
Implant supported overdentures
121
-
Upload
murtaza-kaderi -
Category
Education
-
view
2.167 -
download
12
Transcript of Implant supported overdentures


DR DEEPA PM
IMPLANT SUPPORTED OVERDENTURES

CONTENTS• Introduction• Development of overdentures• Indications and Contra-Indications• Advantages and Disadvantages• Prosthetic options in implant
dentistry • Treatment options for mandibular
implant overdenture• Mandibular Implant Site Selection• Overdenture movement • Treatment plan for completely
edentulous maxilla

CONTENTS• Overdenture attachment• Mandibular Implant overdenture
design and fabrication• Step by step procedure for
fabrication of implant supported over denture
• Complications • Maintenance• Conclusion

Overdenture treatment is a notion which precludes the inevitability of “floating plastic” in edentulous mouths. ( George Zarb).
INTRODUCTION

Conventional denture
Extraction of badly broken teeth Decreased support
Decreased Retention
Increase bone resorption Absence of Proprioceptive
response

• For decades, natural teeth have been retained in the mouths to support/retain overdentures and preserve bone.
• Overdentures supported by implants have a higher probability of success than overdentures supported by the roots of natural teeth (Mericske-Stern, 1994)

DEFINITION• An overdenture is defined as a
removable prosthesis that covers the entire occlusal surface of a root or implant ( Harold W Preiskel).
• Any removable dental prosthesis that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and/or dental implants; a dental prosthesis that covers and is partially supported by natural teeth, natural tooth roots, and/or dental implants (GPT-8).

DEVELOPMENT OF OVERDENTURES
• In 1856, Ledger described a prosthesis resembling an overdenture. His restorations were referred to as “Plates covering fangs”.
• In 1861 a conference held in Connecticut, increased the awareness of the value of such roots in supporting a covering denture.
• In 1888 Evans had described a method of using roots actually to retain restorations.

• In 1896 Essig had prescribed a telescopic like coping. At the same time Peeso also described a removable telescopic prosthesis.
• In 1909 a great blow was delivered by William Hunter by way of his “focal sepsis theory”.
• In 1976 Rothman stated that Hunter’s comments gave dentistry a black eye.

PROSTHETIC OPTIONS IN IMPLANT DENTISTRY
Type Definition
FP-1 Fixed prosthesis; replaces only the crown, looks like a natural tooth.
FP-2 Fixed prosthesis; replaces the crown and a portion of the root; crown contour
appears normal in the occlusal half but is elongated or hypercontoured in the
gingival half.
FP-3 Fixed prosthesis; replaces missing crown and gingival color and portion of the
edentulous site; prosthesis most often uses denture teeth and acrylic gingiva,
but may be porcelain to metal.
RP-4 Removable prosthesis; overdenture supported completely by implant.
RP-5 Removable prosthesis; overdenture supported by both soft tissue and implant.

INDICATIONS FOR IMPLANT SUPPORTED OVERDENTURE TREATMENT
• Severe morphologic compromise of denture supporting areas that significantly undermine denture retention.
• Poor oral muscular coordination • Low tolerance of mucosal tissues• Parafunctional habits leading to
recurrent soreness and instability of prosthesis.

• Unrealistic prosthodontic expectations .
• Active or hyperactive gag reflexes.

CONTRAINDICATIONS• Recent myocardial infarction
• Valvular prosthesis
• Severe renal disorder
• Treatment-resistant diabetes
• Generalized secondary osteoporosis

• Chronic and severe alcoholism
• Treatment – resistant osteomalacia
• Radiotherapy in progress
• Severe hormone deficiency
• Drug addiction
• Heavy smoking habits
ADVANTAGES OF IMPLANT-SUPPORTED PROSTHESIS:
• Minimum anterior bone loss; prevents bone loss
• Improved esthetics • Improved stability (reduces or
eliminates prosthesis movement) • Improved occlusion (reproducible
centric relation occlusion)• Decrease in soft tissue abrasions• Improved chewing efficiency and force

• Improved retention• Improved support• Improved speech • Reduced prosthesis size
(eliminates palate flanges)• Improved maxillofacial prosthesis

CONVENTIONAL DENTURES v/s IMPLANT OVERDENTURES
•Patient satisfaction increased when mandibular implantoverdentures were used instead of conventional complete dentures (Burns, 1995;Boerrigter, 1995). •Implant overdentures generally offer the advantages of improved comfort, support, retention, and stability. •Annual bone resorption is more pronounced in patients who wear conventional complete dentures than implant overdentures(Jacobs, 1993).

