IC67-R: Understanding Pediatric Elbow Fractures to ...
75
All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain. IC67-R: Understanding Pediatric Elbow Fractures to Maximize Outcomes Moderator(s): Joshua M. Abzug, MD Faculty: Andrea S. Bauer, MD, Scott H. Kozin, MD, and Francisco Soldado, MD, PhD Session Handouts 75TH VIRTUAL ANNUAL MEETING OF THE ASSH OCTOBER 1-3, 2020 822 West Washington Blvd Chicago, IL 60607 Phone: (312) 880-1900 Web: www.assh.org Email: [email protected]
Transcript of IC67-R: Understanding Pediatric Elbow Fractures to ...

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
IC67-R: Understanding Pediatric Elbow
Fractures to Maximize Outcomes
Moderator(s): Joshua M. Abzug, MD
Faculty: Andrea S. Bauer, MD, Scott H. Kozin, MD, and Francisco Soldado, MD, PhD
Session Handouts
75TH VIRTUAL ANNUAL MEETING OF THE ASSH
OCTOBER 1-3, 2020
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

7/23/2020
1
IC67-R: Understanding Pediatric Elbow Fractures to Maximize Outcomes
Moderator: Joshua M. Abzug, MD
Faculty: Andrea S. Bauer, MD, Scott H. Kozin, MD, Francisco Soldado, MD, PhD
Joshua M. Abzug, MD
Speaker has no relevant financial relationships with commercial interest to disclose.
Understanding Pediatric Elbow Fractures to Maximize Outcomes: Supracondylar
Fractures
Joshua M. Abzug, [email protected]
1
2
3

7/23/2020
2
Supracondylar Humerus Fractures
Most common pediatric elbow fracture
79% of elbow fractures
3.3% of all pediatric fxs
Epidemiology
5-7 years of age
Males = Females
Non-dominant side (left)
Physical Exam
Observation
Skin puckering, ecchymosis, open wounds, vascular status of hand
Palpation
Specific areas about the elbow
Remainder of upper extremity
Physical Exam
Neurovascular exam
Assess AIN, Median nerve, Radial nerve, Ulnar nerve
Assess Radial artery
4
5
6
7/23/2020
3
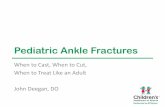
X-rays
Assess for posterior fat pad sign
Assess anterior humeral line
Gartland Classification
I Non‐displaced
II Hinged
A: No rotational deformity
B: Rotational deformity
III Completely displaced
(Most common posteromedial 75%)
Gartland Classification
IV Multidirectional
Unstable in both flexion and extension because of complete loss of a periosteal hinge
•May be due to initial injury or repeated attempts at closed reduction
–Leitch et al.
7
8
9

7/23/2020
4
Treatment
Type I Long arm cast x 3 weeks
Type IIA Long arm cast vs. CRPP
Type IIB CRPP
Type III CRPP
Type IV CRPP
Easiest to use 2 fluoro machines
Preplace pins in distal fragment
TimingIdeal start time
6:30 AM trauma room
Bump first case
How long is too long?
Mehlman
• 8 Hours
Gupta
• 12 Hours
Bales
• 19 Hours
Leet
• 21 Hours
Not All Supracondylar Fractures are Created Equal
10
11
12

7/23/2020
5
The Fine Print
Mehlman, JBJS, 2001
Excluded open and pulseless fractures
The Fine Print
Gupta, et al, JPO, 2004
Excludes vascular injury, ipsilateral fracture and open fracture
My Practice
Emergency room
Orthopedic surgeon/resident evaluation
• Skin
• Neurovascular exam
• Splint– Gentle flexion
• Non-sedating pain medication
13
14
15

7/23/2020
6
Inpatient Management
Nursing
Elevation of limb
Q3-4 hr. NV checks
Increasing pain • CALL Orthopedic
surgeon/resident
• The A’s not the P’s– Anxiety
– Agitation
– Analgesia
Emergency SurgeryIndications
Dysvascular extremity
• Pulseless perfused hand
Open fracture
Skin tenting
“Floating Elbow”
Abnormal neuro exam
• Median nerve neuropraxia
Skin puckering
Significant swelling/ecchymosis
OR Set-up
16
17
18

7/23/2020
7
Reduction
Obtain length before flexing
GENTLE flexion maneuver
Appreciate rotational abnormality
Flexion supracondylar pinned in extension
Milking Maneuver and Reduction
Fluoroscopic views
Jones view (AP)
Lateral view• Externally rotate shoulder
19
20
21

7/23/2020
8
Acceptable Reduction
< 50% translationNo varus
No extension
Pin Size
Remember big pins for big people and big pins for little people
Usually 0.062” or 2.0 mm
Pin Configuration
Lateral entry pins
Type II = 2 pins
Type III = 3 pins
• Check the stability of fixation by stressing the fracture under live fluoroscopy
22
23
24

7/23/2020
9
Optimum Pin Configuration
Medial pin
Lateral pins = crossed pins
Skaggs, JBJS, 2001
Kocher, JBJS, 2007
Medial pin
10% ulnar nerve injury• Extend elbow
Cutdown to epicondyle
Poor Pin Configuration
Failure to engage both fragments with at least two pins
25
26
27
7/23/2020
10
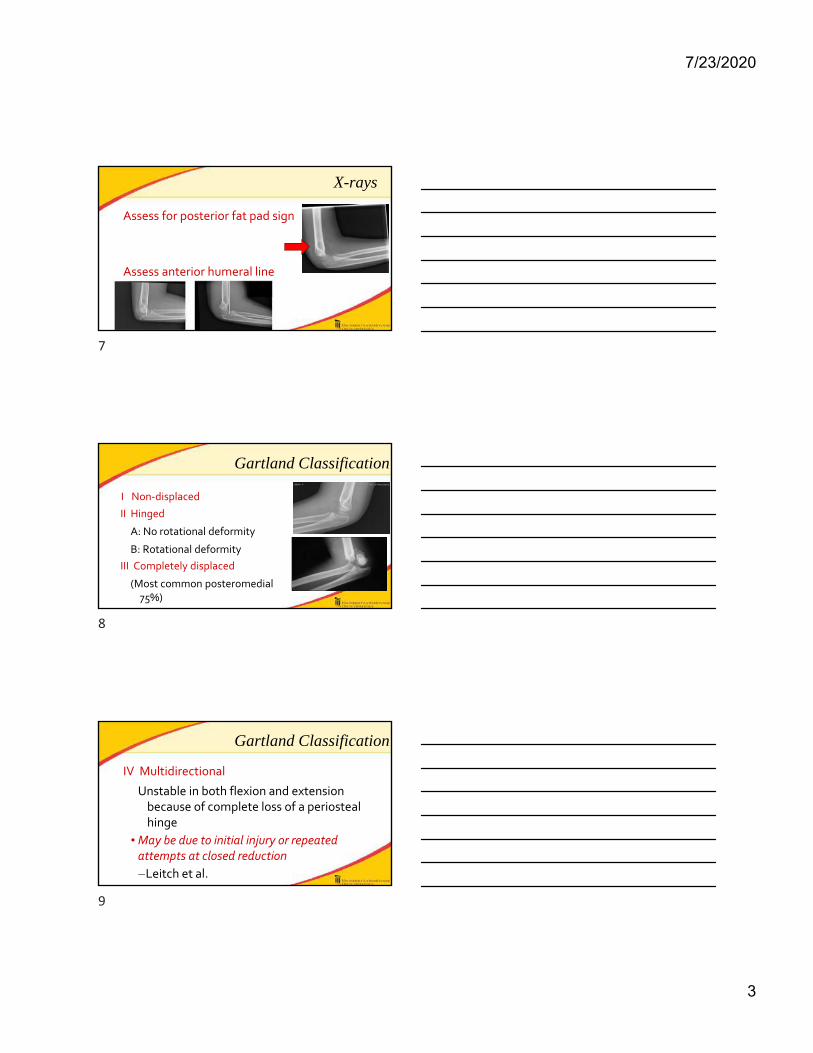
Poor Pin Configuration
Failure to achieve bicortical fixation with at least two pins
Poor Pin Configuration
Failure to achieve ≥2 mm of pin separation at the fracture site (pins cross at fracture site)
Final Check
LIVE Fluoro
28
29
30

