HEPATITIS OBSTRUCTIVE JAUNDICE, AND ACUTE PLASMA: IN … · 2018-04-25 · OBSTRUCTIVE JAUNDICE,...
17
PROTEIN-LIPID RELATIONSHIPS IN HUMAN PLASMA: IN BILIARY CIRRHOSIS, OBSTRUCTIVE JAUNDICE, AND ACUTE HEPATITIS Howard A. Eder, … , Mary M. Wilber, David P. Barr J Clin Invest. 1955; 34(7):1147-1162. https://doi.org/10.1172/JCI103163. Research Article Find the latest version: http://jci.me/103163-pdf
Transcript of HEPATITIS OBSTRUCTIVE JAUNDICE, AND ACUTE PLASMA: IN … · 2018-04-25 · OBSTRUCTIVE JAUNDICE,...

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA: IN BILIARY CIRRHOSIS,OBSTRUCTIVE JAUNDICE, AND ACUTEHEPATITIS
Howard A. Eder, … , Mary M. Wilber, David P. Barr
J Clin Invest. 1955;34(7):1147-1162. https://doi.org/10.1172/JCI103163.
Research Article
Find the latest version:
http://jci.me/103163-pdf

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA: INBILIARY CIRRHOSIS, OBSTRUCTIVEJAUNDICE, AND
ACUTEHEPATITIS 1
By HOWARDA. EDER,2 ELLA M. RUSS, R. A. REES PRITCHETT, MARYM.WILBER, AND DAVID P. BARR
(From the Department of Medicine, The New York Hospital-Cornell Medical Center,New York, N. Y.)
(Submitted for publication July 26, 1954; accepted March 16, 1955)
In 1862, Austin Flint (1) found that cholesterolaccumulated in the blood in obstructive jaundice.Fifty years later Widal, Weill, and Laudat (2)pointed out that the hypercholesterolemia of ob-structive jaundice is due in large measure to in-crease in serum free cholesterol in contradistinc-tion to that of nephrosis, where both free andesterified cholesterol are greater than normal.More recently (3-5) it has been shown thatplasma phospholipid increases even more thancholesterol, so that the ratio of total cholesterolto phospholipid is appreciably less than normal.
The serum lipoproteins have also been meas-ured in patients with liver disease. Pierce andGofman (6) examined the sera of thirty-twopatients with cirrhosis and found levels of the Sf10-20 class slightly higher than normal. Theyalso studied forty-eight cases of acute hepatitis(7) and found elevations of the Sf 0-100 com-ponents with the largest increase in the Sf 12-20class. The increased concentrations correlatedmost closely with the presence of jaundice andtended to decrease when the jaundice subsided.McGinley, Jones, and Gofman (8) found a hugeincrease in the Sf 6 and Sf 8 groups, with varyingincrease in Sf 10-17 in five cases of biliary cir-rhosis. By starch zone electrophoresis, Kunkeland Slater (9) observed that in biliary cirrhosisthere was a high peak consisting predominantlyof phospholipid which had the same relative mo-bility as normal beta lipoproteins. The concen-tration of alpha lipoproteins was extremely low.Snavely, Goldwater, Randolph, and Unglaub (10)by ultracentrifugation of whole serum from pa-
lThese studies have been aided by a grant from theU. S. Public Health Service, by support from the Com-monwealth Fund and the Albert and Mary Lasker Foun-dation, and by gifts from Mrs. Katherine Lilly Conroy.
2 Present address: State University of New York,College of Medicine at New York City, Brooklyn, N. Y.
tients with acute hepatitis found an increase inlight aggregates rich in neutral fat and poor inester cholesterol.
In this present study, plasma proteins in pa-tients with liver diseases in which biliary obstruc-tion is a prominent or suspected feature were frac-tionated by Cohn's method number 10 and thefractions analyzed for protein and lipid constitu-ents. In some of the patients, and especially inthose with acute hepatitis, it was possible to ana-lyze the plasma serially during the disappearanceof jaundice and during the various phases of re-covery from the disease.
SUBJECTS
The cases studied were classified as follows.
Biliary cirrhosisPrimarySecondary
Bile duct obstructionAcute hepatitisPortal cirrhosis
Nxmber of cases
75
123036
The diagnosis of primary biliary cirrhosis was madeon the basis of the clinical picture. In six of the sevenpatients (Table IIA), exploratory laparotomy revealedan appearance of the liver indicating biliary cirrhosis.There was no evidence of extrahepatic biliary obstruc-tion. In one patient (Yaz), laparotomy was not per-formed, but needle biopsy of the liver yielded a specimenregarded as histologically typical of biliary cirrhosis.The duration of illness varied from six months in Peyand Ros, to eight years in Whe and Dor. In Pey,xanthomata were not present (perhaps because of theshort duration of the disease). All of the other patientshad xanthelasma, and with the exception of Whe haddeveloped xanthomata in other areas. All of the pa-tients had large livers and spleens. All of them wereintensely jaundiced and had high concentrations of alka-line phosphatase at the time of plasma fractionation.
The diagnosis of secondary biliary cirrhosis was madein five patients with chronic jaundice in whom laparotomy
1147

H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
and biopsy of the liver presented a picture compatiblewith biliary cirrhosis but in whom there was also evi-dence of extrahepatic biliary obstruction (Table IIB).In Kur and Fit the common bile duct had been damagedby previous surgery. Sto had a large congenital pan-creatic cyst. Although no common duct stone was foundin Drm and Bro, they were classified as secondary biliarycirrhosis because of chronic cholecystitis and the pres-ence of stones in the gall-bladder. Duration of symptomswas from one and one-quarter years in Drm to elevenyears in Fit and Sto. Drm, Fit, and Bro had xanthelasmabut no evidence of xanthomatosis elsewhere. The othersdisplayed no cutaneous lipid deposits. Two of the fivepatients (Drm and Fit) were not intensely jaundiced atthe time of fractionation. All had serum alkaline phos-phatase concentrations greater than thirty Bodanskyunits.
The group designated as bile duct obstruction (TableIII) consisted of six patients with carcinoma of the pan-creas, three with common duct stone, two with metastaticcarcinoma of the liver, and one who had both hema-chromatosis and primary liver cell carcinoma. Theduration of jaundice varied from one to five weeks. Allpatients were jaundiced at the time that they were stud-ied; in Kau and Smi subsequent studies were made fol-lowing the relief of obstruction. In these patients, serumalkaline phosphatase concentration was elevated, andin Kau and Smi decreased along with serum bilirubinconcentration.
Patients with acute hepatitis (Table IV) were notdifferentiated as to etiology. Eight of the thirty hadhistories of blood transfusions; none of them had a his-tory of exposure to toxic substances. For convenience,the date of onset of the disease was arbitrarily defined asthe day on which jaundice or dark urine was first rec-ognized. Since, however, many of the patients had suf-fered vague symptoms for some days preceding the ic-terus, it was impossible to determine the duration of theillness with accuracy. It was thought that, in eleven,studies were initiated during the first week; in five, dur-ing the second; in twelve, during the third and fourth;and in two, still later in the course of the illness. Thoseobserved during the first week after onset probablyrepresent a random sample of cases of hepatitis admittedto the hospital during the period. Those in whom ob-servations were initiated at a later time usually hadpersistent icterus. All of the patients with jaundice hadalso elevated levels of serum alkaline phosphatase andabnormal cephalin flocculation and thymol turbidity.These abnormalities disappeared as the concentrationof bilirubin decreased. Bat and Dre died within a weekof onset, and autopsies showed acute massive necrosisof the liver. Saz and Ols had less fulminating coursesand died after day 23 and 83, respectively. All the otherpatients recovered.
The group of patients with portal cirrhosis (Table V)included thirty with progressive hepatic insufficiency,peripheral edema, and ascites. All but three of them of-fered histories of large alcohol intake. The group alsoincluded one patient with hemochromatosis and five
young women who gave no history of alcoholism but whosuffered from acne, amenorrhea, recurrent attacks offever, jaundice, and other features of the syndrome de-scribed by Bongiovanni and Eisenmenger (11). Severalof the patients with alcoholic cirrhosis had episodes sug-gestive of superimposed obstructive jaundice with markedelevation of serum bilirubin and clay-colored stools. Thiswas apparent in Rob on 2/20/52 and in Guz on 9/16/53.Sko had a hemolytic anemia with high indirect bilirubinand greater than normal excretion of urobilinogen in thestool.
METHODS
Cohn's method number 10 was used for the chemicalfractionation of the plasma proteins. Three fractionswere isolated: IV + V + VI, II, and I + III. Plasmaand all fractions were analyzed for protein and for cho-lesterol by the Bloor method. In some of the cases freeand total cholesterol, phospholipid, and total lipid carbonwere determined in unfractionated plasma and in Frac-tions IV + V + VI and I + III. Details of the procedureof the fractionation of proteins and of the analytic meth-ods have been previously described (12). Free and totalcholesterol were determined by the method of Sperry andSchoenheimer as modified by Sperry and Webb (13).With very dilute samples it was necessary to concen-trate the extracts by evaporation of solvent.
Paper electrophoresis was carried out by the methoddescribed in detail in a previous publication (14).
Ultracentrifugation was carried out in a Spinco modelL preparative ultracentrifuge. The solvent density of theserum was raised to 1.063 by adding to 4 ml. of serum 4ml. of NaCl solution containing 181.7 gm. per liter (15).Tubes were inverted and then centrifuged at 80,000 timesgravity for thirteen hours at 15 to 16° C. The top layerwas removed, using a hypodermic syringe and curvedneedle. The top and bottom layers were analyzed forlipid and subjected to electrophoresis on paper.
RESULTS
In Tables II to V the results of cholesterol andphospholipid analyses of plasma and of the proteinfractions have been assembled together with valuesfor total serum bilirubin and the ratios of free tototal cholesterol on the plasma. Observations onthe Sperry-Schoenheimer (13) determinationsand the free to total ratios of the fractions are pre-sented separately in Table VI.
In order to facilitate comparison, normal valuesand ranges for two age groups have been listedin Table 1. For cholesterol by the Sperry-Scho-enheimer method, normal values are available onlyfor the younger group. In the older age groupthe values would probably be altered in a directionsimilar to that of the cholesterol values by theBloor method (12).
1148

