High risk of cardiac events in hypertrophic cardiomyopathy
24
High risk of cardiac events in hypertrophic cardiomyopathy patients with double/compound heterozygosity Serio A, Pasotti M, Gambarin F, Pilotto A, Serafini E, Diegoli M, Grasso M, Tagliani M, Disabella E, Arbustini E Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia Italy A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Transcript of High risk of cardiac events in hypertrophic cardiomyopathy

High risk of cardiac events in hypertrophic cardiomyopathy patients with double/compound heterozygosity
Serio A, Pasotti M, Gambarin F, Pilotto A, Serafini E, Diegoli M, Grasso M, Tagliani M, Disabella E, Arbustini E
Centre for Inherited Cardiovascular Diseases
IRCCS Fondazione Policlinico San Matteo, Pavia
Italy
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Background
• Hypertrophic Cardiomyopathy (HCM) is caused by mutations of genes coding:– sarcomeric proteins (sarcomeric HCM)
– non sarcomeric proteins (non-sarcomeric HCM)
with considerable genetic heterogeneity and variability in phenotypic
expression.
• Major complications are sudden cardiac death (SCD) and evolution through left ventricular dilatation and dysfunction.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Marian AJ et al. J Mol Cell Cardiol 2001Seidman CE et al. Basic Res Cardiol 1998
Maron BJ. JAMA 2002

Background
• Most HCM are autosomal dominant, associated with a single heterozygous mutation of one disease gene. A minority is associated with double or combined heterozygosity.
• When all known disease genes are systematically screened in consecutive patients, a minority of cases show double/triple or compound heterozygosity.
• The prevalence of these latter cases is still provisional.• Phenocopies (drug toxicity such as chloroquine) may clinically
mimic HCM.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Kwon JB et al. J Clin Reumatol 2010Keating RJ et al. J Am Soc Echocardiogr 2005
Arbustini E et al. Heart 1998Girolami F et al. J Am Coll Cardiol 2010

Background Compound or double heterozygosity
• First implication: genetic screening should systematicallyinclude at least major disease genes
• Second implication: in the families reported by Richard et al.the age of onset, the degree of hypertrophy or the prognosisare related to the number of mutations.
• Compound or double heterozygosity (5%, 4/80 pts) wasassociated with more severe clinical phenotype (more severehypertrophy, more frequent sudden death)
→ CMGCV: genetic diagnosis in families without co-segregationby age is provided as non-conclusive
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Richard et al. Eurogene Heart Failure Project. Circulation 2003
Ingles et al, Seidman, J Med Genet 2005

Purpose
• We aimed at determining the prevalence of double or compound heterozygosity in a consecutive series of genotyped families with HCM and analyzing their outcome during a mean follow-up of 87±65 months
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Methods
• Population: 495 mutated patients
– 188 unrelated probands
– 307 relatives
(December 2009)
• HCM diagnosis:
– done according to the WHO criteria
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Methods
Clinical and instrumental evaluation: • physical examination• ECG• Echocardiography• Holter ECG monitoring• biochemical testing: sCPK, lactic acid, Troponin• neuromyological examination• coronary angiography• electrophysiology study, right catheterization• endomyocardial biopsy (when clinically indicated)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
for probands and relatives