7/23/2020
11
Post-Operative Care
Splint at 70-80° flexion
Tylenol for pain
Home next day
Follow-up
1 week for x-ray
3 weeks for x-ray and pins out
Special Situations
Floating elbow
Fix both
Skin pucker
“Milk” muscles before reducing
Open Reduction
Irreducible closed
Dysvascular hand after CRPP
Open fracture
31
32
33

7/23/2020
12
Pulseless Supracondylar Fracture
No arteriogram
Vascular injury at end of proximal fragment
Algorithm
1. CRPP
2. Reassess vascular status
• Observe “pink, pulseless” hand
3. Open exploration of brachial artery
• Dysvascular hand
• Prophylactic forearm and hand fasciotomies with prolonged ischemia
Supracondylar Fractures
4.2% complication rate
Pin Migration
1.8%
Most common complication
Can require an unanticipated return to the OR
34
35
36

7/23/2020
13
Infection
<1%
Majority are superficial
Semi‐sterile technique is safe
Treat early to avoid septic arthritis
Cubitus Varus
Cubitus varus
Occurs with casting or pinning
Due to inadequate fracture reduction
• Omid et al. JBJS 2008
Typically painless
Good elbow motion maintained
37
38
39

7/23/2020
14
Cubitus varus
Problem
Cosmesis
Repeat fractures
• Lateral condyle
– Takahara et al. JBJS BR 1998
Snapping medial triceps tendon
• Spinner et al. JHS 1999
Cubitus varus
Problem
Tardy posterolateralelbow instability
• Presents 2‐3 decades later
• Lateral elbow pain and recurrent instability
– O’Driscoll et al. JBJS 2001
Cubitus varus - PLRI
Cubitus varusmedial displacement of mechanical axis altered vector of triceps pull
Repetitive external rotation torque applied to ulna attentuation LCL PLRI
Fig. 3
Varu
torq
exte
from
the
O’Driscoll et al. JBJS 2001
40
41
42