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
TABLE I
NormaWvalues of concentration and distribution of protein, cholesterol, and phospholipids in plasma andfractions of normal young men and women
Cholesterol (Bloor)Plasma (mg. per 100 ml.)
Fraction IV+V+VI (mg. per 100 ml.)
Fraction I+III (mg. per 100 ml.)
PhospholipidPlasma (mg. per 100 ml.)
Fraction IV+V+VI (mg. per 100 ml.)
Fraction 1+11I (mg. per 100 ml.)
Cholesterol-phospholipid ratioPlasma
Fraction IV+V+VI
Fraction I+III
Ester choksterol (Sperry-Schoenheimer)Plasma (mg. per 100 ml.)
Fraction IV+V+VI (mg. per 100 ml.)
Fraction 1+111 (mg. per 100 ml.)
Free choksterolPlasma (mg. per 100 ml.)
Fraction IV+V+VI (mg. per 100 ml.)
Fraction I +III (mg. per 100 ml.)
Free/Total choksterolPlasma
Fraction IV+V+VI
Fraction I +III
Primary biliary cirrhosisIn Table IIA the results obtained in the eight
cases of primary biliary cirrhosis have been as-
sembled. Because the studies were made at vari-ous stages of the disease, each case is consideredindividually and averages are not determined.In the Table, the cases are arranged in the orderof decreasing cholesterol concentration. In every
case of the group the total cholesterol is greaterthan normal, although it tends to diminish in thoseof longer duration. The increased cholesterol
tends to accumulate chiefly in Fraction IV + V +VI where in three of the cases it constitutes 70 per
cent or more of the total concentration. In all ofthe patients, the phospholipids of the plasma in-creased more than the cholesterol with resultantmarked lowering of the cholesterol-phospholipidratios. This is almost entirely attributable to a
disproportionate accumulation of phospholipidsin Fraction I + III where the cholesterol-phospho-lipid ratios are grossly lower than normal and fre-quently approximate those of Fraction IV + V +
Young menand womenaged 18-35
199(126-276)
58(39-93)
134(47-228)
228(148-287)
113(73-164)
106(46-157)
0.87(0.62-1.20)
0.51(0.32-0.64)
1.26(0.71-1.56)
Older menand womenaged 45-65
261(171-354)
54(32-80)
187(95-294)
270(202-327)
102(75-140)
155(74-244)
1.00(0.79-1.18)
0.51(0.35-0.61)
1.38(1.12-1.49)
123(89-157)
33(21-51)
81(52-106)
49(42-64)
11(7-15)
39(27-50)
0.29(0.22-0.35)
0.24(0.20-0.28)
0.33(0.27-0.48)
1149

H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
VI where phospholipids increased proportionatelyto the cholesterol and where the cholesterol-phos-pholipid ratios deviated little from the normalaverage of approximately 0.5.
Analysis of the plasma by the Sperry-Schoen-heimer method shows that the increment in plasmacholesterol in all of the patients is due to accumu-lation of free cholesterol with a resultant increasein the ratio of free to total cholesterol. Even inDor, however, where there is no increase intotal plasma cholesterol, the free to total ratio isalso markedly elevated. Analysis of several ofthe fractions (see Table VI) indicates that almostall of the cholesterol in Fraction IV + V + VI isfree, while Fraction I + III contains essentiallyall of the plasma esterified cholesterol in additionto free cholesterol.
In Table IIB are the data from the five cases ofsecondary biliary cirrhosis. The concentration ofplasma cholesterol exceeds the limits of normalbut is increased less than in the cases of primarybiliary cirrhosis. With progressive hepatic fail-ure the concentration tends to fall. The patternof distribution of cholesterol is similar to that inprimary biliary cirrhosis. In all patients, con-centration of bilirubin is markedly elevated, thecholesterol-phospholipid ratios are considerablyreduced, and the free to total cholesterol ratiomarkedly increased both in the plasma and inFraction I + III. In Sto, as the jaundice in-creases the cholesterol-phospholipid ratios inplasma and Fraction I + III decrease, and theratio of free to total cholesterol rises (see TableVI).
Bile duct obstruction
In Table III, the data on the patients with bileduct obstruction have been assembled. Patientswere selected on the basis of considerable constantor increasing jaundice. Cases in which jaundicewas decreasing were not included, although in twoof the cases (Kau and Smi) measurements madeafter jaundice had begun to subside are included.In four of the patients, cholesterol in the plasmaas well as in the two lipid-containing fractions iselevated. All of the patients in this group havelow cholesterol-phospholipid ratios in the plasmaand in Fraction I + III. In nine of the twelvecases in which cholesterol-phospholipid ratios and
free to total cholesterol ratios are extremely ab-normal, history indicates that the obstruction hasbeen of less than six weeks' duration. These pa-tients with bile duct obstruction of relatively shortduration and presumably normal livers demon-strate most clearly the effects of obstructive jaun-dice on plasma cholesterol-phospholipid ratios andfree to total ratios. Restoration of normal lipidinterrelationships after relief of obstruction is in-dicated in Smi.
Acute hepatitis
In Table IV, the data on the thirty cases ofacute hepatitis have been assembled. The patientsare listed in order of time elapsed between the on-set (the day when jaundice or bilirubinemia wasfirst noted) and the first analysis of the plasma.
The deviations in lipid concentration and distri-bution vary both with the duration of the hepa-titis and the degree of icterus. In severely jaun-diced cases studied during the first week followingonset, the level of total plasma cholesterol is appre-ciably reduced, the concentration of phospholipidsis not proportionately reduced, with the resultthat there is a marked lowering in the cholesterol-phospholipid ratio both in the plasma and in Frac-tion I + III. In these cases there is also a markedreduction in esterified cholesterol, with increasein the ratio of plasma free to total cholesterol.This is usually apparent also in Fraction I + IIIbut is most marked in Fraction IV + V + VI,where almost none of the cholesterol is esterified(Table VI). In patients whose total cholesterolis less than normal, the percentage in FractionIV + V + VI tends to be low. In the occasionalpatient with high concentration of total cholesterolthere is an increase -in the cholesterol in FractionIV + V + VI such as is seen in biliary cirrhosis.
These striking deviations in concentration anddistribution of lipids tend to disappear graduallywith recovery from the disease and particularlywith the subsidence of icterus. They may disap-pear entirely before clinical convalescence is com-plete. Among the nineteen cases whose study wasbegun more than a week after the onset, therewere seven whose bilirubin concentration was lessthan 2 mg. per 100 ml. In these cases, low cho-lesterol-phospholipid ratios in the plasma and inFraction I + III were not found. In patients fol-
1150

