TRAUMATOLOGY FRACTURES AND DISLOCATIONS L.Yu.Ivashchuk Lecture:

FEBRUARY 2007 • PODIATRY MANAGEMENTwww.podiatrym.com 175
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (yousave $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 186. Other than those entities cur-rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: PodiatryManagement, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 186).—Editor
Continuing
Medical Education
Goals and Objectives
After completing this CME:
1) The reader will under-stand the variety of pediatricfoot fractures
2) The reader will under-stand the indications forclosed and open treatmentsfor pediatric foot fractures
3) The reader will under-stand the nature of the com-plications encountered in pe-diatric foot fractures
more liable to separate through theepiphyseal plate (Salter-Harris I).
As children age, the physes be-come more mature and correspond-ingly thinner. These physiologicevents predispose them to fracturesthat enter the growth plate and exiteither through the metaphyseal boneor through the epiphysis and into thejoint space (Salter-Harris II and III).
As growth plates become evenmore mature, trauma near articula-tions can fracture across the joint sur-face, epiphysis, physis and metaph-
Continued on page 176
Fractures of the child’s footand ankle occur surprisinglyfrequently. The types of in-
juries are age-dependent and relateto the child’s physical size, develop-mental age and activity levels. In-fants and younger children havelighter body masses, shorter bonylever arms and engage in less stren-uous physical activities. Older chil-dren and adolescents are physicallylarger and engage in sports andother activities that predispose
them to more forceful injuries.Infants and very young children
are more likely to develop cancel-lous fractures of bone that are oftenreferred to as “toddler fractures.”Older children and pre-adolescentsare more likely to have diaphysealand articular injuries.
Growth Plate InjuriesGrowth plate injuries can occur at
any age, and can happen even beforethe secondary centers have begun toossify. Infants and younger childrenhave wide open physes which are
By Edwin Harris, D.P.M.
Here’s when to treatthese open and when totreat these closed.
PediatricFractures andDislocations
P O D O P E D I A T R I C SP O D O P E D I A T R I C S
PediatricFractures andDislocations

Closed FracturesClosed (simple) fractures do not
produce an open wound in the skin.(Figure 1) They are the most commonpediatric foot fractures. They can berelatively innocuous, or may result inconsiderable soft tissue damage (com-plex fractures). Open fractures have abreech in the skin that leads to thebone injury and allows the fracture tocommunicate to the environment.(Figures 2A-C) Thisopening can beproduced by pene-trating traumafrom the outside,or by a sharp seg-ment of bonepiercing the skinfrom within. Openpediatric foot andankle fracturesoccur much lessfrequently thanclosed injuries.
Closed fractures are generallymore benign and have fewer compli-cations. Open fractures are at risk forinfection. Damage to the soft tissuesin both types of fractures may com-promise the blood supply to the frac-ture fragments and surrounding soft
tissues. Both types of fracturesmay have significant displace-ment.
Most closed fractures are easi-ly manipulated back intoalignment unless there is softtissue interposition betweenthe fracture fragments (Figure3). This complication is more
likely to occur in open fractures andit makes manipulative reduction dif-ficult or impossible. Damage to thesupporting soft tissue may make sta-bilization difficult in both open andclosed fractures.
Open FracturesOpen fractures often have consid-
erable skin and subcutaneous tissueloss that may leave an unstable frac-
ture open to theenvironment andnecessitate tempo-rary external fixa-tion. The funda-mental rule is thatclosed fracturesshould remainclosed wheneverpossible and openfractures require ir-rigation, debride-ment, stabiliza-tion, and eventual
wound closure.The majority of forefoot fractures
in children are closed. Just aboutevery fracture pattern has been re-ported. These include greenstick,transverse, spiral, oblique, intra-artic-ular and burst patterns. Fractures maybe single or multiple.
Most open fractures occur withinjuries that produce both the frac-ture itself and some form of lacera-tion. Most of these are simple andrelatively easy to manage. Open rear-foot and ankle fractures, however,can damage the neurovascular struc-tures, epiphyseal plates and joint sur-faces. Some injuries may be limb-threatening.
Some open injuries may have avery tiny skin opening and appear tobe very innocuous. This is particularlytrue of fractures that involve the dis-tal phalanges and the nails (Figure 4).Burst fractures of the distal phalangesfrom falling objects and stubbing in-juries lacerate the nail bed and pro-duce a subungual hematoma.