NATURAL TOOTH OVERDENTURES v/s IMPLANT OVERDENTURES
Overdentures supported by implants have a higher probability of success than mandibular overdentures supported by the roots of natural teeth (Mericske-Stern, 1994).

IMPLANT OVERDENTURE V/S FIXED PROSTHESIS
1. A smaller number of implants are required and that decreases the cost.(Johns, 1992; Cune, 1994).
2. It is possible to provide better support of the facial soft tissues (Johns,1992; Cune, 1994; Mericske-Stern, 1998).
3. There is improved phonetics for completely edentulous patients. (Jemt,1992; Smedberg, 1993; Cune, 1994; Mericske-Stern, 1998).
4. Patients have enhanced access for oral hygiene .(Johns, 1992; Mericske-Stern, 1998).
5. There is a better result when unfavorable jaw relationships are present(Cune, 1994).
6. When there is an opposing complete denture, it will be more stable;particularly when there is a resorbed residual ridge (Johns, 1992; Hutton,1995).
7. It is easier to make modifications to the prosthesis base (Mericske-Stern,1998).
8. There is better access for inspection of the surgical site when surgically created oral defects are present (Mericske-Stern, 1998).

DISADVANTAGES OF OVERDENTURES
• Does not satisfy the psychologic need of these patients
• It requires proper plaque control and denture hygiene.
• It is more costly compared to complete dentures.
• They are bulkier than many other restorations.
• More load to the prosthesis , • The lack of sufficient interarch space
makes an overdenture system more difficult to fabricate and more prone to component fatigue and fracture.

OVERVIEW OF TREATMENT PLANNING
•Medical evaluation
•Dental evaluation
•Formulation of treatment plan

MEDICAL EVALUATION
•Medical history (like heart disease, hepatitis, AIDS)
•Vital signs
•Complete blood count
•Urinalysis
•Chest X-ray and Electrocardiogram

DENTAL EVALUATION
• Dental history
• Clinical evaluation
• Diagnostic records
• Patient expectations

FORMULATION OF TREATMENT PLANNING•Diagnostic records
•Transitional prosthesis
•Surgical/fixture placement
•Surgical / fixture connection
•Definitive restoration
•Maintenance

OVERDENTURE MOVEMENT: (PM)
Misch (1985)• PM 0 : No movement of prosthesis,
requires implant support similar to fixed prosthesis
• PM 2: Prosthesis with hinge motion• PM 3: Prosthesis with hinge and apical
motion• PM 4: Allows movement in four
directions• PM 6: All ranges of prosthesis movement

REMOVABLE PROSTHESES
• There are two types of removable prostheses, depending on the amount of implant support.

REMOVABLE PROSTHESES-4 (RP-4)
•Completely supported by the implants•The restoration is rigid when inserted• Overdenture attachments usually connect the removable prosthesis to a low-profile tissue bar or superstructure that splints the implant abutments.• Usually five implants in mandible and six to eight implants in the maxilla are required.•Denture teeth and the acrylic bulk are required for the restoration.• Requires a more lingual and apical implant placement in comparison with FP-1 and FP-2 prosthesis.

REMOVABLE PROSTHESES-5 (RP-5)
• A removable prosthesis combining implant and soft tissue support.
• Two anterior implants, independent of or splinted in the canine region
• Three splinted implants in the premolar and central areas , or
• Four implants splinted with a cantilevered bar.
• Primary advantage of an RP-5 restoration is the reduced cost.

