In Touch - CSP
49
Members wishing to use the ACPOPC logo should seek committee permission by contacting the PRO: [email protected] In Touch Spring 2011 Number: 82 © ACPOPC Committee Do not copy content without permission
Transcript of In Touch - CSP

Members wishing to use the ACPOPC logo should seek committee permission by contacting the PRO: [email protected]
In Touch
Spring 2011
Number: 82
© ACPOPC Committee
Do not copy content without permission

2
Deadline for next newsletter:
May 31st 2011
Send content to:
DISCLAIMER
Views expressed in this Newsletter are the views of the author and are not necessarily endorsed by the Editor or the Executive Committee. Whilst every care has been taken in the preparation of this Newsletter, no legal responsibility can be accepted
for inaccuracies.

3
Contents
The Committee 4
Regional Representatives 5
Reports 6
Chair’s report 6
Newsletter Editor Update 6
West Midlands regional report 7
ACPOPC SOUTHERN GROUP MEETING 7
North Midlands 7
ACPOPC Region Update 7
Conference Report - Move for health - What is our Role in Exercise and Physical Activity 8
News 10
Minutes of committee meeting held on Friday 15th October 2009, Kings College Hospital, London 10
Changes to your ACPOPC membership details 16
The National Cancer Rehabilitation Advisory Board (NCRAB) Update 19
Update: Modernisation of the CSP CIGs/SIGs 20
The Cochrane Library, February 11 20
ACPOPC EDUCATION & RESEARCH GRANT APPLICATION FORM 22
ACPOPC EDUCATION & RESEARCH GRANT POLICY 23
Bulletin Board 25
Courses 27
Annual Spring Conference 9th& 10th May 2010 27
Transforming Cancer Care 29
THE USE OF ACUPUNCTURE AS AN INTEGRATED MODALITY IN THE FIELD OF ONCOLOGY AND PALLIATIVE CARE 31
Rehabilitation and Participation in Long-Term Conditions 32
Lymphoedema Courses - Session 2011/2012 33
Allied Health Care Professionals - Study Day on Palliative Care Issues 34
Lymphoedema courses 35
The Palliative Management of Gynaecological Malignancy 36
Articles 39
RESEARCH IN ONCOLOGY AND PALLIATIVE CARE 39
Report for Musculoskeletal Oncology Physiotherapy Service (MOPS) One Year Pilot Study 2009 – 2010 for ACPOPC 41
The early rehabilitation of a patient with Acute Lymphoblastic Leukemia and Guillain-Barre Syndrome – A case study 46

4
The Committee
Chairperson
Jane Rankin
The Belvoir Park Suite, Cancer Centre Belfast City Hospital, HSC Trust
Lisburn Road Belfast BT9 7AB
Tel: 028 90699430; Fax: 02890 699459 email: [email protected]
Honorary Secretary Siobhan O'Mahony
Physio. Department Marymount Hospice, St Patrick's Hospital Wellington Road, Cork, Ireland
Tel: 00353 21 4501201 ext 269; Fax: 0035321 501619 email: [email protected]
Membership Secretary
Lucie Hughes
Macmillan Rehab Team
Princess Royal Community Health Centre Greenhead Road, Huddersfield HD1 4EW
Tel: 01484 344290
Fax: 01484 344288 email: [email protected]
Treasurer Kate Baker
Physiotherapy Department
Velindre Cancer Centre Whitchurch , Cardiff CF14 2TL
Tel: 029 20615888 ext 6340
Fax: email: [email protected]
Study Day Liaison Carolyn Moore
Physiotherapy Department Royal Marsden Hospital Downs Road, Sutton, Surrey
SM2 5PT
Tel: 020 8661 3098 Fax: 020 8661 3798 email: [email protected]
Study Day Liaison
Nicola Gingell
Physiotherapy Department Kings College Hospital, Denmark Hill London SE5 9RS
Tel: 0203 2999000 ext 4665 Fax: email: [email protected]
PRO Chiara DeBiase
Macmillan Information and Support Centre Cicely Saunders Institute King’s College Hospital, Denmark Hill London, SE5 9RS
Tel: 0203 299 5227 Fax: email: [email protected]
Newsletter Editor Valerie Young
Physio. Department
Southampton General Hospital Tremona Road Southampton SO16 6YD
Tel: 023 8077 7222 Ext 6459 Bl 1131 Fax: 02380 794756 email: [email protected]
CIG Liaison Office
Mary Gardiner
Physiotherapy Department Countess Mountbatten House,
Moorgreen Hospital Southampton SO30 3JB
Tel: 023 8047 5276 Fax: email: [email protected]
Education and Research Officer
Aileen McCartney
Wisdom Hospice, High Bank St Williams Way, Rochester Kent
ME1 2NU
Tel: 01634 830456 Fax: email: [email protected]
Diversity Officer
Joan Outram
Rehabilitation Unit Christie NHS Trust, Wilmslow Road Manchester M20 4BX
Tel: 0161 446 3795 Fax: 0161 446 8151 email: [email protected]
Regional Reps Liaison Officer Alison Allsopp
St Giles Hospice
Fisherwick Road Whittington Lichfield Staffs WS14 9LH
Tel: 01543 432517 Fax: 01543 433346 email: [email protected]
Member Without Portfolio Hannah Cummins
7 Beechcroft Road Leicester LE2 3DA
Tel: 07985196220
Fax: email: [email protected]
Member Without Portfolio
Margy Budden
Physio. Department Southampton General Hospital Tremona Road
Southampton SO16 6YD
Tel: 023 8077 7222 Ext 6459 Bl 1131 Fax: 02380 794756 email: [email protected]

5
Regional Representatives
Northern Ireland
Diane Wilson
Physiotherapy Dept Belvoir Park Suite, Cancer Centre
Belfast Health and Social Care Trust Belfast BT9 7AB
Tel: 02890699317 Fax: email: [email protected]
South Margy Budden
Physiotherapy Department Southampton General Hospital Tremona Road, Southampton
SO16 6YD
Tel: 023 8077 7222 Ext 6459 Bl 1131 Fax: 02380 794756 email: [email protected]
Scotland Susan Nuttall
c/o Physiotherapy Department Raigmore Hospital Old Perth Road, Inverness IV2 3UJ
Tel: 01463 704000 page 1184 Fax: 01463 711322 email: [email protected]
Yorks & Lincs
Gillian Smith
Physiotherapy Department Wakefield Hospice Aberford Road, Wakefield West Yorkshire, WF1 4TS
Tel: 01924 213900 Fax: 01924 362769 email: [email protected]
North
Midlands
Sally
Jennings
Physiotherapy Department LOROS Hospice
Groby Road, Leicester LE3 9QE
Tel: 0116 2318417 Fax: 0116 2320312
email: [email protected]
East Anglia (vacant) Unavailable Unavailable
North East Rosemary
Wood
Physio. Department, Willowburn Hospice, Maiden Law Hospital, Lanchester, County
Durham, DH7 0QN
Tel: 01207 529224 Fax: 01207529303
email: [email protected]
North West Jackie Barr
East Lancashire Hospice Park Lee Road Blackburn, Lancashire BB2 3NY
Tel: 01254 733447 Fax: email: [email protected]
West
Midlands Susan Horne
Shakespeare Hospice Shottery Stratford-on-Avon Warwickshire CV37 9UL
Tel: 01789 205924 Fax: 01789 415081
email: [email protected]
London Jillian Pemberton
Marie Curie Hospice Hampstead 11 Lyndhurst Gardens London NW3 5NS
Tel: 020 78533431 Fax: email: [email protected]
South East Diana Braithwaite
Hospice in the Weald Maidstone Road
Pembury Tunbridge Wells Kent TN2 4TA
Tel: 01892 820520 Fax: 01892 820520 email: [email protected]
North East Thames
Ann Bryan
Isabel Hospice Howlands Welwyn Garden City
Herts
Tel: 01707 373356 Fax: email: [email protected]
South West Ruth James
Cornwall Macmillan Service 3 St Clement Vean Tregolls Road Truro Cornwall
TR1 1RN
Tel: 01872 354384; 01579347462 Fax: 01872 354383 email: [email protected]
West (vacant) Unavailable Unavailable
South
Wales
Sharon
Thomas
Y Bwthyn Newydd Princess of Wales Hospital Coity Road
Bridgend South Wales CF31 1RQ
Tel: 01656 752003 Fax:
email: [email protected]

6
Reports
Chair’s report The New Year has brought yet more changes! Nigel Senior, who has supported us through the application process to be one of the first tranche of SIGs to transfer onto the new icsp SIG microsite, has been finalising details to action the transfer. Hannah Cummins from the committee is striving to update the old site to allow the transfer to be as smooth as possible, and has introduced quite a few new concepts including a twitter facility! The second piece of significant news is the change of the CSP CIG/SIG groups into Professional Networks (PNs), and I have written an update for the Newsletter describing the changes to date. Karen Robb, ex-committee member, is still beavering away within the CSP research committee and with the Delphi review; happily we still have some of our oncology and palliative care specific titles held. We will watch this evolving process with interest. The committee has recently evaluated undergraduate oncology and palliative care education. This formed the basis of our ARC submission; however we have been informed that the CSP has already identified the need to work with the academic institutions to ensure that programmes reflect the modern NHS need, including the increasing number of patients having and surviving cancer. The National Cancer Rehabilitation Advisory Board (NCRAB) has launched its new webpage www.ncats.nhs.uk which has all the evidence-based tumour and symptom pathways plus the new NCRAB Strategy document. The CSP has shown great support of this national initiative, and Natalie Beswetherick, Director of Practice and Development, has volunteered to be our CSP senior management team representative. NCRAB are also preparing to begin work on the new pathways for sarcoma, haematology and skin, and I would like to thank the members who have already volunteered to help with this project. Any other volunteers would be welcome! Please contact me by the 14th March. As a committee we have been using the online fora to ask for feedback and viewpoints, and I would like to thank the many members who participated in the various discussions….it is great to have such an active voice behind the committee! Jane Rankin-Watt
Newsletter Editor Update After somehow staying on the ACPOPC Committee for much longer than I can remember and having two stints as Newsletter Editor, it is finally time for me to pass this job on to someone else. My colleague Margy Budden ([email protected]) will be taking over this role from now on and will be Editor for the Summer Newsletter. I’ve thoroughly enjoyed my time as a member of the ACPOPC Executive Committee and have found it an extremely positive and dynamic group. Quite an inspiration and support in these difficult times and something I would recommend to people if they have the opportunity. Best wishes, Val Young

