
IMAGING IN NEONATAL GIT
157
Imaging in neonatal GIT S. THIYAGARAJAN
-
Upload
thiyagarajan-shanmugam -
Category
Health & Medicine
-
view
55 -
download
1
Transcript of IMAGING IN NEONATAL GIT

Imaging in neonatal GIT
S. THIYAGARAJAN

Clinical manifestation
The most common clinical findings• Inability to pass RT• Vomiting• Abdominal distension• Failure to pass
meconium/imperforate anus• AN detected

GI Causes of Vomiting
Bilious• Infant/Child
• Intussusception • Malrotation w/ volvulus • Incarcerated hernia
• Neonate • Congenital Atresia • Meconium Ileus• NEC • Hirschsprung’s
Nonbilious• Infant/Child
• Gastroenteritis• GERD• Hepatobiliary• Pancreatitis• PUD• Gastroparesis• Appendicitis
• Neonate• Pyloric Stenosis

Esophageal Atresia & Tracheoesophageal Fistula
• Developmental disorder • Fault in formation and separation
of the primitive foregut into the trachea and esophagus

TYPE A

TYPE B

TYPE C

TYPE D

TYPE E

Radiography
• Radiographic evaluation should always include the abdomen to assess the presence of air in the GI tract
• Blind pouch of the proximal esophagus that is distended with air
• Type A and B - Complete absence of gas in the stomach and intestinal tract
• Type C and D - GIT commonly appears distended with air.

• The type of esophageal atresia is confirmed by advancing a radiopaque feeding tube through the nose to the level of the atresia• The tube will curl when it approaches the blind
end• Atelectasis and pneumonia involving the
upper right lobe • Type E (H-shaped TE fistula without
atresia) - Demonstration of the fistula, which typically courses forward and upward from the esophagus

Oesophageal
atresia
Esophageal Atresia and Tracheoesophageal Fistula
• 25% associated with other GI malformations • Imperforate anus• Pyloric stenosis• Duodenal atresia• Annular pancreas• Less frequently, cardiac,
genitourinary, and vertebral alterations
Esophageal Atresia and Tracheoesophageal Fistula
• The VACTERL complex • Vertebral • Anal • Cardiac• Tracheal• Esophageal• Renal• Limb anomalies
• The best known grouping of anomalies associated with tracheoesophageal lesions
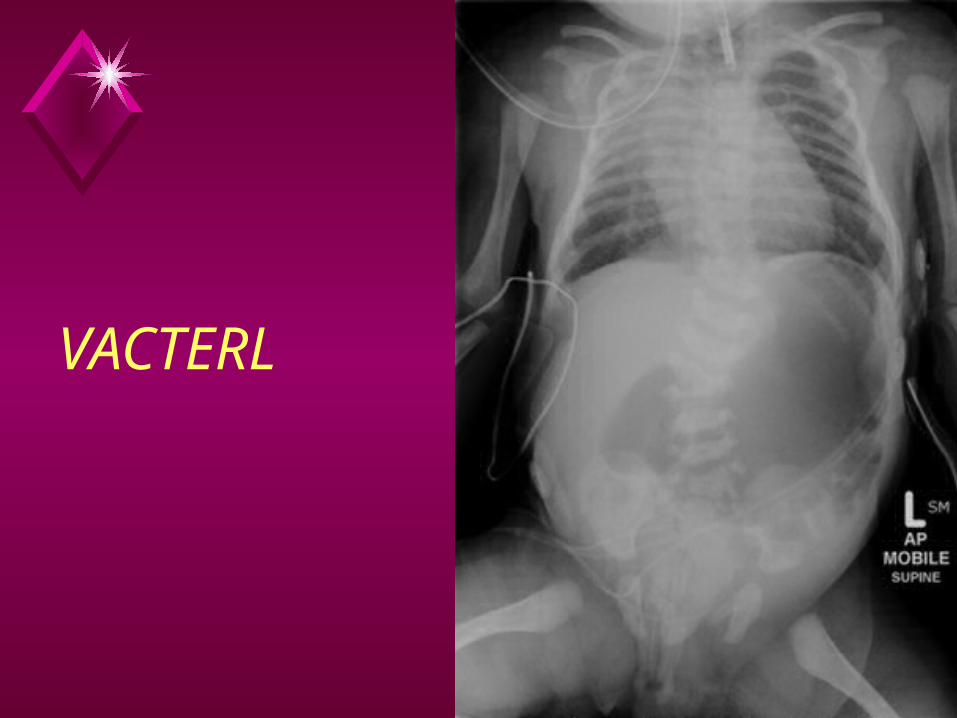
VACTERL

