How Important Is the Role of the Internal Anal Sphincter...
5
How Important Is the Role of the Internal Anal Sphincter in Fecal Continence? An Experimental Study in Dogs By S.Y. Yoo, K.S. Bae, S.J. Kang, S.Y. Kim, and E.H. Hwang Wonju, South Korea • It is a generalized concept that the internal anal sphincter (IAS) plays a significant role in fecal continence by generating high pressure in the anal canal at rest and relaxation during rectal distention. Agreement also exists on the importance of internal sphincter-saving anoplasty on anorectal malforma- tions in establishing anal continence. Twelve dogs were divided into four groups. Group 1, a control group, was subjected to a perirectal dissection only. Group 2 underwent the same perirectal dissection plus a 2-cm resection of the anal canal. Group 3 underwent the perirectal dissection plus a 4-cm resection of the anal canal, and group 4 underwent perirectal dissection and transposition of the anus to the posterolateral portion of the voluntary muscle mass. Clinical continence was evaluated, and manometric results were compared with preoperative measurements. All dogs in groups 1, 2, and 3 were clinically continent without soiling except one in group 3, and also manometric results showed minimal change between preoperative and postoperative anal pressure profiles. The transposed anus of group 4 showed continuous fecal soiling. The anal resting pressure (ARP) was also decreased but still existed in this group. This experimental study showed that the IAS contributes to the anal resting tone. However, resection of the IAS did not completely interfere with fecal continence. The smooth muscle of pulled-through rectum seemed to partly take over the function of the IAS. Copyright © 1995by W.B. Saunders Company INDEX WORDS: Internal anal sphincter; anorectal malforma- tions; fecal continence; anal resting pressure; rectoanal inhibitory reflex. B EFORE Pefia and Devries (1982) 1 introduced the posterior midsagittal approach for anorecto- plasty (PSARP) of anorectal malformations, the ma- jor concern of pediatric surgeons had been how to position the rectum in an anatomically normal posi- tion without damage to the voluntary muscles. The anatomical results have improved remarkably with this procedure, and the functional results have also been better than with other procedures; however, normal bowel control still could not be achieved in many patients. Recently several pediatric surgeons 2-6 have paid attention to the internal anal sphincter (IAS) during operations on anorectal malformations because sev- eral follow-up results after anoplasty showed rela- tively good continence in patients with high anal resting pressure (ARP) and normal rectoanal inhibi- tory reflex (RAIR). 7-1° Also Lembrecht and Lierse 11 in 1987 microscopically showed the presence of the IAS in neonatal pigs with various types of imperforate anus. It has been well known that the IAS generates high pressure in the anal canal at rest and relaxes during rectal distention. However, there are still unanswered questions regarding the significance of the ARP and the RAIR in fecal continence. Is it possible to maintain normal continence without the IAS? The purpose of this study is to evaluate the role of the IAS in fecal continence by noting the change in bowel movements and the anal pressure after resec- tion of the anorectum in dogs. MATERIALS AND METHODS Twelve mongrel dogs, 3 to 6 months-old and weighing 10 to 14 kg, were divided into four groups of 3 animals each. Bowel movement patterns were observed for 1 week before operation, and preoperative manometric examinations were carried out in all the animals. Bowels were prepared with ampicillin (50 mg/kg/d orally), amikacin (15 mg/kg/d intramuscularly) for 48 hours, Colonlyte (1,000 mL/d orally) (Taekwang Pharmaceutical Co, Ltd, Seoul, Korea) for 24 hours, and a saline enema two times before operation. All manometric examinations and operations were done under general anesthesia with intravenous Entobar (pentobarbital sodium, 25 mg/kg) (Hanrim Pharmaceutical Co, Ltd, Seoul, Korea) injection. Group 1, a control group, was subjected to only a circumferential dissection of the anorectum through a posterior midline skin incision, without any voluntary muscle division or split. The perirectal dissection was performed to the level of pelvic perito- neum, without damage to the voluntary muscle. Anoplasty was done with 5-0 Vicryl sutures in the original anal position. Group 2 underwent the same perirectal dissection as group 1, as well as a 2-cm resection of