MANDIBULAR IMPLANT SITE SELECTION

OPTION
DESCRIPTION REMOVABLE PROSTHESIS TYPE 5

OVERDENTURE OPTION 1:( OD-1)
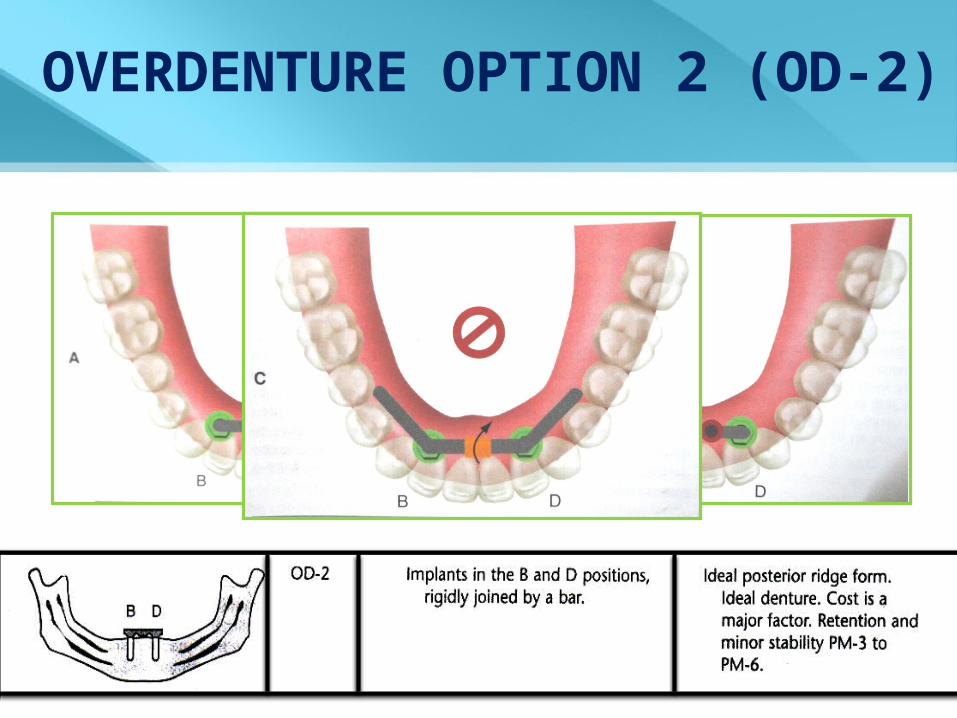
OVERDENTURE OPTION 2 (OD-2)
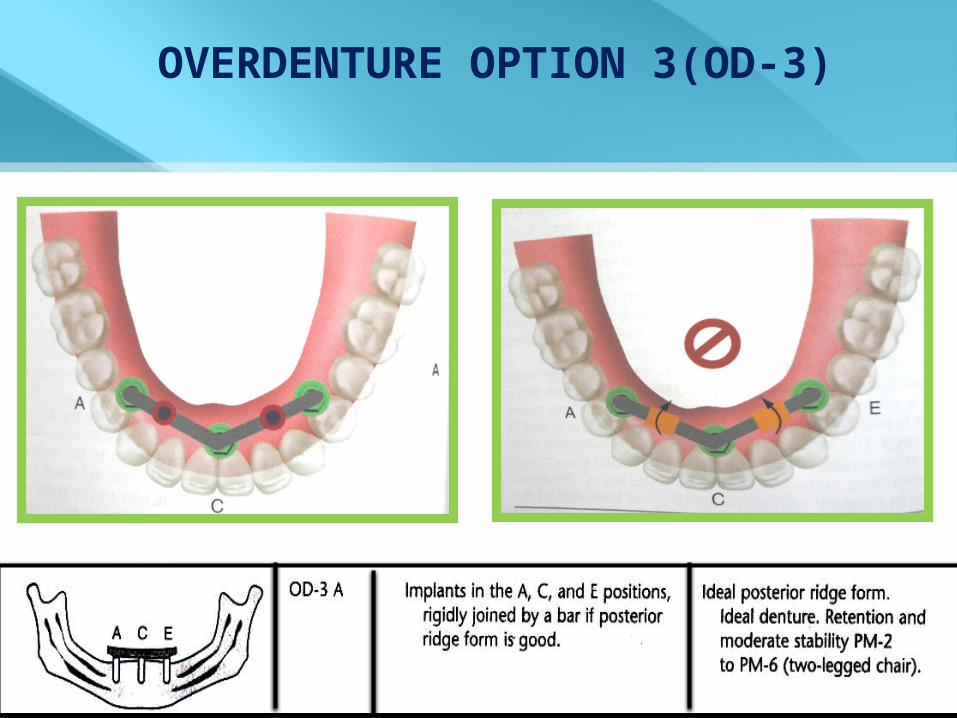
OVERDENTURE OPTION 3(OD-3)

OVERDENTURE OPTION 3 (OD-3B)

OVERDENTURE OPTION 4(OD-4)

OVERDENTURE OPTION 5(OD-5)

ARCH FORMS

HIDDEN CANTILEVER• It is that portion of the cantilever that
extends beyond the connecting bar. If the prosthesis does not rotate at the end of the bar to load the soft tissue, a hidden cantilever exists.
The teeth on the final restoration usually do not extend beyond the bar. This helps prevent a hidden cantilever, which may extend beyond this position.