7
West Midlands regional report
The Midland branch of ACPOPC met on 09.12.10 at the Promrose Day Hospice, Bromsgrove. We each gave a report regarding our own specific hospice issues plus information regarding courses attended and planned for the future. One of our members, who has just completed a CPD profile for the HPC audit, gave us very valuable advice and reassurance regarding this procedure. We are all very aware that we need to raise the profile of the physiotherapy profession in oncology and palliative care with GPs and also within our specific cancer networks, so that physiotherapy interventions are included as an essential element of specific cancer rehabilitation care pathways. Our next meeting is at St Marys Hospice, Selly Oak on 16th March when the main educational topic will be Mindfulness. We also hope to have feedback from courses on Breathlessness, CBT and MND which members will have attended early in the year. Best Wishes, Sue Horne
ACPOPC SOUTHERN GROUP MEETING Thank you to those that attended the meeting at Oakhaven Hospice Trust , Lymington, on Thursday January 20th 2011. There were two presentations on work being undertaken at Oakhaven - The Acorn Project, by Jan Temenos and Oakhaven at Home by Mandie Judd. The Acorn Project described how links are being made with local schools and Oakhaven, encouraging the community through the doors of their local hospice. Oakhaven at Home was presented as a pilot project initially but is now an established part of the service providing “hands-on” specialist palliative care, in partnership with other agencies, for patients with complex needs who would prefer to be at home. A business meeting followed. Janina John Snr Physio Macmillan Professional
North Midlands
The North Midlands Group was relaunched on Sept 29tth 2010 at a successful MND study afternoon at The Leicestershire and Rutland Hospice when ideas for further meetings were sought . The first meeting proper is to take place on April 6th 2011again at LOROS.The focus of this meeting is to set up the group , agree roles ,venues and a future programme of events. Hannah Cummins from the ACPOPC committee will be feeding back from the recent ACPOPC committee meeting.
Margy Budden
ACPOPC Region Update
Please could all members note that the London and South East region has now been removed from the ACPOPC database. Members previously in this category have been assigned to either London or the South East. Unfortunately members who failed to reply to emails regarding their preferred region have now been assigned based on their postal address. Please see the details below for the regional reps for the London category and the South East category.
Regional Rep for London
Jillian Pemberton Marie Curie Hospice
Regional Rep for South East Diana Braithwaite Hospice in the Weald

8
Hampstead 11 Lyndhurst Gardens London NW3 5NS Tel: 020 78533431 Email: [email protected]
Maidstone Road Pembury Tunbridge Wells Kent TN2 4TA Tel: 01892 820520 Fax: 01892 820520 Email: [email protected]
If members are not happy with their new assigned region, please drop me an email at [email protected] and I will allocate you to your preferred choice. Many thanks Lucie Hughes Membership Secretary
Conference Report - Move for health - What is our Role in Exercise and Physical Activity
‘Move for Health’ is a campaign lead by the CSP that aims to encourage people to improve their health and wellbeing by taking regular exercise. On the 9th of September, Move for Health Champions were invited to a conference in London that examined the role of the physiotherapist in exercise and physical activity. Tristan Brice was the first speaker of the day, and explained the concept of public health and its relevance to physiotherapists. The social, economic and environmental factors that contribute to mortality and physical and mental ill health were highlighted. These factors, which include stress, social exclusion, diet and employment, have a massive role in the health of a population but are not always addressed in healthcare services or considered by physiotherapists. Current healthcare services tend to take a ‘reactive’ approach to healthcare, addressing health problems as they arise, but this is a costly and inefficient approach, that often fails to address the underlying causes of negative health behaviours. The recently published white paper ‘Equity and Excellence: Liberating the NHS’, encourages a shift in focus, redirecting money away from acute services to those that address primary prevention and also recurrence and reliance on acute services. For physiotherapists working within oncology this may mean working with those who are at high risk of developing cancer because of genetic or lifestyle factors, as well as helping survivors to self manage and reduce the risk of recurrence. Tristan provided some very useful advice on how to make our services appealing to commissioners. Physios were advised to look at their areas Joint Strategic Needs Assessment (accessible via the council’s webpage’s). This document details the communities health needs and a service that meets these is far more likely to be commissioned. Engagement with service users, to ensure that you are delivering what they need is also important, as is making partnerships with existing local services and the voluntary sector. Working with and training volunteers puts something back into the

9
community and empowers people, but it also helps reduce costs, and both of these help strengthen a business case. ACPOPC has seen some excellent examples of physiotherapists working with leisure centres and volunteers to deliver exercise interventions to cancer patients, and continuing to do this can only help strengthen our profile and raise awareness of the important role of the physiotherapist in cancer care. Tristan also recommended that we ensure that our services feature evidenced based interventions, and deliver outcomes that are important locally. He explained the importance of starting small with pilot schemes, and then developing them as appropriate. He encouraged delegates to be persistent and focus on the ‘long haul’, which involved capitalising on policy priorities and ‘fashions’, but not relying upon them, as well as aiming for funding from core budgets rather than short term project funding. Following on from this, Nick Cavill, from the National Obesity Observatory, explained the role of public health observatories - to give information on health topics, provide data, stats and contacts – all free of charge! Nick highlighted that although we know the value of exercise and physical activity to patients, the problem is often that we do not know the price of it, and thus it is difficult to prove the cost-effectiveness of our interventions. Not only is it very difficult to put a monetary value upon things such as increased longevity and quality of life, often the terms used in economic analyses can be confusing – some of the common terms used were outlined. Nick then spoke about how the public health observatories had been involved in developing an economic assessment tool for cycling. One for walking is in development and may be useful when trying to demonstrate the benefit of such interventions. Jane McClinchy gave some invaluable dietary advice that we can give to patients, especially as we are often faced with patients who have problems with nutrition and low intake. Nutrition and physical health and fitness go hand in hand, so physiotherapists are well placed to give ‘front line’ advice on eating well, observing weight changes and liaising with our dietetics colleagues. She also recommended sign posting patients to ‘NHS Choices – behind the headlines’ and the Food Standards Agency for accurate diet and health information. Jane Simmonds also presented an interesting lecture on the ‘gap’ that exists between early stage treatment in the acute sector, rehabilitation and fitness training. Jane argued that physiotherapists need to apply training variables such as intensity and duration to their exercise regimes, as well as recognising the patient’s readiness and resistance to exercise, in order to empower the patient, overcome barriers and set appropriate, progressive goals. A lot of these principles were covered within ACPOPCs study day on exercise and rehabilitation in conjunction with the University of Ulster but it was useful to have a refresher, and Jane also discussed how we can best help patients learn and maintain lifestyle changes. The day ended with examples from Move for Health Champions who had redesigned their services to meet public health needs. One example was a yoga class for people with neurological conditions. These presentations were particularly interesting as they gave practical tips on actually setting up such services – such as the assessments used, the equipment needed, and other issues such as evaluation and infection control. Overall, the day was extremely topical and useful, and most concluded that physios have a massive role in public health!

10
News
Minutes of committee meeting held on Friday 15th October 2009, Kings College Hospital, London
Present: Siobhan O’Mahony (SM), Kate Baker (KB), Nicola Gingell (NG), Carolyn Moore (CM), Mary Gardiner (MG), Chiara De Biase (CB), Margy Budden (MB), Joan Outram (JO) 1.Apologies: Val Young (VY), Lucie Hughes (LH), Alison Allsopp (AA), Jane Rankin (JR), Hannah Cummins (HC), Aileen McCartney (AM), 2. Minutes: The minutes from the ACPOPC meeting held on the 27th July 2010 at the Royal Marsden, London, were agreed and signed off. 3. Matters Arising a. Constitution MG informed the committee that the CIGLC has ceased to operate (the final meeting took place in September). This is part of the CSP’s reconfiguration of the CIOGs (the Working Together project), which followed a growth in CSP membership and in the number of CIOGs. CIOGs will henceforth be known as professional networks (PN), and each PN will sit in one of six alliances (musculoskeletal, neurology, cardiorespiratory and cardiovascular, client groups, wellbeing and occupational roles and settings). MG is to seek clarification from the CSP as to whether ACPOPC can decide which alliance it will affiliate itself to, or if this will be determined by the CSP. The target date for the completion of this process is December 2011. MG explained that the CSP will stipulate the framework of the constitution of all CIOGs as part of the reconfiguration process and it was agreed that further development of the ACPOPC constitution should cease, pending further direction from the CSP. Following a healthy debate, it was broadly agreed that we need to work with the process and that MG would draft a letter, highlighting our concerns and will contact Simone Morris, to obtain the minutes of the CIGLC committee meeting of 24th September 2010.
MG
b. Education Fund As AM was absent, this topic was deferred until the next committee meeting. However KC (treasurer) was able to inform the committee, that £1970.00 had been awarded from the education fund, to date this year.
AM
c. Working Together Project Update This item was discussed in conjunction with the constitution (item a) d. Regional Reps Project Update AA was absent, but advised the committee that she will be attending the End of Life conference on 19th October as planned and will feedback to the committee at the next meeting. She is still following up
AA

11
some jobs from the last meeting (re: the regional reps)
e. Prescribing Champions Project MG and JO reported that there were no further developments or communications from the CSP, with regard to this project. ACPOPC had proposed several items, such as lymphoedema garments / bandaging, home oxygen, but it would appear that this consultation has a focus on the prescription of medications only. Therefore the committee decision is that ACPOPC has no further interest in this project.
All
f. CSP Website Project It was noted that this item was tabled for discussion on the agenda of the CIGLC meeting on 24th Sept 2010, which MG was unable to attend. MG outlined that all new members would be able to access the website in beta version, which will be run as a test. This will become the master version early in 2011. It was stated that groups which had originally expressed an interest, would be among the first groups to trial the new website and MG is to enquire if ACPOPC is one of those groups.
AGENDA ITEMS 4. ARC Conference 2011 KB volunteered to present the ACPOPC motion at the ARC conference in 2011. It was suggested that she might speak to Karen Robb and Trevelyan Beyer, who had both presented motions on behalf of ACPOPC previously, to familiarise herself with the process. A discussion took place regarding some of the key points to be included in the speech, which comprised
• Teaching to pre-registration physiotherapy students should reflect changes in government policy and patient populations
• Incorporate the results of AM’s survey (of institutions providing pre-registration physiotherapy training), outlining the variation in oncology and palliative care content provided, (including non malignant conditions)
• Highlight the discrepancy in the allocation of resources re: long term conditions
• MacMillan has also identified this education gap and have strategic plans to work in collaboration to address the issue. They are happy to lend their name to support this issue
• Incorporate the survivorship initiative
• The goal is to achieve a national standard for physiotherapy pre-registration education
CM will ask AM to summarize and circulate the results of her survey, MG will ask AM to contact Mike Maynard, who is the ARC rep to CIGLC re: support for the motion. MG to enquire, if there are unsubscribed places at the ARC conference, can another ACPOPC member attend? A training day for presenters at the ARC conference is to take place in London on 27th January 2011
KB,AM, MG,CM