the terminal bowel. The cut end of the proximal bowel was pulled through to the skin level, and anchoring sutures were placed between the rectal wall and the perirectal tissue to prevent mucosal prolapse. All voluntary muscle was preserved, and the anoplasty was done in the same manner as used in group 1. Group 3 underwent the same perirectal dissection and a 4-cm resection of the anorectum (Fig 1). The cut end of the proximal bowel was brought down to the skin, and many anchoring sutures were placed to prevent mucosal prolapse. Group 4 had the same perirectal dissection, and the dissected anorectum was pulled through a new canal made posterolaterally out of the voluntary muscle. Postoperatively all dogs had antibiotic therapy with intrave- nous injection of cephalothin (50 mg/kg/d) and amikacin (15 From the Division of Pediatric Surgery, Department of Surgery, Yonsei University, Wonju College of Medicine, Wonju, South Korea. Presented at the 27th Annual Meeting of the Pacific Association of Pediatric Surgeons, Kagoshima, Japan, May 23-27, I994. Address reprint requests to Soo-Young Yoo, MD, Pediatric Surgery, Yonsei University, Wonju College of Medicine, 162 Ilsandong, Wonju 220- 701, South Korea. Copyright © 1995 by W.B. Sounders Company 0022-3468/ 95/3005-0013503. O0 / 0 Journal of Pediatric Surgery, Vol 30, No 5 (May), 1995: pp 687-691 687
Transcript of How Important Is the Role of the Internal Anal Sphincter...

How Important Is the Role of the Internal Anal Sphincter in Fecal Continence? An Experimental Study in Dogs
By S.Y. Yoo, K.S. Bae, S.J. Kang, S.Y. Kim, and E.H. Hwang Wonju, South Korea
• It is a generalized concept that the internal anal sphincter (IAS) plays a significant role in fecal continence by generating high pressure in the anal canal at rest and relaxation during rectal distention. Agreement also exists on the importance of internal sphincter-saving anoplasty on anorectal malforma- tions in establishing anal continence. Twelve dogs were divided into four groups. Group 1, a control group, was subjected to a perirectal dissection only. Group 2 underwent the same perirectal dissection plus a 2-cm resection of the anal canal. Group 3 underwent the perirectal dissection plus a 4-cm resection of the anal canal, and group 4 underwent perirectal dissection and transposition of the anus to the posterolateral portion of the voluntary muscle mass. Clinical continence was evaluated, and manometric results were compared with preoperative measurements. All dogs in groups 1, 2, and 3 were clinically continent without soiling except one in group 3, and also manometric results showed minimal change between preoperative and postoperative anal pressure profiles. The transposed anus of group 4 showed continuous fecal soiling. The anal resting pressure (ARP) was also decreased but still existed in this group. This experimental study showed that the IAS contributes to the anal resting tone. However, resection of the IAS did not completely interfere with fecal continence. The smooth muscle of pulled-through rectum seemed to partly take over the function of the IAS. Copyright © 1995by W.B. Saunders Company
INDEX WORDS: Internal anal sphincter; anorectal malforma- tions; fecal continence; anal resting pressure; rectoanal inhibitory reflex.
B EFORE Pefia and Devries (1982) 1 introduced the posterior midsagittal approach for anorecto-
plasty (PSARP) of anorectal malformations, the ma- jor concern of pediatric surgeons had been how to position the rectum in an anatomically normal posi- tion without damage to the voluntary muscles. The anatomical results have improved remarkably with this procedure, and the functional results have also been better than with other procedures; however, normal bowel control still could not be achieved in many patients.
Recently several pediatric surgeons 2-6 have paid attention to the internal anal sphincter (IAS) during operations on anorectal malformations because sev- eral follow-up results after anoplasty showed rela- tively good continence in patients with high anal resting pressure (ARP) and normal rectoanal inhibi- tory reflex (RAIR). 7-1° Also Lembrecht and Lierse 11 in 1987 microscopically showed the presence of the IAS in neonatal pigs with various types of imperforate anus. It has been well known that the IAS generates
high pressure in the anal canal at rest and relaxes during rectal distention. However, there are still unanswered questions regarding the significance of the ARP and the RAIR in fecal continence. Is it possible to maintain normal continence without the IAS?