MAXILLARY OVERDENTURE • Only two treatment options are
available.• Independent implants are not an
option because bone quality and force direction are severely compromised.
• Cantilever bars are usually not recommended for the same reasons.
• The crown height space:• 15 mm- anterior space• 12 mm- posterior space

COMPARISON OF MAXILLARY AND MANDIBULAR OVERDENTURES
• Jemt et al reported survival rates of 94.5% for implants and 100% for prosthesis in mandible whereas, 72.4% for implants and 77.9% for prosthesis in maxilla.
• High failure rates were due to poor density and quantity of bone with characteristic cluster failure pattern.
• Misch followed 75 maxillary IODs for 10 years with 97% implant survival and 100% prosthesis survival.
• Greater implant number and key implant positions reduce failure and decrease risk

MAXILLARY RP-5 IMPLANT OVERDENTURE

MAXILLARY RP-4 IMPLANT OVERDENTURE

ALL ON 4 CONCEPT
Dental implants Art and Science, 2nd edition Charles Babbush
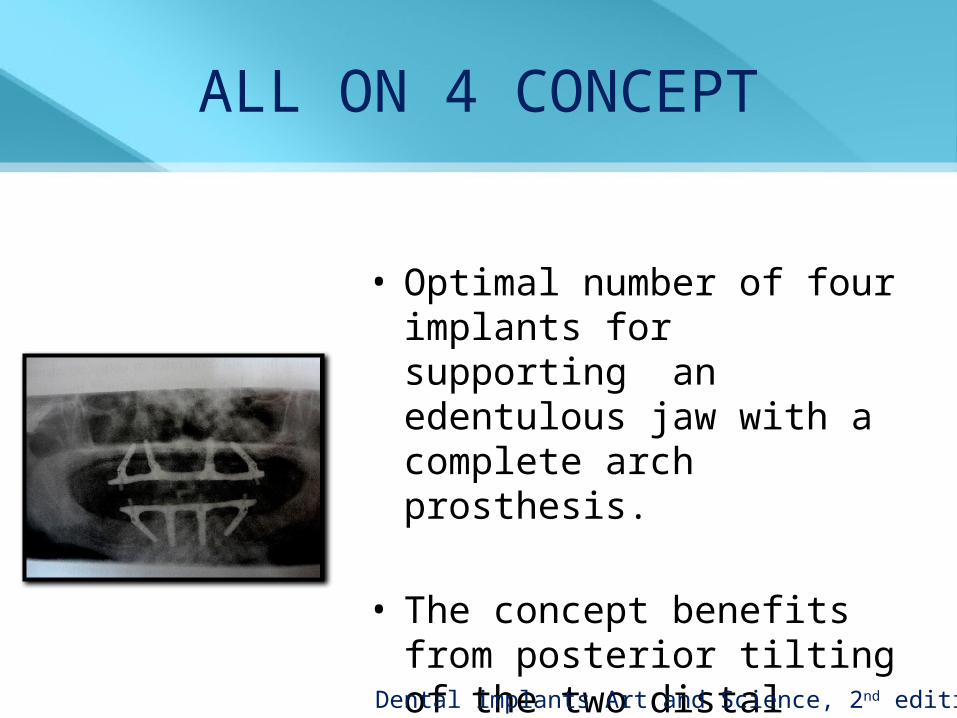
ALL ON 4 CONCEPT
• Optimal number of four implants for supporting an edentulous jaw with a complete arch prosthesis.
• The concept benefits from posterior tilting of the two distal implants with a maximum of a two teeth distal cantilever in the prosthesis.
Dental implants Art and Science, 2nd edition Charles Babbush

ALL ON-4 CONCEPT- Tilted abutments
• The implant support is moved posteriorly.• The implant length can then be increased.• The maxillary implant follows a dense
bone structure(the anterior wall of the maxillary sinus) and reaches high density bone in the anterior maxilla, enhancing the primary stability.
• The desired position of the implants is determined from the prosthetic point of view.
• A favourable inter-implant distance and small cantilevers are possible.
Dental implants Art and Science, 2nd edition Charles Babbush

ALL ON 4 HYBRID
Dental implants Art and Science, 2nd edition Charles Babbush

ALL ON 4 EXTRA MAXILLA
Dental implants Art and Science, 2nd edition Charles Babbush

ALL ON 4 CONCEPT ADVANTAGES
• Elimination of bone grafting procedures:
1. Shorter treatment plan,2. Less patient morbidity,3. Decreased cost,4. Immediate restoration.• Increase in A-P spread
more stable prosthesis.• Elimination or shortening of
cantilevers.• Avoidance of various anatomic
structures.• Fewer implants to support the
prosthesis.
Maxillary All on Four Therapy using Angled Implants, Dent Clin N Am 55(2011) 779-794

SINGLE IMPLANT SUPPORTED OVERDENTURE
• High implant success rate have been achieved by using 2 or more implants to anchor an overdenture (Stephan et al., 2007; Bergendal and Engquist, 1998; Chiapasco et al., 2001; Payne et al., 2001).
• Because mandible is hinge-like and its buttressing lingual bone is shock absorbing, use of 2 implants is optimal for support and retention of overdenture and also some researches know this as a standard for edentulous mandible (Lee and Agar, 2006; Sadowsky and Caputo, 2004).

