High Risk Lymphoma
41
Upfront Auto PBSCT v/s Novel Therapies ,High Grade NHL- Bangkok,31 st August 2014 Dr. S. J. Apte, MD FRCPA Consultant Haematologist, Sahyadri Speciality Hospital, Pune
-
Upload
spa718 -
Category
Health & Medicine
-
view
1.058 -
download
2
Transcript of High Risk Lymphoma

Upfront Auto PBSCT v/s Novel Therapies ,High Grade NHL-Bangkok,31st August 2014
Dr. S. J. Apte, MD FRCPAConsultant Haematologist,
Sahyadri Speciality Hospital, Pune

UPFRONT AUTOTRANSPLANTATION IN AGGRESSIVE LYMPHOMA
Not in 2014

Lessons from History-
• Rituximab was the first major breakthrough in the treatment of NHL and not the Auto SCT

Tran
spla
nts
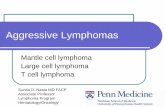
Transplant Activity Worldwide1968-2012

Indications for Hematopoietic Stem Indications for Hematopoietic Stem Cell Transplants in the U.S.Cell Transplants in the U.S.
Num
ber o
f Tra
nspl
ants
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
5,000
5,500
MultipleMyeloma
NHL AML HD ALL MDS/MPD AplasticAnemia
CML OtherLeuk
Non-Malig
Disease
OtherCancer
Allogeneic (Total N=7,012)Autologous (Total N=9,778)

HOW TO DEFINE AGGRESSIVE LYMPHOMA?

Yrs
OS
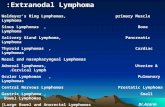
Diffuse Large B-Cell Lymphoma
DLBCL Subgroup 5-Yr OS, %Primary Mediastinal 64Germinal Center B cell like (GCB) 59
Activated B cell (ABC) 30
1.0
0.8
0.6
0.4
0.2
00 2 4 6 8 10
Rosenwald A, et al. J Exp Med. 2003;198:851-862.
Survival by Gene Expression Profiling: DLBCL

Prognosis By Interim PET Scanning
- Mixed results seen in 4 studies- 2 studies confirm predictive value, 2 studies did not
Safar et al, J Clin Oncol 2012;30:184
0
20
40
60
80
100
0 20 40 60 80 100Time (months)
PET positive (n=12)
P=0.02
PET negative (n=73)
Progression Free Survivaln= 98
0
0.2
0.4
0.6
0.8
1.0
0 1 3 5 6 7Time (years)
PET Positive
P=0.146
PET Negative
2 4
Moskowicz et al. J Clin Oncol 2010;11: 1896
Progression Free Survivaln= 112

5Yrs
P < .001
1.00.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 1 2 3 4
Sehn LH, et al. Blood. 2007;109:1857
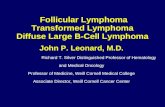
Legend Revised IPI Risk Group
IPI Factors, n
Very good 0
Good 1, 2
Poor 3, 4, 5
• Age >60• Perf Status• Stage 3-4• LDH•Extranodal
Overall Survival According to Revised International Prognostic Index

J Clin Oncol 28:2373-2380.; 2010
Standard International Prognostic Index Remains a Valid Predictor of Outcome
for Patients With Aggressive CD20+ B-Cell Lymphoma in the Rituximab Era

SO, THIS DEBATE IS ALL ABOUT A SMALL PERCENTAGE OF PATIENTS WHO ARE NON RESPONSIVE TO CHEMO IN ‘R’ ERA.

High Risk DiffuseLarge Cell Lymphoma
Autologous HSCT in First CR/PR

J Natl Cancer Inst 2001;93:22–30

J Natl Cancer Inst 2001;93:22–30NO ADVANTAGE OF HDT IN CR 1 / PR 1

J Clin Oncol 21:1255-1262.; 2003
NO ADVANTAGE OF HDT IN CR 1 / PR 1

British Journal of Haematology, 149, 237–243, 2010
NO ADVANTAGE OF HDT IN CR 1 / PR 1

WILL THIS HOLD GOOD IN RITUXIMAB ERA IS THE QUESTION?????