Methods
Genetic testing:– genetic testing was performed after counselling and
written informed consent.
– MYH7, MYBPC3, TNNT2, TNNI3, tCAP, MYL2, TPM1, MYH6, MYL3, MYO6, and MYOZ1 were routinely screened, while LAMP2, PRKAG2 and mtDNA were screened in the presence of specific clinical markers
• Patients with Anderson-Fabry disease were excluded.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Results
• Out of the 495 mutated individuals:
– 361 affected (73%)
– 134 healthy carriers (27%)
• The mean age of affected members was significantly higher compared to those of the healthy carriers
34.3 ± 15.2 versus 26.9 ± 15.3 years (p=0.003)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
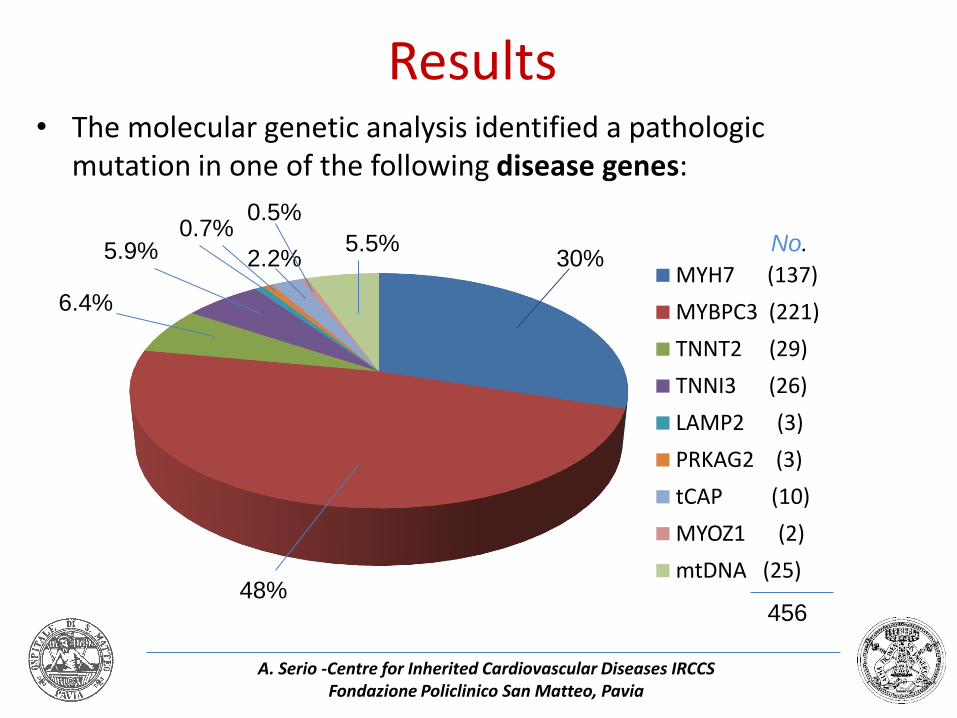
Results• The molecular genetic analysis identified a pathologic
mutation in one of the following disease genes:
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
MYH7 (137)
MYBPC3 (221)
TNNT2 (29)
TNNI3 (26)
LAMP2 (3)
PRKAG2 (3)
tCAP (10)
MYOZ1 (2)
mtDNA (25)48%
30%
6.4%
5.9% 5.5%2.2%
No.
456
0.7%0.5%

Results
• 39 patients (7%) were found to carry a compound or double heterozygosity.
• Among the patients with double or compound heterozygosity:
– 37 were affected (95%)
– 2 were young healthy carriers (13 and 15 y.o.)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

EVENTS IN THE OVERALL GENOTYPED HCM PATIENTSAfter 87±65 months:
79 of 361 (22%) phenotypically affected HCM patients had one of the following events:
12 20 4 43
Results
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
No.
%

Results
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
SCD CHF death
HTx ICD shock
ICD shock + HTx
Total number
%
MYH7 5 6 8 2 1 22 16
MYBPC3 11 3 2 7 2 25 11TNNI3 1 1 4 0 1 7 27TNNT2 3 0 0 2 0 5 17
DOUBLE 3 1 5 3 1 13 33LAMP2* 1 0 0 0 0 1 33PRKAG2* 1 0 0 0 0 1 33TCAP 0 0 0 0 0 0 0
MTDNA 2 1 1 2 0 6 31MYOZ1 0 0 0 0 0 0 0

Genes No. %
Double MYBPC3 16 41.1
MYH7+ MYBPC3 11 28.2
MYH7+ mtDNA 6 15.4
MYH7 + double MYBPC3 4 10.2
tCAP + mtDNA 2 5.1
39 patients (7%)
with double or compound heterozygosity
39
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Eventsin “healthy mutation carriers”
No. events
Mutated clinically affected 79 in 361 pts (22%)
Healthy carriers 0 in 134 pts (0%)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Conclusions
• The prevalence of double/compound heterozygosity in our series was 7%.
• The rate of complications and malignant evolution was higher in HCM associated with double/compound mutation (higher rate of adverse events in a shorter period of time).
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
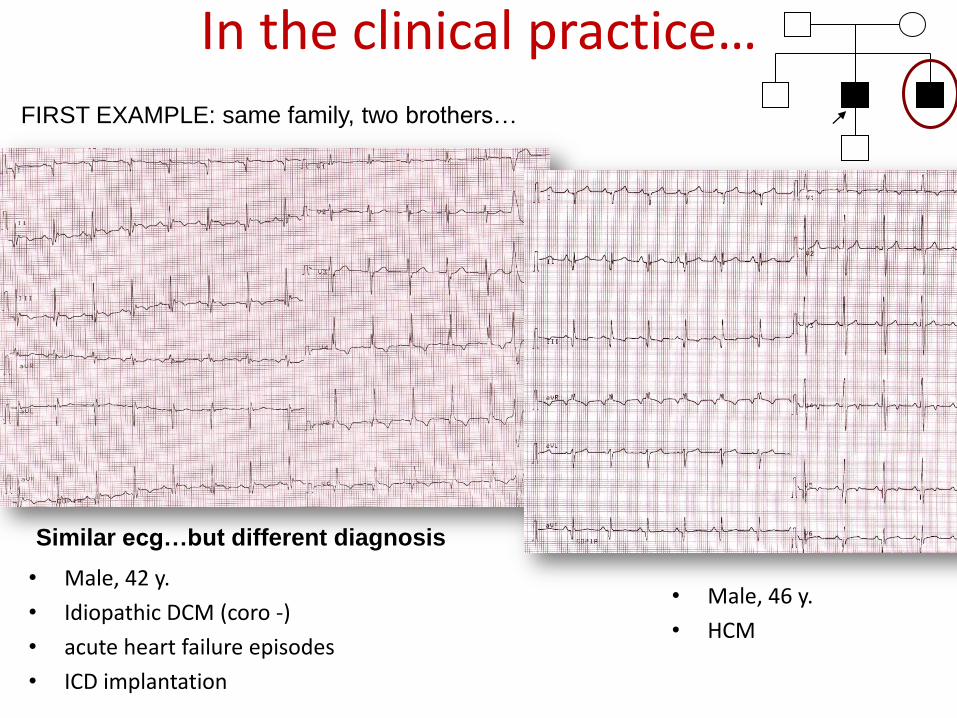
In the clinical practice…
• Male, 42 y.
• Idiopathic DCM (coro -)
• acute heart failure episodes
• ICD implantation
FIRST EXAMPLE: same family, two brothers…
Similar ecg…but different diagnosis
• Male, 46 y.
• HCM