• Yet many patients could not receive implants treatment because of financial problems and with regard to a recent studies that report immediate loaded single implant retained overdenture as a safe, reliable and cost effective treatment (Chiapasco et al., 2001; Liddelow and Henry, 2007, 2010; Kronstrom and Davis, 2010).

SINGLE IMPLANT RETAINED MANDIBULAR OVERDENTURE WITH IMMEDIATE LOADING (CASE REPORT)
Fariborz Vafaee,et al Research Journal of Medical Sciences
Year: 2011 | Volume: 5 | Issue: 5 | Page No.: 273-275
Marginal bone loss was comparable to delayed loading of implant and was 0.5 mm at 6 month, that was acceptable (Misch and Bidez, 2008). There were no signs of BOP and probe depth were not abnormal (3 mm).

ATTACHMENT SYSTEMS FOR MANDIBULAR SINGLE-IMPLANT OVERDENTURES: AN IN VITRO
RETENTION FORCE INVESTIGATION ON DIFFERENT DESIGNS.
Alsabeeha N, Atieh M, Swain MV, Payne AG. Int J Prosthodont. 2010 Mar-Apr;23(2):160-6
. • Six different attachment systems
used for mandibular single-implant overdentures, including two prototype large ball attachment designs.
• Mandibular single-implant overdentures are a successful treatment option for older edentulous adults with early loading protocol using implants of different diameters and with different attachment systems.

THANK YOU

GOOD MORNING

OVERDENTURE ATTACHMENTS
Overdenture restorations
Bar-retained
Conical abutme
ntDirect
abutment Non-hexed
Abutment-retained
Supra-snap abutment
Principles and practice of implant dentistry; Charles Weiss,1st edition.

OVERDENTURE ATTACHMENTS(Based on resiliency)
• Rigid Non- Resilient Attachments: ex: Screw retained hybrid overdenture .
• Restricted Vertical Resilient Attachments: prosthesis can move up and down with no lateral, tipping or rotary movement.
• Hinge Resilient Attachments: resists lateral tipping, rotational and skidding forces. Ex: Hader bar or any other kind of round bar can provide hinge resiliency.
Clinical and laboratory manual of implant overdenture , Hamid R Shafie

OVERDENTURE ATTACHMENTS(Based on resiliency)
• Combination Resilient Attachments: Allow unrestricted vertical and hinge movements ex: Dolder bar joint.
• Rotary Resilient Attachments: prosthesis can provide vertical hinge and rotary movements.
• Universal Resilient Attachments: provide vertical, hinge, translation and rotation movements. Ex: Magnetic attachments.Clinical and laboratory manual of implant overdenture , Hamid R Shafie

ATTACHMENT SELECTION CRITERIA• Available bone.
• Patient’s prosthetic expectations.
• Financial ability of the patient to cover treatment costs.
• Personal choice and clinical expertise of the dentist.
• Experience and technical knowledge of the lab technicians.
Clinical and laboratory manual of implant overdenture , Hamid R Shafie

• Stud attachment– Dalbo attachments– Ceka attachment– Rothermann attachment
• Bar attachment– Dolder bar– Hader bar

• Male component projects from
implant
Intra radicular
• Male element forms part of the denture base and engages a specially produced depression within the root contour
Extra radicular
STUD ATTACHMENTS
Harold W Prieskel. Overdentures made easy

O-RING OR BALL ATTACHMENT
• Doughnut shaped, synthetic gasket
• Ability to bend with resistance and return to their approximate original shape
• Attaches to a post with a groove or undercut area for O-ring

• Advantages: -Ease of changing attachment -Wide range of movement -Low cost -Different degrees of retention - Possible elimination of time and
cost of superstructure

• Classification of O-ring
1. Static 2. Dynamic – one of
the most resilient or mobile types of attachment

PARTS OF O-RING ATTACHMENT
1. Metal encapsulator- permits easy replacement,
Internal cavity- an undercut region that houses ring. Stainless steel is recommended
2. O-ring post- made up of machined titanium alloy
It has a head, neck and body.
Head is wider than neck.3.O - ring – variety of diameters.
( 3 sizes) larger the diameter ,
easier it is to place the O-ring within the encapsulator greater the retention.

• O-ring hardness: Measured with durometer
ranges from 0-100 in a shore A scale softest O-rings are usually 30-40 hardest are- 80-90.• O-ring materials
Nitrile and Flurocarbon is one of the more widely used elastomers.

