Human clinical hemorheological studies in healthy subjects...
68
Human clinical hemorheological studies in healthy subjects and in patients with coronary artery disease PhD dissertation Author: Andras Toth MD Interdisciplinary Medical Sciences Doctoral School Molecular and cellular biochemistry Doctoral Program Doctoral School and Program leader: Prof. Balazs Sumegi PhD, ScD Project leaders: Istvan Battyani MD, PhD Gabor Kesmarky MD, PhD University of Pecs, Medical School Pecs, Hungary 2014
Transcript of Human clinical hemorheological studies in healthy subjects...

Human clinical hemorheological studies in healthy subjects and in
patients with coronary artery disease
PhD dissertation
Author: Andras Toth MD
Interdisciplinary Medical Sciences Doctoral School
Molecular and cellular biochemistry Doctoral Program
Doctoral School and Program leader: Prof. Balazs Sumegi PhD, ScD
Project leaders:
Istvan Battyani MD, PhD Gabor Kesmarky MD, PhD
University of Pecs, Medical School Pecs, Hungary
2014

1
Table of contents
TABLE OF CONTENTS ................................................................................................ 1
ABBREVIATIONS AND SYMBOLS ............................................................................... 4
INTRODUCTION ........................................................................................................ 6
THE BURDEN OF CARDIOVASCULAR DISEASES ............................................................................ 6
THE FRENCH PARADOX ........................................................................................................ 6
HEMORHEOLOGICAL PARAMETERS AS CARDIOVASCULAR RISK FACTORS ........................................ 10
CLINICAL IMPORTANCE OF HEMORHEOLOGICAL PARAMETERS IN CARDIOVASCULAR DISEASES ........... 11
Hematocrit ....................................................................................................................................... 12
Plasma and whole blood viscosity .................................................................................................... 12
Red blood cell aggregation ............................................................................................................... 12
Red blood cell deformability ............................................................................................................. 13
AIMS ...................................................................................................................... 14
HEMORHEOLOGICAL EFFECTS OF MODERATE RED WINE CONSUMPTION ........................................... 14
HEMORHEOLOGICAL PARAMETERS IN CT-DETECTED CORONARY ARTERY DISEASE ........................... 14
HEMORHEOLOGICAL EFFECTS OF MODERATE RED WINE CONSUMPTION ................ 16
METHODS ...................................................................................................................... 16
Subjects ............................................................................................................................................ 16
Blood sampling ................................................................................................................................. 17
Hemorheological measurements ..................................................................................................... 17
Hematocrit ................................................................................................................................................... 17
Plasma and whole blood viscosity ................................................................................................................ 17
Hematocrit per whole blood viscosity ratio ................................................................................................. 18
Red blood cell aggregation ........................................................................................................................... 18
Red blood cell deformability ........................................................................................................................ 20
Statistical analysis ............................................................................................................................ 21
RESULTS ......................................................................................................................... 21
Subjects ............................................................................................................................................ 21
Hematocrit ....................................................................................................................................... 22
Viscosity ............................................................................................................................................ 22
Hematocrit per whole blood viscosity ratio ...................................................................................... 23

2
Red blood cell aggregation ............................................................................................................... 23
Red blood cell deformability ............................................................................................................. 24
DISCUSSION .................................................................................................................... 25
Hematocrit ....................................................................................................................................... 25
Plasma and whole blood viscosity .................................................................................................... 25
Hematocrit per whole blood viscosity ratio ...................................................................................... 26
Red blood cell aggregation ............................................................................................................... 26
Red blood cell deformability ............................................................................................................. 27
CONCLUSIONS ................................................................................................................. 27
HEMORHEOLOGICAL PARAMETERS IN CT-DETECTED CORONARY ARTERY DISEASE.. 28
METHODS ...................................................................................................................... 28
Patients ............................................................................................................................................ 28
Blood sampling ................................................................................................................................. 28
Coronary computed tomography angiography ................................................................................ 29
Hemorheological measurements ..................................................................................................... 29
Central laboratory measurements ................................................................................................... 30
Classification of patients .................................................................................................................. 30
Statistical analysis ............................................................................................................................ 30
RESULTS ......................................................................................................................... 31
Subject characteristics ...................................................................................................................... 31
Hemorheological parameters ........................................................................................................... 32
Hematocrit ................................................................................................................................................... 32
Plasma and whole blood viscosity ................................................................................................................ 32
Red blood cell aggregation ........................................................................................................................... 34
Red blood cell deformability ........................................................................................................................ 34
Central laboratory parameters ......................................................................................................... 35
DISCUSSION .................................................................................................................... 36
Subject characteristics ...................................................................................................................... 36
Hematocrit ....................................................................................................................................... 36
Plasma and whole blood viscosity .................................................................................................... 37
Red blood cell aggregation ............................................................................................................... 38
Red blood cell deformability ............................................................................................................. 39
Other laboratory parameters ........................................................................................................... 39
Study limitations ............................................................................................................................... 40
CONCLUSIONS ................................................................................................................. 41
SUMMARY OF NEW SCIENTIFIC RESULTS ................................................................ 42

3
HEMORHEOLOGICAL EFFECTS OF MODERATE RED WINE CONSUMPTION ........................................... 42
HEMORHEOLOGICAL PARAMETERS IN CT-DETECTED CORONARY ARTERY DISEASE ........................... 42
ACKNOWLEDGEMENTS .......................................................................................... 43
REFERENCES ........................................................................................................... 44
PUBLICATIONS OF THE AUTHOR ............................................................................. 55
PAPERS FROM THE TOPICS .................................................................................................. 55
OTHER PAPERS ................................................................................................................ 56
PUBLISHED ABSTRACTS ...................................................................................................... 57

4
Abbreviations and symbols
ACEI angiotensin-converting enzyme inhibitor
AFRW alcohol free red wine extract
AI LORCA aggregation index
ARB angiotensin-receptor blocker
ASA acetylsalicylic acid
BMI body mass index
CABG coronary artery bypass grafting
CAD coronary artery disease
CHD coronary heart disease
CLP clopidogrel
CT computed tomography
CV cardiovascular
CVD cardiovascular disease
DM diabetes mellitus
EI elongation index
Hct hematocrit
HDL high density lipoprotein
Hgb hemoglobin
LDL low density lipoprotein
LORCA Laser-assisted Optical Rotational Cell Analyzer
M Myrenne aggregation index (M mode)
M1 Myrenne aggregation index (M1 mode)
MCH mean corpuscular hemoglobin
MCHC mean corpuscular hemoglobin concentration
MCV mean corpuscular volume
NSAID non-steroid anti-inflammatory drug
PCI percutaneous coronary intervention
PTP pre-test probability

5
PV plasma viscosity
RBC red blood cell
SDR standardized death ratio
S.E.M standard error of mean
t½ LORCA aggregation half time
WBV whole blood viscosity
WHO World Health Organization

6
Introduction
The burden of cardiovascular diseases
Cardiovascular diseases (CVDs) are the leading cause of death globally. In 2008, around
17.3 million people died of CVDs, representing 30% of total global deaths, of which an
estimated 7.3 million were due to coronary heart disease (CHD). In the high-income
countries, cardiovascular (CV) mortality is decreasing due to the improving prevention
programs and healthcare system, however in the low- and middle-income countries it
increases in a very fast rate. Contrary to popular opinion, over 80% of CV deaths take
place in the low- and middle-income countries, thus in spite of the decreasing trend in
the high-income countries, the global CV mortality is still expected to rise in the future:
by 2030 it is projected to reach 23.3 million and to remain the number one cause of
death. Most of these events could be prevented, therefore further research of their risk
factors, pathogenesis and prevention is essential. In Hungary – considered as an “upper
middle income” country – CV mortality is decreasing since 1993 [standardized death
ratio (SDR), 1993: 640.48/100,000], but it is still much higher [SDR, 2011:
402.08/100,000] compared to the European Union members before May 2004 [SDR,
2011: 160.11/100,000] (Mathers & Loncar, 2006; World Health Organization, 2008;
World Health Organization, 2011; World Health Organization, 2013; World Health
Organization, 2014).
The French paradox
Series of prospective epidemiological studies, such as the Framingham Study (Gordon &
Kannel, 1984), the British Doctors Study (Doll, et al., 2005), the Nurses Health Study
(Fuchs, et al., 1995; Mukamal, et al., 2005), the Physicians’ Health Study (Gaziano, et al.,
2000), the British Heart Study (Emberson, et al., 2005) and the Copenhagen Heart Study
(Schnohr, et al., 2002) observed a J-shaped relationship between the relative risk of CHD
and alcohol intake. According to these studies, low to moderate consumption of

7
alcoholic beverages is associated with reduced risk of CHD, while on the other hand,
binge or heavy drinking increases the risk of CHD. A meta-analysis reported that light or
moderate alcohol consumption may also be protective against total and ischemic stroke,
while heavy alcohol consumption increased their relative risk (Reynolds, et al., 2003).
According to another meta-analysis, involving 34 studies, consumption of alcohol, up to
2 drinks/day in women and 4 drinks/day in men is inversely associated with total and CV
mortality, while higher doses of alcohol are associated with increased mortality (Di
Castelnuovo, et al., 2006).
Further studies have described that wine is more beneficial than any other forms
of alcohol. According to the Copenhagen City Heart Study, low-to-moderate intake of
wine is associated with lower mortality from CV and cerebrovascular diseases, while
similar intake of spirits increases and beer drinking does not affect mortality (Gronbaek,
et al., 1995). A prospective cohort study, carried out in France, reported that moderate
consumption of either beer or wine lowered the risk of CV deaths, but the effect of wine
was more significant. In case of all-cause mortality only wine was associated with
reduced relative risk (Renaud, et al., 1999). A meta-analysis processing 26 studies found
a significant inverse association between low to moderate wine consumption and
vascular risk. Beer drinking was also associated with reduced risk of vascular events, but
failed to show any significant correlation between different amounts of beer intake and
vascular risk (Di Castelnuovo, et al., 2002). Several papers suggest that the greater
benefit seen in wine drinkers compared to other alcohol consumers can also be
attributed to the wine drinkers’ advantageous lifestyle characteristics (Wannametheem
& Shaper, 1999).
The beneficial effect is likely to depend on the type of wine. In spite of the much
lower cholesterol levels in Alsace, a white wine drinking region in France, higher
mortality rates were observed there, compared to the red wine drinking Mediterranean
regions (Opie & Lecour, 2007). Studies examining alcohol free red wine extract (AFRW)
also support that red wine has additional positive effects beyond alcohol alone. In 1993
Frankel, et al. found that 1000-fold diluted red wine inhibited copper-catalyzed low
density lipoprotein (LDL) oxidation, significantly more than alpha-tocopherol, a known
antioxidant. In another study 113 ml of AFRW, but not white wine increased total plasma

8
antioxidant capacity 50 minutes after its ingestion (Serafini, et al., 1998). In a double-
blind, cross-over study either 250 ml of red wine or AFRW decreased arterial stiffness in
patients with coronary artery disease (CAD) (Karatzi, et al., 2005).
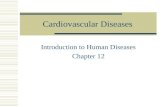
Total mortality is not, but mortality from CVDs is much lower in France than in
other Western-European countries [Fig. 1.1.], although the consumption of saturated
fats [Fig. 1.2.] and blood cholesterol level – considered as major CV risk factors – are
higher in this country. Furthermore, prevalence of other risk factors such as smoking
and hypertension are similar in France as in other developed regions of Europe.
According to epidemiological studies, this phenomenon, called as “French paradox”,
may be caused by the moderate and regular consumption of red wine [Fig. 1.3.] (St
Leger, et al., 1979; Renaud & de Lorgeril, 1992; Renaud, et al., 1999; de Lorgeril, et al.,
2002; Opie & Lecour, 2007; World Health Organization, 2014).
Literature data exist that these epidemiological findings are confounded by
social, cultural, lifestyle and dietary factors. A cross-sectional survey, carried out at the
French MONICA Centers, found that healthy diet and behaviors are more often observed
in wine drinkers than in beer or spirit consumers (Ruidavets, et al., 2004). Another
published confounding factor is called “time lag” hypothesis which states that in the
1960s fat intake was lower in France than nowadays, and it takes about 25-35 years till
dietary changes manifest in mortality data (Law & Wald, 1999).
<= 900
<= 700
<= 500
<= 300
<= 200
<= 125
No data
Min = 100
SDR, diseases of circulatory system, all ages, per 100 000
2009
European Region
384.66
Fig. 1.1. Mortality due to circulatory diseases in Europe, 2009. Source: World Health Organization, HFA-DB. Updated: April 2014.

9
According to several in vitro and in vivo studies, the favorable effect of red wine
may originate from its alcoholic and non-alcoholic components. Moderate intake of
alcohol lowers platelet aggregation and fibrinogen level (Renaud & Ruf, 1996), increases
high density lipoprotein (HDL) level (McConnell, et al., 1997), tissue-type plasminogen
activator level (Ridker, et al., 1994; Aikens, et al., 1998) and production of endothelial
nitrogen monoxide (Abou-Agag, et al., 2005), decreases insulin level and improves
insulin sensitivity (Davies, et al., 2002).
<= 7
<= 6.5
<= 5
<= 3.5
<= 2
<= 0.5
No data
Min = 0
Wine consumed in pure alcohol, litres per capita, age 15+
2009
European Region
2.71
Fig. 1.3. Wine consumption in Europe, 2009. Source: World Health Organization, HFA-DB. Updated: April 2014.
<= 200
<= 160
<= 120
<= 80
No data
Min = 40
Fat available per person per day (g)
2009
European Region
No data
Fig. 1.2. Fat intake in Europe, 2009. Source: World Health Organization, HFA-DB. Updated: April 2014.