12
5. Autumn Study Day –Congress 15/16 October 2010 The committee agreed that ACPOPC’s future attendance at Congress, as a study event, was not appropriate. It was reiterated that in order for ACPOPC members to secure study leave/funding, the content must be expressly relevant to their area of work. Despite actively engaging with the process, we failed to secure a programme that is sufficient to meet the needs of our members. Also, very little notice was given regarding the acceptance of ACPOPC speakers to present at Congress, which did not allow sufficient time to promote/advertise Congress to our members. CM will write to Helen Tyler and the team presenting from the Christie Hospital, Manchester, to thank them for partaking in Congress on ACPOPCs behalf. Following the decision that the ACPOPC committee would not attend congress, the hotel rooms were cancelled, but CM informed the committee that the hotel had billed ACPOPC for £50 for the meeting room. It was decided to contest this and CM/NG will follow this up with a phone call.
CM/NG
6. Sourcing of Compliment Slips KB informed the committee that this is work in progress and she will let the committee know the outcome in due course
KB
7. Acute Oncology Measures JO informed the committee that the National Cancer Peer Review Programme Acute Oncology Measures (including metastatic spinal cord compression) were out for consultation and highlighted her concern regarding the lack of rehabilitation measures included. It was agreed that ACPOPC should coordinate a response. KB will circulate the measures to the committee and will collate comments, which should be submitted by Friday 22nd October 2010. (The consultation closes on 10th November 2010). JO is to enquire if there are other measures out for consultation, that ACPOPC should be aware of.
AM,JO,KB
8.New Peer Review Measures This was discussed under item 7 (as the title was The National Cancer Peer Review Programme – Acute Oncology, including metastatic spinal cord compression measures).
9. Spring Study Day 9th/10th May 2011 The committee were informed that Baroness Finley has agreed to open the conference, which is tabled to start at 10.30am, to allow delegates time to travel on the day. The provisional programme incorporates – Day 1
• Advances in symptom control (pain) – KB to source a registrar to deliver this
• Progressive non-malignant brain conditions
• MSCC – Helen Tyler
• MS update – KB to source (?) Day 2
• AGM at 09.30
• KB – B inspired
KB, CM, NG, VY,

13
• Patient’s perspective
• Oncology (? Communication)
• Problem solving in renal palliative care
• Physiotherapy challenges with HIV and AIDS patients It was proposed that the cost of attendance should be £230 all-in (including all meals, accommodation) or £80 per day. CM/NG to ask VY to put this in the next newsletter. Committee members were asked to see if we can come up with a ‘snappy’ title for the conference.
10. Research Forum for AHPs CB to email a list of topics (?) CB 11. Move for Health Champions HC was not in attendance, but feedback to the committee that she had attended the Move for Health conference, which was excellent. The emphasis was on writing business cases and getting services commissioned and she is going to consider how best to use this information to the benefit of ACPOPC members.
HC
12. NCRAB This item was deferred until the next committee meeting, as JR was absent and no further information was available to attendees.
JR
13. Associate membership A discussion took place about associate membership of ACPOPC, following an expression of interest from an American chiropractor. LH has indicated that all associate memberships except one are from academic institutions, charities or libraries, so this is not an issue that occurs frequently. It was generally felt by those present, that membership should be restricted to physiotherapists, but in view of impending changes in the ‘working together project’ the CSP would probably be more directive in this regard, so the decision is that for the moment, there is no need to change the wording on the membership area of the ACPOPC website, or on the application form.
ALL
14. AOB 1. KB – Subscriptions. The committee were informed that the monies held in ACPOPC accounts were diminishing and we need to be aware of this. It was acknowledged that while certain projects undertaken by ACPOPC (refund for Rehabilitation in Cancer Care book, sponsorship of attendees at the ‘Exercise and Lifestyle in Rehabilitation and Cancer Survivorship’ course, training day for Regional Reps etc) were partly responsible, we must continue to be mindful of the overall financial situation. KB suggested that we might increase the subscription, as it has not been increased in recent years. While people generally agreed, SM reminded the committee that an increase in subscriptions must be voted on at the AGM and SM will put this on the Agenda for the AGM 2011, A broader discussion took place on other cost-cutting measures and the committee members present agreed to waive the subsistence paid to committee members attending the committee meeting, for this meeting only, pending consultation with other committee members
ALL
14
who were absent. This item will be placed on the agenda for the January meeting. It was also suggested that committee members might waive their fee for presenting at conference and it was decided that a fuller discussion should take place on this matter, in the presence of the wider committee. 2. Feedback from LH LH proposed changes to the ACPOPC membership form
1. Including a line about being registered with the Health Professions Council (HPC) and asking applicants/members for their number
2. Writing ‘please write your name and ACPOPC number, if known, on the back of your cheque’ under payment section
3. Asking overseas members to include a photocopy of their professional qualification certificate
4. Add Haematology as a work area – this would need to be added to the database
Items 2 and 4 were agreed and it was felt that a decision on items 1 and 3 should be deferred, pending possible directives from the CSP under the restructuring of CIOGs (the Working Together Project) LH hopes to have her interviews for the Self-Referral Research completed by the end of October. Regional issues – LH expressed her concerns about linking membership with cancer networks, as she felt this could be interpreted as ACPOPC having an oncology focus and suggested that as an alternative, perhaps we could place a link on the website, showing the cancer networks and a list of leads. 3. CB CB outlined Karen Robb (KR)’s response to the CSP’s research priorities project which were
• Safety and efficacy of exercise in rarer cancers ie: not breast, colorectal, prostate
• Long term effects of exercise in common cancers
• TENS for cancer pain
• Risk factors for chronic pain and dysfunction in breast cancer
• Innovative online screening and management of low level rehab needs (in light of the financial climate)
KR stated that other issues had been raised by ACPOPC, (neuro and resp) but these were not relevant to her stream. The Macmillan ‘Consequences of Cancer’ treatment group met this week and the focus of the day was Rehab in Cancer Care. KR has a few action points including
• Speaking to the Macmillan communications team about the profile of rehab HCPs and she will keep the committee updated on this issue.
KR also sent out a request for 2 expert physios (one cancer and one not cancer) in the field of gynae and women’s health, to sit on a steering group. Meetings will be in London. Some names were
LH

15
proposed and it was also suggested that it may be worthwhile to contacting the Women’s Health CIOG. 4. MB MB informed the committee that they have now sourced an external printer for the newsletter and that ‘team Southampton’ are presently stuffing the envelopes themselves and will assess how this is working out. 5. MG MG reported that some time ago, ACPOPC had been asked to contribute to a list of outcome measures which could be incorporated into electronic communications. This was called ‘’the NHS clinical content programme – connecting for health”. MG has received a definitive list of adopted measures (of which only a few were proposed by ACPOPC) and she will circulate them to the committee members. 6. SM SM outlined a request from CPOPC (the Irish CIOG for oncology and palliative care) to use the text from the ACPOPC leaflet and change the layout/background so that the content (which they felt couldn’t be improved on) could be used to create a leaflet for the Irish group. This would expressly acknowledge that the information was reprinted with the kind permission of ACPOPC. A discussion took place and it was considered that
• The material was not copyright, so anyone could copy it from the internet as it stands and use this information
• Why try to reinvent the wheel? SM stated that she would like to seek approval of the decision with the chairperson (JR) who was not in attendance. 8. Dates of Future Meetings:
• JO has booked a room at the Christie Hospital, Manchester for committee meeting on 27th January 2011, but this now clashes with a training day for the ARC conference. JO will check to see if there is any flexibility with the dates and report back to the committee.
• May 8th (Sun) – prior to ACPOPC conference in Cardiff.
• CM will check room availability at the RMH for the July committee meeting and report back to he committee
MG
If members would like more information regarding any item in these minutes, please contact your Regional Representative who will be able to help.

16
Changes to your ACPOPC membership details
Dear Members, We are pleased to inform you that ACPOPC can now record your primary and secondary work areas. Previously, on both the application form and the renewal form, members were only able to detail one work area. From now on a secondary work area can also be recorded. Please also note that haematology has now been added as a new work area. The ACPOPC work areas are now:
� oncology � palliative care
� management in oncology � management in palliative care
� haematology � lymphoedema
� academic � generalist
� other
We are also asking members where appropriate to please indicate one tumour site specialism.
� breast � head and neck � upper GI
� colorectal � gynaecology � urology
� lung � brain CNS � sarcoma
� haematology � skin
As ACPOPC are keen to keep postal costs to a minimum we will not be gathering this information until the next renewals go out. If however members would like to email me their secondary work area and a tumour site specialism where appropriate I would be happy to update their details. Many thanks Lucie Hughes Membership Secretary
The new full application form is shown on the next page.

17
MEMBERSHIP APPLICATION / RENEWAL 2011
� New Member � Existing Member State ACPOPC Membership No � �
I wish to apply for membership for the year 1 January 2011 - 31 December 2011
(Please refer to terms and conditions found at www.acpopc.org.uk for the following membership categories)
A Full Membership £20.00
I am currently a subscribing member of the Chartered Society of Physiotherapy (CSP) and I am registered with the
Health Professional Council (HPC). I enclose a cheque for £20.00.
Signature CSP No.
HPC No.
B Associate Membership £20.00
I am not a member of the CSP but am resident in the UK. If a member of the Health Professional Council (HPC)
please detail your number. I enclose a cheque for £20.00.
Signature HPC No.
C Assistant /Student Membership £10.00
I am an Assistant/student currently studying in the UK. I enclose a cheque for £10.00.
Signature
D Oversees Membership £25.00
I enclose a cheque for £25.00 and a photocopy of my professional qualification certificate. (Please note overseas
cheques should be in Pounds Sterling)
Signature
E Department Membership No charge (but donation welcome)
I am registering on behalf of a University, library or college.
Signature
PERSONAL DETAILS PLEASE COMPLETE IN BLOCK CAPITALS
First Name
Last Name
Grade
Postal Address
Home Address
Post Code
Post Code
Telephone
Telephone
EMAIL (please only give one address)
���� I am unwilling for my postal address details to be released for professional and directory purposes
18
What is your primary area of work in relation to cancer and palliative care?
���� oncology
���� palliative care
���� management in oncology
���� management in palliative care
���� haematology
���� lymphoedema
���� academic
���� generalist
���� other
What is your secondary area of work in relation to cancer and palliative care?
���� oncology
���� palliative care
���� management in oncology
���� management in palliative care
���� haematology
���� lymphoedema
���� academic
���� generalist
���� other
Where appropriate, please indicate a tumour site specialism.
���� breast
���� head and neck ���� upper GI
���� colorectal
���� gynaecology
���� urology
���� lung
���� brain CNS ���� sarcoma
���� haematology
���� skin
Please return this form with remittance to:
Lucie Hughes
ACPOPC Membership Secretary
Macmillan Rehab Team
Princess Royal Community Health
Centre
Greenhead Road
Huddersfield
HD1 4EW
Please enclose a stamped self-addressed envelope if receipt is required
Cheques should be made payable to:
The Association of Chartered Physiotherapists in Oncology and Palliative Care
Please remember to ensure you have written your name and ACPOPC number, if known,
on the back of your cheque
Thank you

