
Healthcare Reform: Improving the Healthcare World in Cleveland & Beyond
52
Healthcare Reform: Improving the Healthcare World in Cleveland & Beyond Barry M. Straube, M.D. Director, The Marwood Group Former Chief Medical Officer, Centers for Medicare & Medicaid Services October 27, 2012 University Hospitals: Case Medical Center Medical Quality Summit: Moving Forward
description
Healthcare Reform: Improving the Healthcare World in Cleveland & Beyond. Barry M. Straube, M.D. Director, The Marwood Group Former Chief Medical Officer, Centers for Medicare & Medicaid Services October 27, 2012 University Hospitals: Case Medical Center - PowerPoint PPT Presentation
Transcript of Healthcare Reform: Improving the Healthcare World in Cleveland & Beyond

Healthcare Reform:Improving the Healthcare World in
Cleveland & Beyond
Barry M. Straube, M.D.
Director, The Marwood GroupFormer Chief Medical Officer,
Centers for Medicare & Medicaid ServicesOctober 27, 2012
University Hospitals: Case Medical CenterMedical Quality Summit: Moving Forward

2

3

4

5

6

7

Life Expectancy at Birth vs.Spending by Country
8Source: OECD Health Data 2010

U.S. Healthcare Quality/Value Challenges• In the U.S. we spend more per capita on healthcare than
any other country in the world• In spite of those expenditures, U.S. Healthcare quality is
often inferior to that of other nations and often doesn’t meet expected evidence-based guidelines
• There are significant variations in quality and costs across the nation with increasing evidence that there may be an inverse relationship between the two
• Healthcare expenditures account for a larger section of the U.S. economy over the years and funding those expenditures is increasingly more difficult– Heretofore we have not addressed the problem of 45+ million
uninsured Americans• Cost Effectiveness Analysis is resisted as a tool
9

U.S. Healthcare Quality/Value Challenges• Care is uncoordinated• Care is not patient-centered, it is more provider centered• Care is inefficient• There continues to be considerable waste (overuse) in the
delivery of healthcare, as well as overt fraud & abuse• Insufficient emphasis is placed on major problems of:
– Patient safety• Healthcare Acquired Conditions
– Prevention– Unnecessary admissions and readmissions– Palliative & End-of-life Care– Health disparities
• Health Information Technology has a critical & unfulfilled role in this
10

U.S. Healthcare Quality/Value Challenges• The private and public sectors collectively have failed to reform
healthcare using conventional healthcare delivery and payment models– Traditional Fee-for-Service is a major reason: Pays for quantity, not
quality– Managed care has intermittently controlled costs > quality– Regardless of payment system we haven’t publicly measured &
compared cost or quality, and payers/providers are not held sufficiently accountable
• “All healthcare is local” means integrated health systems have a significant role to play, Academic Centers special
• The Affordable Care Act of 2010 has great potential to address the healthcare quality/value challenges
11

Ensuring Quality & Value:Tools/Drivers/Enablers
• “Contemporary Quality Improvement”• Transparency: Public Reporting & Data Sharing• Incentives: Payment reform by All Payers• Regulatory vehicles: State & Federal• Payer Benefit Design and Coverage Decision
Making• Demonstrations, pilots, research, innovation
12

“Contemporary” Quality Improvement• Need to set priorities, goals and objectives, strategic framework
first• Evidence-Based goals, metrics, interventions, evaluations
– Includes conformance with evidence-based guidelines, balanced with patient-centered considerations
– Cost-effectiveness, let alone comparative effectiveness, has not yet been addressed adequately
• Rapid-cycle development, implementation and change methodology
• Leveraging of resources and efforts: Current and future models-collaboration, alignment, synergy, priorities
• Many examples: Hospital Quality Initiative, Organ Donation Campaign, QIOs, ESRD Networks, IHI, Bridges to Excellence, NCQA, Nursing & Home Health Campaigns, many health plan collaboratives, local collaboratives, Partnership for Patients, etc.
13