10
Non-alcoholic part of red wine contains polyphenols and anthocyanins.
Anthocyanins are responsible for the color of wines, while polyphenols are considered
as the main source of cardiovascular protection. From this group resveratrol, catechin
and quercetin have been extensively studied and their antioxidant properties have been
reported (Frankel, et al., 1993; Rice-Evans, et al., 1996; Kerry & Abbey, 1997; Serafini, et
al., 1998). The resveratrol content of red wine depends on vintage year and variety
(Edelmann, et al., 2001; Casavecchia, et al., 2007), winemaking technology and winery
regions (Goldberg, et al., 1995; Kontkanen, et al., 2005; Avar, et al., 2007). It has been
revealed that polyphenols increase production of nitrogen monoxide (Leikert, et al.,
2002), inhibit platelet aggregation and decrease the production of proinflammatory
eicosanoids (Pace-Asciak, et al., 1995; Soleas, et al., 1997). Polyphenols also decrease
the oxidation of LDL (Frankel, et al., 1993; Teissedre, et al., 1996), Apo B100 production
and increase the expression of LDL receptors (Pal, et al., 2003).
Hemorheological parameters as cardiovascular risk factors
Decades ago prospective epidemiological studies – such as the Framingham Study –
identified the conventional risk factors of CAD: age, male gender, arterial hypertension,
smoking, diabetes mellitus, dyslipidemia, obesity, stress, low physical activity and
positive family history. Reduction of the modifiable risk factors help to considerably
prevent CV events, but not all the CV events can be explained by the presence of the
classical risk factors thus further investigation of new risk factors is necessary. Further
studies have revealed several additional risk factors: abnormal hemorheological
parameters, hyperuricemia, metabolic syndrome, hyperhomocysteinemia, infections
(e.g. Chlamydia pneumoniae), chronic inflammation, microalbuminuria, chronic renal
failure, oxidative stress, air pollution, noise pollution, carotid intima/media thickness
and high resting heart rate.
The alterations of hemorheological parameters in CAD have been described by
several prospective epidemiological studies. Moreover the Framingham Study (Kannel,

11
et al., 1987), the Edinburgh Artery Study (Lowe, et al., 1993; Lee, et al., 1998), the
MONICA-Augsburg Cohort Study (Koenig, et al., 1998), the Physicians' Health Study (Ma,
et al., 1999), the Caerphilly Study and the Speedwell Study (Yarnell, et al., 1991;
Sweetnam, et al., 1997) identified elevated hematocrit (Hct), whole blood viscosity
(WBV), plasma viscosity (PV) and plasma fibrinogen level as primary CV risk factors. In
the Physicians' Health Study elevated plasma fibrinogen level, independently of other
CV risk factors, was associated with increased risk of future myocardial infarct (Ma, et
al., 1999). In the Edinburgh Artery Study WBV, PV and fibrinogen level correlated linearly
with carotid intima/media thickness even on multivariate analysis. After adjusting all
common CV risk factors, elevated WBV and fibrinogen level still significantly correlated
with carotid intima/media thickness. These results suggest that altered hemorheological
parameters are associated not just with CVDs, but also with the early stages of
atherosclerosis (Lee, et al., 1998).
Clinical importance of hemorheological parameters in cardiovascular diseases
In spite of the systemic nature of CV risk factors, atherosclerotic lesions do not occur
randomly in the vascular system. These lesions tend to develop at specific locations – at
the outer wall of vessel bifurcations, the inlet of branches and the inner, distal wall of
arterial curvatures – suggesting the importance of hemodynamic and hemorheological
factors in their pathogenesis (Chien, et al., 1987; Toth & Kesmarky, 2007). The fact that
hemorheological alterations appear prior to the development of vascular lesions
suggests that they could play a role in the pathogenesis of the atherosclerotic process.
(Vaya, et al., 1996; Toth & Kesmarky, 2007).
The coronary vessel system is a unique part of the human vascular structure due
to the periodic change in perfusion pressure and blood flow. Moreover, it has the
narrowest capillaries in the human vascular system, thus hemorheological alterations
might have a more significant impact on myocardial perfusion compared to other
organs. At normal circumstances coronary blood flow is mainly determined by

12
hemodynamic factors, but in certain conditions, such as a pre-existing coronary stenosis,
alteration of hemorheological parameters may early impair myocardial microcirculation
(Dintenfass, 1969; Chien, et al., 1987; Baskurt, et al., 1991; Toth & Kesmarky, 2007).
Hematocrit
Hct and its determinants, such as RBC count and mean corpuscular volume (MCV), affect
most of the other hemorheological parameters. Both low and high Hct can impair tissue
oxygen supply by either lowering the oxygen binding capacity or increasing WBV and
flow resistance. Elevated Hct has been identified as a CV risk factor by several
epidemiological studies. Furthermore, epidemiological data suggest that increased Hct
even within the normal range is a risk factor of acute myocardial infarct (Toth &
Kesmarky, 2007).
Plasma and whole blood viscosity
Due to the axial migration of RBCs, the mechanical influence of blood flow is mediated
through the plasma. PV is an important parameter determining wall shear stress
(Cabrales & Tsai, 2006) and flow resistance in the microcirculation (Meiselman &
Baskurt, 2006). It has also been demonstrated that PV plays a significant role in the
regulation of vascular tone (Tsai, et al., 1998; Cabrales & Tsai, 2006).
WBV is a major determinant of flow resistance. In case of high WBV, flow
resistance increases, while flow rate decreases proportionally. To maintain adequate
flow, elevated blood pressure and cardiac work is required. The increased stress both to
the heart and the vessels promote cardiac and vascular remodeling, leading to heart
failure and accelerated atherosclerosis. Elevated WBV has also been identified as a CV
risk factor by numerous epidemiological studies.
Red blood cell aggregation
At constant Hct and temperature, RBC aggregation is the primary determinant of low
shear blood viscosity (Cokelet & Meiselman, 2007). Enhanced RBC aggregation alters

13
both macro- and microrheological properties of blood, and can either decrease or
increase flow resistance at different sites of the circulation (Baskurt & Meiselman, 2007).
RBC aggregation is determined by several factors: by membrane surface adhesion
molecules, type and concentration of macromolecules in the plasma, such as fibrinogen.
Alteration of any of the mentioned factors alters RBC aggregation and thus blood flow
characteristics (Cokelet & Meiselman, 2007).
Red blood cell deformability
Deformability of RBCs is essential to pass through the coronary capillaries being
narrower than the cell itself. As mentioned earlier, coronary capillaries are the
narrowest in the human body, therefore perfusion insufficiency due to impaired RBC
deformability may firstly manifest in the myocardium. RBC deformability impairment
may seriously reduce myocardial oxygen supply even in case of normal epicardial vessels
by increasing flow resistance in the capillaries (Baskurt & Meiselman, 2007; Toth &
Kesmarky, 2007).

14
Aims
Atherosclerosis of the coronary arteries starts in the early childhood and progresses
asymptomatically until a significant stenosis develops or a plaque rupture causes acute
coronary syndrome. Hemorheological parameters have been identified as CV risk factors
and supposed to play a pathophysiological role in the development of atherosclerosis.
Our two studies were designed to investigate the alterations of hemorheological factors
in two distant points of the atherosclerotic process: in healthy subjects, on one side and
in patients with CAD, on the other side.
Hemorheological effects of moderate red wine consumption
Until now only, a limited number of controlled studies have reported the medium term
effects of regular red wine intake on hemorheological parameters in healthy volunteers
(Jensen, et al., 2006; Kaul, et al., 2010). These experiments gave information about PV,
WBV and RBC deformability, but no literature data have been found about RBC
aggregation. Our previous in vitro experiments showed that red wine, AFRW and ethanol
significantly and dose dependently decrease RBC aggregation (Rabai, et al., 2010; Rabai,
et al., 2014). In our current study we aimed to confirm the in vitro findings and examine
the effects of moderate red wine consumption on hemorheological parameters,
including viscosity, RBC aggregation and deformability. Ours is the first prospective,
controlled study which examined a complete hemorheological panel in this field.
Hemorheological parameters in CT-detected coronary artery disease
Previous clinical studies reported significantly elevated Hct, WBV, PV, fibrinogen level
and RBC aggregation in CAD (Lowe, et al., 1980; Rainer, et al., 1987; Lee, et al., 2008),

15
however only a few were able to detect statistically significant differences between the
various stages of CAD (Neumann, et al., 1989; Kesmarky, et al., 1998).
Our previous study showed significantly increased Hct, WBV, PV and fibrinogen
levels in CAD compared to healthy controls, moreover significant differences were found
between CAD subgroups, suggesting a correlation with the severity of CAD (Kesmarky,
et al., 1998).
We aimed to conduct a full scale hemorheological study on patients with CAD,
including the measurement of RBC aggregation and deformability which was not carried
out previously. To the best of our knowledge, all previous studies used invasive coronary
X-ray angiography to evaluate for CAD. In our current study, a new and well established
method, coronary CT angiography was used for the evaluation of the coronary vessel
system. This method is able to measure coronary stenosis precisely and can also
determine the total extent of coronary calcification.

16
Hemorheological effects of moderate red wine consumption
Methods
Subjects
The study was approved by the Regional Ethics Committee of the University of Pecs and
written informed consent was signed by all subjects. Forty healthy, non-smoking male
volunteers between the ages of 18-40 were enrolled. None of them had taken any drugs
for one week prior entering the study and during the whole duration of it. In order to
eliminate any possible effect of the previously consumed alcoholic beverages, no alcohol
consumption was allowed in the first 7 days of the study. On the morning of the 8th day
the subjects were assigned into 2 groups:
In the control group, volunteers drunk mostly water for 3 weeks, coffee and soft
drinks were permitted, no alcohol consumption was allowed.
In the red wine group, 2 dl of red wine (2007 Merlot, Polgar Winery, Villany,
Hungary; resveratrol content ≈ 4 mg/l, ethanol content ≈ 13.5 V/V%) was
consumed each day during dinner for 3 weeks, no other forms of alcoholic
beverages were allowed [Fig. 2.1.].
40 healthy young subjects
1st
– 7th
days: no alcohol consumption
Control group No alcohol Mostly tap water Soft drinks and coffee
allowed
Red wine group 2 dl of red wine for dinner No other alcohol Additional fluid intake
similarly to control group
29th
day: 3-week blood samples
8th
day: baseline blood samples
Fig. 2.1. Study protocol.

17
Blood sampling
After fasting for 12 hours, in the mornings of the 8th and 29th days, 17 ml of antecubital
venous blood samples were obtained into Li-heparin coated BD Vacutainer® tubes with
a 21-gauge butterfly needle set with a minimal tourniquet, according to the latest
guideline for hemorheological laboratory techniques (Baskurt, et al., 2009). Blood
samples were stored at ambient temperature until hemorheological measurements.
Hemorheological measurements
Hemorheological measurements were performed within 1 hour from blood sampling at
the Hemorheological Laboratory of the 1st Department of Medicine, University of Pecs
Medical School.
Hematocrit
The anticoagulated blood samples were placed into a native capillary then centrifuged
with Haemofuge microhematocrit centrifuge (Heraeus; Germany) at 12,000 RPM for 3
minutes at room temperature (22±1°C). Hct was determined by the fraction of volume
occupied by RBCs. For further measurements Hct
was adjusted to 40% with autologous plasma.
Plasma and whole blood viscosity
PV and WBV were measured by Hevimet 40 capillary
viscometer (Hemorex; Budapest, Hungary) [Fig.
2.2.]. Plasma was obtained by centrifugation of
blood samples at 2500 g for 10 minutes at 22°C
(Labofuge 400 R, Heraeus; Germany).
The viscometer is composed of a vertical
glass tube and 40 diodes placed next to it. 620 μl of
fluid is injected into the system and released to flow
out, while the height of the fluid column is registered
in the function of time. The height of each diode
vacuum
light source
glass tube
capillary
height of fluid column
sample
oil bath
Fig. 2.2. Hevimet 40 capillary viscometer.

18
from the baseline of the fluid column is known, thus the flow maintaining hydrostatic
pressure and shear stress at each point can be calculated. For the same points, flow
velocity and shear rate is calculated from the height-time function. From the shear stress
and shear rate data points, viscosity values are determined. Viscosity values
interpolated at 90 s-1 shear rate were used in our study. Measurements were performed
at 37 °C temperature.
Hematocrit per whole blood viscosity ratio
From Hct and WBV data, Hct/WBV ratio
was calculated to determine rheological
oxygen carrying capacity of blood.
Oxygen binding capacity linearly,
viscosity and flow resistance
exponentially increases with Hct. In
healthy subjects Hct/WBV ratio reliably
reflects rheological oxygen carrying
capacity of blood (Bogar, et al., 2005).
Values of Hct/WBV in the function of
Hct results in an inverted U-shaped
curve [Fig. 2.3.] (Kenyeres, 2010). Both
in anemia and polycythemia oxygen
supply is impaired and lower Hct/WBV ratios are calculated. In case of anemia, low
oxygen transport originates from low oxygen binding capacity, while in polycythemia
the decreased flow velocity is responsible for the clinical symptoms. A study from our
research group demonstrated that unfavorable Hct/WBV ratio in patients with CHD is
associated with increased risk of cardiac morbidity and mortality (Kenyeres, et al., 2008).
Red blood cell aggregation
RBC aggregation was measured by Myrenne (MA-1 Aggregometer, Myrenne GmbH;
Roetgen, Germany) and LORCA (Laser-assisted Optical Rotational Cell Analyzer; R&R
Mechatronics; Hoorn, The Netherlands) aggregometers. Blood samples were taken from
the same tube.
Fig. 2.3. Hct/WBV ratio at different Hct-s and shear rates.
Source: Kenyeres P., PhD dissertation. University of Pecs, Medical School, 2010.
With the Author’s approval.
Hct (%)
Hct
/WB
V (
mP
a-1s-1
)

19
Myrenne aggregometer [Fig. 2.4.]
employs the light transmission method of
Schmid-Schonbein through a transparent
cone-plate shearing instrument (Klose, et
al., 1972). 30 µl of blood is injected between
the glass cone and plate. The sample is
sheared at 600 s-1 to disperse all pre-existing RBC aggregates, then shear rate falls to
zero (in M mode) or to 3 s-1 (in M1 mode). The instrument measures the infrared light
intensity passing through the blood sample: as RBCs aggregate the light intensity
gradually increases. The extent of aggregation was characterized by the aggregation
indices (M, M1) calculated from the surface area under the light intensity curve in a 10
s period of time (Vaya, et al., 2003). Measurements were performed at room
temperature (22±1 °C).
LORCA aggregometer [Fig. 2.5.] detects the laser back-scattering generated by
the RBCs. To increase back-scattering, blood samples were oxygenated by incubation
with 10-times higher volume of air on a rollerbank for 15 minutes. 1 ml of oxygenated
blood was injected into the gap between the static inner glass cylinder and the rotating
outer glass cylinder which creates a simple shear flow. RBCs are first disaggregated at
500 s-1 shear rate, then shear rate falls to zero. During RBC aggregation, the intensity of
back-scattering laser light is drawn in the function of time (syllectogram) [Fig. 2.6.].
Aggregation behavior of blood was characterized by:
detector
infrared light source
blood sample
glass plate (static)
glass cone (rotating)
Fig. 2.4. Myrenne RBC aggregometer.
laser diode
sample
outer cylinder
inner cylinder
diffraction pattern
camera system
photo diodes (for measurement of
RBC aggregation)
Fig. 2.5. LORCA; RBC aggregation and laser diffraction ellipsometry measurements.

20
the aggregation index (AI), calculated from the first 10 seconds of the syllectogram
after the shape recovery period: AI = A/(A+B) [Fig. 2.6.]
and the time that elapses until peak intensity is reduced by half the amplitude (t½)
(Hardeman, et al., 2001; Dobbe, 2003).
During the measurements temperature was kept at 37 °C. Analyses were performed on
LORCA Aggregation Program v2.1.
Red blood cell deformability
RBC deformability was measured by LORCA [Fig. 2.5.], using the laser diffraction
ellipsometry technique. 25 μl of blood was suspended in 5 ml of high viscosity (32.6
mPas) polyvinylpyrrolidone (Sigma-Aldrich, 360 kDa) solution dissolved in phosphate
buffered saline (290 mOsm/kg, pH = 7.4). 1 ml of this suspension was injected into the
gap between the two cylinders. RBCs are deformed by various shear stresses, generated
0.0
0.7
0.1
Shear stress (Pa)
Elo
ng
ati
on
in
de
x (
EI)
0.6
0.5
0.4
0.3
0.3
-0.1
A
B
EI = (A-B) / (A+B) 0.30 1.00 10.00 30.00
Time (s)
0.01 0.10 10.00 1.00 120.00 0.0
10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0
100.0
Isc
(au
)
shape recovery aggregation
B
A amplitude
AI = A/(A+B)
Fig. 2.6. LORCA syllectogram.
Fig. 2.7. Diffraction pattern and deformability curve.