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
0% 0% e4U) t-'I4666;
U)U)4V-666
000m 'eq co 00
Ut) 00 14'eq ' 0oeq _-
C4 aOmv4O NO0N
l4d 40U)U) -Rdf ~q
c 66)
V- tl-0O00 qw 00
'C4 q-4 4
WE) '0i 4
U)Z .41w0
U) U) e - 00 U)00%%'0 00 U)in0%U)N000 eq 00- - eq eq q 0-
.0co0
coo
.0
t, mor-
04in U) U)
00%Uin<U) In c
a (%00%
'0 00
$ co
0% &-- -
00 0%000 U) )
so "a 0 oU)
'e oq-I eq -
co In !
000008 -;0X4 :4 m
U) 'o 0o eb U) '0 U)
0 In NO In
U) Q4 C0
oo No.~~~~~~~~~~~~~~~~~~6
IRV 0 00 0
_, m
cz- - 00
U 00
'4.
0% U) rM4 U)4
U) 00 UI) U)
0-
or
U) q.o6
00 V) O0 00 o00eq eq 1- 000lq'
- - 0- I-0044
o 6 6 666
00 'O U) 0o rt- 0%o)o) 0 to so cooo'06c .4 6 6 666
0-0%
00N
m0
( co UX C
0 t- 0 U)
eq 00 0 e
'0 F. 0% F-0% 14 00 F-0% 0 F-IzX
0
00cco
C4~~~~~~~300 eq - - *) -
U) U) '0 0 0 F-inO NO cO L O
00'm' 00 0% F-0
eq00D
00 - eq 1- 000% U) '0 _ 0,*
q Ce -
00- 00 eq - eqo0ooeq 1E F- de "F-0 00M
4Ut ) 0000"
4q4 W- -4 t-14 00 UW)-6; 6 C66
00 00 F- eq U) F-F- 0o 0000
0% '0 Id4 0U)o_ 4
o00 0%m)
00 '0-0%o4o '0 U) eq o o_4 00 00 e) eqe
0coF- -
V-0U) eq
00
0030
3.
- 0% 0o Oec0%
- e
o ov""C
00 0) 0U)U)U) ICsC
_00
- 00 --N-
00 0% 00 __400 00 ) t-
4.Ch 0_
_la
0A
UIt
0
Pz4~
+
291a
1151
%Oo00 E " 40 q4 E - 'OtU)) U) d4 tE %O q U) 'o666 6 66 6 6 6 6
tDa0X +%.
-U.E=B.
0
la
a4
Is£4
A0U
-£4
qo£t4
- b
4
t 04
.4 '
a16
00U) % 00 '00% C00. F- 0co) 0 0 'O0 0% '0 oF-_0%4 - 000 O U) eq
_ _
4v
4£4
,
i-6
a
:
6"c

H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
NOI0 %O 'oe cor0O 0 0o
- U) '0e '0 o% b0 00 o' oo - U)a + o6 4 6 666666oo oo.A+ inr'0% 4 d4 o) - 0 - U)_ > 'U)+ 14 m m en4 ) 4 NO
.0 +o> o 666oooo 666
U
0 0% (D.,Z.~CV)00 - D., 0 00 U)
a).2
| U)t+'-4 0% 0%e-bU)e-~m 4 -o in t Uo
X o o~ oo' o'- o4 ooo0% 000% 0% '0o ~ )o. W0 U)om CV)
_-4 C C - -0 4
1.$ +@ b e+ 4'4O
.~ 0 -4', ._
4. 6 U)'- )e W) '0U U) 0-d to'0 o0
>0r C4 U) CDcs oo_7 O+ _ N No - to
oo m ~~~UCV)CV)C)C)4 V V
0 +
00
0.t So . b N ~~~~~~~~~~~m4 U) t- ONonin 0 o
o~~~~~~~~~~~~~~~~~~~~roN.}LO
O enm e +nen_
I.U.)e
-0 ~eI '400 U) 00 '0t- 00 U)0In)'~~ 0% ~~~~- t- '0~~NO It o -it)'1 CV CV 00 '1d4 ON
(6oo6 6 6666 66 (666 C~~~~~~0~ ~ ~ 0
0E (D+ o L W Id -X d4 en o 1 (e4).-'Z ib - Wto 0%
o t=4o No 4o 1o oo o o4 >
* k-0%''4 U) 00 n1"-'1 0 O C) 0, '0 o
U ; NO NO _-
_" en to _ en
+~ 00 U) ' ' oo~ oU)% 0oom e oo 'o '0 V)
" Es e + __ n N mo e o _ooo
0 *)ZD8. 0c % 0 0%o U)'0o
. U) '0 '0 0 1-N ) U) C ) C)
X e~ ~~~~~~~n mme'U) ( (- U) t c '0 e 0
* _V) I1~ I-4~-4 I ) IN 00U) 14 C)0) - 0% '0'4Y N1 et~~~~14CD 1
a o 1
0 '0 o)) -1~ - - -I I I I
M01
M~~~~~~~~~~~4 X X W W W
Ao u)0 m14tn oo4C4 M C1 C1 M
00U) '00) ( 10 0 '1e 0% L 04 00
~~ ~~ c'i '~~~e 'W, 6so~~- 00 00 o %O t
' i z ~4
1152

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
eq4 0 qd NO- CEU) U) - *4 C)
O V 00 t)o000q4 Id4 CE lq4 qd4 lq466666C65
VO 00 U) U) U) 100 eq" CU00666666o-4-o
eq 00 VeO( -0- 00 eq)No4 lq4 00 F- ) d4 CE -i LO
6666666666
1153
0o C4 U) U)Vo U) E -
U) - - )
CE) rV
X6666;*- *m dOqd
F- -o -
o0eq4 "66
C4 o-0 00- No o o 00000 eu4 00 _%4 O %0 %0 4U) eq 00%O I'd NO%ONO " I'd oO 0v 00 00 Ul) --4 in in in o oo oOo 01. in 0, oo 1 u) ooO 000000000 0000000000 0000 00
000F-004 .6 .4 .- .6 ab V0 --~00 00
*CU + _00 CU +4
in OO 0 - 0\f- e6 el cl CO CV-400 F- 0% eq4 w-eq 9- w- -4
00000%000-000
"UVt0O(% F- C'4 F- CE 0% 0eq e . e * e . -. e
00 eq - 0% in "CU 0% 0%~q4 CE
- 1_' 00 F-00 V00'4
0000.0.
CE) 0
_- - _-0000mm"
V 00
02% eq* eq
(OC4
00 eq
VO00
V; C.40%U
* . . @
* u4* 000
0 0d -00
00 OF-U)0Go 0+ ot4
0- C-4 004
eqin
o C- .t 1,
V000- -
0%VNO 0VN I' 0 00.d'F- CE)- 4Ft- o d4 NOeq E)Ul) Veq ) U) VSO CEn VCNOE)00F- F-CE dCU s0o -'000% - u0-.e C VN 0% 000n0i
00CEO M) 000%( E 0%4O F '-t- m .EC )m *V-'*% No eNVO 0e) It oo0- enC Cen V00ooo0ooo **-q' - -: E 00 Ee
ooo6o o :6 ooCooo :666 :o :. 00 o66
U) ef 0000-F-: eqi -- V6 00 eqeqC eq4 CU' V-0% 0- . *q * * -
4e 00 eq
0% 00 eq 1" 0000o
V4 eq 94 - CE) 00V4 F eq F--- -- - - eq eq eq
C) t-00 U) e) eqo -OU Vee in tn lqd ux " NWIld %
-44 00 VlNC; el (IN0% VOU)
e
- F- U) F-
C soVo00t
eq 0
F U)
- sot. uiv- M
U) eU)U)00 OF-U)
eq 00 eq,0 N6Ce
V )14or
- 0%0 00if 0I0F-Oeq N -Iqqd0%4~ - oUt NO'0as00eq00w0 Veq00Cot-. F-V% IR tF..Oeto - - 4 t- F- VOt-VV% CeqOV-00V 0 w00%0 0% 00%E)t- qo eqw 0 CE)00 00 1-..C409- - 4Cl - - 9- -C4"a MC4" ---4eqeqqCEeq eqeqeqeq -4eq eqeq, eq ,eqeq(14
U) VF-eqe V000ecsE)t-
r__
4 OOIO"MO- ~~~~~4eqe
in co0-'F- ' e0NOco'V-CE)0(:% W-eqeqC4 0c
eq4 eqeqeqeq eqeqeqeqeqeq.0) IU ) InLe))W U) In WI)0)
- -e ce - 4eq e cf)00 in0- eqeqeq CE)
Cd 4) >> N0 0
eq F-
4m m 3
.' 00) NV~0% 0000 CE) 0F-F Vi000 V6 '-C e'i eq4C1
- qCE 4 eq4 -4(1 4C- - eq CE) , 4V V F
eqeq eq eq eqeq eq eq eqe
00- F- ) CE 0% V 0 U- CEeqC)- eq eqso eq
CECEe44~ 0000
-N
-E)
NOt- No"66 el;
q00- 0%eq
CE)
-- eq- - -.
F- -
eq
o cU
*a
._r04
la
00 0 0% .eq
6i 006 1
o0 oo *t-
U) co %O * r0 C eli .; . .
0
.
9+4>
to22II,
NO Ieq U)IU)Uo .0*U
VV+O *t..ooo .0
00 C) V * 0
0U0C).Oo
inin .co
ouo.eq
U00O
CD 0- *:ICe) .F-F:- V.0e .0.
e 0c% *- 00. .
.
V- o ( *0_- _4
._
.0.5
am
.C
AU
+bUI%8C-
4 k
+
+x
>.
+0
-4
U-
U.
*.
t44
m b4fz V
h..
.9
bI.0
E0co 0o U)
000cE)o0eq 0%- eq Vq
in Ul) ao oDs -
<6 000'--;00F- CE)eq40 -
0 NOVNm
eq l4 U) CE)
00%V00eq 0%: k.. '-'0
11 - eqNO0%.
00 -00000)
00 ld l)0
. . .
N o _
=EDSCUAs3 4%
a
aE6)
2
CU
co
£
- F-+*- .- .
-
CE) - --u
CE eqe_
0
eq