The lacerated nail bed communi-cates directly to the fracture. Thehematoma under the nail plate servesas a culture medium for bacteria andincreases the risk of osteomyelitis.These injuries require debridement ofthe nail, irrigation and suturing of thenail bed. Stubbing trauma may frac-ture the distal phalanx through itsphysis.
Continued on page 177
176 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
Fractures...
ysis (Salter-Harris IV). These in-juries can displace the articular
surface and cause partial epiphysealarrest. The result is arthrosis and an-gular deformity.
Some injuries (at any age) can to-tally shut down the function of thephysis and result in premature plateclosure (Salter-Harris V).
Contin
uing
Medica
l Edu
catio
n
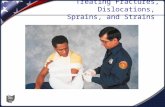
Figure 2A-C: A lawnmower accident in atwo-year-old male produced a severelaceration of the hallux and the plantarof the foot (A). There is an open com-minuted fracture of the distal phalanxwith some bone loss (B). After appropri-ate irrigation of the wound, the unsta-ble fracture was fixated with a Kirschnerwire (C).
Figure 1: A closed comminuted fracture.The skin is intact. The fracture does notcommunicate to the environment.
Infants and
very young children
are more likely to
develop cancellous
fractures of bone.

FEBRUARY 2007 • PODIATRY MANAGEMENTwww.podiatrym.com 177
Although the fracture line isproximal to the eponychium,the nail plate often is avulsedand the nail root is lacerated.(Figure 5 A-B) This allowscommunication to the outsidethrough the lacerated proxi-mal nail fold to the fracturedphysis. Physeal arrest isanother potential com-plication.
Management ofClosed Fractures
Protection AloneSome fractures are best
managed by protectionalone without reduction orthe need for rigid immobi-lization. This amounts totreatment by benign ne-glect. In order for this tobe indicated and success-ful, the fracture has to bestable and not displacedFigure 6A-B).Most healing stress fractures
are easily managed by thistechnique. By the time thatthey are recognized radio-graphically, they are about twoweeks into the healing process.They are identified by pe-riosteal new bone that devel-ops adjacent to the fracture site(Figure 7A-B). Most of thetime, the fracture line itself isnot seen. If a fracture line is vi-
sualized, the probability is that a
Fractures... stress fracture has pro-gressed to a pathological frac-ture (Figure 8).
In spite of this conversion,these fractures usually remain stable.The success of this type of fracturemanagement depends on a number offactors. The location of the fracture is
important, as are the physical size andactivity of the patient. Patient age andcooperation must be factored into thedecision to treat by this technique.
Cancellous fractures are commonin toddlers. These occur in bones thathave minimal cortical developmentaround large amounts of cancellousbone. The cuboid and the calcaneusare the most common sites. (Figure9A-B) The injury may or may not bewitnessed. Frequently, limping or anantalgic gait pattern are the present-ing complaints.
Like stress fractures, this injury isradiographically silent until new bonebegins to form on damaged trabecu-lae about 10 to 14 days after the in-jury. Initial treatment is based on ahigh index of suspicion. By the timethe fracture is recognized, the risk ofdisplacement is minimal. Treatmentis largely directed at comfort for thechild.
Sometimes, the child does notpresent for diagnosis until a fracture isalmost completely healed. At thattime, the risk for additional injury isnegligible. Most of these childrendon’t need any treatment at all (Fig-ure 10A-B).
Immobilization With or WithoutWeight-Bearing
Because of their nature, complexi-
Continuing
Medical Education
Continued on page 178
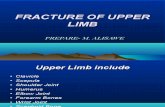
Figure 4: A heavy object fell on the end of the sec-ond toe. The nail plate was traumatically avulsed.The distal phalanx is extensively comminuted.The nail bed was lacerated.
Figure 5: A hyperflexion injury of the halluxproduced an open displaced Salter-Harris II frac-ture of the distal phalanx. The nail root wasavulsed and the nail bed was lacerated at thelunula.
Figure 6A-B: (A) There is a stable diaphyseal fracture of the second proximal phalanx.It is well aligned, and is unlikely to displace. (B) There is a buckle (torus) fracture ofthe distal fifth metatarsal metaphysis. Although the cortex has failed, the fractureline itself is unlikely to progress.
Figure 3: A hyperflexion injury of the halluxproduced a fracture of the physis of the distalphalanx and a fracture of the dorsal portion ofthe base (arrow). Closed reduction was impossi-ble because periosteum from the phalanx in-vaginated into the fracture. Open reduction be-came necessary.