The purpose of this study is to evaluate the role of the IAS in fecal continence by noting the change in bowel movements and the anal pressure after resec- tion of the anorectum in dogs.
MATERIALS AND METHODS
Twelve mongrel dogs, 3 to 6 months-old and weighing 10 to 14 kg, were divided into four groups of 3 animals each. Bowel movement patterns were observed for 1 week before operation, and preoperative manometric examinations were carried out in all the animals. Bowels were prepared with ampicillin (50 mg/kg/d orally), amikacin (15 mg/kg/d intramuscularly) for 48 hours, Colonlyte (1,000 mL/d orally) (Taekwang Pharmaceutical Co, Ltd, Seoul, Korea) for 24 hours, and a saline enema two times before operation. All manometric examinations and operations were done under general anesthesia with intravenous Entobar (pentobarbital sodium, 25 mg/kg) (Hanrim Pharmaceutical Co, Ltd, Seoul, Korea) injection.
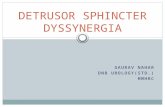
Group 1, a control group, was subjected to only a circumferential dissection of the anorectum through a posterior midline skin incision, without any voluntary muscle division or split. The perirectal dissection was performed to the level of pelvic perito- neum, without damage to the voluntary muscle. Anoplasty was done with 5-0 Vicryl sutures in the original anal position. Group 2 underwent the same perirectal dissection as group 1, as well as a 2-cm resection of the terminal bowel. The cut end of the proximal bowel was pulled through to the skin level, and anchoring sutures were placed between the rectal wall and the perirectal tissue to prevent mucosal prolapse. All voluntary muscle was preserved, and the anoplasty was done in the same manner as used in group 1. Group 3 underwent the same perirectal dissection and a 4-cm resection of the anorectum (Fig 1). The cut end of the proximal bowel was brought down to the skin, and many anchoring sutures were placed to prevent mucosal prolapse. Group 4 had the same perirectal dissection, and the dissected anorectum was pulled through a new canal made posterolaterally out of the voluntary muscle. Postoperatively all dogs had antibiotic therapy with intrave- nous injection of cephalothin (50 mg/kg/d) and amikacin (15
From the Division of Pediatric Surgery, Department of Surgery, Yonsei University, Wonju College of Medicine, Wonju, South Korea.
Presented at the 27th Annual Meeting of the Pacific Association of Pediatric Surgeons, Kagoshima, Japan, May 23-27, I994.
Address reprint requests to Soo-Young Yoo, MD, Pediatric Surgery, Yonsei University, Wonju College of Medicine, 162 Ilsandong, Wonju 220- 701, South Korea.
Copyright © 1995 by W.B. Sounders Company 0022-3468 / 95/3005-0013503. O0 / 0
Journal of Pediatric Surgery, Vol 30, No 5 (May), 1995: pp 687-691 687
688 YOO ET AL
Fig 1. Perirectal dissection and a 4-cm resection of the distal bowel through a posterior midline skin incision.
mg/kg/d) for 24 hours and then oral ampicillin (50 mg/kg/d) for 3 days. A liquid diet was started the day after the operation and was continued for 2 days, followed by a regular diet.
Postoperative fecal continence was clinically evaluated for 2 months with regard to frequency of bowel movements, perineal soiling, and the shape of stools piled or scattered in the bottom of the cages. Those observations were compared with preoperative patterns. Anorectal manometric examinations were performed three times in every dog, at 4, 8, and 12 weeks postoperatively. Anorectal pressure profiles at rest and during rectal ballooning were recorded via a three-channel pressure measurement unit (Model-05, Martin Gruber GmbH & Co KG, Munich, Germany). The anal pressure was measured at a distance of between i and 2 cm from the anal verge, depending on where the highest pressure was recorded. The manometric results were compared with preop- erative pressure profiles.