7/23/2020
15
Cubitus Varus - Treatment
Osteotomy
Lateral closing wedge
• No sagittal deformity
Biplanar
• Coronal and sagittal deformity
Biplanar Osteotomy
Follow-up
43
44
45
7/23/2020
16
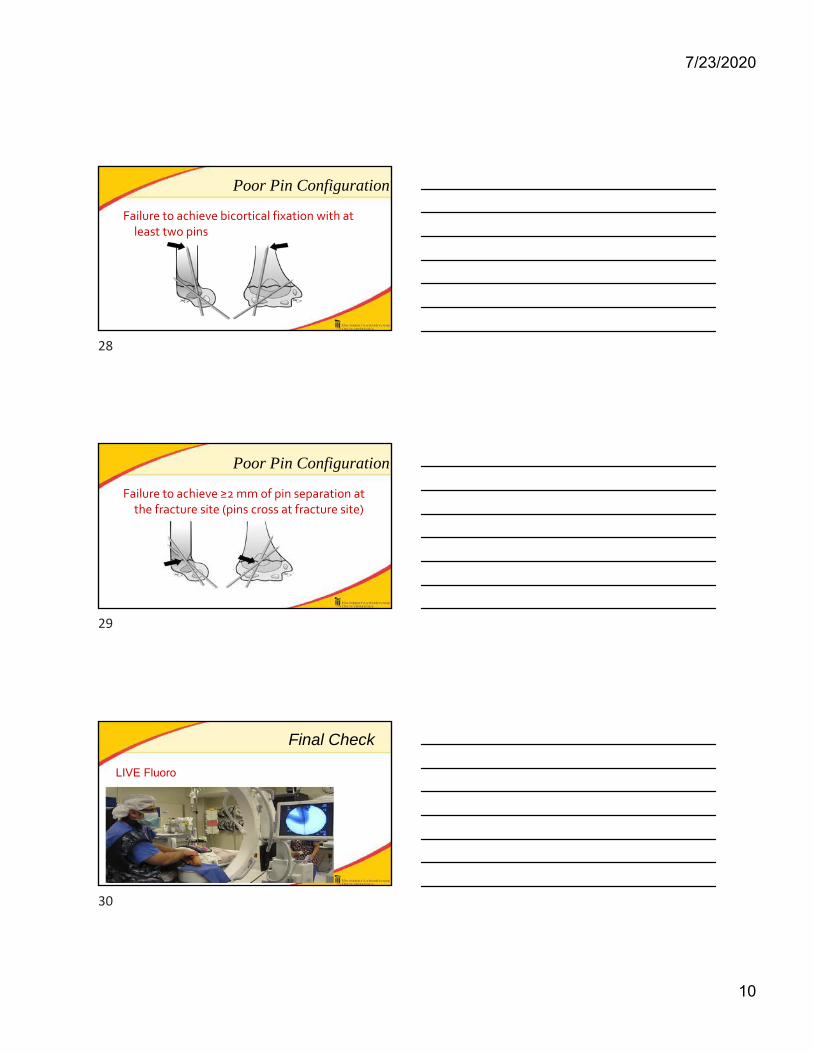
Cubitus varus - Treatment
Osteotomy
Dome
Kim HT, Lee JS, Yoo CI. JBJS 2005
Step‐cut
Cubitus varus - Treatment
Preferred technique – Lateral closing wedge osteotomy
Technically straightforward
Union is reliable
Lateral prominence is asymptomatic and unrecognized
Lower complication rate
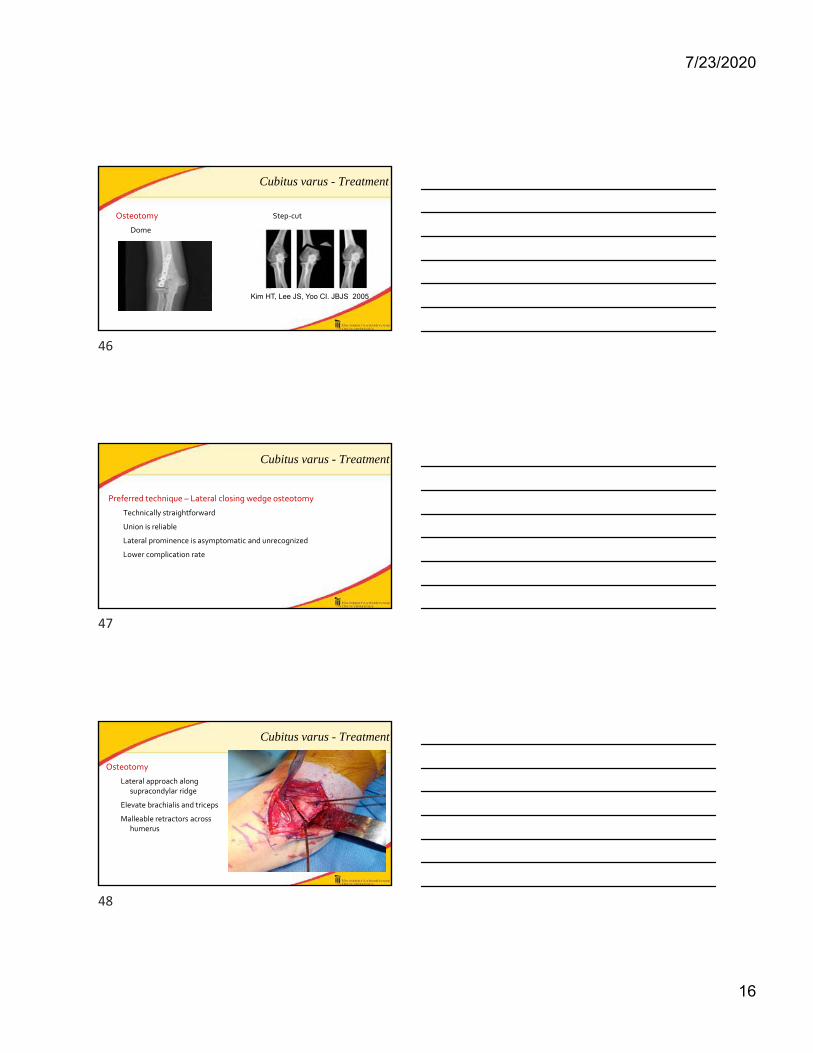
Cubitus varus - Treatment
Osteotomy
Lateral approach along supracondylar ridge
Elevate brachialis and triceps
Malleable retractors across humerus
46
47
48
7/23/2020
17
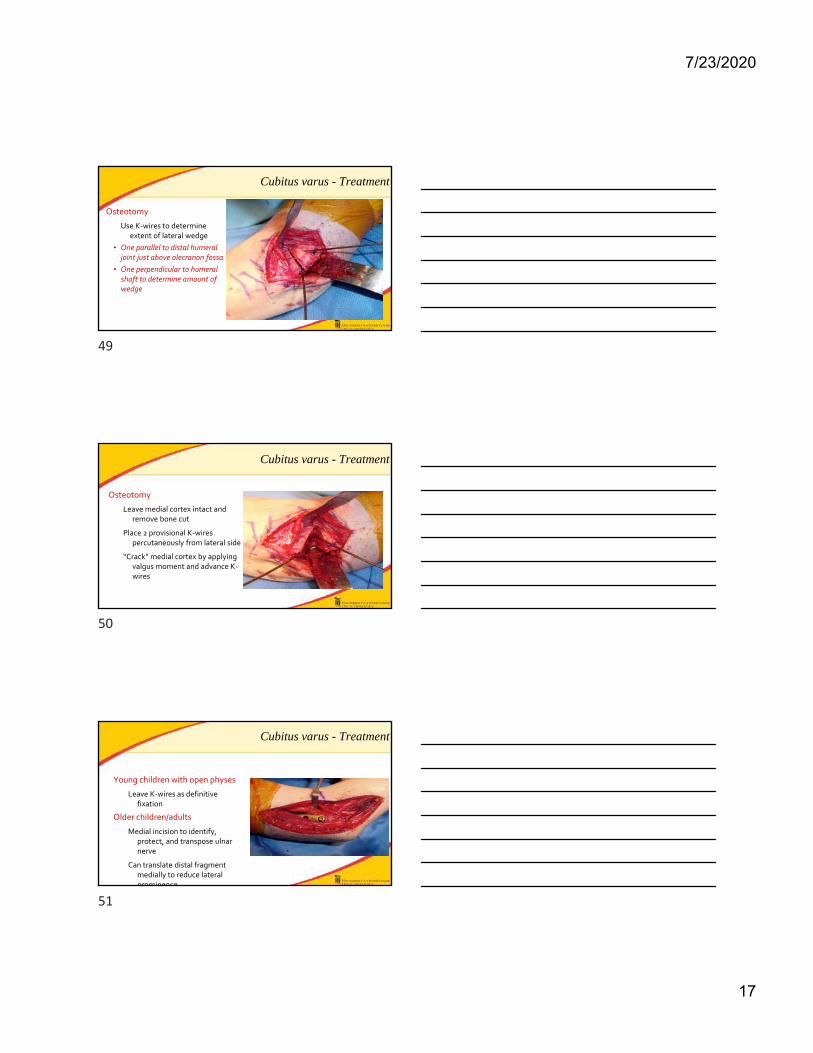
Cubitus varus - Treatment
Osteotomy
Use K‐wires to determine extent of lateral wedge
• One parallel to distal humeral joint just above olecranon fossa
• One perpendicular to humeral shaft to determine amount of wedge
Cubitus varus - Treatment
Osteotomy
Leave medial cortex intact and remove bone cut
Place 2 provisional K‐wires percutaneously from lateral side
“Crack” medial cortex by applying valgus moment and advance K‐wires
Cubitus varus - Treatment
Young children with open physes
Leave K‐wires as definitive fixation
Older children/adults
Medial incision to identify, protect, and transpose ulnar nerve
Can translate distal fragment medially to reduce lateral prominence
49
50
51