Transparency: Public Reporting & Data Availability
• CMS Compare Websites– Hospital Compare– Nursing Home Compare– Home Health Compare– Dialysis Facility Compare– MA Health Plan and Medi-Gap
Compare– Prescription Drug Plan Compare– New under ACA
• Physician Compare• VBP Programs: Above plus
ASCs, LTCHs, IRHs, Hospices, others
• Other comparative websites– www.WhyNotTheBest.org
• MyMedicare.gov• HHS/CMS Data
Dissemination Efforts: www.data.gov, www.healthcare.gov
• Potential explosion of federal govt. & private sector data availability for private sector to drive data use innovation in previously unimaginable ways
14

Incentives• Pay for Reporting and Adoption Programs
– P4R: Hospital Inpatient/Outpatient , PQRI, e-Prescribing, Home Health
– ARRA /HITECH: EHR adoption and “meaningful use”• Value-based Purchasing (VBP)
– ESRD Bundled Payment System January 1, 2011• ESRD Quality Incentive Program (QIP) January 1, 2012
– Hospital VBP (ACA Section 3001) October 1, 2012– VBP in many additional settings in pipeline
• Competitive bidding, gain sharing, shared savings, bundled payment, ACOs, medical homes, salaries, integrated delivery, etc.
• Will any of these be effective ?15

VBP: Issues for Future• Alignment of multiple programs in existence or in pipeline
– Goals and objectives, priorities• What do we want to accomplish other than plain
measurement?• Public-Private alignment
– Measures• Many not actionable or likely to lead to improvement• Process to develop and gain consensus too long, too
contentious, too academic looking for the perfect– Financial Incentives
• Balance of penalties, bonus/rewards, shared savings, etc.• How much?
– Phase out P4R and adoption of outcomes-based VBP16

Regulation• Conditions of Participation or Conditions for Coverage
– COPs are minimum health and safety standards set by CMS for facilities that may receive Medicare payments
– 17 separate provider/supplier settings have COPs• Survey & Certification
– U.S. healthcare facilities certified must be in compliance with current Medicare regulations & applicable state laws
– S&C process uses interpretive guidelines to assess compliance with regulations
• In combination, a powerful tool for quality/value
17

Affordable Care Act (ACA) of 2010
• Title I: Quality, Affordable Health Care for all Americans
• Title II: Role of Public Programs• Title III: Improving the Quality & Efficiency of Health
Care• Title IV: Prevention of Chronic Disease & Improving
Public Health• Title V: Health Care Work Force
18

Affordable Care Act (ACA) of 2010
• Title VI: Transparency and Public Reporting• Title VII: Improving Access to Innovative Medical
Therapies• Title VIII: Community Living Assistance Services &
Support (CLASS) Act• Title IX: Revenue Provisions• Title X: Strengthening Quality, Affordable Health Care
for All Americans (Amendments)
19

20

High Profile ACA Topics• Greater Access to healthcare coverage• National Quality Priorities & Strategic Plan• National Prevention Priorities & Strategic Plan• Attention to not only Medicare & Commercial
healthcare, but Medicaid and Dual-Eligibles• Prevention and Patient Safety
– Numerous prevention initiatives– Population Health: Obesity, Smoking Cessation, etc.– Patient safety & medical errors reduction– Healthcare Acquired Conditions (HACs), Infections
• Focus on better outcomes, greater efficiency21

High Profile ACA Topics• Patient Centeredness• High-cost Chronic Disease Management• Care coordination & care transitions
– Reduction of unnecessary admissions & readmissions• Accountable Care Organizations, Medical Homes• Integration of conventional providers with public
health, community, and non-traditional sites of care• Innovation in payment, delivery systems, care• Rapid cycle change quality improvement• Best practices and learning environments• Attack on healthcare Fraud, Abuse, and
waste/overuse 22

Center for Medicare & Medicaid Innovation:CMMI
• CMMI establishment mandated by January 1, 2011 (Section 3021)– Consultation & input from broad healthcare sector in
implementation• Develop patient-centered payment models• Rapid piloting/testing of new payment programs• Encourage evidence-based, coordinated care for
Medicare, Medicaid, CHIP• Focuses on populations “for which there are deficits
in care leading to poor clinical outcomes or potentially avoidable expenditures”
23