ble and displaced, but the alignmentis acceptable. Muscle pull and gravita-tional forces may cause angulation,rotation, or overriding of the fracturesegments (Figure 13). Additional at-tempts at closed reduction would beunlikely to improve the position andmight make management more com-plicated. Occasionally, an unstable,displaced but almost united fracture isencountered. These usually requiresimple protection alone.
TreatmentThese fractures are initially man-
aged with splints. Once edema hassubsided, immobilization can be con-tinued with casts. At this point, thedecision to treat initially by non-
weight-bearing or allow for immedi-ate weight-bearing immobilizationmust be made. If early weight-bearingmight produce excessive motion orallow displacement, treatment shouldbegin by two to three weeks of non-weight-bearing. Past that point, mostfractures are sufficiently consolidatedso that they can safely tolerate bear-ing weight in a cast.
Under certain circumstances,walking boots may be substituted forcasts. The ability to remove them isboth an advantage and a disadvan-tage. In appropriately selected pa-tients, a walking boot can be removedfor bathing and sleeping. In non-com-pliant patients, there may be extremedifficulty keeping this apparatus on.
Along the same lines,some metatarsal fracturescan be managed withsurgical shoes for select-ed patients.
Manual ClosedReduction
Whenever it is practi-cal and safe, displacedfractures are better man-aged by closed reduc-tion. Simple closed tech-niques can be employedany time reduction is re-quired, reduction can beachieved, and reductionis maintainable (Figure14A-B)
Continued on page 179
178 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
Fractures...
ty and location, some fracturesare inherently unstable or have
the potential to become unstable.These include multiple fractures,comminuted fractures and fracturesthat may displace because of their lo-cation in the bone (Figure 11A-B.)
Comminuted fractures at thebases of the metatarsals are good ex-amples of these types of injuries.Other fractures are unstable becausethey involve insertions of majortendons. Some intra-articular frac-tures may initially have congruentjoint surfaces, but they are at riskfor displacement. These includefractures of the first proximal pha-lanx (Figure 12).
Other fracture patterns are unsta-
Contin
uing
Medica
l Edu
catio
n
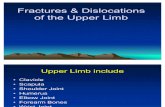
Figure 9A-B: (A) A three-year-old child fell approximately 3 feet and landed on his plantarflexed foot.There was edema, ecchymosis and pain localized over the dorsolateral tarsus. Initial radiographswere negative. Fourteen days later, sclerosis can be seen in the dorsal and proximal cuboid (new bonelaid down on injured trabeculae). This cancellous fracture is sometimes referred to as a “toddler”fracture. (B) A 13 year old male had heel pain following heavy sports activities. Initial radiographswere negative. Two weeks later, a healing cancellous stress fracture can be seen in the calcanealmetaphysis (black arrows).
Figure 8: This healing stress fractureshows an almost complete fracture line(black arrows)
Figure 7A-B: (A) There is a stress fracture of the second metatarsal diaphysis. A cuffof periosteal new bone can be seen (white arrows). More detail can be seen in theinset. (B) More extensive periosteal new bone can be seen in this third metatarsaldiaphyseal stress fracture.

www.podiatrym.com 179
Reduction by TractionReduction by traction as the
principal treatment for fractures hasall but been abandoned. In certainsituations, traction provided by fin-ger traps can be used to pull somefractures back out to length; how-ever, these fractures are likely to beunstable. The result is almost imme-
diate loss of alignment. Vascularcomplications and skin breakdownmake closed reduction by continu-ous traction unattractive. An addi-tional issue is the cost to cover theapparatus and nursing care neededfor the comparatively long convales-cence.
Immediate FixationIn order to decrease morbidity
and get patients back into functionas quickly as possible, some fractures
As long as there is no vascularcompromise, closed reduction can besafely performed under local anesthe-sia with or without sedation. The twomost common reasons for failure ofsuccessful management are inabilityto achieve initial adequate reduction
and subsequent loss of reduction (Fig-ure 15A-B)
In some cases, successful reduc-tion can be achieved by employingpercutaneous Kirschner wires as “joy-sticks” to assist in the reduction, andthen use them to maintain fixation(Figure 16).
Fractures... are best managed by im-mediate fixation. This canbe accomplished through theuse of external fixators, in-tramedullary fixation, percutaneousfixation and fixation with plates andscrews.