RESULTS
Perineal Appearance
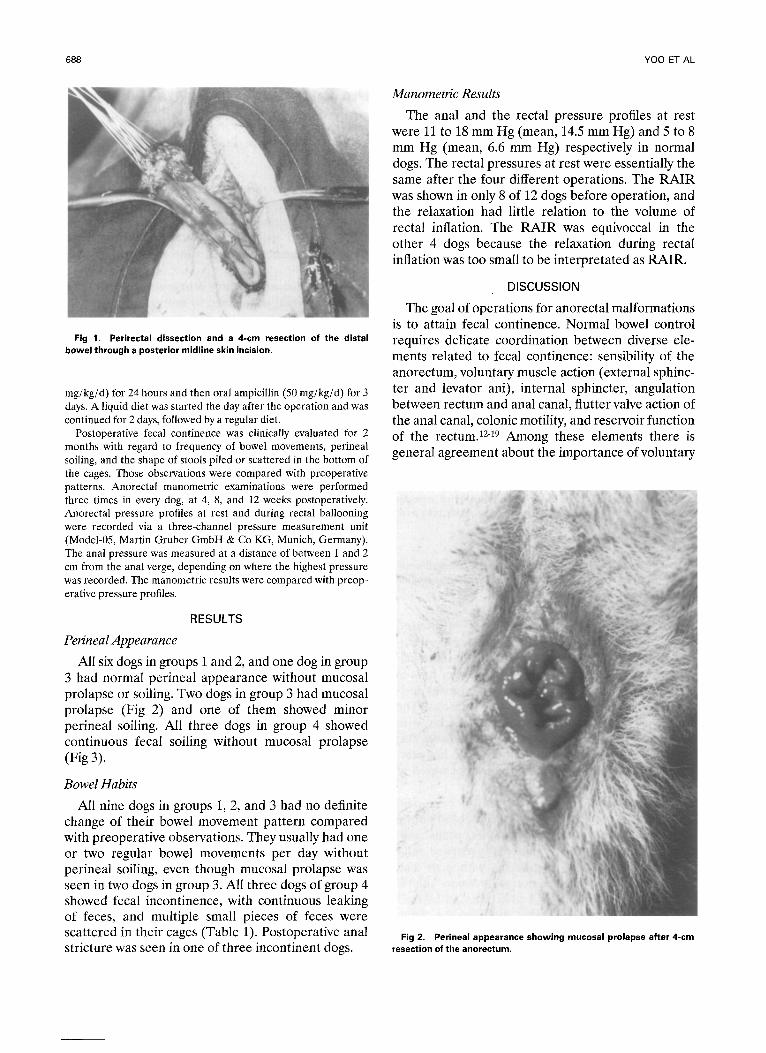
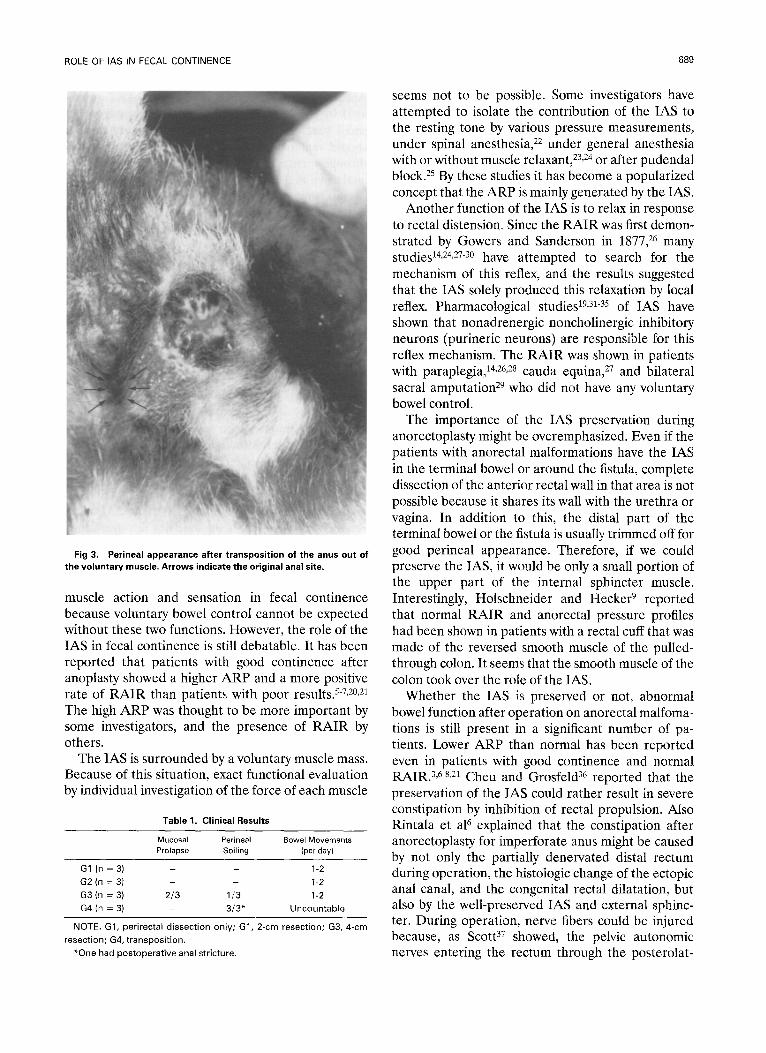
All six dogs in groups 1 and 2, and one dog in group 3 had normal perineal appearance without mucosal prolapse or soiling. Two dogs in group 3 had mucosal prolapse (Fig 2) and one of them showed minor perineal soiling. All three dogs in group 4 showed continuous fecal soiling without mucosal prolapse (Fig 3).
Bowel Habits
All nine dogs in groups 1, 2, and 3 had no definite change of their bowel movement pattern compared with preoperative observations. They usually had one ' or two regular bowel movements per day without perineal soiling, even though mucosal prolapse was seen in two dogs in group 3. All three dogs of group 4 showed fecal incontinence, with continuous leaking of feces, and multiple small pieces of feces were scattered in their cages (Table 1). Postoperative anal stricture was seen in one of three incontinent dogs.
Manometric Results
The anal and the rectal pressure profiles at rest were 11 to 18 mm Hg (mean, 14.5 mm Hg) and 5 to 8 mm Hg (mean, 6.6 mm Hg) respectively in normal dogs. The rectal pressures at rest were essentially the same after the four different operations. The RAIR was shown in only 8 of 12 dogs before operation, and the relaxation had little relation to the volume of rectal inflation. The RAIR was equivoccal in the other 4 dogs because the relaxation during rectal inflation was too small to be interpretated as RAIR.
DISCUSSION