Oesophageal atresia with absent radius - thumb

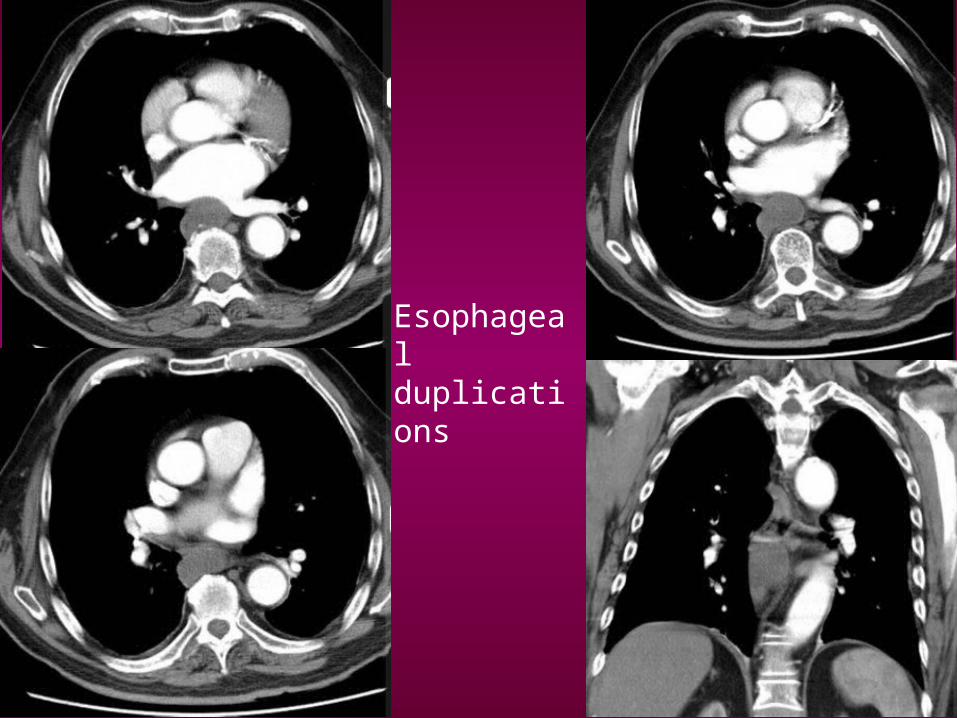
Gastrointestinal duplications
• Three defining characteristics• Have well developed coat of smooth
muscle• Epithelial lining represents some part
of the alimentary tract• Attached to some part of the
alimentary tract• Part of the spectrum of mesenteric
and omental cyst

• Can occur anywhere along the alimentary tract
• Duplication cysts are most often associated with the esophagus and jejunum/ileum

Esophageal duplications
• More often seen on the right side• More common in the lower half of
the chest• Contain gastric mucosa in 30%• Often have associated vertebral
anomalies (neurenteric cyst)
Esophageal duplications

HYPERTROPHIC PYLORIC STENOSIS
• Idiopathic thickening of pyloric muscle in infancy which creates progressive gastric outlet obstruction
• Typically seen in 2-8 week old infants with worsening projectile vomiting
• Incidence of - 2 per 1,000 live births

Radiographic Findings
• Overdistended stomach and minimal bowel gas distally
• Stomach may be collapsed if infant has recently vomited


UGI findings
• Pyloric wall thickness >10 mm• Elongation and narrowing of pyloric
canal (2-4 cm in length)• "Double / triple track sign"
• Crowding of mucosal folds in pyloric channel• "String sign"
• Passing of small barium streak through pyloric channel

• Twining recess = "diamond sign" • Transient triangular tentlike cleft / niche
in midportion of pyloric canal with apex pointing inferiorly secondary to mucosal bulging between two separated hypertrophied muscle bundles on the greater curvature side within pyloric channel
• "Pyloric teat" • Outpouching along lesser curvature due
to disruption of antral peristalsis• "Antral beaking"
• Mass impression upon antrum with streak of barium pointing toward pyloric channel

• Kirklin sign = "mushroom sign" • Indentation of base of bulb (in 50%)
• Gastric distension with fluid• Active gastric hyperperistalsis
• "Caterpillar sign"