Indications for external fixatorsinclude unstable oblique, spiral,and comminuted fractures. Addi-tional considerations include skinloss, neurovascular compromise,bone loss and maintenance oflength and stability in preparation
for skin and bone graft-ing.
Indications for in-tramedullary fixation in-clude unstable oblique,spiral, and minimallycomminuted fractures.Best indication is for frac-tures that can be ade-quately and accurately re-duced by closed means,but the nature of thesefractures makes it unlike-ly that alignment can bemaintained by simple im-mobilization alone.
Continuing
Medical Education
Continued on page 180
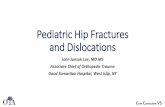
Figure 11A-B: (A) Multiple lesser metatarsal base fractures need protective immobilization. Thelong lever arms will allow movement at the fracture sites. (B) Fifth metatarsal base fractures inchildren may be comminuted and may extend into the joint space. Additionally, the tractionapophysitis of the fifth metatarsal base is often involved. Although they have a very high unionrate, they are better managed in active children by immobilization.
Figure 10A-B: Two fifth metatarsal neck fractures (white arrows). Both are almostcompletely healed at the time that these children presented for diagnosis. No protec-tion is necessary.
Figure 12: Regardless of patient age, frac-tures involving the articular surfacesmust be well aligned in order to preventarthrosis. This comminuted fracture ofthe first proximal phalanx in a 12-year-old girl shows acceptable alignment.There is no step-off in the joint space,and the fracture line is less than 2 mm inwidth. Further reduction is not necessary.
FEBRUARY 2007 • PODIATRY MANAGEMENT

and there are significant step-offs onthe articular surfaces. The fracturemargins need to be perfectly alignedin order to restore the anatomy of thearticular surface (Figure 19A-B).
Displaced FracturesSome fractures displace widely
enough so that surrounding soft tis-sues (tendon, capsule, ligament of thesoft tissues) can enter the fracture gap.They serve as mechanical impedi-ments to reduction and make openreduction necessary. At the sametime, fracture fixation can be accom-plished by replanting and fixating thefracture fragments.
Some fractures are grossly unsta-ble. Some form of reduc-tion can be achieved,but it becomes impossi-ble to maintain this re-duction. This is particu-larly true for metatarsalfractures in the distalone third. Because ofdisplacement and frag-ment rotation, it may beimpossible to achieve aclosed reduction. Ratherthan accept these mis-aligned fractures, treatthese by open reductionand intramedullary fixa-tion (Figure 20A-B).
High-Risk FracturesOnly a very few pe-
diatric foot fracturescarry a high risk of non-union. Jonesfractures are the best examples. Theseoccur at the junction of the diaphysisand the base of the fifth metatarsal.They are more or less transverse, butthey occur in an area of bone that isdeficient in blood flow. Although asignificant number of them will heal,
the nonunion and refracture rates arequite high. They frequently occur inelitist athletes and can prove disas-trous to their careers. Because of thesehigh risks, primary fixation is justified(Figure 21A-B).
Open FracturesBy definition,
any fracture thatpenetrates the skinis an open fracture.With this type ofinjury, there are anumber of addi-tional factors thatmust be consid-ered. First, the skinis breeched. Thiscreates an openwound, the size ofwhich is deter-mined by the na-
180 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
Fractures...
Intra-Articular FracturesIntra-articular fractures must be
reduced precisely anatomically or de-generative arthrosis will result. Majorarticular injuries require screw fixa-tion to maintain joint surface con-gruity. Penetration of the growthplate must be avoided (Figure 17).
Avulsion FracturesAvulsion fractures of the margins
of the small joints of the feet lendthemselves well to percutaneous oropen fixation through the use ofsmooth or threaded Kirschner wires(Figure 18A-B).
Comminuted Intra-ArticularFractures
Comminuted intra-articular frac-tures are particularly difficult to man-age because they are very unstable
Contin
uing
Medica
l Edu
catio
n
Figure 15A-B: (A) This second proximal phalanx fracturewas initially manipulated into reduction. Reduction wascompletely lost. By the time it was recognized, it was toolate to attempt further reduction. (B) Fortunately, there isconsiderable potential for remodeling in young children.During fracture healing, it remodeled to near normal(white arrows)
Figure 14A-B: (A) A 30 month old male stubbed his fifth toe. There is significant angular displacement ofthe fifth proximal phalanx. (B) Under local anesthesia, the fracture was successfully manipulated into bet-ter alignment.
