Horse Related Injuries - monash.edu · involved in 8% of injuries occurring on farms, paddocks and...
16
VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 1 Hazard (Edition No. 23) June 1995 Victorian Injury Surveillance System Monash University Accident Research Centre This edition of Hazard examines horse related injury in the VISS database, the Victorian Coroner’s Facilitation System and the Victorian Inpatient Minimum Dataset. The analysis is undertaken in two sections, with the first assessing injuries occurring during horse riding, the second, injuries sustained during other horse related activities. Prevention strategies are a major focus. The article updates and investigates in more detail horse related injuries as presented in Hazard 7, and for the first time looks at adult horse related injury Horse Related Injuries Fiona Williams Karen Ashby admissions for horse riders and 42% vs 14% of non-riders. Head injuries are responsible for the majority of serious horse riding injuries and the risk of head injury is higher in younger and less experienced riders. (Barone, 1989, Bixby- Hammett et al, 1990). The prevention of horse riding injuries requires adherence to standard horse handling safety practices and the use of protective equipment, such as approved safety helmets and approp- riately designed stirrups, shoes, tack and other protective equipment. Detailed recommendations for pre- vention are included. activities named as equestrian activities in the associated literature. The morbidity and mortality assoc- iated with horse riding activities varies greatly according to a variety of factors such as age, sex, type of activity, experience, helmet use, the type of helmet and both the age, size, character and temperament of the horse. The VISS data shows a predominance of injury to girls (10-19 years) who account for 41% of riding and 23% of the non-riding related injuries. Children’s injuries (under 15 years) were of a more serious nature than their adult counterparts accounting for 31% of children vs 22% of adult Summary Horses and horse riding provide enjoyable recreational and sporting activities, however the potential for injury is high due to the size and sometimes unpredictable nature of horses. (Sherry, 1991). Of the 1330 cases of injury involving horses on the Victorian Injury Surveillance System database 80% were to horse riders, the remainder occurred during horse handling activities or unrelated activities around horses. The latter categories will be referred to in this article as non-riding activities and activities specified as horse riding will encompass those V.I.S.S.
Transcript of Horse Related Injuries - monash.edu · involved in 8% of injuries occurring on farms, paddocks and...

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 1
Hazard(Edition No. 23)June 1995
Victorian InjurySurveillance System
Monash UniversityAccident Research Centre
This edition of Hazard examines horse related injury in the VISS database, the Victorian Coroner’s Facilitation Systemand the Victorian Inpatient Minimum Dataset. The analysis is undertaken in two sections, with the first assessing injuriesoccurring during horse riding, the second, injuries sustained during other horse related activities. Prevention strategiesare a major focus. The article updates and investigates in more detail horse related injuries as presented in Hazard 7,and for the first time looks at adult horse related injury
Horse Related InjuriesFiona WilliamsKaren Ashby
admissions for horse riders and 42%vs 14% of non-riders.
Head injuries are responsible for themajority of serious horse ridinginjuries and the risk of head injury ishigher in younger and less experiencedriders. (Barone, 1989, Bixby-Hammett et al, 1990).
The prevention of horse riding injuriesrequires adherence to standard horsehandling safety practices and the useof protective equipment, such asapproved safety helmets and approp-riately designed stirrups, shoes, tackand other protective equipment.Detailed recommendations for pre-vention are included.
activities named as equestrianactivities in the associated literature.
The morbidity and mortality assoc-iated with horse riding activities variesgreatly according to a variety of factorssuch as age, sex, type of activity,experience, helmet use, the type ofhelmet and both the age, size, characterand temperament of the horse.
The VISS data shows a predominanceof injury to girls (10-19 years) whoaccount for 41% of riding and 23% ofthe non-riding related injuries.
Children’s injuries (under 15 years)were of a more serious nature thantheir adult counterparts accountingfor 31% of children vs 22% of adult
SummaryHorses and horse riding provideenjoyable recreational and sportingactivities, however the potential forinjury is high due to the size andsometimes unpredictable nature ofhorses. (Sherry, 1991).
Of the 1330 cases of injury involvinghorses on the Victorian InjurySurveillance System database 80%were to horse riders, the remainderoccurred during horse handlingactivities or unrelated activities aroundhorses. The latter categories will bereferred to in this article as non-ridingactivities and activities specified ashorse riding will encompass those
V.I.S.S.

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 2
IntroductionHorse Related Activities– the RisksThe majority of injuries in mostreported studies occur whilst horseriding or driving (or whilst preparingfor/completing these activities) whichhave been noted as equestrianactivities, but around 25% of horserelated injuries are sustained duringgeneral horse handling activities(feeding, grooming, shoeing, leadinginto/out of floats etc) and unrelatedactivities (eg. playing in the vicinity).Horse riders were named as one offour priority population groups to betargeted for reductions in sports andrecreational injury in the Common-wealth Department of Human Serviceand Health’s Injury Prevention andControl Implementation Strategy.(Nutbeam et al, 1993, CommonwealthDepartment of Human Services andHealth, 1994). Although total injuryrates are relatively low compared tosome other sports, internationalstudies estimate that participants inequestrian sports are at higher risk ofserious injury, in terms of exposure(participation in hours), thanparticipants of most other sportingrecreational activities, includingmotorcycle and automobile racing.(Firth, 1985) (Silver et al, 1991).
Injury incidence in AustraliaTo date, only limited information hasbeen available on the incidence ofhorse riding injuries in Australia. Arecent report ranked horse ridingactivities in the top twenty sports/recreational activities resulting inpresentation to a hospital emergencydepartments for treatment. Of moreconcern, however, was their rankingas the third highest sport/recreationalactivity requiring hospital admissionfollowing presentation to an
emergency department for children(34% of cases were subsequentlyadmitted) and as the fourth highest foradults (20% of presentations wereadmitted). (Finch et al, 1995). InVictoria, the average annual frequencyof horse riding injuries requiringhospitalisation in public hospitals isapproximately 700. (Watt, 1995) Thisfigure is estimated from themechanism of injury code “animalbeing ridden”, based on 96% ofanimals being ridden being identifiedas horses among VISS admitted cases.The New South Wales FarmsafeCommittee has identified horses asinvolved in 8% of injuries occurringon farms, paddocks and fields and hasset, as a priority, the prevention ofhorse related injury (FarmsafeAustralia, 1994). Eighteen horserelated fatalities occurring in SouthAustralia during 1973-1983 wereexamined by Pounder, who foundthat head injuries were responsiblefor 78% of these deaths. None ofthese cases wore helmets.Unfortunately, information from othersources about equestrian injuries hasyet to be reported. (Pounder, 1984).
Horse RidingRelated InjuriesThese cases related to riding or drivinga horse or whilst preparing to start orfinish these activities (saddling,mounting, dismounting etc.). Horseriding is integral, for example, tohacking (ie riding for recreation andpleasure), trekking, racing, showjumping, dressage, eventing, huntingand polo, but not to horse drivingtrials, trotting or harness for pleasure.Participation data in equestrianactivities is limited in Australia, butin 1993/94, estimates were at least120,000 regular and 100,000 socialhorse riders in Australia. (Brokensha,1994). The Population Survey
Monitor conducted by the ABS in1994 estimated a total of 150,000participants aged 15 years or more inorganised horse riding activitiesthroughout Australia. At least 60% ofall participants are female and aboutone third of all Australian horse ridingactivity occurs in Victoria.
Emergency Department Data(VISS) (N = 1068)Seven campuses of five publichospitals have participated in thecollection of emergency departmentdata for the VISS database, which asof February 1995 contained 160,000records. The collection periods differbetween hospitals and are as follows:Royal Children’s Hospital (1988-93),Preston and Northcote CommunityHospital (1989-93 children, 1992adult), Western Hospital (1989-93children, 1991-92 adult), RoyalMelbourne Hospital (1992-93 adult),and Latrobe Regional Hospitals (fromJuly 1991-present, all ages). Of theLatrobe Regional Hospital andWestern Hospital, when all agecollections, only one third of caseswere to children. However, a biastowards children in the total VISSdatabase results in 58% of total casesbeing to children.
‘Rural’ as used in this study refers tothe Latrobe Regional Hospital and‘urban’ the remaining hospitals, alllocated in Melbourne.
Age and Sex DistributionStudies conducted elsewhere reportthat the majority of equestrian injurycases occur in young females (Nelsonet al, 1992, McGhee et al, 1987).VISS data in the two all-agecollections, Western and LatrobeRegional Hospitals show that overallchildren account for 35% of cases.The age groups with the greatest casenumbers of injury were the 10-14