RADIOLOGICAL SIGNS
beak
caterpillar
mush diamond
teat
track shoulder


US findings • "Target sign"
• Hypoechoic ring of hypertrophied pyloric muscle around echogenic mucosa centrally on cross-section
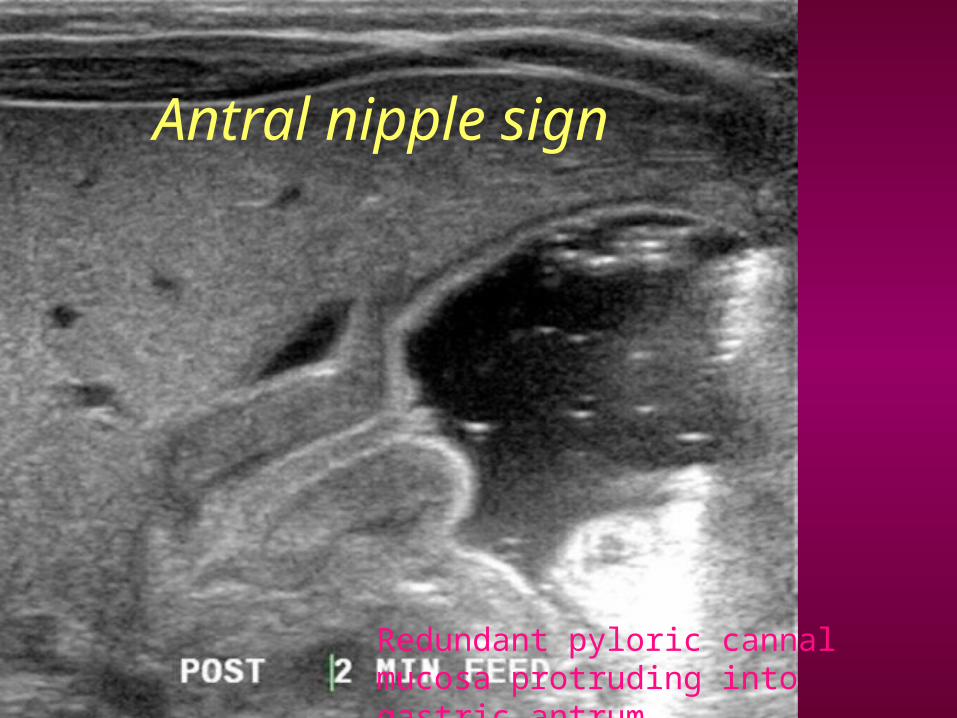
• "Cervix sign" • Indentation of muscle mass on fluid-
filled antrum on longitudinal section• "Antral nipple sign"
• Redundant pyloric channel mucosa protruding into gastric antrum

US findings
• Thickened pylorusCommonly accepted threshold values
• Single wall thickness of pylorus > 3 mm
• Pyloric channel length > 16 mm• Pyloric diameter > 7 mm
• Exaggerated peristaltic waves• Delayed gastric emptying of fluid
into duodenum• Complications: Hypochloremic metabolic
alkalosis

US findings
• Pyloric volume >1.4 cm3
[maximum pyloric diameter]2 x pyloric length
4
• Most criteria independent of contracted or relaxed state
• [Pyloric length (mm) + 3.64] x muscle thickness (mm) > 25

Pyloric stenosis


Target sign
Antral nipple sign
Redundant pyloric cannal mucosa protruding into gastric antrum

Cervix sign
Indentation of the pylorus into the fluid-filled antrum

GASTRIC VOLVULUS
• Rotation all or part of stomach > 180 degrees, ± closed-loop obstruction, possible strangulation
• It is the rotation and not the obstruction which defines the presence of volvulus

• Organoaxial volvulus: Rotation around longitudinal axis (most common)• Around line extending from cardia to pylorus• Stomach twists anteriorly or posteriorly• Antrum moves inferior to superior

• Mesenteroaxial volvulus: Rotation about mesenteric axis• Axis running across stomach right
angles to lesser & greater curves• Rotation right to left or left to right
about gastrohepatic omentum
• Mixed volvulus • Combination of
OAV & MAV
Radiography• Abdominal plain films; patient upright
• Double air-fluid level• Large, distended stomach; spheric viscus
displaced upward to left• Elevation of diaphragm• Small bowel collapsed; paucity distal gas• Intramural emphysema gastric wall
• Chest X-ray• Intrathoracic up-side down stomach• Retrocardiac fluid level
• 2 air-fluid interfaces different heights• Simultaneous fluid levels above & below
diaphragm