21
by the rotation of the outer cylinder, meanwhile a laser diode is projecting through the
sample. The elongated RBCs create a laser diffraction pattern captured by a video
camera and analyzed by LORCA Elongation Program v2.1.
RBC deformability was characterized by the elongation index (EI), calculated
from the two radiuses of the ellipsoid diffraction pattern as (A-B)/(A+B), at shear stresses
from 30 Pa to 0.3 Pa. From these data the deformability curve was drawn [Fig. 2.7.]
(Hardeman, et al., 1994; Dobbe, 2003).
Statistical analysis
Continuous variables are presented as mean values ± S.E.M. Differences were analyzed
using paired (dependent samples between baseline and 3rd week results) and un-paired
(independent samples between the control and the red wine group) Student’s t-test. A
two-tailed p value less than 0.05 was considered statistically significant.
Results
Subjects
There was no significant difference between the control and the red wine group in age,
body mass index (BMI) and average physical activity [Table 2.1.]. One volunteer from
the wine drinking group was withdrawn due to complaints of heartburn.
Table 2.1.
Subject characteristics.
Control group Red wine group
Age (years) 27.5 ± 1.2 26.8 ± 1.0
BMI (kg/m2) 24.9 ± 0.87 23.9 ± 0.64
Physical activity score 3.0 ± 0.2 3.1 ± 0.2 Physical activity score: 1: none, 2: monthly, 3: weekly, 4: daily, 5: professional

22
Hematocrit
Red wine consumption had no effect on Hct and no difference was found between the
two groups neither at baseline, nor after 3 weeks [Table 2.2.].
Table 2.2.
Hemorheological parameters.
Baseline 3 weeks
Control Red wine Control Red wine
Hct (%) 47.8 ± 0.6 46.6 ± 0.5 47.4 ± 0.7 46.4 ± 0.5
PV 1.27 ± 0.02 1.25 ± 0.03 1.26 ± 0.02 1.26 ± 0.02
WBV (mPa·s) 3.9 ± 0.1 3.8 ± 0.1 3.9 ± 0.1 3.7 ± 0.1c
Hct/WBV
(mPa-1s-1)
10.4 ± 0.3 10.7 ± 0.2 10.4 ± 0.3 11.0 ± 0.3c
M 8.6 ± 0.7 9.0 ± 0.4 8.1 ± 0.5 8.1 ± 0.3b
M1 16.0 ± 0.7 15.2 ± 0.7a 14.1 ± 0.6a 12.8 ± 0.4b,c
AI 57.2 ± 2.2 55.4 ± 1.7 54.1 ± 1.9 53.5 ± 1.8b
t½ (s) 2.9 ± 0.3 3.2 ±0.3 3.4 ± 0.3 3.5 ± 0.3b
EI (at 30 Pa) 0.631 ± 0.002 0.630 ± 0.003 0.632 ± 0.002 0.632 ± 0.003b a: significant (p<0.05) difference compared to the control group at baseline b: significant (p<0.05) difference compared to the red wine group at baseline c: significant (p<0.05) difference compared to the control group after 3 weeks
Viscosity
PV did not change during the 3 weeks in either group compared to baseline, and there
was no significant difference between the two groups nor at baseline, neither after 3
weeks [Table 2.2.].
Adjusted WBV remained constant in the control group, while in the red wine
group it decreased, and after 3 weeks WBV in the red wine group became significantly
lower compared to the control group (p<0.05) [Table 2.2.].

23
Hematocrit per whole blood viscosity ratio
The Hct/WBV ratio remained steady during the 3 weeks in the control group, while in
the red wine group the parameter tended to increase compared to baseline. After 3
weeks, significantly higher (p<0.05) ratio was calculated in the red wine group compared
to the control group [Table 2.2., Fig. 2.8.].
Fig. 2.8. Change in hematocrit/adjusted whole blood viscosity ratio. Arrow represents significant (p<0.05) difference.
Red blood cell aggregation
Both Myrenne (M and M1) and LORCA aggregation indices significantly decreased
(p<0.05) in the red wine group [Table 2.2., Fig. 2.9., 2.10.]. LORCA t½ also indicates
significantly (p<0.05) decreased RBC aggregation in the red wine group [Table 2.2.].
Furthermore, after 3 weeks, Myrenne M1 parameter was also significantly lower
(p<0.05) in the red wine group compared to the control group. M1 significantly
decreased (p<0.05) in the control group after 3 weeks, but none of the other RBC
aggregation parameters (M, AI, t½) showed a significant change [Table 2.2., Fig. 2.9.,
2.10.].
90
95
100
105
110
115
Baseline 3 weeks
1/(
Pa·
s)
Hct/WBV ratio (40%)
Control Red wine

24
Fig. 2.9. Red blood cell aggregation in adjusted samples measured by Myrenne. Arrow represents significant (p<0.05) difference.
Fig. 2.10. Red blood cell aggregation in adjusted samples measured by Myrenne.
Arrows represent significant (p<0.05) differences.
Red blood cell deformability
At the highest shear stress (30 Pa), the EI significantly increased (p<0.05) in the red wine
group after 3 weeks compared to baseline, while it did not change in the control group
[Table 2.2.].
5.0
6.0
7.0
8.0
9.0
10.0
Baseline 3 weeks
Myrenne M (40%)
Control Red wine
5
7
9
11
13
15
17
19
Baseline 3 weeks
Myrenne M1 (40%)
Control group Red wine group

25
Discussion
Only limited data have been presented on the hemorheological consequences of
medium and long-term red wine consumption. Several studies have demonstrated an
inverse association between red wine or polyphenol intake and cardiovascular events,
but not all sources of this cardioprotective effect are known. Most authors have
emphasized the effect of elevated HDL level, decreased platelet aggregation and
fibrinogen level, thus these were mostly examined. In a randomized crossover study,
five-week red wine consumption significantly decreased collagen-induced platelet
aggregation and increased HDL level (Pikaar, et al., 1987), moreover in another study
collagen-induced platelet aggregation and fibrinogen level were significantly reduced
after 4-week red wine intake (Pellegrini, et al., 1996).
Only a few controlled results are known about other important hemorheological
parameters – such as PV, WBV, RBC aggregation and RBC deformability – in healthy
human subjects consuming red wine. A randomized controlled study reported that
moderate red wine consumption (6 or 12 ounces/day; ≈ 1.77 or 3.55 dl/day), up to 2
weeks, significantly increased HDL level, but it did not change Hct, WBV, RBC
deformability and fibrinogen level (Kaul, et al., 2010). Another controlled experiment
observed significantly reduced PV and fibrinogen level after 3-week moderate red wine
intake (Jensen, et al., 2006). Our prospective, controlled study presents new data about
the in vivo hemorheological effects of moderate red wine consumption.
Hematocrit
Red wine consumption had no significant effect on Hct, confirming the results of Kaul,
et al. (2010). In order to completely eliminate the influence of Hct on the dependent
hemorheological parameters (WBV and RBC aggregation) Hct was standardized to 40%.
Plasma and whole blood viscosity
PV did not change significantly after 3-week red wine consumption. Although we did not
measure plasma fibrinogen level (the main determinant of PV), Kaul, et al. (2010)

26
reported no significant change after 2 weeks of red wine intake. On the other hand,
lower plasma viscosity and fibrinogen level were measured after 3 weeks in a different
study (Jensen, et al., 2006).
The observed reduction of WBV in the red wine group may result from the
reduction of RBC aggregation and the increased RBC deformability. Red wine
consumption increased WBV of Hct-standardized samples after 3 hours, but no
difference from baseline was observed 13 hours after ingestion (Fehr, et al., 2008). This
suggests that the observed reduction of WBV in our study was not due to the short-term
effect of the red wine, consumed in the previous evening. Kaul, et al. (2010) found no
changes after 2 weeks of red wine consumption, but Jensen, at al. (2006) reported
decreased WBV after 3 weeks. It is assumed that more time is required until the effect
can be detected.
Hematocrit per whole blood viscosity ratio
The significantly higher Hct/WBV ratio in the red wine group (due to unaffected Hct and
lowered WBV) means greater oxygen carrying capacity of the blood.
Red blood cell aggregation
The reduction of RBC aggregation was observed both by Myrenne and LORCA in the red
wine group. These findings confirm our previous in vitro results, where red wine, AFRW
and ethanol inhibited RBC aggregation (Rabai, et al., 2010; Rabai, et al., 2014). The
decrease of RBC aggregation may be a consequence of the modifications of plasma
proteins. It is known that polyphenols, such as resveratrol, are bounded to plasma
proteins due to their poor water solubility. The phenol-protein interactions may change
the properties of plasma proteins and RBC surface molecules, therefore reducing the
capability to form cross links between cellular components and decreasing RBC
aggregation. It has been reported that resveratrol binding to albumin or hemoglobin
changes their secondary structures (Lu, et al., 2007). The absorption of resveratrol in
humans is about 70%, but due to the extensive metabolism, resveratrol is mostly
present in sulphate and glucuronide conjugated forms and only minimal amounts of

27
unchanged resveratrol can be detected in the plasma (Walle, et al., 2004). The reported
fibrinogen lowering effect of red wine (Jensen, et al., 2006) may also be a reason of the
observed decrease in RBC aggregation.
Red blood cell deformability
RBC deformability was enhanced at the highest shear stress in the red wine group. EI at
30 Pa approximates the maximal deformability of RBCs. In our earlier in vitro study, no
significant changes were observed after direct addition of red wine or AFRW to the blood
samples (Rabai, et al., 2010). It was assumed that under no significant oxidative stress,
RBC of healthy humans has optimal deformability; therefore no further improvement
could be expected. On the other hand, RBC deformability even of healthy volunteers
could be improved with moderate red wine consumption. Contrarily, another study
reported no significant changes in RBC deformability after 2 weeks of red wine
consumption (Kaul, et al., 2010). It is possible again, that more time is required till the
changes become significant.
Conclusions
This in vivo study confirmed our previous in vitro findings about the beneficial
hemorheological effects of ethanol, AFRW and red wine on RBC aggregation. Decreased
WBV, RBC aggregation, higher calculated oxygen carrying capacity and increased RBC
deformability may positively affect microcirculation. These findings may take part in the
cardiovascular protection of moderate red wine consumption.

28
Hemorheological parameters in CT-detected coronary artery disease
Methods
Patients
The study was approved by the Regional Ethics Committee of the University of Pecs. 130
patients, admitted to coronary CT angiography at the Department of Radiology,
University of Pecs Medical School, participated in the study. Informed consent was
signed by all subjects prior to enrollment. Patients were questioned regarding previous
medical history and existing medications. Patients with autoimmune disorders or
malignancies were not enrolled.
Blood sampling
Blood samplings were performed according to the latest guideline for hemorheological
laboratory techniques (Baskurt, et al., 2009). Samples were obtained via an antecubital
vein just before the coronary CT examination, using a 21-gauge butterfly needle set with
minimal tourniquet into the following BD Vacutainer® tubes:
2x6 ml Li-heparin anticoagulated (for hemorheological measurements)
3 ml K2EDTA anticoagulated (for qualitative and quantitative blood cell analyses)
2.7 ml Na-citrate anticoagulated (for fibrinogen level)
5 ml SST native (for lipid profile)
Blood samples were stored at ambient temperature until hemorheological
measurements.

29
Coronary computed tomography angiography
Coronary CT angiography examinations were performed at the Department of
Radiology, University of Pecs Medical School with a first generation 64-slice, dual source
Siemens Somatom Definition CT device. The instrument has two X-ray tubes and dual
detector system in perpendicular position: during coronary CT measurements the two
systems work simultaneously, providing better temporal resolution, which reduces the
presence of motion artefacts (Dérczy & Battyány, 2008).
Prior to the examinations no food or caffeine containing fluid consumption was
allowed for 4 hours. Sublingual nitrate was given to all patients and depending on the
resting heart rate, intravenous beta-blocker was administered. First a native scan was
carried out to estimate total coronary calcification. After that a contrast enhanced scan
was performed to evaluate coronary system. Coronary calcification was characterized
by Agatson-score; lesions were defined as area stenosis. Data processing and image
evaluation was done with Siemens syngo software on Siemens Multimodality
workstation (Dérczy & Battyány, 2008).
Hemorheological measurements
Hemorheological measurements were performed within 2 hours from blood sampling
at the Hemorheological Laboratory of the 1st Department of Medicine, University of Pecs
Medical School. The instruments and measurement protocols used in this study are
identical to the ones in the previous work, therefore only the differences will be detailed
here:
Hct, PV and WBV were measured with the same settings.
RBC aggregation was determined only by Myrenne aggregometer. Both native
samples and suspensions of RBCs, adjusted to 40% Hct with autologous plasma
were measured. Instrument settings were identical.
For RBC deformability measurements, blood was suspended in 29.43 mPas
viscosity polyvinylpyrrolidone solution. Other conditions remained unchanged.

30
Central laboratory measurements
Central laboratory measurements were carried out at the Department of Laboratory
Medicine, University of Pecs Medical School. The following parameters were measured:
Hct, Hgb concentration, RBC count, MCV, MCH, MCHC, LDL, HDL and fibrinogen level.
Classification of patients
Patients were classified into four groups based on their coronary vessel state, according
to Table 3.1.
Table 3.1.
Classification of patients.
Negative
(Neg)
no coronary stenosis or atherosclerotic lesion and
zero calcium-score
Non-significant
(NS)
below 40% area stenosis on one or more coronary vessels and
no PCI or CABG
Single-vessel
(SV)
1. over 40% area stenosis on one coronary vessel or
2. history of PCI or CABG on one coronary vessel
Multi-vessel
(MV)
1. over 40% area stenosis on multiple coronary vessels or
2. over 40% area stenosis on one coronary vessel and history of
PCI or CABG on one coronary vessel or
3. history of PCI or CABG on multiple coronary vessels
Statistical analysis
Continuous variables are presented as mean ± S.E.M. Discrete variables are described
through relative or absolute frequencies. Continuous variables were analyzed with one-
way ANOVA; in case of dichotomous variables χ2 test was used. A two-tailed p value less
than 0.05 was considered statistically significant.