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 3
year olds (24% of cases at each of thetwo all age collection hospitals) andthe 15-19 year olds (24% at WH and18% LRH).
The predominance of riding-relatedinjuries in females to age 20 is likelyto be a reflection of their greater levelsof participation. Bixby-Hammett andBrooks suggest, however, that giventhe increasing proportion of injuriesin males in the U.S.A. over recentyears, further research is needed intothe role of gender (Bixby-Hammett etal, 1990).
Females predominated both in childcases (77%) and the adult collections(59%). Males began to dominateslightly from the age of 30, however,this only becomes marked in the LRH40-49 year age group (16% ), perhapsreflecting the greater proportion ofoccupational injury cases in thiscollection.
Seasonal VariationsThe warmer months, October to April,are the most common months forhorse riding injuries.
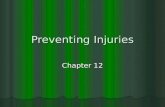
LocationThe most frequently reported locationsfor horse riding injuries are fields/paddocks (29%) and public roads(16%). The yard of a private home(mainly the victim’s), national (orother) parks and private/commercialamusement areas (racetracks, ridingschools and centres) were also notableproportions at 8%, 7% and 6%respectively. (See figure 1).
The pattern of locations was similarfor adults and children, but differedbetween the urban and rural regions.Not surprisingly, fields and paddockswere more frequently reported in ruralregions for both adults (33% rural vs22% urban) and children (38% vs26%).
Injuries occurring on public roadswere also much more frequentlyreported in the rural regions for bothadults (22% rural vs 8% urban) andchildren (34% vs 12%). The data alsoshowed a greater proportion of injuriesoccurred during transport and travelactivities in rural areas.
The importance of roads as a factor inequestrian injuries, generally, has beenrecognised by the draft ProposedAustralian Road Rules currentlyundergoing consultation. (AustRoads,1995). The draft includes a proposalthat the use of specified safetymeasures by horse riders when onpublic roads be made mandatory. Theproposals include requirements thatall horse riders wear a helmet,reflectors when riding at night and beallowed to use footpaths and naturestrips. The promotion of equestrianhelmets in Australia is likely to needa similar approach to that used topromote and effectively introducemandatory helmet wearing forbicyclists in this country. (Finch et al,1992).
Riding schools are reported in anumber of studies as the location ofthe injury event (Pounder, 1984Bixby-Hammett, 1992). VISS datashows that at least 10% of child injuriesin the urban area and 12% of injuriesin the rural areas occurred in ridingclubs/schools/centres.
ActivityHorse riding activities differ withriding speeds, terrain, and fitness andexperience levels of the rider. (Firth,1985). In turn, these factors havedifferent implications for frequency,nature and severity of injury. (Firth,1985). In the VISS data, although thespecific riding activity (dressage,mustering, cross-country) wasrecorded in the narratives of only afew cases, important data on the stageof the activity undertaken wasprovided in many of the casenarratives. Of the 1068 cases of riding-related injury, all but 34 appear tohave occurred whilst riding the horse.These 34 cases of injury occurredwhilst preparing to/finishing ride,dismounting/mounting and horsedriving (it must be remembered that
Horse Riding Injury by Location Figure 1
Field/paddock29%
Public road16%
Farm4%
Home yard8%
Park7%
Unknown18%
Private/commercialamuesment area
6%
Other12%
VISS: RCH, WH, PANCH, RMH, LRH (N = 1068)