Fluoroscopic Findings• Massively distended stomach left upper
quadrant, may extending into chest• Inversion of stomach
• Greater curvature above lesser• Cardia & pylorus at same level• Downward pointing pylorus & duodenum
• May see "beaking" at point of twist• OAV: 2 points of twist; luminal obstruction• Contrast in stomach may not pass beyond
pylorus• MAV: Antrum & pylorus lie above gastric
fundus

Organoaxial volvulus

CT Findings
• Not generally performed for GV• CT appearance may be variable
• Depends on extent of gastric herniation, points of torsion, position of stomach
• May be linear septum within gastric lumen (area of torsion)
• Large hiatal hernia accompanied by partial GV• "Pseudothrombosis" of inferior vena
cava on CT

Mesenteroaxial gastric volvulus

DUODENUM
Duodenal Obstruction• Complete duodenal obstruction is
seen much more frequently than congenital gastric obstruction.
• Vomiting is usually delayed until after the first feeding but increases progressively thereafter

Radiographic Appearance of Duodenal Obstruction
Complete obstructionGasless abdomenGas in stomach and prox. duodenum“Double bubble”Gas distally if bifid common bile duct
Partial obstructionGastric distentionDistended small bowel“Double bubble”Scattered gas-filled bowel loops distallyNormal if vomiting decompressed stomach
and duodenum



DDX Duodenal Obstruction
• Intrinsic (Often complete obstruction)-Duodenal atresia-Duodenal stenosis-Duodenal web, diaphragm, or “wind
sock”• Extrinsic (Often partial obstruction)
-Malrotation with midgut volvulus-Malrotation with Ladd’s bands-Annular pancreas-Preduodenal portal vein-Hematoma

Duodenal atresia
• Most important cause of complete duodenal obstruction.
• Failure of recanalization of the duodenum between approximately the 9th and 11th weeks of gestation


Jejunal atresia
• Normal or near normal size colon• Seen in jejunal and proximal ileal
atresias• Colon receives succus entericus from
remaining small bowel

Jejunoilealatresia

JEJUNOILEAL ATRESIA

Ileal atresia - Contrast enema
• Microcolon (small unused colon)• The earlier in gestation the
obstruction occurs

Ileal atresia

Small Bowel Atresia Ba enema

Rotation of Gut

Abnormal Gut Rotation
• Nonrotation• When both limbs return to abdomen without further
rotation• Small bowel on right and colon on left• Wide mesentery – less risk of volvulus
• Gastroschisis; Omphalocele; Diaphragmatic Hernia
• Malrotation• Duodenojejunal limb remains in nonrotation in the
right midabdomen• Cecocolic limb in partial rotation in the midupper
abdomen fixed to abdominal wall by Ladds bands

Malrotation - Radiography
• X ray abdomen : less informative• Abnormal configuration of gas in right
hypochondrium, the duodenal triangle suggests diagnosis
• Volvulus : • Corkscrew sign• Tapering of beaking of the bowel in complete obstruction • Malrotated bowel configuration
• Distal obstruction• Closed loop syndrome features - thick walled
edematous loops with pneumatosis• Gas less abdomen due to prolonged vomiting



• Upper GI series - Modality of choice• Clearly abnormal position of
duodenum (81%)Duodenum and Jejunum to right of spineCorkscrew duodenum and jejunumDJJ low and in midline
• Unusual abnormal position of duedenum (16%)
DJJ over right pedicle DJJ left of spine but low Duodenal redundency to right of spine Z shaped configuration of duodenum &
Jejunum



USG - Midgut volvulus• Clockwise whirlpool sign• Abnormal superior mesenteric vessels
• Inverted SMA/SMV relationship• Solitary hyperdynamic pulsating SMA• Truncated SMA• Inapparent SMV
• Abnormal bowel• Dilated duodenum proximal to obstruction• Thickened wall of small bowel distal to
obstruction• Dilated fluid filled loops of small bowel
• Ascites

CT
• SMV to the left of SMA in 80%• Aplastic or hypoplastic uncinate process
of pancreas• Chylous mesentric cyst (from
interference of lymphatic drainage)• Midgut volvulus
• Whirlpool sign of twisted mesentary• Bowel obstruction• Free fluid / free gas in advanced cases

Whirlpool sign

Whirlpool sign

Angiography
• Barber pole sign – spiralling of SMA• Tapering or abrupt termination of
mesentric vessels• Mesentric vasoconstriction • Prolonged contrast transit time• Absent venous opacification• Dilated tortures superior mesentric
vein.

