Pneumonia By: Nicole Smidt & Sarah Nainggolan. Types of Pneumonia 1. Community-acquired (CAP) 2....
44
Pneumonia By: Nicole Smidt & Sarah Nainggolan
-
Upload
alicia-stevens -
Category
Documents
-
view
219 -
download
1
Transcript of Pneumonia By: Nicole Smidt & Sarah Nainggolan. Types of Pneumonia 1. Community-acquired (CAP) 2....

Pneumonia
By: Nicole Smidt & Sarah Nainggolan

Types of Pneumonia
1. Community-acquired (CAP)2. Hospital-acquired (nosocomial) (HAP)3. Ventilator-associated (VAP)

(CAP) Pathophysiology
-CAP is acquired by the body via an inhalational or aspirational route.
-Sometimes, CAP can be obtained as a secondary bacteremia from another part of the body resulting in pneumonia caused by bacteria common to other areas of the body.
-CAP tends to affect the elderly, immunocompromised, and those with underlying lung conditions (i.e. COPD, chronic bronchitis).

H&P in a (CAP) patient• History– Varying degrees of
fever with acute onset– Productive cough with
yellow/green sputum– Pleuritic chest pain– SOB
• Physical– Auscultation of rales
over the involved lobe or segment
– Increased tactile vocal fremitus, bronchial breathing, and egophony (e>a sound)
– Purulent sputum– Blood-tinged sputum– Signs of consolidation

Bacterial Pathogens of (CAP) ~85% of CAPs
• Streptococcus pneumoniae– MCC
• H. influenzae- COPD
• Moraxella catarrhalis– MC in patients with chronic bronchitis & COPD

Common Pathogens/Atypical Hosts-Staph aureus causes CAP in the setting of
postviral influenza.
-Klebsiella pneumoniae causes CAP in chronic alcoholics. Aspiration pneumonia is typically caused by multiple pathogens.
-Pseudomonas aeruginosa is a cause of CAP in patients with cystic fibrosis and bronchiectasis.

Atypical Pathogens of CAP• Zoonotic
– Chlamydia psittaci• Psittacosis• Recent close contact with
birds
– Francisella tularensis• Tularemia• Contact with deer or
rabbits or recent bite by a tick or deer fly
– Coxiella burnetii• Q fever• Contact with a cat or
sheep that has given birth recently
• Non-zoonotic (~15% of CAPs)– Legionella– Elderly, smokers,
immunocompromised
–Mycoplasma pneumoniae
– Young and healthy
– Chlamydia pneumoniae
– Young & healthy

Atypical CAP-Atypical pneumonias commonly present with dry
cough, extrapulmonary involvement, and patchy interstitial pattern on CXR.

Differential Dx of CAP
-Chronic bronchitis-Myocardial infarction-Asthma-CHF-Pulmonary edema-PE-Acute hypersensitivity reaction-Bronchogenic carcinoma

Laboratory Studies of CAP-CBC with differential showing a neutrophilia w/left shift,
electrolytes, elevated BUN/Cr, elevated glucose, abnormal LFTs
-Sputum Gram stain and/or culture (should have <10 squamous cells/lpf/purulent should have >25 PMNs/lpf)
-2-3 sets of blood cultures (before antibiotics) to detect presence of bacteria in the blood
-Serum cold agglutinin titers (Mycoplasma)
-Urinalysis
-Serological testing if zoonotic atypical pathogens are suspected

Imaging Studies of CAP-Chest x-ray
*Repeat chest x-ray within 24 hours if first x-ray shows negative findings with high clinical suspicion
-Serial chest x-rays to observe for progression or check for resolution
-Chest CT scan *If failing to respond to therapy

Community Acquired Pneumonia (CAP) Treatment
• Decision to hospitalize1. Pneumonia Severity Index (PSI)
Points given for 20 variables i.e. age, comorbid conditions, abnormal PE & lab findings
Add up the points; patients are categorized into 5 classes
Total points Risk Class % Mortality Treat as:
No predictors I 0.1 Outpatient
≤70 II 0.6 Outpatient
71-90 III 2.8 Inpatient, briefly
91-130 IV 8.2 Inpatient
>130 V 29.2 Inpatient

Decision to hospitalize, cont.
2. CURB-65 Five variables
C=Confusion U=Urea > 7mmol/L R=Respiratory rate ≥ 30 B=BP systolic ≤ 90, diastolic ≤ 60 Age ≥ 65
Add up the points, patients are categorized into 3 classes

