


High risk pregnancy4
52
Detecting High Risk Pregnancy Dr. Varsha L. Deshmukh Assoc. Prof & Unit Incharge Govt. Medical College, AURANGABAD
-
Upload
varsha-deshmukh -
Category
Documents
-
view
29 -
download
0
Transcript of High risk pregnancy4

Detecting High Risk Pregnancy
Dr. Varsha L. DeshmukhAssoc. Prof & Unit Incharge
Govt. Medical College,
AURANGABAD

Introduction
• Pregnancy including labour & delivery is itself a high risk event.
• The aim of risk assessment is to identify the factors that may constitute greater than average risk to a pregnancy.
• This permits the prediction of potential adverse pregnancy outcomes & enables the process of selecting women who may benefit from extra researches.

Receiving quality antenatal, intranatal & postnatal services
is one of the reproductive rights of women

Introduction
• It is impossible for the process of risk assessment to predict every perinatal event.
• WHO recommends that a risk assessment approach be used in the mgt. of maternal, fetal health care.
• It also suggest arrangement for delivery at tertiary care center for high risk obst. pts.
.

Aim
• To identify women with maternal complications & obst. risk factors.

Why to Identify or Detect Women with High Risk Factors

• It will reduce the number of cases brought in a state of emergency when t/t is most difficult & least effective.
• If t/t is started in time, it is possible to save life of both mother & baby.
• Timely referral after appropriate medication is important improving the prognosis.


Maternal Mortality
Major causes of maternal mortality are • PIH• Eclampsia• APH• PPH• Puerperal sepsis• Obstructed labour• Unsafe abortions

Maternal mortality is a gender issue & speaks about the status of women
in the society.
Maternal mortality is an equity issue as maximum maternal death are reported from people living below poverty line from under privilege
community

Except for hemorrhage other causes of maternal mortality can be identified &
treated effectively, thus maternal mortality can be greatly reduced.

Obstetric Emergencies
The obst. emergencies are life threatening • Fatality rate is more• Difficult to treat• Surgery rate is increased• BT rate is increased• Hospitalization prolonged• Morbidity more

Cost Effectiveness
• Early diagnosis leads to less emergencies hence less drug requirement & less morbidity
• Thus the risk assessment system along with timely referral is highly cost effective.

What to Do ?
1. Early diagnosis
2. Community awareness about antenatal care
3. Early initiation of appropriate therapy
4. T/t plan stream lining
5. Early identification
6. Timely referral

What to Tell ?
Every clinic must emphasize the following
1. ANC it is essential need
2. Eat more
3. Rest more
4. Get immunized (Inj TT)
5. Take Tab. FS
6. Hospital delivery

Ante-natal care
• Periodic check-ups
• Risk factors identified on time
• Treatment started early
• Hospital delivery
• Maternal complications diagnosed early
• Maternal & fetal mortality less
Early Registration
• Early – before 12 wks (preferably)
• Before 20 wks
• At 32 wks
• At 36 wks
• Encourage to visit more often in 3rd trimester
ANC
• Careful history
• Physical examination
• Pregnancy progressing normally
• Complications if occurs diagnosed early
• Timely referral
• Institutional delivery

History• LMP/EDD• Age of the patient < 18 yrs. > 35
yrs.• Order of pregnancy primigravida or
grand multi.• Interval of < 2 yrs since last
pregnancy• H/o cardiac disease, diabetes,
chronic hypertension

Past Obst. History
• Parity • H/o still birth• IUFD• BOH• Preterm labour• Macrosomic baby• IUGR baby• Sev. PIH

Life Threatening Situations
• H/o PPH• H/o APH• H/o MRP• H/o Eclampsia/HELLP• H/o Other complications
associated with pregnancy which were life threatening

Complaints• Breathlessness• Excessive tiredness• Palpitation• Puffiness of face• Headache• Blurring of vision• Bleeding p/v• Leaking p/v• Pain in abdomen