INTUSSUSCEPTION• Invagination of more proximal
bowel (the intussusceptum) into lumen of more distal bowel (the intussuscipiens) in a telescope-like manner
• Most common site: • Terminal ileum/ileocecal valve• 90% ileocolic

Radiography
• Soft tissue mass surrounded by a crescent of gas
• Evidence of distal small bowel obstruction • Absence of or decreased gas in the colon • Pneumoperitoneum • May be normal
• Left-side-down decubitus/prone views can be helpful in showing lack of air-filled cecum


Intussusception
• Meniscus sign Produced by the rounded apex of the intussusceptum protruding into the column of contrast
• Coiled spring appearanceEdematous mucosal folds of the returning limb of the intussusceptum are outlined by contrast material in the lumen of the colon


Intussusception

Target sign (Doughnut sign)
USG
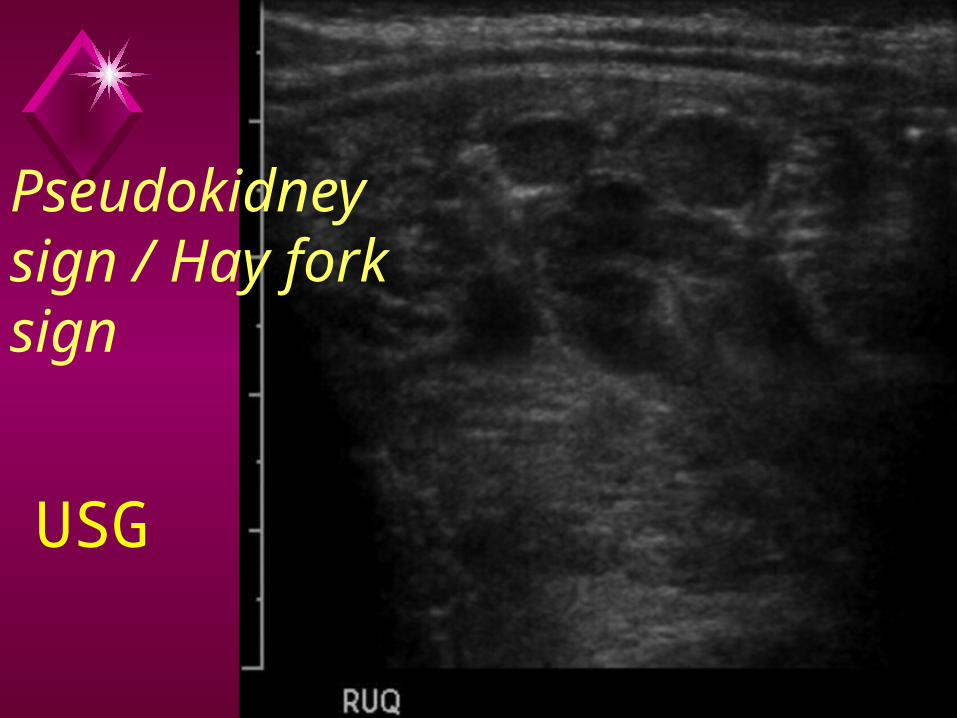
Pseudokidney sign / Hay fork sign
USG

Mesenteric vessels dragged between entering and returning wall of intussusceptum

Intussusception DIFFERENTIAL DIAGNOSIS
• Normal position of sigmoid colon• Appendicitis• Gastroenteritis• Ovarian pathology• Meckel diverticulum

MECKEL DIVERTICULUM
• Remnant of the omphalomesenteric duct• Bleeding (when contain ectopic gastric mucosa)• Intussusception • Bowel obstruction• Perforation
• Rule of 2's :• 2% Incidence of general population• 2 feet of ileocecal valve• Before age 2 years

Radiography
• Right lower quadrant mass • Displacement of bowel loops, • Obstruction• Enteroliths• May be normal

Fluoroscopic Findings
• Barium studies show indirect evidence of mass and inflammatory changes in adjacent bowel
Ultrasonographic Findings
• Heterogeneous echotexture mass in RLQ, may mimic appendicitis
• Thick walled tubular structure or hyperemic bowel loops in RLQ
• Inflamed Meckel diverticulum may present as a cyst

