Hoschander raua reat 215 4:2 14172216712221244 Jo Journal of … · 2018-04-17 · facial...
3
Volume 4 • Issue 2 • 1000244 J Trauma Treat ISSN: 2167-1222 JTM, an open access journal Research Article Open Access Hoschander, J Trauma Treat 2015, 4:2 DOI: 10.4172/2167-1222.1000244 Case Report Open Access ISSN: 2167-1222 Repair of a Facial Zygomaticomaxillary Complex Fracture Mordechai Hoschander* Department of Oral and Maxillofacial Surgery, NY Presbyterian Lower Manhattan Hospital, New York, NY, USA Keywords: Facial zygomaticomaxillary; Oral and maxillofacial surgery; Anesthesia; Zygo maticomaxillary complex Introduction One of the most important social cues among humans is a pleasant, balanced, unscarred facial appearance. Given that few societies accept or desire facial covering, facial trauma resulting in altered facial architecture, sensation, and movement that cannot be easily disguised can be emotionally devastating. Patients such as these are among those who spend many millions, indeed billions, of dollars each year on surgeries on eyes, ears, nose, lips, cheekbones, necks, jaws, chins, etc., in hopes of achieving a more perfect image. For the surgeon, it is no small challenge to recreate a face aſter it has been disfigured or disrupted. Multiple variables-including vision, anatomical norms, sensory pathways, tissue tolerance, healing capacity, and infection control-must be considered upon entering an operating room to repair facial trauma. It is also important to remember that some bells cannot be “unrung”-ie, even the best possible outcome under the circumstance may not be “good enough” in the eyes of the patient. e author makes a practice of photographing patients while they are still swollen, bleeding, and oſten while they are still open prior to laceration repair, to enable them to postoperatively recognize how far they have come from their starting point. It is important to thus recreate a new baseline for such patients, because, despite the best efforts of surgeons, they may never again appear as they did prior to being injured. In fact, some patients actually expect improvement from their previous baseline. is is not only unrealistic, but expectations of improvement beyond that achievable can lead to disappointment on the part of the patient, which can be counterproductive to both doctor and patient. Patient Report A 33-year-old white male was injured when the motorcycle he was riding was hit by a car. He was initially brought to another institution, but was transferred several days post trauma to New York Presbyterian Hospital, Lower Manhattan Campus, in New York, New York, where he was treated by the author. As part of the intake workup for every patient there, it is standard practice for patients sustaining any type of facial trauma-eg, orbital or mid-face fractures-to be evaluated by Oral and Maxillofacial Surgery (OMFS), plastic surgery, and ophthalmology specialists. Computed Tomography (CT) scans must include axials, coronals, saggital, and 3-D reconstruction, where applicable. In addition, there are consultations with neurology for documented or suspected loss of consciousness, neurosurgery for skull fracture components, ENT for airway issues, medicine for complex medical problems, and general surgery for trauma sustained to other parts of the body. *Corresponding author: Mordechai Hoschander, Department of Oral and Maxillofacial Surgery, NY Presbyterian Lower Manhattan Hospital, New York, NY, USA, Tel: +1 917-374-2900; E-mail: [email protected] Received January 14, 2015; Accepted April 24, 2015; Published April 26, 2015 Citation: Hoschander M (2015) Repair of a Facial Zygomaticomaxillary Complex Fracture. J Trauma Treat 4: 244. doi:10.4172/2167-1222.1000244 Copyright: © 2015 Hoschander M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. As can be seen in the pre-operative facial photographs (Figures 1A-1E) and CT scans (Figure 2A-2E), this patient sustained a compound comminuted ZMC fracture, with marked anterior maxillary comminution.Most who deal with facial trauma are familiar with Zygo Maticomaxillary Complex (ZMC), or tripod, fractures. ese can be challenging because there can be unintended complications, such as enophthalmos, ectropion, diplopia, paraesthesia, anesthesia, oral antral fistula, malocclusion, mal-union, facial asymmetry, facial paralysis, and a whole host of untoward, unwanted, and very troublesome postoperative complications. Some are relatively easy to repair; others are less so. Nearly all cause some degree of anxiety. e surgical approach in this case involved a lateral brow incision, subcillary incision, and a wide oral mucobuccal fold incision (Figures 3A-3C). Using a combination of plates, screws, and Porex® sheeting to Abstract Repair of facial trauma such as that sustained during a high-speed motor vehicle accident, as described in this patient report, can be functionally and esthetically challenging. Here, successful postsurgical management of wound breakdown following a zygomaticomaxillary complex fracture repair included use of a self-adhesive hydrogel wound dressing. 1A 1B 1C 1D 1E Figure 1: Clinical photographs taken upon patient presentation showing the extent of facial injuries sustained in a motorcycle accident. Journal of Trauma & Treatment J o u r n a l o f T r a u a m & T r e a t m e n t ISSN: 2167-1222
Transcript of Hoschander raua reat 215 4:2 14172216712221244 Jo Journal of … · 2018-04-17 · facial...