Figure 13: The long-term effects of dis-placed fractures can be malalignment,osteonecrosis and non-union.
Continued on page 181

FEBRUARY 2007 • PODIATRY MANAGEMENTwww.podiatrym.com 181
skin grafting. Second, the risk of os-teomyelitis is quite high. Third, openfractures are often complicated by lossof bone. This requires grafting a bonein order to restore length, alignmentand stability.
Penetrating TraumaSince the foot is a weight-bearing
organ, sharp and blunt objects maypenetrate the skin with considerableforce. They may go to the bone andproduce comminuted fractures orbone can be gouged away (Figure22A-B).
ture of the injury. Significant tissueloss makes management of the frac-ture very difficult.
Not only is it necessary to stabilizethe fracture so that it heals in the bestanatomic position, but skin loss ne-cessitates preparation of a viable bedfor subsequent split or full thickness
Fractures... Gunshot wounds tothe foot are also very com-mon. Bone and soft tissue dam-age depend on the size of the pro-jectile and the proximity of the vic-tim to the muzzle of the gun. In mostcases, considerable soft tissue damagealso occurs. Compartment pressuresmay be elevated enough to warrantfasciotomy. Multiple fractures are therule. Fractures are usually comminut-ed, and alignment of the fracture frag-ments is difficult to achieve andmaintain (Figure 23).
Fractures may also occur in asso-
Continuing
Medical Education
Figure 19A-B: (A) An extensively comminuted fracture of the first proximal phalanxshows significant articular surface displacement. This fracture was reduced under di-rect vision, the articular surface was restored and the fracture was fixated withKirschner wires (B).
Figure 18A-B: Pull-off fractures of the articular margins of short tubular bones can in-volve a significant portion of the articular surface (A). These may be fixated withsmooth or threaded Kirschner wires (B).
Figure 17: This complex triplane frac-ture of the distal tibia involves the artic-ular surface as well as the metaphysis. Itis necessary to anatomically align andfixate the articular surface under directvision.
Figure 16: A 13 year old spastic diplegicfractured and completely displaced hissecond proximal phalanx. Attemptedclosed reduction failed, so the fracturewas percutaneously fixated with aKirschner wire.
Continued on page 182

arrest may result from epiphysealavascular necrosis or from direct dam-age to the physes when they are in-volved in the fracture (Figure 27).Arthrosis may occur when joint sub-
182 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
Fractures...
ciation with major lacerations.These usually come from lawn-
mower injuries, marine propellerinjuries and farming accidents. Thewounds are usuallygrossly contaminated.
Fractures may be-come open when a seg-ment of bone piercesthe skin from within. Asimilar thing may hap-pen when violent dislo-cation occurs (Figure24A-B.)
The wounds associ-ated with open fracturesrequire special manage-ment to remove con-tamination, debridenecrotic tissue, and pre-pare them for closurewith or without surgicalintervention. Impropermanagement will resultin soft tissue infection, osteomyelitis,vascular compromise, and even lossof the limb.
DislocationsDislocations may occur with or
without a fracture and may be openor closed (Figure 25A-B). Successful re-duction can only occur when there isno soft tissue interposition to preventjoint realignment. Tendon, capsule,and ligaments are the tissues that usu-ally prevent reduction. On occasion,nerve and blood vessel may betrapped in the dislocation.
Dislocations may be subtle. Fail-ure to recognize the dislocation andpromptly reduce it often results inlong-term arthrosis and suboptimalfunction.
Complications
Avascular NecrosisBoth open and
closed management offractures may result inpredictable complica-tions. Avascular necrosisof the epiphyses ingrowing children canoccur if they are dam-aged either by the trau-ma of the fracture or re-sulting edema (Figure26). This may result injoint collapse. Growth
Contin
uing
Medica
l Edu
catio
n
Figure 22A-B: An 11 year old male jumped from a swing and impaled his heel on the threads of alarge screw. This foreign body penetrated bone and gouged out several small fragments from the cal-caneus.
Figure 21A-B: (A) Jones fractures of the fifth metatarsal base have a high nonunionrate. Screw fixation stabilizes the fractureand produces compression across the frac-ture line (B).