7/23/2020
18
Compartment Syndrome
Compartment Syndromes at Boston Children’s Hospital 1992-1997- 33 children
Bae et al, Journal of Pediatric Orthopedics 2001; 21:680-688
Diagnosis
23 compartment syndromes diagnosed on admission
10 diagnosed while in house
3 fractures s/p fixation
3 elective osteotomies
4 non-displaced fractures or soft tissue injuries
52
53
54
7/23/2020
19
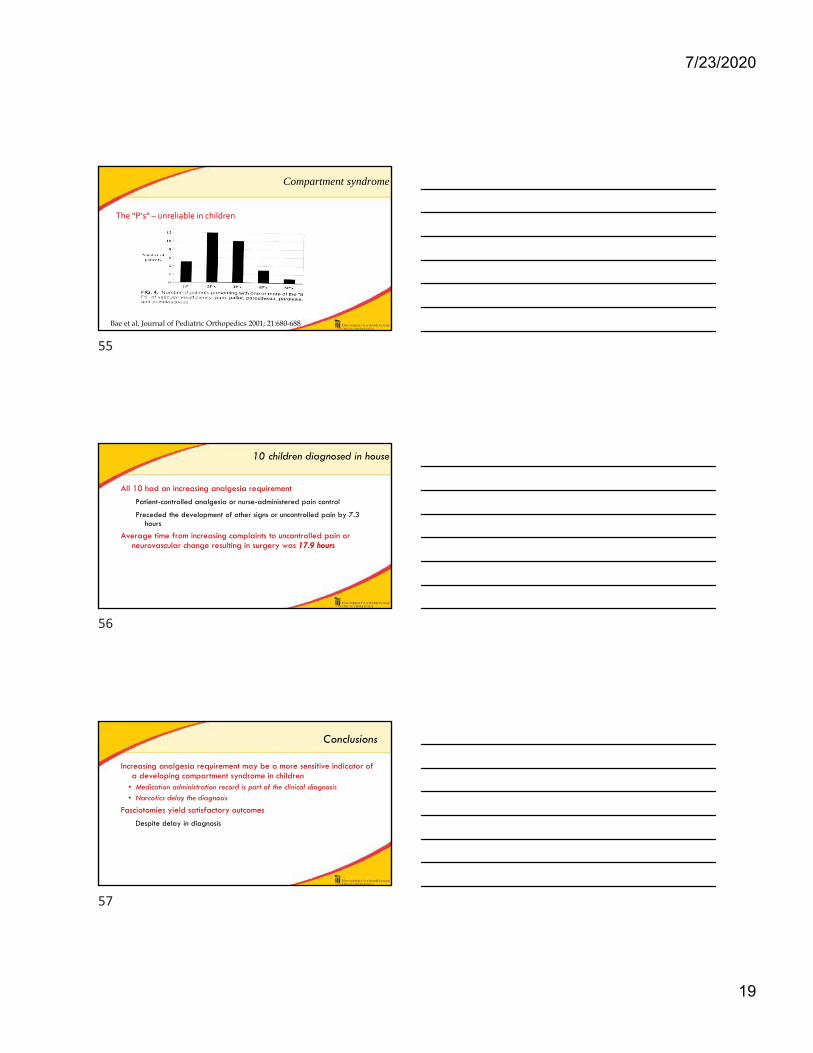
Compartment syndrome
The “P’s” – unreliable in children
Bae et al, Journal of Pediatric Orthopedics 2001; 21:680-688
10 children diagnosed in house
All 10 had an increasing analgesia requirement
Patient-controlled analgesia or nurse-administered pain control
Preceded the development of other signs or uncontrolled pain by 7.3 hours
Average time from increasing complaints to uncontrolled pain or neurovascular change resulting in surgery was 17.9 hours
Conclusions
Increasing analgesia requirement may be a more sensitive indicator of a developing compartment syndrome in children
• Medication administration record is part of the clinical diagnosis• Narcotics delay the diagnosis
Fasciotomies yield satisfactory outcomes
Despite delay in diagnosis
55
56
57
7/23/2020
20
Compartment Syndrome
The “A’s”
Anxiety
Agitation
Analgesia
Give non‐narcotic/ non‐sedating low‐dose medications
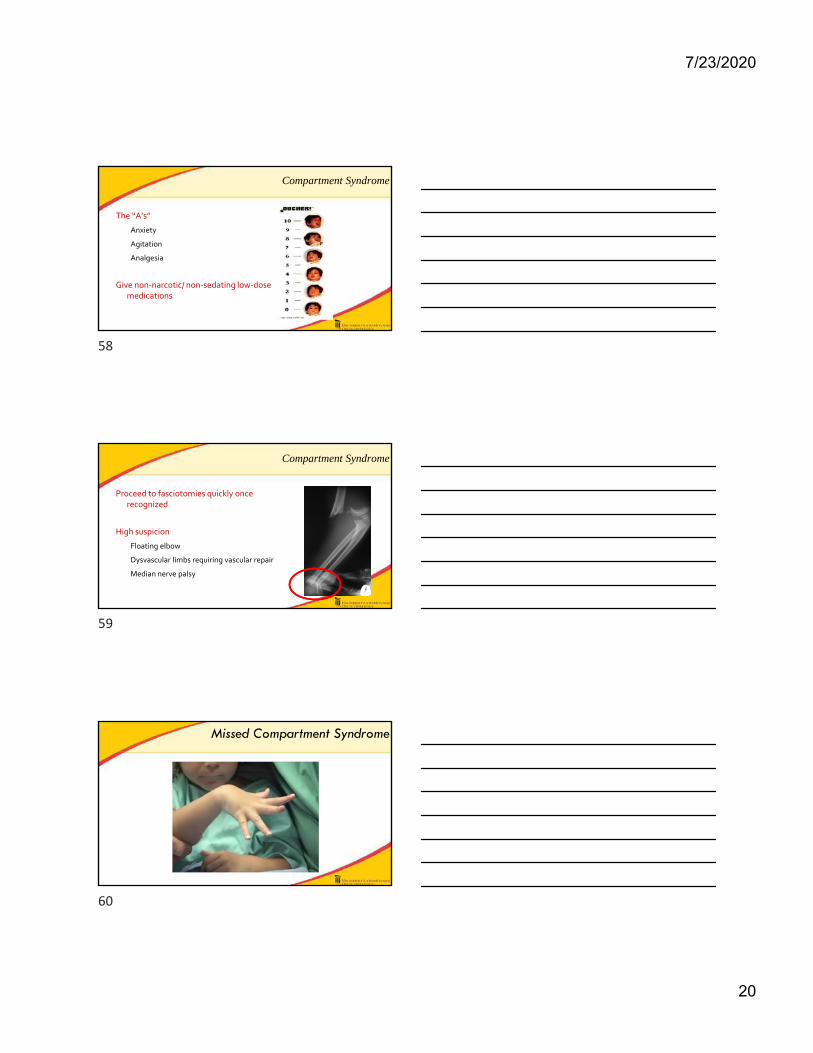
Compartment Syndrome
Proceed to fasciotomies quickly once recognized
High suspicion
Floating elbow
Dysvascular limbs requiring vascular repair
Median nerve palsy
Missed Compartment Syndrome
58
59
60

7/23/2020
21
Pre-Operative
Flexor Slide
Flexor Slide
Ulna
BrachialisBiceps Tendon
RadiusAIN FDP/FDS
61
62
63

