
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, PATHOGENESIS & PREVENTION 2014 David Jay Weber, M.D.,...
79
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, PATHOGENESIS & PREVENTION 2014 David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health Care Medical Director, Hospital Epidemiology University of North Carolina at Chapel Hill
-
Upload
toby-quinn -
Category
Documents
-
view
221 -
download
2
Transcript of HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, PATHOGENESIS & PREVENTION 2014 David Jay Weber, M.D.,...

HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY,
PATHOGENESIS & PREVENTION 2014
David Jay Weber, M.D., M.P.H.
Professor of Medicine, Pediatrics, & Epidemiology
Associate Chief Medical Officer, UNC Health Care
Medical Director, Hospital Epidemiology
University of North Carolina at Chapel Hill

HAZARDS IN THE ICU
Weinstein RA. Am J Med 1991;91(suppl 3B):180S


TOPICS: HCAP, HAP, VAP
Epidemiology Impact of healthcare-associated infections Definitions NHSN surveillance definitions Incidence and prevalence of HCAP, HAP, VAP
Pathogenesis Mechanisms of pneumonia Microbiology Risk factors Diagnosis
Prevention
GOALS OF LECTURE
Understand the epidemiology of nosocomial pneumonia Impact Incidence Risk factors for acquisition and mortality
Understand the pathophysiology of HAP & VAP Microbiology Diagnosis Treatment
Understand methods of prevention

Marrow LE, Kollef MH. Crit Care Med 2010;38[suppl]:S352-S362

Chroneou A, et al. Expert Opinion 2007;8:3117-31


HEALTHCARE-ASSOCIATED PNEUMONIA
HAI An infection is considered an HAI if ALL elements of a CDC/NHSN
site-specific criterion were first present together on or after the 3rd hospital day (day of admission is Day 1). For an HAI, an element of the infection criterion must be present during the first 2 hospital days as long as it is also present on or after Day 3. All elements used to meet the infection criterion must occur within a timeframe that does not exceed a gap of 1 calendar day between elements
Pneumonia (PNEU) Pneumonia is identified using a combination of radiologic, clinical and
laboratory criteria. For VAP the date of the event is the date when the last element used to meet the pneumonia criteria are occurred.
http://www.cdc.gov/nhsn/acute-care-hospital/vae/index.html

VENTILATOR-ASSOCIATED EVENT(adult patients >18 years of age
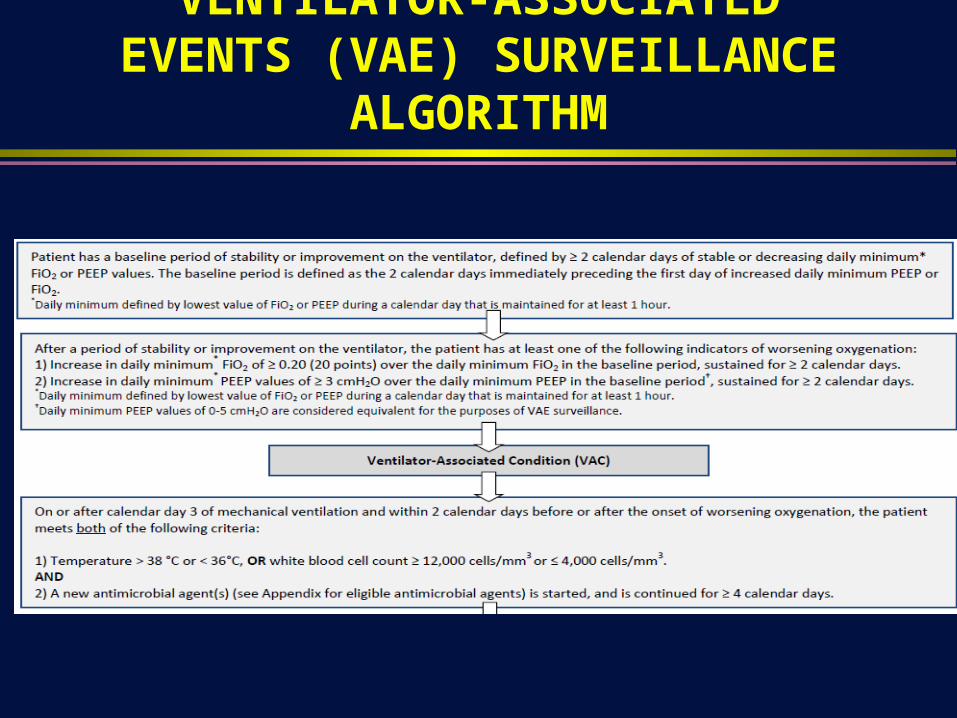
VENTILATOR-ASSOCIATED EVENTS (VAE) SURVEILLANCE ALGORITHM