CMMI: Statutory Descriptors
• “Risk-based comprehensive payment or salary-based payment” models
• “Geriatric assessments and comprehensive care plans…interdisciplinary care teams…multiple chronic conditions…”
• “transition health care providers away from fee-for-service-based reimbursement and towards salary-based”
• “health information technology-enabled provider network that includes care coordinators, chronic disease registry, home telehealth technology”
24

CMMI: “The Innovation Center”
• Other key characteristics in the statute for payment models– Varying payment for advanced diagnostic imaging services– Medication therapy management services– Community-based health teams to assist in care management– Patient decision-support tools– State flexibility for dual-eligibles and all-payer payment reform
demonstrations– Collaboratives of high-quality, low-cost institutions
• $10 billion over 10 years funding
25
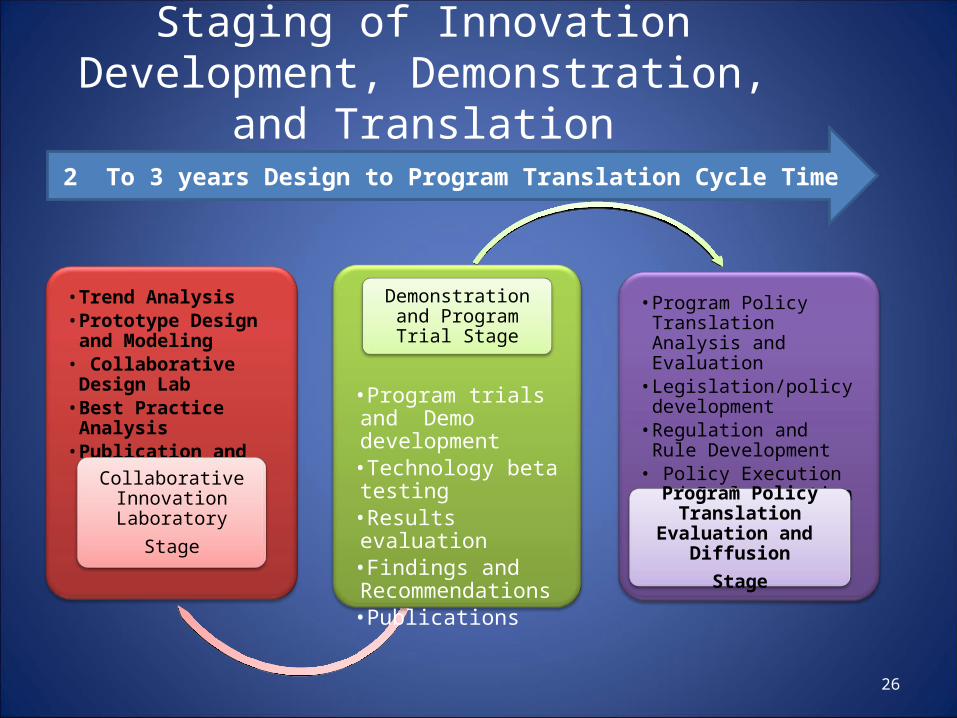
Staging of Innovation Development, Demonstration, and Translation
26
• Trend Analysis• Prototype Design and
Modeling• Collaborative Design Lab• Best Practice Analysis• Publication and
Collaborative Learning
Collaborative Innovation Laboratory
Stage
•Program trials and Demo development
•Technology beta testing
•Results evaluation•Findings and Recommendations
•Publications
Demonstration and Program Trial Stage
• Program Policy Translation Analysis and Evaluation
• Legislation/policy development
• Regulation and Rule Development
• Policy Execution and Implementation
• Re Evaluation/ Publication
Program Policy Translation Evaluation and Diffusion
Stage
2 To 3 years Design to Program Translation Cycle Time