The goal of operations for anorectal malformations is to attain fecal continence. Normal bowel control requires delicate coordination between diverse ele- ments related to fecal continence: sensibility of the anorectum, voluntary muscle action (external sphinc- ter and levator ani), internal sphincter, angulation between rectum and anal canal, flutter valve action of the anal canal, colonic motility, and reservoir function of the rectum. 12-19 Among these elements there is general agreement about the importance of voluntary
Fig 2. Perineal appearance showing mucosal prolapse after 4-¢m resection of the anorectum.
ROLE OF IAS IN FECAL CONTINENCE 689
Fig 3. Perineal appearance after transposition of the anus out of the voluntary muscle. Arrows indicate the original anal site.
muscle action and sensation in fecal continence because voluntary bowel control cannot be expected without these two functions. However, the role of the IAS in fecal continence is still debatable. It has been reported that patients with good continence after anoplasty showed a higher ARP and a more positive rate of RAIR than patients with poor results. 5-7,2°,21 The high ARP was thought to be more important by some investigators, and the presence of RAIR by others.
The IAS is surrounded by a voluntary muscle mass. Because of this situation, exact functional evaluation by individual investigation of the force of each muscle
Table 1. Clinical Results
Mucosal Perineal Bowel Movements Prolapse Soiling (per day)
G1 (n = 3) - - 1-2
G2 (n = 3) - - 1-2
G3 (n = 3) 2 /3 1/3 1-2
G4 (n = 3) - 3 /3* Uncountable
NOTE. G1, perirectal dissection only; G1, 2-cm resection; G3, 4-cm
resection; G4, transposit ion.
