is to continue 3 months
postpartum.
THERAPEUTIC IRON SUPPLEMENTATION
The oral preparation of iron to treat iron deficiency anemia is100 to200mg elemental
iron. Therapeutic dose of iron should be continued till the hemoglobin becomes normal
and should be followed with prophylactic dose of iron 3 months postpartum. The
reticulocyte count begins to rise within 5-10 days. And hemoglobin should increase
0.8gm/dl /week, .Patients who were not responding to iron therapy should be evaluated
for non compliance,presence of ongoing blood loss,any other infections,other nutrient
deficiency.
The ministry of health, Govt of India now recommends 100 mg of elemental iron and
500 micrograms of folic acid as routine supplementation.

46
PARENTRAL THERAPY
The main advantage with parenteral iron is with the certainity of administration.The
increase in hemoglobin is more or less similar to oral iron 1gm/week.
DOSE OF IRON NEEDED mg=normal Hb –patients Hb X weight in kg X 2.21
Another 1000gm of iron to be added to this for replenishment of iron stores
INDICATIONS FOR PARANTERAL IRON
• Intolerance to oral iron
• Non compliance
• Malabsorption syndromes
• No response to oral iron after 4 weeks of therapy
• Moderate to severe anemia in later weeks of gestation
The available iron preparations are iron dextran,iron sorbitol citrate. The intravenous
iron is associated with the possibility of anaphylactic reactions.Other problems are
tachycardia, hypotension,flushing,and syncope.At the site of infusion, thrombophlebitis
can occur.Oral iron should be stopped for atleast 48 hours before paranteral iron to
prevent iron intoxication.At 14 weeks of gestation ,T. ALBENDAZOLE 400mgm should
be given for deworming.
5.14 .BLOOD TRANSFUSION
It is indicated in the following cases of iron defiency anemia,
• Severe anemia with Hb is less than 7grams at any gestational age
• Moderate anemia ( Hb 7-10gm) patients ,when there is no response iron
therapy,after 36 weeks

47
• Severe ante partum hemorrhage and postpartum hemorrhage Packed cell blood
transfusion is preferred than whole blood transfusion because of less volume
overload, lesser incidence of transfusion reactions. One unit of packed cells raise
the hematocrit by 3 to4% and hemoglobin by 0.8 to1gms.
5.15 INTRAPARTUM MANAGEMENT
Strict asepsis should be maintained to prevent purperal sepsis
Nasal oxygen 5 litres /min to the mother to prevent fetal hypoxia.
Adequate cross matched blood should be kept ready
No fluid overload
Second stage of labour should be cut short by prophylactic outlet forceps to prevent
maternal exhaustion.
Active management of third stage of labour should be followed.
Anticipate post partum hemorrhage and kept everything ready.
In case of PPH, adequate amount of blood should be replaced
5.16 POSTPARTUM MANAGEMENT
During puerperium, strict asepsis should be maintained.close monitoring of pulse rate
,blood pressure should be done , measure ment of hemoglobin in the postnatal period is
mandatory.
There is the possibility of deepvein thrombosis,cardiac failure in the immediate puerperal
period ,it should be watched for and managed appropriately. Contraception Advice
regarding spacing of pregnancies contraceptive pills like progesterone only pill should be
prescribed
48
6. PRE ECLAMPSIA
6.1 DEFINITION;
Preeclampsia is defined as a multisystem disorder of unknown
etiology characterized by development of hypertension to the extent of 140/90 mmHg or
more with proteinuria after 20 weeks of gestation in a previously normotensive and non
proteinuric women.
INCIDENCE
The incidence of preeclampsia varies from5-15%. The incidence in
primigravida is about 10% and multigravida is about 5%
6.2 CLASSIFICATION OF HYPERTENSIVE DISORDERS OF PREGNANCY
NHBPEP 2000
GESTATIONAL HYPERTESION
1)Blood pressure 140/90mmHg or more for the first time in pregnancy after 20 weeks of
gestation.
2)No proteinuria
3)Return of BP to normal with in 12 weeks after delivery
4) Other signs of pre eclampsia like headache, epigastric discomfort,or
thrombocytopenia may be present.Final diagnosis is made only after 3 months of
delivery.

49
PRE ECLAMPSIA
BASIC CRITERIA
• Blood pressure 140/90mmHg or more after 20 weeks of gestation.
• Proteinuria 300mgms or more in 24 hours or persistent 1+ or more in dipstick
random samples
DEFINITIVE CRITERIA
• Blood pressure 160/110mm Hg or more
• Proteinuria 2+ on dipstick or 2 gms in 24 hours sample
• Raised serum creatinine(>1.2mg)
• Thrombocytopenia(platelets <1 lakh)
• Evidence of hemolysis(raised LDH levels)
• Elevated liver enzymes ( raised SGOT and SGPT)
• Symptoms of severe pre eclampsia like persistent headache, cerebral or visual
disturbances, or persistent epigastric pain.
ECLAMPSIA
Development of convulsions in a case of preeclampsia ,in the absence of other causes
of convulsion.
SUPERIMPOSED PREECLAMPSIA
Onset of proteinuria of 300 mg/24 hours or more in a woman who had hypertension
but no proteinuria before 20 weeksgestation. Development of sudden increase in
proteinuria ,hypertension,or thrombocytopenia in a womanwho had hypertension or
proteinuria before 20 weeks of gestation.

50
CHRONIC HYPERTENSION
• A known hypertensive woman becoming pregnant with BP 140/90mmHg or
more before pregnancy or diagnosed before 20 weeks of pregnancyin the absence
of gestational troblastic disease.
• Hypertension diagnosed first after 20 weeks but persisting 12 weeks after
delivery.
6.3 ETIOLOGY
The exact etiology of preeclampsia is not known ,it may be due to multiple risk factors.
Various theories put forward to explain the etiology,
ABNORMAL TROBLASTIC INVASION AND PLACENTAL ISCHEMIA
THEORY;
Preeclampsia occurs in two stages
Stage 1; there is failure of secondary wave of trophoblastic invasion of the spiral
arterioles.and the blood supply to the placenta gets reduced.
Stage 2; the effect of placental ischemia due to generalized vasospasm on the mother and
fetus
GENETIC HYPOTHESIS
Genetic conflict hypothesis by Heigs says that maternal BP is determined by the balance
between the fetal factors increasing BP and maternal factors decrease the BP. The level
of raise in solubleFlt-1 denotes the disease severity.

51
IMMUNOLOGICAL THEORY;
This theory states that preeclampsia arises due to inadequate maternal immune response
to the fetal allograft with vascular damage from circulating immune complexes. The
trophoblasts invasion into the myometrium and decidua is mainly cotrolled by
immunological factors. Regulatory Tcells are responsible for specific immune tolerance
to fetal antigens .Previous exposure to paternal antigens is protective against
preeclampsia ,because of this preeclampsia is more common in primigravida.
6.4 RISK FACTORS FOR PREECLAMPSIA
GENETIC FACTORS
Race and Ethnicity more common in Blacks and Asians
Family history of preeclampsia (mothers and sisters)
PRECONCEPTIONAL FACTORS
Nulliparous women
Women with the age group of less than 19 years
Women with age group of more than 40 years
PARTNER RELATED FACTORS
Donor insemination of sperm
Oocyte donation
Change of male partner

52
PRESENCE OF SPECIFIC UNDERLYING DISORDERS
Chronic hypertension
Renal disease
Obesity
Insulin resistance
Maternal low birth weight
Gestational diabetes
Type I diabetes mellitus
Activated protein C resistance
Protein S deficiency
Antiphospolipid antibodies
Hyper homocysteinemia
Sickle cell disease,sickle cell trait.
PREGNANCY ASSOCIATED RISK FACTORS
Multiple pregnancy
Structural congenital anomalies
Hydrops fetalis
Chromosomal anomalies(trisomy13,triploidy
Hydatidiform moles
Urinary tract infection