Accountable Care
Coordinated Care
• Organized care delivery– Aligned incentives– Linked by HIT
• Integrated Provider Networks
• Focus on cost avoidance and quality performance
– PC Medical Home– Care management– Transparent Performance
Management
IntegratedHealth
Patient Centered
• Patient Care Centered– Personalized Health Care– Productive and informed interactions
between Patient and Provider– Cost and Quality Transparency – Accessible Health Care Choices– Aligned Incentives for wellness
• Multiple integrated network and community resources
• Aligned reimbursement/care management outcomes
• Rapid deployment of best practices
• Patient and provider interaction– Information focus– Aligned self care management– E-health capable
• Fee For Service– Inpatient focus– O/P clinic care– Low Reimbursement– Poor Access and Quality– Little oversight
• No organized networks
• Focus on paying claims
• Little Medical Management
Un-managed
Driving Healthcare SystemTransformation
27
Fee for Service

Driving Healthcare Delivery System Reform and
Transformation 2011-2019
28
2011-2019
2012-2019
2014-2019

CMMI Programs• ACO Programs• Bundled Payment• Comprehensive Primary Care
Initiative• Financial Alignment Initiative• FQHC Advanced Primary
Practice Demonstration• Graduate Nurse Education
Demonstration• Health Care Innovation
Awards• Independence at Home
Demonstration
• Initiative to Reduce Avoidable Hospitalizations Among Nursing Home Residents
• Innovations Advisors Program• Medicaid Emergency Psychiatric
Demonstration• Medicaid Incentives for the
Prevention of Chronic Diseases• Million Hearts• Partnership for Patients: Care
Transitions: Community-based• State Innovations Models• Strong Start for Mothers &
Newborns29

Accountable Care Organizations (ACOs)• Medicare Shared Savings Program (Section 3022)
– Implementation of the Medicare ACO Program mandated by January 1, 2012
– Encourages multiple providers of services and supplies to:• Join together and create ACOs• Be jointly accountable for health & experience of
care for individuals over a period of time• Improve population health, overlap with community• Reduce rate of healthcare spending, improve quality
30

CMS ACO Proposed Rule• ACO Notice of Proposed Rulemaking (NPRM) issued
March 31, 2011• An ACO is an organization of healthcare providers that
agrees to be accountable for the quality, cost, and overall care of assigned Medicare beneficiaries who are enrolled in Medicare FFS
• Eligible organizations– Physicians in group practice arrangements– Physicians in networks of practices– Partnerships or joint venture arrangements between physicians
and hospitals– Hospitals employing physicians– Other forms that the HHS Secretary deems appropriate 31

Reaction to ACO NPRM• Largely negative
– Too complicated, too restrictive– Too much undefined risk– No specialty-focused ACOs– Negative comments about each criteria component
• CMS responded in interim– Pioneer ACO Model– Advance Payment ACO Model– Accelerated Development Learning Sessions
• Final rule issued November 2, 2011: Many revisions, less complicated, more options
32

33
What’s An Accountable Care Organization?

34
What’s An Accountable Care Organization?

CMS ACO Status Update• Medicare Shared Savings Program ACOs: 153
– 27 named in April, 2012– 88 named in July, 2012– 32 Pioneer ACOs– 6 Physician Group Practice Demo
• Half are physician-driven groups serving < 10,000 patients• Serve 2.4 million Medicare beneficiaries• 33 Quality Measures
– Care coordination and patient safety– Preventive health services– Improved care for at-risk populations– Patient and caregiver experience of care
35

Overall U.S. ACO Status Report• The number and types of ACOs are expanding• Growth is centered in larger population centers• Hospital systems appear to be the primary
backers of ACOs, but physician groups are playing an increasingly larger role
• Non-Medicare ACOs are experimenting with more diverse models than Medicare-backed ACOs
• The success of any particular ACO model is still undetermined
36Source: Leavitt Partners report “Growth and Dispersion of Accountable Care Organizations, May 2012

37Source: Leavitt Partners report “Growth and Dispersion of Accountable Care Organizations, May 2012

38
Source: Leavitt Partners report “Growth and Dispersion of Accountable Care Organizations, May 2012

39
Source: Leavitt Partners report “Growth and Dispersion of Accountable Care Organizations, May 2012

40Source: Leavitt Partners report “Growth and Dispersion of Accountable Care Organizations, May 2012