*One had postoperat ive anal stricture.
seems not to be possible. Some investigators have attempted to isolate the contribution of the IAS to the resting tone by various pressure measurements, under spinal anesthesia, 22 under general anesthesia with or without muscle relaxant, 23,24 or after pudendal block. 25 By these studies it has become a popularized concept that the ARP is mainly generated by the IAS.
Another function of the IAS is to relax in response to rectal distension. Since the RAIR was first demon- strated by Gowers and Sanderson in 1877, 26 many studies 14,24,27-3° have attempted to search for the mechanism of this reflex, and the results suggested that the IAS solely produced this relaxation by local reflex. Pharmacological studies 19,31-35 of IAS have shown that nonadrenergic noncholinergic inhibitory neurons (purineric neurons) are responsible for this reflex mechanism. The RAIR was shown in patients with paraplegia, 14,26,28 cauda equina, ~7 and bilateral sacral amputation 29 who did not have any voluntary bowel control.
The importance of the IAS preservation during anorectoplasty might be overemphasized. Even if the patients with anorectal malformations have the IAS in the terminal bowel or around the fistula, complete dissection of the anterior rectal wall in that area is not possible because it shares its wall with the urethra or vagina. In addition to this, the distal part of the terminal bowel or the fistula is usually trimmed off for good perineal appearance. Therefore, if we could preserve the IAS, it would be only a small portion of the upper part of the internal sphincter muscle. Interestingly, Holschneider and Hecker 9 reported that normal RAIR and anorectal pressure profiles had been shown in patients with a rectal cuff that was made of the reversed smooth muscle of the pulled- through colon. It seems that the smooth muscle of the colon took over the role of the IAS.
Whether the IAS is preserved or not, abnormal bowel function after operation on anorectal malfoma- tions is still present in a significant number of pa- tients. Lower ARP than normal has been reported even in patients with good continence and normal RAIR. 3,6-8,21 Cheu and Grosfeld 36 reported that the preservation of the IAS could rather result in severe constipation by inhibition of rectal propulsion. Also Rintala et al 6 explained that the constipation after anorectoplasty for imperforate anus might be caused by not only the partially denervated distal rectum during operation, the histologic change of the ectopic anal canal, and the congenital rectal dilatation, but also by the well-preserved IAS and external sphinc- ter. During operation, nerve fibers could be injured because, as Scott 37 showed, the pelvic autonomic nerves entering the rectum through the posterolat-

690 YO0 ET AL
eral surface in cases of high imperforate anus are easily vulnerable while the rectum is being pulled through to the perineum. In addition, Li et a138,39
found that the number, size, and density of sensory nerve endings are reduced, and that the number of motoneurons in the sacrum also significantly de- creased in patients with anorectal malformations.
We produced two kinds of animal models, one with absence of the IAS because of resection of the anal canal, and another with absence of surrounding voluntary muscle because of reconstruction of the anorectum out of the voluntary muscle. The first model was subdivided into two groups by length of the anal canal resected to assure the complete elimi- nation of the IAS zone. The second model was provided to show the contribution of the IAS to the ARP with absence of voluntary muscle mass. Al- though Pefia et al 4° reported that perirectal dissection up to the supralevator space resulted in mucosal prolapse, fecal soiling, and reduction of ARP, our animals with prolapse had regular bowel movements.
It was impossible to check the bowel movements of all animals every time. We evaluated the fecal conti- nence with perineal soiling, the pattern of scattered feces, and number of fecal piles. Our result suggests that the IAS is not a decisive factor in fecal conti- nence because all animals without IAS maintained their continence clinically. Manometrical examina- tions supported the clinical results. The interesting finding was the minimal change of the anal resting tone in all dogs with a resection of the anal canal.
According to the previous studies, the ARP gener- ated by the IAS should be diminished and only a small part of the pressure from voluntary muscle should remain. Our study showed that the pulled- through rectum compensated for the function of the anal canal in the resting tone and in fecal continence.