53
EXOGENEOUS FACTORS
Smoking(risk reduction)
Stress,work related psychosocial strain
Previous history of preeclampsia
6.5 PATHOGENESIS
KEY FEATURES;
Impaired endo vascular cytotrophoblast invasion in the spiral arterioles
Endothelial cell dysfunction and vasospasm
Exaggerated inflammatory response
PLACENTAL DYSFUNCTION
In normal pregnancy ,the cytotrophoblasts invade the spiral arteies of placenta,and the
elastic ,muscular coats are replaced by fibrinoid material. In the second trimester second
wave of tropoblastic invasion occurs,it coverts the blood supply in to slow resistance
high flow system ,there by it increase the uteroplacental blood flow. The primary
tropoblstic invasion is impaired and second wave of invasion is absent in preeclampsia.It
will result in reduced uteroplacental blood flow.
ENDOTHELIAL CELL DYSFUNCTION
Endothelium is one of the main organ involved in the pathophysiology .There is
imbalance between the prostacylin and thomboxaneA2,impairment of nitric oxide-cylic
guanosine monophospate pathway. This results in relative increase in
thrombaxane,which causes vasoconstriction and platelet aggregation

54
ACTIVATION OF THE COAGULATION SYSTEM
Activation of the platlets and cogulation system by the tissue factor which was released
during endothelial cell dysfunction. It will result in consumption of clotting factors and
platelets resulting in thrombocytopenia,all these changes lead to wide spread multiple
small haemorrhages and fibrin deposition in many organs.
PROANGIOGENIC AND ANTIANGIOGENIC PROTEINS;
Proangiogenic proteins are more during early pregnancy for placental angiogenesis, but
nearing term antiangiogenic factors are more towards the preparation of labour. In the
preeclampsia placenta, messenger RNA for sFlt is upregulated,resuting in increased sFlt
in the circulation . This will cause decrease in the concentration of free VEGF and PLGF
in preeclampsia.Another factor soluble form of endoglin starts to increase 6-10 weeks
before the clinical symptoms of preeclampsia.
6.6 PATHOLOGICAL CHANGES IN ORGANS
PLANCETA
Acute atherosis of spiral arteries ,charecterised by fibrinoid necrosis,macrophages and
mononuclear cell infiltration.
KIDNEY
The main pathology is glomerular endotheliosis,this characterized by swollen endothelial
cells due to fibrin deposition.It is clinically presented as proteinuria. In severe cases
,reduction in the glomerular filtration rate and cretinine clearance may occur ,it will
cause increase in the blood urea and serum creatinine, Acute renal injury can occur due
to acute tubular necrosis.

55
LIVER
Subcapsular haemorrhages and periportal necrosis are the main pathological features in
severe form of preeclampsia.SGOT and SGPT are elevated.Subcapsular haematoma may
stretch the liver capsule and produce epigastic pain which is the imminent symptom of
eclampsia.
BRAIN
Cerebral vasospasm in the main pathology,small cerebral
haemorrhages,thrombosis,fibrinoid necrosis,cerebral edema will occur in
eclampsia.Temporary cortical blindness can rarely occur due to the edema of the
occipital lobe.
EYES
The commonest finding is localized retinal vasospasm. Very rarely retinal detachment
may occur , it usually improve
CARDIOVASCULAR SYSTEM;
The commonest findings are generalized vasospasm,increased peripheral
resistance,reduced central venous pressure and pulmonary wedge pressure.
WATER AND ELECTROLYTES;
There is sodium and water retention, it increases the extracellular fluid volume.It will
result in reduction of intravascular compartment and hemoconcentration.

56
6.7 CLINICAL FEATURES
SYMPTOMS;
Usually signs will precede the symptoms.
Edema and excessive weight gain are the usual symptoms.,
Acute onset of preeclampsia presented as follows
Central nervous system; Headache,mostly in the frontal region or in the occipital region
which was not relieved by analgesics.
Gastro intestinalsystem; 1)Epigastric pain or right upper quadrant pain
2)Nausea and vomiting
Visual symptoms like blurring of vision or dimness of vision,scotoma are usually due to
retinal artery spasm and retinal edema, some times loss of vision ,but it usually regains
with in 4-6 weeks after delivery.
Renal symptoms like oliguria haematuria rarely anuria
Pulmonary symptoms like difficulty in breathing due to pulmonary edema or cardiogenic
edema.
SIGNS;
Abnormal weight gain ; Rapid gain in weight may be the first sign in some patients
,weight gaining of more than 1Kg/week or more than 3Kg in a month is significant.
Hypertension; The diastolic blood pressure begins to rise before the systolic pressure
Edema; edema of the non dependent parts usually not relieved by rest, generalized
edema indicates imminent sign for eclampsia.
Pulmonary edema ,because of low oncotic pressure and leaky capillaries.
57
Visual examination reveals retinal artery spasm,retinal hemorrhages,cotton wool
exudates,and papilledema occurs in severe cases.
Abdominal examination shows hepatic enlargement, epigastric tenderness,ascites,
scanty liquor.
6.8 INVESTIGATIONS
(1)Renal function tests;
Urine for protein,pus cells,red cell casts.
24 hours urinary protein
Serum uric acid
Blood urea and serum creatinine
(2)Liver function tests;
SGOT and SGPTwill be elevated
Bilirubin will be elevated
(3)Haematological investigations
Haematocrit,
Evidence of hemolysis on peripheral smear
Thombocytopenia
Lactic dehydrogenase will be elevated
Prolongation of clotting time,APTT,and prothombin time Clot retraction time
4)FUNDUS EXAMINATION ;
(There will be retinal arteriolar vasospasm,and retinal edema initially,it may extend to
cotton wool exudates ,retinal haemorrhages and retinal detachment will rarely occur.

58
6.10 MANAGEMENT
PRIMARY PREVENTION;
PREPREGNANCY;
Women who are overweight or obese advised regarding the benefit of maintaining the
ideal body weight before conception to prevent the incidence of preeclampsia.
First trimester folic acid supplementation and B12 supplementation not only reduce the
neural tube defects and also preeclampsia risk is reduced to 50%
Women with chronic hypertension should be advised regarding control of their BP
before conception. Women with pregestational diabetes should be advised to complete
their family before the development of vascular complications.
SECONDARY PREVENTION
Recurrent risk of preeclampsia in subsequent pregnancies is about 14%, but in women
with prior early onset preeclampsia and chronic hypertension the recurrence is
about50%.
Antiplatelet agents ; Low dose aspirin 50-150mg/day was prescribed ,the mechanism of
action is aspirin will inhibit thromboxane A2 synthesis there by altering the balance
between prostacylin and thromboxaneA2, thus it will prevent the development of
preeclampsia.
Calcium supplementation; The mechanism of action of calcium is to reduce the
parathyroid hormone release and intracellular calcium, this leads to reduce the smooth
muscle reactivity and vasodilatation will occur. Extracellular calcium ion

59
concentrations is the factor involved in the production of endothelial nitric oxide. The
decreased production of nitric acid is implicated in the pathophysiology of preeclampsia.
Heparin or lowmolecular weight heparin; It can be used in women with renal disease and
thrombophilia. Anti oxidants vitamins,Protein and salt restriction has no role in the
prevention of preeclampsia.
6.10 MILD PREECLAMPSIA
OBJECTIVES
• To control the hypertension and prevents its progression in to severe
preeclampsia.
• To prevent the maternal complications like cerebro vascular accidents,renal
failure ,placental abruption,and pulmonary edema.
• To prevent eclampsia
• Delivery of a healthy baby with least trauma.
• Complete restoration of maternal health.
Ideally all cases of preeclampsia should be admitted for evalution and treatment.
Some cases of uncomplicated preeclampsia ,remote from term should be advised home
management, they were instructed regarding the signs and symptoms of imminent
eclampsia,regular antenatal visits twice in a week

60
HOSPITAL MANAGEMENT
Rest in the left lateral position,
ANTIHYPERTENSIVE THERAPY
Anti hypertensive drugs are prescribed when the blood pressure is more than 140/90
mmHg.
Labetalol is a safe and effective drug to control hypertension in the pregnant women.It is
a non selective beta blocker with some alpha blocking property. The dose is 100-200 mg
thrice daily.( maximum of 1200mg)
Nifidipine is a calcium channel blocker the dose is 10-20 mg tds(maximum 120mg).
Alpha methyl dopa 250-500mg tds ,it is a central and peripherally acting anti adrenergic
drug.
MATERNAL MONITORING
• Every 4th hourly BP moitoring
• Daily weight chart
• Urine for proteinuria
• Presence of facial edema and abdominal wall edema
• Symptoms of imminent eclampsia like persistent frontal or occipital
headache,blurring of vision,and epigatric pain
• Intake output chart
• Hemoglobin and platelet count twice in a week
• Renal and liver function tests twice in a week

