How Trillium Health Partners Challenge: Providing Quality...
4
About Trillium Health Partners Trillium Health Partners (THP) encompasses three main sites – Credit Valley Hospital, Mississauga Hospital, and Queensway Health Centre – offering the full range of acute care hospital services, as well as a variety of community-based, specialized programs. THP serves the entire population of Mississauga Ontario, the 6th largest city in Canada. In 2016/2017, THP had 1,252 funded inpatient beds, over 270,000 emergency department visits, and over 63,000 admissions. How Trillium Health Partners Addressed Issues with High Patient Volumes and Coordinating Complex Care Challenge: Providing Quality Care Amidst Hospital Overcrowding Crisis Ontario’s healthcare system is facing an overcrowding crisis with hospitals regularly operating at or over 100% bed capacity, forcing them to treat patients in hallways. Trillium Health Partners is no different but as the only hospital serving the 6th largest city in Canada, which is expected to add 650,000 new residents by 2035 1 , the crisis was severe. While increasing capacity with more beds is the long-term solution and Government is supporting this, engagement with frontline clinicians identified that issues with communication had the greatest day-to-day impact on the quality and efficiency of patient care they delivered. Relying on outdated and unsecure methods to communicate, physicians, nurses, and allied health staff were unable to work cohesively as a team, resulting in burnout, unsafe practices, and ultimately a poor patient experience. Patients and family members were often left in the dark, unsure of the care being provided and not knowing who to ask when they had questions. Case Study Figure 1: Outdated & unsecure communication methods Accreditation Canada and the Joint Commission in the US highlight that effective communication is critical to the successful delivery of health care services 2,3 . Inefficient communications on average cost US hospitals $1.75M USD each year 4 .
Transcript of How Trillium Health Partners Challenge: Providing Quality...

About Trillium Health Partners
Trillium Health Partners (THP) encompasses three main sites – Credit Valley Hospital, Mississauga Hospital, and Queensway Health Centre – offering the full range of acute care hospital services, as well as a variety of community-based, specialized programs. THP serves the entire population of Mississauga Ontario, the 6th largest city in Canada. In 2016/2017, THP had 1,252 funded inpatient beds, over 270,000 emergency department visits, and over 63,000 admissions.
How Trillium Health Partners Addressed Issues with High Patient Volumes and Coordinating Complex Care
Challenge: Providing Quality Care Amidst Hospital Overcrowding Crisis
Ontario’s healthcare system is facing an overcrowding crisis with hospitals regularly operating at or over 100% bed capacity, forcing them to treat patients in hallways. Trillium Health Partners is no different but as the only hospital serving the 6th largest city in Canada, which is expected to add 650,000 new residents by 20351, the crisis was severe. While increasing capacity with more beds is the long-term solution and Government is supporting this, engagement with frontline clinicians identified that issues with communication had the greatest day-to-day impact on the quality and efficiency of patient care they delivered. Relying on outdated and unsecure methods to communicate, physicians, nurses, and allied health staff were unable to work cohesively as a team, resulting in burnout, unsafe practices, and ultimately a poor patient experience. Patients and family members were often left in the dark, unsure of the care being provided and not knowing who to ask when they had questions.
Case Study
Figure 1: Outdated & unsecure communication methods
Accreditation Canada and the Joint Commission in the US highlight that effective communication is critical to the successful delivery of health care services2,3. Inefficient communications on average cost US hospitals $1.75M USD each year4.