31
Results
Nine patients were excluded from the study due to classification-limiting CT image
quality.
Subject characteristics
There is an increasing trend in average age, BMI and proportion of males in
Negative<Non-significant<Single-vessel<Multi-vessel rank order. The average age in the
Multi-vessel group is significantly higher compared to the Negative group. The
proportion of males is greatly higher in the CAD (Non-significant, Single-vessel and Multi-
vessel) groups compared to the Negative group, and continues to increase in a smaller
extent in the CAD subgroups [Table 2.2.].
The prevalence of hypertension, diabetes mellitus (DM) and smoking has a
similar rank order: Negative<Non-significant<Single-vessel<Multi-vessel. In the Single-
vessel and Multi-vessel groups all of them are significantly higher compared to the
Negative group. PCI and CABG are only present in the Single-vessel and Multi-vessel
groups, being highest in the Multi-vessel group. Ca-score also has the previously
described trend [Table 2.2.].
Table 2.2.
Demographic data, Ca-score, risk factors and revascularization procedures.
Neg NS SV MV
N 32 27 32 30
Age (years) 56.8 ± 2.0 59.2 ± 11.4 58.8 ± 1.5 62.1 ± 1.5a
Males 22 % 70 %a 75 %a 90 %a
BMI (kg/m2) 27.6 ± 0.9 29.3 ± 0.9 29.5 ± 0.8 29.7± 1.0
Ca-score 0 145.7a 264.9a 425.8a,b
Hypertension 66 % 70 % 87 %a 90 %a
DM 6 % 22 % 35 %a 35 %a
Smoking 19 % 33 % 43 %a 45 %a
PCI 0 % 0 % 19 %a,b 33 %a,b
CABG 0 % 0 % 6 % 30 %a,b,c a: significant (p<0.05) difference compared to the Negative group
b: significant (p<0.05) difference compared to the Non-significant group
c: significant (p<0.05) difference compared to the Single-vessel group

32
The use of antiplatelet, statin, angiotensin-converting enzyme inhibitor (ACEI),
angiotensin-receptor blocker (ARB) and beta-blocker medication is already considerable
in the Negative group and follows an increasing trend. The prevalence of acetylsalicylic
acid (ASA), clopidogrel (CLP), statin and beta-blocker medication in the Multi-vessel
group is significantly higher compared to the Negative group. Statin use is significantly
higher in all CAD subgroups compared to the Negative group. Dual anti-platelet therapy
is only used in the Single-vessel and the Multi-vessel groups.
Table 2.3.
Medications.
Neg NS SV MV
Antiplatelet agents:
Mono antiplatelet therapy 41 % 62 % 55 % 57 %
Dual antiplatelet therapy 0 % 0 % 6 % 21 %a,b
ASA 38 % 46 % 58 % 68 %a
CLP 3 % 15 % 10 % 32 %a,c
Statin 31 % 62 %a 58 %a 64 %a
ACEI/ARB 59 % 62 % 68 % 79 %
Beta-blocker 47 % 63 % 61 % 75 %a a: significant (p<0.05) difference compared to the Negative group
b: significant (p<0.05) difference compared to the Non-significant group
c: significant (p<0.05) difference compared to the Single-vessel group
Hemorheological parameters
Hematocrit
Hct increases in a Negative<Non-significant<Single-vessel<Multi-vessel manner. In the
Non-significant, Single-vessel and Multi-vessel groups it is significantly higher compared
to the Negative group [Table 2.4., Fig. 3.1.].
Plasma and whole blood viscosity
No significant difference was found in PV [Table 2.4.]. WBV shows the following rank
order: Negative<Non-significant<Single-vessel<Multi-vessel. WBV in the Multi-vessel
group is significantly higher compared to the Negative group [Table 2.4., Fig. 3.2].

33
Table 2.4.
Hemorheological parameters.
Neg NS SV MV
Hct (%) 42.7 ± 0.4 44.1 ± 0.7a 44.3 ± 0.6a 44.9 ± 0.6a
PV (mPa·s) 1.31 ± 0.2 1.28 ± 0.2 1.29 ± 0.2 1.27 ± 0.2
WBV (mPa·s) 4.3 ± 0.1 4.4 ± 0.1 4.4 ± 0.1 4.5 ± 0.1a
M 5.5 ± 0.3 5.7 ± 0.3 6.1 ± 0.3 6.4 ± 0.3a
M (40 %) 5.9 ± 0.3 6.1 ± 0.4 6.6 ± 0.3 7.0 ± 0.4a, b
M1 12.3 ± 0.3 12.6 ± 0.5 12.8 ± 0.4 13.0 ± 0.4
M1 (40 %) 12.8 ± 0.4 12.9 ± 0.6 13.5 ± 0.4 14.0 ± 0.5a
EI (at 30 Pa) 0.624 ± 0.002 0.620 ± 0.001a 0.622 ± 0.001 0.621 ± 0.002
EI (at 16.8 Pa) 0.594 ± 0.002 0.590 ± 0.001a 0.592 ± 0.002 0.591 ± 0.003 a: significant (p<0.05) difference compared to the Negative group
b: significant (p<0.05) difference compared to the Non-significant group
c: significant (p<0.05) difference compared to the Single-vessel group
Fig. 3.1. Hematocrit. Arrows represent significant (p<0.05) differences.
Fig. 3.2. Whole blood viscosity at 90 s-1 shear rate. Arrow represents significant (p<0.05) difference.
38
39
40
41
42
43
44
45
46
Neg NS SV MV
%
Hematocrit
3.9
4.0
4.1
4.2
4.3
4.4
4.5
4.6
4.7
Neg NS SV MV
mP
a·s
Whole blood viscosity (90 s-1)

34
Red blood cell aggregation
In native samples, both M and M1 parameters increase in Negative<Non-
significant<Single-vessel<Multi-vessel manner. The M parameter is significantly higher
in the Multi-vessel group compared to the Negative group [Table 2.4., Fig. 3.3.].
In case of adjusted samples, the M and M1 parameters show similar
Negative<Non-significant<Single-vessel<Multi-vessel trend. Both indices are
significantly higher in the Multi-vessel group compared to the Negative group, moreover
the M parameter is significantly higher in the Multi-vessel group compared to the Non-
significant group [Table 2.4., Fig. 3.4.].
Red blood cell deformability
RBC deformability shows a decreasing trend at all shear stresses. EI at 30 and 16.87 Pa
was significantly lower in the Non-significant group compared to the Negative group
[Table 2.4.].
Fig. 3.3. Red blood cell aggregation in native and adjusted (Hct=40%) samples measured by Myrenne. Arrows represent significant (p<0.05) differences.
4.0
4.5
5.0
5.5
6.0
6.5
7.0
7.5
Neg NS SV MV
Myrenne M
native
adjusted

35
Fig. 3.4. Red blood cell aggregation in native and adjusted (Hct=40%) samples measured by Myrenne. Arrow represents significant (p<0.05) difference.
Central laboratory parameters
RBC count, Hbg concentration, MCV, MCH, and MCHC have the same rank order:
Negative<Non-significant<Single-vessel<Multi-vessel. In the Multi-vessel group all
parameters are significantly higher compared to the Negative group. LDL levels are
similar in all groups. HDL has a decreasing trend and it is significantly lower in the Multi-
vessel group compared to all the other ones. Fibrinogen level has an increasing tendency
in the CAD subgroups, although no significant difference was found [Table 2.5.].
Table 2.5.
Central laboratory parameters.
Neg NS SV MV
RBC count (G/l) 4.5 ± 0.1 4.6 ± 0.1 4.6 ± 0.1 4.7 ± 0.1a
Hbg concentration (g/l) 134.7 ± 1.5 140.6 ± 2.2a 140.5 ± 2.3a 145.3 ± 2.1a
MCV (fl) 90.5 ± 0.7 91.0 ± 1.0 91.7 ± 1.2 92.2 ± 0.6a
MCH (pg) 30.0 ± 0.3 30.5 ± 0.4 30.7 ± 0.5 31.0 ± 0.3a
MCHC (g/l) 331.0 ± 1.4 334.7 ± 2.2 334.8 ± 2.4 336.6 ± 2.1a
LDL (mmol/l) 3.1 ± 0.2 2.7 ± 0.2 3.1 ± 0.3 3.1 ± 0.2
HDL (mmol/l) 1.5 ± 0.1 1.4 ± 0.1 1.3 ± 0.1 1.2 ± 0.1a,b,c
fibrinogen (g/l) 3.06 ± 0.10 2.97 ± 0.20 3.04 ± 0.11 3.28 ± 0.16 a: significant (p<0.05) difference compared to the Negative group
b: significant (p<0.05) difference compared to the Non-significant group
c: significant (p<0.05) difference compared to the Single-vessel group
11.0
11.5
12.0
12.5
13.0
13.5
14.0
14.5
Neg NS SV MV
Myrenne M1
native
adjusted

36
Discussion
Subject characteristics
Age, male gender, obesity, hypertension, DM and smoking are major CV risk factors,
thus the Negative<Non-significant<Single-vessel<Multi-vessel trend was expected. The
high prevalence of hypertension in the Negative group can be explained by the relatively
high average age of this cluster. The same increasing trend was observed in the
prevalence of PCI and CABG procedures. These procedures are indicated in
hemodynamically significant coronary stenosis, therefore they are only present in the
most severe CAD subgroups.
Generally, the amount of applied medication increases with the deteriorating
coronary status. The use of anti-platelet, statin, ACEI/ARB and beta-blocker is already
notable in the Negative group and increases in the CAD subgroups. According to the
latest guideline for the management of CAD, prescription of these drugs is indicated in
all cases, if contraindications are not present (The Task Force on the management of
stable coronary artery disease of the European Society of Cardiology, 2013).
Unfortunately, in the CAD subgroups not all patients receive proper medication. These
drugs are also present in the Negative group. It is likely that these patients receive these
drugs due to existing hypertension (ACEI/ARB, beta-blocker) or dyslipidemia (statin).
Dual antiplatelet therapy is only present in the Single-vessel and Multi-vessel groups,
where PCIs were performed and dual therapy is routinely used.
Hematocrit
Hct was significantly higher in the CAD subgroups compared to the patients with no
vessel disease which result is similar to the findings of our earlier study (Kesmarky, et
al., 1998). However, we were not able to detect significant differences between CAD
subgroups, although the increasing tendency is well visible. Elevated Hct has also been
reported by Lowe, et al. (1980) and Rainer, et al. (1987). On the other hand Pfafferott,
et al. (1999) did not find significant difference between healthy controls, patients with

37
stable/unstable angina and acute myocardial infarct, but the epidemiological studies
strongly support our findings.
It has been demonstrated, that vascular mechanisms can reduce flow resistance
increment, caused by increased Hct in isolated dog hind limb (Whittaker & Winton,
1933). Baskurt, et al. (1991) reported, that 57% increase of Hct elevated coronary flow
resistance only by 8% in healthy dogs, demonstrating the substantial coronary
autoregulatory reserve. However, after exhausting the coronary reserve by inducing
critical stenosis, coronary flow resistance increased by 22%. This result suggests that in
case of an existing stenosis – e.g. in severe CAD, where hemorheological alteration are
greater – altered hemorheological parameters have more impact on the coronary
circulation.
Plasma and whole blood viscosity
Our study found similar PV levels in all groups, supporting the findings of Lowe, et al.
(1980). On the other hand, our earlier study (Kesmarky, et al., 1998), Rainer, et al.
(1987), Pfafferott, et al. (1999) and Lee, et al. (2008) found significantly elevated PV in
CAD.
No significant difference was found in fibrinogen level, although an increasing
trend is evident in CAD subgroups. Lowe, et al. (1980) reported similar plasma fibrinogen
levels in CAD compared to healthy controls, while Kesmarky, et al. (1998) and Rainer, et
al. (1987) observed a significant increase. The dissimilar findings in PV and fibrinogen
levels may originate from the nowadays widely used statin medication. Ten years ago in
the same region Marton, et al. (2003) reported only 13% statin medication in patients
admitted to hospital due to acute coronary syndrome. This is two times lower compared
to our Negative group and four times lower compared to the CAD subgroups.
WBV was significantly elevated in the most severe vessel state, confirming our
previous result (Kesmarky, et al., 1998). This result is supported by the findings of Lowe,
et al. (1980), Rainer, et al. (1987) and Lee, et al. (2008). Kesmarky, et al. (1998) and Lee,
et al. (2008) reported statistically significant differences between CAD subgroups, while
Vosseler, et al. (2012) found no significant difference between CAD and healthy controls.

38
Increased WBV has also been observed in hypertension and diabetes mellitus, therefore
the elevated WBV in the Multi-vessel group may be a consequence of the increased
prevalence of these comorbidities.
Red blood cell aggregation
RBC aggregation was significantly increased in CAD and significant difference was found
between the subgroups. Rainer, et al. (1987), Pfafferott, et al. (1999) and Lee, et al.
(2008) confirm our results.
RBC aggregation alters both macro- and microrheological properties of blood
and can either decrease or increase flow resistance. These effects depend on several
factors: vessel diameter, geometry, orientation or flow rate. On one hand, enhanced
RBC aggregation reduces flow resistance by increasing axial migration of RBCs,
promoting Fahraeus effect and plasma skimming (Baskurt & Meiselman, 2007).
On the other hand, elevated RBC aggregation increases low shear viscosity which
may affect flow resistance in large blood vessels when shear forces are sufficiently low.
RBC aggregation also has impact at the microcirculatory level: aggregates must be
dispersed in order to enter the microcirculation. In case of elevated RBC aggregation,
higher force is required which increases microvascular flow resistance (Baskurt &
Meiselman, 2007). Studies have also demonstrated in vivo, that RBC clumps may
become entrapped at the entrance to the capillaries (Lipowsky, 2007).
In isolated in situ guinea pig hind limb preparation, elevated RBC aggregation had
no significant effect on flow resistance with intact vascular control mechanisms.
However, after inhibition of smooth muscle tone, perfusion with a series of increasing
aggregating RBC suspensions, flow resistance first increased, then returned to control
and finally increased again (Yalcin, et al., 2004). These results also support the complex
effect of RBC aggregation on hemodynamics and the effect of exhausted vascular
compensation (which is present in CHD).

39
Red blood cell deformability
RBC deformability has a decreasing trend, being significantly lower in non-significant
vessel disease compared to patients with no vessel disease. Pfafferott, et al. (1999)
reported no significant difference of RBC filterability.
RBC deformability is the primary determinant of flow resistance in blood vessels
with dimensions similar to the RBC size. Lower RBC deformability negatively affects
microcirculation by increasing the flow resistance in the capillaries. Again, the
magnitude of this effect depends on the available vascular compensatory mechanisms.
Baskurt, et al. (2004) reported that if RBCs were minimally hardened with
glutaraldehyde, EI decreased by 16% and flow resistance increased by 78% in isolated-
perfused rat hind limb. However, after the pharmacological elimination of vascular tone,
the flow resistance increased by 250% for the same amount of deformability
impairment. This suggest that in case of CHD, where the vascular compensatory
mechanisms are limited, even a slight change in RBC deformability might have a great
effect on myocardial microcirculation.
Other laboratory parameters
RBC count, Hgb concentration, MCV, MCH and MCHC were significantly increased in
severe CAD. Increase of RBC count and MCV explains the same elevating trend of Hct.
Increased Hgb concentration may be a counter mechanism against stenosis-caused low
flow rate, in order to maintain oxygen delivery. In case of increased MCV, RBCs may
require higher force to enter and to pass thought the capillaries. Elevated MCH and
MCHC may increase intracellular viscosity, which can decrease RBC deformability (Cooke
& Lim, 2007).
LDL levels were similar in each group. Though LDL is a CV risk factor and expected
to be elevated in CAD patients, the much higher use of statins in CAD groups
counteracts. The decreasing HDL levels were also expected in CAD.