VENTILATOR-ASSOCIATEDCONDITION (VAC)

INFECTION-RELATED VENTILATOR-ASSOCIATED COMPLICATIONS (IVAC)

POSSIBLE VENTILATOR-ASSOCIATED PNEUMONIA (VAP)

PROBABLE VENTILATOR-ASSOCIATED PNEUMONIA (VAP)

THRESHOLD VALUES FOR CULTURED SPECIMENS USED IN THE PROBABLE VAP DEFINITION

NHSN DEFINITIONS OF HAP AND VAP (children, <18 years of age)
Table 1. Specific site algorithms for clinically defined pneumonia (PNU1)
Table 2. Specific site algorithms for pneumonia with common bacterial or filamentous fungal pathogens and specific laboratory findings (PNU2)
Table 3. Specific site algorithms for viral, Legionella, and other bacterial pneumonias with definitive laboratory findings (PNU2)
Table 4. Specific site algorithm for pneumonia in immunocompromised patients (PNU3)

Marrow LE, Kollef MH. Crit Care Med 2010;38[suppl]:S352-S362

PNU1

PNU2

PNU2

PNU3

HAP & VAP: IMPACT
Potential complications of mechanical ventilation Pneumonia, acute respiratory distress syndrome (ARDS), pulmonary
embolism, barotrauma, pulmonary edema, and death
Complications result in longer ICU stays, increased costs, and increased risk of disability and death Mortalioty in patient with acute lung injury, estimated to range from 24% in
patients 15-19 years of age to 60% for patients >85 years of age Prevalence: 2010 NHSN = 3,525 cases of VAP Incidence: 2010 NHSN = 0.0-5.8 per 1,000 ventilator days

Magill SS, et al. New Engl J Med 2014;370:1198

HAP: IMPACT
Accounts for ~15% of all healthcare-associated infections (3rd most common cause of HAIs after UTIs and SSIs) Accounts for ~25% of all nococomial infections in the ICU (50%
of antibiotics provided) Number of cases per year: ~275,000 Prevalence
VAP develops in 10% to 20% of mechanically ventilated patients
VAP rate = 1-4 cases/1,000 ventilator-days