61
FETAL MONITORING
• Daily fetal movement count
• Non stress test twice a week
• If non reactive NST, biophysical profile
• Ultra sound evaluation of fetal growth every two weeks
INDICATION FOR DELIVERY
Maternal indication;
• Persistent rise in blood pressure ,increase in proteinuria
• Development of imminent signs for eclampsia
• Progreesive decline in the platelet count
• Elevated liver enzymes
• Evidence of hemolysis
Fetal indication;
• Gestational age 37 completed weeks
• Severe oligo hydraminos
• Severe intra uterine growth restriction
• Non reactive NST with abnormal biophysical profile
MANAGEMENT OF LABOUR
INDUCTION OF LABOUR;
At 37 completed weeks of gestation , termination of pregnancy is desirable. If the cervix
is favorable Bishops score more than 6 ,low rupture of membranes followed by

62
syntocinon acceleration shoud be done. If the cervix is unfavourable ,Bishops score less
than 6, prostaglandin E2 induction can be done
INTRAPARTUM MANAGEMENT;
Monitoring of maternal pulse,blood pressure, respiration every 3o minutes
Hourly Urine output, intake chart
Continuous electronic fetal heart rate monitoring or intermittent auscultation of fetal
heart once in 15 minutes during 1st stage of labour, and every 5 minutes during second
stage of labour.
Vaginal delivery is preferred,because operative delivery is associated with more post
operative morbidities.Caesarean section should be performed onlyfor obstetric
indications.Active management of third stage of labour should be followed to reduce the
postpartum blood loss.
6.11 SEVERE PREECLAMPSIA
All severe preeclampia patients should be admitted in the tertiary care hospital. Anti
Hyper tensive therapy should be started immediately,Propylactic anti convulsant regimen
should be given .The goal of anti hypertensives is to keep the diastolic BP between 90-
100 to prevent complications

63
6.11.1 MATERNAL MONITORING
• Bed rest in the left lateral position
• BP monitoring second hourly
• Urine albumin twice a day
• Liver function test Renal function tests on alternate days
• Corticosteroid administration (if the gestational age is less than 34 weeks)
6.11.2 FETAL MONITORING
• Daily fetal movement count
• Daily non stress test
• Ultra sound for liquor adequacy once in two days
• Ultra sound biweekly for assessing fetal growth
6.11.3 INDICATIONS FOR DELIVERY
Persistent rise in BP > 160/110 mm of Hg on women who is receiving anti hypertensives
Oliguria urine output of less than 500ml or less in 24 hours
Thrombocytopenia platelet count less than 50,000
Serum creatinine is raised
Severe head ache or visual disturbances
Any alteration in the coagulation profile
HELLP Syndrome
Placental abruption
Pulmonary edema
Eclampsia
64
Severe IUGR with oligo hydraminos
Doppler parameter alterations CPR <1,reversal of umbilical artery blood flow
Intra uterine death
INDUCTON OF LABOUR
Termination of pregnancy is the treatment for severe preeclampsia, it should be
terminated at 36 weeks .Depending upon the Bishops score we have to induce labour , if
the cervix is favourable , ARM. Oxytocin acceleration shold be done . If the cervix is
unfavourable PGE2 gel to be kept .
INTRAPARTUM MANAGEMENT
Vaginal delivery is preferred . Caesarean section should be performed only for obstetric
indications .Partogram should be maintained.careful monitoring of the fetal heart
because most of the babies are having growth restriction ,they cannot withstand the stress
of labour,more likely to get asphyxiated.Intake output chart should be strictly
monitored.Urine output should be measured hourly.prophylactic magnesium sulphate
regimen should be continued for24 hours.
POSTPARTUM
Active management of third stage of labour should be followed to prevent postpartum
hemorrhage.Anti hypertensives should be continued in the post partum period.Close
observation of severe preeclamptic patients is must ,because of redistribution of blood
flow , they may develop pulmonary edema.

65
6.11.4 COMPLICATIONS OF SEVERE PREECLAMPSIA
MATERNAL COMPLICATIONS
• Elampsia
• Accidental hemorrhage particularly placental abruption
• Cerebral hemorrhage
• Renal failure mostly acute renal injury
• Cardiac failure
• Coagulation failure DIC
• Preterm labour
• HELLP Syndrome
• Visual complications
• Post partum hemorrhage
• Pulmonary edema
FETAL COMPLICATIONS
• Intrauterine growth restriction
• Preterm babies because of induction of labour
• Intra uterine death
• Intrapartum asphyxia
After discharge patient should be followed for 6 weeks , We have to advise the patient to
continue antihypertensive therapy., weekly checkup in the postpartum period.If the blood
pressure is not coming down after six weeks , we have to evaluate the patient for chronic
hypertension.

66
7.AIM OF THE STUDY
• To find out the incidence of preeclampsia in mild, moderate, and severe anemia.
• To analyse the synergistic effect of anemia with preeclampsia in pregnancy
associated Morbidity and Mortality.
8. MATERIALS AND METHODS
This prospective observational study was carried out at Govt.KasturbaGandhi
Hospital for women and children,Madras medical college, Chennai,during the period of
December 2012 to December 2013 on 200 patients. The study was approved by the
hospital ethical committee.
8.1 INCLUSION CRITERIA
All antenatal women diagnosed to be having anemia with singleton pregnancy after 20
weeks of gestation,
8.2 EXCLUSION CRITERIA
• Multiple pregnancies
• Pre gestational diseases like renal disease, diabetes mellitus, autoimmune disease,
• Known hypertensive
• Immunocompromised individuals
• Gestational age less than 20 weeks
• Other hemolytic anemia and heritaryanemia
67
8.3 METHODS
Pregnant women attending the antenatal out patient department and labour ward in
Govt.Kasturba Gandhi Hospital with hemoglobin value less than 11gms and after 20
weeks of gestation were selected for the study.The patients who selected were explained
about the study and their consent obtained.
The base line data recored at the first antenatal visit included the following;
• Maternal age
• Gestational age at present
• Parity status
• Socio economic status
• Associated pregnancy complications
• Previous pregnancy
• Interpregnancy interval
• Family history of preeclampsia
• Maternal weight
• H/o smoking
• Blood pressure
• Hemoglobin value at first visit
• Urine albumin
After recording the base line data, patients with moderate and severe anemia were
advised admission for anemia evaluation and treatment .In these patients the incidence of
preeclampsia at the time of admission were calculated. The patients with preeclampsia
were admitted and the following investigations were carried out.

68
• Complete haemogram with peripheral smear
• Blood sugar, urea ,serum creatinine,
• Liver function test
• Urine analysis
• 24 hours urinary protein
• Fundus examination
• ECG In all leads
The selected patients were monitored and followed till delivery. According to the
severity of anemia and the gestational age, patients were treated with oral iron, parenteral
iron,or by blood transfusion. All preeclampsia patients were classified in to mild and
severe type, according to the severity gestational age, they were treated with
antihypertensives, prophylactic anticonvulsant regimen,and termination of pregnancy.
They were followed through the antepartum,intrapartum,and post partum period . Finally
I analysed the mode of delivery,pregnancy complications, maternal outcome ,morbidity
and mortality and perinatal outcome.
8.4 STATISTICAL METHODS
The statistical methods employed in the study were The Excel were used for data
entry,and SPSS software were used for analysis

69
MEAN
CHI SQUARE TEST
X2=∑ (Oi-Ei)2
Ei
Where Oi is observed frequency and Ei is expected frequency, with (n-1) difference.
SIGINIFICANT P VALUE
If the P value is 0.000 to 0.010 it imply Significant at 1 level (Highly Significant)
If the P value is 0.011 to 0.050 it imply Significant at 5 levels (Significant)
If the P value is 0.051 to 1.000 it imply Not Significant at 5 level (Not Significant)

70
9.RESULTS AND ANALYSIS
This prospective observational study was conducted at Govt. Kasturba Gandhi Hospital
during the period of December 2012 to December2013.
Sample of the study was 200 cases.

