Hospital Acquired Pneumonia(HAP): is defined as a pneumonia which occurs after 48 hours of admission...
22
-
Upload
archibald-young -
Category
Documents
-
view
222 -
download
1
Transcript of Hospital Acquired Pneumonia(HAP): is defined as a pneumonia which occurs after 48 hours of admission...
• Hospital Acquired Pneumonia(HAP): is defined as a pneumonia which occurs after
48 hours of admission to hospital .
• Hospital Acquired Pneumonia(HAP): is defined as a pneumonia which occurs after
48 hours of admission to hospital .
• Ventilator-associated Pneumonia (VAP): is defined as pneumonia occurring 48 to 72
hours after intubation.
• Ventilator-associated Pneumonia (VAP): is defined as pneumonia occurring 48 to 72
hours after intubation.• HCAP occurs in patients from the community who
reside in long-term care facilities or nursing homes; visit hemodialysis clinics or hospitals; were hospitalized for ≥2 days within the last 90 days; or received intravenous (IV) antibiotic therapy, chemotherapy, or wound care within the past 30 days.
• HCAP occurs in patients from the community who reside in long-term care facilities or nursing homes; visit hemodialysis clinics or hospitals; were hospitalized for ≥2 days within the last 90 days; or received intravenous (IV) antibiotic therapy, chemotherapy, or wound care within the past 30 days.

Classification of HAPEarly-onset Late-onset Occurs during the first 4 days
More than 4 days
•S. Pneumoniae•MSSA (methicillin-sensitive S aureus) •H. Influenza •anaerobes.
•G(-) organisms, esp. P.aeruginosa, •Acinetobacter•Enterobacteriaceae (klebsiella, Enterobacter, Serratia) •MRSA.
Monotherapy Combination therapy
Classification of VAP
Early-onset Late-onset
within 48-72 hours after tracheal intubation, which complicates the intubation process
after 72 hours
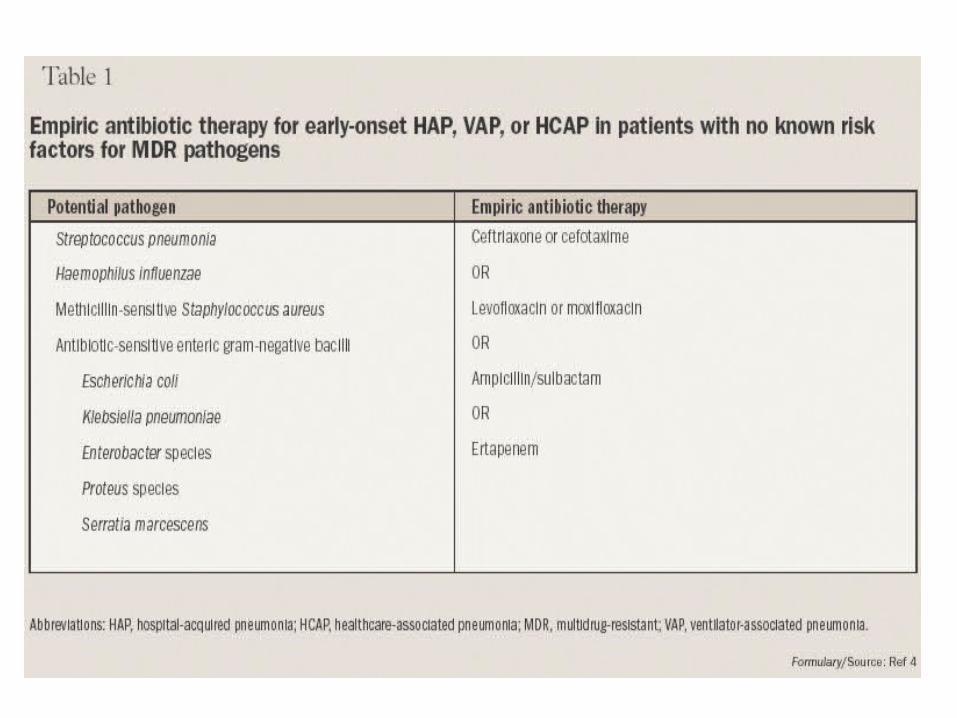
Most initial therapy is empiric because no pathogen is identified or results are not available when antimicrobial decisions are made in most patients.
Most initial therapy is empiric because no pathogen is identified or results are not available when antimicrobial decisions are made in most patients.