40
Study limitations
This is a cross-sectional study; therefore inference on the relationship between the
measured variables may be speculative. According to the latest American
(ACCF/AHA/ACP/AATS/PCNA/SCAI/STS, 2012) and European guidelines (The Task Force
on the management of stable coronary artery disease of the European Society of
Cardiology, 2013), coronary CT is indicated in medium pre-test probability of CAD [Fig.
3.5.], while coronary X-ray angiography is performed on high risk patients. In our study
this resulted in a lower number of patients with severe CAD compared to our previous
study where 65% of patient had multi-vessel disease. Due to these guidelines, much
fewer multi-vessel CAD cases were expected therefore 40% area stenosis was chosen as
a cut-off-point. Another important difference between our studies is the “distance”
between control and severely ill groups. We did not have healthy controls, and the most
severe cases are likely to be less severe compared to our earlier study. As a
consequence, the differences in severity of CAD between the groups are lesser and
significant differences are harder to be observed. Another possible reason for the
scarcity of significant differences between CAD subgroups is the relatively poor
discriminatory power of CT: this method is good at excluding CAD, but not as good in
distinguishing high-grade from non-high grade stenosis.
Pre-test probability (PTP) for the presence of coronary stenosis
Low PTP (<15%) Intermediate PTP (15-85%) High PTP (>85%)
Coronary CT angiography in patients at low intermediate
PTP (15% - 50%)
Stress testing for ischemia
Investigate other causes
Consider functional coronary disease
Diagnosis of stable CAD
established
Risk stratification Guideline-directed medical
therapy Invasive coronary angiography
Fig. 3.5. Non-invasive testing in patients with suspected stable CAD. Based on: 2013 ESC guidelines on the management of stable coronary artery disease.

41
Conclusions
Our results indicate that both macro- and microrheological parameters are altered in
CAD, therefore myocardial oxygen supply may be reduced at both macro- and
microcirculatory levels, and may play a pathophysiological role in the deterioration of
this disease.

42
Summary of new scientific results
Hemorheological effects of moderate red wine consumption
Our controlled study demonstrated beneficial effects of 3-week moderate red wine
consumption on hemorheological parameters in healthy volunteers:
1. Three-week red wine intake decreases whole blood viscosity in healthy subject.
2. As a consequence, red wine consumption improves hematocrit per whole blood
viscosity ratio, suggesting improved oxygen transport efficiency of blood even in
healthy volunteers.
3. Moderate drinking of red wine lowers red blood cell aggregation.
4. Moderate consumption of red wine improves red blood cell deformability.
Hemorheological parameters in CT-detected coronary artery disease
Our study revealed that hemorheological parameters are altered in CT-detected
coronary artery disease:
1. Hematocrit is higher in patients with coronary artery disease. The increase was
already significant in the least severe group.
2. Whole blood viscosity is elevated in patients with severe coronary artery disease.
3. Red blood cell aggregation is increased in severe coronary artery disease.
4. Red blood cell deformability is lower in patients with coronary artery disease.
5. These findings support that in CT-detected coronary artery disease beyond the
impaired hemodynamic factors (stenosis), hemorheological parameters are also
negatively affected.

43
Acknowledgements
I would like to express my greatest gratitude to my program leader, Professor Balazs
Sumegi for his great support throughout my PhD studies. I am grateful for the
continuous help and ideas of my project leaders, Dr. Istvan Battyani and Dr. Gabor
Kesmarky.
I am thankful to Prof. Dr. Kalman Toth, Dr. Istvan Juricskay, Dr. Laszlo Czopf, Dr.
Zsolt Marton and Dr. Peter Kenyeres for assisting my work with useful ideas. I would like
to express my special thanks to the present and former Ph.D. students, Dr. Barbara
Sandor, Dr. Miklos Rabai and to our technician Kornelia Tapasztone Fazekas for the
evening shifts. Moreover, I thank Dr. Judit Papp, Dr. Katalin Biro, Dr. Kinga Totsimon and
to the student researchers and the other colleagues for their support and for the friendly
lab community.
I am greatly thankful to Dr. Sandor Szukits, Dr. Edit Varady and the assistants and
technicians at the Department of Radiology for the friendly atmosphere and for the
continuous assistance.
The first study was supported by SROP-4.2.1.B-10/2/KONV-2010-0002 (TAMOP 4.2.1.B).

44
References
1. ABOU-AGAG L.H., KHOO N.K., BINSACK R., WHITE C.R., DARLEY-USMAR V.,
GRENETT H.E., BOOYSE F.M., DIGERNESS S.B., ZHOU F., PARKS D.A. Evidence of
cardiovascular protection by moderate alcohol: role of nitric oxide. Free Radic
Biol Med, 39 (2005), 540-548.
2. AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION/AMERICAN HEART
ASSOCIATION TASK FORCE ON PRACTICE GUIDELINES, AND THE AMERICAN
COLLEGE OF PHYSICIANS, AMERICAN ASSOCIATION FOR THORACIC SURGERY,
PREVENTIVE CARDIOVASCULAR NURSES ASSOCIATION, SOCIETY FOR
CARDIOVASCULAR ANGIOGRAPHY AND INTERVENTIONS, SOCIETY OF THORACIC
SURGEONS. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the
Diagnosis and Management of Patients With Stable Ischemic Heart Disease.
Circulation, 126 (2012), 354-471.
3. AIKENS M.L., GRENETT H.E., BENZA R.L., TABENGWA E.M., DAVIS G.C., BOOYSE
F.M. Alcohol-induced upregulation of plasminogen activators and fibrinolytic
activity in cultured human endothelial cells. Alcohol Clin Exp Res, 22 (1998), 375-
381.
4. AVAR P., POUR NIKFARDJAM M.S., KUNSAGI-MATE S., MONTSKO G., SZABO Z.,
BODDI K., OHMACHT R., MARK L. Investigation of Phenolic Components of
Hungarian Wines. Int J Mol Sci, 8 (2007), 1028-1038.
5. BASKURT O.K., LEVI R., CAGLAYAN S., DIKMENOGLU N., UCER O., GUNER R.,
YORUKAN S. The role of hemorheologic factors in the coronary circulation. Clin
Hemorheol, 11 (1991), 121-127.
6. BASKURT O.K., YALCIN O., MEISELMAN H.J. Hemorheology and vascular control
mechanisms, Clin Hemorheol Microcirc, 30 (2004), 169-178.
7. BASKURT O.K., MEISELMAN H.J. In Vivo Hemorheology. In: Baskurt O.K.,
Hardeman M.R., Rampling, M.W., Meiselman H.J. (eds.). Handbook of
Hemorheology and Hemodynamics, 322-338. IOS Press, Amsterdam, 2007.

45
8. BASKURT O.K., BOYNARD M., COKELET G.C., CONNES P., COOKE B.M., FORCONI
S., LIAO F., HARDEMAN M.R., JUNG F., MEISELMAN H.J., NASH G., NEMETH N.,
NEU B., SANDHAGEN B., SHIN S., THURSTON G., WAUTIER J.L.; INTERNATIONAL
EXPERT PANEL FOR STANDARDIZATION OF HEMORHEOLOGICAL METHODS. New
guidelines for hemorheological laboratory techniques. Clin Hemorheol Microcirc,
42 (2009), 75-97.
9. BOGAR L., JURICSKAY I., KESMARKY G., KENYERES P., TOTH K. Erythrocyte
transport efficacy of human blood: a rheological point of view. Eur J Clin Invest,
35 (2005), 687-690.
10. CABRALES P., TSAI A.G. Plasma viscosity regulates systemic and microvascular
perfusion during acute extreme anemic conditions. Am J Physiol Heart Circ
Physiol, 291 (2006), H2445-H2452.
11. CASAVECCHIA C., MAGNISI R., LA PERA L., MAISANO R., DUGO G. Classification
of Sicilian Red Wines from Autochthonous and Allochthonous Cultivars
According to Anthocyanin Pattern. Am J Enol Viti, 58 (2007), 286-290.
12. CHIEN S., DORMANDY J., ERNST E., MATRAI A. Clinical Hemorheology, Nijhoff
Publishers, Dordrecht Martinus, 1987.
13. COKELET G.R., MEISELMAN H.J. Macro- and Micro-Rheological Properties of
Blood. In: Baskurt O.K., Hardeman M.R., Rampling, M.W., Meiselman H.J. (eds.).
Handbook of Hemorheology and Hemodynamics, 45-71. IOS Press, Amsterdam,
2007.
14. COOKE B.M., LIM C.T. Mechanical and Adhesive Properties of Healthy and
Diseased Red Blood Cells. In: Baskurt O.K., Hardeman M.R., Rampling, M.W.,
Meiselman H.J. (eds.). Handbook of Hemorheology and Hemodynamics, 91-113.
IOS Press, Amsterdam, 2007.
15. DAVIES M.J., BAER D.J., JUDD J.T., BROWN E.D., CAMPBEL W.S., TAYLOR P.R.
Effects of moderate alcohol intake on fasting insulin and glucose concentrations
and insulin sensitivity in postmenopausal women: a randomized controlled trial.
JAMA, 287 (2002), 2559-2562.

46
16. DE LORGERIL M., SALEN P., PAILLARD F., LAPORTE F., BOUCHER F., DE LEIRIS J.
Mediterranean diet and the French paradox: two distinct biogeographic
concepts for one consolidated scientific theory on the role of nutrition in
coronary heart disease. Cardiovasc Res, 54 (2002), 503-515.
17. DÉRCZY K., BATTYÁNY I. Koronária-betegségek CT-diagnosztikája. IME, Képalkotó
diganosztikai különszám (2008), 26-29.
18. DI CASTELNUOVO A., ROTONDO S., IACOVIELLO L., DONATI M.B., DE GAETANO
D. Meta-analysis of wine and beer consumption in relation to vascular risk.
Circulation, 105 (2002), 2836-2844.
19. DI CASTELNUOVO A., COSTANZO S., BAGNARDI V., DONATI M.B., IACOVIELLO L.,
DE GAETANO G. Alcohol dosing and total mortality in men and women: an
updated meta-analysis of 34 prospective studies. Arch Intern Med, 166 (2006),
2437-2445.
20. DINTENFASS L. Blood rheology in pathogenesis of the coronary heart diseases.
Am Heart J, 77 (1969), 139-147.
21. DOBBE J.G.G. Laser-assisted Optical Rotational Cell Analyzer User Manual,
Academic Medical Center, University of Amsterdam, Dept. Medical
Technological Development, Amsterdam, 2003.
22. DOLL R., PETO R., BOREHAM J., SUTHERLAND I. Mortality in relation to alcohol
consumption: a prospective study among male British doctors. Int J Epidemiol,
34 (2005), 199-204.
23. EDELMANN A., DIEWOK J., SCHUSTER K.C., LENDL B. Rapid method for the
discrimination of red wine cultivars based on mid-infrared spectroscopy of
phenolic wine extracts. J Agric Food Chem, 49 (2001), 1139-1145.
24. EMBERSON J.R., SHAPER A.G., WANNAMETHEE S.G., MORRIS R.W., WHINCUP
P.H. Alcohol intake in middle age and risk of cardiovascular disease and
mortality: accounting for intake variation over time. Am J Epidemiol, 116 (2005),
856-863.

47
25. FEHR M., GALLIARD-GRIGIONI K.S., REINHART W.H. Influence of acute alcohol
exposure on hemorheological parameters and platelet function in vivo and in
vitro. Clin Hemorheol Microcirc, 39 (2008), 351-358.
26. FRANKEL E.N., KANNER J., GERMAN J.B., PARKS E., KINSELLA J.E. Inhibition of
oxidation of human low-density lipoprotein by phenolic substances in red wine.
Lancet, 341 (1993), 454-457.
27. FUCHS C.S., STAMPFER M.J., COLDITZ G.A., GIOVANNUCCI E.L., MANSON J.E.,
KAWACHI I., HUNTER D.J., HANKINSON S.E., HENNEKENS C.H., ROSNER B. Alcohol
consumption and mortality among women. N Engl J Med, 332 (1995), 1245-1250.
28. GAZIANO J.M., GAZIANO T.A., GLYNN R.J., SESSO H.D., AJANI U.A., STAMPFER
M.J., MANSON J.E., HENNEKENS C.H., BURING J.E. Light-to-moderate alcohol
consumption and mortality in the Physicians' Health Study enrollment cohort. J
Am Coll Cardiol, 35 (2000), 96-105.
29. GOLDBERG D.M., YAN J.N.G.E., DIAMANDIS E.P., KARUMANCHIRI A., SOLEAS G.,
WATERHOUSE A.L. A Global Survey of Trans-Resveratrol Concentrations in
Commercial Wines. Am J Enol Vitic, 46 (1995), 159-165.
30. GORDON T., KANNEL W.B. Drinking and mortality. The Framingham Study. Am J
Epidemiol, 120 (1984), 97-107.
31. GRONBAEK M., DEIS A., SORENSEN T.I., BECKER U., SCHNOHR P., JENSEN G.
Mortality associated with moderate intakes of wine, beer, or spirits. BMJ, 310
(1995), 1165-1169.
32. HARDEMAN M.R., GOEDHART T.P., SCHU N.H. Laser-assisted optical rotational
cell analyser (LORCA). II: Red blood cell deformability: elongation index versus
cell transit time. Clin Hemorheol, 14 (1994), 619-630.
33. HARDEMAN M.R., DOBBE J.G., INCE C. The Laser-assisted Optical Rotational Cell
Analyzer (LORCA) as red blood cell aggregometer. Clin Hemorheol Microcirc, 25
(2001), 1-11.

48
34. JENSEN T., RETTERSTOL L.J., SANDSET P.M., GODAL H.C., SKJONSBERG O.H. A
daily glass of red wine induces a prolonged reduction in plasma viscosity: a
randomized controlled trial. Blood Coagul Fibrinolysis, 17 (2006), 471-476.
35. KANNEL W.B., D'AGOSTINO R.B., BELANGER A.J. Fibrinogen, cigarette smoking,
and risk of cardiovascular disease: Insights from the Framingham Study. Am
Heart J, 113 (1987), 1006-1010.
36. KARATZI K.N., PAPAMICHAEL C.M., KARATZIS E.N., PAPAIOANNOU T.G.,
AZNAOURIDIS K.A., KATSICHTI P.P., STAMATELOPOULOS K.S., ZAMPELAS A.,
LEKAKIS J.P., MAVRIKAKIS M.E. Red wine acutely induces favorable effects on
wave reflections and central pressures in coronary artery disease patients. Am J
Hypertens, 18 (2005), 1161-1167.
37. KAUL S., BELCIK T., KALVAITIS S., JAYAWEERA A.R., CHOI S.W., WEI K. Effect of
modest alcohol consumption over 1-2 weeks on the coronary microcirculation of
normal subjects. Eur J Echocardiogr, 11 (2010), 683-689.
38. KENYERES P., JURICSKAY I., TARSOLY P., KESMARKY G., MUHL D., TOTH K., BOGAR
L. Low hematocrit per blood viscosity ratio as a mortality risk factor in coronary
heart disease. Clin Hemorheol Microcirc, 38 (2008), 51-56.
39. KENYERES P. Hemoreológiai paraméterek prognosztikai jelentősége és mérésük
módszertana. PhD disszertáció, Pécsi Tudományegyetem Általános
Orvostudományi Kar, Pécs, 2010.
40. KERRY N., ABBEY M. Red wine and fractionated phenolic compounds prepared
from red wine inhibit low density lipoprotein oxidation in vitro. Atherosclerosis,
135 (1997), 93-102.
41. KESMARKY G., TOTH K., HABON L., VAJDA G., JURICSKAY I. Hemorheological
parameters in coronary artery disease. Clin Hemorheol Microcirc, 18 (1998), 245-
251.
42. KLOSE H.J., VOLGER E., BRECHTELSBAUER H., HEINICH L., SCHMID-SCHONBEIN H.
Microrheology and light transmission of blood. I. The photometric effects of red
cell aggregation and red cell orientation. Pflugers Arch, 333 (1972), 126-139.