Lancet Oncol 2011; 12: 1013–22

Lancet 2011; 378: 1858–67

High Risk Diffuse Large B Cell NHL:Frontline Autologous HCT
Phase II Trials containing rituximab
Group n aaIPI >2 Therapy CR
RatePFS/EFS OS Follow
upTarella2007 112 100 Mod R-HDS 80 73 76 4 yrs
Vitolo2009 97 100 R-mega CEOP x
BEAM/HCT 82 73 80 4 yrs
Dilhudy2010 42 100 R CEEP BEAM
HCT 55 55 74 5 yrs
Fitoussi2011 209 100 R-ACVBP +
BEAM/HCT 60 76 78 4 yrs

Only patients with two or three risk factors (Ann Arbor stage III or IV, elevated lactate
dehydrogenase, Eastern Cooperative Oncology Group [ECOG] performance status 2 or
3) of the age-adjusted IPI were eligible Lancet Oncol 2012; 13: 1250–59

Lancet Oncol 2012; 13: 1250–59

Lancet Oncol 2012; 13: 1250–59

Lancet Oncol 2012; 13: 1250–59
NO ADVANTAGE OF HDT IN CR 1 / PR 1

First-line rituximab (R) high-dose therapy (R-HDT) versus R-CHOP14 for young adults with diffuse large B-cell lymphoma: Preliminary results of the GOELAMS 075 prospective multicenter randomized trial.
Results: 340 pts included 01/2005 to 06/2010, 286 pts evaluable at time of abstract, 143 in each arm. Characteristics of the pts in the 2 arms are super imposable. Overall 56% bulk, 72% >2 AA stage and 58% aa IPI>1. The Rdz tx was completed in 67% in the R-CHOP arm and 53% in the R-HDT arm. The interm evaluation showed the same rate of response with CT scan (CR + CRu: 65% and 62% following 4 x R-CHOP14 and first 3 courses of R-HDT). PET remained more often pos after the first 3 courses of R-HDT (41% vs 28%; p=0.03). Of the 98 pts with pos interm PET, 84 had a salvage of which 62 underwent auto PBSCT. On ITT the ORR (CR + Cru) was 82% and 76% in the R-CHOP and R-HDT arms respectively (p=0.8). With a med FU of 25 m, the 3y OS is 83%. No difference according to the tx arm in any of the aaIPI strata. The 3y PFS and DFS are 76% and 83%, no difference according to the tx arm. The 3 y OS and DFS for pts in R-CHOP arm and in R-HDT arm acc to interm PET are shown in the table. Conclusions: R-CHOP14 is as efficient, less toxic, and spares resources as compared to this R-HDT program. Salvage based on interm PET is not harmful and provides excellent results.
PET neg PET pos
R-CHOP 3y OS/DFS 88% / 80% 84% / 82%R-HDT 3y OS/DFS 80% /92% 86% / 89%
J Clin Oncol 29: 2011 (suppl; abstr 8003)

Ann Oncol 2011;22(Suppl 4):072.

Randomized phase III U.S./Canadian intergroup trial (SWOG S9704) comparing CHOP ± R for eight cycles to CHOP ± R for six cycles followed by autotransplant for patients with high-intermediate (H-Int) or high IPI grade diffuse aggressive non-Hodgkin lymphoma (NHL).
Results: Of 370 induction eligible pts 253 were randomized to standard (128) or transplant (125) therapies; 35% had High IPI
Conclusions: For advanced stage H-Int and High IPI diffuse aggressive NHL, early autotransplant improves PFS for responders, including those induced with CHOP-R, with a stronger outcome seen for those with High IPI grade.
J Clin Oncol 29: 2011 (suppl; abstr 8001)



DESPITE HIGH CR RATES, THERE IS NO BENEFIT FOR HIGH DOSE CHEMOTHERAPY WITH SCT AS A FIRST LINE TREATMENT IN PATIENTS WITH AGGRESSIVE NHL.

Interpretation and Conclusions. Overall, the analysis of published
evidence reveals very heterogeneous results and no overall
survival benefit. Therefore, HDT/ASCT can- not be recommended
as standard first line treatment for patients with aggressive NHL.
However, the exploratory analyses presented here may help to
design new trials for this treatment modality.Haematologica 2003; 88:1304-1315

SO, CURRENT EVIDENCES DO NOT SUPPORT HIGH DOSE THERAPY IN PATIENTS WITH AGGRESSIVE LYMPHOMA AS THERE IS NO SURVIVAL ADVANTAGE. WE NEED TO WAIT FOR SOME MORE TIME (!!) TILL THIS CAN BE CONSIDERED AS A STANDARD RECOMMENDATION.
TILL THEN NO ASCT AT CR1 FOR AGGRESSIVE NHL IN CR1!!!!!!!