Unfortunately, the RAIR cannot be compared in this study because the reflex was not clearly shown even in some normal dogs who did not have an operation. The others showed the RAIR, but the depression was less pronounced. The length of the anal canal was just 6 to 10 mm in resected cases, and the length of the IAS zone may have been too short to routinely present the RAIR. It is uncertain whether the general anesthesia with intravenous pentobarbi- tal depressed the RAIR; however, large doses of pentobarbital can depress the transmission in auto- nomic ganglia and reduce the nicotinic excitation by c h o l i n e esters . 41,42
This study attempted to prove the function of the IAS, which could not be solely isolated in vivo, in fecal continence. Although the number of animals studied was small, our results suggest that the IAS may not be a fundamental element in fecal conti- nence because the animals without the IAS were continent with regular bowel movements. Also the reduction of the anal resting tone was not significant. On the other hand, all the animals with anorectum malpositioned out of the voluntary muscle showed fecal soiling. This finding suggests the importance of voluntary muscle in fecal continence.
REFERENCES
1. Pefia A, Devries PA: Posterior sagittal anorectoplasty: Impor- tant technical considerations and new applications. J Pediatr Surg 17:796-811, 1982
2. Rintala R, Lindahl H, Sariola H, et al: The rectourogenital connection in anoreetal malformations is an ectopic anal canal. J Pediatr Surg 25:665-668, 1990
3. Rintala R, Lindahl H, Louhimo I: Anorectal malformations-- Results of treatment and long term follow-up in 208 patients. Pediatr Surg Int 6:36-41, 1991
4. Frenckner B, Husberg B: Internal anal sphincter function after correction of imperforate anus. Pediatr Surg Int 6:202-206, 1991
5. Husberg B, Lindahl H, Rintala R, et al: High and intermedi- ate imperforate anus after surgical correction with special respect to internal sphincter function. J Pediatr Surg 27:185-189, 1992
6. Rintala R, Lindahl H, Marttinen E, et al: Constipation is a major functional complication after internal sphincter-saving poste- rior sagittal anorectoplasty for high and intermediate anorectal malformations. J Pediatr Surg 28:1054-1058, 1993
7. Scharli AF, Kiesewetter WB: Imperforate anus: Anorectosig- mold pressure studies as a quantitative evaluation of postoperative continence. J Pediatr Surg 4:694-704, 1969
8. Taylor I, Duthie HL, Zachary RB: Anal continence following surgery for imperforate anus. J Pediatr Surg 8:497-503, 1973
9. Holschneider AM, Hecker WC: Reverse smooth muscle plasty: A new method treating anorectal incontinence in infants with high anal and rectal atresia. J Pediatr Surg 16:917-920, 1981
10. Penninckx F, Kerremans R: Internal sphincter-saving in imperforate anus with or without fistula: A manometric study. Int J Colorect Dis 1:28-32, 1986
11. Lembrecht W, Lierse W: The internal sphincter in anorectal malformations: Morphologic investigations in neonatal pigs. J Pediatr Surg 22:1160-1168, 1987
12. Gaston EA: The physiology of fecal continence. Surg Gyne- col Obstet 87:280-290, 1948
13. Gaston EA: Fecal continence following resections of various portions of the rectum with preservation of the anal sphincters. Surg Gynecol Obstet 87:669-678, 1948
14. Gaston EA: Physiological basis for preservation of fecal continence after resection of rectum. J A M A 146:1486-1489, 1951
15. Phillips SF, Edwards DAW: Some aspects of anal conti- nence and defaecation. Gut 6:396-406, 1965
16. Duthie HL: Dynamics of the rectum and anus. Clin Gastro- enterol 4:467-477, 1975
17. Goligher J: Surgical anatomy and physiology of the anus,

ROLE OF IAS IN FECAL CONTINENCE 691