Physical Examination
• Maternal weight
• Maternal height < 140 cm
• Look for pallor, puffiness of face, oedema of feet.
• Blood pressure 120/80 mmHg > 140/90 mmHg after 20 wks. S/o PIH
Abdominal Examination
• Abdominal examination is done to monitor the progress of pregnancy, fetal growth, fetal lie and fetal presentation.
• Height of uterus 12 wks just palpable
24 wks at umbilicus
36 wks at xiphisternum
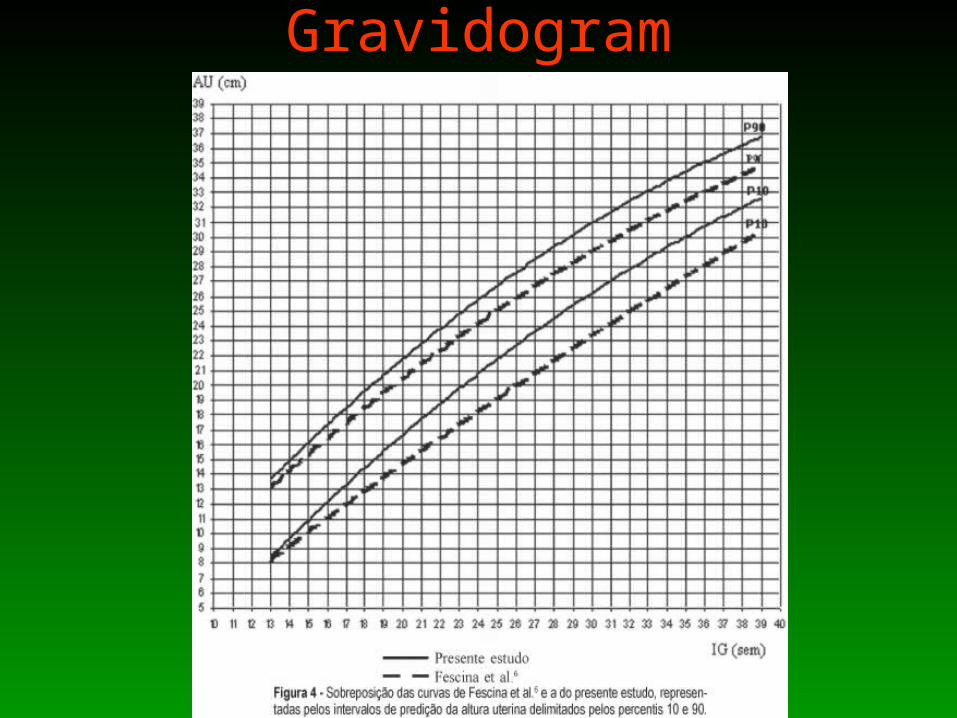
Gravidogram
Fetal Lie
• Vertical
• Transverse
• Oblique

Fetal Presentation
• Vertex
• Breech
• Shoulder
• Cord
• Hand• Compound
FHS• Normal 120-160 b.p.m.
• Fetal tachycardia > 160 b.p.m.
• Fetal bradycardia < 120 b.p.m.
• Loss of fetal movement
• Passage of meconium
• All suggestive of fetal distress

Advise to Mothers
• Food and rest

Advise to Mother
• Anaemia prophylaxis
• Tab. FS + FA 100 mg 1OD x 3 mths.
• S/o anemia present - Tab. FS + FA 100 mg one B.D. x 3 mths.
• Tab. Mebendazol 1 B.D. x 3 days.
• Dietary advise
Advise to Mother
• TT immunization
• Preparation for labour
Laboratory Test
• Anemia (Hb < 10 gm%)
• Rh –ve blood group
• Blood sugars
• HIV
• Hepatitis B
• Urine microscopy

Current Pregnancy Status
• Multiple gestation• Vaginal bleeding• Decreased fetal movements• Preterm labour or cervical change• PIH• Abnormal uterine size (IUGR/V mole)• Abnormal amniotic fluid volume• Postdatism

Low Risk Labour
• Spontaneous onset at 37 to 40 wks
• Single fetus with vertex presentation
• Estimated fetal weight average
• Normal vital signs
• No pregnancy complications
• No abnormal intrapartum bleeding

Normal Low Risk Labour
• Acceptable rate of cervical dilatation
• FHS normal
• Head engaged at full dilatation
• Normal delivery within 2 hrs of good expulsive force
• Third stage < 30 min
• Total blood loss < 500 ml

High Risk Labour
• Abnormal FHS
• Meconium stained liquor
• Malpresentation
• Intrapartum hemorrhage
• PROM
• Instrumental delivery
• PIH
High Risk Labour
• Multiple pregnancy• Cord prolapse• Fetal macrosomia• Dysfunctional labour• Previous LSCS• Prolonged labour• CPD• Rupture uterus• Chorioamniotis
Labour
5 Cs• Clean hands
• Clean surface
• Clean razor
• Clean cord tie
• Clean cord stump

Partogram

Partogram
• Cervical dilatation
• Descent of head
• Uterine contractions
• Drugs given
• Fetal heart rate record

Partogram
• Concept of alert line
• Concept of action line
• Assessment of maternal condition
• Assessment of fetal condition
• Timely referral

Each and every one working in the health department is committed to reduce the maternal mortality and to
realize the reproductive rights of a women.

Obst. Emergencies
• ANC• Anemia• PIH• Eclampsia• Placenta previa• Abruptio placenta• PPH• Retained placenta• Malpresentations • Obstructed & prolonged labour• Rupture uterus

Referral Obst. Emergencies
• Position of the patient• Left lateral position• Mouth gag• Start IV fluid – ringer lactate• First dose of broad spectrum antibiotics• Other specific medication as indicated e.g. inj.
MgSo4 in eclampsia• Breast feeding to be continued during transfer
in cases of PPH

Referral Note• Should mention salient
points about the history
• Main clinical findings • Medications (dose,
route, time of administration)
• If telephonic facility is available should alert the referral hospital

Advise to Family Members
• About high risk situation
• About blood donation
• About financial aspects
• Blood donors
• Senior members for consent

Referral• Should be transported by the quickest
mode of transport
• 3 delays

Through a team approach all of the skills of the health care members involved can be combined to provide the best possible approach to meet the pregnancy’s need. The role of patient education can not be
over emphasized. Incorporating the mother as an active member in her health
care is an investment in time and effort that is cost effective both during
pregnancy and labour.
A systematic & a well begun programme with a positive thinking will definitely show road to success
to accept this challenge



