19
The National Cancer Rehabilitation Advisory Board (NCRAB) Update
The National Cancer Rehabilitation Advisory Board (NCRAB) met with Cancer Network AHP Leads and the Professional Body CIG/PN Chairs (COT, RCSLT, BDA and CSP) in early February to agree the national work plan and education framework. This was a dynamic and positive AHP meeting with outcomes including:
• Agreement to move from the NICE (2004) supportive and palliative care guidance for adults with cancer's 4 tier model for the cancer rehab workforce to the DH Modernising AHP Careers Framework model
• Discussion re education requirements (pre and post registration) and associated competencies
• Agreement of two-way communications pathway from NCRAB to CIGs/PNs and professional bodies
• Agreement of the new electronic format for the evidence based AHP cancer (and symptom) pathways launched by the Cancer Action Team in Jan 10, and to produce an additional 3 pathways for haematology, skin and sarcoma
• Key issues for physiotherapy: As the number of people diagnosed with cancer increases (currently 1:3), this condition is going to be referred more and more frequently to the physiotherapy workforce, in both the specialist and generalist setting. Cancer patients who are palliative now live with their disease for many years and this will also impact greatly on the profession through recurrent acute admissions and long term domiciliary/hospice management. The aspect of survivorship is also an exciting field for physiotherapy with the recognition that safe exercise can actually reduce the risk of some cancers recurring. As a result this has a very high profile at the moment both with the DH and cancer charities. As a profession, we need to ensure that our current and future workforce is competent at dealing with the survivorship and palliative care aspects of cancer management. ACPOPC submitted an 2010/11 ARC proposal suggesting that the CSP must ensure that undergrad curricula reflect the changes in the modern patient population, and we were impressed to be informed that this would be covered by the new CSP professional practice policy. Naturally, we would like to monitor and ensure that this contains influencing for cancer and palliative care. Many of the issues discussed and agreed at the national meeting will have an impact on the physiotherapy workforce from an education/competency aspect alone. In recognition of this, Natalie Beswetherick, Director of CSP Practice and Development has agreed to be the formal CSP link with NCRAB, alongside myself as ACPOPC chair. Links have also been agreed with the COT, BDA and RCSLT. Jane Rankin-Watt Chair ACPOPC

20
Update: Modernisation of the CSP CIGs/SIGs
In January, I circulated a letter via icsp, the ACPOPC online forum and the regional reps, describing the new format of the CSP CIGS or, as we are now known, Professional Networks (PNs). The CSP has been working through a process of modernisation over the past 2 years with regard to this new structure. ACPOPC have been very active in this process including online fora and In Touch Newsletter briefings, and have welcomed all membership input. In my letter I had requested members’ thoughts regarding changing our title to “modernise” our corporate image (as recommended by the CSP), however the over whelming feedback was to keep our name as it is. The committee are very happy about this as we also think it is both professional and reflects our expertise. There has been some debate regarding the new survivorship role and, whilst we had considered squeezing an “S” into the mnemonic, we decided that we would review this next year when the immediate changes have been embedded. Secondly, I had asked for feedback regarding the new structure which consists of the 6 Alliance groups. The PNs will sit independently within one of the Alliance groups. The 6 groups are:
• Neurosciences
• Neuromuscular
• Respiratory
• Wellbeing and therapies
• Client groups
• Occupational roles and settings From the feedback discussion, it was felt that we sit best in the client group option along with Women’s Health/Continence, Paediatrics, Learning Disability and a couple more cross cutting core groups potentially including AGILE. It is also agreed that we should have formal communication links with the neurosciences, neuromuscular, respiratory and wellbeing/ therapies groups as many of our roles and work would also, at times, link in with each of their work. Adrian Coleman, the CSP project officer for this modernisation work, has agreed to attend the ACPOPC committee meeting in July to report on the project at the half way point. I will also provide an update for each Newsletter. Jane Rankin-Watt, ACPOPC Chair
The Cochrane Library, February 11
Interventions to enhance return-to-work for cancer patients
Background Cancer survivors are 1.4 times more likely to be unemployed than healthy people. It is therefore important to provide cancer patients with programmes to support the return-to-work process. Objectives To evaluate the effectiveness of interventions aimed at enhancing return-to-work in cancer patients. Search strategy We searched the Cochrane Central Register of Controlled Trials (CENTRAL, in The Cochrane Library Issue 2, 2010), MEDLINE, EMBASE, CINAHL, OSH-ROM, PsycINFO, DARE, ClinicalTrials.gov, Trialregister.nl and Controlled-trials.com to February 2010, reference lists of included articles and selected reviews, and contacted authors of relevant articles. Selection criteria
21
Randomised controlled trials (RCTs) and controlled before-after studies (CBAs) of the effectiveness of psychological, vocational, physical, medical or multidisciplinary interventions enhancing return-to-work in cancer patients. The primary outcome was return-to-work measured as either return-to-work rate or sick leave duration. Secondary outcome was quality of life. Data collection and analysis Two authors independently selected trials, assessed the risk of bias and extracted data. We pooled studies with sufficient data, judged to be clinically homogeneous in different comparisons. We assessed the overall quality of the evidence for each comparison using the GRADE approach. Main results Fourteen articles reporting 14 RCTs and 4 CBAs were included. These studies involved a total of 1652 participants. Results indicated low quality evidence of similar return-to-work rates for psychological interventions compared to care as usual (odds ratio (OR) = 2.32, 95% confidence interval (CI) 0.94 to 5.71). No vocational interventions were retrieved. Very low evidence suggested that physical training was not more effective than care as usual on improving return-to-work (OR = 1.20, 95% CI 0.32 to 4.54). Eight RCTs on medical interventions showed low quality evidence that functioning conserving approaches had similar return-to-work rates as more radical treatments (OR = 1.53, 95% CI 0.95 to 2.45). Moderate quality evidence showed multidisciplinary interventions involving physical, psychological and vocational components led to higher return-to-work rates than care as usual (OR = 1.87, 95% CI 1.07 to 3.27). No differences in the effect of psychological, physical, medical or multidisciplinary interventions compared to care as usual were found on quality of life outcomes. Authors' conclusions Moderate quality evidence showed that employed patients with cancer experience return-to-work benefits from multidisciplinary interventions compared to care as usual. More high quality RCTs aimed at enhancing return-to-work in cancer patients are needed.
Interventions to enhance return-to-work for cancer patients Each year cancer survival rates are going up and the number of cancer survivors is rising sharply. Many survivors are doing well, although cancer survivors can continue to experience long-lasting problems such as fatigue, pain, and depression which may become chronic. These long-term effects can clearly cause problems with work participation of cancer survivors. Therefore, cancer is a significant cause of absence from work, unemployment and early retirement. Individuals, their families and society at large all carry part of the burden. This review evaluated the effects of interventions aimed at enhancing return-to-work in cancer patients. It included 18 studies involving 1652 participants. Four types of interventions were found: psychological interventions, interventions aimed at physical functioning, medical interventions, and multidisciplinary interventions which incorporated physical, psychological and vocational components. No vocational interventions aimed at work-related issues were retrieved. Results suggest that multidisciplinary interventions involving physical, psychological and vocational components led to higher return-to-work rates of cancer patients than care as usual, while quality of life was similar.
• Publication Date: 16 Feb 2011
• Publication Type: Systematic Review
• Publisher: John Wiley & Sons, Ltd
• Source: Cochrane
• Creator: de Boer Angela GEM,Taskila Taina,Tamminga Sietske J,Frings-Dresen Monique HW,Feuerstein Michael,Verbeek Jos H

22
ACPOPC EDUCATION & RESEARCH GRANT APPLICATION FORM
Please complete all sections or your form will be returned which could delay the application
process
NAME_______________________________________________________________
ADDRESS______________________________________________________________________
________________________________________________________________________________
_______________________________________________
TEL NO _______________________________________
EMAIL____________________________________________________
ACPOPC MEMBERSHIP NUMBER__________________
Please confirm how long you have been a member of ACPOPC_______________
Purpose of application:
Research
Course
Conference
Other (please state) _________________________
Total Funding Requested_______________________________________________
Have you applied for funding elsewhere? Please provide details and how much has been
granted
________________________________________________________________________________
________________________________________________________________________________
_______________________________________________
Please provide a supporting statement of your application including course details/research
project details, aims and objectives, dates (if applicable) and why ACPOPC should support
your study. Please make sure to include how this will impact on your practice, how patients
will benefit and how you plan to disseminate your learning. Feel free to attach supporting documentation with your application.
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________

23
________________________________________________________________________________
________________________________________________________________________________
____________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
___
Please send your completed application form and supporting documentation (if applicable) to
Aileen McCartney, ACPOPC Education and Research Officer, Wisdom Hospice, High Bank,
Rochester, Kent ME1 2NU or email to [email protected]
*From 1
st March 2011 until 1
st November 2011 I will be on maternity leave and therefore all
applications to the ACPOPC Education Grant should be made to Chiara De Biase either by email to
[email protected] or by post to Chiara De Biase, Macmillan Information and Support Centre,
Cicely Saunders Institute, Kings College Hospital, Denmark Hill, London SE5 9RS*
ACPOPC EDUCATION & RESEARCH GRANT POLICY 1. A total of £2000 will be available per annum from ACPOPC income as an education grant for the
period January-January.
2. Applicants will have been a member of ACPOPC for at least 12 months.
3. ACPOPC members are invited to apply for financial assistance towards
research/conferences/courses and postgraduate course fees that are shown to be linked to
physiotherapy in oncology and/or palliative care. Applications will be accepted for consideration
up to 3 weeks prior to the start of the course/conference to facilitate committee funding agreement.
4. ACPOPC membership number must be quoted when applying
5. Applications for the award should be in writing to the education and research officer on the
education fund application form, which is available on the ACPOPC website or from the education
and research officer.
6. The application form requires detailed information on the course and it is the applicant’s
responsibility to ensure all relevant information is provided. This includes details on any other
funding applied for and if these have been successful or not.
7. The education and research officer will consider each application and will consult the chairperson
to decide which applications will receive a grant and the value of that grant
8. A maximum of £350 can be awarded at any one time and only one award will be made to an
individual each year.

24
9. A maximum of £1000 can be awarded to any one individual over a 5 year period.
10. As a minimum, applicants will be required to feedback on their learning, by writing a report for
the ACPOPC newsletter, but may be required to present at an APCOPC study day.
11. The treasurer will issue a cheque to each successful applicant. The successful applicant must
provide details of whom the cheque should be issued to within 2 months or the grant will be
reallocated.
12. Applicants will be informed in writing regarding the success of their application within 4 weeks.
13. In the event that the full fund is not utilised in any year, the remainder will be returned to the
main ACPOPC account but earmarked for education purposes. In the event that there are
insufficient funds, applications may be declined.
14. This policy will be reviewed each year at the ACPOPC Executive Committee summer meeting.