H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
00 0% 00 00
664qd .oIoI
U)(0 t4'U)00
O_w
_6Xoo
ll CII Il0 .- . .:
-0 OO0
0o0 * 0 t.U )0000: 008 14 00c
6 . 0 0c0. . * *
e U) * *. c
00 *'0'0
V-4 - - 4
CD -00.- .00W
'- 0 00-6 oooo1-t-0
e4i e4 Ilvo NOCD
C~40 - d4tU)0% *0C
)mU) - U) -U) U) I4 qd4 to666 66C
MV_ oUxW4 eqcs :
%O~o r- Il
U)0+U)
RV in i
0000.;JCU)
0% U
0 -4
U) .J4t66;
00 t.. q 0'0 _C4 U)
U N0 00 d44 .d4 d4666 6
in %'0 C~4
t- U)0
U) to Il4 U)6 6c
U),- IU 'o0 0000o '0- d4 %eNOC q4 ON%4Zro00 o0% 000%00 It-* 00 U)000000 1-000%
66666 6 6C 6c .C5 c; C; :* 66.66 6666.. C;
co-00.'e00' *U)'-
0 '000* -ooo * Mo
0%4T-.0 '-40"00 t.o * 00-%0 t- t- 0a
o oo
l) 0C40
00 (14 lU )
U) 0
e. 0
to. -10 "
-4
U) t0 0%Ln - 4ch toN - - -
' - 4 0
0%1 U) 0 -4
C* U *4 -
10 0 0 N000 U),' -'0 00 Il4 1
1.4I"V-
c0 C4 0
00 (4 U)U) I4 qd4666
U)U) 4 U)U) -S e Uon -
--
%O _1 _eq 4
0'C000c..
NOcrl b U) 00 00 C0666 6666
00 00o
C" U) 00
C -
o0
0 U) O00Z.. t. 00 ~.00 C4 U) (4
%0 'o 0 U)
oU 000ui etm 0000 t
- 0% .d4 '0'0e%IC4.10 4 U)C14 - v4
t-o0'0'0U 0 0'Uo)oLo *0NoNo t- 0% - 14 0co 0%0U)o No0UooU)0 00 0 %N'0Uc) 0 '000 on)00 0'%n UU)
* - - - -e 00l0 -. ~ U)0.*0. 0 000. **
U) 000 4-
0 4 U) ~6_0; t-- -- - --C1 n el o It: r
0 4 00 C1Ce
U) U) U) lq4 U) N0
- q' 0 Ul)*
00* -
V- W-4 C-4 W-4
C- C4'%6 t- if elC14 4 lq %O
U)00V4 w00 " C 10 %000%Ot'.-400U) U)t..00v- eq4 v- eq V- eq4 V-4--4 eq4
en .U)0% .4 U*0 *- * - t- - U) oo00 - 0%e 0%00 *0 ** .U)( .q... . **.
00 0 ) I. ... *.o66c :66:: - *- :6: -6666 6.- oo.o
00 -00e4-i -4:C l
0 e14 14 U) 00UC;w )'0wU) e4 U) 1"4
9-- 0 OQ'-4
so N l' U U
Go UW) C4er. v: o6 - ;S
O
co0.0gi _O
u fioU) "
Co s
00C000
t- - U) 0%w- C.4 eq w-
_14 0 Z- U1
- U) U) >4
t1..000i o6
C~4 00 lq4 C~44 - C4 C4
- U) Rdq '0
C4 t-. N0 NO
00 4o0t. 00 t-C0% 0% 0
-4 U) C%4
os4m q:
-000
0 lqd 0% zt'
C-4 N4 U) U)
eq4 U) .4 U)
eq 0 0l: 00C'U00'0U)Oi t- '0 C14 'IOC14 O t-..0'00 U)144 0%0%00'0eq t..co0% 0% 0UU))00 0 0- Ot %'00"d "d4 '0'- 0 iU)Uin) eq00U) -
'- -4W4'4V4 eq eqeqeq4- V--l -eqU)en -e4U)e4eqeq4C14- V-4 -eqe.
00eqt-U U))O0
-WU) 00 -" eqe -.
U)Weq- *N_-eq
4 mU)t- U) U) U) U)
U)-cU)u)r <enuz
Q4C1
1154
10
._
._U
'a:1
0m +._
+
(d
(
0 4i
>.90to+t
za >+Dl+ ;g04;.
0.6.0
0)0
.0
.00Iol4
0-a -
0.4 ~4=
VI
"I U co
_ -
v+ $>
m +42+$8E._
Et}t'.
.00 ' U). -
*q U)- to.. 0 U
v4 4 v-U)U)0
- e
- - -- eq eq
Vt- U) - U) t-
-- C U-
.0
(U..1;
(U9=
(U
-l)000c
-oo CD\0
U
U) U) UOU) U)q V- e - U)
-4 -40----
_ N
OU___
eq
0V
_ 0U) inC4 O
U)U)
0
Ocuo
M-C
U) C4 0
_- _- _- C-4
--- eq
_4_
en
U)U)U)UU) ) U
00 eq l' 0%0 ei U)* -
mO 0 1-1
-1 C4 U)'04eq eq O eq
U) U) U) U)
t.V 0~ -
U) 0-
9Z4
00
0
co 00 -
-0
' 04 00-41 eq 00_- CNt-
eq eq eqU') U) U)
R14 W0-4U) U)
eqV
0
m L
_0% U) 0-
- Cto t-U) eU
U) 0 0-. 00
eq e eq eqU) U) U) W)
+4 00 U)'
U) .'14
W u
_e
CU