71
AGEDISTRIBUTION TABLE 1
Frequency Percent Valid < 19 27 13.5 20-29 144 72.0 30-35 28 14.0 > 35 1 .5
Most of the patients in the study population were in the age group of 20 to 29
years.followed by age group of 30-35 years.
13.5% of the patients were in age group less than 19 years.
The youngest age in the sample was 14 years, and the eldest was 36 years.
AGE DISTRIBUTION
<19
20-29
30-35
>35

72
DISTRIBUTION OF GRAVIDITY TABLE 2
Frequency Percent Primi 89 44.5 Second
Gravida 97 48.5
Third Gravida
14 7.0
Most of the cases were in second gravida .48.5% of cases were in second gravida.
44.5% of cases were in primigravida.
7% of cases were in third gravida.
DISTRIBUTION OF GRAVIDITY
PRIMI
G2
G3

73
DISTRIBUTION OF SOCIO ECONOMIC CLASS TABLE 3
Frequency Percent IV
155 77.5
V 45 22.5
Most of the cases were in lower socioeconomic groups.
77.5% of cases were in class IV socio economic group.
22.5% of cases were in class V socioeconomic group.
DISTRIBUTION OF SOCIOECONOMIC CLASS

74
DISTRIBUTION OF BOOKING STATUS TABLE 4
Frequency Percent B
199 99.5
UB 1 .5
99.5% were booked cases
0.5% was unbooked case . there was only one case unbooked among 200 study
population.
Booked status

75
REFERRAL STATUS TABLE-5
Frequency Percent Yes
55 27.5
No 145 72.5
27.5% of cases were referred from near by govt.hospitals, because of associated
pregnancy complications.

76
LITERACY STATUS TABLE 6
Frequency Percent Illiterate 15 7.5 Primary 35 17.5 Middle 44 22.0 High
School 79 39.5
HSc 22 11.0
Graduate 5
2.5
39.5%of cases were studied up to high school level.
7.5% were illiterate.
22% of cases were studied at primary level.
11% of cases were studied up to higher secondary level.
5% of cases were graduates.

77
DISTRIBUTION OF MATERNAL WEIGHT
Frequency Percent < 50 5 2.5
50-60 80 40.0 60-70 83 41.5 > 70 32 16.0
Most of the cases were in the weight group of 60 to 70 kg constitutes about 41.5%.
2.5%of the cases were in the weight range of under 50 kg.
40% of the cases were in the weight range of 50 to60 kg.
16% of cases were in the weight range of above 70 kg.

78
DISTRIBUTION OF GESTATIONAL AGE TABLE 8
Frequency Percent TERM
153 76.5
36-38 15 7.5 34-36 25 12.5 28-34 5 2.5 < 28 2 1.0
76.5% Of the cases were in the term gestation.
12.5% of the cases were in the 34 to 36 weeks of gestation.
7.5% of the cases were in the 36 to 38 weeks of gestation.
2.5% of cases were in the 28 to 34 weeks of gestation.
1% of cases were in the<28 weeks of gestation.

79
DISTRIBUTION OF SEVERITY OF ANEMIA TABLE 9
Frequency Percent
10-11 12 6.0
7-10 166 83.0
< 7.0 22 11.0
83% of the cases were in the moderate anemia.(Hb 7.5-10gms).
11% of the cases were in the severe anemia(Hb < 7.0 gms).
6% of the cases were in the mild anemia (Hb 10-11gms).
SEVERITY OF ANEMIA
10-11gms
7-10gms
<7gms

80
DISTRIBUTION OF PERIPHERAL SMEAR TABLE 10
Frequency Percent Microcytic hypo chromic 170 85.0
Normal 30 15.0
Total 200 100.0
DISTRIBUTION OF PERIPHERAL SMEAR
Microcytic hypochromic
Normocytic normochromic

81
DISTRIBUTION OF PLATELET COUNT - TABLE 11
Frequency Percent > 100000 195 97.5
100000-50000 4 2.0 < 50000 1 .5
Most of the cases were having the platelet count above 1 lakh count, it consistutes about
97.5%.
2% of cases were having the platelet count between 1 lakh-50,000.
0.5% of cases were having thrombocytopenia( plate count <50.000).

82
DISTRIBUTION OF SEVERITY OF BLOOD PRESSURE TABLE 12
Frequency Percent 120/80
128 64.0
DBP 90
19 9.5
DBP 100
30 15.0
>160/110 23 11.5
64% of the cases were in the normotensive group in the blood pressure range of
(120/80)mmHg.
11.5% of the cases were in the blood pressure range of >160/110mmHg.
15% of the cases were in the diastolic blood pressure 100 .9.5%of the cases were in the
diastolic blood pressure 90

83
DISTRIBUTION OF URINE ALBUMIN TABLE 13
Frequency Percent
Nil 150 75.0
Trace 17 8..5
1+ 11 5.5
2+ 13 6.5
3+ 6 3
4+ 3 1.5
75% of the cases were having urine albumin nil.
8.5% of the cases were having urine albumin trace.
5.5% of the cases were having urine albumin1+.
6.5% of the cases were having urine albumin2+.
3% of the cases were having urine albumin3+.
1.5% of the cases were having urine albumin4+

84
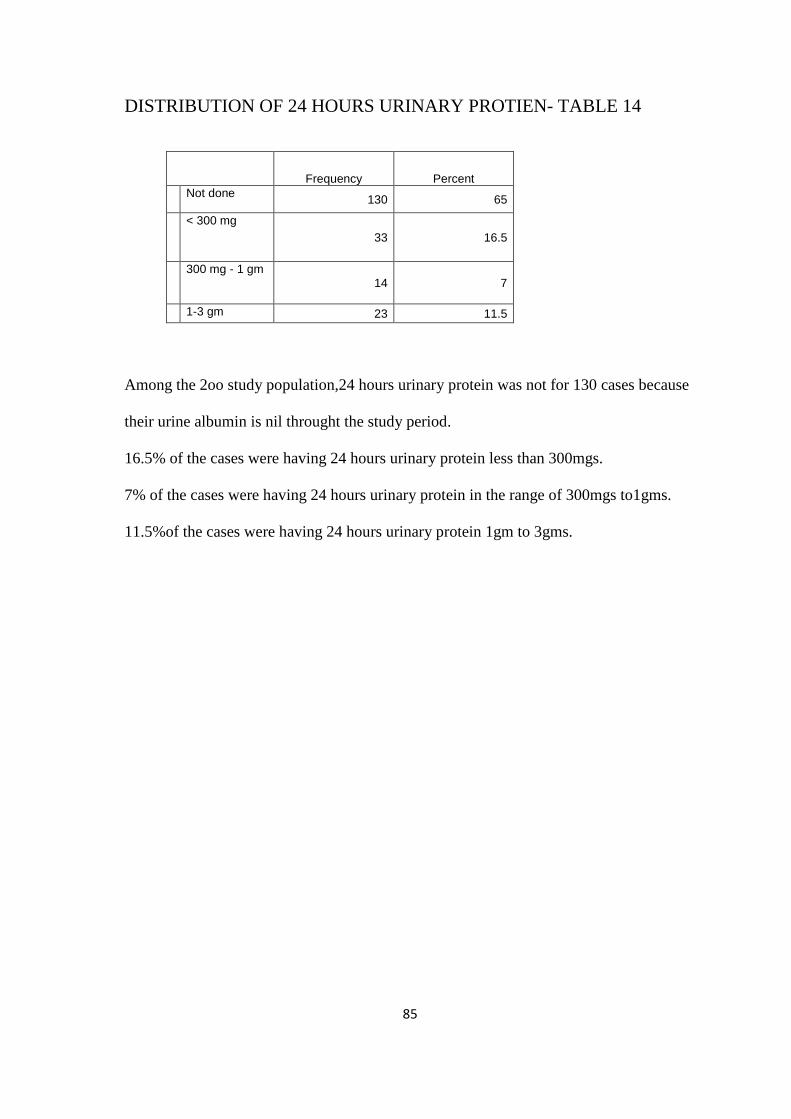
85
DISTRIBUTION OF 24 HOURS URINARY PROTIEN- TABLE 14
Frequency Percent Not done 130 65
< 300 mg 33 16.5
300 mg - 1 gm 14 7
1-3 gm 23 11.5
Among the 2oo study population,24 hours urinary protein was not for 130 cases because
their urine albumin is nil throught the study period.
16.5% of the cases were having 24 hours urinary protein less than 300mgs.
7% of the cases were having 24 hours urinary protein in the range of 300mgs to1gms.
11.5%of the cases were having 24 hours urinary protein 1gm to 3gms.

86
ONSET OF LABOUR TABLE 15
FREQUENCY PERCENTAGE
ELECTIVE LSCS 13 6.5
SPONTANEOUS ONSET 146 73
INDUCTION OF LABOUR 41 20.5
73% of the cases were developed spontaneous onset of labour , followed by
syntocinon acceleration.
6.5% of cases were posted for elective LSCS.
20.5% of the cases were undervent induction of labour.