Figure 20A-B: (A) A fall from a height produced stable fractures of the second and third metatarsalsand a completely displaced distal fourth metatarsal fracture. An attempt was made to reduce this inthe emergency room, but 24 hours later the fourth metatarsal was unreduced. Radiographs on severalother planes showed a very wide separation of the fracture fragments that could only be appreciatedon the oblique projections. (B) Open reduction and Kirschner wire fixation stabilized the fracture.
Continued on page 182

FEBRUARY 2007 • PODIATRY MANAGEMENTwww.podiatrym.com 183
ing potential for children is muchhigher. Fractures close to the epiphy-ses, with deformation in the plane ofjoint motion, are likely to remodelalmost completely and leave littlefunctional deformity. Fractures at
luxations and dislocations are not rec-ognized and treated (Figure 28).Arthrosis can also result from step-offinjuries to the articular surface itself.
Mal-alignmentMal-alignment is always a risk.
Even if the fracture is explored in theoperating room and reduced underdirect vision, instability can result inshortening or angular deformity (Fig-ure 29). Unlike adults, the remodel-
Fractures... right angles to joint mo-tion do not have much po-tential for spontaneous remod-eling. Therefore, it is necessary tosecure and maintain good anatomi-cal alignment.
ConclusionsThere are a number of practical
points to be made. Fractures are bettermanaged closed whenever possible.Risk of infection is reduced almost tozero. Vascular supply to the fracturefragments is preserved. As long as sur-rounding soft tissues don’t block frac-ture reduction, they tend to supportthe fracture fragments and maintainalignment.
Open fractures havetheir own inherentrisks of infection andvascular damage. Theyhave to be managed assuch with attentiongiven to preparing thewound by irrigation,debridement, and stabi-lization of the bone inanatomical alignment.
Some fractures areopen by their very na-ture, but the breech inthe skin is very subtle.Comminutions of thephalanges with subun-gual hematomas are al-ways open fractures.Epiphyseal plate in-juries of the distal pha-langes of the toes areusually open fractures.
Soft tissue in the resulting defect inthe physis may prevent realignmentand jeopardize healing.
Percutaneous fixation (if possi-ble) is preferable to open reduction.In order for this to be successful, the
surgeon must have theskill to perform this typeof procedure, and musthave imaging modalitiesreadily available.
Open reduction is in-dicated if satisfactoryalignment cannot beachieved, the fracture isirreducible because ofsoft tissue interposition,the fracture is unstable,or the nature and thenatural history of thefracture warrant it.
Continuing
Medical Education
Figure 25A-B: (A) A close irreducible fifth metatarsopha-langeal joint dislocation required open reduction to re-store position of the plantar plate and long flexor tendonthat were preventing reduction. (B) An open hallux inter-phalangeal joint dislocation resulted in a jagged lacera-tion of the plantar and medial skin. The dislocation wasirreducible and required open reduction and Kirschnerwire fixation.
Figure 24A-B: A fracture in the distal second metatarsal resulted in a portion of the distal fragmentthat rotated dorsally and penetrated the skin (A and B)
Figure 23: Gunshot wounds result inmultiple fractures, considerable soft tis-sue damage with the potential for in-creased compartment pressure andresidual fragments of the projectile. Thefractures tend to be extensively com-minuted and difficult to stabilize.
Continued on page 184

Carrol N, 1994. Fracture and Disloca-tion of the Tarsal Bones. In: Management
of Pediatric Fractures (LettsRM, ed.). New York:Churchill Livingstone;751-766.
Conklin MJ, 2004. Pedi-atric Fractures. In: Frac-tures of the Foot andAnkle (Guman G, ed.).Philadelphia: ElsevierSaunders; 336-369.
Crawford AH, Al-Sayyad MJ, 2003. Fracturesand Dislocations of theFoot and Ankle. In: Skele-tal Trauma in Children,Third Edition ed. (GreenNE, Swiontkowski MF,eds.). Philadelphia: Saun-ders; 516-586.
Gross RH, 1991. Frac-tures and Dislocations of theFoot. In: Fractures in Chil-
dren, Third Edition ed. (Rockwood CA,Wilkins KE, King RE, eds.). Philadelphia: J.B. Lippincott Company; 1383-1453.
Gross RH, 1996. Fractures and Dislo-cations of the Foot. In:Fractures in Children,Fourth Edition ed.(Rock-wood CA, Wilkins KE,Beaty JH, eds.). Philadel-phia: Lippincott-Raven;1429-1497.