CT Findings
• Findings very similar to appendicitis• Thick walled blind ending structure near
cecum with surrounding inflammation• If perforated may see abscess and free air• CT is more accurate in diagnosing Meckel
diverticulum than arteriography when presenting symptom is gastrointestinal bleeding in pediatric patients

Nuclear Medicine Findings
Tc-99m pertechnetate scan• The most specific test for Meckel diverticulum
is the Tc-99m pertechnetate scan: Accuracy -90%
• Pertechnetate accumulates in mucous cells when they are in an acidic environment, in this case in ectopic gastric mucosa
• The diverticulum typically does not communicate with the bowel lumen, so the radiotracer does not appear to move downstream in bowel unless there is active bleeding


MECONIUM PLUG SYNDROME
• Small left colon syndrome.• Transient functional obstruction of
the newborn colon• Common cause of distal neonatal
bowel obstruction

Radiography
• Multiple dilated loops of bowel• Cannot differentiate dilated large
from small bowel loops in neonates• Findings nonspecific, cannot
differentiate from other causes of distal bowel

Contrast enema• R/S ratio usually> 1• Descending and sigmoid colon small in
caliber• Abrupt zone of caliber transition in region of
splenic flexure• Filling defects within colon• Ascending and transverse colon increased in
caliber• Difficult to differentiate from long segment
Hirschsprung disease• Enema often therapeutic; passage of
meconium plugs during or just after enema


Small left colon syndrome
• Functional immaturity of colon• Narrow caliber of the left colon.• Abrupt transition at the splenic
flexure. • Multiple filling defects in the left
colon are due to meconium plugs • These infants present at 1-2 days of
age with failure to pass meconium.


MECONIUM ILEUS
• Neonatal obstruction of the distal ileum due to abnormally thick, tenacious meconium
• Meconium becomes inspissated and obstructs the distal ileum and is usually a manifestation of cystic fibrosis
• Presenting illness in approximately 15% of CF patients

Radiography• Difficult to distinguish neonatal large vs.
small bowel• Uncomplicated Type
• Multiple dilated bowel loops• Bubbly lucencies right lower quadrant • Few air-fluid levels (sticky meconium)
• Complicated Type• Soft tissue mass or gas less abdomen• ± Intrauterine perforation and peritonitis• Curvilinear calcifications on peritoneal surface or
lining pseudocyst

“Bubbly" appearance of the distended intestinal loops

Contrast enema
• Smallest of microcolons• Reflux contrast into terminal ileum• Meconium pellets in terminal
ileum; not much in colon• Can be therapeutic in
uncomplicated type

Meconium ileus

MECONIUM PERITONITIS
• Chemical peritonitis from in utero bowel perforation and peritoneal leakage of sterile meconium
• At least four types are recognised:• Fibro-adhesive • Cystic • Generalised• Healed

Meconium peritonitis
Soft tissue mass, punctate or curvilinear calcifications, ascites, dilated bowel loops


Meconium peritonitis

AN - USG• Highly echogenic linear or clumped foci
(calcifcation )• Snowstorm appearance • Abdominal circumference may be
increased• Associated anomalies such as
dilated fetal bowel and/or meconium pseudocysts
• Meconium pseudocyst: Heterogeneous mass with calcified wall
• Fetal ascites and/or polyhydramnios

NECROTIZING ENTEROCOLITIS
• Idiopathic enterocolitis • VLBW premature infants • Combination of infection and
ischemia characterized by coagulative and hemorrhagic necrosis
• Inflammation of portions of the small and large intestine

Location
• Most common right colon and terminal ileum
• Can occur anywhere in gastrointestinal tract

Radiography• Findings range from normal to
suggestive to diagnostic• Normal• Suggestive findings
• Asymmetric bowel dilation• Featureless "unfolded" bowel loops• Separation of bowel loops• Fixed configuration of bowel loops over
serial films

Necrotising enterocolitis

Definitive finding: Pneumatosis
Bubble-like (submucosal) or curvilinear (serosal) lucencies

Pneumatosis intestinalis (intramural gas)

Portal venous gas
Definitive finding: Portal venous gas
Branching lucencies over the liver