TROUBLESHOOTING
1. Extrusion and Nibbling Cause: when O-ring materials are too soft or ring
is too large
Solution: use harder O-ring material install a properly sized O-ring

2. Spiral failure
Cause: when certain segments of O-ring slide while other segments simultaneously roll.
Solution: evaluation of the post to ensure that it is not out of round, increasing O-ring Hardness and making sure that patient uses lubricant daily

3. Abrasion :Cause: -bruxism - lifting and
seating of overdenture as nervous habit
- rough metal surface
Solution: use recommended metal finishes

4. Compression set:Cause: -Para-functional
clenching of the prosthesis
- selection of an elastomer with poor compression set
Solution: remove prosthesis at night, reduce O-ring hardness

5. Installation damage; Cause: -sharp edges on
the encapsulator, or on the O-ring post head,
-too large an O-ring for encapsulator
-twisting of the O-ring, too small O-ring for post
Solution: intallation of properly sized O- ring using lubrication during
assembly.

DALBO STUD ATTACHMENT
Rigid unit
Ball and socket unit(Vertical and
rotational movement)
Nylon ring – protects the lamella Retention – altering
the positions of free ends of the lamella

ROTHERMAN ECCENTRIC ATTACHMENT
Button shaped attachment Patrix – eccentric cylinder with undercut or groove Matrix – Clip or clasp armActivation : Bending the clasp arm towards center
Resilient unit
Rigid units

ZEST ANCHOR ATTACHMENT
Polyethylene – Nylon stud
Matrix
Funnel shaped tube
Instrumentation kit
Advantages : Reduce vertical space requirement Loads are transferred more apically.

CEKA ATTACHMENT
Ceka revax
Extra radicular
Intra radicular
Patrix – metal ring Matrix – attachment pin (split metal post)

DOLDER BAR
Egg shaped bar in cross sectionOpen sided sleeve Two sizes 3.5mm x 1.6mm,
3.0mm x 2.2mmSpacer – degree of movement

MOVEMENTS SEEN IN DOLDER BAR

HADERBAR Helmut Hader in 1960 Available as a prefabricated plastic pattern
Notable feature Resin / plastic
sleeve No spacer- more
support
English, Donnel & Staubli (1992) Hader EDS system
System with 3mm height (8.3mm).

Clips with metal encapsulator
Advantage
Prefabricated plastic pattern – no need for soldering.
Precise fit, simplicity, versatility

Advantages of bar attachments : Rigidly splint the teeth Provides good retention, stability and support Provides cross arch stabilizationPositioned close to the alveolar bone (exhibit less leverage)
Disadvantages : Bulk of bar Plaque accumulation Wearing Soldering procedure Manual dexterity
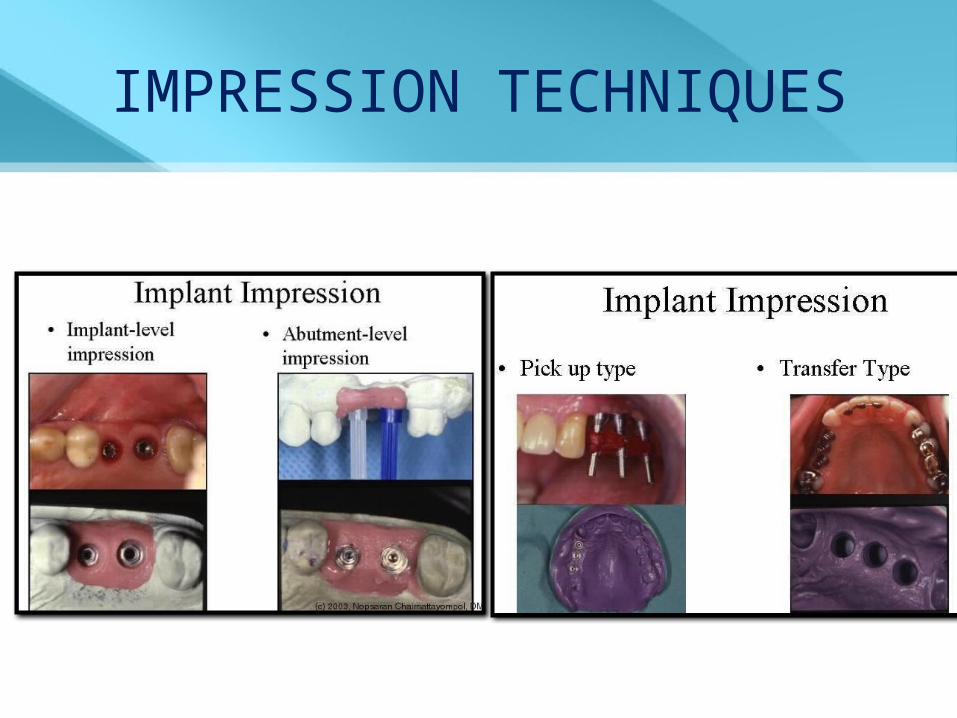
IMPRESSION TECHNIQUES