Treatment
Initially be treated with a broad-spectrum antibiotic regimen aimed at covering all likely bacterial pathogen
This regimen should subsequently be narrowed, according to the result of culture (de-escalate)
The mortality can be reduced with early appropriate empiric therapy.(Form 30 % with appropriate therapy to more than 90 % with inappropriate therapy)
Inappropriate initial antibiotic therapy was associated with:
1. Higher crude hospital mortality (60.7 vs. 47.3%) 2. Longer ICU stay in survivors (20 vs. 12 days) 3. Longer duration of mechanical ventilator
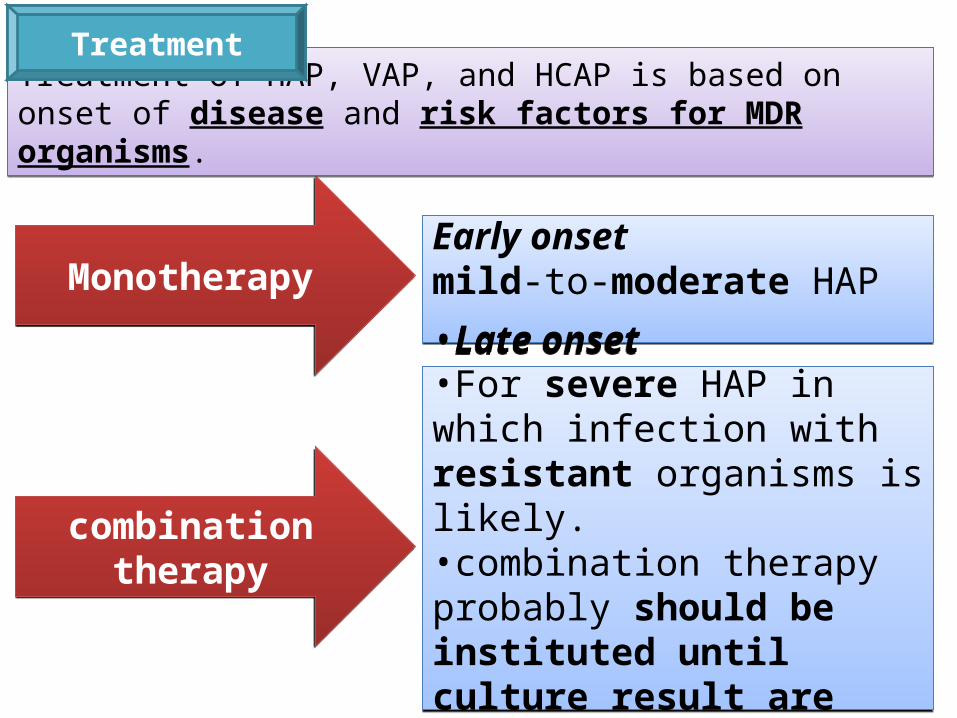
MonotherapyMonotherapy
combination therapycombination therapy
Early onsetmild-to-moderate HAPEarly onsetmild-to-moderate HAP
•Late onset•For severe HAP in which infection with resistant organisms is likely.•combination therapy probably should be instituted until culture result are available.
•Late onset•For severe HAP in which infection with resistant organisms is likely.•combination therapy probably should be instituted until culture result are available.
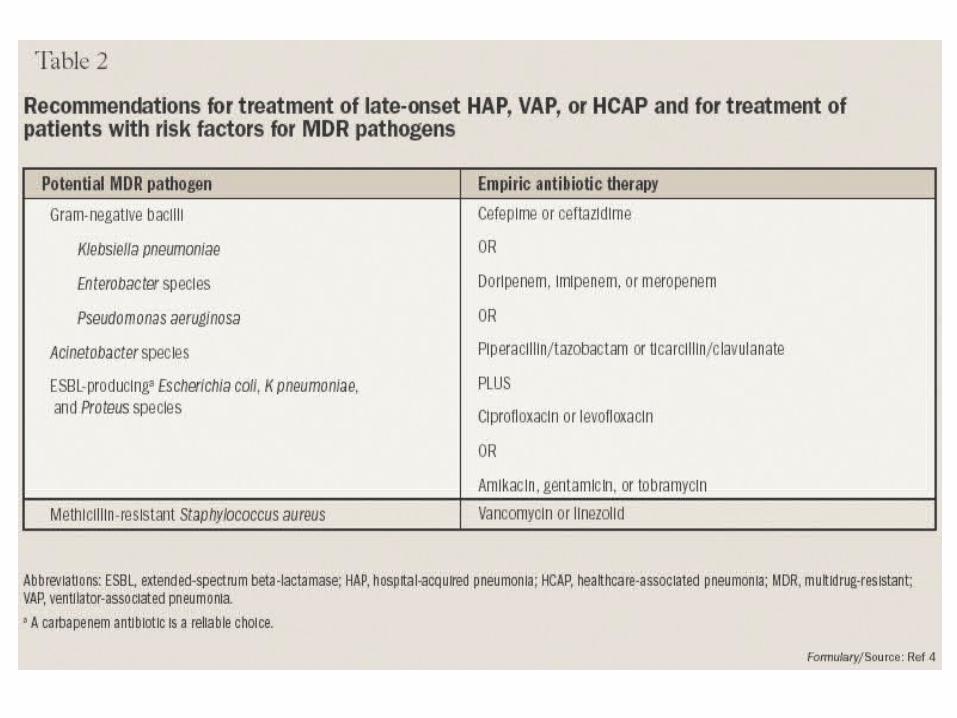
Treatment of HAP, VAP, and HCAP is based on onset of disease and risk factors for MDR organisms.Treatment of HAP, VAP, and HCAP is based on onset of disease and risk factors for MDR organisms.