49
43. KOENIG W., SUND M., FILIPIAK B., DORING A., LOWEL H., ERNST E. Plasma
viscosity and the risk of coronary heart disease: results from the MONICA-
Augsburg Cohort Study, 1984 to 1992. Arterioscler Thromb Vasc Biol, 18 (1998),
768-772.
44. KONTKANEN D., REYNOLDS A.G., CLIFF M.A., KING M. Canadian terroir: sensory
characterization of Bordeaux-style red wine varieties in the Niagara Peninsula.
Food Res Int, 38 (2005), 417-425.
45. LAW M., WALD N. Why heart disease mortality is low in France: the time lag
explanation. BMJ, 318 (1999), 1471-1476.
46. LEE A.J., MOWBRAY P.I., LOWE G.D., RUMLEY A., FOWKES F.G., ALLAN P.L. Blood
viscosity and elevated carotid intima-media thickness in men and women: the
Edinburgh Artery Study. Circulation, 97 (1998), 1467-1473.
47. LEE B.K., DURAIRAJ A., MEHRA A., WENBY R.B., MEISELMAN H.J., ALEXY T.
Hemorheological abnormalities in stable angina and acute coronary syndromes.
Clin Hemorheol Microcirc, 39 (2008), 43-51.
48. LEIKERT J.F., RATHEL T.R., WOHLFART P., CHEYNIER V., VOLLMAR A.M., DIRSCH
V.M. Red wine polyphenols enhance endothelial nitric oxide synthase expression
and subsequent nitric oxide release from endothelial cells. Circulation, 106
(2002), 1614-1617.
49. LIPOWSKY H.H. Blood Rheology Aspects of the Microcirculation. In: Baskurt O.K.,
Hardeman M.R., Rampling, M.W., Meiselman H.J. (eds.). Handbook of
Hemorheology and Hemodynamics, 307-321. IOS Press, Amsterdam, 2007.
50. LOWE G.D., DRUMMOND M.M., LORIMER A.R., HUTTON I., HUTTON C.D.,
PRENTICE C.R.M., BARBENEL J. Relation between extent of coronary heart
disease and blood viscosity. Br Med J, 280 (1980), 673-674.
51. LOWE G.D., FOWKES F.G., DAWES J., DONNAN P.T., LENNIE S.E., HOUSLEY E.
Blood viscosity, fibrinogen, and activation of coagulation and leukocytes in
peripheral arterial disease and the normal population in the Edinburgh Artery
Study. Circulation, 87 (1993), 1915-1920.

50
52. LU Z., ZHANG Y., LIU H., YUAN J., ZHENG Z., ZOU G. Transport of a cancer
chemopreventive polyphenol, resveratrol: interaction with serum albumin and
hemoglobin. J Fluoresc, 17 (2007), 580-587.
53. MA J., HENNEKENS C.H., RIDKER P.M., STAMPFER M.J. A prospective study of
fibrinogen and risk of myocardial infarction in the Physicians' Health Study. J Am
Coll Cardiol, 33 (1999), 1347-1352.
54. MARTON Z., HORVATH B., ALEXY T., KESMARKY G., GYEVNAR Z., CZOPF L.,
HABON T., KOVACS L., PAPP E., MEZEY B., ROTH E., JURICSKAY I., TOTH K. Follow-
up of hemorheological parameters and platelet aggregation in patients with
acute coronary syndromes. Clin Hemorheol Microcirc, 29 (2003), 81-94.
55. MATHERS C.D., LONCAR D. Projections of global mortality and burden of disease
from 2002 to 2030. PLoS Med, 3 (2006), e442.
56. MCCONNELL M.V., VAVOURANAKIS I., WU L.L., VAUGHAN D.E., RIDKER P.M.
Effects of a single, daily alcoholic beverage on lipid and hemostatic markers of
cardiovascular risk. Am J Cardiol, 80 (1997), 1226-1228.
57. MEISELMAN H.J., BASKURT O.K. Hemorheology and hemodynamics: Dove
andare? Clin Hemorheol Microcirc, 35 (2006), 37-43.
58. MUKAMAL K.J., JENSEN M.K., GRONBAEK M., STAMPFER M.J., MANSON J.E.,
PISCHON T., RIMM E.B. Drinking frequency, mediating biomarkers, and risk of
myocardial infarction in women and men. Circulation, 112 (2005), 1406-1413.
59. NEUMANN F.J., TILLMANNS H., ROEBRUCK P., ZIMMERMANN R., HAUPT H.M.,
KUBLER W. Haemorrheological abnormalities in unstable angina pectoris: a
relation independent of risk factor profile and angiographic severity. Br Heart J,
62 (1989), 421-428.
60. OPIE L.H., LECOUR S. The red wine hypothesis: from concepts to protective
signalling molecules. Eur Heart J, 28 (2007), 1683-1693.

51
61. PACE-ASCIAK C.R., HAHN S., DIAMANDIS E.P., SOLEAS G., GOLDBERG D.M. The
red wine phenolics trans-resveratrol and quercetin block human platelet
aggregation and eicosanoid synthesis: implications for protection against
coronary heart disease. Clin Chim Acta, 235 (1995), 207-219.
62. PAL S., HO N., SANTOS C., DUBOIS P., MAMO J., CROFT K., ALLISTER E. Red wine
polyphenolics increase LDL receptor expression and activity and suppress the
secretion of ApoB100 from human HepG2 cells. J Nutr, 133 (2003), 700-706.
63. PELLEGRINI N., PARETI F.I., STABILE F., BRUSAMOLINO A., SIMONETTI P. Effects
of moderate consumption of red wine on platelet aggregation and haemostatic
variables in healthy volunteers. Eur J Clin Nutr, 50 (1996), 209-213.
64. PFAFFEROTT C., MOESSMER G., EHRLY A.M., BAUERSACHS R.M. Involvement of
erythrocyte aggregation and erythrocyte resistance to flow in acute coronary
syndromes. Clin Hemorheol Microcirc, 21 (1999), 35-43.
65. PIKAAR N.A., WEDEL M., VAN DER BEEK E.J., VAN DOKKUM W., KEMPEN H.J.,
KLUFT C., OCKHUIZEN T., HERMUS R.J. Effects of moderate alcohol consumption
on platelet aggregation, fibrinolysis, and blood lipids. Metabolism 36, (1987),
538-543.
66. RABAI M., TOTH A., KENYERES P., MARK L., MARTON Z., JURICSKAY I., TOTH K.,
CZOPF L. In vitro hemorheological effects of red wine and alcohol-free red wine
extract. Clin Hemorheol Microcirc, 44 (2010), 227-236.
67. RABAI M., DETTERICH J.A., WENBY R.B., TOTH K., MEISELMAN H.J. Effects of
ethanol on red blood cell rheological behavior. Clin Hemorheol Microcirc, 56
(2014), 87-99.
68. RAINER C., KAWANISHI D.T., CHANDRARATNA P.A., BAUERSACHS R.M., REID C.L.,
RAHIMTOOLA S.H., MEISELMAN H.J. Changes in blood rheology in patients with
stable angina pectoris as a result of coronary artery disease. Circulation, 76
(1987), 15-20.
69. RENAUD S.C., RUF J.C. Effects of alcohol on platelet functions. Clin Chim Acta,
246 (1996), 77-89.

52
70. RENAUD S., DE LORGERILM M. Wine, alcohol, platelets, and the French paradox
for coronary heart disease. Lancet, 339 (1992), 1523-1526.
71. RENAUD S., GUEGUEN R., SIEST G., SALAMON R. Wine, beer, and mortality in
middle-aged men from eastern France. Arch Intern Med, 159 (1999), 1865-1870.
72. REYNOLDS K., LEWIS B., NOLEN J.D., KINNEY G.L., SATHYA B., HE J. Alcohol
consumption and risk of stroke: a meta-analysis. JAMA, 289 (2003), 579-588.
73. RICE-EVANS C.A., MILLER N.J., PAGANGA G. Structure-antioxidant activity
relationships of flavonoids and phenolic acids. Free Radic Biol Med, 20 (1996),
933-956.
74. RIDKER P.M., VAUGHAN D.E., STAMPFER M.J., GLYNN R.J., HENNEKENS C.H.
Association of moderate alcohol consumption and plasma concentration of
endogenous tissue-type plasminogen activator. JAMA, 272 (1994), 929-933.
75. RUIDAVETS J.B., BATAILLE V., DALLONGEVILLE J., SIMON C., BINGHAM A.,
AMOUYEL P., ARVEILER D., DUCIMETIERE P., FERRIERES J. Alcohol intake and diet
in France, the prominent role of lifestyle. Eur Heart J, 25 (2004), 1153-1162.
76. SCHNOHR P., JENSEN J.S., SCHARLING H., NORDESTGAARD B.G. Coronary heart
disease risk factors ranked by importance for the individual and community. A
21 year follow-up of 12 000 men and women from The Copenhagen City Heart
Study. Eur Heart J, 23 (2002), 620-626.
77. SERAFINI M., MAIANI G., FERRO-LUZZI A. Alcohol-free red wine enhances plasma
antioxidant capacity in humans. J Nutr, 128 (1998), 1003-1007.
78. SOLEAS G.J., DIAMANDIS E.P., GOLDBERG D.M. Wine as a biological fluid: history,
production, and role in disease prevention. J Clin Lab Anal, 11 (1997), 287-313.
79. ST LEGER A.S., COCHRANE A.L., MOORE F. Factors associated with cardiac
mortality in developed countries with particular reference to the consumption
of wine. Lancet, 1 (1979), 1017-1020.
80. SWEETNAM P.M., THOMAS H.F., YARNELL J.W.G., BESWICK A.D., BAKER I.A.,
ELWOOD PC. Fibrinogen, viscosity and the 10-year incidence of ischemic heart
disease: The Caerphilly and Speedwell Studies. Eur Heart J, 17 (1997), 1814-1820.

53
81. TEISSEDRE P.L., FRANKE E.N., WATERHOUSE A.L., PELEG H., GERMAN J.B.
Inhibition of in vitro human LDL oxidation by phenolic antioxidants from grapes
and wines. J Sci Food Agri, 70 (1996), 55-61.
82. THE TASK FORCE ON THE MANAGEMENT OF STABLE CORONARY ARTERY DISEASE
OF THE EUROPEAN SOCIETY OF CARDIOLOGY. 2013 ESC guidelines on the
management of stable coronary artery disease. Eur Heart J, 34 (2013), 2949-
3003.
83. TOTH K., KESMARKY G. Clinical Significance of Hemorheological Alterations. In:
Baskurt O.K., Hardeman M.R., Rampling M.W., Meiselman H.J. (eds.), Handbook
of Hemorheology and Hemodynamics, 392-432. IOS Press, Amsterdam. 2007.
84. TSAI A.G., FRIESENECKER B., MCCARTHY M., SAKAI H., INTAGLIETTA M. Plasma
viscosity regulates capillary perfusion during extreme hemodilution in hamster
skinfold model. Am J Physiol, 275 (1998), H2170-H2180.
85. VAYA A., MARTINEZ M., DALMAU J., LABIOS M., AZNAR J. Hemorheological
profile in patients with cardiovascular risk factors. Haemostasis, 26 Suppl. 4
(1996), 166-170.
86. VAYA A., FALCO C., FERNANDEZ P., CONTRERAS T., VALLS M., AZNAR J.
Erythrocyte aggregation determined with the Myrenne aggregometer at two
modes (M0, M1) and at two times (5 and 10 sec). Clin Hemorheol Microcirc, 29
(2003), 119-127.
87. VOSSELER M., BEUTEL A.A., SCHAFER S., MUXEL S., JABS A., FORCONI S., PARKER
J.D., MUNZEL T., GORI T. Parameters of blood viscosity do not correlate with the
extent of coronary and carotid atherosclerosis and with endothelial function in
patients undergoing coronary angiography. Clin Hemorheol Microcirc, 52 (2012),
245-254.
88. WALLE T., HSIEH F., DELEGGE H., OATIS M.J.E., WALLE U.K. High absorption but
very low bioavailability of oral resveratrol in humans. Drug Metab Dispos, 32
(2004), 1377-1382.

54
89. WANNAMETHEEM S.G., SHAPER A.G. Type of alcoholic drink and risk of major
coronary heart disease events and all-cause mortality. Am J Public Health, 89
(1999), 685-690.
90. WHITTAKER S.R., WINTON F.R. The apparent viscosity of blood flowing in the
isolated hindlimb of the dog, and its variation with corpuscular concentration. J
Physiol, 78 (1933), 339-369.
91. WORLD HEALTH ORGANIZATION. The global burden of disease: 2004 update.
World Health Organization, Geneva, 2008.
92. WORLD HEALTH ORGANIZATION. Global atlas on cardiovascular disease
prevention and control. World Health Organization, Geneva, 2011.
93. WORLD HEALTH ORGANIZATION. Fact sheet on cardiovascular diseases [Online].
Version: March 2013. Accessed: 5 June 2014.
http://www.who.int/mediacentre/factsheets/fs317/en/
94. WORLD HEALTH ORGANIZATION. European Health for All database. Updated:
April 2014. WHO Regional Office for Europe.
95. YALCIN O., UYUKLU M., ARMSTRONG J.K., MEISELMAN H.J., BASKURT O.K.
Graded alterations of RBC aggregation influence in vivo blood flow resistance.
Am J Physiol, 287 (2004), 2644-2650.
96. YARNELL J.W., BAKER I.A., SWEETNAM P.M., BAINTON D., O'BRIEN J.R.,
WHITEHEAD P.J., ELWOOD P.C. Fibrinogen, viscosity, and white blood cell count
are major risk factors for ischemic heart disease. The Caerphilly and Speedwell
collaborative heart disease studies. Circulation, 83 (1991), 836-844.