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
'O 0 C" a W U)U) U)0%00-6 6o---4,
eq *~0 . 0*eq
6 6666
if) 0 NOU) 0% 0
%O000e
W- ) 446C;o
O% 0% 00%l40 00 V-4-4
o- o4 moo
-; 05 C5
U) . 440%eq6 .444444 U)000%00 _o_-
0 *U) *_eqU) *oeq o044 ..4 .I4 .44 . Io . o: oC o: C
0 00 Owe-- U U)eq_- o to_C
*4 * C* .4oq o ooeq44P I44 U)q44
6; 6; 66
'0 t- t-0% U) t'.
o 66*% .O) oo4
U) U)
*- m
U) U66
e) t U)0%0Q t. oo44 eq U ,40 0o )0 )Goc o--I eq U U )- co eqO 0%U)
U) 0t0000 O)t.. 000.t-.N0 44 t00t-000c00oI 0 0t in 440%0i0t 44o 446 66666 666 6; 46 400co. 66666C;C;c :666 6 66466 6C ;C 6 66C
0 00000
i%0 00U)4e*1 * . * *
oo krC0%o--w40 eq C'4 eq 0U) e4q V-4-
U) *eq
U) *C'_ -
U -0U)
4400 00
0 0 coo
* C. e -
O a0 -0%
44 U) 00%W") 0
0 -000U)0 ~-40%
eq) U)eqeqwe -Mq-
eq .eq 0UW)0 - 0%000U) .4 :60~ :6 %6 dU) .00 .t'-U)NO'0- ..'t..
0 0 eq0V) wU)414 44 --
0 44" 40%O +
0 00U) '0eq'0 eqU
U- O 0)
U) 00%t- '000
OU)t*. -00
eq -
0'0
t- 00U)U )00- 0%CIeq k- 00ec 0 q"4e *0000u) 0% '0U) 0%- 0
'o 0o0'O 00_-4 ,-,'-44 '00o U* U) t. 00 Oe 0O_- )n mm C 4CV>U <e M^NC4 M - NW*e"<N *ol" e " 04M eC4 C4 V>Stqd
00e * - " * . * * 4 ,* o\0 k- 0 00 a 0 **o*O-7*O0'% * to 0 W)U) : :
I.00 I0 . e. : : oo000 o6:6-6*6O6*6O6*0000000006*6*6* .- * O * *0
U) 0000000 %00%4 t-..0t- e 0 e * . -
an Xo 0o t- lo
Uvo) i) r,U f -4 VW-o"
6; :4W- -
'i-U)W
0 0C U) qo. '0 000
- coo
W) U) ) -oC 0a Qff- - 444
00 0t-e"o UU)W4 o '0O-00 0"q -U) eto o 0O
Meq eq _-- _"
U)
0
U)
V-.4
9-4
__
t-
40% 44 U) U)
I440 t.-
U) Ul) U) U)
tl.. U) - 00 U)
- ---
'z4
eqe
00co t U)'I 0
t_.' 00 00
inU)UWI) U) U)
00 &..U) w-M- ~-... Uo) W-
eqeq 00 U)
U) No AO
44W i...
-
04-
_eqe
U) U)
W-4 4-44_
'zo
0
4too0oo0-0 *troeq_--- e - - _- --
M001-Cl) -Inlw0oo
co eq - U 0 0000 0044qdl00eq 44 U -eq eq eq ) eq eq eq
U) 44 0m
0s oi b0UQ "on
- - - -
8 - t4 e
- eqoU) 4 U)
-o -q C0 0eteq -U
00%eq -
0 U)e -
eq -q el%*4 w-
%O% 04Go440+ 0 00 0 U) - 0 U) 000 %OAU)t'.0% 0%U)00tt 00t.r-.. - 0 U)00%%v U) eq"--- - " ---- - e" - - - eq q -
000N0U)q0%W)NO
U) U) U) U1) U) U) U) U) U) Ul)
ao:0044 -44qCw eq Cq4~ eq
eq t.
U) )U
'0 -
0% '0 .
N0 00eq
eq __
4-
-
-4-4 -4
-- .4-U) 0U)
-4 --.
1-.. 0% -4
WZ4 (D
U)
0a 19 rx
'0
4444
U) in)WI'0 44_
fdo "4
44
'z4 %O
%0
000%
t-.
U) U)
--4 -4-
0 0-
.2
S +
_4>
3aco
.5A
.i
U
1155
la
0.0A4
.0U
.2ta
.2
"4
P4 + t8
+ 8
>
E1 ti8.;
I .06E.,
a
H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
'.
1,+*0
'I
130. a
Ii.;IX. 9U: D
X
0
It
0
p
Days
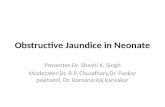
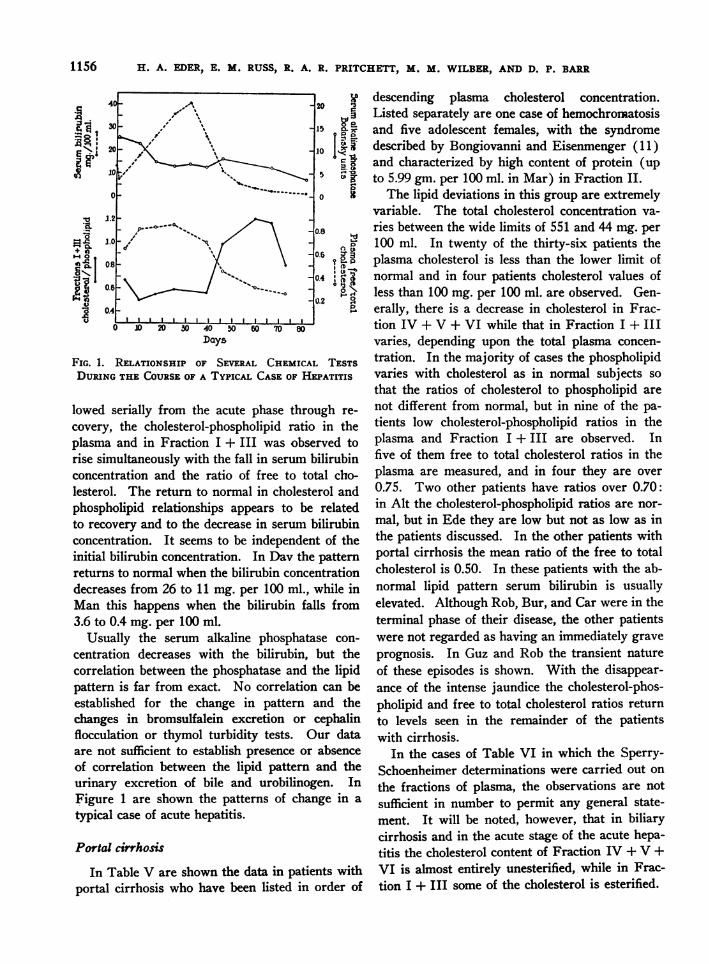
FIG. 1. RELATIONSHIP OF SEVERAL CHEMICAL TESTSDURINGTHE COURSEOF A TYPICAL CASEOF HEPATITIS
lowed serially from the acute phase through re-
covery, the cholesterol-phospholipid ratio in theplasma and in Fraction I + III was observed torise simultaneously with the fall in serum bilirubinconcentration and the ratio of free to total cho-lesterol. The return to normal in cholesterol andphospholipid relationships appears to be relatedto recovery and to the decrease in serum bilirubinconcentration. It seems to be independent of theinitial bilirubin concentration. In Dav the patternreturns to normal when the bilirubin concentrationdecreases from 26 to 11 mg. per 100 ml., while inMan this happens when the bilirubin falls from3.6 to 0.4 mg. per 100 ml.
Usually the serum alkaline phosphatase con-
centration decreases with the bilirubin, but thecorrelation between the phosphatase and the lipidpattern is far from exact. No correlation can beestablished for the change in pattern and thechanges in bromsulfalein excretion or cephalinflocculation or thymol turbidity tests. Our dataare not sufficient to establish presence or absenceof correlation between the lipid pattern and theurinary excretion of bile and urobilinogen. InFigure 1 are shown the patterns of change in a
typical case of acute hepatitis.
Portal cirrhosis
In Table V are shown the data in patients withportal cirrhosis who have been listed in order of
descending plasma cholesterol concentration.Listed separately are one case of hemochromatosisand five adolescent females, with the syndromedescribed by Bongiovanni and Eisenmenger (11)and characterized by high content of protein (upto 5.99 gm. per 100 ml. in Mar) in Fraction II.
The lipid deviations in this group are extremelyvariable. The total cholesterol concentration va-ries between the wide limits of 551 and 44 mg. per100 ml. In twenty of the thirty-six patients theplasma cholesterol is less than the lower limit ofnormal and in four patients cholesterol values ofless than 100 mg. per 100 ml. are observed. Gen-erally, there is a decrease in cholesterol in Frac-tion IV + V + VI while that in Fraction I + IIIvaries, depending upon the total plasma concen-tration. In the majority of cases the phospholipidvaries with cholesterol as in normal subjects sothat the ratios of cholesterol to phospholipid arenot different from normal, but in nine of the pa-tients low cholesterol-phospholipid ratios in theplasma and Fraction I + III are observed. Infive of them free to total cholesterol ratios in theplasma are measured, and in four they are over0.75. Two other patients have ratios over 0.70:in Alt the cholesterol-phospholipid ratios are nor-mal, but in Ede they are low but not as low as inthe patients discussed. In the other patients withportal cirrhosis the mean ratio of the free to totalcholesterol is 0.50. In these patients with the ab-normal lipid pattern serum bilirubin is usuallyelevated. Although Rob, Bur, and Car were in theterminal phase of their disease, the other patientswere not regarded as having an immediately graveprognosis. In Guz and Rob the transient natureof these episodes is shown. With the disappear-ance of the intense jaundice the cholesterol-phos-pholipid and free to total cholesterol ratios returnto levels seen in the remainder of the patientswith cirrhosis.
In the cases of Table VI in which the Sperry-Schoenheimer determinations were carried out on
the fractions of plasma, the observations are notsufficient in number to permit any general state-ment. It will be nQted, however, that in biliarycirrhosis and in the acute stage of the acute hepa-titis the cholesterol content of Fraction IV + V +VI is almost entirely unesterified, while in Frac-tion I + III some of the cholesterol is esterified.
1156