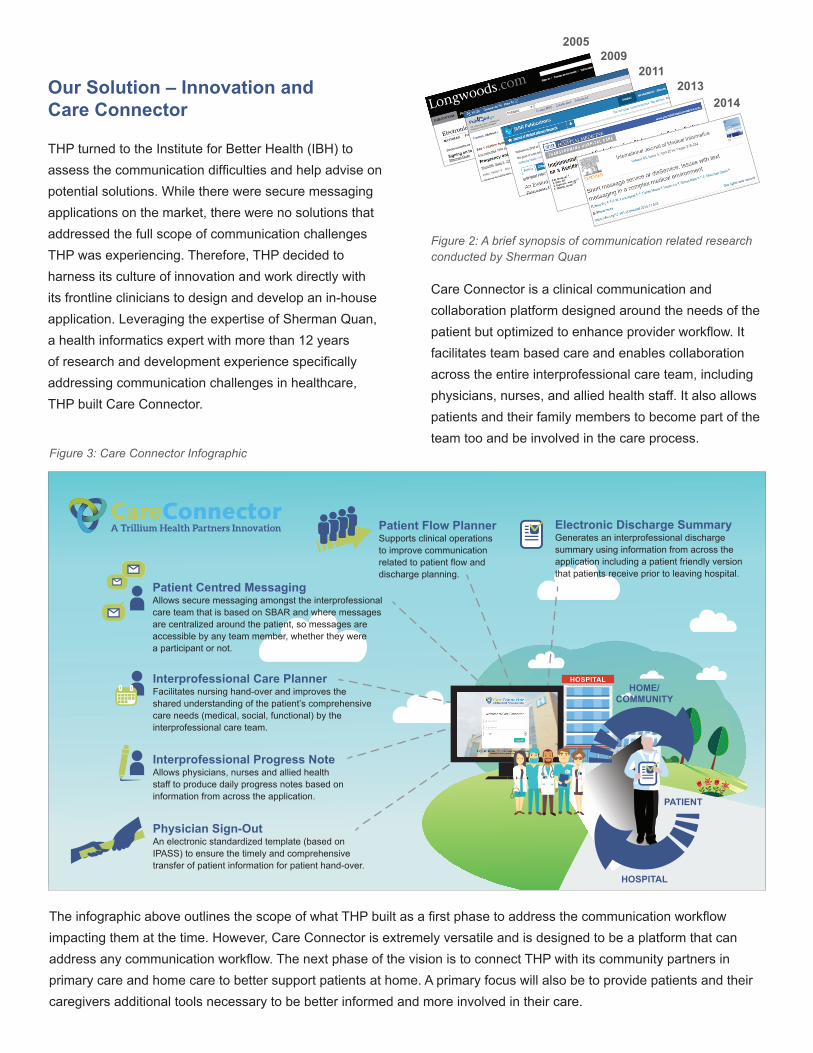
Our Solution – Innovation and Care Connector
THP turned to the Institute for Better Health (IBH) to assess the communication difficulties and help advise on potential solutions. While there were secure messaging applications on the market, there were no solutions that addressed the full scope of communication challenges THP was experiencing. Therefore, THP decided to harness its culture of innovation and work directly with its frontline clinicians to design and develop an in-house application. Leveraging the expertise of Sherman Quan, a health informatics expert with more than 12 years of research and development experience specifically addressing communication challenges in healthcare, THP built Care Connector.
Care Connector is a clinical communication and collaboration platform designed around the needs of the patient but optimized to enhance provider workflow. It facilitates team based care and enables collaboration across the entire interprofessional care team, including physicians, nurses, and allied health staff. It also allows patients and their family members to become part of the team too and be involved in the care process.
Electronic Discharge SummaryGenerates an interprofessional discharge summary using information from across the application including a patient friendly version that patients receive prior to leaving hospital.
HOME/COMMUNITY
HOSPITAL
Interprofessional Progress NoteAllows physicians, nurses and allied health staff to produce daily progress notes based on information from across the application. PATIENT
Interprofessional Care PlannerFacilitates nursing hand-over and improves the shared understanding of the patient’s comprehensive care needs (medical, social, functional) by the interprofessional care team.
Patient Centred MessagingAllows secure messaging amongst the interprofessional care team that is based on SBAR and where messages are centralized around the patient, so messages are accessible by any team member, whether they were a participant or not.
Patient Flow PlannerSupports clinical operations to improve communication related to patient flow and discharge planning.
Physician Sign-OutAn electronic standardized template (based on IPASS) to ensure the timely and comprehensive transfer of patient information for patient hand-over.
The infographic above outlines the scope of what THP built as a first phase to address the communication workflow impacting them at the time. However, Care Connector is extremely versatile and is designed to be a platform that can address any communication workflow. The next phase of the vision is to connect THP with its community partners in primary care and home care to better support patients at home. A primary focus will also be to provide patients and their caregivers additional tools necessary to be better informed and more involved in their care.
20052009
20112013
2014
Figure 2: A brief synopsis of communication related research conducted by Sherman Quan
Figure 3: Care Connector Infographic
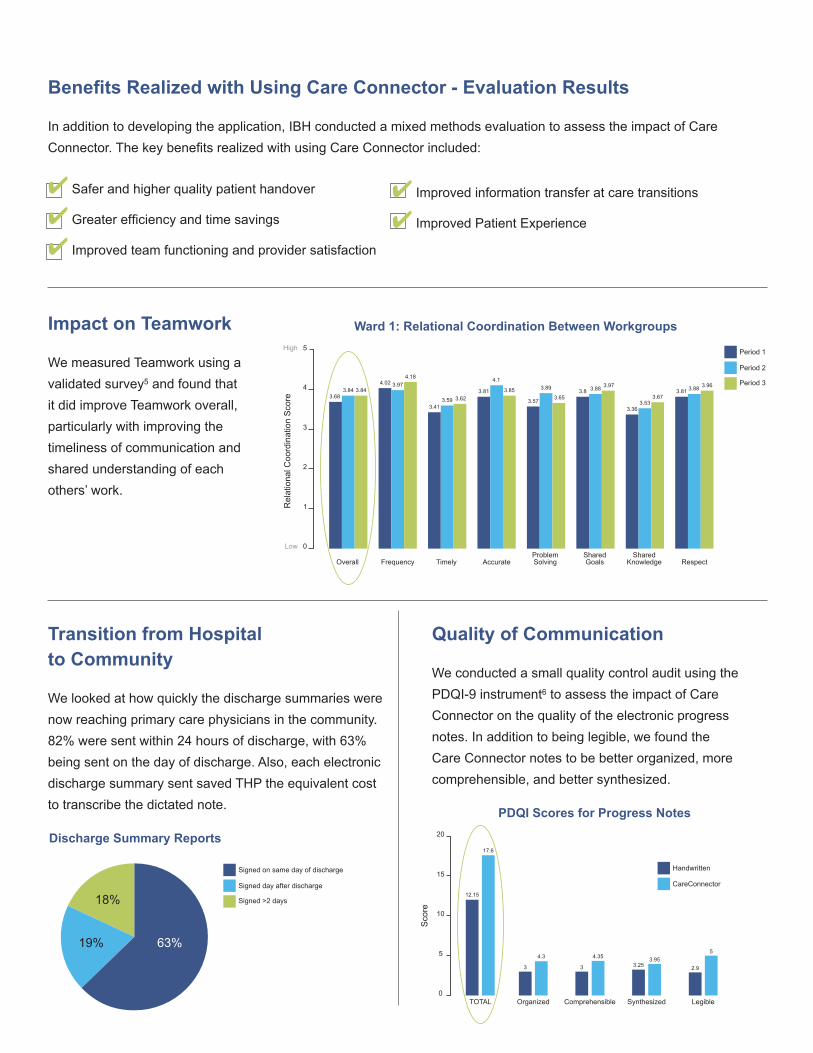
Benefits Realized with Using Care Connector - Evaluation Results
In addition to developing the application, IBH conducted a mixed methods evaluation to assess the impact of Care Connector. The key benefits realized with using Care Connector included:
4 Safer and higher quality patient handover
4 Greater efficiency and time savings
4 Improved team functioning and provider satisfaction
Impact on Teamwork
We measured Teamwork using a validated survey5 and found that it did improve Teamwork overall, particularly with improving the timeliness of communication and shared understanding of each others’ work.
Transition from Hospital to Community
We looked at how quickly the discharge summaries were now reaching primary care physicians in the community.
Quality of Communication
We conducted a small quality control audit using the PDQI-9 instrument6 to assess the impact of Care Connector on the quality of the electronic progress notes. In addition to being legible, we found the Care Connector notes to be better organized, more comprehensible, and better synthesized.
4 Improved information transfer at care transitions
4 Improved Patient Experience
3.68
3.41
3.81 3.85 3.89 3.8
12.15
17.6
3.363.53
3.673.81 3.88 3.963.88 3.97
3.57 3.65
4.1
3.623.59
3.84 3.844.02 3.97
4.18
Overall
TOTAL
3
4.3
Organized
3
4.35
Comprehensible
3.253.95
Synthesized
2.9
5
Legible
Frequency Timely AccurateProblemSolving
SharedGoals
SharedKnowledge Respect
Period 1
Period 2
Period 3
Signed on same day of discharge
Signed day after discharge
Signed >2 days
Handwritten
CareConnector
Rel
atio
nal C
oord
inat
ion
Sco
re
Low
High
0
1
2
3
4
5
Ward 1: Relational Coordination Between Workgroups
Discharge Summary Reports
PDQI Scores for Progress Notes
18%
19% 63%
Sco
re
0
5
10
15
20
3.68
3.41
3.81 3.85 3.89 3.8
12.15
17.6
3.363.53
3.673.81 3.88 3.963.88 3.97
3.57 3.65
4.1
3.623.59
3.84 3.844.02 3.97
4.18
Overall
TOTAL
3
4.3
Organized
3
4.35
Comprehensible
3.253.95
Synthesized
2.9
5
Legible
Frequency Timely AccurateProblemSolving
SharedGoals
SharedKnowledge Respect
Period 1
Period 2
Period 3
Signed on same day of discharge
Signed day after discharge
Signed >2 days
Handwritten
CareConnector
Rel
atio
nal C
oord
inat
ion
Sco
re
Low
High
0
1
2
3
4
5
Ward 1: Relational Coordination Between Workgroups
82% were sent within 24 hours of discharge, with 63% being sent on the day of discharge. Also, each electronic discharge summary sent saved THP the equivalent cost to transcribe the dictated note.
Discharge Summary Reports
PDQI Scores for Progress Notes
18%
19% 63%
Sco
re
0
5
10
15
20
3.68
3.41
3.81 3.85 3.89 3.8
12.15
17.6
3.363.53
3.673.81 3.88 3.963.88 3.97
3.57 3.65
4.1
3.623.59
3.84 3.844.02 3.97
4.18
Overall
TOTAL
3
4.3
Organized
3
4.35
Comprehensible
3.253.95
Synthesized
2.9
5
Legible
Frequency Timely AccurateProblemSolving
SharedGoals
SharedKnowledge Respect
Period 1
Period 2
Period 3
Signed on same day of discharge
Signed day after discharge
Signed >2 days
Handwritten
CareConnector
Rel
atio
nal C
oord
inat
ion
Sco
re
Low
High
0
1
2
3
4
5
Ward 1: Relational Coordination Between Workgroups
Discharge Summary Reports
PDQI Scores for Progress Notes
18%
19% 63%
Sco
re
0
5
10
15
20

For more information or to schedule a demo, contact:
Clinician Feedback
We also conducted formal interviews with frontline clinicians to understand their experiences with using the Care Connector application. This is what our clinicians told us:
1. The Credit Valley Hospital and Trillium Health Centre. Strategic Planning, Setting the Stage: Environmental Scan, Appendix to the Strategic Planning Discussion Framework. May 7,2012
2. Accreditation Canada Required Organization Practices Handbook 20173. Joint Commission. https://www.jointcommission.org/facts_about_patient-centered_communications/ 4. Spyglass Consulting report in a 2014 on a point of care communications study5. Relational Coordination Analytics Survey: http://rcanalytic.com/6. Stetson PD et al. 2012. Assessing Electronic Note Quality Using the Physician Documentation Quality Instrument (PDQI-9) Appl Clin Inform 3(2):164-74
“I think that it’s affected teamwork in a positive way.” [Allied Health]
I think it’s great - it provides a lot of consistency in terms of the information that you get in handover, it’s just an effective way to pass information on so that nothing is missed.” [Nurse]“
Because any time you have these complex patients with lots of needs, where you hand off the care from person to person, having something like this is a Godsend… it’s better, it’s easier, it’s safer.” [Physician]
“
“It’s user friendly. I have never seen something as simple, so easy to use, as care connector. I think it’s because we’re building it from the ground up. We’re building it from the user perspective. [Nurse]