So Novel approaches may be the way
• Antibody
• Kinase Inhibitors
• Immune Modulation
• Other Targets

Newer AntibodiesDrug• Ofatumumab [60] Anti-CD20 mAb R/R DLBCL II No ORR: 11%; CR: 4%; mDR: 6.9 months;
mPFS: 2.5 months• GA101 [67] Anti-CD20 mAb R/R DLBCL and MCL II Yes EOTR: All: 28%; DLBCL: 29%; MCL:
27%• Veltuzumab [56] Anti-CD20 mAb R/R NHL I/II No ORR: DLBCL: 43%; MZL: 83%,
including CR/CRu: 33% ORR: FL: 44%, including CR/CRu: 27%• Epratuzumab [69] Anti-CD22 mAb R/R NHL (with rituximab) II No ORR: 47%; DLBCL:
CR: 33%• Epratuzumab [70] Anti-CD22 mAb Previously untreated DLBCL (with R-CHOP) II No
ORR: 95%; CR/CRu: 73%; 1-year EFS rate: 80%; 1-year PFS rate: 82%; 1-year OS rate: 88%• Milatuzumab [57] Anti-CD74 mAb R/R NHL (with veltuzumab) I/II Dose-finding PR: 1/3 in
Cohort 1 (8 mg/kg); 2/3 in Cohort 2 (16 mg/kg)• Dacetuzumab [77] Anti-CD40 mAb R/R DLBCL (with rituximab and gemcitabine)Ib Dose-
finding ORR: 54%• Lucatumumab [74] Anti-CD40 mAb R/R HL or NHL Ia/II Dose-finding RR: R refractory:
40%; ORR: DLBCL: 11% (phase Ia); ORR: DLBCL: 15% (phase II)• Blinatumomab (MT103) [83] Single-chain bispecific anti-CD19 and CD3 mAb construct R/R
NHL I Dose-finding FL: 11/21 responses; MCL: 3/21 responses

Newer Antibodies
• Drug Eligibility (and design) Randomized Results
• I-131 tositumomab Previously untreated DLBCL (with R-CHOP)No 1-year PFS rate: 75%; 1-year OS rate: 83%
• Inotuzumab ozogamicin CD22 targeted cytotoxic immunoconjugate R/R CD22+ and CD20+ NHL (with R)I No ORR: 80%; 1-year PFS rate: 89%
• Inotuzumab ozogamicin CD22 targeted cytotoxic immunoconjugate R/R CD22+ and CD20+ DLBCL prior to HDT-ASCT (with R) No ORR: 21%
• 90Y-epratuzumab tetraxetan [92] Radiolabeled humanized anti-CD22 mAb R/R NHL I/IIDose-finding ORR: 62%; CR/CRu: 48%; mPFS: 9.5 months
• 90Y-epratuzumab tetraxetan [97] Radiolabeled humanized anti-CD22 mAb Consolidation after first-line R-CHOP in DLBCL II No Improved remission status 6 weeks after RIT: 30.7%
• Brentuximab vedotin (SGN-35) [104] Antitubulin monomethyl auristatin E (MMAE) anti-CD30 mAb conjugate R/R lymphoma I ORR: 46%; CR: 29%

Current Trials with novel Approaches
•• Enzastaurin DLBCL –CR1 after R-CHOP NCT00332202 PRELUDE
Ongoing; not recruiting NA•• Inotuzumab ozogamicin + R versus investigator's choice of gemcitabine +
R or B + R R/R aggressive NHL NCT01232556 Recruiting NA
• Single-agent pixantrone dimaleate versus investigator’s choice therapy [49]Third-line treatment of R/R aggressive NHL NCT00088530 EXTEND (PIX301) Completed; final results presented at ASH 10 Pixantrone superior to other single-agent therapies
• Pixantrone + R versus gemcitabine + R R/R DLBCL patients not eligible for SCTNCT01321541 PIX-R (PIX306) Recruiting NA