1157PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
-4 0OO 0'- - --M loom V-o *N _
1;mon
V4 *o4:. V
o 0 0 0 0qo *%O co 0D'0 U)'J'U
Y *00 oo '0-C666 C; 6 (6 (66C
'0 U>')C4 N00V"4 U) i) 0- U)co inU000%00 0 0002%
0. 0.. .0%. . . 0.
Uz) oo 0%' oO O 00 e0%
_. 00I 000 .00 00ooo0000 -- - ~4 -4 V- W- W-
U) 'o_ 00 LeU) U)eq*i .i .. 0.
':j '1'U)' 0U) 4.* .- - Ooo
00 _u) '0 _' en0 eq0 No 0C
."
I.v* 0
-4
(4
In
' -o *)0e4 u ) i 1'0000* .4..U 00 U)*
o4'u) equ) *U) 0 U)4-0-00 -eq -C o eq-Id, W) °+d4 -1 OW)
w-'00' -4W-U)000 - '0
c..N
4'. U) 4".
S) '_"4U) C4 0 UW)0
0o4~1
'C0 "j0 eq00eq qiC1 Rdf NO-s e
6 -.e.i6 6 0 4 -4(N4 -
0e '- -
U) WU)U)) UUu)U)) U) U)v) U) U) U) U)
co U) 4- - ..'-- - eq - -
0'0 R q- -
'0~~~~eco L-)
0 -
- - U) U)
U) U) +
4J 3 D <x v
.6V-
0% U) 0
* 0 -
o4 oq oVlq4 C1NII 6 o1
eE 0% 0
1- t- r#
_. _ '*; .4 C0
666_
*-
- -
U) U) U)1- -- 1-- 0%
-
"- -1 00
00 00
0 '114
U) U)
%O "t Le)
J
0
U) +4 4.
oo vo00 -
eE) 4f) 1
6 6C; C;
C4 o0 -
Ul) 4..00 r
6 6
- O U) eN NOv 4 0 '14 s 00oo 'O 0
* o t oo oo t- o, 1_ t_ WI) t- In r* .. 0 0 4. 0 . . U . U .
*.o66666o 66o 66o 66o
* 0
. 00
* ooW-
. 6* 4'
to 0 0
'o 0 eqeq
U) 0% eq5eq l4 00
ooqo_ 4 I00 00 eq
U) I 00oC114 00 '0* .
0 - 0o4- 0 '0 'O 4- U) U)
eC eq ce
00-
W- e
00*qC j-' 00 00
*- 00 -
V- WQ
O eq
e -
uo 6U) 000a C;
00 +' 00 eq 0'0 0 0Q eq"~ 00 (" eq e
. -i 0 . Iq V- 0. .t *) . NO *66o~~~~~~~~~ ~ ~ ; ; :C ; :C ;C
0% U) 00 0 4'00 4.'. 00 0% 0*- 0 t. U)
c- e - - -
t- e - WI) 0
U) e U) - U)
- 0 0%U) '0 4'- - -
'0 4. 00
U) 00 ueIn m C4
o eq Neeq U) '0U) 0 0
eq4 0% 0o00 C"4 U)
0 0
00 -
0o 00
("4 00
e _- 00
U) U) U)
0
_
0 0v + e
*0._
h.rll-
0 +C3 +
+g.
co
(4i
'a0.00o.00
at
4,
.10la
"44,
4,
"44,
"4
"4
'(4I.I..4..
4,
'(4
..i.('4
I.'(4
'(4
I.
(4
(4(44,
4,"4I.
b4(4I.
"4
'(4I.,(4
I.
(44,
I-
0
- '-'00'0 0'O O "4 4-b 4 'o 'o 4- 0 - 0 (4 " 0 0 0 '-'U) 0C0e0 " q-.S O4 . %O0 1_d 4 00 e+ eq -4 - _0 0% t- '0 '0 '0U) -e q0-e q00en " "eq eq e q e 4 e- -N4 I -

1158 H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
I N0 * o W) -o. : C : : el' 'I oo
*
%oq* * _ o-4 0 .- 0v-e
eq U . .00 eN
oi * o * . o oo
to U)~ooW
U) U)Co
*'0 '0 - U).00 0%. 0%
*00 0o .W
o~o
* 0
o o
U)i UU) U)
C4 C4 * t- No * qs " inO ) **t o *' I)n O
co *o o * 6 o o
*0
9-
.0U)U)
0 - 0 0 V-
0. . 6 t.:k.
W), U) 0
CU). .. 4..oz
-.4 . & eq
.w U) . 0%. U)i q eq(4 o * %O W. * co wi "e-q .*0 -. *
eq
ao~~~~~~~~L
*. . 'X * °0 )*
+ _X bo. s kYm
so U)°_ 0
0 0 o, 004 Soeqei c CZ -r ad
oNo:$ e4 m 4 0% e4'o e - W a
WI) " v I-
e4 - -- - e
U)t'.. eq~~ 0 0 %O
00'0'0aU
eq * * * eq*
4. - U) 0%
-* 4 g- 0
0%m 8 V- 0 V-4..l ~ t 0 0 .
* 0 . C ;C ;C
0%4 0% U) 0% cmU) t'0 i w4 -i%
* * . - 8 N - - - -
* 0o * - (4 C* WI) * -t U)U) . ... .
U)
*o* : 00o
U) - U)k- e; 6 elU) - eq- - - -
0% U) eq e
- C'4 .- e
U) soI% 4.*2
4'.. .
*f-- U
tw .
4.. 0% W NO W-fe e 0 '00o 0U) O'0 U) U) ""e W4'1 - R ZV- W- W- W- W- W- V- W- 9- 9-4
NO - 'v 0 00 U NO No'.. W- NOe-i N * to; 4- el;el
eq --
W- co CC' - - eeq to eq ,o 0%o U) U) U) 0%
'N eq e - +q- eq %, -N~' N eq
U) 0% o ao0 - e Ueq eq .
e4 C4~~~~0C4 in in~~~~~~U
.0la -8 sa
%00oC;
o;
E+I4A
C)
U) -44 Co
Cs o
0%.
U)
0Go
0C%
* OA
: Cseq
U) 4. 0
4.. Mf40%
'0 U)C'4I
I
la
044.0
+0
14
+p3] +48
X ti
t d
I to
>V3¢
V-
-AF A1
jF
eq
0.
.0 o'-4N6 oz geq0% co 00
) 40 r-Meif ell o6 CU) U) --
0%0%
0%4..
t0I... U)
U)- -U) U) U)~
U) eq -- eq -do 0 0%
" q -4M-
eq X 0
e4 Go P0qw0 o
z5 .fi U:3 i' z : m
I,u 0 2 Z 0 x9,g
4