Volume 4 • Issue 2 • 1000244J Trauma TreatISSN: 2167-1222 JTM, an open access journal
Research Article Open Access
Hoschander, J Trauma Treat 2015, 4:2 DOI: 10.4172/2167-1222.1000244
Case Report Open Access
ISSN: 2167-1222
Repair of a Facial Zygomaticomaxillary Complex FractureMordechai Hoschander*
Department of Oral and Maxillofacial Surgery, NY Presbyterian Lower Manhattan Hospital, New York, NY, USA
Keywords: Facial zygomaticomaxillary; Oral and maxillofacialsurgery; Anesthesia; Zygo maticomaxillary complex
IntroductionOne of the most important social cues among humans is a pleasant,
balanced, unscarred facial appearance. Given that few societies accept or desire facial covering, facial trauma resulting in altered facial architecture, sensation, and movement that cannot be easily disguised can be emotionally devastating. Patients such as these are among those who spend many millions, indeed billions, of dollars each year on surgeries on eyes, ears, nose, lips, cheekbones, necks, jaws, chins, etc., in hopes of achieving a more perfect image. For the surgeon, it is no small challenge to recreate a face after it has been disfigured or disrupted. Multiple variables-including vision, anatomical norms, sensory pathways, tissue tolerance, healing capacity, and infection control-must be considered upon entering an operating room to repair facial trauma. It is also important to remember that some bells cannot be “unrung”-ie, even the best possible outcome under the circumstance may not be “good enough” in the eyes of the patient.
The author makes a practice of photographing patients while they are still swollen, bleeding, and often while they are still open prior to laceration repair, to enable them to postoperatively recognize how far they have come from their starting point. It is important to thus recreate a new baseline for such patients, because, despite the best efforts of surgeons, they may never again appear as they did prior to being injured. In fact, some patients actually expect improvement from their previous baseline. This is not only unrealistic, but expectations of improvement beyond that achievable can lead to disappointment on the part of the patient, which can be counterproductive to both doctor and patient.
Patient ReportA 33-year-old white male was injured when the motorcycle he was
riding was hit by a car. He was initially brought to another institution, but was transferred several days post trauma to New York Presbyterian Hospital, Lower Manhattan Campus, in New York, New York, where he was treated by the author. As part of the intake workup for every patient there, it is standard practice for patients sustaining any type of facial trauma-eg, orbital or mid-face fractures-to be evaluated by Oral and Maxillofacial Surgery (OMFS), plastic surgery, and ophthalmology specialists. Computed Tomography (CT) scans must include axials, coronals, saggital, and 3-D reconstruction, where applicable. In addition, there are consultations with neurology for documented or suspected loss of consciousness, neurosurgery for skull fracture components, ENT for airway issues, medicine for complex medical problems, and general surgery for trauma sustained to other parts of the body.
*Corresponding author: Mordechai Hoschander, Department of Oral andMaxillofacial Surgery, NY Presbyterian Lower Manhattan Hospital, New York, NY, USA, Tel: +1 917-374-2900; E-mail: [email protected]
Received January 14, 2015; Accepted April 24, 2015; Published April 26, 2015
Citation: Hoschander M (2015) Repair of a Facial Zygomaticomaxillary Complex Fracture. J Trauma Treat 4: 244. doi:10.4172/2167-1222.1000244
Copyright: © 2015 Hoschander M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
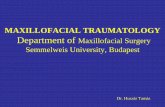
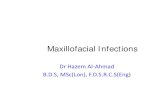
As can be seen in the pre-operative facial photographs (Figures 1A-1E) and CT scans (Figure 2A-2E), this patient sustained a compound comminuted ZMC fracture, with marked anterior maxillary comminution.Most who deal with facial trauma are familiar with Zygo Maticomaxillary Complex (ZMC), or tripod, fractures. These can be challenging because there can be unintended complications, such as enophthalmos, ectropion, diplopia, paraesthesia, anesthesia, oral antral fistula, malocclusion, mal-union, facial asymmetry, facial paralysis, and a whole host of untoward, unwanted, and very troublesome postoperative complications. Some are relatively easy to repair; others are less so. Nearly all cause some degree of anxiety.