7/23/2020
22
Flexor Slide
UlnaIOM
PQAIN/AIA
Intra Op
Post-op
64
65
66

7/23/2020
23
Compartment Syndrome - Pitfalls
Increasing analgesia requirements
Failure to recognize
Compartment Syndrome
My protocol
Admit for 24 hours
• 48 hours if neurovascular injury
Tylenol for pain
Q3‐4 neurovascular checks
Loss of reduction
67
68
69
7/23/2020
24
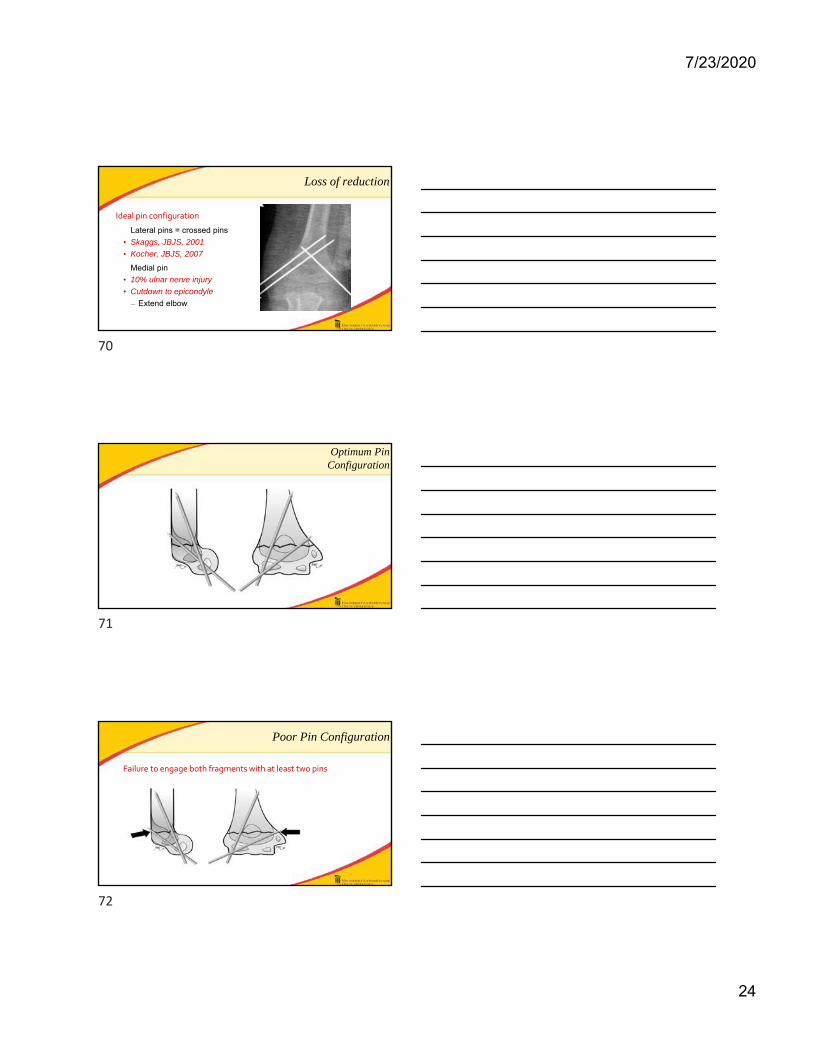
Loss of reduction
Ideal pin configuration
Lateral pins = crossed pins
• Skaggs, JBJS, 2001
• Kocher, JBJS, 2007
Medial pin
• 10% ulnar nerve injury
• Cutdown to epicondyle
– Extend elbow
Optimum Pin Configuration
Poor Pin Configuration
Failure to engage both fragments with at least two pins
70
71
72

7/23/2020
25
Poor Pin Configuration
Failure to achieve bicortical fixation with at least two pins
Poor Pin Configuration
Failure to achieve ≥2 mm of pin separation at the fracture site (pins cross at fracture site)
Loss of reduction - Pearls
Live fluoroscopy
Use 3 pins
Appropriate configuration
Open placement of medial pin
Avoid ulnar nerve injury
73
74
75

7/23/2020
26
Nerve Injury
Nerve Injury
11% overall rate
Extension type
AIN Median Radial Ulnar
Flexion type
Ulnar most common
Nerve Injury - Pearls
Obtain thorough pre and post‐operative neurological exams
Obtain exam by proxy or through repeat exams
76
77
78
7/23/2020
27
Nerve Injury - Pearls
Cut down to epicondyle to place medial pin
Recognize “rubbery” feeling during reduction
Pitfalls
Failure to obtain a pre‐operative exam
4 yo female
Nerve Injury -Pitfalls
ED Physician
79
80
81

7/23/2020
28
Nerve Injury -Pitfalls
Attending post‐op note
Thanks!!!
82
83

7/26/2020
1
Francisco Soldado, MD, PhD
Speaker has no relevant financial relationships with commercial interest to disclose.
F SoldadoPediatric Upper Extremity and Microsurgery
[email protected]+34 688999890Barcelona, Spain
Humeral Lateral Condyle Fractures
10–15 % pediatric elbow fractures. Second most common elbow Fx (Landin JPO B 1992)
Epidemiology
1
2
3