25
Bulletin Board
ATTENTION!! APPLICATIONS TO ACPOPC EDUCATION GRANT
From 1st March 2011 until 1st November 2011 I will be on maternity leave and therefore all applications to the ACPOPC Education Grant should be made to Chiara De Biase either by email to [email protected] or by post to Chiara De Biase, Macmillan Information and Support Centre,
Cicely Saunders Institute, Kings College Hospital, Denmark Hill, London SE5 9RS Any other matters relating to ACPOPC research and education should also be addressed to Chiara
in the first instance and will be dealt with by the ACPOPC committee. Thank you!
Aileen McCartney (Education and Research Officer)
The NCRI Survivorship After Cancer and End of Life Care Research Grantsmanship Gateway is an outcome of the NCRI Rapid Review of research in survivorship after cancer and end of life
care, and aims to assist early career researchers in the survivorship after cancer and end of life care fields by signposting towards expert advice on grant application development.
http://www.ncri.org.uk/grantsmanship/
Stop press stop press……………………………
ACPOPC Autumn Study Day 2011
November 2011(date to be confirmed)
CSP 14 Bedford Row London WC1R 4ED
Acupressure for Physiotherapists in Oncology and Palliative Care
Jeanne Burnett Physiotherapy research in exercise and cancer
Matthew Maddocks
Plus a fantastic opportunity to network with colleagues working with oncology and palliative care patients
in a wide variety of settings! For further information please contact : Nicola Gingell [email protected]
Haematology Physiotherapist, Kings College Hospital, Denmark Hill, London, S.E.5 9RS

26
Self-referral Research Update I’d like to say a big thank you to all of you who completed and returned your questionnaires and also to the participants who took part in the telephone interviews. Just to let you all know that I’m excited about the findings and will be writing a summary for the next newsletter. In the meantime if you have any questions about the research, please feel free to email me at [email protected] Thanks , Lucie Hughes
The Department of Health are now welcoming comments on their draft Sarcoma measures. The consultation document can be found on http://www.dh.gov.uk/en/Consultations/Liveconsultations/DH_124539 If you would like to have your thoughts and comments heard then please forward any responses to the ACPOPC PRO Chiara De Biase on [email protected] The consultation ends on the 16th May so please have your comments to Chiara by Monday 9th May, 2011 so they can be submitted in one document.

27
Courses
Annual Spring Conference 9th& 10th May 2010
A 2 day conference
Palliative Care Update Topics to include …
Churchills Hotel
No3 Llandaff Place,
Cardiff Road
Llandaff, Cardiff, CF5 2AE
Please send cheques and completed application forms to;
Nicola Gingell, Physiotherapy department, Kings College Hospital Denmark Hill, London,
Telephone: e-mail: [email protected]
ACPOPC Spring Conference Application Form (please tick required rate)
Rates Member Tick Non member Tick Student Tick
All inclusive package –
2 day delegate rate,
overnight accommodation &
all meals (including
conference dinner)
£230 £275 £200
1 Day delegate rate £80 £95 £70 2 Day delegate rate £150 £180 £130 Accommodation for 8th May £55 £55 £55 Dinner £20 £20 £20
NAME:(please print) Mr/Mrs/Miss/Ms _______________________________________
ACPOPC membership number;
POST HELD / PLACE OF WORK ____________________________________________
_____________________________________________________________________
ADDRESS FOR CORRESPONDENCE:________________________________________
_____________________________________________________________________
_____________________________________________________________________
e-mail________________________________________________________________
CONTACT TELEPHONE No. _______________________________________________
Do you have any special requirements, dietary or otherwise? (Please give details)
________________________________________
Do you need ground floor accommodation in view of your special needs? Yes / No
I enclose fee of £…………… (Cheques payable to: “ACPOPC”)
28
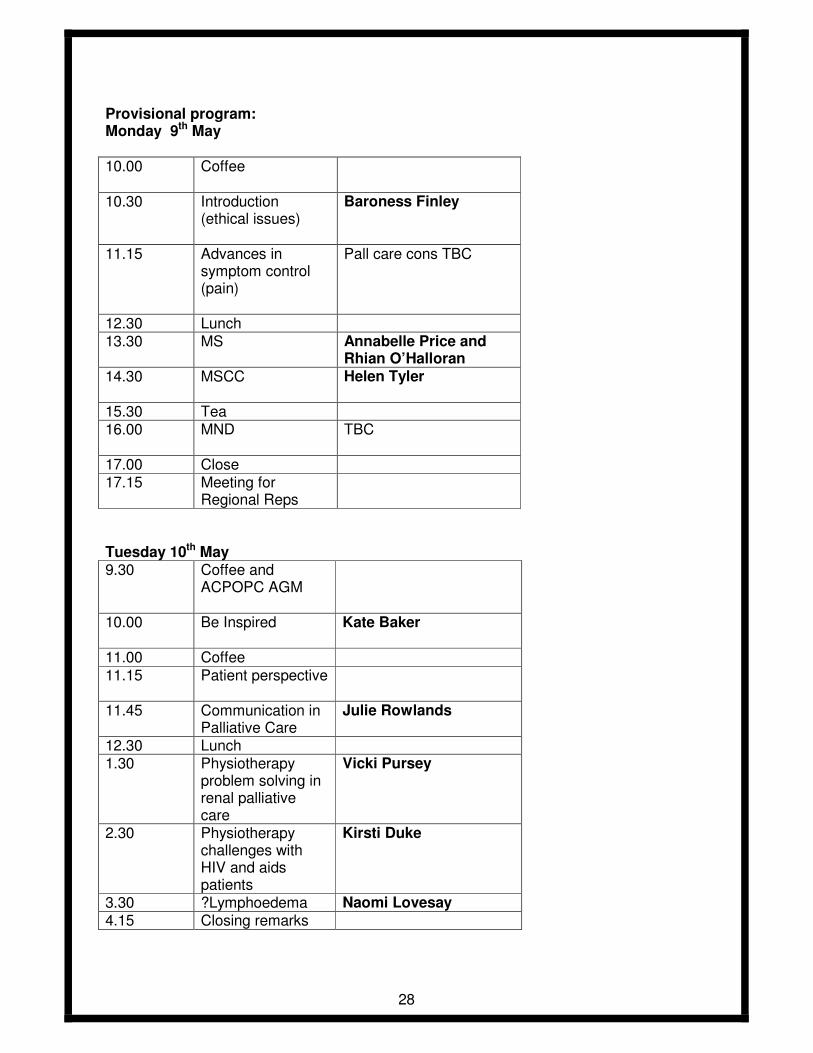
Provisional program: Monday 9th May 10.00 Coffee
10.30 Introduction (ethical issues)
Baroness Finley
11.15 Advances in symptom control (pain)
Pall care cons TBC
12.30 Lunch 13.30 MS Annabelle Price and
Rhian O’Halloran 14.30 MSCC
Helen Tyler
15.30 Tea 16.00 MND
TBC
17.00 Close 17.15 Meeting for
Regional Reps
Tuesday 10th May 9.30 Coffee and
ACPOPC AGM
10.00 Be Inspired
Kate Baker
11.00 Coffee
11.15 Patient perspective
11.45 Communication in Palliative Care
Julie Rowlands
12.30 Lunch 1.30 Physiotherapy
problem solving in renal palliative care
Vicki Pursey
2.30 Physiotherapy challenges with HIV and aids patients
Kirsti Duke
3.30 ?Lymphoedema Naomi Lovesay 4.15 Closing remarks
29
Transforming Cancer Care

30

31
THE USE OF ACUPUNCTURE AS AN INTEGRATED MODALITY IN THE FIELD OF ONCOLOGY AND PALLIATIVE CARE
12 Hours CPD
16th & 17th July 2011
Venue: Parks Therapy Centre
86 Cambridge Street St Neots Cambs
PE19 1PJ
Course Tutor: Jennie Longbottom MSc MMEd BSc FCSP MBAcC Henry McGrath Lic Ac, MBAcC, MCHM
Course Fee From: £180
Including Manuals, Lunch & Refreshments
The primary aim of this course is to integrate the systemic approach to cancer care
through the use of TCM theory with Henry McGrath, whilst mapping this theory against the neurophysiological evidence from western acupuncture research with
Jennie Longbottom. As such this course will be the first of its kind to offer delegates an integrated approach for the effective use of acupuncture in oncology
and palliative care (OPC). The course will support delegates working in this complex area of care who have clinical training in acupuncture for pain relief.
For further course details please contact ALIED LTD. on 01480 394739 or email [email protected]

32
Rehabilitation and Participation in Long-Term Conditions

33
Lymphoedema Courses - Session 2011/2012
A comprehensive and flexible programme of courses are available, to cater for health care
professionals at various levels, from those with a role in risk reduction to those involved in specialist and complex treatment.
Exit award qualifications
. CPD Certificate with or without academic credit
. Graduate Certificate/Diploma (Level 4)
. Postgraduate Certificate (Level M)
. Option to continue to PG Diploma or Masters
. Keyworker Qualification
. Casley-Smith MLD Practitioner Qualification
. Casley-Smith Specialist Updates Course Dates offered
Lymphoedema: Diagnosis, Assessment & Risk Reduction, 20 credits
Glasgow: 27th - 30th Sept 2011 Newcastle: 17th -20th Jan 2012
Lymphoedema: Assessment & Management, 20 credits
Glasgow: 7th - 9th Dec 2011 Newcastle: 4th-6th April 2012
Managing Complicated Lymphoedema (Casley-Smith DLT), 40 credits
Pt 1: 24th-27th Jan 2012 Pt 2: 6th-9th March 2012 Pt 3: 6th-8th June 2012
Managing Oedema due to Advanced Disease, 20 credits
20th - 23rd September 2012
Lymphoedema: Specialist Service Development, 20 credits
14th - 17th Feb 2012
Lymphoedema: Casley-Smith Update Course
24th to 26th May 2011 May/June 2012
Costs: All 20 credit courses = £500 per course. 40 credit course = £1000 per
course For further information please contact Emma Fisher or Margaret Sneddon Tel: 0141 330 2072/2071 Email: [email protected]
www.gla.ac.uk/departments/nursing/
Rated FIRST in the UK for Nurse Education in the National Student Survey (NSS) 2010.
The 2010 NSS results show that 100% of our BN undergraduate students are satisfied with their experience.
RAE 2008: 60% of our Nursing & Health Care research is world leading or internationally excellent and a further 30% is of international quality. The University of Glasgow, charity number SC004401

34
Allied Health Care Professionals - Study Day on Palliative Care Issues
NEW FOR 2011! This study day has been designed specifically for Allied Health Care Professionals interested in enhancing their knowledge and skills related to palliative care. The focus of the day will be on two conditions, Sarcoma and Progressive Supranuclear Palsy (PSP) that require supportive palliative care provided by the multidisciplinary team (including goal setting). Key Learning outcomes of this study day are:
• Enhanced knowledge and understanding of Sarcoma, treatment options and psychosocial issues
• Enhanced knowledge and understanding of Progressive Supranuclear Palsy (PSP)
• Enhanced knowledge of role of Speech and Language Therapist in PSP
• Enhanced understanding of goal setting in palliative care Dates: 13th May 2011 Time: 9.30am – 4.30pm Venue: Strathcarron Hospice Cost: £70.00 Facilitators: Lena Richards, Senior Physiotherapist, Christies Joyce Firth, LHCC Speech and Language Therapist, NHS Forth Valley Cathy Kelly/Sheila Brown, Clinical Nurse Specialist, Strathcarron Hospice Sally Boa, Research Nurse, Strathcarron Hospice Ideal for: All qualified Allied Health Care Professionals.
For further details please contact: Catherine Haggerty
Education Department Administrator Strathcarron Hospice
Email: [email protected] Tel: 01324 826222 Fax: 01324 824576 Registered Charity No SC006704
35
Lymphoedema courses
The following Lymphoedema courses are available in the ABMUHB based in Swansea
KEY WORKER COURSES
Tuesday 29th March 2011 Chronic Oedema/Measuring Wednesday 30th March 2011 MLLB-lower limb Tuesday 12th April 2011 MLLB-upper limb Wednesday 13th April 2011 SLD/Case Studies/Measuring Casley-Smith Lymphoedema Management Course £850 This is the full lymphoedema management course Part 1: Upper Limb and Trunk Tuesday May 24th –Thursday May 26th 2011 Part 2: Lower Limb and Trunk Tuesday 5th July 2011 – Thursday 7th July 2011 Part 3 Assessment, Head and Neck swelling /Genital Oedema Tuesday 6thSeptember & Wednesday 7th September 2011
Casley Smith UPDATE £275
10th, 11th, 12th May 2011
1st, 2nd 3rd November 2011 Contact Beverley Morgan on 01792 285252 for more details and application forms.
10 % discount for ACPOPC members