INDIRECT (CLOSED-TRAY)
TRANSFER TECHNIQUE

• Step 1
Note : if working with multiple implants, remove one healing abutment at a time to place the impression coping.
IMPRESSION TECHNIQUE

Step2
• Place impression (tapered)coping…• Once it is seated…
A radiograph / a non-abrading explorer used to assure that the impression coping is fully seated.

Step3 Block out the hex holes
Step 4
Verify fit of tray

Step 5
Once impression material is fully set, remove tray.

• Step 6 Remove impression coping…• Attach the appropriate replica to the
impression coping.

Step7• Reinsert impression coping into the
impression. The cut out area on the impression coping should align perfectly into impression.

Step8 Create soft tissue modelAfter applying lubricant, soft tissue replica material placed around analog
Step 9Fabricate working cast

DIRECT (OPEN-TRAY) TRANSFER TECHNIQUE / PICK-UP IMPRESSION TECHNIQUE

Custom impression tray / select a stock tray and mold the border with greenstick compound material
Custom tray : Make a full-arch impression of the Healing Collars or Surgical Cover Screws, edentulous areas and remaining dentition and fabricate primary cast.
Block out the areas above the Healing Collars or Surgical Cover Screws with base plate wax to
simulate the positions of the implant transfers that will be used.
Fabricate the custom impression tray with auto polymerizing or light-cure tray resin.
TRAY SELECTION

• This transfer procedure requires a custom tray or modified stock tray with screw access holes in the areas occlusal to the implants
• Create an opening above the implant areas to allow for access to the Direct Transfer screws.

Step 1 Remove Healing Abutment
Step 2Place Pick-up CopingRadiographic ally verify correct seating of the coping.
IMPRESSION TECHNIQUE

Step 3 Verify screw/tray clearance
Step 4
Make full-arch impressionunscrew and remove all the retaining screws. Then remove tray, capturing the transfers in the impression

Step 5Attach analog to Pick-up Coping
Step 6Create soft tissue model
Step 7Fabricate working cast
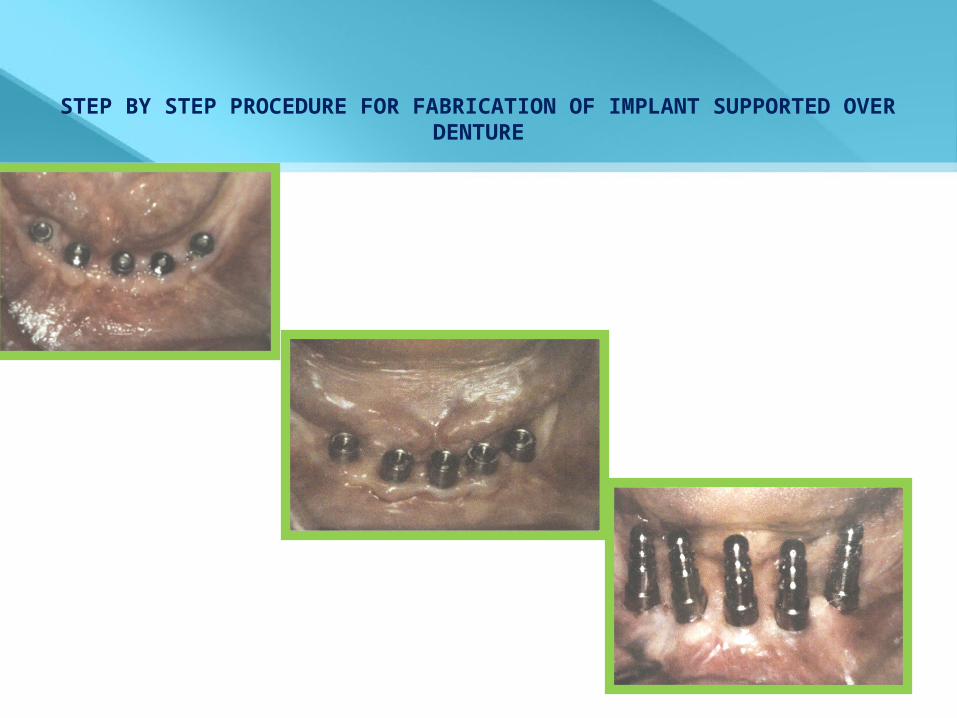
STEP BY STEP PROCEDURE FOR FABRICATION OF IMPLANT SUPPORTED OVER DENTURE