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 4
these cases exclude non-riding relatedinjury cases, which are covered in thesecond section).
Whilst riding (n=1034)Contributing factorsUseful data on factors contributing tothe injury event was provided in thenarratives of 251 (24%) cases. Themajor groups of factors recorded were:horse behaviour (39%); jumping(16%); ground conditions (14%);equipment problems (8%); riderbehaviour (8%); and ‘other’ (15%).In a further 182 cases (17%) it wasrecorded that the horse bolted, buckedor reared but no details on underlyingreasons were given.
Horse behaviour (n=98)In all but 15 cases, a fright received bythe horse was the factor leading to theinjury event. Dogs (17) and vehicles(10) were the leading sources of fright,but the reason for fright was notspecified in 31 cases. Another horsewas involved in a further 11 cases,contributing to changes in horsebehaviour. Horse behaviour was givenas a factor in a greater proportion ofchild cases (61% or cases relating tohorse behaviour), compared withadults (39%).
Jumping (n=41)Injury to 18 children and 23 adultswas reported to have occurred whilstjumping. In a few cases, a fall duringthe jump was noted to have occurredwhen the horse clipped or struck theitem to be jumped (hurdle, gate, fenceetc) but in most cases further detail onthe injury event was not recorded.
Ground conditions (n=34)In 19 cases, the horse stumbled,slipped or tripped. Muddy/soft ground(8) and avoiding ditches (6) werefurther contributing factors. This is
not surprising given the predominanceof paddocks as locations of injury.
Equipment problems (failure anddislodgment) (n=29)In 5 cases, failure (ie. breakage) ofequipment was reported and includedbreakage of stirrups (3) and girth (2).In a further 24 cases, dislodgment ofequipment was noted and included:saddles (10), stirrups (6) and loss ofreins (7).
Rider behaviour (n=19)Rider behaviour was given as acontributing factor in 19% of childcases where a contributing factor wasapparent, and in only 4% of suchadults. Twelve cases were associatedwith bareback riding, and 10 of theseoccurred in metro areas. Other factorsmentioned were incorrect seating (1),riding too fast (1), inexperience (1)and lack of concentration (1).
Other (n=30)The rider was injured by a horse otherthan the horse he/she was riding in 14cases. In a further 18 cases, the horseand/or rider struck an object such as atree, fence, traffic sign or otherstructure. Although striking an objectdid not constitute a major proportionof events, 2 of the 10 fatalities to bediscussed later were the result ofstriking an object.
Other factors associated withinjuryOther factors such as rider experienceand supervision, previous injuries tothe rider and details of the horseinvolved (eg. age, size, type) havebeen reported by in-depth studiesoverseas (Ingemarson et al, 1989),but this level of data is generallyunavailable from a general injurysurveillance system.
The proportion of injured riders, whohad sustained a previous injury was
around 40% in 2 reported studies(Silver et al, 1991, Bixby-Hammett,1990). In fact, almost one-fifth ofinjured riders were reported to havehad more than 3 previous injuries,and one-quarter of injured ridersreported having had horse relatedincidents before beginning horseriding. (Bixby-Hammett, 1990).
Factors such as the age, size andcharacter of the horse are alsoassociated with injury occurrence,with each being inversely proportionalto injury occurrence. Thus, the olderand smaller the horse, the less is therisk of injury (Ingemarson et al, 1989).
Preparing for/completing riding(n=10)In 10 cases, injury occurred while thevictim was preparing to ride or drivethe horse (7) or preparing to finish (3).Injury was most frequently reportedto have occurred whilst saddling thehorse. Scenarios included the riderbeing distracted (and hit in the face bythe stirrups) and the rider tripping onthe reins after the horse moved itshead.
Mounting/dismounting (n=14)Injuries at the time of mounting thehorse were reported in 11 cases (5children, 6 adults). Again, no patternwas evident, but scenarios included:the horse kicking over the item beingused by the victim to stand on (drum,stool etc); or the horse becoming upsetor frightened. Only 3 injuries werereported as occurring at the time ofdismounting, and included fallingawkwardly and dismountingbackwards.
Driving the horse (n=10)In 10 cases, the horse was being drivenand injury occurred when the victimfell off a buggy or out of a sulky. In2 cases, this followed a fright to the

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 5
Injury Severity by Age and Sex - Horse Riding Injuries Table 2
Disposition of patient <15 years 15+ years <15 all 15+allM F M F
N % N % N % N % N % N %No treatment given 9 7 32 8 7 3 18 6 41 8 25 5
Treated, no referral/review 22 16 63 15 40 20 79 25 85 16 119 23
Review/referral 58 43 190 47 110 53 155 48 248 45 265 50
Admission to hospital/ transfer 46 34 121 30 49 24 68 21 167 31 117 22
Fatality - - 1 0 - - - - 1 0 - -
Total 135 100 407 100 206 100 320 100 542 100 526 100
VISS: RCH, WH, PANCH, RMH, LRH (N = 1068)
Body Regions Injured by Mechanism of Injury Table 1
Body RegionFall/thrownfrom horsen = 1009%
Kickedn = 51%
Rolled/trodon by horsen = 111%
Dragged byhorse
n = 33%
Othern = 126%
Head/face injuries 20 35 24 33 18
Upper limbs 47 12 20 27.5 39
Lower limbs 19 43 33 27.5 33
Trunk 13 6 17 9 10
Other 1 4 6 3 -
Total 100 100 100 100 100
VISS: RCH, WH, PANCH, RMH, LRH (N = 1330). NB up to 3 injuries per case.
horse and in another 2 it followedcollision with another horse in a race.
Mechanism of injury(N = 1068)Falls predominated in both childrenand adults and in urban and rural areasaccounting for 77% of all cases. Alsoreported were crushes when the horserolled on or stood on the victim (7%),kicks (4%) or the rider being draggedafter getting their foot caught in thestirrup (2%).
Resulting injuries are shown below inTable 1.
The predominance of falls as amechanism of injury has beenrecognised in many studies, (Barone75%, McGhee 90%, Hobbs 63%).Ingemarson, in an analysis of 406cases of riding injury reported thatfalls predominated in leisure riders,
but the horse rolling over wasresponsible for more of the contestriders and suggests that thepredominance of falls reflects thepredominance of leisure riders.
Injury SeverityNearly half (48%) of victims of horseriding injuries required significanttreatment, ie, a referral or review afterthe initial consultation in theemergency department. A further27% of victims required admission tohospital. Table 2 shows a breakdownof treatment required.
The severity of falls from a height(over one metre for horse riding) isevidenced by 27% of fall victimsrequiring hospital admission.
Nature of InjuryVISS allows up to 3 injuries per caseto be recorded. Fractures were the
most common injury, followed bysoft tissue injury (lacerations, bruising,abrasions), strains/sprains andconcussion. Fractures accounted for43% of child injuries and 30% ofadult injuries. This compares with18% of child presentations in the entireVISS database and 16% of adultpresentations, indicating the seriousnature of horse riding related injury.
Fractures were predominantly to theupper limbs, particularly the radius/ulna (16% of children’s injuries vs5% of adult injuries), humerus (8% vs2%) and wrist (4% vs 5%). Another4% of adult injuries were rib fractures.
Soft tissue injuries (bruising, lacer-ations, abrasions) accounted for 33%of child injuries and 29% of adultinjuries. Most soft tissue injurieswere to the face and scalp (4% of totalinjuries sustained).