Kinase Inhibitors in Aggressive NHL• Dinaciclib [183] CDK1, 2, 5, 9 inhibitor R/R in low-grade lymphoma and DLBCL I No
PR: DLBCL: 1/7; SD: FL: 2/7; MCL: 1/1
• Fostamatinib [198] Syk inhibitor R/R B-cell NHL and CLL I/II No ORR: DLBCL: 22%; FL: 10% SLL/CLL: 55% in SLL/CLL: MCL: 11%; overall mPFS: 4.2 months
• Dasatinib [202] RTK inhibitor of BCR-ABL, SRC, c-Kit, PDGF and ephrin receptor kinases R/R NHL I/II No ORR: 32%; 2-year PFS: 13%; 2-year OS: 50%
• Enzastaurin [201] Protein kinase beta inhibitor R/R DLBCL II No FFP: 22%
• PCI-32765 [204] Bruton’s tyrosine kinase inhibitorR/R B-cell NHL I Dose-findingORR: 43%
• SB1518 [208] JAK2 inhibitor R/R lymphoma I Dose-finding PR: 3/26 (2 in MCL)• Sorafenib [221] TKI inhibitor of RAF/MEK/ERK/c-kit/Flt3, VEGFRs, PDGFRs, RET R/R NHL
II No ORR: 10%; CR: 5%• Sorafenib [222] TKI inhibitor of RAF/MEK/ERK/c-kit/Flt3, VEGFRs, PDGFRs, RET R/R
lymphoma (with Akt inhibitor perifosine) II No ORR: 23% (all PR; all in HL)
• Sorafenib [223] TKI inhibitor of RAF/MEK/ERK/c-kit/Flt3, VEGFRs, PDGFRs, RET R/R MM or lymphoma (with mTOR inhibitor everolimus) I/II Dose-finding ORR: 33%

Targeted Therapies• Drug MOA (target) Eligibility Phase Randomized
Results
• Bortezomib [127] Proteasome inhibitor Previously untreated DLBCL (with R-CHOP) I/II Dose-finding CR/CRu: 92%• Bortezomib [128] Proteasome inhibitor R/R DLBCL (with chemotherapy) II No ABC versus GCB: ORR: 83%
versus 13%; mOS: 10.8 versus 3.4 months
• Everolimus [151] mTOR inhibitor R/R NHL II No ORR: 30%; mDR: 5.7 months• Everolimus [152] mTOR inhibitor R/R NHL I 2 dose cohorts 2 responses in DLBCL and 2
responses in FL, in 13 patients
• Temsirolimus [154] mTOR inhibitor R/R NHL (with rituximab) II No ORR: 59%; CR: 19%; PR: 40%
• Vorinostat [167] Deacetylase inhibitor R/R lymphoma (with R-ICE) I No 19/27 responses• Vorinostat [168] Deacetylase inhibitor R/R lymphoma (with DOXIL) I Dose-finding 4/14 disease control
• Oblimersen sodium [183] Bcl-2 antisense oligonucleotide R/R B-cell NHL (with R) II No ORR: 42%; ORR in FL: 60%
• PF-3512676 [209] TLR9-antagonist R/R NHL (with R) I Dose-finding ORR: 24%; ORR in extended treatment cohort: 50%
• Bevacizumab [221] Anti-VEGF mAb Previously untreated DLBCL (with R-CHOP) II No 1-year PFS rate: 77%; 2-year PFS rate: 69%; 1-year OS rate: 86%; 2-year OS rate: 79%
• Aflibercept [220] VEGF fusion protein Previously untreated B-cell lymphoma (with R-CHOP) I Dose-findingORR: 100%; CR: 80%

Immunomodulatory Agents
• Drug Eligibility Phase Randomized Results
• Lenalidomide aggressive NHL II No ORR: 35%; CR/CRu: 12%; mDR: 6.2 months; mPFS: 4.0 months
• Lenalidomide aggressive NHL II No ORR: 35%; CR/CRu: 13%; mPFS: 3.5 month5.6 month
• Lenalidomide Previously untreated DLBCL (with R-CHOP21) I/II Dose-finding CR: 15/21; PR: 1/21

Summary
• In ‘ R “ Era novel approaches may be the way to go.
• Newer trials will mature and may HELP us or Confuse us.
• Data may not be extrapolated across the IPIs or subtypes

ACKNOWLEDGEMENTACKNOWLEDGEMENT
• Patients and Family members• My teachers from CMC Vellore & Westmead
Hospital , Sydney.
• Nursing and Medical Teams, SSH• Blood Bank & Pathology teams , SSH• Administrative staff and SSH
• Megh Apte & Dr. Netra Apte,Parents