55
Publications of the Author
Papers from the topics
1. RÁBAI M., TÓTH A., KENYERES P., MÁRK L., MÁRTON Z., JURICSKAY I., SÜMEGI B.,
TÓTH K. Vörösbor és alkoholmentes vörösborkivonat kedvező in vitro
haemorheologiai hatásai. Érbetegségek, 2 (2009), 45-52.
2. RABAI M., TOTH A., KENYERES P., MARK L., MARTON Z., JURICSKAY I., TOTH K.,
CZOPF L. In vitro hemorheological effects of red wine and alcohol-free red wine
extract. Clin Hemorheol Microcirc, 44 (2010), 227-236.
3. TOTH A., SANDOR B., PAPP J., RABAI M., BOTOR D., HORVATH Z., KENYERES P.,
JURICSKAY I., TOTH K., CZOPF L. Moderate red wine consumption improves
hemorheological parameters in healthy volunteers. Clin Hemorheol Microcirc, 56
(2014), 13-23.
4. TOTH A., PAPP J., RABAI M., KENYERES P., MARTON Z., KESMARKY G., JURICSKAY
I., MEISELMAN H.J., TOTH K. The role of hemorheological factors in cardiovascular
medicine. Clin Hemorheol Microcirc, 56 (2014), 197-204.
5. TOTH A., SZUKITS S., VARADY E., SANDOR B., RABAI M., PAPP J., JURICSKAY I.,
KESMARKY G., TOTH K., SUMEGI B., BATTYANI I. Hemorheological parameters in
coronary artery disease detected by multi-slice CT. Korea-Aust Rheol J, 26 (2014),
229-235.

56
Other papers
6. VEKASI J., KOLTAI K., GAAL V., TOTH A., JURICSKAY I., KESMARKY G. The effect of
aspirin on hemorheological parameters of patients with diabetic retinopathy. Clin
Hemorheol Microcirc, 39 (2008), 385-389.
7. KENYERES P., RABAI M., TOTH A., KESMARKY G., MARTON Z., TOTH K. Reviewing
data reduction methods for ektacytometry. Clin Hemorheol Microcirc, 47 (2011),
143-150.
8. PAPP J., TOTH A., SANDOR B., KISS R., RABAI M., KENYERES P., JURICSKAY I.,
KESMARKY G., SZABADOS S., TOTH K. The influence of on-pump and off-pump
coronary artery bypass grafting on hemorheological parameters. Clin Hemorheol
Microcirc, 49 (2011), 331–346.
9. PAPP J., BÓTOR D., SÁNDOR B., TÓTH A., BIRÓ K., CSERNUS Z., TÓTH K., KÉSMÁRKY
G. A Raynaud-jelenség hemoreológiai vonatkozásai. Érbetegségek, 20 (2013), 33-
39.
10. PAPP J., SANDOR B., VAMOS Z., BOTOR D., TOTH A., RABAI M., KENYERES P.,
CSEPLO P., JURICSKAY I., MEZOSI E., KOLLER A., TOTH K. Antiplatelet effect of
acetylsalicylic acid, metamizole and their combination - in vitro and in vivo
comparisons. Clin Hemorheol Microcirc, 65 (2014), 1-12.
11. BIRO K., SANDOR B., TOTH A., KOLTAI K., PAPP J., RABAI M., TOTH K., KESMARKY
G. In vitro hemorheological effects of parenteral agents used in peripheral arterial
diseases. Korea-Aust Rheol J, 26 (2014), 243-247.
12. SANDOR B., VARGA A., RABAI M., TOTH A., PAPP J., TOTH K., SZAKAY P. Aspirin
resistance as cardiovascular risk after kidney transplantation. Korea-Aust Rheol J,
26 (2014), 237-241.

57
Published abstracts
1. RÁBAI M., KENYERES P., TÓTH A., KÉSMÁRKY G., MÁRTON Z., TÓTH K. Lehetőségek
ektacitometriás eredmények egyszerűsítésére, korrekciójára és
összehasonlítására. A Magyar Haemorheologiai Társaság XVII., a Magyar
Mikrocirkulációs és Vaszkuláris Biológiai Társaság, illetve a Magyar
Szabadgyökkutató Társaság I. Közös Kongresszusa, 2008. március 18-19.,
Balatonkenese. Érbetegségek, 15 (2008), 21.
2. RÁBAI M., TÓTH A. Lehetőségek ektacitometriás eredmények egyszerűsítésére,
korrekciójára és összehasonlítására. PTE ÁOK Tudományos Diákköri Konferencia
2008, 2008. április 3-5., Pécs. Absztraktok, 155.
3. KENYERES P., RABAI M., TOTH A., KESMARKY G., MARTON Z., TOTH K. Methods to
simplify, correct and compare ektacytometric results. 13th International Congress
of Biorheology and 6th International Conference on Clinical Hemorheology, 9-13
July 2008, State College, USA. Biorheol, 45 (2008), 138.
4. RABAI M., TOTH A., KENYERES P., MARTON Z., KESMARKY G., TOTH K. Rheological
benefit of red wine and its alcohol free extract. 13th International Congress of
Biorheology and 6th International Conference on Clinical Hemorheology, 9-13 July
2008, State College, USA. Biorheol, 45 (2008), 147.
5. TOTH K., KESMARKY G., MARTON Z., JURICSKAY I., TOTH A., ALEXY T., MEISELMAN
H.J. Hemorheological parameters in acute and stable forms of coronary heart
disease. 13th International Congress of Biorheology and 6th International
Conference on Clinical Hemorheology, 9-13 July 2008, State College, USA. Biorheol,
45 (2008), 47.
6. KENYERES P., RABAI M., TOTH A., KESMARKY G., TOTH K. The impact of in vitro
aging on erythrocyte aggregation. 25th Conference of the European Society for
Microcirculation, 26-29 August 2008, Budapest, Hungary. J Vasc Res, 45 (2008),
105.

58
7. KENYERES P., RÁBAI M., TÓTH A., KÉSMÁRKY G., BOGÁR L., TÓTH K. Egy új
megközelítés az optimális hematokrit értelmezésében akut koronária szindrómás
betegek adatai alapján. A Magyar Kardiológusok Társasága 2009. évi Tudományos
Kongresszusa, 2009. május 6-9., Balatonfüred. Card Hung, 39 Suppl. A (2009), A66.
8. RÁBAI M., PÁLFI A., BARTHA É., KENYERES P., TÓTH A., MAGYAR K., SÜMEGI B.,
TÓTH K. Vörösbor és alkoholmentes vörösborkivonat protektív hatásai
állatkísérletes és in vitro hemoreológiai modellekben. A Magyar Kardiológusok
Társasága 2009. évi Tudományos Kongresszusa, 2009. május 6-9., Balatonfüred.
Card Hung, 39 Suppl. A (2009), A74.
9. KENYERES P., RÁBAI M., TÓTH A., TÓTH K. Új módszer a hematokrit - vérviszkozitás
arány, és a virtuális optimális hematokrit meghatározására. 6. Magyar
Mikrokeringés Kongresszus, 2009. május 22-23, Balatonkenese. Érbetegségek, 2
(2009), 59.
10. KENYERES P., RABAI M., TOTH A., TOTH K. New method to determine hematocrit
to blood viscosity ratio and virtual optimal hematocrit. 15th Conference of the
European Society for Clinical Hemorheology and Microcirculation, 28 June - 1 July
2009, Pontresina/St. Moritz, Switzerland. Clin Hemorheol Microcirc, 42 (2009),
191.
11. RABAI M., KENYERES P., TOTH A., PALFI A., BARTHA E., MAGYAR K., SUMEGI B.,
TOTH K. In vitro hemorheological and cardioprotective effects of red wine and
alcohol free red wine extract. 15th Conference of the European Society for Clinical
Hemorheology and Microcirculation, 28 June - 1 July 2009, Pontresina/St. Moritz,
Switzerland. Clin Hemorheol Microcirc, 42 (2009), 191-192.
12. SÁNDOR B., TÓTH A. A hiperhomociszteinémia hatása a vér reológiai
paramétereire. XVII. Tudományos Diákköri Konferencia, 2010. március 18-21.,
Marosvásárhely. Orvosi és Gyógyszerészeti Szemle, 56 Suppl. 1 (2010), 12.
13. SÁNDOR B., TÓTH A. Hemoreológiai vizsgálatok hiperhomociszteinémiás patkány
modellen. PTE ÁOK Tudományos Diákköri Konferencia 2010, 2010. április 15-17.,
Pécs. Absztraktok, 166.

59
14. TÓTH A. A vörösbor és alkoholmentes vörösbor kivonat hatásának vizsgálata in
vitro hemoreológiai modellen. PTE ÁOK Tudományos Diákköri Konferencia 2010,
2010. április 15-17., Pécs. Absztraktok, 194.
15. SÁNDOR B., TÓTH A. A hemoreológia és a hyperhomociszteinémia
összefüggéseinek vizsgálata. XV. Korányi Frigyes Tudományos Fórum, 2010. április
29-30., Budapest. Absztraktok, 118.
16. PAPP J., SANDOR B., TOTH A., RABAI M., VAMOS Z., KENYERES P., KOLLER A., TOTH
K. Effects of Hyperhomocysteinemia on Various Hemorheological Parameters. 2nd
International Symposium on Hypertension, 18-21 November 2010, Osijek, Croatia.
Kidney Blood Press Res, 35 (2010), 428.
17. PAPP J., TÓTH A., SÁNDOR B., KISS R., RÁBAI M., KENYERES P., SZABADOS S., TÓTH
K. On-pump és off-pump technikával végzett koszorúér bypass műtétek (CABG)
hemoreológiai összehasonlítása. A Magyar Kardiológusok Társasága 2010. évi
Tudományos Kongresszusa, 2010. május 5-8., Balatonfüred. Card Hung, 40 Suppl.
G (2010), G89.
18. SÁNDOR B., PAPP J., TÓTH A., RÁBAI M., KENYERES P., KOLLER Á., TÓTH K.
Hiperhomociszteinémia hatása a vér reológiai paramétereire. A Magyar
Kardiológusok Társasága 2010. évi Tudományos Kongresszusa, 2010. május 5-8.,
Balatonfüred. Card Hung, 40 Suppl. G (2010), G69.
19. PAPP J., TÓTH A., SÁNDOR B., KISS R., RÁBAI M., KENYERES P., SZABADOS S., TÓTH
K. Különböző technikákkal végzett koszorúér bypass műtétek (CABG)
hemoreológiai összehasonlítása. XVII. Magyar Klinikai Hemoreológiai
Kongresszus, a Magyar Haemorheologiai Társaság, a Magyar Mikorcirkulációs és
Vaszkuláris Biológiai Társaság és a Magyar Szabadgyökkutató Társaság II. közös
kongresszusa, 2010. június 25-26. Pécs. Absztraktok, 25.

60
20. SÁNDOR B., PAPP J., TÓTH A., RÁBAI M., KENYERES P., KOLLER Á., TÓTH K.
Hemoreológiai vizsgálatok hiperhomociszteinémiás patkány modellen. XVII.
Magyar Klinikai Hemoreológiai Kongresszus, a Magyar Haemorheologiai
Társaság, a Magyar Mikorcirkulációs és Vaszkuláris Biológiai Társaság és a
Magyar Szabadgyökkutató Társaság II. közös kongresszusa, 2010. június 25-26.
Pécs. Absztraktok, 18.
21. PAPP J., TOTH A., SANDOR B., KISS R., RABAI M., KENYERES P., SZABADOS S., TOTH
K. The influence of on-pump and off-pump coronary artery bypass grafting (CABG)
on hemorheological parameters. 18th International Meeting of the Alpe-Adria
Association of Cardiology, 16-18 September 2010, Vienna, Austria. J Kardiol, 17
Suppl. A (2010), 19-20.
22. TÓTH A., SÁNDOR B. On-pump és off-pump technikákkal végzett koszorúér bypass
műtétek (CABG) hatása a hemoreológiai paraméterekre. PTE ÁOK Tudományos
Diákköri Konferencia 2011, 2011. február 17-18., Pécs. Absztraktok, 144.
23. KENYERES P., PAPP J., TÓTH A., RÁBAI M., FEHÉR G., KOLTAI K., KÉSMÁRKY G.,
TÓTH K. Szinergizmus és kereszthatás az acetilszalicilsavval és tienopiridin
származékokkal elérhető thrombocyta aggregáció gátlás esetében. 7. Magyar
Mikrokeringés Kongresszus, 2011. április 1-2., Dobogókő. Érbetegségek, 18 Suppl.
1 (2011), 13.
24. PAPP J., TÓTH A., SÁNDOR B., RÁBAI M., KENYERES P., KISS R., SZABADOS S., TÓTH
K. On-pump és off-pump technikával végzett koszorúér bypass műtétek (CABG)
hatása a hemoreológiai és vérzési-transzfúziós paraméterekre. 7. Magyar
Mikrokeringés Kongresszus, 2011. április 1-2., Dobogókő. Érbetegségek, 18 Suppl.
1 (2011), 20-21.
25. KENYERES P., TÓTH A., KOLTAI K., FEHÉR G., PAPP J., RÁBAI M., TÓTH K.
Acetilszalicilsav és tienopiridinek trombocitaaggregáció gátlásának szinergizmusa.
A Magyar Kardiológusok Társasága 2011. évi Tudományos Kongresszusa, 2011.
május 1-14., Balatonfüred. Card Hung, 41 Suppl. F (2011), F33.

61
26. PAPP J., TÓTH A., KISS R., SÁNDOR B., RÁBAI M., KENYERES P., SZABADOS S., TÓTH
K. Különböző technikákkal végzett koszorúér bypass műtétek (CABG) hatása a
hemoreológiai és vérzési-transzfúziós paraméterekre. A Magyar Kardiológusok
Társasága 2011. évi Tudományos Kongresszusa, 2011. május 1-14., Balatonfüred.
Card Hung, 41 Suppl. F (2011), F47-F48.
27. PAPP J., VÁMOS Z., SÁNDOR B., TÓTH A., RÁBAI M., KENYERES P., CSÉPLŐ P.,
KOLLER Á., TÓTH K. Acetilszalicilsav és metamizol trombocita aggregáció gátló
hatásának in vitro összehasonlítása egészséges önkéntesek vérmintáin. FAMÉ,
2011. június 8-11., Pécs. Acta Phys, 202 Suppl. 684 (2011), 91-92.
28. PAPP J., TOTH A., SANDOR B., RABAI M., KISS R., TOTH K. The influence of various
coronary artery bypass grafting (CABG) methods on hemorheological parameters.
16th Conference of the European Society for Clinical Hemorheology and
Microcirculation, 18-21 June 2011, Munich, Germany. Abstract book, 96.
29. TOTH A., RABAI M., KENYERES P., MEISELMAN H.J., TOTH K. In vitro
hemorheological effects of red wine, alcohol free red wine extract and alcohol.
16th World Congress on Heart Disease, 23-26 July 2011, Vancouver, BC, Canada. J
Heart Dis, 8 (2011), 10.
30. KENYERES P., PAPP J., TOTH A., RABAI M., FEHER G., KOLTAI K., TOTH K. Synergic
antiplatelet effect of acetylsalicylic acid and thienopyridines. 19th International
Meeting of the Alpe-Adria Association of Cardiology, 15-17 September 2011,
Budapest, Hungary. Interventional Medicine & Applied Sciences, 3 (2011), 148.
31. TÓTH A. Vörösbor, alkohol és alkoholmentes vörösbor kivonat in vitro
hemoreológiai hatásának vizsgálata. PTE ÁOK TDK Miniszimpózium, 2011
november 24., Pécs. Absztraktok, 7.
32. TÓTH A., BÓTOR D., HORVÁTH Z. A vörösbor fogyasztás hatása a hemoreológiai
paraméterekre egészséges önkénteseken. PTE ÁOK Tudományos Diákköri
Konferencia 2012, 2012. április 17-18., Pécs. Absztraktok, 118.