Treatment
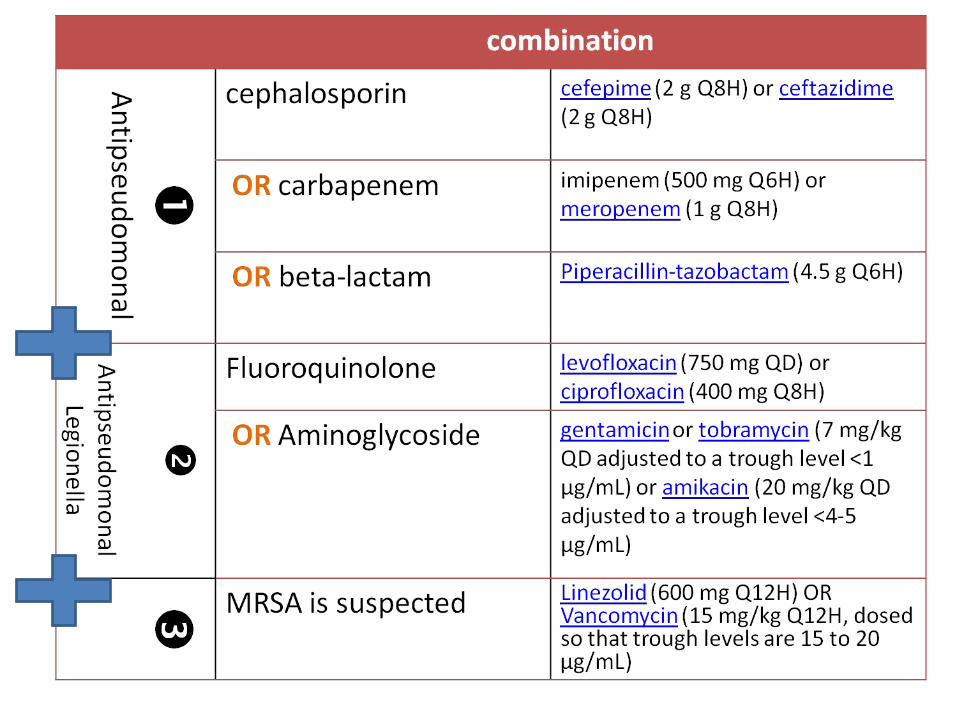
Treatment• Combination of antipseudomonal drugs is
controversial:1. Traditional: antipseudomonal beta-lactam + an Aminoglycoside.
Synergy but potential nephrotoxicity.2. Another approach: antipseudomonal beta-lactam + a Fluoroquinolone. No benefit of synergy but nephrotoxicity, and
quinolone gets into the lungs at higher concentrations.
Treatment• Patients for S. aureus infection, agents against this
organism are necessary, including Vancomycin if MRSA is suspected.
• Linezolid is comparable with Vancomycin. The advantage of Linezolid is less possible
nephrotoxicity ---- current opinion in infectious disease 2002, 15:387-94, copyright LWW
Treatment• Results:
1. Some pathogens, such as H. influenzae, cure rate is high, and 7 to 10 days is adequate.
2. Highly resistant G(-) organisms (Acinetobacter or
pseudomonas) require prolonged combination therapy for 21 days.