The football sign / air dome sign
• Right upper quadrant gas
• Rigler’s (double wall) sign
• Ligament visualization
• Inverted V sign• Triangular air• The cupola sign• Football or air dome• Scrotal air
Definitive finding: Free intraperitoneal air

Bell classification
• Stage I: Early or suspected NEC• Nonspecific• Scalloping/separation/unfolding bowel loops• Asymmetric bowel distention
• Stage II: Definite NEC• Pneumatosis intestinalis: Mucosal, serosal; not always
correlating with clinical symptoms/signs• Stage III:
• Advanced disease (perforation or impending perforation)
• PVG, free intraperitoneal air, persistent loop sign, ascites

Fluoroscopic Findings
• Enema contraindicated in presumed acute NEC
• Mucosa permeable to water-soluble contrast and excreted into kidneys
• Stricture: • Single or multiple• Small bowel or colon• Chronic complication of NEC

Ultrasonographic Findings
• Thickened bowel wall loops• Increased (inflamed) or decreased
(infarcted) vascularity• Ascites

Differential diagnosis
• In the correct clinical scenario the presence of gas within bowel wall has little differential. • Pneumatosis coli• Neonatal appendicitis• Meconium ileus• Hirschsprung disease• Infectious enterocolitis

HIRSCHSPRUNG DISEASE
• Functional obstruction of the bowel due to lack of intrinsic enteric ganglion cells
• Morphology• Denervated colon is small, narrow,
spasmodic• Innervated more proximal bowel is dilated• Affected portion always includes the anus
and variable length of Rectum• Continuous disease• No proximal without distal involvement

• Short segment disease : ~ 75% * • Rectal and distal sigmoid colonic involvement
only • Long segment : ~ 15%
• Typically extends to splenic flexure / transverse colon
• Total colonic aganglionosis : 2 - 13% • Zuezler-Wilson syndrome• Occasional extension of aganglionosis into small
bowel • Ultrashort segment disease
• 3 – 4 cm of internal anal sphincter only• Controversial entity

Associations
• Isolated abnormality in 70% of cases• Down syndrome : in ~ 10%• Neurocristopathy syndromes
• Waardenburg-Shah syndrome• Haddad syndrome• MEN IIa
• other non-neurocristopathy syndromes • Aarskog syndrome• Bardet-Biedl syndrome• Fryns syndrome• Pallister-Hall syndrome• Smith-Lemli-Opitz syndrome

Radiography
• Multiple loops of dilated bowel
• Paucity of gas in the rectum

Contrast enema
• Rectum smaller than sigmoid (R/S ratio < 1)• Transition zone from abnormally small distal to
dilated proximal colon• Fasciculations or sawtooth appearance of
mucosa of involved colon: Spasm• Thickened, ulcerated colon in patients with
associated colitis• Microcolon: Total colonic disease



Differential diagnosis
• Functional megarectum• Necrotising enterocolitis• Microcolon : appears similar to
long segment / whole colon Hirschsprung disease

Megacystis-microcolon-intestinal hypoperistalsis syndrome
• The duodenum and proximal jejunum are mildly dilated.
• Small bowel is dilated and shortened, and the colon is a microcolon
• Abundance of ganglion cells in the entire gastrointestinal tract.
• Megacystis and megaureters


ANORECTAL MALFORMATION
• Abnormal separation of genitourinary system from hindgut
• Spectrum; true imperforate anus (thin membrane) to atresia distal rectum
• Classification controversial • Anatomic: Relation of rectal pouch to
pubococcygeal line • Surgical: Prognostic and therapeutic,
"Pena“ classification

• Low• Usually visible perineal orifice; stenotic or
membrane• No GU tract communication
• Intermediate• Usually features of high lesion
• High• Usually rectourinary fistula in males• Usually rectovaginal or vestibular in females• Possible vaginal, uterine, or bladder anomalies