87
MODE OF DELIVERY TABLE 16
Frequency Percent Labour natural 92 46.0 Primary LSCS 63 31.5 Breech 4 2.0 Rpt LSCS 15 7.5 Instrumental 8 4.0 Rpt LSCS with ST 10 5.0 Rpt LSCS with CuT 4 2.0 VBAC 1 .5 SpontaneousExpulsion 3 1.5
46% of the cases were delivered labour naturally.
Primary LSCS constitutes about 31.5%.
Assisted breech delivery constitutes about2%
Repeated LSCS delivery constitutes about 14.5%.
Instrumental delivery constitutes about 4%.
Vaginal birth after caesarean constitutes about 0.5%
Spontaneous expulsion of the fetus was occurring in 1.5%.
MODE OF DELIVERY
Labour natural
Primary LSCS
Breech
Repeat lscs
Instrumental
VBAC
Spont.expulsion

88
MATERNAL OUTCOME TABLE 17
Complications Frequency Percentage ATONIC PPH 12 6 WOUND INFECTION 4 2 PULMONARY EDEMA 3 1.5 DEATH 1 0.5 HELP SYNSDROME DIVC 1 0.5 ABRUPTIO PLACENTA 2 1 ACUTE RENAL INJURY ECLAMPSIA 4 2
AtonicPPH occurs in 6% of the study population.Pulmonary edema occurred in 1.5%,
Death occurred in one case in the studypopulation.Both HELLP and DIVC occurred in
one case 0.5%.Abruptio placenta occurred in 1%.Eclampsia occurred in 2% of the cases.

89
FETAL OUTCOME - TABLE 18
Frequency Percent Term
155 77.5
Preterm
15 7.5
IUGR 24
12.0
Still Birth 6 3.0
77.5% of the babies were term babies.
Preterm babies constitutes about 7.5%.
IUGR babies constitutes about 12%.
3% of the babies were still born.

90
BIRTH WEIGHT TABLE 19
KG FREQUENCY PERCENT
<1.5 7 3.5
1.6 – 2.0 17 8.5
2 – 2.5 63 31.5
2.5 – 3.0 62 31
3.0 – 4.0 51 25.5
31% of the babies born were in the birth weight 2.5 to 3Kg.
31.5% of the babies born were in the birthweight 2to 2.5.kg.
25.5% of the babies born were in the birth weight 3to 4Kg.
8.5%of the babies born were in the birth weight 1.6 to2Kg.
3.5% of the babies born were in the birthweight <1.5 Kg.
.
BIRTH WEIGHT
<1.5KG
1.6-2KG
2-2.5KG
2.5-3KG
3-4 KG

91
BLOOD TRANSUSION TABLE 20
Frequency Percent Yes
75 37.5
No 125 62.5
Among the 200 sample population , blood transfusion was given for 37.5%.

92
CROSS TABLE HEMOGLOBIN AND BLOOD PRESSURE TABLE 21
HEMOGLOBIN
Gms/dl
BLOOD PRESSURE mm Hg
120/80 DBP 90 DBP100 >160/110
10-11 10 2 0 0
7-10 112 15 24 15
<7 6 2 6 8
FREQUENCY 128 19 30 23
PERCENT 64% 9.5% 15% 11.5%
Chi-Square Tests
Value df Asymp. Sig. (2-
sided) Pearson Chi-Square 24.465(a) 6 .000
Likelihood Ratio 24.034 6 .001 Linear-by-Linear Association
20.547 1 .000
This study showed the incidence of preeclampsia increases with the severity of anemia
,the p value is .000 which was highly significant.

93
Heamoglobin
< 7. 7-1010-11
Count
120
100
80
60
40
20
0
BP
120/80
DBP 90
DBP 100
>160/110

94
CROSS TABLE MATERNAL OUTCOME AND BP TABLE 22
COMPLICATIONS
FREQUENCY
BLOOD PRESSURE mmHg
120/80
DBP90
DBP100
>160/110
1.ATONIC PPH 12 7 1 4 0
2.WOUND INFECTION 4 2 0 2 0
3.PULMONARY EDEMA 3 1 1 0 1
4.DEATH 1 0 0 0 1
5.HELLP SYNDROME&DIVC 1 0 0 1 0
6.ABRUPTIOPLACENTA 2 0 1 1 0
7.ECLAMPSIA 4 0 0 2 2
Chi-Square Tests
Value df Asymp. Sig.
(2-sided) Pearson Chi-Square 60.882(a) 30 .001 Likelihood Ratio 44.083 30 .047 Linear-by-Linear Association 9.644 1 .002
N of Valid Cases 200
The cross table relates the maternal outcome with the severity of blood pressure, which
was significant with the p value of0.001.

95
10. DISCUSSION
This prospective observational study was conducted in Govt. KasturbaGandhi hospital
during the period of December 2012 to December2013. To find out the incidence of
preeclampsia in 200 antenatal anemic mothers and assessing the maternal morbidity and
mortality in anemia associated preeclampsia.
TABLE 1
Most of the patients in the study population were in the age group of 20 to 29
years, It constitutes about 72%
This is consistent with the study conducted by Emre Karashin at Gilbane Military
Medical Academy during the period 2006, showed that the mean age of anemic mothers
was 28.3 years.
TABLE 2
DISTRIBUTION OF GRAVIDA
Most of the cases were in the second gravida 48.5%.
A Retrospective cohort study conducted by Ram Hari Ghimire at Nepal to study the
association between maternal and perinatal complications during the period of April
2011- April 2012 stated that anemia was more common in multigravida ,that study
consistuted 6o% of the cases were multigravida. Women with their last child birth with
in 1 year 6 month developed moderate anemia(7.2%) and severe anemia (31.8 %) in the
study population.The estimated p value is .010 which was significant.

96
TABLE 3
In this study, all the patients were belonging to lower socioeconomic class. Of these
77.5% were in the class IV socio economic status.
A Multi Center Cross sectional study conducted at Kualalampur Malaysia Clinal
Research Center, by Jamaiyah Haniff during the period March 2005 stated that anemia
was more common in the lower socioeconomic class 3 and 4 constituted about 56%..
TABLE 4 & 5;
In this study, most of the cases about 99.5% were booked. Among these booked cases
only 70% were booked in our hospital.
27.5% of the patients were referred from nearby Primary health center , Government
hospitals and private hospitals for Institutional management.
TABLE 6
EDUCATIONAL STATUS;
In this study , only 7.5% of the patients are illiterate.39.5% of the patients were studied
up to high school,17% of the patients were studied up to primary school.But this was not
correlate with other studies stated that anemia was more prevalent among the illiterate .
This study was consistent with the Multicenter Cross sectional study at Malaysia during
the period March 2005 showed 61.2% of women were studied up to secondary level.

97
TABLE 7:
MATERNAL WEIGHT
40% Of the patients were in the weight range 50 to 60 kg, 41.5% of the patients were in
the weight range of 60- 70 kg. 16% of the patients were in weight group above 70kg.
This study was found that there was no significant association between maternal weight
and anemia.
A retrospective population based study conducted by AK Mach , JL Kornosky to study
the association between obesity subtypes and the risk of early and late onset
preeclampsia, the results showed that increased BMI and rate of increase in weight gain
increased the incidence of preeclampsia.
The women weighing more than 70 kg were developed preeclampsia (50%). There was
significant association between maternal excessive weight and preeclampsia, the p value
was0.000 which was highly significant.
TABLE -8
DISTRIBUTION OF GESTATIONAL AGE AMONG THE STUDY POPULATION;
76.5% of the patients were in term gestation, this study was correlate with other studies
that anemia was more prevalent during the third trimester. A prospective observational
study was conducted by Nesa Asnafi, Saeed sina at Yahyanejud Gynaecology and
obstetric clinic during the period of March 2000 to August 2000 to find out the
prevalence o anemia in pregnant women and its relationship to mothers age and
gestational age stated that anemia was more common in the third trimester than first and
second trimester (p value was < 0.05).