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
TABLE VI
Free cholesterol, esterified cholesterol, and free to total cholesterol ratios in Fractions I V+ V+ VI and I+III
Cholesterol
Plasma Fraction IV +V+VI Fraction I +IIIEster Free Ester Free Ester Free
mg. per mg. per Free/ mg. per mg. per Free/ mg. per mg. per Free/Name Date 100 ml. 100 ml. Total 100 ml. 100 ml. Total 100 ml. 100 ml. Total
Primary biliary cirrhosisRos 12/21/51 17.0 1,023.0 0.90 15.0 816.0 0.98 115.0 167.0 0.89Yaz 9/2/52 157.0 509.0 0.76 0 410.0 1.00 106.0 113.0 0.52Whe 4/8/53 96.0 390.0 0.80 4.0 230.0 0.98 87.0 109.0 0.56
Secondary biliary cirrhosisSto 11/19/51 108.0 110.0 0.51 4.5 24.1 0.84 85.0 86.0 0.50
Bile duct obstructionZik 9/7/51 96.0 1,095.0 0.92 17.0 860.0 0.98 83.0 148.0 0.64Smi 3/18/53 145.5 90.5 0.38 54.7 41.7 0.43 76.8 47.7 0.38
Acute hepatitisDav 3/31/52 37.0 161.0 0.81 0 51.3 1.00 131.0 120.0 0.92
4/15/52 25.0 143.0 0.85 0 27.6 1.00 41.4 101.1 0.71Stu 10/22/51 42.5 134.5 0.76 0 64.6 1.00 43.2 65.8 0.60
11/1/51 129.5 61.5 0.32 20.8 7.0 0.25 100.6 45.4 0.3111/12/51 154.0 54.0 0.26 35.2 8.8 0.20 102.4 40.6 0.28
Lau 11/12/51 179.3 66.7 0.27 27.6 8.4 0.23 136.7 57.3 0.30Saz 1/10/52 0 63.2 1.00 1.3 0.7 .... 7.5 63.2 0.88Ran 11/7/51 40.0 244.0 0.86 0 141.0 1.00 34.9 94.1 0.73
11/15/51 138.0 193.0 0.58 1.2 94.0 0.89 91.4 81.6 0.47Hoo 1/7/52 17.0 104.0 0.86 0 15.0 1.00 25.6 82.4 0.76
1/23/52 60.0 124.0 0.67 3.6 27.0 0.88 42.0 99.5 0.707/9/52 117.4 37.2 0.24 29.1 5.2 0.15 78.2 37.8 0.33
Ols 9/11/52 21.7 44.6 0.67 5.0 5.0 0.50 27.1 38.0 0.58
Portal cirrhosisRob 2/20/52 28.5 84.8 0.75 2.1 9.7 0.82 25.0 74.0 0.75
5/6/52 145.1 106.6 0.42 21.3 15.5 0.42 104.0 62.9 0.38Gau 6/19/52 165.4 87.6 0.35 20.2 6.2 0.23 127.7 65.8 0.34Pri 6/1/53 88.3 89.2 0.50 24.4 26.0 0.52 63.4 61.5 0.49Lew 2/3/53 77.1 120.5 0.61 4.6 26.9 0.85 78.3 75.2 0.48Hog 6/2/53 55.3 53.3 0.49 24.3 15.3 0.39 39.2 33.2 0.46Piz 6/1/53 58.8 64.0 0.52 21.9 17.0 0.44 40.6 47.2 0.54
Filter paper electrophoresisNormal plasma has two principal lipid-staining
components; namely, an intense deeply-stainedspot occurs in the beta globulin area and another,less intense, in the area between alpha, globulinand albumin. In biliary cirrhosis, despite the highlipid content of the plasma, the alpha componentis negligibly small and all of the stainable lipidappears to be present in the beta area. Similarpatterns have been found in obstructive jaundiceand acute hepatitis. With disappearance of ic-terus, stainable lipid then appears in the alphaarea.
Fraction IV + V + VI from the plasma of a
patient with biliary cirrhosis was subjected topaper electrophoresis, and all the lipids were foundto migrate with the mobility of beta globulin, and
when run on a starch block the fraction had alarge single lipid peak with a cholesterol-phospho-lipid ratio of 0.50. The lipoprotein of FractionI + III on filter paper also migrated to the betaarea.
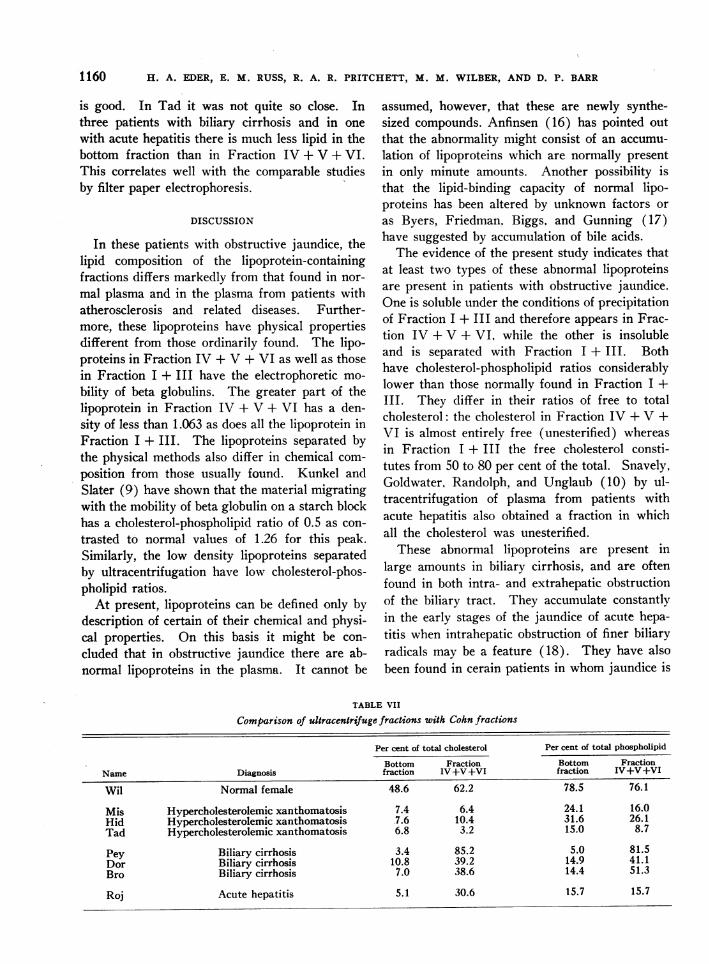
Ultracentrifutgal flotationIn Table VII are shown comparisons of the
separation made by ultracentrifugal flotation withthose made by Cohn fractionation. In this table,the per cent of total cholesterol and phospholipidfound in the bottom fraction (containing alphalipoproteins) is compared with that found inFraction IV + V + VI which ordinarily containsalpha lipoproteins. In one normal subject and intwo patients with hypercholesterolemic xanthoma-tosis the correlation between the two techniques
1159
H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
is good. In Tad it was not quite so close. Inthree patients with biliary cirrhosis and in one
with acute hepatitis there is much less lipid in thebottom fraction than in Fraction IV + V + VI.This correlates well with the comparable studiesby filter paper electrophoresis.
DISCUSSION
In these patients with obstructive jaundice, thelipid composition of the lipoprotein-containingfractions differs markedly from that found in nor-
mal plasma and in the plasma from patients withatherosclerosis and related diseases. Further-more, these lipoproteins have physical propertiesdifferent from those ordinarily found. The lipo-proteins in Fraction IV + V + VI as well as thosein Fraction I + III have the electrophoretic mo-
bility of beta globulins. The greater part of thelipoprotein in Fraction IV + V + VI has a den-sity of less than 1.063 as does all the lipoprotein inFraction I + III. The lipoproteins separated bythe physical methods also differ in chemical com-
position from those usually found. Kunkel andSlater (9) have shown that the material migratingwith the mobility of beta globulin on a starch blockhas a cholesterol-phospholipid ratio of 0.5 as con-
trasted to normal values of 1.26 for this peak.Similarly, the low density lipoproteins separatedby ultracentrifugation have low cholesterol-phos-pholipid ratios.
At present, lipoproteins can be defined only bydescription of certain of their chemical and physi-cal properties. On this basis it might be con-
cluded that in obstructive jaundice there are ab-normal lipoproteins in the plasma. It cannot be
assumed, however, that these are newly synthe-sized compounds. Anfinsen (16) has pointed out
that the abnormality might consist of an accumu-
lation of lipoproteins which are normally present
in only minute amounts. Another possibility isthat the lipid-binding capacity of normal lipo-proteins has been altered by unknown factors or
as Byers, Friedman, Biggs. and Gunning (17)have suggested by accumulation of bile acids.
The evidence of the present study indicates thatat least two types of these abnormal lipoproteinsare present in patients with obstructive jaundice.One is soluble under the conditions of precipitationof Fraction I + III and therefore appears in Frac-tion IV + V + VI, while the other is insolubleand is separated with Fraction I + III. Bothhave cholesterol-phospholipid ratios considerablylower than those normally found in Fraction I +III. They differ in their ratios of free to totalcholesterol: the cholesterol in Fraction IV + V +VI is almost entirely free (unesterified) whereasin Fraction I + III the free cholesterol consti-tutes from 50 to 80 per cent of the total. Snavely,Goldwater, Randolph, and Unglaub (10) by ul-tracentrifugation of plasma from patients withacute hepatitis also obtained a fraction in whichall the cholesterol was unesterified.
These abnormal lipoproteins are present inlarge amounts in biliary cirrhosis, and are oftenfound in both intra- and extrahepatic obstructionof the biliary tract. They accumulate constantlyin the early stages of the jaundice of acute hepa-titis when intrahepatic obstruction of finer biliaryradicals may be a feature (18). They have alsobeen found in cerain patients in whom jaundice is
TABLE VII
Comparison of ultracentrifuge fractions with Cohn fractions
Per cent of total cholesterol Per cent of total phospholipid
Bottom Fraction Bottom FractionName Diagnosis fraction IV +V+VI fraction IV +V+VI
Wil Normal female 48.6 62.2 78.5 76.1
Mis Hypercholesterolemic xanthomatosis 7.4 6.4 24.1 16.0Hid Hypercholesterolemic xanthomatosis .7.6 10.4 31.6 26.1Tad Hypercholesterolemic xanthomatosis 6.8 3.2 15.0 8.7
Pey Biliary cirrhosis 3.4 85.2 5.0 81.5Dor Biliary cirrhosis 10.8 39.2 14.9 41.1Bro Biliary cirrhosis 7.0 38.6 14.4 51.3
Roj Acute hepatitis 5.1 30.6 15.7 15.7
71160