rectum and colon, in Goligher J (ed): Surgery of the anus, rectum and colon (ed 5). London, Bailliere Tindall, 1984, pp 1-47 chap 1
18. Scharli AF: Anorectal incontinence: Diagnosis and treat- ment. J Pediatr Surg 22:693-701, 1987
19. Holschneider AM, Freeman NV: Anatomy and function of the normal rectum and anus. Birth Defects 24:125-154, 1988
20. Lubowski DZ, Nicholls RJ, Burleigh DE, et al: Internal anal sphincter in neurogenic fecal incontinence. Gastroenterology 95: 997-1002, 1988
21. Hedlund H, Pefia A, Rodriquez G, Maza Je t al: Long-term anorectal function in imperforate anus treated by a posterior sagittal anorectoplasty: Manometric investigation. J Pediatr Surg 27:906-909, 1992
22. Frenckner B, Ihre T: Influence of autonomic nerves on the internal anal sphincter in man. Gut 17:306-312, 1976
23. Schweiger M: Method for determining individual contribu- tions of voluntary and involuntary anal sphincters to resting tone. Dis Colon Rectum 22:415-416, 1979
24. Duthie HL, Watt JM: Contribution of the external anal sphincter to the pressure zone in the anal canal. Gut 6:64-68, 1965
25. Frenckner B, Euler CV: Influence of pudendal block on the function of the anal sphincter. Gut 16:482-489, 1975
26. Gowers WR, Sanderson JSB: The automatic action of the sphincter ani. Proc R Soc London Biol Sci 29:77-74, 1877
27. Denny-Brown D, Robertson EG: An investigation of the nervous control of defecation. Brain 58:256-310, 1935
28. Schuster MM, Hedrix TR, Mendeloff AL: The internal sphincter response: Manometric studies on its normal physiology, neural pathways, and alteration in bowel disorders. J Clin Invest 42:196-207, 1963
29. Gunterberg B, Kewenter J, Petersen I, et al: Anorectal function after major resection of the sacrum with bilateral or unilateral sacrifice of sacral nerves. Br J Snrg 63:546-554, 1976
30. Lubowski DZ, Nicholls R J, Swash M, et al: Neural control of internal anal sphincter function. Br J Surg 74:668-670, 1987
31. Nissan S, Vinograd Y, Hadari A, et al: Physiological and pharmacological studies of internal anal sphincter in the rat. J Pediatr Surg 19:12-14, 1984
32. Burleigh DE, D'Mello A, Park AG: Responses of isolated human internal anal sphincter to drugs and electrical field stimula- tion. Gastroenterology 77:484-490, 1979
33. Yamato S, Rattan S: Role of alpha adrenoceptors in opossum internal anal sphincter. J Clin Invest 86:424-429, 1990
34. Speakman CrM, Hoyle CHV, Kamm MA, et al: Adrenergic control of the internal anal sphincter is abnormal in patients with idiopathic faecal incontinence. Br J Surg 77:1342-1344, 1990
35. Nurko S, Rattan S: Role of neuropeptide Y in opossum internal anal sphincter. Am J Physiol 21:59-64, 1990
36. Cheu HW, Grosfeld JL: The atonic baggy rectum: A cause of intractable obstipation after imperforate anus repair. J Pediatr Surg 27:1071-1074, 1992
37. Scott JES: The anatomy of the pelvic autonomic nervous system in cases of high imperforate anus. Surgery 45:1013-1028, 1959
38. Li L, Li Z, Hou HS, et al: Sensory nerve endings in pubo- rectalis and anal region: Normal findings in the newborn and changes in anorectal anomalies. J Pediatr Surg 25:658-664, 1990
39. Li L, Li Z, Wang LY, et al: Anorectal anomaly: Neuropatho- logical change in the sacral spinal cord. J Pediatr Surg 28:880-885, 1993
40. Pefia A, Amroch D, Baeza C, et al: The effects of the posterior sagittal approach on rectal function (experimental study). J Pediatr Surg 28:773-778 , 1993
41. Frenckner B, Molander ML: Influence of general anesthesia on ano-rectal manometry in healthy children. Acta Paediatr Scand 68:97-101, 1979
42. Rall TW: Hypnotics and sedatives: Ethanol, in Gilman AG, Rall TW, Nies AS, et al (eds): The pharmacological basis of therapeutics (ed 8). Singapore, Pergamon Press, 1991, pp 345-382 (chap 17)