98
A prospective observational study was conducted at The health center Tuzla during the
period Jan2009 to 2010 by Lejla Mesalic to to find out the prevalence of anemia per
each trimester as well as the correlation between anemia parameters and gestational age
stated that the average value of haematocrit in the third trimesterwere significantly lower
than the firstand second trimester , the p value was ( 0.0008).
TABLE 9
SEVERITY OF ANEMIA
In this study 83% of the patients were in the moderate anemia with Hb 7.to 10 gms. 11%
of the patients were in the severe anemia with H b less than7grams. This study was
correlated with the descriptive case study at Karnataka by R. G. Viveki during the
period of March 2010 to July 2010 showed that 82.9% of the study population were
mildly anemic, 50% were moderatively anemic and 7% were severely anemic.
A Hospital based Record study was conducted at the tertiary hospital in Pune by Pankaj
kumar during the period of July 2011 to August 2011 showed that 44.4% of the cases
were moderately anemic, 2% of the cases were severely anemic and 53.96% of the
cases were mildly anemic.
TABLE 11
PLATELET COUNT
Most of the cases were having the platelet count above 1 lakh count, it consistutes about
97.5%. 2% of cases were having the platelet count between 1 lakh-50,000. 0.5% of cases
were having thrombocytopenia (plate count <50.000). There was significant association
between platelet count and severe preeclampsia.

99
TABLE 12
DISTRIBUTION OF SEVERITY OF BLOOD PRESSURE
This study was showed that 64% of the cases were in the normotensive group in the
blood pressure range of (120/80)mmHg. 11.5% of the cases were in the blood pressure
range of >160/110mmHg. 15% of the cases were in the diastolic blood pressure 100.
In India the incidence of pre eclampsia was about 8 to 10 % of all pregnancies. This
study showed the incidence of preeclampsia was about 18.5%, and the gestational
hypertension consistuted about 17.5% in anemia complicating pregnancy.23%of cases
were received antihypertensive drugs, 13.5%of cases were treated with Mg so4 regimen.
A retrospective cross sectional study was conducted at Anand district Gujarat during the
period of Febuary 2007 – May 2007 by Punam .D. Sachdeva , B.G. Patel to find out the
incidence and management of pregnancy induced hypertension showed that the
incidence of pregnancy induced hypertension was 14.7% .
TABLE 13 AND 14
URINE ALBUMIN
In this study 6.5% of the patients were having 2+ urine albumin. 3% of the patients were
having 3+ urine albumins. 1.5 % of the patients were having 4+ urine albumin.
24 HOURS URINARY PROTEIN
16.5% of the cases were having 24 hours urinary protein less than 300mgs.
7% of the cases were having 24 hours urinary protein in the range of 300mgs to1gms.
11.5%of the cases were having 24 hours urinary protein 1gm to 3gms.

100
Only 10% of the patients were having significant protienuria by using salphosalicylic
method for estimating urinary protein.By comparing it with 24 hours urinary protein,
18.5% of the cases were found to be having significant proteinuria.
TABLE15
ONSET OF LABOUR
In this study ,73% of the patients were having spontaneous onset of labour, which was
accelerated by low rupture of membranes and oxytocin acceleration.
20.5% of the patients undervent induction of labour using prostaglandinE2 gel.,of these,
5% of the patients were induced for postdatism,11.5% of the patients were induced
because of preeclampsia. 2% were induced for imminent eclampsia, 2% were induced
for oligohydraminos.
TABLE16
MODE OF DELIVERY
46% of the cases were delivered labour naturally .Primary LSCS constitutes about
31.5%.
Assisted breech delivery constitutes about2% Repeated LSCS delivery constitutes about
14.5%.
Instrumental delivery constitutes about 4%. Vaginal birth after caesarean constitutes
about 0.5% .Spontaneous expulsion of the fetus were occurring in 1.5%.
INDICATION FOR PRIMARY LSCS
Fetal distress consistuted about 15.5%, Cephalo pelvic disproportion consistuted about
6.5%,Failed induction -3.5%, Severe oligohydraminos-3%, Preeclampsia-2%, In anemia

101
associated preeclamptic patients , 8% were delivered labour naturally,Primary LSCS -
12.5%, Repeat LSCS -3%.
Of these preeclamptic anemic patients, Indication for primary LSCS were fetal distress
in 4.5%, failed induction-2.5%,severe oligohydraminos1.5%,preeclampsia -2%,
Cephalopelvic disproportion-2%
This was comparable with the study conducted by Vitthal.G.Kuchae , Sunny .K.Kohalae
at Indira Gandhi Memorable hospital during the period July2009-Febuary2010 showed
that in preeclamptic patients 34.24% had normal vaginal delivery.65.5% had caesarean
section.
TABLE17
MATERNAL OUTCOME
AtonicPPH occurs in 6% of the study population.Pulmonary edema occurred in 1.5%,
Death occurred in one case in the studypopulation.Both HELLP and DIVC occurred in
one case 0.5%.Abruptio placenta occurred in 1%.Eclampsia occurred in 2% of the cases.
The comparison of maternal outcomes with anemia complicating patients and anemia
associated with preeclamptic patients were atonic postpartum hemorrhage in anemic4%
and preeclampsia associated patients -2%, post operative wound infection1% in the both
groups, pulmonary edema 1% in anemic patients,0.5% in preeclamptic patients,Death
occurs in one patient among the study population the cause of death was severe
preeclampsia associated with pulmonary edema and severe anemia.HELLP syndrome
occurs in one patient we saved the patient with l8 units of fresh frozen plasma.Abruptio

102
placentae 0.5% in both the groups.Among the eclampsia 3 patients had antepartum
eclampsia and one patient had postpartum eclampsia.
This study was correlated with the descriptive study conducted at J. Ayub Medical
college Abbottabad by Riaz, S.Habib during the period of Jan2010-Dec2010 among the
100 patients with pregnancy induced hypertension showed the following Placental
abruption occurred in 4%.pulmonary edema in 2%,HELLPsyndrome in 5%, ecclampsia
in3%,1 maternal death.
TABLE 18 AND19
FETAL OUTCOME AND BIRTH WEIGHT OF THE BABIES
77.5% of the babies were term babies.Preterm babies constitutes about 7.5%. IUGR
babies constitutes about 12%.3% of the babies were dead 1.5% intrauterine .1.5%
perinatal death. 31% of the babies born were in the birth weight 2.5 to 3Kg.31.5% of the
babies born were in the birthweight 2to 2.5.kg.25.5% of the babies born were in the birth
weight 3to 4Kg. 8.5%of the babies born were in the birth weight 1.6 to2Kg.3.5% of the
babies born were in the birthweight <1.5 Kg.
This study was compared with a retrospective cohort study at Nobel medical college
Nepal by Ram Hari Ghimire, SitaGhimire during the period of April 2011 to April2012
to find out the association between anemia and perinatal and maternal complications
showed the following, Intra uterine death occurred in 6%, Preterm babies about 9.9% ,
IUGR babies -8.6%,Low birth babies -22%, Perinatal death 11%.
In this study , 72% of the patient had taken iron and folic acid,22% of the patient had
treated with parenteral iron preparations, 37.5% of the patient received blood
103
transfusion,2.5% of the patients had received fresh frozen plasma along with blood
transfusion.
TABLE 21
STATISTICAL ANALYSIS BETWEEN HEMOGLOBIN AND BLOOD PRESSURE
This study showed the association between anemia and the preeclampsia, anemic
patients were more prone to develop preeclampsia due to associated hypo proteinemia.
More severe the anemia, greater the chance to get preeclampsia. Incidence of
preeclampsia in the study was 18.5%, the p value shows .000 highly significant,
This study was co relate with the study conducted by J.J.Zhang, J. Grewal,J.P.souza,
they used the data from WHO Global Surveyfor maternal and perinatal health collected
in hospitals from2007-2008 to analyse the several types of anemia were risk factors for
developing hypertensive disorders during pregnancy in the developing countries,the
results showed that multiparous women with severe anemia were increased chance to get
gestational hypertension( ODDS RATIO 1.58)confidence interval of( 1.15-2.19).
Nulliparous women with severe anemia were having significant correlation with
preeclampsia(OR)3.55; 95% CI2.87-4.41, Multiparous women with severe anemia were
having increasedrisk to develop preeclampsia (OR;3.94;95% CI 3.05-5.09).Cochrane
case control trial titled as Interrelationship between iron deficiency anemia and
impaired renal function in toxemia of pregnancy by Fernandez.G, Diez EM, Velaquez
N, conducted during1976, showed that increased coexistence of preeclampsia in anemic
patients.