62
33. BÓTOR D., PAPP J., HORVÁTH Z., TÓTH A, SÁNDOR B, RÁBAI M, CSERNUS Z, SZABÓ
Z, TÓTH K, KÉRMÁRKY G. Raynaud-kór: Az életet megkeserítő betegség
hemoreológia vonatkozásai. A Magyar Haemorheologiai Társaság, a Magyar
Mikorcirkulációs és Vaszkuláris Biológiai Társaság és a Magyar Szabadgyökkutató
Társaság III. közös kongresszusa, 2012. április 27-28., Balatonkenese.
Programfüzet, 29.
34. PAPP J., SANDOR B., TOTH A., HORVATH Z., BOTOR D., RABAI M., KENYERES P.,
JURICSKAY I., VAMOS Z., CSEPLO P., KOLLER A., TOTH K. In vitro and vivo
comparison of platelet aggregation inhibitory effect of acetylsalicic acid,
metamizole and their combination. A Magyar Haemorheologiai Társaság, a
Magyar Mikorcirkulációs és Vaszkuláris Biológiai Társaság és a Magyar
Szabadgyökkutató Társaság III. közös kongresszusa, 2012. április 27-28.,
Balatonkenese. Programfüzet, 19.
35. TOTH A., SANDOR B., PAPP J., BOTOR D., HORVATH Z., RABAI M., KENYERES P.,
JURICSKAY I., TOTH K. Red wine and hemorheology: complex results of in vivo and
in vitro studies in healthy volunteers. A Magyar Haemorheologiai Társaság, a
Magyar Mikorcirkulációs és Vaszkuláris Biológiai Társaság és a Magyar
Szabadgyökkutató Társaság III. közös kongresszusa, 2012. április 27-28.,
Balatonkenese. Programfüzet, 22.
36. PAPP J., KOLTAI K., TÓTH A., BÓTOR D., SÁNDOR B., RÁBAI M., CSERNUS Z., TÓTH
K., KÉSMÁRKY G. Hemoreológiai tényezők szerepe perifériás vazospasztikus
kórképekben. A Magyar Kardiológusok Társasága 2012. évi Tudományos
Kongresszusa, 2012. május 9-12., Balatonfüred. Card Hung, 42 Suppl. A (2012), A2.
37. TOTH A., SANDOR B., PAPP J., BOTOR D., HORVATH Z., RABAI M., KENYERES P.,
JURICSKAY I., TOTH K. Red wine and hemorheology: complex results of in vitro and
in vivo studies in healthy volunteers. 14th International Congress of Biorheology
and 7th International Conference of Clinical Hemorheology, 4-7 July 2012, Koc
University, Istanbul, Turkey. Biorheol, 49 (2012), 109.

63
38. PAPP J., SANDOR B., TOTH A., HORVATH Z., BOTOR D., RABAI M., KENYERES P.,
JURICSKAY I., VAMOS Z., CSEPLO P., KOLLER A., TOTH K. In vitro and in vivo
comparison of platelet aggregation inhibitory effect of acetylsalicylic acid,
metamizole and their combination. 14th International Congress of Biorheology and
7th International Conference of Clinical Hemorheology, 4-7 July 2012, Koc
University, Istanbul, Turkey. Biorheol, 49 (2012), 110.
39. KESMARKY G., PAPP J., KOLTAI K., TOTH A., BOTOR D., SANDOR B., RABAI M.,
CSERNUS Z., TOTH K. Raynaud’s disease: haemorheological characteristics. 14th
International Congress of Biorheology and 7th International Conference of Clinical
Hemorheology, 4-7 July 2012, Koc University, Istanbul, Turkey. Biorheol, 49 (2012),
131.
40. KÉRMÁRKY G., BÍRÓ K., SÁNDOR B., PAPP J., TÓTH A., KOLTAI K. A perifériás
ütőérbetegség ellátása a bizonyítékok fényében. A Magyar Haemorheologiai
Társaság 20. Kongresszusa. 2013. július 8., Pécs. Érbetegségek, 20 (2013), 31-32.
41. TÓTH A., SANDOR B., PAPP J., BÓTOR D., RÁBAI M., KENYERES P., JURICSKAY I.,
TÓTH K. A vörösbor fogyasztás hatása a hemoreológiai paraméterekre egészséges
önkénteseken. A Magyar Kardiológusok Társasága 2013. évi Tudományos
Kongresszusa, 2013. május 8-11., Balatonfüred. Card Hung, 43 Suppl. B (2012),
B46.
42. PAPP J., SÁNDOR B., TÓTH A., BÓTOR D., RÁBAI M., KENYERES P., VÁMOS Z.,
KOLLER Á., TÓTH K. Trombocitaaggregáció-gátlás metamizollal, acetilszalicilsavval
és kombinációjukkal: in vitro és in vivo összehasonlítás. A Magyar Kardiológusok
Társasága 2013. évi Tudományos Kongresszusa, 2013. május 8-11., Balatonfüred.
Card Hung, 43 Suppl. B (2012), B115.
43. SÁNDOR B., TÓTH A., PAPP J., RÁBAI M., JURICSKAY I., MEZEY B., TÓTH K.,
SZABADOS E. Fizikai tréning hatása a hemoreológia paraméterekre ambuláns
kardiológiai rehabilitációban résztvevő iszkémiás szívbetegeknél. A Magyar
Kardiológusok Társasága 2013. évi Tudományos Kongresszusa, 2013. május 8-11.,
Balatonfüred. Card Hung, 43 Suppl. B (2012), B52.

64
44. SÁNDOR B., TÓTH A., MEZEY B., PAPP J., RÁBAI M., JURICSKAY I., TÓTH K.,
SZABADOS E. Fizikai tréning hatása az ambuláns kardiológiai rehabilitációban
résztvevő iszkémiás szívbetegekben. A Magyar Élettani, Farmakológiai és
Mikrocirkulációs Társaságok 2013. évi közös Tudományos Kongresszusa. 2013.
június 5-6., Budapest, Absztraktok, A-0013.
45. TOTH A., TOTSIMON K., SZUKITS S., VARADY E., SANDOR B., BOTOR D., VRYZAS N.,
PAPP J., RABAI M., KENYERES P., JURICSKAY I., KESMARKY G., BATTYANI I., SUMEGI
B., TOTH K. Hemorheological parameters in ischemic heart disease. 17th
Conference of the European Society for Clinical Hemorheology and
Microcirculation, 6-9 July 2013, Pecs, Hungary. Clin Hemorheol Microcirc, 52
(2013), 178.
46. SANDOR B., TOTH A., MEZEY B., RABAI M., PAPP J., JURICSKAY I., TOTH K.,
SZABADOS E. Effect of physical activity in ischemic heart disease patients
participating in a cardiological ambulatory rehabilitation program. 17th Conference
of the European Society for Clinical Hemorheology and Microcirculation, 6-9 July
2013, Pecs, Hungary. Clin Hemorheol Microcirc, 52 (2013), 178-179.
47. SANDOR B., BIRO K., TOTH A., JURICSKAY I., VARGA A., RABAI M., PAPP J., TOTH K.,
SZAKAY P. Aspirin resistance after kidney transplantation. 17th Conference of the
European Society for Clinical Hemorheology and Microcirculation, 6-9 July 2013,
Pecs, Hungary. Clin Hemorheol Microcirc, 52 (2013), 139.
48. KESMARKY G., SANDOR B., TOTH A., BIRO K., KOLTAI K., PAPP J., RABAI M., TOTH
K. Peripheral vascular diseases: Role of hemorheological factors. 17th Conference
of the European Society for Clinical Hemorheology and Microcirculation, 6-9 July
2013, Pecs, Hungary. Clin Hemorheol Microcirc, 52 (2013), 180.
49. KENYERES P., MIKO A., TOTH A., SANDOR B., CSALODI R., TOTH O., KOSZTOLANYI
S., SZOMOR A., NAGY A. Hemorheological disturbances in patients with chronic
myeloid neoplasms. 17th Conference of the European Society for Clinical
Hemorheology and Microcirculation, 6-9 July 2013, Pecs, Hungary. Clin Hemorheol
Microcirc, 52 (2013), 187.

65
50. TOTH A., BIRO K., SANDOR B., PAPP J., BOTOR D., RABAI M., KENYERES P.,
JURICSKAY I., TOTH K. The effects of red vine on hemorheological parameters in
healthy volunteers. Conference of Hungarian Medical Association of America
2013. 16-17 August 2013, Balatonfüred, Hungary. Archives of the Hungarian
Medical Association of America, 21 (2013), 34.
51. RÁBAI M., TÓTH A., SÁNDOR B., PAPP J., TÓTSIMON K., KENYERES P., JURICSKAY I.,
MEISELMAN H.J., TÓTH K. Vörösbor, alkoholmentes vörösborkivonat és etanol
hemoreológiai hatásai. Magyar Belgyógyász Társaság Dunántúli Szekciójának LVII.
Vándorgyűlése és a Hámori Artur Belgyógyászati Napok VI. 2013. június 6-8., Pécs
Magyar Belorvosi Archivum, 66 Suppl. 1 (2013), 42.
52. SÁNDOR B., TÓTH A., RÁBAI M., PAPP J., MEZEY B., TÓTH K., SZABADOS E.
Iszkémiás szívbetegek által végzett hosszú távú anaerob fizikai tréning
hemoreológiai és laboratóriumi hatásai. A Magyar Haemorheologiai Társaság, a
Magyar Mikrocirkulációs és Vaszkuláris Biológiai Társaság és a Magyar
Szabadgyökkutató Társaság IV. közös kongresszusa, 2014. április 4-5.,
Balatonkenese. Érbetegségek, 21 (2014), 43-44.
53. TÓTH A., SZUKITS S., VÁRADY E., SÁNDOR B., PAPP J., RÁBAI M., JURICSKAY .I, TÓTH
K., BATTYÁNI I., KÉSMÁRKY G. Haemorheológiai paraméterek szív CT-vel igazolt
coronaria-betegségben. A Magyar Haemorheologiai Társaság, a Magyar
Mikrocirkulációs és Vaszkuláris Biológiai Társaság és a Magyar Szabadgyökkutató
Társaság IV. közös kongresszusa, 2014. április 4-5., Balatonkenese. Érbetegségek,
21 (2014), 45.
54. SÁNDOR B., TÓTH A., RÁBAI M., PAPP J., MEZEY B., TÓTH K., SZABADOS E. Hosszú
távú fizikai tréning hatásai ambuláns kardiológiai rehabilitációban résztvevő
iszkémiás szívbetegekben. A Magyar Kardiológus Társaság 2014. évi Tudományos
Kongresszusa, 2014. május 14-17., Balatonfüred. Card Hun, 44 Suppl. E (2014), E5.
55. TÓTH A., SZUKITS S., VÁRADY E., SÁNDOR B., RÁBAI M., JURICSKAY I., KÉSMÁRKY
G., TÓTH K. Hemoreológiai paraméterek CT-vel igazolt koszorúér-betegségben. A
Magyar Kardiológus Társaság 2014. évi Tudományos Kongresszusa, 2014. május
14-17., Balatonfüred. Card Hun, 44 Suppl. E (2014), E89-E90.

66
MTMT közlemény és idéző összefoglaló táblázat
Tóth András adatai (2014.06.23.)
Közlemény típusok Száma Hivatkozások1
Teljes tudományos közlemények2 Összesen Részletezve Független Összes
I. Tudományos folyóiratcikk 12 --- --- ---
nemzetközi szakfolyóiratban --- 10 17 22
hazai kiadású szakfolyóiratban idegen nyelven --- 0 0 0
hazai kiadású szakfolyóiratban magyar nyelven --- 2 0 0
II. Könyvek 0 --- --- ---
a) Könyv, szerzőként 0 --- --- ---
idegen nyelvű --- 0 0 0
magyar nyelvű --- 0 0 0
b) Könyv, szerkesztőként 0 --- --- ---
idegen nyelvű --- 0 3--- ---
magyar nyelvű --- 0 --- ---
III. Könyvrészlet 0 --- --- ---
idegen nyelvű --- 0 0 0
magyar nyelvű --- 0 0 0
IV. Konferenciaközlemény folyóiratban vagy konferenciakötetben
0 --- --- ---
Idegen nyelvű --- 0 0 0
Magyar nyelvű --- 0 0 0
Tudományos közlemények összesen (I.-IV.) 12 --- 17 22
További tudományos művek4 --- 4 0 0
Összesített impakt faktor 14,5 --- --- ---
Idézetek száma5 --- --- 17 22
Hirsch index5 3 --- --- ---
Oktatási művek
Felsőoktatási tankönyv 0 --- --- ---
Idegen nyelvű --- 0 0 0
Magyar nyelvű --- 0 0 0
Felsőoktatási tankönyv része idegen nyelven --- 0 0 0
Felsőoktatási tankönyv része magyar nyelven --- 0 0 0
További oktatási művek 0 --- 0 0
Oltalmi formák 0 --- 0 0
Alkotás 0 --- 0 0
Ismeretterjesztő művek
Könyvek 0 --- 0 0
További művek 0 --- 0 0

67
Közérdekű és nem besorolt művek 0 --- 0 0
Absztrakt 51 --- 0 0
Egyéb szerzőség 0 --- 0 0
Idézők disszertációban, egyéb típusban 0 --- 1 8
Megjegyzések:
--- : Nem kitölthető cella
1 A hivatkozások a disszertáció és egyéb típusú idézők nélkül számolva. A disszertáció és egyéb típusú idézők összesítve a táblázat végén találhatók.
2 Teljes tudományos közlemény ebben az adatbázisban:
Folyóiratcikk: szakcikk/tanulmány, összefoglaló cikk, rövid közlemény, sokszerzős vagy csoportos szerzőségű közlemény, forráskiadás, recenzió/kritika, műkritika, esszé
Könyv: szakkönyv, monográfia, kézikönyv, tanulmánykötet, forráskiadás, kritikai kiadás, műhelytanulmány, atlasz
Könyvrészlet: szaktanulmány, fejezet, esszé, forráskiadás, recenzió/kritika, műkritika, műtárgyleírás, térkép, műhelytanulmány része
Konferenciaközlemény: folyóiratban, könyvben, egyéb konferenciakötetben megjelent legalább 3 oldal terjedelemben
Oltalmi formák: szabadalmak, mintaoltalmak (részletek) 3 Szerkesztőként nem részesedik a könyv idézéséből 4 Ide értve a teljes közlemények listájában nem szereplő publikációkat, a nem ismert lektoráltságú folyóiratokban megjelent műveket és minden olyan tudományos művet, ami a I.-IV. sorokban nem került összeszámlálásra. 5 A disszertációk és egyéb típusú idézők nélkül számolva (részletek)