HAP: IMPACT
Cost Increases hospital stay by an average of 7-11 days Cost per patient >$40,000 Direct cost (estimated) of excess hospital stays = $1.5 billion/year
Mortality Crude mortality: 30-70% (average 40%) Attributable mortality: 33-50%
Deaths Deaths directly caused by infection: 7,085 (3.1%) Deaths to which infection contributed: 22,983 (10.1%)
PREVALENCE: ICU (EUROPE)
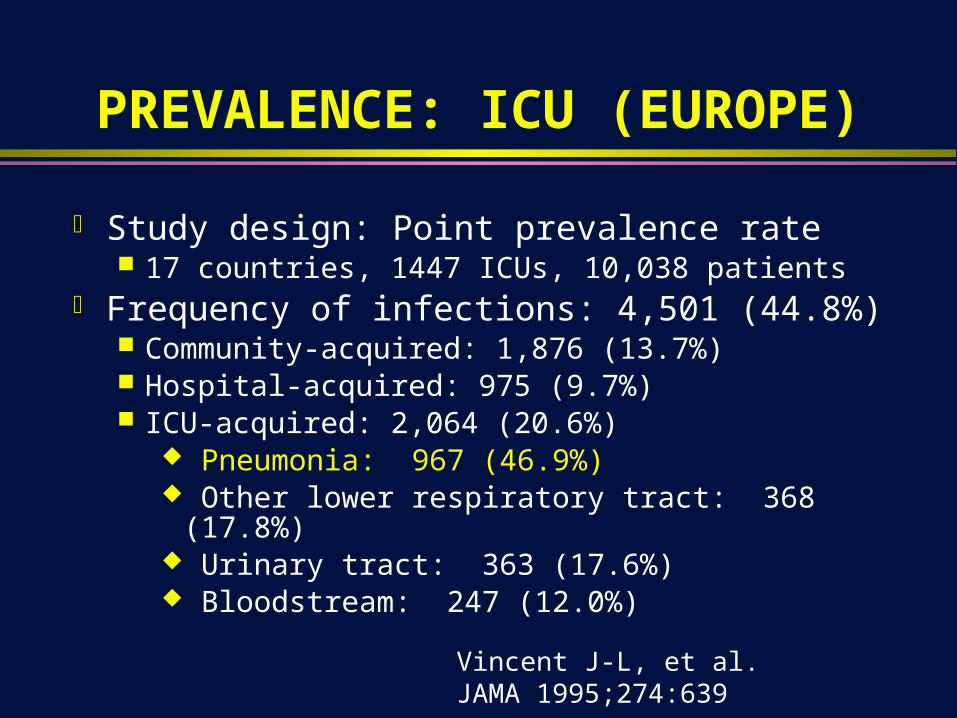
Study design: Point prevalence rate 17 countries, 1447 ICUs, 10,038 patients
Frequency of infections: 4,501 (44.8%) Community-acquired: 1,876 (13.7%) Hospital-acquired: 975 (9.7%) ICU-acquired: 2,064 (20.6%)
Pneumonia: 967 (46.9%) Other lower respiratory tract: 368 (17.8%) Urinary tract: 363 (17.6%) Bloodstream: 247 (12.0%)
Vincent J-L, et al. JAMA 1995;274:639

PREVALENCE: ICU (WORLDWIDE) Study design: Point prevalence, 8 May 2007
75 countries, 1265 ICUs, 13,796 adult patients Frequency of infections: 7,087 (51%)
Sites of infectionRespiratory tract:: 4,503 (63.5%)Abdominal: 1,392 (19.6%)Bloodstream: 1,071 (15.1%)Renal/urinary tract: 1,011 (14.3%)
Antibiotic therapy: 71% Pathogens of infected patients: 47% GPC, 62% GNR, 19% fungi Infected patients had higher ICU (25.3% vs 10.7%) and hospital
mortality (33.1% vs 14.8%)
Vincent J-L, et al. JAMA 2009;302:2333-2329

VENTILATOR-ASSOCIATED PNEU RATES, NHSN, 2012
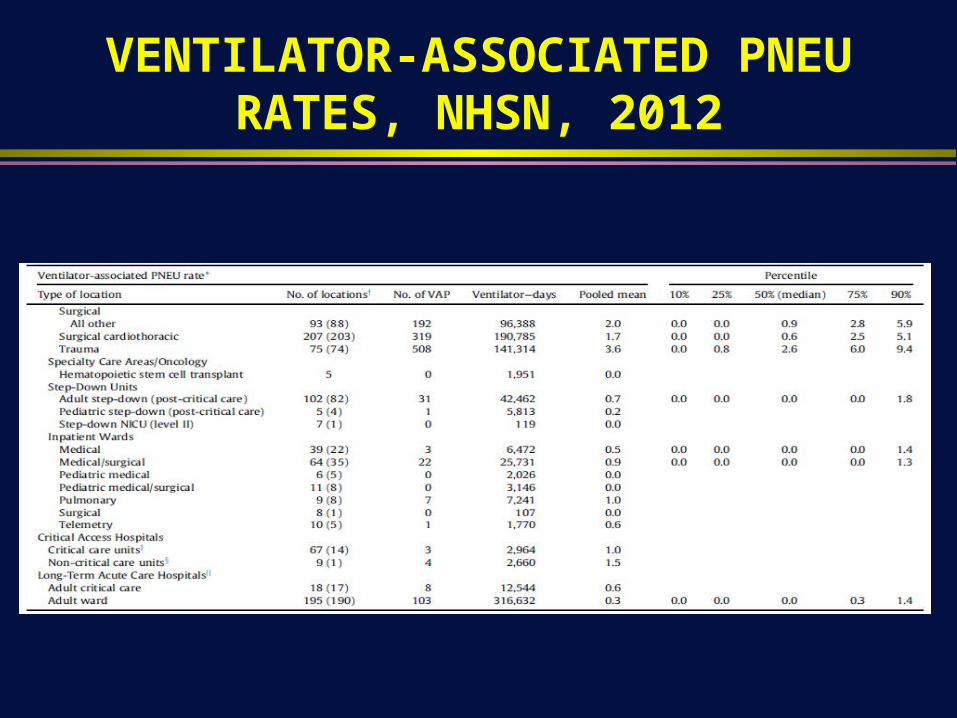
VENTILATOR-ASSOCIATED PNEU RATES, NHSN, 2012