36
Presents
The Palliative Management of Gynaecological
Malignancy
The Grand Theatre, Swansea
Friday 17 June 2011 – 9.15-4.45
Abertawe Bro Morgannwg University Health Board Specialist Palliative Care Service
37
For further details please see programme and booking form
ABERTAWE BRO MORGANNWG UNIVERSITY HEALTH BOARD
SPECIALIST PALLIATIVE CARE SERVICE
The Palliative Management of Gynaecological Malignancy Friday 17 June 2011 – 9.15am-4.45pm, The Grand Theatre, Swansea
Booking Form (Please Complete in BLOCK CAPITALS)
The charge for this study day is Doctors £50, Nurses and AHPs £40
(includes lunch and refreshments)
Full Name and
Title:
Post or Job Title:
Home:
Address: Work:
Contact No (inc
code):
Email Address:
(Please write
clearly)
NB: We regret that we are unable to issue a refund if you cancel your booking after 30 April 2011
It is your responsibility to ensure payment has been received by us and a place booked for you
Special dietary requirements: Vegetarian � Other (please specify)____________________________
Accommodation information required: � Payment Details:
Please send your completed booking form and payment (cheques payable to ABMUHB) to:
Angela Sinclair
Medical Secretary Hospital Palliative Care Team
Room 227, Radiotherapy Dept
Singleton Hospital, Swansea
SA2 8QA
If you require further information please contact:
Claire Job Macmillan CNS (Hospital Palliative Care Team Leader) – [email protected] or
Angela Sinclair (Team Secretary) – [email protected] or

38
Or telephone - 01792 285337

39
Articles
RESEARCH IN ONCOLOGY AND PALLIATIVE CARE
This is a new feature in “In Touch” to try to keep our members up to date with recently published research with relevance to oncology and palliative care. The page could also be used to offer useful information such as how to write a research proposal or where to get funding. If you want to feedback on this new page or if you have any other ideas for useful additions to this page please do get in touch [email protected] New Articles: van Weert E, May AM, Korstjens I, et al. Cancer-related fatigue and rehabilitation: a randomized controlled multicenter trial comparing physical training combined with cognitive-behavioral therapy with physical training only and with no intervention. Phys Ther. 2010 Oct;90(10):1413-25. Epub 2010 Jul 22. (Original) PMID: 20651011 This randomized controlled trial compared the effect on cancer-related fatigue of physical training combined with cognitive behavioral therapy with physical training alone and with no intervention. INTERVENTIONS: Physical training consisting of 2 hours of individual training and group sports took place twice weekly, and cognitive-behavioral therapy took place once weekly for 2 hours. CONCLUSIONS: Physical training combined with cognitive-behavioral therapy and physical training alone had significant and beneficial effects on fatigue compared with no intervention. Physical training was equally effective as or more effective than physical training combined with cognitive-behavioral therapy in reducing cancer-related fatigue, suggesting that cognitive-behavioral therapy did not have additional beneficial effects beyond the benefits of physical training. Acupuncture for cancer pain in adults. Paley et al (2011) Cochrane Database of Systematic Reviews. Three RCTs (204 participants) were included. One high quality study investigated the effect of auricular acupuncture compared with auricular acupuncture at 'placebo' points and with non-invasive vaccaria ear seeds attached at 'placebo' points. Participants in two acupuncture groups were blinded but blinding wasn't possible in the ear seeds group because seeds were attached using tape. This may have biased results in favour of acupuncture groups. Participants in the real acupuncture group had lower pain scores at two month follow-up than either the placebo or ear seeds group. There is insufficient evidence to judge whether acupuncture is effective in treating cancer pain in. The whole article is available from: http://onlinelibrary.wiley.com/o/cochrane/clsysrev/articles/CD007753/pdf_fs.html Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. Torres Lacomba et al (2010) OBJECTIVE: To determine the effectiveness of early physiotherapy in reducing the risk of secondary lymphoedema after surgery for breast cancer. DESIGN: Randomised, single blinded, clinical trial. SETTING: University hospital in Alcala de Henares, Madrid, Spain. PARTICIPANTS: 120 women who had breast surgery involving dissection of axillary lymph
40
nodes between May 2005 and June 2007. INTERVENTION: The early physiotherapy group was treated by a physiotherapist with a physiotherapy programme including manual lymph drainage, massage of scar tissue, and progressive active and action assisted shoulder exercises. This group also received an educational strategy. The control group received the educational strategy only. CONCLUSION: Early physiotherapy could be an effective intervention in the prevention of secondary lymphoedema in women for at least one year after surgery for breast cancer involving dissection of axillary lymph nodes. Abstract available from: http://www.library.nhs.uk/booksandjournals/advanced/search.aspx?ItemSubCollection=bnj.ovi.emez&ItemId=ovid.com:/bib/embase/20068255&Id=2 Late effects of breast cancer treatment and potentials for rehabilitation. Ewertz (2011). BACKGROUND: Breast cancer is the most frequent malignant disease among women world wide. Survival has been improving leading to an increasing number of breast cancer survivors, in the US estimated to about 2.6 million.MATERIAL AND METHODS: The literature was reviewed with focus on data from the Nordic countries. DISCUSSION: To improve rehabilitation, specific goals have to be formulated into national guidelines and high priority directed towards research into developing and testing new interventions for alleviating symptoms and side effects experienced by breast cancer survivors. Abstract available from: http://www.library.nhs.uk/booksandjournals/advanced/search.aspx?ItemSubCollection=bnj.ovi.prmz&ItemId=ovid.com:/bib/medline/21231780&Id=1 Physical therapy in palliative care: from symptom control to quality of life: a critical review. Kumar (2010) Critical review of physiotherapy in palliative care, with particular reference to its use in India. Abstract available from: http://www.library.nhs.uk/booksandjournals/advanced/search.aspx?ItemSubCollection=bnj.ovi.prmz&ItemId=ovid.com:/bib/medline/21218003&Id=11 Yang CY, Tsai JC, Huang YC, et al. Effects of a home-based walking program on perceived symptom and mood status in postoperative breast cancer women receiving adjuvant chemotherapy. J Adv Nurs. 2011 Jan;67(1):158-68. doi: 10.1111/j.1365-2648.2010.05492.x. Epub 2010 Oct 25. (Original) PMID: 20973811 AIM: This paper is a report of a study analysing the effect of a home-based walking exercise program on symptoms and mood distress among breast cancer women receiving chemotherapy postoperatively. RESULTS: Women in the exercise group reported significantly lower symptom severity scores and mood disturbance compared with those in the control group throughout the study period. CONCLUSION: Regular moderate-intensity exercise can play an important role in improving treatment-related symptoms and mood in women with breast cancer. A home-based walking exercise program can be easily incorporated into care for women with breast cancer undergoing chemotherapy. Abstract available from: http://plus.mcmaster.ca/EvidenceUpdates/NewArticles.aspx?Page=1&ArticleID=38395#Data

41
Editor’s note: This article was published in the Winter 2010 Newsletter and generated a lot of interest. Unfortunately Clare Lait’s name and contact
details were not published with the article. Apologies to Clare and here it is again with full details.
Report for Musculoskeletal Oncology Physiotherapy Service (MOPS) One Year Pilot Study 2009 – 2010 for ACPOPC
Last October 2009 we set up a years pilot study within our trust providing Musculoskeletal Outpatient Physiotherapy for patients post cancer surgery, chemotherapy and radiotherapy. The effects that these treatments have on patients is widespread and it has been reported in the literature that many patients suffer with pain, decreased arm range of movement, arm weakness, neck and back pain, headaches, carpal tunnel problems, lymphoedema, cording (Border et al 1994 Bouffard et al 2007, Box et al 2002, Cheville et al 2007, Fourie 2004, 2006, 2008, Ghazinouri et al 2005, Gottrup et al 2005, Jung et al 2003, Karki et al 2005, Lash and Silliman 2000, Lauridsen et al 2005, Mcneely et al 2006, Reitman et al 2002, Stecco et al 2007 Wyrick et al 2006) and the list continues, post treatment and for many years after too (Lash and Silliman 2000 and Karki et al 2005). Many of these problems as well as the physical effects of cancer and its treatments such as fatigue, nausea, osteoporosis, cardiovascular disease and the psychosocial and emotional issues, have been proven to be improved by physiotherapy and exercise (Lacomba 2009, Box et al 2002, Beurskens et al 2007, Macleod and Koelling, McNeely et al 2009, Jonsson and Johannsson 2009, Milne et al 2008, Sprod et al 2005). Our pilot study was funded by the Thames Valley Cancer Network and was initiated by a questionnaire sent out to patients who attended the Breast Recovery Class with our lymphoedema specialist. This backed the research and suggested within our area that there were still 30% of patients who complained of ongoing problems. The national statistics taken from a review of the literature in 2008 stated that in the UK 72% of patients continued with pain, 67% developed impaired arm function, 34% lymphoedema and 34% upper limb weakness (Fourie). Further surveys have also documented similar statistics based on patients 12 months post operation (Macmillian Health and Well Being Survey 2008). A report by RAGE (radiotherapy action group exposure) carried out by the Maher Committee (1995) highlighted that on top of this need the problems had not been resolved by generalist physiotherapy and only 20% demonstrated improvements and there was therefore a need for Specialist Physiotherapists with a knowledge of cancer and its subsequent treatments and their effects on patients. In light of the government guidelines aiming for Level 3/4 specialists in rehabilitation this was what our service hoped to achieve. My colleague and I have a background in outpatient physiotherapy and so we have a good understanding of the biomechanics of the shoulder joint and the surrounding structures. We attended Willie Fouries’ Myofascial course in London before beginning the service. Willie describes a technique of gentle myofascial release which has been proven to be effective at treating cancer patients due to the effects that it has over the pathological formation of scar tissue post surgery and radiotherapy (Bouffard et al 2007). This provided us with an extra skill to address the common problems that these patients experience. We set the service up to cover three sites, Reading, Newbury and Wokingham based in community hospitals. As part of the government agenda to look at services within the