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 6
is not surprising given that the rider’shead can be 3 metres above the groundlevel prior to a fall (McGhee et al,1987) and that the speed of a horse canbe up to 65 km/hour (Silver et al,1991).
Prevention of injury is importantparticularly for (i) upper limbs becauseof their frequency and (ii) head regionbecause of the predominance of severeinjury. In the case of head injury, thestandards-approved equestrian helmetis (despite the lack of a full evaluation)currently the most important item ofprotective equipment. (Firth, 1985)
Hospital Admissions DataThe Victorian Inpatient MinimumDataset provides data on all publichospital admissions in Victoria. Datacovering the years 1987-1993 has beenexamined to explore riding injuries.The ICD9 coding system is limited to“animal being ridden” for identifyingrelevant cases. This figure is estimated
Children’s Horse Riding Figure 2Injuries by Body Part
(NB up to 3 injuries per case).VISS: RCH, WH, PANCH, RMH, LRH.
Adult Horse Riding Figure 3Injuries by Body Part
(NB up to 3 injuries per case).VISS: WH, PANCH, RMH, LRH.
Sprains and strains accounted for 6%of child and 15% of adult presen-tations, with the most commonlyaffected areas being ankles (2%),shoulders, wrists and neck (each 1%).
Concussion accounted for 8% ofpresentations in both children andadults, 65% of whom requiredadmission to hospital. The proportionof child and adult presentations forconcussion is greater for horse ridinginjury than for all sports injuries onthe VISS database, where 4% of childand 3% of adult injuries are forconcussion.
When the first injury only is examined,compared with up to 3 injuriesrecorded, fracture proportions arehigher, soft tissue injuries are lowerand sprains/strains and concussionshows little difference.
Body region injured- (up to 3 injuries per case)VISS data showed that 50% of childand 34% of adult injuries are to theupper limbs, most commonly to theradius/ulna (9% of total number ofinjuries-all ages, all cases), the elbow(5%), the humerus (4%) and theshoulder (4%). Figures 2 (children)and 3 (adults) show the most commonbody regions injured.
Lower limbs also accounted for asubstantial proportion (17% ofchildren and 27% of adults), but Hobbssuggests that lower limb injuries areless likely to be associated with fallsand are more likely to be associatedwith being trodden on or fallen on bya horse.
The head and face comprise 22% ofchild and 20% of adult injuries, butthey are over-represented in thoseadmitted to hospital (36% of childand 27% of adult admissions) . This

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 7
from the mechanism of injury code“animal being ridden”, based on 96%of animals being ridden beingidentified as horses among VISSadmitted cases. Thus, there were anestimated 4109 cases identified inthis way representing a rate of injuryof 16 per 100,000 population, with anannual average of 685.
The peak age for injury was 10-14years (consistent with the VISS data).Head and face injuries combinedaccounted for 29% of injuriessustained including, importantly,intracranial injuries (12%), concussion(11%) and other head/face injuries(6%). A further 26% of injury was tothe upper limbs and 4% to the spineincluding 14 cases over the 5 yearperiod of injury to the spinal cord.
The average stay in hospital wasapproximately 4 days with a medianof 2 days. Figure 4 shows the trendsfor horse riding injury as recorded inthe VIMD.
Although a downward trend in horseriding injuries requiring hospital-isation is observed, this trend is notstatistically significant.
It should be noted that cases of horseriding injuries are also frequentlyadmitted to private hospitals inVictoria. In an 18 month period fromJanuary 1993 - June 1994, 162admissions were recorded, with a ratioof 2 females to 1 male. Thus thisimpacts on the total state incidence,increasing the annual averagefrequency to approximately 785 andthe rate to 18 per 100,000.
Mortality DataData from the Coroner’s database isavailable for the period 1988/89 and1991/92 inclusive. Seventeen horserelated deaths were reported in thistime, with 10 of these being riding-related injuries. In two of these 10cases, the victim was riding a horseand fell; in two cases, the victimstruck an object (fence, power pole);the victim was struck by a vehicle ina further case and in the final case,two horses collided and fell on thevictim. Two of these cases resultedfrom equipment failure (broken reins),one from the horse stopping suddenlyand one where the horse stumbled. In3 cases, bolting by the horse (reasonnot specified) led to the injury event
and in one case, the victim’s foot wascaught in the stirrup and the victimwas dragged for some distance.
Of the 17 cases, 71% recorded injuriesto the head and a further 71% to thechest. Helmet use was not recorded inthe narrative of any of the cases.
Most previous studies report thepredominance of head injuriesamongst fatalities. Few mortalitystudies have been done in Australia,but Pounder examined 18 fatalities(inc. two natural deaths) in SouthAustralia from 1973-1983. Headinjuries accounted for 14 of the 18fatalities.
Studies in Sweden (Aronson & Tough,1993, Ingemarson et al, 1989) andUSA (Bixby-Hammett, 1992) alsoreported that head injuries account forthe majority of fatalities, with helmetuse almost nil in the former study.Ingemarson reported that all fatalitiesfollowed cerebral trauma, and that ofthe 22 out of 38 who wore helmets,only two helmets provided protection.The rest were the classic riding helmet(consisting of only two layers - anouter concussion - preventive and aninner layer for comfort), this offerspoor protection for avoiding serioushead injury.
Prevention of InjuriesThe prevention of horse riding injuriesrequires adherence to standard horsehandling safety practices and the useof protective equipment, such asapproved safety helmets andappropriately designed stirrups, shoes,tack and other protective equipment.The most important of these is a safetyhelmet that meets the currentAustralian Standard AS2063.3.Training (of horses, riders and horsehandlers) is also an important strategyfor safety. Other prevention measuresinclude responsible course
Trends in all age Horse Riding Injuries - Victorian InpatientMinimum Dataset Figure 4
Year
Rat
e/10
0,00
0 po
pula
tion
14
15
16
17
18
1987 1988 1989 1990 1991 1992
S lope = -0.3 (95%CI -0.8, 0.2), p=0.14 ns
VIMD: July 1987-June 1993 (Public Hospitals)

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 8
construction, adequate casualtypreparation, practice in fallingtechniques and licensing of ridingschools and supervisors.
Protective EquipmentHelmetAlthough a full evaluation of the effectof equestrian helmets on injury ratesis yet to be reported, one study hasshown that the wearing of an approvedhelmet by professional jockeys isassociated with a reduction in theincidence of severe head injury.(Barone et al, 1989). Overseas studiesreport that many injuries are associatedwith the wearing of no helmet, thewearing of an inadequate helmet or ahelmet that dislodges from the headduring a fall. (Ingemarson et al, 1989,Sherry, 1991, Nelson et al, 1992).Further, concussion in children in theUnited States Pony Clubs decreasedfrom 12% to 8.7% following therequirement for children to wear asafety helmet with chin strap (Barone,1989). In addition, helmet use (usuallytype of helmet not specified) wasreported as low in a number of studiesof persons injured or killed duringequestrian activities. (Sherry, 1991)(Barone et al, 1989). This is furthersupported by the decreased risk ofhead injury in bicyclists and motor-cyclists associated with helmetwearing.
The VISS data shows that 42% ofurban child riders and 49% of ruralchild riders recorded wearing a helmet.In adults, only 23% of metro caseswore a helmet, with 41% of those innon-metro areas wearing a helmet. Inmany cases, as in other studies, noinformation was provided about thetype of helmet used and, given thevariation in available helmets, aboutthe level of protection afforded.
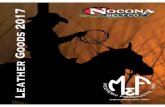
In those reported to have worn helmets,the level of protection afforded isquestionable given that onlystandards-approved equestrianhelmets are designed to provideadequate safety and that even thesehelmets have been reported to provideinadequate protection. The functionof the equestrian helmet is to (i) preventskull penetration and deformation and(ii) absorb and transfer energy,reducing energy transfer to the brain.(Firth, 1985). The helmet needs to beproperly worn and needs to stay onand in place throughout impact. (Firth,1985). Helmet design shouldincorporate an outer cover for aestheticreasons, a hard smooth shell to preventpenetration and major distortion,spreading localised blows over a largerarea of the impact energy layer, alining (space or structure) that isenergy absorbing and a chin strapwith 4 point suspension (Firth, 1985).
In Australia, to be approved as anational safety standard (AS 2063.3),helmets need to be extensively testedfor such factors as shock absorption,penetration resistance, visionclearance, strength/retention systems
and peak flexibility (Sherry, 1991).The helmet shown in figure 5 meetswith the AS 2063.3.
The classic riding helmet is consideredinadequate in that it is designed withtwo layers only (an outer layer to helpprevent concussion and a comfort-promoting inner layer) and thusprovides poor protection against headinjury. It is also only secured at twopoints, not the recommended fourpoints and often is only secured by anelastic strap.
Surveyed horse riders report low levelsof regular helmet wearing, despitedemonstrating a high awareness ofthe need for helmets. In Australia, astudy of school pupils in rural areasby Lower and Wolfenden (1995) alsoreported a high level of safetyknowledge generally, but reported thatthis was not reflected in attitudes andbehaviour. Although 90% specified astandards-approved (ASA) helmet ascorrect gear, only 57% wore an ASAhelmet when riding and one-quarterbelieved that it was safe to ride withouta helmet.
Features of a Standards approved riding helmet Figure 5