VAP: TIME COURSE
Cumulative Incidence ICU VAP
0%
10%
20%
30%
40%
50%
60%
5 10 15 20 25 30
Garrard C. Chest 1995;108:17S
Days

VAP: TIME COURSE
Mean Daily Risk Of VAP
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
0-5 6-136 11-15 16-20 21-25 26-30
Days


TOP 7 PATHOGENS ASSOCIATED WITH VAP: NHSN, 200
0% 5% 10% 15% 20% 25% 30%
Other
Serratia spp.
E. coli
Acinetobacter
Enterobacter spp.
Klebsiella pneumoniae/oxytoca
P. aeruginosa
S. aureus
Sievert DM. ICHE 2013; 34;1-14

Pathogen NNIS INVASIVE DXS. aureus (ORSA 55.7%) 19% 20.4%S. Pneumoniae NA 4.1%Streptococcus spp. 3% 8.0%Coagulase-negative staphylococcus 2% 1.4%Enterobacteriaceae 26% 14.15Pseudomonas aeroginosa 17% 24.4%Acinetobacter spp. 4% 7.9%Stenotrophomonas maltophilia <1% 1.7%Hemophilus spp. 7.1% 9.8%Neisseria spp. <1% 2.6%Anaerobes 2% 0.9%Fungi 7% 0.9%Other (<1% each) 3.8%
ETIOLOGIC AGENTS ASSOCIATED WITH HAP: NNIS vs INVASIVE DX
Chastre J, Fagon J-Y. Am J Respir Crit Care Med 2002;165:867-903

MICROBIOLOGY
Determinants of pathogens Setting Prior antibiotic use Duration of hospitalization
Early (<5 days): S. pneumoniae, H. influenzae, MSSA Late (>5 days): P. aeruginosa, MRSA, Gram (-) bacilli
ICU stay Colonization
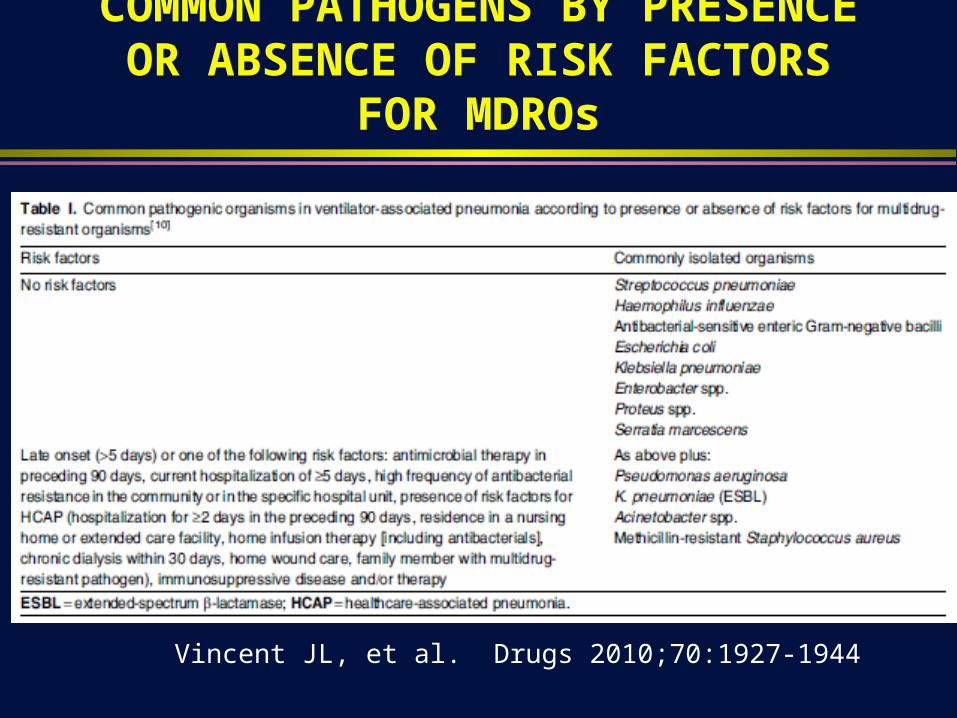
COMMON PATHOGENS BY PRESENCE OR ABSENCE OF RISK FACTORS FOR MDROs
Vincent JL, et al. Drugs 2010;70:1927-1944