ACA: Academic Health Systems• ACA Section 3025: Hospital Readmission Reduction
Program• ACA Section 3026: Community Based Care Transition
Program• Healthcare Delivery Research (Section 3501, AHRQ
coordinating with CMS)– Identifies best practice institutions, organizations, etc.– Supports innovation in health care delivery system
improvement
• Quality Improvement Technical Assistance (Section 3501)
41

ACA: Academic Health Systems• Establishing Community Health Teams to Support the
Patient-Centered Medical Home (Section 3502)• Medication Management Services in the Treatment of
Chronic Diseases (Section 3503)• Emergency medicine regionalized systems and research,
trauma care centers access & payment• Demonstration to integrate quality improvement and
patient safety education into healthcare worker education (Section 3508)
• National Health Care Workforce Commission (Section 5101)– Recruitment, education and training, retention
42

ACA: Academic Health Systems• National Center for Health Care Workforce
Analysis (Section 5103)• Multiple student loan programs, various training
& retention programs, & demonstration programs established– Primary care– Nurse-led care, advanced practice nursing, etc.– Allied health, public health, dental, pediatric, direct
care professionals, geriatric, mental health, cultural competency in disabilities, mid-career, etc.
43

ACA: Academic Health Systems• United States Public Health Services Track (Part D,
Section 271)• Centers of Excellence-additional funding• Medical Residency funding enhancements• Teaching grants and demonstrations in graduate
medical education• The list goes on and on and on…….• But………, will ACA survive the legal, political and
funding challenges in its entirety?– If not, which sections?– Whether or not, will savings estimates be achieved?
44

Conclusions• The Affordable Care Act provides innumerable
opportunities to improve the quality, value and efficiency of healthcare in the United States
• CMS/HHS is a major implementation center for this historic piece of legislation, but the private sector has an equally important role– Individual integrated health systems, particularly those
with a focus on innovation and evidence, are essential to the success of healthcare reform
– Implementation affects fee-for-service as well as managed care models, plus untested new models
45

Conclusions• There are numerous opportunities and needs for
involvement of integrated/academic health systems in implementation of ACA and further health reform in the future:– Design of and leadership in contemporary quality
improvement initiatives• Huge gap in comparative- & cost-effective
analysis/improvement, let alone basic clinical knowledge
– Ongoing input in review and improvement in clinical guidelines
• Balancing evidence-based population RCT viewpoint with need for individual patient-centered concerns
46

Conclusions• Additional roles for integrated/academic health systems:
– Education of multiple audiences in evidence-based medicine use:
• Clinicians: Current/future, academic/community• Policy makers• Payers• Patients, consumers and their families
– Development and use of quality and value metrics• Multiple perspectives: Clinicians, patients, payers, etc.• Relevance, actionability, accountability, attribution
– Alignment/integration of traditional & community healthcare resources and models 47

Conclusions• Additional roles for integrated/academic health
systems:– Collection, analysis, reporting and use of healthcare data
• Health Information Technology development, adoption and “meaningful use” via EHRs
• Other forms of data collection: Registries, claims, encounter data, telehealth, chart review, surveys, etc.
• Balance of scientific rigor vs.. “information efficiency”• Minimization of burden• Privacy & security• Dissemination of data for widest possible appropriate use
48
Conclusions• Additional roles for integrated/academic
health systems:– Development of and participation in new
reimbursement and delivery systems• Higher quality leading to overall lower costs• Innovation, rapid change & adaptability• Care transitions and coordination• Integration of delivery systems• Patient-Centered, all of IOM Quality Aims• Public health focus, as well as individual health
49

Conclusions• We cannot continue to cover and pay for everything
that’s available without considering:– Evidence-based coverage & payment decision
making– Comparative effectiveness and cost effectiveness
analysis– Overall costs involved, including global costs of lost
productivity, quality of life, etc.• But are Academic Health Systems ready?
– Rapid-cycle change, integrated systems (no departmental silos), authenticity & will to change (e.g., academic tenure?)
50

Conclusions• The under-emphasized topics (?ignored):
– End-of-life care– Health disparities reduction: Action needed, not talk
• Racial/ethnic• Geographic• Age• Gender• Socioeconomic• LGBT• Medical Conditions
51

Thank you for your contributions in improving the American healthcare
system!
Questions?Discussion & Dialogue
52


