42
community these seemed appropriate places. These sites are all easy to access, away from the acute hospital and have plenty of parking, all areas that encourage a stress free visit. Collectively my colleague and I worked 19 hours clinically and 3.5 hours were set aside for co-ordinating the project. We were also allocated 4 hours Band 2 administration and clerical time. Both my colleague and I throughout the project worked at a Band 6. Referrals were made by a referral form that could be posted or faxed to a single point of access. Since January – October 2010 we received 107 referrals. I still believe that there are many more patients with problems that are not being addressed. The majority of our referrals came from the Breast Care Nurses and Lymphoedema Specialists but some from Oncologists and Consultants and a few from the GP. Our service has not yet been widely marketed to GPs but the plan is to do this in the near future now that the service has been continued for now. The majority of the patients were post breast cancer but we did have some head and neck and lung cancer patients too. The type of surgery was variable although a lot of patients had had more than one type. The referring problem was also variable and included: multiple reasons, anxiety, tight scars, difficulties with ADLs, cording, reduced range of movement and pain. The time since surgery was interesting with the majority of patients being 0-6 months post operative but a large proportion were 1-2 years or greater than 4 years with one patient being 10 years post op. We also documented those patients with pre-existing musculoskeletal problems but the majority had had none. In terms of looking at those patients pre-operatively and those that may be at risk this makes it difficult to predict. We also identified those patients who had had physiotherapy post op and those that had been given exercises by the Breast Care Nurse. Most of the patients had had leaflets and exercises but only about 15% reported having seen a physiotherapist. The research suggests that leaflets and exercises alone are not as effective as actually seeing a physiotherapist and the government pathways for cancer highlight that a physiotherapist is a requirement for patients post operatively and beyond. The question is where is the most appropriate place for a patient to see a physiotherapist that will address the problems that they encounter. There is talk within our trust of decreasing hospital stay for these patients to 23 hours which would not be enough time for a physiotherapist to see these patients on the ward. The patients coming through this service reported that often they did not have a problem immediately post op but some time after despite doing the exercises given to them by the Breast Care Nurses. Obviously there is a large proportion of patients who only need the exercises and advice and they manage very well. However there is also a large proportion who need the support, such as our service can provide, that is away from the place where they had their surgery and treatment, which has huge psychological implications, and is focusing on quality of life and returning to full function at home, work and leisure activities. The problems that they encounter have been documented to reoccur on and off for 21 months and often for months and even years after. A service such as that provided by ourselves is ideally situated to address these issues and we as Specialist Physiotherapists are ideally skilled and knowledgeable enough to deal with them too. This is backed by the results and feedback that we achieved in the pilot study. The results of the study have been fantastic. We used the DASH outcome measure which looks specifically at Disabilities of the Arm, Shoulder and Hand and is an orthopaedic tool and the FACT G Quality of Life Questionnaire (although the majority of our patients were breast cancer patients we did have some that were not and we were unsure how many initially of each we would see. We have now begun to use the FACT B as this is more specific to these patients.) We also used a patient satisfaction questionnaire.
43
Our patients documented that:
• 70% had reduced pain
• 66% improved movement
• 66% managed their symptoms better
• 54% felt less anxious Our outcome measures suggested that:
• 90% improved in their shoulder function through the DASH whilst
• 10% worsened.
This could be explained through a decline in medical conditions. Of those that filled the questionnaire in 100% had returned to work and leisure activities. The results of the FACT G were also excellent. Physically patients showed:
• 68% improvement
• 16% ISQ
• 16% worsened Functionally:
• 84% improvement
• 11% ISQ
• 5% worsened
The service has identified areas of interest that could, providing the service is continued beyond March 201,1 which is uncertain at present, be developed, such as looking in depth at the areas of fatigue and emotional problems that these patients experience. Emotionally patients seemed to get worse especially with the fear of dying and re-occurrence of their cancer. This needs further investigation. The government’s agenda at present is focussed around patient survivorship. Beginning in 1995 with the Calman Hine Report that initiated the formation of Cancer Networks and promoted the publications such as:
• The NHS Cancer Plan 2000
• The Cancer Reform Strategy 2007
• Rehabilitation Care Pathways 2009
• The National Cancer Survivorship Initiative 2008
and culminating with the National Cancer Survivorship Initiative Vision January 2010 that states that the focus for the patients is on supported care. More specifically on the provision of Specialist Rehabilitation services across the country that use outcome measures and can prove good quality care and cost effectiveness. We are as a service already doing all of these things. It is suggested that by providing services that help self management of these conditions within the community and address the effects of treatment we can improve our patient’s quality of life in many ways and our pilot study backs this. It not only addresses the physical problems but the emotional ones too and by providing support such as this reduces stress and effectively reduces the number of emergency admissions to hospital and visits to GPs. As physiotherapists we are in an excellent position with our background skills to look at pain and restrictions and relate it to a mechanical problem, an emotional one or a combination of a number of factors that we can help. We can relate functional tasks to certain movements and therefore help to

44
address patients concerns about not being able to do them or help them to adapt to move in more effective ways. We are also able to look at pain or restrictions and decipher if in fact they are not related to an area that we can address and that they may be a result perhaps of a development of a secondary cancer. Our service has picked up 4 patients who we have sent back with the suspected development of secondary cancers. We also have good palpatory skills and as part of our assessment we are able to pick up if lymph glands are enlarged and similarly refer patients back to the most appropriate source. One of our patients was so tight in her neck that it was difficult to feel beyond the muscles but in a side lying position when all the muscles and structures were relaxed, a lymph gland was palpated that was not palpable on the other side. Research suggests that 70-75% of secondary cancers are picked up outside Consultation appointments by patients themselves; however we have found that some patients feel they are being paranoid mentioning lumps that they have found and so have failed to mention them. This may mean that we are in a good position to pick up secondary cancers earlier if we are aware of these facts. The government is also focussing their attention towards Vocational Rehabilitation for these patients and again we can demonstrate that with the right support and addressing the functional problems encountered, patients can return to work fully functionally. By addressing this element of rehabilitation we can save the economy billions of pounds of tax contributions and benefits and the government has demonstrated the benefits of it financially (NHS Confederation briefing June 2010) There is so much evidence in the literature that suggests that these patients continue with problems post operatively and post adjuvant treatments, that currently is not being addressed and this is backed by our pilot study. Many patients just accept it as part of what happens post treatment but this should not be the case. As Specialist Physiotherapists we can help with many of these effects both physically and emotionally. We are in a fantastic position to help these patients “live a healthy and active a life as possible for as long as possible” as is suggested in the National Cancer Survivorship Initiative Vision 2010. Our funding has been continued until March 2011 but we will continue to fight to keep this service going as not only do we have proof that we are effective from an outcome measures point of view but patient and clinician satisfaction and feedback has been brilliant and very positive. The evidence suggests that all of these factors help to provide a cost effective service for the NHS and the general economy and more importantly it allows our patients to not only survive but thrive too (Dietz 1980). Clare Lait Specialist Physiotherapist Thames Valley Cancer Network [email protected]

45
References
1) Beurksens C, Uden C, Strobbe L, Oostendorp R and Wobbes T The efficacy of physiotherapy
upon shoulder function following axillary dissection in breast cancer, a randomized controlled
studyBMC Cancer 2007:166doi:10.1186/1471-2407-7-166 2)Border WA, Noble NA, 1994. Mechanisms of disease: Transforming Growth Factor (Beta) in tissue fibrosis. N Engl J Med, 331(19): 1286-1292 3) Bouffard NA, et.al. 2008. Tissue stretch decreases soluble TGF-β and type-1 procollagen in mouse subcutaneous connective tissue: Evidence from ex vivo and in vivo models. J Cell Physiol. 214: 389-395 4) Box RC, Reul-Hirche HM, Bullock-Saxton JE, Furnival CM 2002 Shoulder movement after breast cancer surgery: results of a randomized controlled study of postoperative physiotherapy. Breast Cancer Res Treat 75:35-50 5) Cheville A, Khemka V and Mahony S (2007) The role of cancer rehabilitation in the maintenance of functional integrity and quality of life. In: Choices in Palliative care (pp62-83) New York Springer Science and Business Media 6) Dietz JH JNr (1980) Adaptive rehabilitation in Cancer. Postgraduate Medicine 68 (1) 145 – 153 7) Fourie 2004 WIDENING OUR TREATMENT OPTIONS: UNDERSTANDING THE ROLE OF CONNECTIVE TISSUE IN POST MASTECTOMY PAIN www.wayforward.co.za 8) Fourie W J Nat. Dip. PT (2006) CONSIDERING WIDER MYOFASCIAL INVOLVEMENT AS POSSIBLE CONTRIBUTORS TO UPPER EXTREMITY DYSFUNCTION FOLLOWING TREATMENT FOR PRIMARY BREAST CANCER. www.wayforward.co.za 9) Fourie (2006) New focus on managing painful dysfunction following treatment for Breast Cancer. www.wayforward.co.za 10) Fourie (2008) Lymphatic scarring and secondary lymphoedema post breast cancer treatment. www.wayforward.co.za 11) Ghazinouri R, Levy C, Ben-Porat L, Stubblefield MD 2005 Shoulder impairments in patients with breast cancer: a retrospective review Rehabil Onc 23: 5-8 12) GOTTRUP, H.; ANDERSON, J.; ARENDT-NIELSEN, L; JENSEN, T.S.; Psychophysical examination in patients with post mastectomy pain. Pain, 87 (200) 275 – 284. 13) Jonsson C and Johannsson K (2009) Pole Walking for patients with breast cancer related arm lymphedema Physiotherapy Theory and Practise 25(3) 165-173 14)JUNG, B.F. AHRENDT, G.M.; OAKLANDER, A.L.; DWORKIN, R.H.; Neuropathic pain following breast cancer surgery: proposed classification and research update. Pain, 104 (2003) 1 – 13. 15) Kärki A, Simonen R, Mälkiä E, Selfe J 2005 Impairments, activity limitations and participation restrictions 6 and 12 months after breast cancer operation. J Rehabil Med 37: 180-188
16)Lacomba M, Sanchez M, Goni A, Merino D, Mayoral del Moral O, Tellez E, Mogollon E
Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer:

46
randomised, single blinded, clinical trial BMJ 2010; 340:b5396 doi: 10.1136/bmj.b5396 (Published
12 January) 17) Lash TL, Silliman RA 2000 Patient characteristics and treatments associated with decline in upper-body function following breast cancer therapy. J Clin Epidemiol, 53: 615-622
18) Lauridsen MC, Christiansen P, Hessov I. The effect of physiotherapy on shoulder function in
patients surgically treated for breast cancer: a randomized study. Acta Oncol. 2005;44:449–57.
19) Macleod H and Koelling “Physiotherapy for Patients with Breast Cancer” from Breast Cancer;
Nursing Care and Management Ed: Victoria Harmer 20) Mcneely m, Campbell K, Rowe B, Klassen T, Mackey J and Courneya K (2006) The Effects of exercise on breast cancer patients and survivors: a systematic review and meta-anaylysis 21) Milne H, Wallman K, Gordon S, Courney K (2008) Effects of a combined aerobic and resistance exercise program in breast cancer survivors: a randomised controlled trial 22) Rietman JS, Dijkstra PU, Hoekstra HJ, et al 2002 Late morbidity after treatment of breast cancer in relation to daily activities and quality of life: a systematic review . EJSO 29:229-238. 23) Stecco C, Gagey O, Macchi V, et al 2007 Tendinous muscular insertions onto the deep fascia of the upper limb first part: anatomical study. Morphologie, doi:10.1016/j.morpho.2007.05.001 24) Stecco L 2004 Fascial Manipulation for Musculoskeletal Pain. Piccin Nuova Libraria S.p.A., Padova. Travell 25) Sprod L, Drum S, Bentz A, Carter S, Schneider C (2005) The Effects of Walking Poles on shoulder function in breast cancer survivors. Integrative Cancer Therapies Vol 4 No 4 287 – 293
26) Wyrick SL, Waltke IJ, Ng AV. Physical therapy may promote resolution of lymphatic coding in
breast cancer survivors. Rehab Oncol. 2006;24:29–34. 27) www.nordicwalking.co.uk
The early rehabilitation of a patient with Acute Lymphoblastic Leukemia and Guillain-Barre Syndrome – A case study
Katherine Veitch, Susan Brown Introduction This case study focuses on the early rehabilitation of a patient while in intensive care, who had Acute Lymphoblastic Leukemia and developed Guillain-Barré Syndrome.