7/26/2020
2
Problems
Articular injury : Loss of motion
Fragment Instability: Nonunion
Terminal vascularization: Osteonecrosis
Milch (J Traum 1964)
Type I Transcapitelum Type II Transtrochlea
Jakob (JBJS Br 1954)
Type INon‐displaced (Hinged)
Type IIDisplaced
Type IIIRotated
Classification and Radiology
4
5
6
7/26/2020
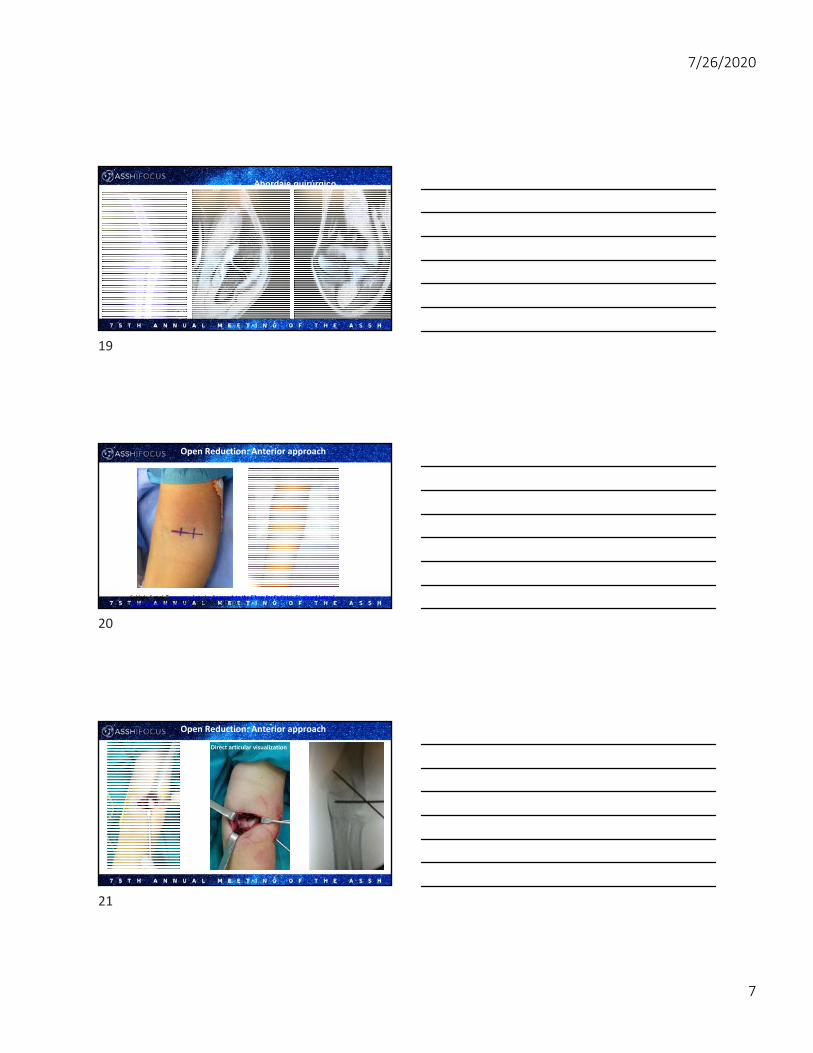
3
Amount of displacement (mm)
Internal oblique x-ray view
Classification and Radiology
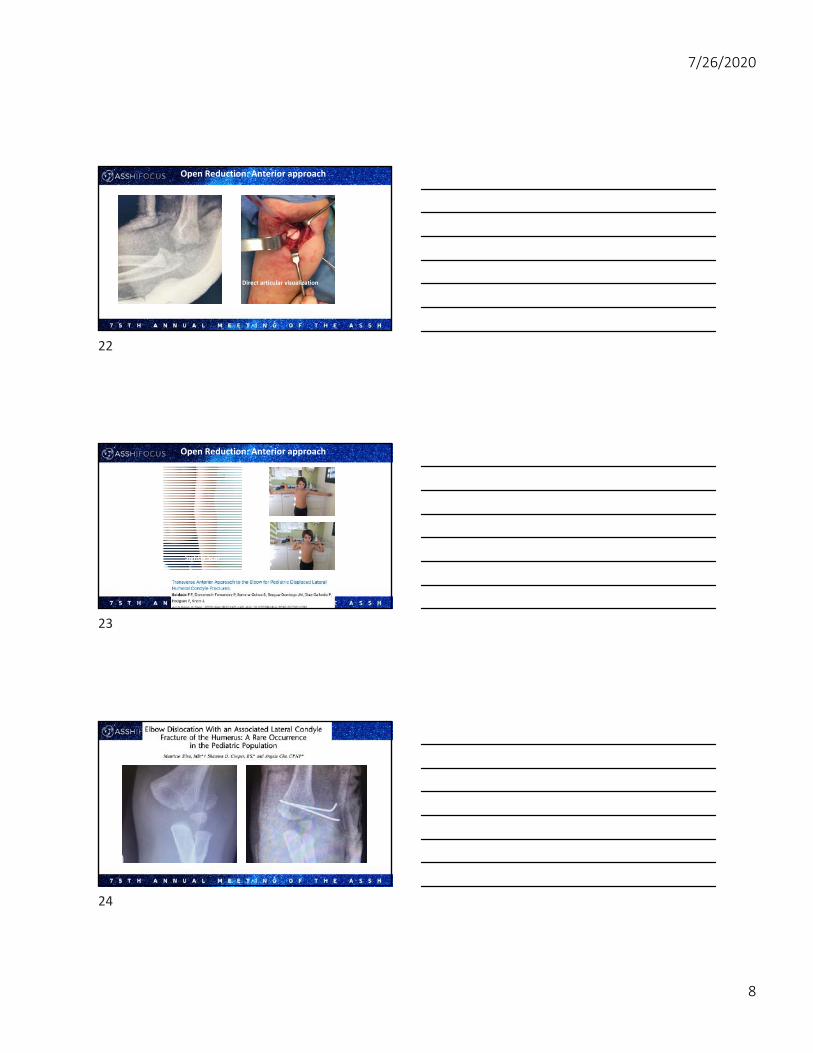
6%
Treatment: Minimally displaced <2mm (Flynn JBJS Am 1975)
Weekly follow-up possible: Long arm cast (supination, wrist extension)
Weekly follow-up not possible: Percutaneous pinning
‐
7
8
9

7/26/2020
4
Mechanical factor: Extensor-supinator mass
3-4mm 13% risk of nonunion (Flynn JBJS 75)
Instability: Risk Nonunion
Closed reduction (Song JBJS Am 2008):Elbow varus Forearm supination KW joystick
Treatment: Displaced >2mm
Residual displacement <2mm: Percutaneous pinning
Residual displacement >2mm: ORIF
Arthrogram (Arthroscopy)
10
11
12

7/26/2020
5
Arthrogram (Arthroscopy)
Disrupted capsule
KW configuration
13
14
15

7/26/2020
6
KW configuration
Compression by cannulated screws might decrease need for ORIF (Stein JPO 2015)‐
Treatment
Open Reduction: Lateral approach
Difficult articular visualization Unsightly Scar
16
17
18
7/26/2020
7
Abordaje quirúrgico
Open Reduction: Anterior approach
Soldado F et al. Transverse Anterior Approach to the Elbow for Pediatric Displaced Lateral Humeral Condyle Fractures . 2020: 8(2)‐142‐146
Open Reduction: Anterior approach
Direct articular visualization
19
20
21
7/26/2020
8
Open Reduction: Anterior approach
Direct articular visualization
Sightly Scar
Open Reduction: Anterior approach
22
23
24

7/26/2020
9
-70%-Correlation initial displacement -Does not influence final outcome
Lateral spurring
Minor 8%: Pin tract infection, granuloma, Keloid
Major 6%: Malunion 3%, osteonecrosis 0.6%, nonunion 0.6%, stiffness 0.6%
Complications (Weiss JPO 2009)
Nonunion
25
26
27

7/26/2020
10
Late diagnosisSafe to operate up to 2 weeks
Nonunion: Vascularized humeral periosteal flap
3s 6s 4m
28
29
30

7/26/2020
11
Dome osteotomyVascularized periosteal flap
31
32
33

7/26/2020
12
To Maximize Outcomes:
To Stay To Maximize Outcomes:
Internal Oblique Rx
34
35
36