OCCLUSAL CONSIDERATIONS• The most common implant
treatment, which includes a traditional soft tissue supported complete denture, is a maxillary denture opposing a mandibular implant supported restoration.
• The occlusal scheme for this condition:
1. Raises the posterior occlusal plane, 2. Uses a medial positioned lingualized
occlusion, and has a bilateral balanced scheme.
• Whether the mandibular restoration is FP-1, FP-2, FP-3, RP-4, or RP-5, the maxillary denture follows these guidelines.

• The mandibular implant supported restoration may exert greater force on the premaxilla than a mandibular denture and cause accelerated bone loss.
• Therefore modification of the occlusal scheme aims at protecting the premaxilla under a maxillary denture by the total elimination of anterior contacts with the mandibular anterior teeth in centric occlusal relation.

MAINTENANCE


COMPLICATIONS• While procedural complications can and do
occur during the fabrication phase of prosthodontic treatment following abutment connection, most are technique-related and are usually reversible.
• Following the placement of a completed prosthesis, the loss of implant anchorage or soft tissue or mechanical complications may also occur.

• The loss of anchorage or nonintegration is generally the latent result of
- surgical trauma, - contamination, - or prosthesis overload.
Clinical experience has shown that precise, atraumatic, sterile surgical technique is essential for osseointegration.

• Among other causes, loss of anchorage attributed to fixed prosthesis function can result from an
1. Ill-fitting metal frame,
2. Overextended cantilevers,
3. Or a poorly conceived occlusal scheme .

INADEQUATE TORQUE APPLICATION
• Amount of torque suggested by the manufacturers on the abutment screw range from 20 to 35 N/cm and a torque wrench is required to obtain a more consistent value

INADEQUATE FRAMEWORK ABUTMENT INTERFACE

OCCLUSAL DISCREPANCY AND JAW RELATION
• Occlusal forces should be shared evenly by all implants .
• Occlusal adjustments during lab remounts , as well as intraorally during insertion of prosthesis.

• Destructive screw loosening as well as fracture of the screw may take place due to destructive forces .

FRAMEWORK FRACTURE

CONCLUSION• Implant overdentures borrow several
principles from tooth supported overdentures.
• The advantage relates to the ability to place rigid, healthy abutments in anterior positions of choice.
• The retention and stability achievable with the implant overdenture may far exceed that otherwise obtained with successful conventional treatment.
• The dentist should design the overdenture to satisfy the patient’s desires and anatomical limitations predictably.

REFERENCES• Carl E. Misch. Dental implant
prosthodontics.• Babbush. Dental implants: principles
and practice • Hamid Shafie. Clinical and laboratory
manual for implant overdentures• Harold Prieskel. Overdentures made
easy• Charles M. Weiss. Principles and
Practice of Implant Dentistry. Mosby Publication.
• Mericke-Stern R, Hofman J, Wedig A, etal. In vivo measurements of maximum occlusal force and minimal pressure threshold on overdentures supported by implants or natural roots: a comparative study. Part I. Int J Oral Maxillofac Implants 1993; 8:641-649.
• Jemt T, Book K, Lindén B, Urde G. Failures and complications in 92 consesecutively inserted overdentures supported by Brånemark implants in severely resorbed edentulous maxillae: A study from prosthetic treatment to first annual check-up. Int J Oral Maxillofac Implants 1992;7:162-167.

• Burns DR, Under JW, Elswick Jr. RK, Beck DA. Prospective clinical evaluation of mandibular implant overdentures: Part I – retention, stability, and tissue response. J Prosthet Dent 1995;73:354-363.
• Burns DR, Unger JW, Elswick Jr. RK, Giglio JA. Prospective clinical evaluation of mandibular implant overdentures: Part II – patient satisfaction and preference. J Prosthet Dent 1994;73:364-369.
• Johns RB, Jemt T, Heath MR, Hutton JE, McKenna S, McNamara DC, van Steenberghe D, Taylor R, Watson RM, Herrmann I. A multicenter study of overdentures supported by Brånemark implants. Int J Oral Maxillofac Implants 1992;7:513-522.

• Cune MS, de Putter C, Hoogstraten J. Treatment outcome with implant-retained overdentures: Part I – Clinical findings and predictability of clinical treatment outcome. J Prosthet Dent 1994;72:144-151.

THANK YOU


