104
A retrospective case control study conducted at Sudan by Abdel Aziem A Ali showed
that the corrected risk of preeclampsia increased only in severe anemia
(OR=3.6,p=0.007)
Disscussion
NEAR MISS CASES IN THE STUDY
There were three cases found to be near miss throughout the study period.
CASE 1
23 years old primi with term gestation , referred from Koovathur PHC, admitted with
complaints of epistaxis and hemoptysis , we diagnosed her, as a case of severe
preeclampsia with severe anemia . Her hemoglobin was 7gms and platelet count was 1
lakh twenty thousand, we had treated her with 8 units of fresh frozen plasma,Mgso4
regimen was started, cerviprime gel induction was done, patient was delivered labour
naturally after 8 hours of induction, Active management of third stage of labour was
followed, 2 hours later she developed pulmonary edema, we treated her with frusemide
and connected to the continuous positive pressure ventilation. Her Hb was 6 gms in the
postnatal period we transfused with two units of packed cell transfusion.
CASE 2
20 years primi with 34 weeks of gestation , referred from chemmancherry PHC, as
severe anemia with preeclampsia admitted with labour pains,we diagnosed her as a case
of severe preeclampsia associated with severe anemia (Hb 6.7 gms , platelet count
normal) patient was in active stage of labour , she delivered a preterm baby with in 2
hours of admission.we treated her with antihypertensives and Mgso4 regimen, suddenly
she developed post partum eclampsia and became unconscious , we connected the
patient to the ventilator, strict fluid management, intravenous labetalol was given ,After
105
36 hours, patient was slowly weaned off from artificial respiration.After giving
frusemide we transfused 3 units of packed cell transfusion once in 5 days in the
postnatal period.
CASE 3
28 years primi with term gestation, known case of gestational hypertension with on
T.Labetalol for the past one month ,admitted with labour pains On examination patient
was found to be moderately anemic Hb was 8.4 gms and platelet count was 1 lakh,10
thousand , Emergency LSCS was done for CPD with fetal distress. Two hours after
surgery , patient developed abdominal distension and difficulty in breathing,ultrasound
abdomen & pelvis was done it showed that there was some fluid collection in the
peritoneal cavity. Emergency Relaparotomy was done, uterus was found to be atonic
stepwise devascularisation was proceeded, the patient platelet count was 50,000 and
elevated liver enzymes was there , diagnosed as partial HELLP and DIVC. Patient was
connected to the ventilator,totally 9 units of packed cells, 26 units of fresh frozen
plasma, 16 units platelets, 4 units cryoprecipitate was given. In the post operative period
she developed wound gappimg,for which wound resuturing was done

106
11. SUMMARY
This prospective study titled as Incidence of preeclampsia in 200 antenatal anemic
mothers attending the tertiary care referral center and maternal mortality in anemia
associated preeclampsia was conducted at Govt.KasturbaGandhi Hospital for women
and children,Madras medical college, Chennai,during the period of December 2012 to
December 2013 .
Sample size was 200 antenatal women with anemia ( hemoglobin concentration less than
11gms)
The observation of this study were the following
• Most o the patients in the study population were in the age group20-29 years (72%).
• 48.5% of the patients were second gravida.
• 77.5% of the patients were belonging to class IV socioeconomic class.
• 99.5% of the cases were booked Of this 70% were booked at KGH.
• 27% of the cases were referred from other hospitals of these 14.5% had hypertensive
disorder,5.5% of the cases had severe anemia.
• 41.5% of the patients in the study population were in the weight group 60-70 kg .
• 76.5% of the study population were in the term gestation.
• 83% of the patients were moderately anemic.
• 11% of the patients were severely anemic.
• 85% of the study population were microcytic hypochromic peripheral smear picture
and 15% were normochromic normocytic picture.
• Incidence of severe preeclampsia was 11.5%.
• Incidence of mild preeclampsia was 7%.

107
• 11.5% of the patients had 1-3gms of protein in 24 hours urinary collection.
• 13.5% of the patients were treated with Magnesium sulphate regimen along with
antihypertensive drugs.
• 73% of the study population had spontaneous onset of labour,20.5% of the cases
labour was induced .
• 46% of the cases delivered labour naturally,31.5% of patient had primary caesarean
section,14.5% had repeat caesarean section, Instrumental delivery constitutes about
4%. Vaginal birth after caesarean constitutes about 0.5% .Spontaneous expulsion of
the fetus were occurring in 1.5%.
• Indication for primary LSCS ;Fetal distress consistuted about 15.5%, Cephalo
pelvic disproportion consistuted about 6.5%,Failed induction -3.5%, Severe
oligohydraminos-3%, Preeclampsia-2%, of the study population
• Maternal outcome; AtonicPPH -6%.Pulmonary edema -1.5%, Death occurred in
one case in the studypopulation.Both HELLP and DIVC occurred in one case
0.5%.Abruptio placenta occurred in 1%.Eclampsia occurred in 2% of the cases.
• 77.5% of the babies were term babies.Preterm babies constitutes about 7.5%. IUGR
babies constitutes about 12%.3% of the babies were dead 1.5% intrauterine .1.5%
perinatal death.
108
12.CONCLUSION
In most of the developing countries, anemia during pregnancy is the major problem
causing maternal morbidity and mortality and adverse neonatal outcome. Anemia is
responsible for both direct and indirect cause of maternal mortality. Anemia was the
direct cause for 20% of maternal deaths in India. The indirect causes of death due to
anemia was constituted about 20% It may be due to cardiac failure, post partum
hemorrhage, infection and preeclampsia .One of the most important complication of
preeclampsia is eclampsia , which was the direct cause of maternal mortality of about
13% in India. The incidence of preeclampsia was increased more so when it was
associated with chronic severe anemia and hypoproteinemia.
The coexistence of preeclampsia in anemic women’s worsening the situation. In
preeclampsia, there was already intravascular volume depletion hence anemia gets
masked the patients are not able to cope up even with mild blood loss during delivery, In
anemia associated with preeclampsia, even a small volume of blood loss of about 200ml
during the third stage of labour causes postpartum collapse and death if the blood loss
was not adequately replaced with blood transfusion. The fluid management in severe
preeclampsia with anemia is very difficult task in view of leaky pulmonary capillaries
that would result in volume overload, and pulmonary edema.
Various researches had shown that, during the antenatal visits less than 50% of pregnant
women were getting health education about preeclampsia and long term complications of
hypertensive disorders of pregnancy in the western population. In India most of the
pregnant women were unaware of the anemia and hypertensive disorders of pregnancy
and its complications. We have to counsel the pregnant mothers during their antenatal

109
checkup regarding the importance of blood pressure monitoring, screening and
correction of anemia prior to pregnancy and Iron and folic acid supplementation.
The risk factors of preeclampsia, any excessive weight gain ,any pedal edema which was
not relieved by rest and signs of imminent eclampsia should be informed to the antenatal
women, so that when it appears ,they would reach the nearby Emergency obstetric center
on right time, this requires community participation.
The data from National Nutritional Monitoring Bureau (NNMB) stated that the intake of
iron and folic acid in all the age groups were still low even after the implementation of
National Anemia prophylaxis programme.
In this study we had three near miss cases, all the cases were referred from primary
Health Center as preeclampsia with anemia, during their stay in the hospital, they
developed both the complications of anemia and preeclampsia like postpartum
eclampsia, pulmonary edema, HELLP syndrome and DIVC. Being a Tertiary care
Institute we were able to manage them successfully hence those cases were grouped
under Near Miss cases .The delivery of the preeclamptic anemic patients , should be
conducted in the Tertiary Care center with High dependency unit along with neonatal
intensive care unit, and blood bank .Careful monitoring of both the mother and baby
and anticipation of severe complications like eclampsia , postpartum hemorrhage,
abruption placenta, pulmonary edema, HELLP syndrome readiness to tackle those
complications will go a long way to reduce the maternal morbidity and mortality. The
Tenth plan strategies has to be effectively implemented to all pregnant women with
anemia to reduce the maternal mortality and morbidity and long term consequences of
anemia.