PUBOCOCCYGEAL LINE:
• Line is drawn between upper and middle third of pubis to lower border of S5
• Bowel ends just above this line are termed high malformation and below one is termed low malformation.
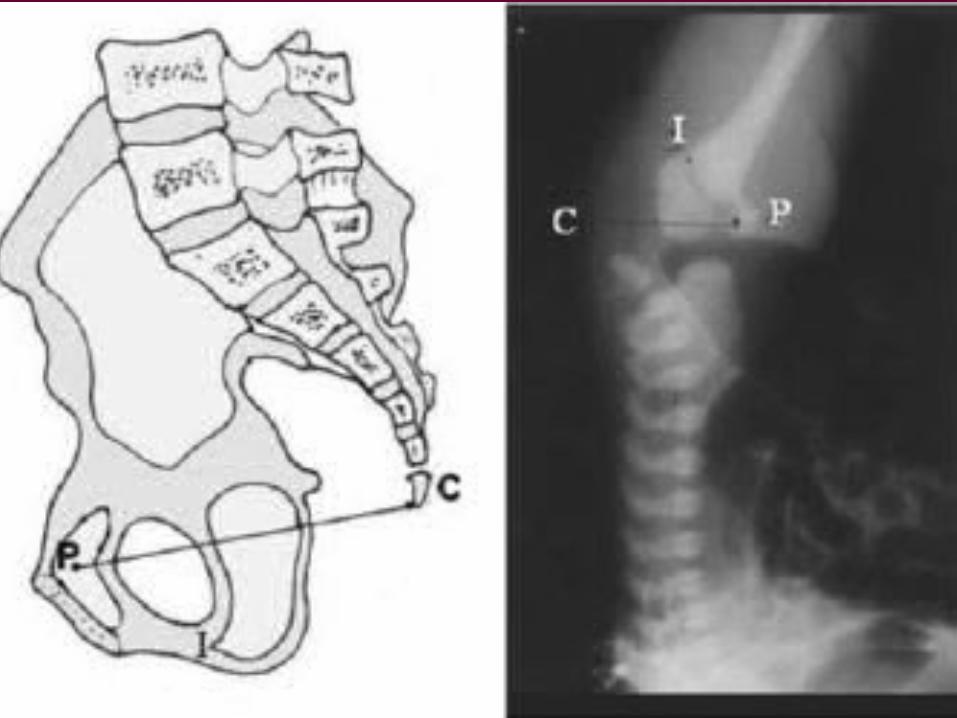

ISCHIAL LINE
• Line drawn below parallel to the pubococcygeal line at the level of the ossified ischial bone
• Corresponds to the most proximal level of bulbous urethra
• Anomalies between this two lines are termed intermediate
• If fistulas occur, they open in the bulbous urethra in male or in to vestibule or lower part of vagina in the female.

PIT LINE
• This line is parellal to the ischial line but one to two centimetre caudal to it.
• This marks the posteroinferior part of the bulbocavernous muscle.
• If bowel gas ended below this area Called imperforate anal membrane or low ARM

Radiography• Distal bowel obstruction, intraluminal
calcification• ± Gas in bladder in males, vagina in
females• Air in rectal pouch on prone cross table
lateral view: Inaccurate for level• Bony landmark PCL• "M" line: Horizontal to pelvis divides lower
1/3, upper 2/3 ischium• Low lesions appear high: Meconium-packed
pouch• High lesions appear low: Straining, crying,
excessive distention pouch

ARM

Voiding Cystourethrogram
• Catheter into cloaca (single perineal orifice)• Enters bladder, vagina, or colon
• Bladder findings• Normal; vesicoureteral reflux (VUR); wall-
thickening; neurogenic bladder; fistula to rectum• Urethral findings
• Opens to cloaca, fistula from rectum to posterior> bulbous> penile urethra
• Vaginal findings• Normal; rectovaginal fistula; congenital anomalies
(septate, duplicated, etc.)
High pressure distalcolostography
• Several months after colostomy prior to repair
• Key view is lateral• Document connection to urethra,
bladder, or vagina

Ultrasound
• Hypoechoic rectal pouch-perineal distance• < 10 mm: Low lesion;• > 10-15 mm - high or intermediate
• Reliability similar to radiography with similar inaccuracies

MR Findings
• Pelvic musculature, neorectum, and anal sphincter position/integrity• Normal to absent levator muscle• Normal to absent anal sphincter complex
• Muscle complex malpositioned or atrophic
• Spine• Tethered cord, spinal dysraphism, sacral
agenesis

Urinary tract anomalies associated with ARM • Renal agenesis• Renal ectopia• Megaureter• HN (PUJ obstruction)• VUR• PUV• Epispadias/Hypo• Prune belly syn• VATER anomaly

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…

To summarize…


Announcement!!!
GUEST LECTUREOn
VASCULAR INTERVENTIONBy
Dr. A.L. Periyakaruppan, M.D.R.D.,D.M.
Consultant Radiologist,Apollo hospitals, Madurai.
Date: 12.11.2011,Saturday


