PROTEIN-LIPID RELATIONSHIPS IN HUMANPLASMA
marked and biliary obstruction apparently pres-ent. In two of the cases in this series (Alt andSko) intense jaundice developed without accu-mulation of abnormal lipoproteins. In one of them(Sko) the jaundice may have been hemolyticrather than obstructive. In the other, no ex-planation is offered for the lack of correlation.In patients whose portal cirrhosis is associatedwith only moderate degrees of jaundice, theselipoproteins are not found.
It appears that the concentration of these ab-normal lipoproteins is related to the liver's syn-thetic capacity. Thus, in patients with earlybiliary cirrhosis in whom liver function is rela-tively unimpaired, high plasma concentrations ofthese lipoproteins are found. As the diseaseprogresses and liver function is impaired, the con-centrations fall. In hepatitis, where hepatic func-tion is of course impaired, high levels of abnormallipoproteins are not found. Data from electro-phoretic and ultracentrifugal separations indicatethat when the abnormal lipoproteins accumulatethere is certainly depression of the alpha lipo-protein concentration and probably also of thenormal beta lipoprotein concentration. In re-covery from acute hepatitis the return of the nor-mal lipoproteins is indicated by a return of thelipid in Fraction IV + V + VI to normal concen-trations and by elevation of the cholesterol-phos-pholipid ratio in Fraction I + III.
Accumulation of lipoproteins of altered chemicalcomposition offers an explanation of some of thedeviations in plasma-lipid relationships of liverdisease that are common to our own data andthose of Man, Kartin, Durlacher, and Peters (3)and of Albrink, Man, and Peters (5). In all theobservations there is a correlation between lowplasma cholesterol-phospholipid ratios and highplasma ratios of free to total cholesterol. It isevident that if most of the plasma lipoproteins havelow cholesterol-phospholipid ratios, the plasmaitself will also have a low ratio. Since little ofthe cholesterol in these lipoproteins is esterified,the plasma free to total cholesterol ratio will beelevated. Albrink, Man, and Peters (5) notedthat "the ratio of free to total cholesterol israrely as abnormal in cirrhosis with little or noicterus as it is in obstructive jaundice, althoughthe liver damage may be far greater." This isconsistent with the concept that these high free
to total ratios are a consequence of the productionof abnormal lipoproteins rather than an indicationof parenchymal liver damage as had been earliersuggested (19).
The alterations in plasma lipids encountered inobstructive jaundice in man can be reproduced tosome extent in animals by ligation of the commonbile duct. In rats, Chanutin and Ludewig (20)demonstrated increases in serum free cholesterolwith no increase in ester cholesterol and an in-crease in phospholipid proportional to the in-crease in free cholesterol. Byers, Friedman, andMichaelis (21) found similar changes in choles-terol. They showed (22) that hepatectomy pre-vented the rise in cholesterol and that (23) theamount of cholesterol that accumulated in theplasma was greater than could be explained byfailure of biliary excretion. Subsequently, Fred-rickson, Loud, Hinkelman, Schneider, and Frantz(24) showed that this increase in serum choles-terol following bile ligation is accompanied by asignificant increase in the rate of cholesterol syn-thesis by the liver. It may be that the abnormallipoproteins present in this circumstance may alterthe partition of cholesterol between liver andplasma, and that this partition may control therate of cholesterol synthesis.
SUMMARY
In obstructive jaundice and in early acute hepa-titis the lipid composition of the lipid-containingprotein fractions is markedly deviant from thatof normals and of all other diseases we havestudied.
In Fraction IV + V + VI there is approxi-mately twice as much phospholipid as cholesterol,just as is found normally in that fraction. How-ever, almost all of the cholesterol in the fractionis unesterified. The lipoproteins in this fractionhave the electrophoretic and ultracentrifugalproperties of beta lipoproteins, whereas nor-mally they are high-density alpha lipoproteins.
The lipoproteins in Fraction I + III, like thosenormally in this fraction, have the physical char-acteristics of beta lipoproteins. Their proportionof ester cholesterol is less than normal. The moststriking difference from normal lies in their cho-lesterol-phospholipid ratios which may be as lowas 0.5 by weight.
1161

H. A. EDER, E. M. RUSS, R. A. R. PRITCHETT, M. M. WILBER, AND D. P. BARR
It is concluded that in biliary cirrhosis, in somecases of obstructive jaundice, and in early acutehepatitis there are at least two types of abnormallipoproteins, the one found in Fraction IV + V +VI and the other in Fraction I + III.
During the recovery phase of acute hepatitisand following the removal of biliary tract obstruc-tion, the abnormal lipoproteins are replaced bylipoproteins of normal composition.
The lack of correlation between the appearanceof these lipoproteins and the degree of hepaticdamage in cases of portal cirrhosis indicates thatfactors other than inj'ur to the liver are implicatedin their formation.
REFERENCES
1. Flint, A., Jr., Experimental researches into a newexcretory function of the liver; consisting in theremoval of cholesterine from the blood, and itsdischarge from the body in the form of ster-corine. Am. J. M. Sc., 1862, In.s. 44, 305.
2. Widal, F., Weill, A., and Laudat, M., La lipemie desbrightiques; rapports de la retinite des brightiquesavec l'azotemie et la cholesterinemie. Semanamed., 1912, 32, 529.
3. Man, E. B., Kartin, B. L., Durlacher, S. H., andPeters, J. P., The lipids of serum and liver inpatients with hepatic diseases. J. Clin. Invest.,1945, 24, 623.
4. Ahrens, E. H., Jr., and Kunkel, H. G., The relation-ship between serum lipids and skin xanthomatain eighteen patients with primary biliary cirrhosis.J. Clin. Invest., 1949, 28, 1565.
5. Albrink, M. J., Man, E. B., and Peters, J. P., Serumlipids in infectious hepatitis and obstructive jaun-dice. J. Clin. Invest., 1950, 29, 781.
6. Pierce, F. T., and Gofman, J. W., Lipoproteins,liver disease, and atherosclerosis. Circulation,1951, 4, 25.
7. Pierce, F. T., Jr., Kimmel, J. R., and Burns, T. W.,Lipoproteins in infectious and serum hepatitis.Metabolism, 1954, 3, 228.
8. McGinley, J., Jones, H., and Gofman, J., Lipopro-teins and xanthomatous diseases. J. Invest. Der-mat., 1952, 19, 71.
9. Kunkel, H. G., and Slater, R. J., Lipoprotein pat-terns of serum obtained by zone electrophoresis.J. Clin. Invest., 1952, 31, 677.
10. Snavely, J. R., Goldwater, W. H., Randolph, M. L.,and Unglaub, W. G., The lipid composition ofultracentrifugates of serum from patients withacute hepatitis. J. Clin. Invest., 1952, 31. 664.
11. Bongiovanni, A. M., and Eisenmenger, W. J.,Adrenal cortical metabolism in chronic liver dis-ease. J. Clin. Endocrinol., 1951, 11, 152.
12. Russ, E. M., Eder, H. A., and Barr, D. P., Protein-lipid relationships in human plasma. I. In nor-mal individuals. Am. J. -Med., 1951, 11, 468.
13. Sperry, XVT. M., and WVebb, M., A revision of theSchoenheimer-Sperry method for cholesterol deter-mination. J. Biol. Chem., 1950, 187, 97.
14. Russ, E. M., Eder, H. A., and Barr, D. P., Protein-lipid relationships in human plasma. III. In preg-nancy and the newuborin. J. Clin. Invest., 1954, 33,1662.
15. Boyle, E., Personal communicationi.16. Anfinsen, C. B., Symposium on Atherosclerosis,
Irving Page, ed., National Research Council,Washingtoin, D. C., 1955, Publ. No. 338, 249 p.
17. Byers, S. O., Friedman, 'I., Biggs, MI. XV., and Gun-ning, B., Observations concerninig the productionand excretion of cholesterol in mammals. IX.The mleclhaniisnm of the hypercholesteroleimiic ef-fect of cholic acidl. J. Exper. Mled., 1953, 97,511.
18. XVatson, C. J., and Hoffbauer, F. XV., Liver func-tion in hepatitis. Ann. Int. Med., 1947, 26, 813.
19. Thaninhauser, S. J., and Schaber, H., tber dieBeziehuingein des Gleichgewichtes Cholesterin un(lCholesteriinester im Blut und Serum zur Leber-funktioni. Klin. Wchnschr., 1926, 5, 252.
20. Chanutini, A., and Ludewig, S., The blood plasmacholesterol and phospholipid phosphorus in ratsfollowing partial hepatectomy and following liga-tion of the bile duct. J. Biol. Chem., 1936, 115, 1.
21. Byers, S. O., Friedman, M., and Michaelis, F., Ob-servations concerning the production and excre-tion of cholesterol in mammals. I. Plasma cho-lesterol after bile duct ligation and free choles-terol injection. J. Biol. Chem., 1950, 184, 71.
22. Byers, S. O., Friedman, MI., and Michaelis, F.,Observatioins concerning the production and ex-cretion of cholesterol in mammals. III. Thesource of excess plasma cholesterol after ligationof the bile duct. J. Biol. Chem., 1951, 188, 637.
23. Byers, S. O., and Friedman, M., Observations conI-cerniing the production and excretion of choles-terol in mammals. V. The relation of biliary re-tention of cholesterol, distention of the biliarytract, the shunting of bile to the vena cava, andthe removal of the gastro-intestinal tract to thehypercholesteremia coInsequeInt oIn biliary obstruc-tioin. J. Exper. Med., 1952, 95, 19.
24. Fredrickson, D. S., Loud, A. V., Hinkelman. B. T..Schneider, H. S., and Frantz, I. D., Jr., Theeffect of ligation of the commoni bile duct oni cho-lesterol sy-nthesis in the rat. J. Exper. -Med.,1954, 99, 43.
1162