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 9
Attitudinal barriers to the use ofprotective helmets were reported as:discomfort (heavy and hot) ; expense;appearance of the helmet; the fact thatthey are quickly outgrown (insert padsnot used as in bicycle helmets); andthe inappropriateness for some ridingstyles where a brimmed hat istraditionally worn (such as in westernand trail riding). (Condie et al, 1993,Nelson et al, 1994).
Lower and Wolfenden also report lowlevels of formal instruction as apotential barrier to reported safetybehaviour generally. Only 40% ofrespondents had received formalinstruction, with the remainderreceiving information from family andfriends. The authors reported that thelogistics and costs of transporting thehorse to clubs for instruction weremajor barriers. The frequency ofopportunistic (unplanned) riding isalso a barrier to formal instruction.
Overcoming barriers to helmetwearing clearly needs to be multi-faceted, requiring attention to manyfactors. Making helmet wearingmandatory is likely to be difficult toenforce, except on public roads and atriding clubs or events, particularlygiven that much riding is on privateproperty (Lower & Wolfenden, 1995)and attention needs to be directed tofactors such as design, risk perceptionand instruction.
Heeled riding boots, stirrupsand safety stirrupsGiven the predominance of injuriesfrom falls, protective equipment andprecautions allowing rapid dis-engagement during a fall are vital.Trapping of the rider’s foot in thestirrup may result in dragging of thehead and body along the ground, withthe potential for severe injury. Thecombination of boots and stirrups
worn is essential, heeled riding bootsmust be individually matched to thestirrup for size and fit to be effectiveagainst injury and thus help preventthe rider’s foot from being trapped inthe stirrup. (Firth, 1985, Ingemarsonet al, 1989). Boots should be withoutgrip, featuring smooth heels and soles,and should feature elastic sides toensure the foot can be pulled out if thevictim is falling and prevent beingdragged if the shoe were to be caught.
Correct stirrup size is important, astirrup that is too large is a risk forinstability.
Safety stirrups that feature a curvedfront on one side of the stirrup iron,which should always be placed to theoutside, are recommended widely.However improper usage ie, the curvenot being placed to the outside couldplausibly cause the foot to becomecaught in the stirrup, thus care shouldalways be taken in the securing of thestirrup.
Safety stirrups with a pressure releaseallow quick release of the stirrup onincreased foot pressure. These maybe more appropriate for leisure ridingthan competition. Evaluation studiesare required to determine theeffectiveness of the various safetystirrups for particular activities.
Recommendations
1. Choose a horse of appropriate size, temperament, character and age for therider’s size and skill level, in conjunction with a trained and experiencedhorseperson. No beginner or child should have a horse aged less than fiveyears, older horses are better for beginners.
2. Routine checks before mounting: check equipment for signs of fatigue andcorrect adjustment of fit. Regular maintenance checks of all equipmentshould be undertaken.
3. Strongly recommended equipment: ASA-approved helmet, stirrupsmatched to size of smooth heeled and soled boots with elastic sides andnon-slip gloves. Loose clothing should be avoided, long hair should betied back and do not wear spectacles (if possible).
4. Where possible, avoid excessively soft/muddy ground and ditches, holesand uneven terrain with rocks and exercise caution if these surfaces areunavoidable.
5. Develop riding skills progressively and thoroughly and have a goodknowledge of horse behaviour. Over time, develop a bond with the horseand don’t undertake bareback riding.
6. Exercise caution when riding in the presence of objects or animals thatcould frighten the horse (eg. other horses, dogs, vehicles) - this isparticularly applicable to children.
7. An educational program is recommended to encourage recreational ridersto have riding lessons with accredited instructors.
8. Limit riding in outside paddocks to experienced riders, inexperiencedriders should always be supervised whilst riding.
9. Consider parental training schemes in instruction methods in rural areas.