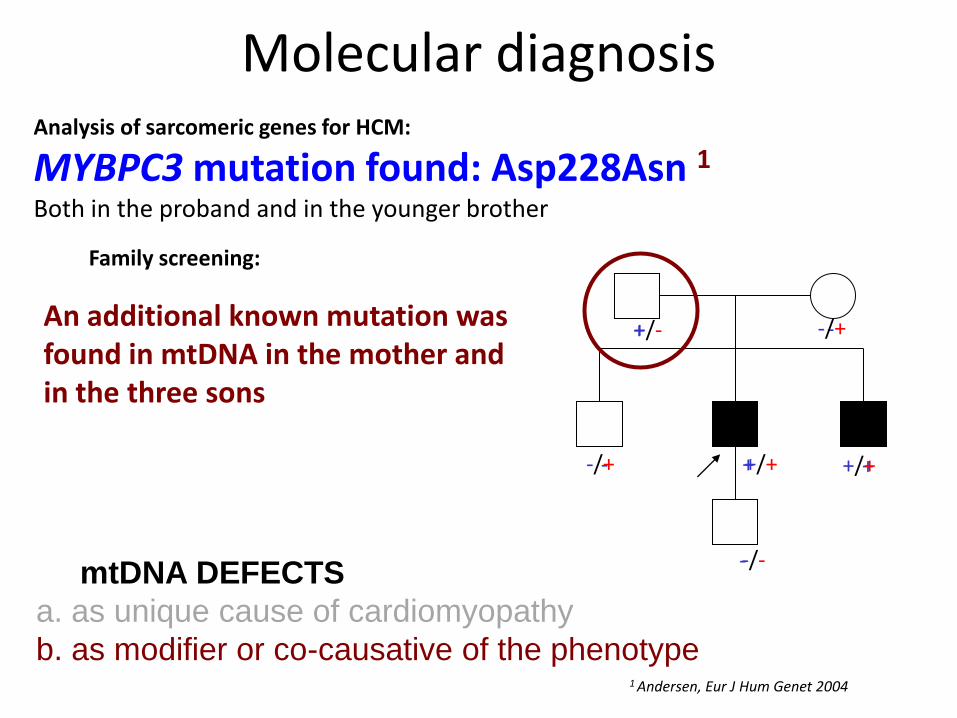
Molecular diagnosisAnalysis of sarcomeric genes for HCM:
MYBPC3 mutation found: Asp228Asn 1Both in the proband and in the younger brother
1 Andersen, Eur J Hum Genet 2004
Family screening:
+ -
- + +
-
An additional known mutation wasfound in mtDNA in the mother and in the three sons
+/- -/+
-/+ +/+ +/+
-/-mtDNA DEFECTS
a. as unique cause of cardiomyopathy
b. as modifier or co-causative of the phenotype

MYH7 ex 22M849C
MYBPC3 ex 18 R597W
GENETIC Analysis
MYH7+MYBPC3 - RELATED FAMILIAL HCM
SECOND EXAMPLE: same family, brother, sister and nephew…

• proband with HCM evoluted in dilated form with LV
dysfunction and CHF, heart transplanted (52 y.)
• mother “with cardiac problems” (HCM?)
• sister with HCM, initial LV dysfunction
• nephew with HCM
FAMILY HISTORY
?

proband
nephew
sister

LV enlargement
LV progressive dysfunction (EF 25%)
Loss of hypertrophy (12 mm)
progressive atrial enlargement
Nephew
EF 50%
Septum 21 mm
Sister
EF 40%
Septum 14 mm

Thank you