Decision to hospitalize, cont.
• CURB-65, cont.
• PSI-less practical• CURB-65-less studies done
Total points 30-day Mortality Risk Treat as:
0 1.5% Outpatient
1-2 9.2% Inpatient
≥ 3 22% ICU

CAP Treatment
• Empiric antibiotic treatment– Outpatient treatment• Previously healthy or no antibiotics in last 3 months• Comorbidities or antibiotics in last 3 months
– Inpatient treatment• Non-ICU patients• ICU patients

CAP TreatmentOutpatient antibiotics
Guidelines per IDSA and ATS
Previously healthy/no antibiotics in last 3 months
Comorbidities/antibiotics in last 3 months
Clarithromycin 500 mg PO BID, or Levofloxacin 750 mg PO QD, or moxifloxacin 400 mg PO QD, or gemifloxacin 320 mg PO QD, OR
Azithromycin 500 mg PO once, then 250 mg PO QD, or
Amoxicillin 1g TID, or Amoxicillin/clavulanate 2g BID, or
Doxycycline 100 mg PO BID Ceftriaxone 1-2g IV QD, cefpodoxime 200 mg PO BID, cefuroxime 500 mg PO BID , plus a macrolide

CAP TreatmentInpatient Antibiotics
Inpatient, non-ICU Inpatient, ICU
Levofloxacin 750 mg PO or IV QD, or moxifloxacin 400 mg PO or IV QD, or gemifloxacin 320 mg PO QD
Cefotaxime 1–2 g IV q8h, or ceftriaxone 2 g IV QD, or ampicillin-sulbactam 2 g IV q8h plus azithromycin or a fluoroquinolone *
*PCN-allergic: use resp. fluoroquinolone and aztreonam 2 g IV q8h
Cefotaxime 1–2 g IV q8h, or ceftriaxone 1–2 g IV QD, or ampicillin 1–2 g IV q4–6h, or ertapenem 1 g IV qd in selected patients plus a macrolide (oral clarithromycin or azithromycin; or IV azithromycin 1 g once, then 500 mg QD)**
**PCN-allergic: use resp. fluroquinolones

CAP Treatment Special Considerations
• Pseudomonas– piperacillin/tazobactam 4.5 g IV q6h, cefepime 1–2 g IV
q12h, imipenem 500 mg IV q6h, meropenem 1 g IV q8h plus either ciprofloxacin 400 mg IV q12h or levofloxacin 750 mg IV, or
– piperacillin/tazobactam 4.5 g IV q6h plus amikacin 15 mg/kg qd or tobramycin 1.7 mg/kg qd and azithromycin, or
– piperacillin/tazobactam 4.5 g IV q6h plus an aminoglycoside plus an antipneumococcal fluoroquinolone
– If PCN-allergic: substitute aztreonam

CAP TreatmentSpecial Considerations
• Community-Acquired MRSA– Add linezolid 600 mg IV q12h or vancomycin 1 g IV
q12h

CAP Treatment
• Most patients admitted to the hospital for CAP receive IV antibiotics
• A switch to oral drugs is appropriate, so long as the patient can ingest and absorb the drugs, is hemodynamically stable, and showing clinical improvement
• Duration: Patients are usually treated for 10-14 days, but recent studies with fluoroquinolones suggest that a 5-day course is sufficient for uncomplicated CAP.

CAPFollow-up
• Fever usually resolves within 2 days, while leukocytosis may improve within 4 days
• Abnormalities in CXR take 4-12 weeks to clear, depending on the age of the patient and the underlying lung disease
• Follow-up CXR can be done 4-6 weeks later • If recurrence is seen in the same lung segment,
possible neoplasm should be taken into consideration

CAPPrognosis
• Depends on age, comorbidities, inpatient/outpatient• Young patients without comorbidities fully recover in
2 weeks • Older patients with comorbidities take longer• Overall mortality rates– Outpatient: < 1%– Inpatient: 10%, with about 50% of the deaths directly
attributable to pneumonia

Healthcare-associated Pneumonia
1. Hospital-acquired pneumonia (HAP)
2. Ventilator-associated pneumonia (VAP)The main difference from CAP: significantly lower
incidence of atypical pathogens, EXCEPT Legionella

Hospital-acquired pneumonia (HAP)
Defined as pneumonia that occurs more than 48 hours after admission but that was NOT
incubating at the time of admission.
The American Thoracic Society further subdivides nosocomial pneumonia into early (occurring within the first 4 days of hospitalization) and late (occurring after the 5th day of admission) onset.