7/26/2020
13
To Maximize Outcomes:
Pin minimally displaced LCF if follow‐up not possible
To Maximize Outcomes:
Arthrogram
To To Maximize Outcomes:
Divergent pins
37
38
39
7/26/2020
14
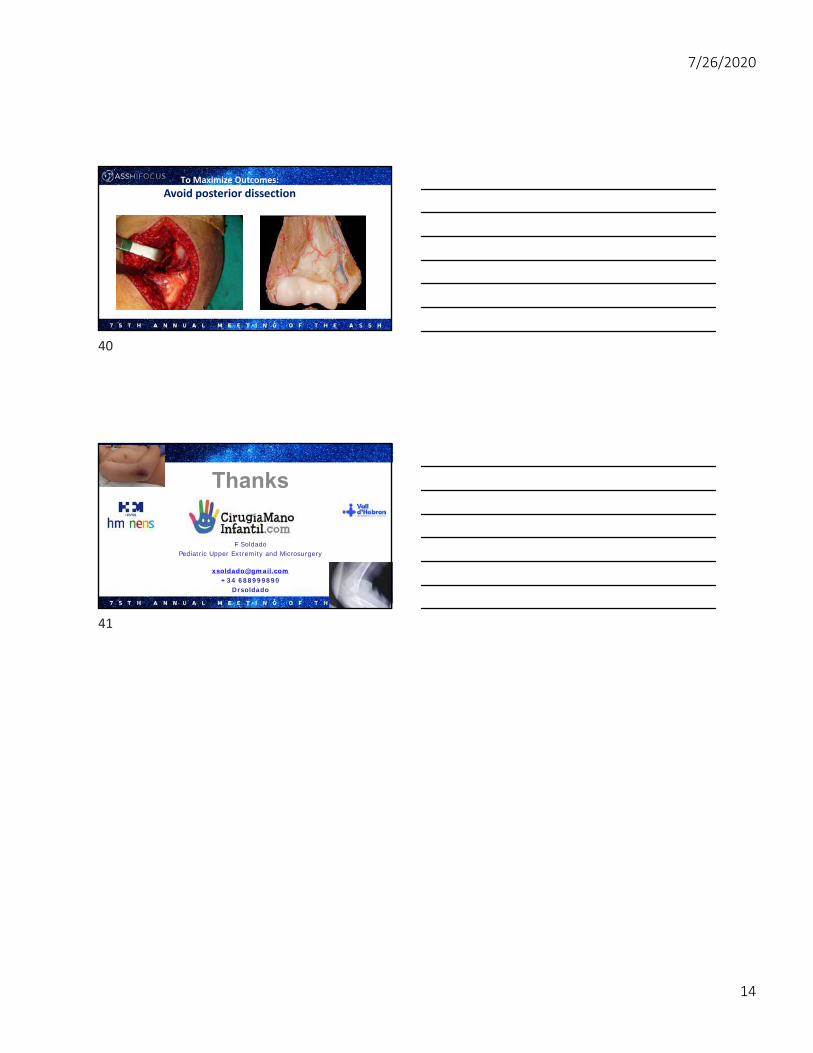
To Maximize Outcomes:
Avoid posterior dissection
Thanks
F SoldadoPediatric Upper Extremity and Microsurgery
[email protected]+34 688999890
Drsoldado
40
41
7/23/2020
1
Scott H. Kozin, MD
Speaker has no relevant financial relationships with commercial interest to disclose.
Monteggia Fracture Dislocations
Scott H. Kozin, MDShriners Hospital for ChildrenPhiladelphia, PA
Take Home Points
• Don’t miss the diagnosis• Early treatment uniformly successful• Subacute consistently successful• Chronic treatment less reliable• Ulna is the key!
1
2
3

7/23/2020
2
Acute
• Natalie• 5 year-old fell 2 days ago• Diagnosed greenstick fracture in ER• Referred to orthopaedic surgeon
Orthopaedic Surgeon Concerned
• Asked radiologist if radial head was “located”• YES!• WTF?
CT Scan
4
5
6

7/23/2020
3
Treatment?
Now What?
7
8
9

7/23/2020
4
Healed
Range of Motion
Subacute
• Michael G• 7 year-old male• Tripped over tree trunk 7/31/13 • ER- no fracture and sling• Ortho f/u 8/20/13
10
11
12

7/23/2020
5
Treatment
• Surgery 8/26/13• Closed reduction unsuccessful, open reduction• Not quite satisfied• MRI following surgery
Second Opinion
Treatment ?
13
14
15

7/23/2020
6
Final Fixation
16
17
18

7/23/2020
7
Subacute
• Gavin B • 6 year-old fell off slide 3 months ago• Treated for “fracture”• Elbow ROM 10 to 110 degrees• Full pronation and supination
Referred with X-rays & MRI
We Can Fix It!
19
20
21
7/23/2020
8
Technique
• Position• Approach• Technique- Pearls!• Rehabilitation
Position
• Supine• Standard prep and drape• Antibiotics• Tourniquet
Approach
• Extended Kocher approach• ECU- Anconeous interval• Expose ulna and open radiocapitellar (RC) joint
22
23
24

7/23/2020
9
Approach
• Remove interposed tissue• Cut ulna (step or transverse)• Reduce RC joint and place Steinman pin• Fix ulna in situ
Close-Up
25
26
27

7/23/2020
10
Next…
• Remove Steinman Pin• Range of motion• Stable → Go home • Unstable → Assess situation ulna• Annular ligament reconstruction
Post-Operative
• Splint or cast• Careful follow-up• X-ray every week for 3 weeks
Two week Follow-up
28
29
30

7/23/2020
11
ROM
• Begin at 6 weeks• Active mainly• Kids are resilient
Three Month Follow-up
Three Month Follow-up
Hang Tight!
31
32
33

7/23/2020
12
• ROM• supination 90°• pronation is 75°• elbow flexion 155°• elbow extension 0°
Final X-rays
That is How We Do It !!
34
35
36

7/23/2020
13
Chronic Monteggia- Different Problem
Michael S
• 11 year-old right forearm fracture 5 years ago• Missed Monteggia with plastic deformation ulna• Range of motion 0 to 90º• Medial laxity
X-rays
37
38
39

7/23/2020
14
Chronic Monteggia- Different Problem
• Need length first- distraction osteogenesis
Chronic Monteggia
• Subsequent bony angular correction & open reduction after length achieved
Chronic Monteggia
• May need annular ligament reconstruction• Currently favor detaching biceps from radius,
reattach to ulna, split half around radial neck to from ligament
40
41
42

7/23/2020
15
Annular Ligament Reconstruction
Annular Ligament Reconstruction
X-ray Outcome Consolidation!
43
44
45

7/23/2020
16
Radial Head Reduced!
Jeremiah B
• 16 year-old• Right elbow injury at 3 years of age• Pain• Progressive valgus instability
• No radial head buttress• Ulnar collateral ligament attentuation
46
47
48

7/23/2020
17
Can We Fix It?
Round #1
• Radial shortening osteotomy• Acute ulnar angulation osteotomy• Open reduction radial head• Reduced but subluxates in pronation
49
50
51

7/23/2020
18
6 Weeks Post-Operative
Round #2
• Detach biceps• Annular ligament reconstruction
One Year Follow-up
52
53
54
7/23/2020
19
55
56
57
7/23/2020
20
Is There a Role for Non-operative Management?
13 Year-old Ethiopian Child
• Vague history right elbow injury• No pain
13 Year-old Ethiopian Child
• Complains of decreased forearm rotation• Supination neutral• Full pronation
• Full elbow flexion and extension
58
59
60

7/23/2020
21
Supination/ Pronation
Neutral 50 degrees
Flexion/ Extension
Full Hyperextends 10 degrees
Don’t Just Do Something, Stand There
61
62
63