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 10
Other protective equipmentThe efficacy of body protectors hasnot yet been established, but it hasbeen suggested that these, as asecondary safety measure, mayprotect from soft tissue injuries andfractured ribs. (Bixby-Hammett et al,1990).
Spectacles are suggested asinadvisable due to the risk of facialfractures or facial-ocular laceration.As a result contact lenses aremandatory under Jockey Club rules(Firth, 1985). Gloves should be non-slip (Firth, 1985) and loose clothingshould be avoided because of the riskof catching on passing objects (eg.tree branches) (Nelson et al, 1992).Long hair should be tied back to avoidpossible scalping injuries.
Safety precautionsAlong with the protective equipmentoutlined above, strategies such as goodinstruction and good maintenance ofequipment are important. (Firth,1985).
Routine checking and maintenance ofall equipment (saddles, bridles etc)and of pre-mounting and pre-dismounting checks are suggested asimportant safety measures.
Further researchThe need to conduct further researchinto equestrian injury counter-measures has been identified by theEquestrian Federation of Australia inthe 1995 edition of the AustralianSport Commission’s Sports ResearchNeeds publication. The followingpotential countermeasures, in partic-ular, require implementation andevaluation: increasing general aware-ness of safety issues by riders,adequate supervision of children,coach awareness, use of protectiveclothing, particularly helmets and back
protectors and the correct fitting ofhelmets. Further information isrequired in the extent and nature ofexposure to horse riding and barriersto use of countermeasures.
Horse Related Injury– Non Riding (N = 262)The definition of non-riding relatedinjury, for the purposes of this article,includes injuries occurring other thanduring horse riding/driving (or whilstpreparing for/completing theseactivities). This includes horse relatedactivities (feeding, grooming, shoeing,leading into/out of floats etc) andunrelated activities (eg. uninvolvedbystanders). Two hundred and sixty-two cases of injury occurred whileundertaking these activities and mostwere the result of horse behaviour.
These injuries, although less numerousthan riding injuries, are a seriousproblem, particularly in children. Onehalf of child injuries were to the headand face and 42% of children requiredadmission to hospital. Age and sexpatterns are discernible in certain non-riding activities. For example 10-14year old females predominate ininjuries occurring whilst walking andleading the horse, boys under 5 yearsof age were commonly injured whilstplaying around the horse, and adultswere more commonly injured whilegrooming and shoeing horses. Interms of the body region injured, thehead and face was the most commonregion injured in children (50%) whileadult injuries were more common tothe upper limbs (42%), particularlythe fingers. The single most commonmechanism of injury was kicks (44%).
Age and Sex DistributionVISS data in the two all-agecollections, Western and LatrobeRegional Hospitals show that overallchildren account for one quarter of
cases. The age groups with the greatestcase numbers of injury varied betweenthe urban and rural hospitals. Childrenin the 10-14 year old age group werethe most common victims at the urbanhospital (24% of WH vs 10% LRH).In contrast injury peaked in the 30-34year old age group for the rural hospital(17% of LRH vs 3% WH). Nearlytwo thirds of child and one half ofadult cases were to females.
Fields and paddocks (29%), thevictim’s own home yard (18%) andareas of transport (7%) were the mostcommon sites for injury. Another18% of cases occurred at anunspecified location.
Safety devices were not commonlyused when undertaking these otherhorse activities, only 7 cases recordedany use of a safety device. Four victimswere wearing helmets and 3 werewearing protective footwear.
Injury DetailsBruising (23%), fractures (22%) andlacerations (19%) were the mostcommon injuries, however there wereconsiderable differences betweenchildren’s and adult injuries in regardto the body regions injured. (Seefigure 6). This is not surprising giventhe nature of activity differs betweenthe age groups.
Half of child injuries were to the headand face, the most common beinglacerations to the face and scalp (9%),fractures of the skull (8%), concussion(8%) and bruising to the face andscalp (4%). Of the total 184 injuries(VISS can record up to 3 injuries percase), bruising to the abdomen (4%)and feet (3%) were also common.Bites represented only 2% of injury,but Hobbs has suggested that manybite victims may not seek attentionfor their injuries, thus making the trueproportion of bite injuries difficult toascertain. (Hobbs, 1994).

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 11
Common Injury ScenariosAn examination of the case narrativesindicates common scenariosassociated with other horse relatedinjury, the most frequent of these arediscussed below. Of the 262 cases,72% provided sufficient informationin the narratives for furtherexamination and half of these arecategorised and discussed below. Theremainder, due to the small numbersinvolved, have not been analysedfurther.
Walking/Leading (N = 52)Fifty-two victims were injured whilewalking or leading a horse, with 16 ofthese cases involving loading orunloading the horse onto a float. Thesescenarios most frequently involvedgirls in the 10-14 year old age group(21%) and in one third of cases thelocation was a field or paddock.
Just over 20% of cases involved thehorse shying or taking fright, howeveronly 3 cases noted any reason for this(2 horses were frightened by motorvehicles and 1 by a dog).
Another 11 victims were injured whentheir finger or hand was caught in thelead rope or rein, this is reflected in
Non-Riding Horse Injuries by Body Part Figure 6
(NB up to 3 injuries per case). VISS: RCH, WH, PANCH, LRH.
Other Horse related injury by treatment received Table 3
DisposalChildren
%( N = 132)
Adult%
( N = 130)
No treatment 8 1
Treated, no referral 20 26
Treated, referral Outpatients 6 15
Treated, referral GP 10 27
Other referral 1 2
Casualty review 8 15
Admission 46 14
D.O.A or died in casualty 1 -
TOTAL 100 100
VISS: RCH, WH, PANCH, RMH, LRH (N = 262)
(26%). Another 20% of child victimswere treated without further referral.(See table 3).
There were a total of 154 injuries toadults, most frequently to the upperlimbs (42%), particularly the fingers(21% of total injuries). The mostcommon injuries sustained werefinger lacerations (6%), lacerationsof the face and scalp (5%), fracturesof the foot (4%) and fractures of thefinger (3%).
Forty-two percent of child victimsand 14% of adult victims were injuredseriously enough to require admissionto hospital. It is worth noting that theadmission rate for children in non-riding related injuries is higher thanthe children’s admission rate for horseriding related injury (30%). Adultvictims were more often treated andreferred to a general practitioner (27%)or treated without further referral

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 12
the fact that 26% of injuries in thisgroup were to the fingers, particularlyfractures and dislocations. “Attempt-ing to remove horse from float. Horsereared. Finger caught in rope.”
A NSW Pilot Education Program (year5 and 6 students) concluded that“knowledge about horse handling asdistinct from riding, was less certainand appears to be an area whichrequires further emphasis”. (Loweret al, 1995). For example only two-thirds knew the correct way to hold alead.
Feeding (N = 25)Again one third of injury was tochildren in the 10-14 age group andhalf occurred in paddocks. Kicks (12cases) and bites (6 cases) wereprevalent and in 3 cases these injurieswere inflicted by a horse other thanthe one the victim was feeding. Whilethe injuries sustained in this groupwere varied, 12% of injury were bitesto the finger. eg. “Feeding horses.Another horse attacked her to getfeed. Bitten by horse”. Childrenshould be instructed that hand feedingof horses should always be done witha flat palm to ensure fingers do not getin the way and risk being bitten.
Playing/Bystander (N = 23)Nearly three quarters of injuries inthis category were to children agedunder 5, particularly boys (61% oftotal group). Nearly half of theseinjuries were to the head and face, and19% of total injuries (7 cases) werefractures of the skull. Sixteen of thetotal cases (70%) were kicks, four ofwhich occurred when the victimmoved either behind a horse or into agroup of horses. “Whilst playing,chased horse. Horse kicked child inmouth.”. There was one associatedfatality on the VISS database whichfalls into this category, a 2 year old
was kicked by a horse after climbingfrom a pusher and running behind ahorse at a pony club event.
Grooming (N = 16)This group encompasses activitiessuch as brushing (5 cases), grooming(3) and washing (2) the horse. Victimsin this group tended to be older than inthe other groups, three quarters wereaged 20 years and over. Three quartersof victims were female. Bruisingaccounted 35% of all injuries to thisgroup and again finger injuries werethe most common (4 cases).
Half of the victims were kicked byhorses, in two cases these were horsesother than the one the victim wasattending to. Where possible the horsebeing treated should be isolated fromother horses.
Shoeing (N = 12)All but one victim was aged over 15years and two-thirds of victims weremale. Injuries most frequentlyoccurred when the horse moved itsleg while being shod and the shoe nailcut the victim, “Shoeing a horse.Horse dropped his foot. Nail exposed.Cut by nail”. Another 4 victims wereinjured when the horse stood on thevictim’s feet and fingers, “Pickingout horses back hoof. Horse stood onfingers.” Of the remainder, 3 victimswere kicked and one was lacerated bya knife used in the shoeing process.
Other InjuriesThere were 8 cases of road trafficcollisions with a horse on the database, these involved 4 cars, twominibuses and two motorbikes. Ofthe remaining cases a further 65victims were kicked by horses, 6 whilepatting the horse, 3 while catching thehorse, two while assisting the matingof the horse and two when letting thehorse out of its enclosure. Another 18
victims were trod on by the horse, 8were knocked by the horse, 6 hadfingers caught in ropes or reigns whileholding the horse, a further 4 werebitten and 4 were jammed betweenthe horse and another object.
Work RelatedOf the 262 cases discussed in thisarticle 20 victims were working at thetime of injury. Three quarters ofvictims were male and were mostcommonly aged between 15 and 19(30%). Victims were most commonlyemployed in the animal handlingindustry (55%), and were mostfrequently walking/leading (8 cases),holding (3) and shoeing (2) the horsewhen the injury occurred. Still only 3victims recorded the use of any safetydevice, 2 wore skull caps and the thirdwork boots.
Mortality DataOf the 17 deaths relating to horses onthe Victorian Coroners Databaseoccurring during the period 1989/90and 1991/92, 7 were related to non-riding activities as defined in thisarticle. This figure is a much higherproportion than that found on theVISS database, thus re-enforcing thepossible serious nature of these typesof injuries. Three victims were kickedby horses, two were involved in roadtraffic crashes when their car hit ahorse that strayed onto the roadwayand the remaining two were trampledby horses.
AcknowledgmentsWe gratefully acknowledge thevaluable comment made by thefollowing people: Dr Craig McCauley- Knox Private Hospital, GillianCanapini - Equestrian Federation ofAustralia, Frances Correy - Pony ClubAssociation of Victoria, Julia Palmer- Latrobe Regional Hospital andGiulietta Valuri for assistance withanalysis.

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 13
References• Aronson H, Tough SC., 1993, Horse relatedfatalities in the province of Alberta, 1975-1990. The American Journal of ForensicMedicine and Pathology, 14(1): 28-30.• AustRoads., 1995, Proposed Australianroad rules: draft for public comment.Canberra.• Barone GW, Rodgers BM., 1989, Paediatricequestrian injuries: a 14-year review. Journalof Trauma, 29(2): 245-247.• Bixby-Hammett D., 1985, Youth accidentswith horses. Physician and Sports Medicine,13: 105-117.• Bixby-Hammett D, Brooks WH., 1990,Common injuries in horseback riding: areview. Sports Medicine, 9(1): 36-47.
• Bixby-Hammett DM., 1992, Pediatricequestrian injuries. Pediatrics, 89(6): 1173-1176.• Brokensha P., 1994, Available data andsources for the sport and recreation industry.First draft prepared for the Sport andRecreation Ministers Council. Adelaide.• Commonwealth Department of HumanServices and Health., 1994, Better healthoutcomes for Australians. Canberra:Australian Government Publishing Service.• Condie C, Rivara FP, Bergman AB., 1993,Strategies of a successful campaign topromote the use of equestrian helmets. PublicHealth Reports, 108(1):121-126.• Farmsafe Australia Program Report, 7February 1994, p 12.• Finch CF, Heiman L, Neiger D., 1993,Bicycle use and helmet wearing rates inMelbourne, 1987 to 1992: the influence ofthe helmet wearing law. Melbourne: MonashUniversity Accident Research Centre ReportNo.45.• Finch CF, Ozanne-Smith J, Williams F.,1995, The feasibility of improved datacollection methodologies for sports injuries.Melbourne: Monash University AccidentResearch Centre Report No. 69.• Firth JL., 1985, Equestrian injuries. In (eds)Schneider RC, Kennedy JC, Plant ML: Sportsinjuries: mechanisms, prevention andtreatment. Baltimore: Williams and Wilkins.• Hobbs GH, Yealy DM, Rivas J., 1994,Equestrian injuries: a five-year review.Journal of Emergency Medicine, 12(2): 143-145.• Ingemarson H, Grevsten S, Thoren L., 1989,Lethal horse riding injuries. Journal ofTrauma. 29(1): 25-30.• Lower, T. and Wolfenden, K., 1995,Preventing Horse Related Injury - A PilotEducation Program. Health• Promotion Journal of Australia, 5(1): 46-50.• McGhee CN, Gullan RW, Miller JD., 1987,Horse riding and head injury. British Journalof Neurosurgery, 1(1): 131-136.• Nelson DE, Bixby-Hammett D., 1992,Equestrian injuries in children and youngadults. American Journal of Diseases ofChildren, 146(5): 611-614.• Nelson DE, Rivara FP, Condie C., 1994,Helmets and horseback riders. AmericanJournal of Preventive Medicine, 10(1): 15-19.• Nutbeam D, Wise M, Bauman A, Harris E,Leeder S., 1993, Goals and targets forAustralia’s health in the year 2000 andbeyond., Canberra: Commonwealth Depart-ment of Health, Housing and CommunityServices.
• Pounder DJ., 1984, The grave yawns forthe horseman. Medical Journal of Australia,141: 632-635.• Sherry K., 1991, Horse related injuries.Hazard, 7:1-5. Melbourne, Victorian InjurySurveillance System.• Silver JR, Lloyd Parry JM., 1991, Hazardsof horse riding as a popular sport. BritishJournal of Sports Medicine, 25(2): 105-110.• Watt G., 1995, Hospitalised InjuriesVictoria, July 1989 - June 1993. Melbourne:Monash University Accident Research CentreReport No.67.
Recommendations
1. Small children should separatedfrom horses. Safety precautionsaround horses should be taughtfrom an early age under closesupervision. The routine use ofhelmets in any smaller childrenaround horses is recommended.
2. Further emphasis on safety inthe area of risk factors for horsehandling (as distinct from horseriding) is needed. Awarenessof the potential hazardsassociated with horse handlingneeds to be increased as doesknowledge of the behaviour andunpredictable nature of horses.
3. Sturdy boots should be wornwhen undertaking horsehandling activities.
4. If possible the horse should beisolated from other horses whenundertaking the types ofactivities described in thisarticle.
5. Effective hand, particularlyfinger protection warrantsinvestigation, with particularrelevance to rope handling.
6. Avoid the back legs of horses atall times.
SHORT COURSE ONINJURY EPIDEMIOLOGYAND PREVENTIONThis course will be conducted inassociation with the Third Inter-national Injury Prevention & ControlConference.
Dates: Feb. 12–16 (incl.) 1996
Venue: Janet Clarke Hall, Universityof Melbourne (a short tram ride fromthe centre of Melbourne). Low costaccommodation on location at A$35/night (bed and breakfast).
Objectives: To provide intensivetraining to improve the injuryprevention knowledge, research andprevention skills of practisingprofessionals and graduate studentsfrom both industrialised and non-industrialised countries.
Responsible Organisations:Monash University AccidentResearch Centre (Australia) andWHO Collaborating Centre forResearch and Training in SafetyTechnology, Delhi (India).
Registration: A$500, includingcourse materials and lunches.
Further Details:Ms Fiona Williams,Accident Research Centre,Monash University,Clayton 3168, Victoria, AustraliaPhone: 61 3 9905 1808Fax: 61 3 9905 1809

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 14
- INDEX -Subject Edition PagesArchitectural glass .......................................................................................................................... 22 ...................................... 1-5Babywalkers, update .................................................................................................................. 16,20........................... 1-4,12-13Bunkbeds ......................................................................................................................................... 11 ....................................... 12Bicycles
- Bicycle related injuries ....................................................................................................... 6 ...................................... 1-8- Cyclist head injury study ................................................................................................... 2, ......................................... 2- Cyclist head injury study updates ............................................................................... 7,8,10 ................................. 8,13,9
Burns- Scalds ................................................................................................................................... 3 ...................................... 1-4- Burns prevention ............................................................................................................... 12 .................................... 1-11
Chainsaws ........................................................................................................................................ 22 .................................. 13-17Child care settings ........................................................................................................................... 16 .................................... 5-11Data base use, interpretation & example of form ............................................................................ 2 ...................................... 2-5Deaths from injury (Victoria) ......................................................................................................... 11 .................................... 1-11Dishwasher machine detergents - Update ...................................................................................... 18 ....................................... 11Dogs
- Dog related injuries ............................................................................................................. 3 ...................................... 5-6- Dog bite injuries ................................................................................................................ 12 ....................................... 12
Domestic architectural glass ............................................................................................................. 7 .................................... 9-10Domestic Violence .......................................................................................................................... 21 ...................................... 1-9Drownings/near drownings
- Immersions .......................................................................................................................... 2 ......................................... 3- Pool fencing legislation, update....................................................................................... 2,7 ...................................... 3,7- Drownings & near-drownings at home ............................................................................... 5 ...................................... 1-4
Exercise bicycles, update ............................................................................................................... 5,9 ...............................6,13-14Home injuries .................................................................................................................................. 14 .................................... 1-16Horse related injuries ........................................................................................................................ 7 ...................................... 1-6Infants - injuries in the first year of life ........................................................................................... 8 .................................... 7-12Intentional injuries .......................................................................................................................... 13 .................................... 6-11Latrobe Valley
- The first three months ......................................................................................................... 9 .................................... 9-13- Latrobe Valley injuries .................................................................................. * March 1992 ...................................... 1-8- Injury surveillance & prevention in the L. V. ..................................................... *Feb 1994 .................................... 1-14
Lawn mowers .................................................................................................................................. 22 ...................................... 5-9Martial arts ...................................................................................................................................... 11 ....................................... 12Motor vehicle related injuries, non-traffic ..................................................................................... 20 ...................................... 1-9Needlestick injuries......................................................................................................................... 11 ....................................... 12Older people, injuries among.......................................................................................................... 19 .................................... 1-13Off-street parking areas .................................................................................................................. 20 .................................. 10-11Playground equipment ...................................................................................................................... 3 ...................................... 7-9Poisons.................................................................................................................................................
- Child resistant closures ....................................................................................................... 2 ......................................... 3- Drug safety and poisons control ......................................................................................... 4 ...................................... 1-9- Dishwasher detergent, update ........................................................................................10,6................................. 9-10,9
Roller Blades ................................................................................................................................... 15 .................................. 11-13School injuries................................................................................................................................. 10 ...................................... 1-8Shopping trolleys ............................................................................................................................ 22 .................................. 10-12Skateboard injuries............................................................................................................................ 2 ...................................... 1-2Smoking Related injuries ................................................................................................................ 21 .................................. 10-12Sports
- Sports related injuries.......................................................................................................... 8 ...................................... 1-6- The 5 most common sports ................................................................................................. 9 ...................................... 1-8- Adult sports injury............................................................................................................. 15 .................................... 1-10
Trampolines..................................................................................................................................... 13 ...................................... 1-5VISS: early overview ........................................................................................................................ 1 ...................................... 1-5VISS: how it works ........................................................................................................................... 1 ...................................... 6-8Work Related Injuries ................................................................................................................ 17,18........................... 1-13,1-10* Special edition

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 15
VISS StaffDirector: Dr Joan Ozanne-Smith
Co-ordinators: Virginia RoutleyFiona Williams
Research Assistant: Karen Ashby
Administrative Assistant: Christine Chesterman
Data Processors: Julia Palmer Latrobe Regional Hospital
Associate Director: Dr Terry Nolan(Child Injuries)
GeneralAcknowledgementsParticipating HospitalsLatrobe Regional Hospital (Traralgon and Moe)
The contributions to the collection of VISS data by the director and staff of theEmergency Departments of these hospitals, other particpating clinicians, MedicalRecords Departments, and ward staff are all gratefully acknowledged. Thesurveillance system could not exist without their help and co-operation.
Coronial ServicesAccess to coronial data and links with the development of the Coronial Service’sstatistical database are valued by VISS.
National Injury Surveillance UnitThe advice and technical back-up provided by NISU is of fundamental importanceto VISS.
How toAccess VISSData:VISS collects and tabulates infor-mation on injury problems in order tolead to the development of preventionstrategies and their implementation.VISS analyses are publicly availablefor teaching, research and preventionpurposes. Requests for informationshould be directed to the VISS Co-ordinators or the Director by contact-ing them at the VISS office.
VISS is located at:Accident Research CentreMonash UniversityBuilding 70Wellington RoadClayton, Victoria, 3168
Postal address:
As above
Phone:
Reception (03) 9905 1808
Co-ordinators (03) 9905 1805(03) 9905 1815
Director (03) 9905 1810
Fax (03) 9905 1809

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 23 page 16
VISS is a project of the Monash University Accident Research Centre.
Hazard was produced by the Victorian Injury Surveillance Systemwith the layout assistance of Glenda Cairns, Monash University Accident Research Centre.
Illustrations by Jocelyn Bell, Education Resource Centre, Royal Children’s Hospital.
ISSN-1320-0593
Printed by Sands and McDougall Printing Pty. Ltd., North Melbourne
Project Funded byVictorian Health Promotion Foundation




![Horse SA [Horse] Volunteers are Gold](https://static.fdocuments.net/doc/165x107/588b07f51a28abdf3b8b52f1/horse-sa-horse-volunteers-are-gold.jpg)