HAP Pathophysiology-HAP is primarily acquired though aspiration of
oropharyngeal secretions into the trachea.-Although uncommon, hematogenous spread is
also possible.-HAP is mainly caused by aerobic gram-negative
bacilli of two forms: necrotizing and nonnecrotizing.*Necrotizing cause rapid cavitation, microabscess formation, blood-vessel invasion, and hemorrhage (i.e. P. aeruginosa).

HAP
-Usually bacterial in nature.-Common in patients with mechanical
ventilation as intubation and ventilation support bypass the normal host defense mechanisms.
-One of the most common diagnoses in the medical and surgical ICUs.

H&P of HAPHistory:-SOB-Productive cough-Fever
Physical:-Rales on auscultation
over affected area-Generally NO
consolidation in nosocomial pneumonia

HAP Microbiology-P. aeruginosa-Klebsiella-E. coli
-Acinetobacter (common in ICU patients)-Staph aureus-Strep pneumoniae-H. influenzae

Dx of HAP
Laboratory:-White blood cell
count-Blood cultures
Imaging Studies:-Serial chest x-rays to
check for progression and resolution
-CT or spiral CT scan

Hospital-acquired Pneumonia (HAP)
• Main differences from VAP: – Lower incidence of MDR pathogens (allows more
monotherapy)– Better host immunity
• Anaerobes are more common• Specific therapy aimed at anaerobes is not
indicated, unless aspiration is a concern• Lower risk of antibiotic failure in comparison to VAP• Lower mortality rates than VAP

Ventilator-associated pneumonia
Defined as pneumonia that develops 48 hours or longer after mechanical ventilation is given via
endotracheal tube or tracheostomy.

VAP Pathophysiology
-VAP is caused by invasion of the lower respiratory tract and lung tissue by microorganisms caused by decreased integrity of the oropharynx and trachea allowing oral and gastric sections to enter.
-The incidence of VAP increases with the duration of ventilation.
-Pseudomonas and Acinetobacter pneumonia is associated with the greatest mortality.

Dx of VAPHistory:1. Hospitalization of greater than
5 days
2. Hospital admission of more than 2 days in the last 90 days
3. Antibiotic use in the last 90 days
4. Residing in a nursing home or skilled care facility
5. Home infusion therapy or wound care
6. Dialysis within the last 30 days
7. Immunocompromised
Diagnostic Triad:1. Fever2. Purulent secretions3. Leukocytosis

Work-up of VAP-CBC with differential to evaluate white blood cell
count-Routine blood tests to assess patient's baseline
renal and hepatic function to properly dose antibiotics
-Blood cultures-Respiratory secretion cultures-Portable chest radiography -Air bronchogram

Ventilator-associated Pneumonia (VAP)
• Empirical Antibiotic Treatment
Patients with NO risk factors for MDR pathogens
Patients with risk factors for MDR pathogens
Ceftriaxone 2 g IV q24h, or 1. Ceftazidime 2 g IV q8h or cefepime 2 g IV q8–12h, or
Moxifloxacin 400 mg IV q24h, ciprofloxacin 400 mg IV q8h, or levofloxacin 750 mg IV q24h, or
Piperacillin/tazobactam 4.5 g IV q6h, imipenem 500 mg IV q6h or 1 g IV q8h, or meropenem 1 g IV q8h, plus
Ampicillin/sulbactam 3 g IV q6h, or 2. Gentamicin or tobramycin 7 mg/kg IV q24h or amikacin 20 mg/kg IV q24h orCiprofloxacin 400 mg IV q8h or levofloxacin 750 mg IV q24h, plus
Ertapenem 1 g IV q24h 3. Linezolid 600 mg IV q12h orVancomycin 15 mg/kg, up to 1 g IV, q12h

VAP Treatment
• Duration: 8 days (associated with less frequent emergence of antibiotic-resistant strains)
• Pseudomonas aeruginosa: causes high rates of clinical failure and death, despite combo therapy
• VAP caused by MRSA: 40% clinical failure rate when treated with standard-dose vancomycin, so treat with linezolid instead.