7/23/2020
22
Thank You
64
65

7/27/2020
1
Andrea S. Bauer, MD
Speaker has no relevant financial relationships with commercial interest to disclose.
TRASH Lesions of the Elbow
Andrea S. Bauer, MD
Boston Children’s Hospital
IC67‐R: Understanding Pediatric Elbow Fractures to Maximize Outcomes
Disclosures
• No financial disclosures
• Thank you to my partners– Carley Vuillermin & Don Bae
– Peter Waters & James Kasser
1
2
3
7/27/2020
2
TRASH
What is a TRASH lesion?
Elbow “TRASH” Lesions
The
Radiographic
Appearance
Seemed
Harmless
A small subset of injuries that are readily missed and together
result in poor outcomes when not initially identified
“More is missed by not looking than not knowing”
McCrae 1870-1935
Elbow “TRASH” Lesions
4
5
6

7/27/2020
3
Elbow “TRASH” Lesions
• Transphyseal Distal Humerus Separation
• Medial Condyle Fractures
• Complex osteochondral elbow fracture-dislocations
• Osteochondral fractures with joint incongruity
• Entrapped medial epicondylar fractures
• Lateral condylar avulsion shear fractures
• Anterior radial head fractures with progressive radiocapitellar subluxation
• Monteggia fracture dislocations
Elbow “TRASH” Lesions
• Transphyseal Distal Humerus Separation
• Medial Condyle Fractures
• Complex osteochondral elbow fracture-dislocations
• Osteochondral fractures with joint incongruity
• Entrapped medial epicondylar fractures
• Lateral condylar avulsion shear fractures
• Anterior radial head fractures with progressive radiocapitellar subluxation
• Monteggia fracture dislocations
• Capitellar fractures
7
8
9

7/27/2020
4
Radiographic Evaluation
First impressions can be deceiving• Ossification centers• Joint alignment• Signs of subtle injuries
Assess in conjunction with• The mechanism• Patient findings
Be cautious under 4Be suspicious under 10
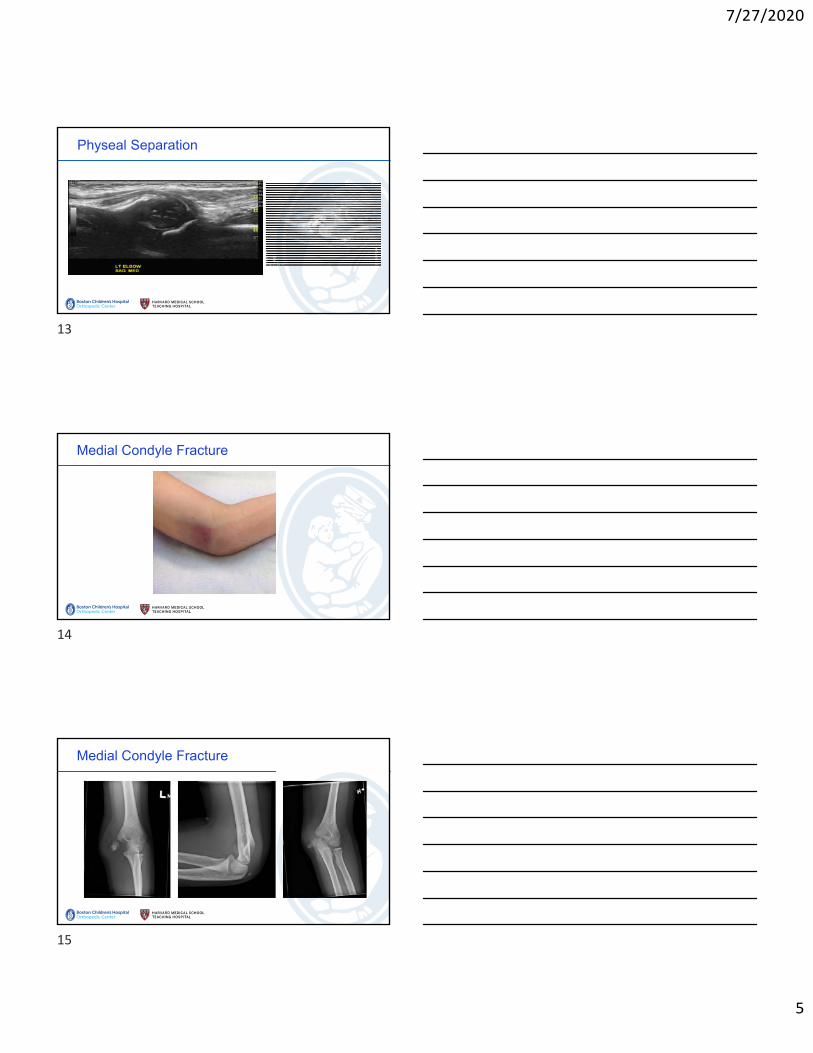
Physeal Separation
Physeal Separation
10
11
12
7/27/2020
5
Physeal Separation
Medial Condyle Fracture
Medial Condyle Fracture
13
14
15

7/27/2020
6
Medial Condyle Fracture
Osteochondral Injuries
Small fragments can represent major injuries in children’s elbows
Proper recognition is key
• High suspicion
• Advanced imaging
Osteochondral Injuries
16
17
18

7/27/2020
7
Osteochondral Injuries
Incarcerated Medial Epicondyle Fractures
Incarcerated Medial Epicondyle Fractures
Is this good enough?What to do?
Waters & Bae, Pediatric Hand & Upper Limb Surgery: A Practical Approach, 2012
19
20
21

7/27/2020
8
• All should be managed operatively
• Can be missed and present late
• Suspect the injury if the medial epicondyle is ‘at the level of the joint’
• 44% had associated ulnar nerve injury
Radial Head/neck Fractures
Commonly not isolated injuries
Small fragments can represent larger injuries
The greater the intervention, the higher the likelihood of stiffness– Stepwise approach – closed/percutaneous/open reduction
Radiocapitellar alignment and stability is critical– If any doubt exists after reduction in a young child then an arthrogram can
be helpful
Radial Head/neck Fractures
22
23
24

7/27/2020
9
<1% Elbow Fractures
4 sub-types– Anterior shear
– Posterolateral shear
– Acute chondral shear
Not all require surgical management however maintain a high index of suspicion
Type I: Non‐displaced Type II: Posterior shear
Type III: Anterior shear Type IV: Acute osteochondral injury
Capitellar Fractures
Capitellar fractures: Type II Posterior Shear
• 19%
• Average age 12.4y (8-15)
• Associated with known dislocation
• Poorly visualized on plain radiographs
• Best seen on sagittal CT
• Better outcomes with primary surgical treatment
25
26
27

7/27/2020
10
• 15%
• Age 13y (9-14)
• Best diagnosed on sagittal MRI
• All required surgery
Capitellar Fractures: Type IV Acute OCD
Summary
It’s easy to be wise in retrospect
Be suspicious from the beginning!– Age
– Mechanism
– Clinical presentation
– Imaging
Sometimes the perspective we are looking from prevents us from seeing.
28
29
30