3. MRSA, requiring prolonged therapy.
Response of TherapyResponse of Therapy
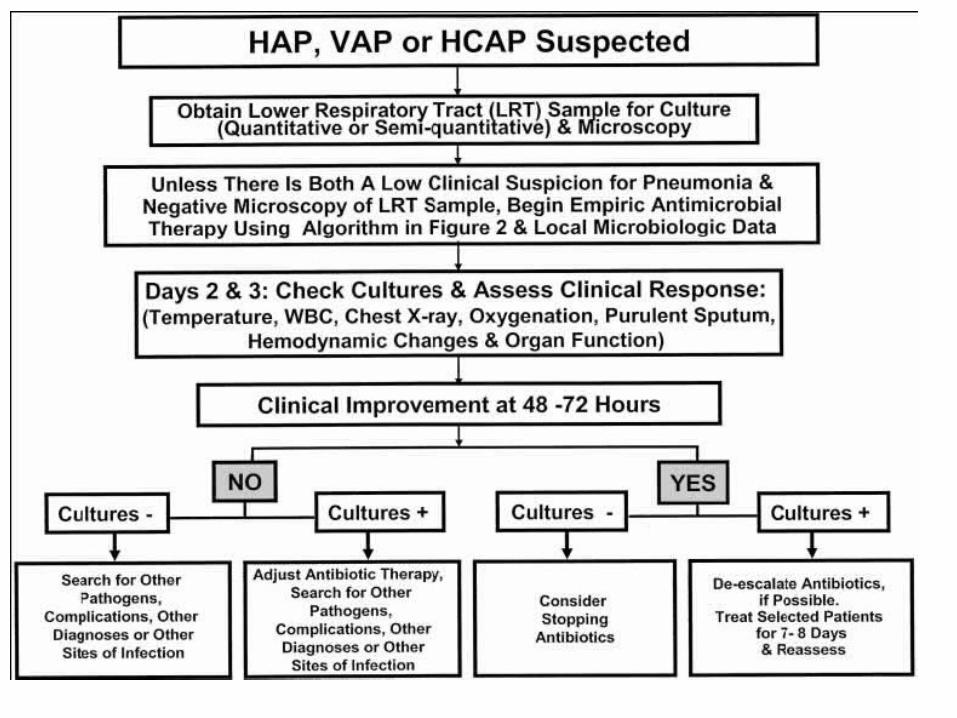
Response of Therapy• Because of the delays in clinical response of treatment, it is
thought that unless there is significant clinical deterioration or new microbiologic information, therapy should not be changed for at least the first 48 to 72 hours
• Measured by quantitating the bacterial load in the lower respiratory tract at the initiation of therapy and several days later.
Bacterial concentrations decreased or no growth -- clinical improvement Elevated -- experienced clinical failure

NEW AGENTS FOR THE
TREATMENT OF HAP
Doripenem Tigecycline
Doripenem
•Doripenem is a carbapenem antibacterial with broad in vitro activity similar to imipenem and meropenem. •It has in vitro potency against Enterobacteriaceae similar to that of ertapenem and meropenem but is 2-fold more potent in vitro than imipenem. •Doripenem has activity similar to that of meropenem against P aeruginosa but is again 2-fold more potent in vitro than imipenem. •In vitro activity against MSSA has been demonstrated to be similar to that of imipenem.
•Doripenem is a carbapenem antibacterial with broad in vitro activity similar to imipenem and meropenem. •It has in vitro potency against Enterobacteriaceae similar to that of ertapenem and meropenem but is 2-fold more potent in vitro than imipenem. •Doripenem has activity similar to that of meropenem against P aeruginosa but is again 2-fold more potent in vitro than imipenem. •In vitro activity against MSSA has been demonstrated to be similar to that of imipenem.
Tigecycline
•Tigecycline is a glycylcycline antimicrobial •a synthetic derivative of minocycline•with in vitro activity against Enterobacteriaceae and resistant gram-positive bacteria, including MRSA. •However, this agent lacks appreciable activity against P aeruginosa and Proteus species.•On May 29, 2008, FDA issued an approvable letter for tigecycline for the treatment of community-acquired pneumonia (CAP).
•Tigecycline is a glycylcycline antimicrobial •a synthetic derivative of minocycline•with in vitro activity against Enterobacteriaceae and resistant gram-positive bacteria, including MRSA. •However, this agent lacks appreciable activity against P aeruginosa and Proteus species.•On May 29, 2008, FDA issued an approvable letter for tigecycline for the treatment of community-acquired pneumonia (CAP).