VAPFollow-up
• Clinical improvement is usually seen within 48-72 hours following initial antibiotic therapy
• CXR worsens during initial treatment, so less helpful
• In very ill patients, follow-up CXR can be done every few days
• Once patient has improved, CXR may not be necessary for a few weeks

VAPPrognosis
• Associated with high crude mortality rates (50-70%)• Stenotrophomonas maltophilia: prognosis is very
poor (death is almost inevitable)

Question #1From USMLEWORLD
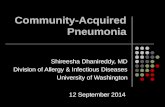
• A 65-year-old white male who has a history of COPD, CHF, and CAD presented with a three-day history of worsening SOB, cough with yellowish expectoration, and fever. He is not on steroids and does not use oxygen at home. He takes ipratropium, albuterol, aspirin, digoxin, furosemide, metoprolol, and lisinopril. He lives at home with his wife. His temp is 103 F, BP is 110/70, pulse is 110, and respirations are 24. He is saturating 88% on room air. He was started on 3-liters of oxygen to keep the saturations above 92%. The CXR of the patient is shown below. What is the most appropriate next step in the management of this patient?
A. Admit the patient and give ampicillin
B. Outpatient trimethoprim-sulfamethoxazole
C. Admit the patient and start levofloxacin
D. Admit the patient and start ciprofloxacin
E. Admit the patient and start vancomycin
F. Outpatient clindamycin therapy

Question #1CXR

Answer #1• C. Admit the patient and start levofloxacin
– The clinical presentation and CXR of this patient is highly suggestive of CAP. The first step in the management of CAP is to decide whether the patient needs hospitalization. The decision to admit the patient is generally made using the Pneumonia Severity Index (PSI) based on medical history, PE, and lab and radiographic findings. This patient has other comorbidities such as CHF, COPD, and CAD, and his oxygen saturation is less than 90%. Thus he falls under risk class III or IV and needs to be hospitalized.
– The most common cause of lobar pneumonia in this setting is pneumococcus. The new generation flouroquinolones (i.e. levofloxacin) is used for the inpatient treatment of CAP. About 97% of the Streptococcus pneumonia are sensitive to these drugs. They also cover the atypical organisms.
– For the management of outpatient therapy in stable patients with no comorbidities, either azithromycin or doxycycline can be used.

Question #2A 68-year-old woman with polymyositis is evaluated in the office because of increased difficulty swallowing and a 2-week history of low-grade fever, intermittent cough, and sputum production.
On physical examination, temperature is 37.9 °C (100.2 °F), and crackles are heard at the base of the right lung posteriorly. The leukocyte count is 9700/μL with 85% neutrophils, 12% lymphocytes, 2% monocytes, and 1% eosinophils.
A chest radiograph shows patchy pulmonary infiltrates in the right lower lobe. Sputum Gram stain shows many neutrophils, a few squamous epithelial cells, and several morphologic types of both gram-negative rods and gram-positive cocci. Results of sputum culture are pending.
Which of the following is the most appropriate management at this time?
A. Bronchoscopy
B. Clindamycin
C. Metronidazole
D. Penicillin

Answer #2B. This patient should be started on clindamycin. The presence of underlying polymyositis and difficulty swallowing place this patient at risk for aspiration and the development of aspiration pneumonia. Other risk factors for aspiration pneumonia include episodes of depressed consciousness (e.g., patients with alcoholism) or mechanical factors that increase the likelihood of secretions entering the tracheobronchial tree (e.g., patients with esophageal obstruction). Although aspiration of acidic gastric contents can result in a chemical pneumonitis, aspiration of oral secretions typically results in an anaerobic pneumonia caused by anaerobic organisms that are normally present in the mouth. A sputum Gram stain often shows both gram-positive and gram-negative organisms of different morphologic types, as was found in this patient. The typical location of aspiration pneumonia depends upon the patient's position at the time of aspiration. Based on gravitational flow of airway secretions, the pneumonia is preferentially localized in the dependent regions of the lung at the time of aspiration. In an upright patient, the lower lobes are usually affected, more so on the right than on the left. In a supine patient, common sites of aspiration pneumonia are the posterior segment of the right upper lobe and the superior segment of the right lower lobe.
Although options for antibiotic coverage of anaerobic aspiration pneumonia have generally included either penicillin or clindamycin, controlled studies have shown that antibiotic failure rates have been higher for penicillin than for clindamycin. Metronidazole does not adequately cover microaerophilic and aerobic streptococci from the mouth, which are contributing organisms in many patients with aspiration pneumonia. Bronchoscopy is not indicated because it is unable to confirm anaerobic infection, since anaerobic organisms from the mouth will contaminate the specimens obtained.

References• Mandell LA, Wunderick R, et al. Harrison’s Principles
of Internal Medicine, 17th ed. 2008. • Chesnutt MS, Gifford AH, Prendergast TJ. Current
Medical Diagnosis & Treatment 2010. • Agabegi SS, Agabegi ED. Step-Up to Medicine, 2nd
ed. 2008. • Fischer C, Reichert S. USMLE Master the Boards.
2009. • Burke A Cunha, MD. Emedicine.medscape.com.
2010.