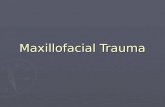
The surgical approach in this case involved a lateral brow incision, subcillary incision, and a wide oral mucobuccal fold incision (Figures 3A-3C). Using a combination of plates, screws, and Porex® sheeting to
AbstractRepair of facial trauma such as that sustained during a high-speed motor vehicle accident, as described in this
patient report, can be functionally and esthetically challenging. Here, successful postsurgical management of wound breakdown following a zygomaticomaxillary complex fracture repair included use of a self-adhesive hydrogel wound dressing.
1A 1B
1C 1D
1E
Figure 1: Clinical photographs taken upon patient presentation showing the extent of facial injuries sustained in a motorcycle accident.
Journal of Trauma & TreatmentJour
nal o
f Trau am & Treatment
ISSN: 2167-1222

Citation: Hoschander M (2015) Repair of a Facial Zygomaticomaxillary Complex Fracture. J Trauma Treat 4: 244. doi:10.4172/2167-1222.1000244
Page 2 of 3
Volume 4 • Issue 2 • 1000244J Trauma TreatISSN: 2167-1222 JTM, an open access journal
2A 2B
2C 2D
2E
Figure 2: 3-D CT scans revealed a compound comminuted ZMC fracture, with marked anterior maxillary comminution.
3A 3B
3C Figure 3: Surgical approaches including lateral brow incision, subcillary incision, and a wide oral muccobuccal fold incision.
4A 4B
4C 4D
4E 4F
4G 4H
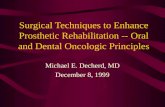
Figure 4: CT shows potential compromise of blood supply due to severe comminution of the anterior maxillary sinus wall resulting in an intraoral closure that would not be entirely over bone.
5A 5B
Figure 5: Early wound breakdown of the intra-oral suture line.

Citation: Hoschander M (2015) Repair of a Facial Zygomaticomaxillary Complex Fracture. J Trauma Treat 4: 244. doi:10.4172/2167-1222.1000244
Page 3 of 3
Volume 4 • Issue 2 • 1000244J Trauma TreatISSN: 2167-1222 JTM, an open access journal
support the almost non-existent orbital floor, the surgery succeeded in reducing and aligning the ZMC. Although the multiple comminuted fragments of the anterior wall of the maxillary sinus proved to be too small to plate, an inverted “L” plate was used to stabilize the maxilla to the ZMC buttress, leaving a rather large hole in the anterior maxilla. More importantly, it meant that the intraoral closure would not be entirely over bone, and thus the blood supply would be compromised, as shown in CT scans (Figures 4A-4H).
As wound breakdown was apparent during one of the postoperative visits, (Figures 5A and 5B) the author applied a self-adhesive hydrogel wound dressing (PerioPatch®, Izun Pharmaceuticals Corp, (Figures 6A and 6B), increased the antibiotic coverage, and followed the patient closely. PerioPatch has been shown to reduce inflammation, and enhance tissue repair. It is particularly useful in high-risk surgical procedures, as well as promoting healing in areas that are not responding well to treatment.
Several weeks later, the situation had largely resolved, leaving no exposure of the plate, oral antral fistula, fluid reflux, or infection (Figures 7A and 7B). It is likely that aggressive management of the patient averted a potential therapeutic misadventure. While complete healing has not yet occurred, the patient now appears to be on the way to a complete recovery (Figures 8A and 8B).
Discussion/ConclusionThe author believes that protecting the suture line from further
trauma and inflammatory response using the absorbent and flexible barrier was pivotal in achieving the desired result and avoiding an adverse outcome. Between the patch’s adhesion promoted by its botanical compounds and absorptive capacity, it is able to physically reduce toxic inflammatory exudate and promote healing, thus allowing for natural resolution of the inflammation, as was achieved in this case.
6A 6B
Figure 6: Self-adhesive hydogel wound dressing application followed by observation of wound.
7A 7B
Figure 7: Reduction in inflammation is apparent following aggressive management with hydogel dressing and antibiotic treatment.
8A 8B Figure 8: While healing is not yet complete, patient appears to be on track for a complete recovery.
Submit your next manuscript and get advantages of OMICSGroup submissionsUnique features:
• User friendly/feasible website-translation of your paper to 50 world’s leading languages• Audio Version of published paper• Digital articles to share and explore
Special features:
• 400 Open Access Journals• 30,000 editorial team• 21 days rapid review process• Quality and quick editorial, review and publication processing• Indexing at PubMed (partial), Scopus, EBSCO, Index Copernicus and Google Scholar etc• Sharing Option: Social Networking Enabled• Authors, Reviewers and Editors rewarded with online Scientific Credits• Better discount for your subsequent articles
Submit your manuscript at: http://www.omicsonline.org/submission