47
Acute Lymphoblastic Leukemia (ALL) is a cancer of the white blood cells and affects approximately 200 adults per year in the UK. ALL patients have a compromised immune system due to overproduction of lymphoblast cells1. Neurological complications arise in approximately 50-70% of patients undergoing allogeneic bone marrow transplant (BMT) (Wen et al, 1997). Although most of these complications involve the central nervous system (CNS), the peripheral nervous system (PNS) may also be affected.
Guillain-Barré Syndrome (GBS) is an immune mediated illness of the peripheral nerves and nerve roots (Hughes, 2005). It presents with features such as progressive, symmetrical ascending paralysis, loss of tendon reflexes, dysautonomia, sensory deficits and respiratory insufficiency usually peaking within four weeks of onset (Khan et al, 2010). It affects about 1500 adults per year in the UK (Guillain-Barré Syndrome Support Group, 2011). The most significant risk factors for GBS include recent acute respiratory infection and recent bone-marrow transplantation (Simmons, 2010). Immune-modulating treatments, such as plasmaphoresis and intravenous immunoglobulin (IVIg) are principal disease modifying treatments which aim to reduce nerve damage, and have been shown to hasten the recovery process. (Raphael et al, 2008 and Hughes et al, 2010). While two thirds of patients with GBS achieve a good physical recovery (Chio et al, 2003), around 20% are left with persistent and significant disability (Hughes et al, 2005). Though there is little evidence of the efficacy of physiotherapy, a recent survey of patients with GBS reported that patients who did not receive physiotherapy as an in-patient experienced considerable levels of disability with a significant amount of those requiring a wheelchair for mobility (Davidson et al, 2009).
History
A previously fit and active 57 year old man was diagnosed with Pro B2 ALL in November 2009 after a short history of fatigue. He was treated following the UKALL 12 protocol3 and had a double cord blood transplant4 in May 2010. The graft failed and he went on to receive a haplo-identical allogeneic5 stem cell transplant in August 2010. He initially tolerated the transplant procedure well and was discharged home within three weeks. He had not returned to work and continued to be limited by fatigue and diarrhoea.
In September 2010 he presented to the outpatient clinic with flu-like symptoms and was treated for Para-flu 3 infection. In early October he was beginning to recover from this when he developed severe weakness and altered sensation in his hands and feet.
He was admitted to A&E with progressive weakness and difficulty breathing. He was intubated and ventilated before being transferred to the critical care unit (CCU) at his local cancer centre at the end of October. On transfer he underwent IVIg and plasmaphoresis treatments.
1 Lymphoblast cells form from an over-development of immature Lymphocyte cells. Lymphoblasts cause death by
proliferating uncontrollably and crowding out normal cells in the bone marrow and by metastasising to other organs.
ALL is more common in children, but in adults approximately 35 – 60% of patients have long-term disease free
survival.
2 An immature subtype of ALL characterised by: aggressive clinical features, frequent central nervous system
involvement, and a poor prognostic outcome.
3 A Chemotherapy treatment recommended for ALL patients. It is a combination of 5 different drugs and is given over a
period of 28 days.
4 Umbilical cord blood transplantation from two donors, as the small supply of blood in each cord is often inadequate to
meet the needs of an adult patient. This type of transplantation is now widely becoming used as an alternative stem cell
source for patients without a matched unrelated, or matched related donor.
5 A blood transplantation from a mismatched family donor for patients without an HLA identical sibling donor.
48
Physically he presented with quadriplegia, and a left sided facial palsy. He was unable to effectively ventilate or spontaneously cough. He had some flickers of activity around his shoulders and was attempting to mouth words.
His multi-disciplinary rehabilitation began two days after admission. His physiotherapy treatment was aimed at:
1. minimising the risk of developing respiratory tract infections and maximising lung volumes
2. preventing avoidable physical complications, such as contractures and deconditioning
The therapy team produced a structured timetable, ensuring time with each healthcare professional, and agreed rehabilitation goals with the patient and CCU team. Goals were reviewed and set weekly. His treatments and achievements were recorded in a diary as suggested by the NICE guidance for Rehabilitation after Critical Care (2009). A letter board was used to facilitate successful communication. The timetable ensured there was protected time for weaning from ventilatory support, which consisted of reducing the support with periods of cuff deflation and use of a Passy-Muir speaking valve. This was carefully coordinated alongside the physical rehabilitation, so that incremental functional goals, e.g. being able to wash his own face, were continually being met.
The significant limiting factors to his rehabilitation were:
Pain: particularly in feet. He perceived light touch as excruciating, most notably when first standing on the tilt table and weight bearing to initiate sit-to-stand. This is commonly seen in people with GBS and is neuropathic in origin, often managed with Gabapentin (Sulton, 2002). Therapy interventions included de-sensitising techniques and passive stretching, in addition to massage to alleviate residual pain which reduced over a period of six weeks. These techniques have been supported as effective in treating neuropathic pain by Khan and Ng (2009).
Diarrhoea: a symptom of low grade Graft Versus Host Disease (GvHD)6 which is a common problem for patients post allogenic blood transplant. The frequency of diarrhoea affected his nutrition, his PEG feed was discontinued to reduce the high volumes of diarrhoea and TPN was commenced. A Flexi-SealTM flexible bowel management tube was used. These measures managed the diarrhoea sufficiently for rehabilitation to continue.
Fatigue: a long-standing symptom related to ALL, also known to persist in 80% of patients with GBS (Khan and Ng, 2009). For him, this was compounded by poor nutrition, neuropathic pain, abdominal cramps and muscle deconditioning.
In January 2011 he had been decannulated and had no residual respiratory or speech problems; he was transferred to the haematology ward where rehabilitation continued. He had regained significant strength in the limbs and trunk to enable him to sit unsupported for short periods, use his arms to assist with personal care, and transfer with a standing hoist. Though he had generalised stiffness throughout, functionally significant contractures had been prevented.
Discussion
We felt this case to be unusual but Wen et al, (1997) highlighted that an increasing number of patients undergoing BMT are suffering with complications of GBS, and as more people undergo BMT and survivorship increases, the incidence of GBS in such patients could well rise.
There is no specific evidence for exercise in critical care for haematology patients although there is some evidence to support the treatment of fatigue using exercise in the post
6 An inflammatory disease unique to allogeneic blood transplants. It is an attack of the ‘new’ bone marrow immune
cells against the recipient’s tissues. It mainly affects the skin, mouth, stomach and gut, and liver.
49
treatment stage (Dimeo, 1997). Treatment is therefore problem-based using evidence from general populations in critical care and followed recommendations from the NICE guidance Rehabilitation after Critical Care (2009).
A recent Cochrane review of multidisciplinary (MDT) care for Guillain-Barré Syndrome (Khan et al. 2010) found three observational studies but concluded that it found some support for improved disability in the short term when high intensity inpatient MDT rehabilitation was provided. It reported contributions to improvements in quality of life and participation.
Fatigue and diarrhoea specific to this patient’s ALL were limiting factors to the intensity of this patient’s rehabilitation but the case demonstrates that an early, structured rehabilitation programme with structured weaning facilitated this patient to achieve treatment goals beyond those expected. The MDT reflected that the close communication and regular review of goal setting and achievements with the patient provided an important boost to his motivation and therefore concordance with therapy. The patient reported that the regular goal setting, along with the fact that he was given some choice over his rehabilitation interventions, contributed to an overall positive experience.
Conclusion
This case study reinforces the importance of early, structured rehabilitation and tailored weaning in complex haematology patients in order to achieve patient centred goals and maximise functional recovery where there is potentially limited prognosis.
References
CancerBackup (2011) What is Acute Lymphoblastic Leukemia? Available at: (Accessed 17.02.11).
Chio, A., Cocito, D., Leone, M., Giordana, M., Mora, G., Mutani, R. (2003) Guillain-Barre Syndrome : a prospective, population-based incidence and outcome survey. Neurology, 60, 1146-50.
Davidson, I., Wilson, C., Walton, T., Brissnden, S. (2009) Physiotherapy and Guillain-Barre Syndrome: results of a national survey. Physiotherapy 95, 157-63
Dimeo, F., Tilmann, M., Bertz, H., Kanz, L., Mertelsamann, R., Keul, J.(1997) Aerobic exercise in the rehabilitation of cancer patients after high dose chemotherapy and autologous peripheral stem cell transplantation, Cancer, 79, 1717-1722.
Guillain-Barré Syndrome Support Group (2011) A quick guide to GBS and CIDP. Available at: http://www.gbs.org.uk/quickguide.html (Accessed 24.02.11).
Hughes RA. (2005) Guillain-Barré Syndrome, Lancet, 2005;366 (9497): 1653–66. Hughes RA, Raphael JC, Swan AV, Van Doorn PA. Intravenous immunoglobulin for Guillain Barre syndrome. Cochrane Database of Systematic Reviews: (2010), Issue 6. Art. No.: CD002063. DOI: 10.1002/14651858.CD002063.pub4.
Khan, F., Ng, L. (2009) ‘Guillain-Barré Syndrome: An update in Rehabilitation, International Journal of Therapy and Rehabilitation, 16 (8), 451-460.
Khan F, Ng L, Amatya B, Brand C, Turner-Stokes L. Multidisciplinary care for Guillain-Barré Syndrome. Cochrane Database of Systematic Reviews 2010, Issue 10. Art. No.: CD008505. DOI: 10.1002/14651858.CD008505.pub2.
National Institute for Health and Clinical Excellence (2009) Rehabilitation after Critical Care. Available at: http://www.nice.org.uk (Accessed: 24.2.11).
Raphael, JC., Chevret, S., Hughes, RA., Annane, D. Plasma exchange for Guillain- Barre syndrome. Cochrane Database of Systematic Reviews (2008) Issue 2. Art. No: CD001798. DOI: 10.1002/14651858.CD001798.
Simmons, S. (2010) Guillain-Barré Syndrome: A nursing nightmare that usually ends well, Nursing, January, 24-29.
Sulton, L. L. (2002) Meeting the Challenge of Guillain-Barré Syndrome, Nursing Management, 33 (7), 25-31.
Wen, P. Y., Alyea, E. P., Simon, D., Herbst, R. S., Soiffer, R. J., Antin, J. H. (1997) Guillain-Barré Syndrome following allogeneic bone marrow transplantation, Neurology, 49, 1711-1714.