Harris EJ, GastwirthBW, 2001. Fracture Man-agement in the PediatricPatient. In: McGlamry’sComprehensive Textbookof Foot and Ankle Sur-gery, Third Edition ed.(Banks AS, Downey MS,Martin DE, Miller SJ,eds.). Philadelphia: Lip-pincott Williams &Wilkins; 1957-1993.
Jarvis JG, 1994. TibialTriplane Fractures. In:Management of PediatricFractures (Letts RM, ed.).
New York: Churchill Livingstone; 735-750.
Lalonde F, Pring ME, 2005. Ankle. In:Rang’s Children’s Fractures, Third Editioned. (Rang MC, Pring ME, Wenger D, eds.).Philadelphia: Lippincott Williams &Wilkins; 228-242.
Lalonde F, Wenger D, 2005. Foot. In:Rang’s Children’s Fractures Third Editioned. (Rang MC, Pring ME, Wenger DR,eds.). Philadelphia: Lippincott Williams &Wilkins; 243-252.
Main K, Rand F, 1993. Ankle Frac-tures. In: Pediatric Fractures A PracticalApproach to Assessment and Treatment(MacEwen CD, Kasser JR, Heinrich SD,eds.). Baltimore: Williams & Wilkins;328-341.
Rang MC, 1983. Children’s Fractures,Second Edition ed. Philadelphia: J. B. Lip-pincott.
San Giovani TP, Gross RH, 2001.Fractures and Dislocations of the Foot. In:Rockwood and Wilkins’ Fractures in Chil-dren, Fifth Edition ed. (Beaty JH, KasserJR, eds.). Philadelphia: LippincottWilliams & Wilkins; 1169-1222.
184 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
Fractures...
Open reduction is indicated tofacilitate faster healing, easier re-
habilitation and earlier mobiliza-tion. ■
Recommended ReadingsAshworth A, Hedden D, 1994. Frac-
tures of the Ankle. In: Management of Pe-diatric Fractures (Letts RM, ed.). NewYork: Churchill Livingstone; 713-734.
Baxter MP, 1994. Fractures and Dislo-cations of the Metatarsals and Phalangesof the Foot. In: Management of PediatricFractures (Letts RM, ed.). New York:Churchill Livingstone; 767-788.
Bordelon R, 1993. Fractures of thechild’s foot. In: Pediatric Fractures: Apractical approach to assessment and
treatment (MacEwen CD, Kasser JR, Hein-rich SD, eds.). Baltimore: Williams andWilkins; 343-365.
Contin
uing
Medica
l Edu
catio
n
Dr. Harris isClinical Associ-ate Professor De-partment of Or-thopaedics andRehabilitation at the StritchSchool of Medi-cine of LoyolaU n i v e r s i t yChicago. He is aDiplomate, of the American Board ofPodiatric Surgery and the AmericanBoard of Podiatric Orthopedics and Pri-mary Podiatric Medicine, and a Fellowof the American College of Foot andAnkle Surgeons.
Figure 28: Long-standing dislocationsmay result in permanent arthrosis.
Figure 27: Fractures across the growth plate can result inpartial or complete growth arrest. This child sustained aSalter IV fracture of the third metatarsal (white arrows).The physis subsequently closed prematurely and resultedin significant disturbance of the metatarsal parabola(inset, open black arrow).
Figure 26: A Salter I second metatarsal fracture was diag-nosed in an eight-year-old girl following trauma. Twomonths later, there is sclerosis of the second metatarsalhead and some minimal collapse. This avascular necro-sis is reminiscent of Freiberg’s infraction.
Intra-articular
fractures must be
reduced precisely
anatomically
or degenerative
arthrosis will
result..

FEBRUARY 2007 • PODIATRY MANAGEMENTwww.podiatrym.com 185
6) Cancellous fractures of thecalcaneus and cuboid in infantsand toddlers are treated by im-mobilization in order to:
A) prevent displacementB) provide pain relief forthe childC) provide stability for po-tentially unstable fracturesD) prevent conversion topathological fracture
7) Stress fractures and cancel-lous fractures may be radio-graphically invisible until:
A) one to two days afterthe traumaB) ten to 14 days after thetraumaC) three to four weeks afterthe traumaD) may never visualize
8) Which of the following frac-tures does not require immobi-lization?