110
BIBILIOGRAPHY
1.AbdelAziem A Ali1, Duria A Rayis2, Tajeldin M Abdallah1 Severe anaemia is
associated with a higher risk for preeclampsia and poor perinatal outcomes in Kassala
hospital, eastern Sudan www.biomedcentral.com 1760500/4/311
2.Fernandez G,Diez EM The Cochrane Central Register of Controlled trials 2011 Issue
4 , , -Interrelationship between iron deficiency anemia and impaired renal function in
toxemia of pregnancy- EMBASE 1978106114
3.Th Masoomeh Goodarzi Khigani, Shadi Golie relationship of hemoglobin and
hematocrit in the first and second half of pregnancy with pregnancy outcome * IJNMR/
February 2012; Vol 17, Special Issue S
4.Emre Karashin,Seyit Temel Ceyhan-Maternal anemia and perinatal outcome . Perinatal
journal December 2007 Volume 15 Issue 3
5.Vitthal G.Kuchake, Sunny G.Kolhe-Maternal and Neonatal outcomes in preeclampsia
syndrome. International Journal of Pharmaceutical Sciences and research 2010 volume1
issue 11
6. Liu, Shiliang MD, PhD; Joseph, K. S. MD, PhD; Liston, Robert M. MD;
Bartholomew, Sharon MHSc; Walker, Mark MD, MSc; León, Juan Andrés
MD,Incidence, Risk Factors, and Associated Complications of Eclampsia
7.M. Dr.Pankaj Kumar, Dr.Prasad Pore, Dr.Usha pat maternal anemia and its impact
on perinatal outcome in a tertiary care Hospital of Pune, in Maharashtra Indian
Journal of Basic and Applied Medical Research March 2012 Volume 1 issue 2

111
8. MA Brown, CMakenzie, W Dunsmuir Can we predict recurrence of preeclampsia or
gestational hypertension, BJOG 2007 114;984-993.
9. James .N. Martin ,Brian K.Rinehart The spectrum of severe preeclampsia
Comparative analysis by HELLP syndrome classification,-American Journal of
Obstetrics Gynaecology1999, volume 180, Number 6, part 1.
10. .Ayaz A, Muhammad T, Hussain SA, Habib S Neonatal outcome in pre-eclamptic
patients.. Journal of Ayub Med Coll Abbottabad 2009 Apr-Jun volume;21 issue (2):
11. Mohammad A Salahat and Abdallah I. Ibrahim Jordan Prevalence of anemia among
Jordanian Pregnant Women and the effect of early pregnancy on Alakaline phospatase
activity Journal of Biological Sciences March 2012 volume 5 Number 1
12. Jamaiyah Haniff , Anita Das Anemia in Malaysia; cross sectional survey -. Asia
Pacific Journal of Clinical nutrition2007 volume 16 issue 3 .
13. Historical Review of anemia British Journal of Haematology,2003, 122 554–56
14. Mandy J. Bell A Historical Overview of Preeclampsia-Eclampsia J Obstet Gynecol
Neonatal Nursing 2010 September ; 39(5): 510–51.
15 L Raman, AB Pawashe, P Yasod .Hyperferritinemia in pregnancy induced
hypertension and eclampsia. Journal of postgraduate medicine1992 April-June | Volume
38 | Issue 2 PMID:0001432830
16.Clinical obstetrics and gynaecology Volume 42 Number 3 Lippincott Williams and
Wilkins.
17 J.J. Zhang*J. Grewal M. Roosen-RungeA.P. Betran Lazaga.Severe . anemia, sickle
cell disease, and thalassemia as riskfactors for preeclampsia in developing countries

112
Pregnancy Hypertension: An International Journal of Women's Cardiovascular Health
Volume 2, issues 191-192, July 2012 PII: S2210-7789(12)00059-
18 Khandait D W Ambadikar NN .Zodpey PS etal . Risk factors for anemia in
pregnancy J Obstet Gynaec of India2001 Jan –Feb 51(1) 42-44
19. F.Gary Cunningham Hematological disorders and Pregnancy Hypertension,
Williams Obstetrics 23rd edition ,
20 Dr.J.B.Sharma Anemia complicating pregnancy .Text book of Obstetrics 1st edition.
21 AUAlexander JM, Bloom SL, McIntire DD, Leveno KJ .Severe preeclampsia and the
very low birth weight infant: is induction of labor harmful? Obstet Gynecol.
1999;93(4):485. PMID10214819
22 Iron parameters .Harper biochemistry 22nd edition.
23.D. C.Dutta Medical disorders in pregnancy Text book of Obstetrics seventh edition
24 Ram HariGhimire Sita Ghimire .Maternal and Fetal outcome following severe
anemia in pregnancy, and Journal of Nobel Medical college 2012 volume 2 No1 issue 3.
25. - Anthony R Gregg Hypertension in pregnancy -Obstetrics and Gynaecology clinics
of North America 2004 volume 31.
26.K.Kalaivani Prevalence of and consequences of anemia in pregnancy Indian J Med
Res 130, November 2009,pp627-633.
27.Jane Strong and Jane M .Rutherford, Anemia and white blood cell disorders High
Risk Pregnancy Management Options Fourth edition chapter 38.

113
PROFORMA
1. Name : __________________ IPNO : __________
2. Address: ________________ Phone : __________
3. Referral : Y / N DOA : / / 2013
4. Booked : B/ UB Immunized : Y / N
5. Age : (a) < 19 (b) 20 -29 (c) 30-35 (d) 36<
6. Obstetrics code :_________
(a) Primi (b) G2P1L1 (b1) Previous LSCS (b2) previous FTND (c) Abortions
(d) G3P2L2
7 Socio economic class : (a) I (b) II (c) III (d) IV (e) V
8Educational qualification : (a) IL (b) Primary (c) Middle school (d) High school
(e) HSS (d) degree
9Weight of the mother : (a) < 50 kg (b) 50 -60 kg (c) 60 -70 kg (d) 71 <
10Expected date of delivery : / / 2013
11Past obsterrics history :
(a) PIH (b) IUGR (c) IUD (d) Preterm (e) GDM (f) Perinatal death (g) Still
birth
12Past medical history : (a)Heart disease (b) hypo thyroid (c) Seizure disorder (d)
TB (e) Fibroid (f) Br.Asthma (g) DM (h) Previous Blood Transfusion (i)
Jaundice
13. Family history: (a) present (b) absent
14. Gestational age: ________
(a) Term (b) 36-38 weeks (c) 34-36 weeks (d) 28-35 weeks (e) < 28 weeks
15. Blood pressure:
(a) 120/80 (b) diastolic BP 90 (c) diastolic 100 (d) 160/110 <.

114
Investigation:
16. Heamoglobin:
(a) 10 -11gm (b) 7-10gm (c) < 7gm
17. Peripheral smear: (a) Microcytic hypo chromic (b) Normal study
(c) macrocytic hypochromic
18. Urine albumin: (a) nil (b) trace (c) 1+ (d) 2+ (e) 3+ (f) 4+
19. 24 hrs urinary protein: (a) < 300mg (b) 300mg -1gm (c) 1-3gm (d) >3gm
20. Anti HT drugs: (a) Yes (b) No
21. MgSO4 regimen (a) Yes (b) No
22. Other pregnancy complications: (a) Prev IUD (b) breech (c) Prev LSCS (d)
PIH
(e) GDM meal plan (f) GDM on insulin (g) heart disease (h) placentaprevia (i)
fibroid
(j) Twins ( k) VBAC ( m) Rh negative
23. Onset of labour: (a) Spontaneous (b) Induction – (b1) Postdated (b2)
Preeclampsia
.(b3) Imminenteclampsia (b4) others
24. Maternal Outcome: (a) Atonic PPH (b) wound infection (c) Pulmonaryedema
(d) death
(e) HELLP syndrome (f) DIVC (g) Abruptioplacacenta (h) ARF ( i)
Eclampsia( AP/IP/PP)
25. Mode of delivery: (a) Labour natural (b) Primary LSCS (c) Breech (d) Rpt
LSCS
(e) Instrumental (f) Rpt LSCS with ST (g) Rpt LSCS with CuT (h) VBAC
26. Fetal Outcome: (a) Term (b) Preterm (c) IUGR (d) Still born

115
27. Birth weight: (a) < 1.5 kg (b) 1.6- 2kg (c) 2 -3kg (d) 3 - 4 Kg
28. Treatment: (a) Oral Iron (b) IV/IM iron inject ion (c) Blood Transfusion
29. Renal function test: (a) Normal (b) elevated
30. Platelet count : (a) >1 lakh (b) 1 lakh to 50,000 (c) < 50,000
31 Liver function test: (a) Normal (b) Elevated
32.Last child birth;(a) 1-1year 6months (b)1yr 6 months-3years (3)>3years.
33.Indication for LSCS (a)fetal distress (b)failed induction (c)severe
oligohydraminos (d) severe preeclampsia(e)previous LSCS in labour (f) previous
LSCS at term (g)cpd minor (h)twins delivery.

116

117

118


















