HOW TO SPOT A NEUROLOGIC CONDITION
3
APRIL 2021 | 41 SUBFOCUS NEURO-OPTOMETRY T he eye is a window to the brain and the rest of the central ner- vous system, enabling optome- trists to identify telltale signs of neurologic conditions. Some of these disorders are sight-threatening and others can be life-threatening. The ability to recognize both the dis- tinct and subtle symptoms and clini- cal signs of neuro-ophthalmic disease puts optometry in a position to posi- tively affect a patient’s quality of life. Prompt, appropriate examination and additional workup are critical in estab- lishing an accurate diagnosis. Facilitating timely medical or surgical treatment, when necessary, is of utmost impor- tance to ensure a positive ocular and systemic outcome. This article describes some of the “don’t miss” signs that every clinician should know about. HISTORY AND BASELINE NEURO-OPHTHALMIC EXAMINATION The neuro-ophthalmic examination always begins with a thorough history. This includes eliciting the patient’s chief complaint along with his or her specific medical history, ocular history, social his- tory, review of systems, and list of present medications. The history should be fol- lowed by a comprehensive ophthalmic assessment of the afferent visual system. 1 Spatial resolution of vision (ie, BCVA) in each eye should be determined at distance and near (refraction, pinhole, or potential acuity images). Color vision via Ishihara pseudo-isochromatic plates or Hardy-Rand-Rittler plates, pupillary testing, visual field testing (confrontation field, static automated perimetry, Goldmann kinetic manual perimetry, or tangent screen), contrast sensitivity, brightness comparison, and photostress recovery testing should all HOW TO SPOT A NEUROLOGIC CONDITION Keep an eye out for red flags and you just might save a life. BY CARLO J. PELINO, OD, FAAO; JOSEPH J. PIZZIMENTI, OD, FAAO; AND CLAIRE E. PIZZIMENTI, OD, FAAO
Transcript of HOW TO SPOT A NEUROLOGIC CONDITION

APRIL 2021 | 41
SUBFOCUS NEURO-OPTOMETRY �
The eye is a window to the brain and the rest of the central ner-vous system, enabling optome-trists to identify telltale signs of neurologic conditions. Some of
these disorders are sight-threatening and others can be life-threatening. The ability to recognize both the dis-tinct and subtle symptoms and clini-cal signs of neuro-ophthalmic disease puts optometry in a position to posi-tively affect a patient’s quality of life.
Prompt, appropriate examination and additional workup are critical in estab-lishing an accurate diagnosis. Facilitating
timely medical or surgical treatment, when necessary, is of utmost impor-tance to ensure a positive ocular and systemic outcome. This article describes some of the “don’t miss” signs that every clinician should know about.
HISTORY AND BASELINE NEURO-OPHTHALMIC EXAMINATION
The neuro-ophthalmic examination always begins with a thorough history. This includes eliciting the patient’s chief complaint along with his or her specific medical history, ocular history, social his-tory, review of systems, and list of present
medications. The history should be fol-lowed by a comprehensive ophthalmic assessment of the afferent visual system.1
Spatial resolution of vision (ie, BCVA) in each eye should be determined at distance and near (refraction, pinhole, or potential acuity images). Color vision via Ishihara pseudo-isochromatic plates or Hardy-Rand-Rittler plates, pupillary testing, visual field testing (confrontation field, static automated perimetry, Goldmann kinetic manual perimetry, or tangent screen), contrast sensitivity, brightness comparison, and photostress recovery testing should all
HOW TO SPOT A NEUROLOGIC CONDITION
Keep an eye out for red flags and you just might save a life. BY CARLO J. PELINO, OD, FAAO; JOSEPH J. PIZZIMENTI, OD, FAAO; AND CLAIRE E. PIZZIMENTI, OD, FAAO

42 | APRIL 2021
� SUBFOCUS NEURO-OPTOMETRY
be performed, along with a thorough examination of the fundus with direct and indirect ophthalmoscopy.
The neuro-ophthalmic examination should then concentrate on the effer-ent system. Disorders of this system usually include ocular misalignment or motility (comitant or incomitant) issues such as diplopia, head tilt, face turn, etc. The testing should be performed in a systematic way to efficiently identify a potential neuro-ophthalmic cause and potential life-threatening condition. Evaluation of the efferent system should include ductions and versions, saccades, pursuits, eyelid positioning and function, pupillary testing (symmetry, size, and reactivity), and nystagmus evaluation. Forced duction and doll’s head maneu-ver testing may be performed as needed. The optometrist may need to perform a quick exam to evaluate the patient’s mental status, motor reflexes, coordina-tion/gait, and general sensory receptors.
TELLTALE SIGNS AND SYMPTOMSThe signs and symptoms discussed
below, even though they may be intertwined at times, should make the eye care provider aware of a possible neurologic etiology. A discussion of the tests that would rule out a neurologic etiology is beyond the scope of this article, but in all cases of neurologic eye disease the clinician should use his or her professional judgement in deciding when to obtain consultation or make a referral. When in doubt, such consult or referral should be prompt, and the patient should be evaluated by a neuro-ophthalmologist, a neurologist, or an optometrist skilled in neuroeye disease.
Sudden Vision LossFrequent causes include arteritic and
nonarteritic anterior ischemic optic neu-ropathy, branch or central retinal artery occlusion, ocular ischemia, optic neuritis, pituitary apoplexy, ischemic or hemor-rhagic stroke, and acute meningitis.2-4
PtosisAn acquired ptosis may occur in con-
ditions such as a third cranial nerve palsy,
myasthenia gravis, and Horner syndrome (carotid artery dissection, intracranial malformations, and apical lung lesion).2-4
Binocular DiplopiaThis condition may be caused by cra-
nial nerve paresis (due to aneurysm, arte-ritic anterior ischemic optic neuropathy, multiple sclerosis, stroke, tumors), myop-athies (myasthenia gravis), and nutrition-al deficiency (Wernicke encephalopathy). Diplopia is the most common symptom of the efferent system. Cranial nerve 3, 4, and 6 palsies, myasthenia gravis, thyroid eye disease, skew deviation, internuclear ophthalmoplegia, chronic progressive external ophthalmoplegia, and dorsal midbrain syndrome (a.k.a. Parinaud syn-drome) should all be ruled out.2-4
AnisocoriaNonphysiologic anisocoria may pres-
ent in partial or complete third cranial nerve paresis (cerebral aneurysm/ischemia), Horner syndrome, and uncal (transtentorial) herniation.2-4
An example of a true ocular emer-gency affecting the efferent system is a pupil-involved third cranial nerve palsy. The presenting signs and symptoms may signal an apparent aneurysm that could eventually rupture and lead to a subarachnoid hemorrhage. Also known as the oculomotor nerve, the third cra-nial nerve supplies several extraocular muscles, the levator muscle, the ciliary muscle, and the iris sphincter.5
Because of this nerve’s vast repre-sentation, a third nerve palsy has a varied presentation that can include ocular movement disturbances, ptosis, and pupillary abnormalities such as a sluggish or dilated fixed response. In this instance, time is of the essence to rule out a compressive lesion (aneu-rysm), giant cell arteritis, pituitary
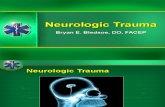
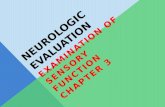
Figure 1. Retinal imaging showing bilateral disc edema in a 24-year-old Black male with complaints of recent-onset transient visual obscurations in each eye and bilateral pulsatile tinnitus. Neuroimaging with subsequent lumbar puncture confirmed a diagnosis of idiopathic intracranial hypertension.
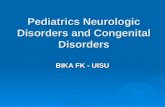
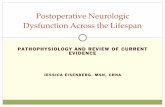
Figure 2. OCT of the patient in Figure 1 revealed significant bilateral disc elevation with profoundly thick peripapillary retinal nerve fiber layer in both eyes, consistent with optic disc edema. These qualitative and quantitative parameters are expected to improve with continued treatment of the patient’s idiopathic intracranial hypertension.
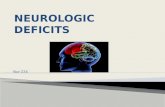
Figure 3. Optic disc edema should prompt the clinician to rule out its myriad causes, from compression to demyelination to ischemia.

APRIL 2021 | 43
SUBFOCUS NEURO-OPTOMETRY �
apoplexy, midbrain infarction, or demyelinating disease. Blood tests, along with certain neuroimaging techniques such as MR angiography or CT angiography, must be performed.5
PapilledemaTrue papilledema is defined as optic
disc swelling due to high intracranial pressure (ICP).6 Its causative condi-tions can include hydrocephalus, spinal cord lesions, cerebral sinus drainage impairment, intracerebral mass, idiopathic intracranial hyperten-sion (Figures 1–3), cerebral hemor-rhage, and meningitis (see Differential Diagnosis of Bilateral Disc Edema).
A thorough neuro-ophthalmic workup helps the clinician sort through the many differential diagnoses. Visual function loss is the feared morbidity of papilledema. Treatment is directed at the underlying cause of the high ICP, and options include both medical and surgical modalities.
NystagmusNystagmus is a spontaneous, repeti-
tive, to-and-fro movement of the eyes. Acquired nystagmus may result from transient ischemic attack, stroke, intracranial hemorrhage, demyelinat-ing disease, or tumor.7
The two main types of acquired adult nystagmus are jerk, named for its fast corrective phase, and pendular, which has slow, back-and-forth phases. Neoplastic disease presenting as an acquired nystagmus may involve brain stem and/or cerebellar-vestibular path-ways from the otoliths to the cerebel-lum, and from the entire brainstem up to the thalamus.7
Head and Neck TraumaNeuro-ophthalmic signs may include
carotid-cavernous fistula (CCF), pain-ful Horner syndrome (secondary to carotid artery dissection), and traumatic optic neuropathy. CCF is an abnormal connection between the cavernous sinus and the carotid artery and/or its branches.8 A CCF may be either direct (high-flow) or spontaneous (indirect or low-flow). CCF can develop because of either trauma or spontaneous causes.
Traumatic CCF may occur after a head injury in which the intracavernous carotid artery is torn.8 Patients with CCF present with the classic triad of chemo-sis, pulsatile exophthalmos, and ocular bruit. Proptosis, diplopia, and visual loss may result from these fistulas.8
KNOW WHAT TO LOOK FORSudden-onset ptosis, a dilated pupil,
diplopia, and a sore scalp with jaw pain are among the signs and symptoms of a neuro-ophthalmic condition that can threaten sight and life. The optometrist is sometimes the first health care prac-titioner the patient sees. It is essential to know how to take a proper history, conduct a thorough examination, and order laboratory testing and imaging, and when to refer a patient to the appro-priate subspecialist in order to ensure timely treatment and management. n
1. Savino, PJ, Danish-Meyer HV. Color atlas and synopsis of clinical ophthalmology. In: Rapuano CJ, ed. Neuro-Ophthalmology. Examination of the Afferent Visual System. Lippincott, Williams & Wilkins; 2018: 2-11 and 284-298.2. Lemos J, Eggenberger E. Neuro-ophthalmological emergencies. Neurohospitalist. 2015;5(4);223-233.3. Turgut B, Karanfil FÇ, Turgut FA. Neuro-ophthalmological emergency disorders: a general view. Int J Clin Exp Ophthalmol. 2017;1:060-066.4. Cooper T. Neuro-ophthalmology illustrated chapter 19 – diagnosis of headache and facial pain 2. Stanford School of Medicine. September 8, 2020. neuro-ophthalmology.stanford.edu. Accessed March 15, 2021.5. Doran M, Karmel, M, Stuart A. 4 Neuro conditions not to be missed. EyeNet Magazine. June 2012.6. Rigi M, Almarzouqi SJ, Morgan ML, Lee AG. Papilledema: epidemiology, etiology, and clinical management. Eye Brain. 2015;7:47-57.7. Stahl JS, Averbuch-Heller L, Leigh RJ. Acquired nystagmus. Arch Ophthalmol. 2000;118(4):544-549.8. Heydenrych LG, Du Toit N, Le Feuvre D. Open-angle glaucoma and an enlarged superior orbital fissure caused by trauma. JAMA Ophthalmol. 2016;134(1):103-104.
CARLO J. PELINO, OD, FAAOn Chief, The Eye Institute of Salus University,
Chestnut Hill, Pennsylvanian [email protected] Financial disclosure: None
CLAIRE E. PIZZIMENTI, OD, FAAOn Senior Clinical Instructor, Rosenberg School of
Optometry, University of the Incarnate Word, San Antonio, Texas
n [email protected] Financial disclosure: None
JOSEPH J. PIZZIMENTI, OD, FAAOn Professor, Rosenberg School of Optometry,
University of the Incarnate Word, San Antonio, Texasn pizzimen@uiwtx@edu; Twitter @jpizzodn Financial disclosure: None
s
Neuro-ophthalmic disease can have many different presentations.
s
A patient with sudden vision loss, relative afferent pupillary defect, bitemporal hemianopia, and a pale optic nerve, along with acute-onset nystagmus, new ptosis, binocular diplopia, anisocoria, trauma, or optic disc edema should put optometrists on high alert.
s
Proper history, thorough examination, testing, imaging, and communication are essential for timely diagnosis and management.
AT A GLANCE
• Idiopathic intracranial hypertension
• Compressive optic neuropathy
• Hydrocephalus/venous sinus thrombosis
• Optic neuritis
• Metabolic/toxic optic neuropathy
• Diabetic papillopathy
• Malignant hypertension
• Pseudopapilledema
• Anterior ischemic optic neuropathy
• Blood dyscrasias
• Autoimmune processes
DIFFERENTIAL DIAGNOSIS OF BILATERAL DISC EDEMA1