A) an oblique fracture ofthe fifth metatarsal shaftthat is almost healedB) a fracture of the firstproximal phalanxC) multiple metatarsal basefracturesD) successfully closed re-duced, but unstable frac-tures
9) Fractures associated withsignificant edema are bestmanaged initially by:
A) immediate castingB) splintsC) ice and dependent posi-tioningD) Ace bandages
10) Which of the followingfractures is best managed in anonweightbearing cast?
A) a fracture of the fifthmetatarsal tuberosityB) a cancellous fracture of
1) The most common fracturepattern in the infant and youngchild is:
A) fracture of the epiphysisB) fracture through thegrowth plateC) fracture in cancellous boneD) fracture into the jointspace
2) The most important determin-er for the pattern of growthplate fractures is:
A) the mechanism of injuryB) the weight of the childC) the gender of the childD) the maturity of thegrowth plate
3) The most common cause forfailure of closed reduction in pe-diatric fractures is:
A) comminution of the frac-ture endsB) uncontrolled edemaC) soft tissue interposed be-tween the fracture fragmentsD) intact periosteum
4) Burst fractures of the distalphalanges with subungualhematomas and disrupted nailbeds must be regarded as
A) open fracturesB) grossly necrotic boneC) grossly unstable fracturesD) benign with no specialtreatment indicated
5) Which of the following frac-tures best meets the criteria formanagement by simple protec-tion?
A) fractures that require openreductionB) fractures that requireclosed reductionC) fractures less than 24hours oldD) fractures that are almosthealed
the cuboidC) a fracture of the distalfirst metatarsalD) a fracture of the second,third and fourth proximalphalanges
11) Complications resultingfrom managing fractures bytraction techniques include allof the following except:
A) vascular compromiseB) skin breakdownC) prolonged immobiliza-tion timeD) premature growth plateclosure
12) Fractures that can be ade-quately and accurately reducedby closed means, but are un-likely to maintain alignment arebest managed by:
A) casting off-weight-bear-ingB) internal fixation withKirschner wires, screws orplatesC) splints or a Jones dress-ing until edema subsidesD) immediate bone grafting
13) Which of the following isnot an indication for applica-tion of an external fixator for afracture?
A) fracture with skin lossB) fracture with bone lossC) neurovascular compro-miseD) closed, but mal-alignedfracture
14) The long term complicationof mal-united intra-articularfractures is:
A) joint instabilityB) angular deformityC) arthrosisD) avascular necrosis
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 187.
Continued on page 186

186 PODIATRY MANAGEMENT
15) Which of the following pediatric fractures ismost likely to result in nonunion?
A) fracture of the distal third of the metatarsalB) Jones fracture of the fifth metatarsalC) calcaneal stress fractureD) oblique fracture of the fifth proximal phalanx
16) A significant risk in Jones fractures of the fifthmetatarsal is:
A) mal-alignmentB) infectionC) avascular necrosisD) re-fracture
17) The initial step in the management of openfractures is:
A) Early primary closure of the woundB) Radical debridement of the margins of thewoundC) Removal of all loose bone fragmentsD) Irrigation of the wound and removal of allgross contamination
18) Mal-aligned fractures close to the functioninggrowth plates in children are likely to remodel aslong as:
A) the mal-alignment is under 5°B) the mal-alignment is at right angles to theplane of joint motionC) the mal-alignment is in the plane of jointmotionD) the mal-alignment has a rotatory component
19) The initial treatment for fractures and disloca-tions that cannot be reduced is:
A) external fixationB) casting until the edema subsidesC) repeat attempt at closed reduction until successfulD) surgical exploration to remove the impedi-ment to reduction
20) Which of the following is not an indication foropen or percutaneous reduction of foot fractures?
A) the fracture is irreducibleB) closed reduction cannot be achievedC) minor mal-alignment remains after closedreductionD) when faster healing and convalescence be-come critical issues
E X A M I N A T I O N
(cont’d)
See answer sheet on page 187.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. Each lessonis approved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of partici-pation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania

Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $20.00 for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $139.00 (thus saving me $61 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcredit card information to: Podiatry Management, P.O. Box490, East Islip, NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded and may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your credit card information to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
187
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $20.00 per exam, or $139 to cover all 10 exams(thus saving $61* over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet

✄
188 www.podiatrym.comPODIATRY MANAGEMENT • FEBRUARY 2007
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)Con
tinuin
g
Medica
l Edu
catio
n
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #2/07Pediatric Fractures and Dislocations
(Harris)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle: