Histomorphometric analysis of the repair of a segmental diaphyseal defect with ceramic and titanium...
8
Journal of Orthopaedic Research 2439-446 The Journal of Bone and Joint Surgery, Inc 0 1994 Orthopaedic Research Society Histomorphometric Analysis of the Repair of a Segmental Diaphyseal Defect with Ceramic and Titanium Fibermetal Implants: Effects of Bone Marrow David Wolff, Victor M. Goldberg, and Sharon Stevenson Department of Orthopaedics, Case Western Reserve University, Cleveland, Ohio, U.S.A. Summary: We used a rat femoral diaphyseal defect/implant model to quantify the ingrowth of bone, cartilage, and fibrous connective tissue in a comparative study of woven sintered titanium fibermetal and porous hydroxyapatiteltricalcium phosphate ceramic implanted with and without the addition of syngeneic bone marrow cells. The patterns of tissue growth into the implants were analyzed with respect to time, type of implant, and the presence or absence of syngeneic marrow. Significantly more bone was found in ceramic implants than in fibermetal implants, with the addition of syngeneic marrow than without it, and at 4 months than at 2 months. Significantly more bone was found at both time periods in ceramic implants with bone marrow than in any other combination studied. We hypothesize that these findings resulted from interactions between the implanted material and its surroundings, specifically its ability to serve as a substratum for cell attachment, and cells in and around the defect, whether surgically implanted or arising from the soft-tissue bed. Large segmental defects in long bones, resulting from trauma or resection, are a common orthopae- dic problem. A variety of materials other than bone have been used to fill these defects; however, there is no consensus concerning the best material or com- bination of materials for this purpose. The ideal material should be crack-resistant and exhibit excel- lent fatigue characteristics, particularly under impact loads, it should have a compliance similar to that of bone (l), and it should be osteoconductive. Porous materials appear to offer the best potential for bone ingrowth and thus eventual overall strength. Galante and Rostoker (16) described the suitable porous prosthetic material as having pore channel continu- ity and pore diameters greater than 100 pm and as being inert in vivo, impact-resistant, and manufactur- able to precise dimensions. Candidate prosthetic ma- terials include porous ceramics and fibermetals. Received December 14,1992; accepted August 23,1993. Address correspondence and reprint requests to Dr. S. Ste- venson at Department of Orthopaedics, 2074 Abington Road, Cleveland, OH 44106, U.S.A. Sintered woven titanium fibermetal has been used in a variety of studies of segmental bone defects (1-4,24,25,28,29). Use of a pore volume of approx- imately 50% and a pore size of approximately 200 pm or larger has led to good results: adequate bone ingrowth and strength of the construct (1,24,29). Woven fibermetal has shown the ability to support bone ingrowth when stable fixation is achieved and grafts of optimum pore size and pore density are utilized (1). Woven fibermetal has the advantages of being strong in compression immediately postoper- atively and of being nonresorbable; however, its ca- pacity to remain inert after implantation over long periods of time has yet to be defined. Porous ceramics of tricalcium phosphate and hy- droxyapatite are available commercially and have been shown to be osteoconductive (27,30,32,34) and biocompatible (13,18,19,26,32), although there is controversy as to whether they are bioresorbable (8,19-22).They are wear-resistant and available with adequate pore sizes (greater than 100 pm [32]). Ce- ramics, especially tricalcium phosphates, appear to have tensile and compressive strength similar to, 439
-
Upload
david-wolff -
Category
Documents
-
view
216 -
download
3
Transcript of Histomorphometric analysis of the repair of a segmental diaphyseal defect with ceramic and titanium...

Journal of Orthopaedic Research 2439-446 The Journal of Bone and Joint Surgery, Inc 0 1994 Orthopaedic Research Society
Histomorphometric Analysis of the Repair of a Segmental Diaphyseal Defect with Ceramic and Titanium Fibermetal Implants: Effects of Bone Marrow
David Wolff, Victor M. Goldberg, and Sharon Stevenson
Department of Orthopaedics, Case Western Reserve University, Cleveland, Ohio, U.S.A.
Summary: We used a rat femoral diaphyseal defect/implant model to quantify the ingrowth of bone, cartilage, and fibrous connective tissue in a comparative study of woven sintered titanium fibermetal and porous hydroxyapatiteltricalcium phosphate ceramic implanted with and without the addition of syngeneic bone marrow cells. The patterns of tissue growth into the implants were analyzed with respect to time, type of implant, and the presence or absence of syngeneic marrow. Significantly more bone was found in ceramic implants than in fibermetal implants, with the addition of syngeneic marrow than without it, and at 4 months than at 2 months. Significantly more bone was found at both time periods in ceramic implants with bone marrow than in any other combination studied. We hypothesize that these findings resulted from interactions between the implanted material and its surroundings, specifically its ability to serve as a substratum for cell attachment, and cells in and around the defect, whether surgically implanted or arising from the soft-tissue bed.
Large segmental defects in long bones, resulting from trauma or resection, are a common orthopae- dic problem. A variety of materials other than bone have been used to fill these defects; however, there is no consensus concerning the best material or com- bination of materials for this purpose. The ideal material should be crack-resistant and exhibit excel- lent fatigue characteristics, particularly under impact loads, it should have a compliance similar to that of bone (l), and it should be osteoconductive. Porous materials appear to offer the best potential for bone ingrowth and thus eventual overall strength. Galante and Rostoker (16) described the suitable porous prosthetic material as having pore channel continu- ity and pore diameters greater than 100 pm and as being inert in vivo, impact-resistant, and manufactur- able to precise dimensions. Candidate prosthetic ma- terials include porous ceramics and fibermetals.
Received December 14,1992; accepted August 23,1993. Address correspondence and reprint requests to Dr. S. Ste-
venson at Department of Orthopaedics, 2074 Abington Road, Cleveland, OH 44106, U.S.A.
Sintered woven titanium fibermetal has been used in a variety of studies of segmental bone defects (1-4,24,25,28,29). Use of a pore volume of approx- imately 50% and a pore size of approximately 200 pm or larger has led to good results: adequate bone ingrowth and strength of the construct (1,24,29). Woven fibermetal has shown the ability to support bone ingrowth when stable fixation is achieved and grafts of optimum pore size and pore density are utilized (1). Woven fibermetal has the advantages of being strong in compression immediately postoper- atively and of being nonresorbable; however, its ca- pacity to remain inert after implantation over long periods of time has yet to be defined.
Porous ceramics of tricalcium phosphate and hy- droxyapatite are available commercially and have been shown to be osteoconductive (27,30,32,34) and biocompatible (13,18,19,26,32), although there is controversy as to whether they are bioresorbable (8,19-22). They are wear-resistant and available with adequate pore sizes (greater than 100 pm [32]). Ce- ramics, especially tricalcium phosphates, appear to have tensile and compressive strength similar to,
439

440 D. WOLFF ET AL.
but less than, that of cancellous bone (20); however, they are brittle and do not offer much resistance to impact forces (23) or rapid loading. Ceramics have been used as bone graft expanders with other ma- terials such as demineralized bone matrix (23) and have been used with (30,37) and without (18,19) bone marrow with some success in demonstrating adequate bone ingrowth and resultant composite strength.
Osteogenic precursor cells, which are capable of producing bone, have been demonstrated among the stromal and endosteal cells of bone marrow (15,35). The addition of autologous bone marrow to pros- thetic materials has been shown to result in a sub- stantial increase in the growth of bone into ceramics placed in subcutaneous or intramuscular sites (32,33) as well as in osseous defects (18,19,34,37,44). The enhancement of osteoinductivity of cortical or can- cellous bone grafts by the addition of bone marrow, probably by the provision of osteoprogenitor cells and undifferentiated target cells that may be influ- enced by bone inductive factors (4,7,27,39,40,43), is well established (27,34).
MATERIALS AND METHODS Experimental Design
Forty-eight male Fisher rats received implants. Independent variables included (a) the presence or absence of syngeneic bone marrow; (b) the type of implant used-woven sintered titanium fiberme- tal or porous 60/40 hydroxyapatiteltricalcium phos- phate ceramic; and (c) the time of observation-2 or 4 months postoperatively. All combinations were studied, yielding eight groups. The fibermetal im- plant was 5 mm in diameter and 8 mm long, with a 2.0 mm central canal and pore diameters of 200-450 pm (Zimmer, Warsaw, IN, U.S.A.). The ceramic im- plant was approximately 4 mm in diameter and 8 mm long, with a central canal of 1.5 mm and pore diam- eters of 250-400 pm (Zimmer).
Surgical Model A lateral approach was made to the femur, and the
muscles and periosteum were elevated. A small (23 x 5 x 5 mm) polyacetyl plate was fastened to the an- terolateral aspect of the femur with two threaded Kirschner wires and a cerclage wire in both the prox- imal and distal portions. A mid-diaphyseal8 mm seg- ment of the femur was removed and replaced with the implant, which was secured in place with another full cerclage wire. The muscles were apposed, and the fascia and skin were closed in routine fashion.
TABLE 1. Histomorphometric data
2 months 4 months No. Area No. Area
Bone Ceramic
With marrow Without marrow
With marrow Without marrow
Fibermetal
Cartilage Ceramic
With marrow Without marrow
With marrow Without marrow
Fibermetal
31.7 f 9.8" 5.3 f 2.1
9.8 f 1.9 6.5 f 2.6
1.7 f 0.3 2.9 f 1.7
0.4 f 0.2 3.0 f 1.7
40.0 f 7.6" 7.7 f 2.6
20.2 k 5.0b 14.7 k 6.4
0.1 ? O.lb
0.5 f 0.4
1.9 k 0.8 6.4 ?r 4.5
Fibrous connective tissue
Ceramic With marrow 6 66.7 f 10.0" 6 59.6 k 7.6' Without marrow 6 91.9 +_ 3.8 6 91.8 +_ 2.8
With marrow 5 89.8 f 2.0 4 77.9 k 5.7b Without marrow 5 90.1 & 3.7 6 77.4 f 10.0
Means of all cross sections from each segment expressed as % of available area (group mean +_ group SEM). Two animals died: one in the 2-month and one in the 4-month fibermetal with marrow groups; the other two specimens were lost.
'Different from all other groups at that time period (p < 0.05). Different from the corresponding 2-month value (p < 0.015).
'Less than ceramic without marrow at 4 months (p < 0.05).
Fibermetal
This model is similar to one previously described; however, the defect is larger (8 mm compared with 5 mm) (14). The animals were allowed full activity in cages postoperatively. They were killed at 2 or 4 months after surgery.
Bone Marrow Syngeneic bone marrow was harvested from fe-
murs of male rats by hydrostatic pressure with use of normal rat serum. Bone marrow cells were dis- persed by multiple passages through a 20-gauge nee- dle, and the cell suspension was mixed with a half volume of bovine collagen solution (Vitrogen 100; Collagen Corporation, Palo Alto, CA, U.S.A.). The implants were immersed in this suspension and were implanted following gelation; approximately 7.5 x lo6 cells were implanted with each implant. Previous studies have shown that cell viability is greater than 90% with these procedures (33).
Histomorphometric Analysis Following fixation in cold 40% ethanol, the speci-
mens were dehydrated, cleared, and embedded in
J Orthop Res, Vol. 12, No. 3, 1994

441 HIS TOM 0 R PH 0 METRIC A NA LYSIS 0 F IMPLANTS
methylmethacrylate. Cross sections of the implant were cut with a water-cooled diamond saw. The sec- tions were mounted on opalescent 2 mm thick plastic blocks, with the order of the sections noted from proximal to distal, which then were ground to 100 pm, polished, and surface-stained with toluidine blue by the method of Schenk et al. (38). Five or six sec- tions of the fibermetal implants and three to six sec- tions of the ceramic implants were analyzed per implant. With use of the Bioquant IV system (R and M Biometrics, Nashville, TN, U.S.A.), total cross- sectional areas of bone, cartilage, and fibrous con- nective tissue were measured for each section. The template utilized was a circle with a radius 2 pm larger than the radius of the implant being measured, and values were expressed as a percentage of the total area of this circle that was available for in- growth: A (available) = A (circle) - A (implant ma- terial). Areas of tissue ingrowth measured from the sections were averaged to give location data for proximal (sections 1 and 2), middle (sections 3 and 4), and distal (sections 5 and 6) grafts. Averages of all cross sections from each segment also were cal- culated for each dependent variable when location was not considered as an independent variable.
Statistical Analysis There were three dependent variables (percent-
age of cross-sectional area of bone, cartilage, and fibrous connective tissue) and three or four inde- pendent variables, dependent on whether or not lo-
cation was considered as a variable. The independent variables were implant type, presence or absence of syngeneic bone marrow cells, time of observation, and-in certain analyses-location (proximal, mid- dle, or distal). The mean and SD of the dependent variable values were calculated for each of the eight groups. The data were analyzed by one-way, two-way, and three-way analysis of variance and independent t tests with use of SPSS (Chicago, IL, U.S.A.) and PC Statistician (Human System Dynamics, Northridge, CA, U.S.A.) software. The Newman-Keuls test was used as the post hoc test. When multiple t tests were done, the Bonferroni t test was used.
RESULTS The means and variance for each experimental
group are presented in Table 1. When analyses of variance were performed to determine the influence of individual independent variables on the data set, several trends became evident. For example, signif- icantly more bone was found in ceramic implants (21.2%) than in fibermetal implants (12.8%), with syngeneic bone marrow cells (26.7%) than without marrow cells (8.7%), and at 4 months (21.3%) than at 2 months (13.7%) (p < 0.001). There was an im- portant two-way interaction between type of implant and presence or absence of bone marrow (p < 0.001): significantly more bone was present in ceramic im- plants with marrow than in ceramic implants without marrow or in fibermetal implants with or without marrow at both 2 and 4 months. Although there con-
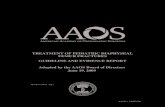
Percent
505
301
" proximal middle
Location
distal
-FBM+BM
-- FBM
'CM+BM
CM
FIG. 1. The amount of bone present, expressed as a percentage of available space (mean 5 SEM), is graphically illustrated. The data are plotted against location within the segment: proximal 2.5 mm, middle 2.5 mm, and distal 2.5 mm. These data pool 2 and 4-month observations (N = minimum of 8, maximum of 12) and illustrate the abundance of bone in ceramic implants with bone marrow compared with other groups. FBM = fibermetal, BM = bone marrow, and CM = ceramic. *Significantly higher than all other groups (p < 0.05) and **significantly higher than all other groups (p < 0.01).
J Orthop Res, Vol. 12, No. 3, 1994

442 D. WOLFF ET AL.
(p < 0.021). Overall, cartilaginous area significantly increased in the fibermetal implants from 2 months (1.67%) to 4 months (4.46%) and significantly de- creased in the ceramic implants over the same period (2 months, 2.30%; 4 months, 0.33%) (p < 0.014). These trends also were evident in comparisons of individual groups (Table 1).
The area of fibrous connective tissue varied in-
FIG. 2. Lamellar bone is present throughout this middle cross section from a ceramic implant with bone marrow at 4 months after surgery. Bone is present in the central canal, within pores, and peripherally (arrows). Toluidine blue stain, 100 pm section, original magnification ~14.
FIG. 4. The bone (arrows) that formed in and around fibermetal implants was predominantly woven at 2 months after surgery. Note its distance from the surface of the fibers on this proximal cross section. Toluidine blue stain, 100 Frn section, original magnification x17.5.
FIG. 3. When ceramic implants were inserted without bone marrow, very little bone formed on and around them. This middle cross section at 2 months demonstrated only a little peripheral bone (white arrow). The implant region has been revascularized, as evidenced by loose connective tissue in the central canal (black arrow). Toluidine blue stain, 100 pm sec- tion, original magnification x14.
sistently was less bone in the middle section of im- plants than in the proximal or distal section, the dif- ference was not significant. However, bone was distributed more uniformly throughout ceramic im- plants to which marrow had been added than in any other experimental group (Fig. 1).
when imp1ants were placed without marrow (3*11'0) than when they were placed with marrow (0.99%)
FIG. 5. Only one island of bone (arrow) is present 2 months after surgery on this middle cross section from a fibermetal
are vessels perfused with India ink. It is evident that these implants have been well revascularized. Toluidine blue stain, 100 pm section, original magnification x17.5.
m e area of cartilage was significantly greater implant without bone marrow. The small, tortuous structures
J Orthop Res, Vol. 12, No. 3, 1994

H I S T O M O R P H O M E T R I C A N A L Y S I S OF I M P L A N T S 443
A
B
FIG. 6. A: At 4 months, woven and lamellar bone were intimately apposed to the surface of the ceramic implant. In certain areas, an admixture of bone and ceramic was noted (arrow). B: Bone was formed at some distance from the surface of the titanium fiber- metal. The intervening space was filled with loose fibrous connective tissue and vessels. Toluidine blue stain, 100 pm section, original magnification x56.
versely with the area of bone: there was significantly more fibrous connective tissue in fibermetal im- plants (84.16%) than in ceramic implants (77.49%), in implants without marrow (88.19%) than in those with marrow (72.31%), and at 2 months (84.3%) than at 4 months (76.5%). Ceramic implants with marrow contained significantly less fibrous connec- tive tissue than ceramic implants without marrow or fibermetal implants with or without marrow at 2 months- and contained significantly less fibrous con-
nective tissue than ceramic implants without marrow at 4 months (Table 1).
Histologically, ceramic implants with bone mar- row were characterized by abundant formation of lamellar new bone directly on the ceramic surface throughout the cross section of the implant (Fig. 2). When marrow was omitted, scanty peripheral forma- tion of new bone occurred directly on the surface of the ceramic. The interstices of the implant were well vascularized and were filled with loose areolar con-
J Orthop Res, Voi. 12, No. 3, 1994

444 D. WOLFF ET AL.
nective tissue (Fig. 3). Woven bone was formed in the interstices of, and at some distance from the surface of, fibermetal implants with bone marrow (Fig. 4). At 2 months, the bone in fibermetal implants with bone marrow was more often woven than lamellar, but by 4 months lamellar bone predominated in these implants. Although well vascularized, fibermetal im- plants without bone marrow contained very little bone. The bone was woven and at some distance from the surface of the implant (Fig. 5). Woven and lamellar bone formed directly on the surface of ce- ramic implants. In addition, fragments of ceramic were observed to be completely surrounded by bone. Islands of woven bone first formed in the interstices of fibermetal implants. Although subsequent lamel- lar bone formed on the surface of these bone islands, bone did not approach close to the surface of the fibermetal implants, and a space filled with fibrous connective tissue and vessels always persisted be- tween the bone and the fibermetal (Fig. 6).
DISCUSSION Our data demonstrate the multifactorial determi-
nants of the repair of a segmental defect with two clinically used materials. In this study, we controlled for the effects of construct stability and properties of the soft-tissue bed by standardizing the surgical ap- proach and size of the defect in healthy animals and by providing stable internal fixation, thus isolating the variables of time, type of implant, and presence or absence of bone marrow. Not only did the type of implant and the presence or absence of bone marrow affect bone ingrowth and repair of the defect, but there was a significant interaction between these variables. We also saw significant changes in most dependent variables with time, illustrative of the pro- gressive nature of segmental defect filling.
The characteristics of an implant material that have been reported to affect bone ingrowth include material (type of ceramic or metal), pore size, por- osity, and surface characteristics (hydrophobic or hydrophilic) (1,6,11-13,22,29,33). Our results with ti- tanium fibermetal are consistent with those of others (36,41,42): relatively sparse, initially woven bone formed at some distance from the titanium fiberme- tal, although lamellar bone may develop and isolated areas of direct bone-metal apposition may be seen (18,29). By contrast, lamellar bone was formed di- rectly on the surface of ceramic implants; this also is consistent with the findings of others (9,10,31,41). The porosity and pore size of the two implants that we studied were similar, but the surface properties
were different. Calcium-containing crystal surfaces such as ceramic have been shown to leach calcium and to bind fibronectin in a biologically active con- figuration (5 ) . Osteoblasts anchor, attach, spread, and proliferate on such a surface in vitro (5). How- ever, implant properties alone do not determine bone ingrowth. The source and quantity of bone- forming cells are additional important determinants of the process.
Bone formation in a segmental defect is a complex process that may originate from surgically implanted cells, from adjacent bone-forming cells at the host- implant interface, or from cells of the soft-tissue bed that are induced to become bone-forming cells. Cells of the soft-tissue bed may be induced to become bone-forming cells by bioactive proteins in the im- plant, such as in demineralized matrix, or by bioac- tive proteins synthesized and released by cells in the defect. In this study, little bone was present in fiber- metal or ceramic implants that were placed without marrow; this suggests that neither type was inher- ently osteoinductive. Others have made the same observations (30,36). Slightly more bone was present in the proximal and distal regions than in the central region of those implants; this may reflect the contri- butions of cells originating from the host-implant interfaces. The addition of whole, unfractionated marrow significantly enhanced growth of bone into ceramic implants but not into fibermetal implants. A recent study has indicated that potentially bone- forming cells require an osteophilic substrate if they are to attach, proliferate, and differentiate (5). In this study, the titanium fibermetal did not appear to be a suitable substrate for the adhesion and differen- tiation of marrow cells. By comparison, abundant bone formed in ceramic implants when bone marrow was used. Calcium phosphate ceramics have been shown to be suitable substrates for the attachment and proliferation of bone cells (5,36). The relative contributions to the reparative bone mass of cells originating from the implanted marrow and their progeny and of cells originating from the soft-tissue bed that were induced to become bone-forming cells cannot be determined from our data. It has been shown in previous experiments that the early bone formation is predominantly by cells originating from marrow while later bone formation is by an admix- ture of cells from marrow and the host soft-tissue bed (17).
The quantity of fibrous connective tissue in the implants was inversely proportional to the quantity of bone in the implant. It is interesting to note that,
J Orrhop Res, Vol. 12, No. 3, 1994

445 HISTOMORPHOMETRIC ANALYSIS OF IMPLANTS
although small in absolute volume, more cartilage was present in fibermetal implants without marrow than with marrow. In addition, over time, cartilage mass decreased in ceramic implants and increased in fibermetal implants. The signals or stimuli that may have permitted or enhanced formation of cartilage in these implants are unknown.
The parameters of the repair tissue measured in this study changed significantly over time. These ob- servations emphasize the necessity of multiple, se- quential observations to identify the direction and rate of the complex processes that repair diaphyseal defects. With the exception of ceramic implants with- out marrow, all implants in our study were still gain- ing bone mass at 4 months; this suggests the need for long-term observations in studies of the repair of large skeletal defects.
In conclusion, significantly more bone had formed in ceramic implants than in fibermetal implants, with bone marrow than without bone marrow, and at 4 months than at 2 months. The composite of ceramic implant and bone marrow resulted in significantly more bone, at both time periods, than any other com- bination. We hypothesize that these findings result from interactions between the implanted material and its surroundings, specifically its ability to serve as a substrate for cell attachment, and between the implanted material and cells in and around the de- fect, whether surgically implanted or arising from the soft-tissue bed.
Acknowledgment: The implants used in this project were supplied by Zimmer Corporation. The authors wish to acknowledge the expert technical assistance of E. Man- ning and D. Zart. The study was supported in part by funds from the National Institutes of Health.
REFERENCES 1. Andersson GBJ, Gaechter A, Galante JO, Rostoker W Seg-
mental replacement of long bones in baboons using a fiber titanium implant. J Bone Joint Surg [AmJ 6031-40,1978
2. Andersson GBJ, Galante JO, Rostoker W Segmental re- placement of the femur in baboons: comparison of fixation through bone ingrowth with and without methylmethacry- late. Arch Orrhop Trauma Surg 99:47-51,1981
3. Andersson GBJ, Lereim P, Galante JO, Rostoker W. Seg- mental replacement of the femur in baboons with fiber metal implants and autologous bone grafts of different par- tide size. Acra Orthop Scand 53:349-354,1982
4. Aspenberg P, Wittbjer J, Thorngren K-G: Pulverized bone matrix as an injectable bone graft in rabbit radius defects. Clin Orfhop 206:261-269,1986
5. Bagambisa FB, Joos U: Preliminary studies on the phenom- enological behaviour of osteoblasts cultured on hydroxy- apatite ceramics. Biomuferinls 1150-56,1990
6. Bobyn JD, Pilliar RM, Cameron HU, Weatherly GC: The optimum pore size for the fixation of porous-surfaced met-
al implants by the ingrowth of bone. Clin Orrhop 150:263- 270,1980
7. Burwell RG: Studies in the transplantation of bone. VII: The fresh composite homograft-autograft of cancellous bone: an analysis of factors leading to osteogenesis in mar- row transplants and in marrow-containing bone grafts. J Bone Joint Surg [Br] 46:llO-140,1964
8. Cameron HU, Macnab I, Pilliar RM. Evaluation of a biode- gradable ceramic. J Biomed Mater Res 11:179-186,1977
9. Daculsi G, Passuti N, Martin S, Deudon C, Legeros RZ, Raher S: Macroporous calcium phosphate ceramic for long bone surgery in humans and dogs: clinical and histological study. J Biomed Mater Res 24:379-396,1990
10. De Lange GL, De Putter C, De Wijs FLJA: Histological and ultrastructural appearance of the hydroxyapatite-bone in- terface. J Biomed Mater Res 24:829-845,1990
11. Deporter DA, Komori N, Howley TP, Shiga A, Ghent A, Hansel F', Parisien K: Reconstituted bovine skin collagen enhances healing of bone wounds in the rat calvaria. Calcif Tissue Int 42:321-325,1988
12. Ducheyne P, Beight J, Cuckler J, Evans B, Radin S: Effect of calcium phosphate coating characteristics on early post- operative bone tissue ingrowth. Biomaferials 11:531-540, 1990
13. Dutton RO, Dawson EG, Ackerman D, Dickstein H L Pre- liminary observations in segmental femoral substitution with porous hvdroxvapatite implants in the dog. Orthou _ . Transm5:267, 1981
I
14. Einhorn TA. Lane JM. Burstein AH. Kouman CR. Vieorita VJ: The healing of segmental bone defe'cts induced b; de- mineralized bone matrix: a radiographic and biomechanical study. J Bone Joint Surg [Am] 66:274-279,1984
15. Freidenstein AJ: Precursor cells of mechanocytes. Znr Rev
16. Galante J, Rostoker W Fiber metal composites in the fixa- tion of skeletal prosthesis. J Biomed Muter Res 4:43-61,1973
17. Goshima J, Goldberg VM, Caplan AI: The origin of bone formed in composite grafts of porous calcium phosphate ceramic loaded with marrow cells. Clin Orrhop 269274-283, 1991
18. Grundel RE, Chapman MW, Yee T The evaluation of a biphasic calcium phosphate ceramic in diaphyseal defects in the canine ulna and metaphyseal defects in the canine hu- merus. Trans Orrhop Res SOC 12:218,1987
19. Grundel RE, Chapman MW, Yee T, Moore DC: Autogeneic bone marrow and porous biphasic calcium phosphate ce- ramic for segmental bone defects in the canine ulna. Clin Orrhop 266:244-258,1991
20. Hollinger JO, Battistone GC: Biodegradable bone repair materials: synthetic polymers and ceramics. Clin Orthop
21. Holmes RE: Bone regeneration within a coralline hydroxy- apatite implant. Plasr Reconst Surg 63:626-633.1979
22. Holmes RE, Bucholz RW, Mooney V: Porous hydroxyapa- tite as a bone graft substitute in diaphyseal defects: a histo- morphometric study. J Orthop Res 5:114-121,1987
23, Hopp SG, Dahners LE, Gilbert JA: A study of the mechan- ical strength of long bone defects treated with various bone autograft substitutes: an experimental investigation in the rabbit. J Orrhop Res 7519-584,1989
24. Hulbert SF, Klawitter JJ, Talbert CD, Fitts C T Materials of construction for artificial bone segments. In: Research in Dental and Medical Materials, p 43. Ed by E Korostoff. New York, Plenum Press, 1969
25. Jasty M, McGann W, Rubash HE, Paiement G, Bragdon C, Harris WH: Comparison of bone ingrowth into cobalt chrome spheres vs. titanium fiber mesh coating on canine cementless acetabular components. Truns Orrhop Res SOC 12:433,1987
26. Kato K, Aoki H, Tabata T, Ogiso M: Biocompatibility of
CytOl47:327-359,1976
207~290-305,1986
J Orthop Res, Vol. 12, No. 3, 1994

446 D. WOLFF ET AL.
apatite ceramics in mandibles. Biomater Med Devices Artif Organs 7:291-297,1979
27. Klein L, Zika JM, Davy DT, Stevenson S, Goldberg VM. Fresh and frozen syngeneic femur grafts with and without bone marrow: effect on morphology, metabolic turnover, and bone mass in grafts from prelabeled rats. Trans Orthop Res Soc 12:92,1987
28. Kuo KN, Gitelis S, Sim FH, Pritchard D, Chao E, Rostoker W, Galante JO, McDonald P: Segmental replacement of long bones using titanium fiber metal composite following tumor resection. Clin Orthop 176:108-114,1983
29. Lembert E, Galante J, Rostoker W Fixation of skeletal replacement by fiber metal composites. CIin Orthop 87:303- 310,1972
30. Moore DC, Chapman MW, Manske D: The evaluation of a biphasic calcium phosphate ceramic for use in grafting long-bone diaphyseal defects. J Orthop Res 5:356-365,1987
31. Muller-Mai CM, Voigt C, Gross U: Incorporation and deg- radation of hydroxyapatite implants of different surface roughness and surface structure in bone. Scanning Microsc
32. Nade S, Armstrong L, McCartney E, Ceram FI, Baggaley B: Osteogenesis after bone and bone marrow transplantation: the ability of ceramic materials to sustain osteogenesis from transplanted bone marrow cells: preliminary studies. Clin Orthop 181:255-263,1983
33. Ohgushi H, Goldberg VM, Caplan AI: Heterotopic osteo- genesis in porous ceramics induced by marrow cells. J Or- thop Res 7568-578,1989
34. Ohgushi H, Goldberg VM, Caplan AI: Repair of bone de- fects with marrow cells and porous ceramic: experiments in rats. Acta Orthop Scand 60:334-339,1989
35. Owen M: Lineage of osteogenic cells and their relationship to the stromal system. In: Bone and Mineral Research. Vol
4:613-624,1990
3, pp 1-25. Ed by WA Peck. Amsterdam, Elsevier, 1985 36. Rivero DP, Fox J, Skipor AK, Urban RM, Galante JO: Cal-
cium phosphate-coated porous titanium implants for en- hanced skeletal fixation. J Biomed Mater Res 22:191-201, 1988
37. Sandhu HS, Lane JM, Dowling C, Burstein A, Piez K, Kin- caid S: Calcium phosphate ceramic supplementation of col- lagen and marrow composite bone graft. Trans Orthop Res SOC 12:93,1987
38. Schenk RK, Olah AJ, Herrmann W Preparation of calcified tissue for light microscopy. In: Methods of Calcified Tissue Preparation, pp 1-56. Ed by GR Dickson. Amsterdam, El- sevier, 1984
39. Simmons DJ, Ellsasser JC, Cummins H, Lesker P: The bone inductive potential of a composite bone allograft-marrow autograft in rabbits. Clin Orthop 97:237-247,1973
40. Simmons DJ, Lesker PA, Ellsasser JC: Survival of osteo- competent marrow cells in vitro and the effect of PHA- stimulation on osteoinduction in composite bone grafts. Proc SOC Exp Biol Med 148:986-990,1975
41. Spivak JM, Ricci JL, Blumenthal NC, Alexander H: A new canine model to evaluate the biological response of in- tramedullary bone to implant materials and surfaces. J Bio- med Mater Res 24:1121-1149,1990
42. Stephenson PK, Freeman MAR, Revel1 PA, Germain J, Tuke M, Pirie CJ: The effect of hydroxyapatite coating on ingrowth of bone into cavities in an implant. JArthroplasty
43. Takagi K, Urist MR: The role of bone marrow in bone morphogenetic protein-induced repair of femoral massive diaphyseal defects. Clin Orthop 171:224-231,1982
44. Uchida A, Nade S, McCartney E, Ching W Bone ingrowth into three different porous ceramics implanted into the tibia of rats and rabbits. J Orthop Res 3:65-77,1985
6~51-58,1991
J Orthop Res, Vol. 12, No. 3, 1994