Weber DJ, et al. ICHE 2007;28:825-831

ICU (NNIS, 1989-99): Ventilator-Associated Pneumonia
Fridkin SK. Crit Care Med 2001;29:N67
Open bars <7 days hospitalizationClosed bars >7 days hospitalization

PATHOGENS AS A FUNCTION OF DURATION OF HOSPITALIZATION
Weber DJ, et al. ICHE 2007;28:825-831

Antibiotic-Resistant VAP
Prior MV>7 days 60.009
Prior ABs 13<0.001
Broad ABs 40.025
0
5
10
15
20
25
–/– –/+ +/– +/+
MV>7 Days/Prior Antibiotics
Org
an
ism
(%
)
P aeruginosaAcinetobacter baumanniiMRSA
MV = Mechanical ventilation.MRSA = Methicillin-resistant S aureus.
Trouillet JL, et al. Am J Respir Crit Care Med. 1998;157:531-539.
Variable OddsRatio P Value

PATHOGENESIS
Colonization, aspiration, pneumonia in the setting of impaired host defenses
Inhalation Instillation Bacteremic spread Contiguous spread

Kollef MH, et al. Chest 2004;32:1396

VAP: RISK FACTORS
Intrinsic Risk Factors Chronic lung disease/COPD Severity of illness ARDS Witnessed aspiration Age >60 years Coma Head trauma/ICP monitoring Upper abdominal surgery Thoracic surgery Fall-winter season
Extrinsic Risk Factors Duration of intubation Emergent intubation Reintubation Elevated gastric pH Prior antibiotic therapy Nasogastric tube Enteral nutrition Supine head position Patient transport out of ICU
Kollef M. Crit Care Med 2004;32:1396 (adapted)

%Hospital Mortality by Classification
0
5
10
15
20
25
30
CAP HCAP HAP VAP
Kollef MH, et al. Chest 2005;128:3854
10.0 19.8 18.8 29.3
P > 0.05
P < 0.0001
P < 0.001

METHODS OF DIAGNOSIS
Clinical findings (symptoms, signs) Blood, pleural fluid analysis & cultures, tissue diagnosis Non-bronchoscopic
Endotracheal aspiration Percutaneous needle aspiration Blind bronchial sampling (“Blind” BAL)
Bronchoscopic techniques Protected specimen brush (PSB) Bronchoalveolar lavage (BAL)

CLINICAL DIAGNOSIS
Symptoms and signs: Fever, respiratory distress Chest radiography: Infiltrate, consolidation, cavity Laboratory: Leukocytosis, leukopenia Sputum: Purulence (WBC), culture Clinical diagnosis (ATS/IDSA)
New or progressive infiltrate >2 of the following: Temperature >38 oC, leukocytosis or
leukopenia, purulent secretions

DIFFERENTIAL DIAGNOSIS:FEVER AND PULMONARY INFILTRATES
Pulmonary infection Pulmonary embolism Pulmonary drug reaction Pulmonary hemorrhage Chemical aspiration Sepsis with acute respiratory distress syndrome Drug reaction

DIAGNOSING VAP PNEUMONIAD IAG N O SIN G NO SO C O M IA L PN EU M O NIA (M eduri G , et al. Chest 1994;106:221)
50patients completed
the study
14concomitant
infections
19pneumonia
11concomitant
infections
14sinusitis
catheter infectionurinary tract infection
0concomitant
infections
candidemiacholecystitis
empyemaperitonitis
37infectious
5 fibroproliferation1 chemical aspiration
6pulmonary
1 pancreatitis1 drug fever
2extra-pulmonary
8noninfectious only
45patients with a
definitive sourceof fever identified

INDICATIONS FOR INVASIVE DIAGNOSIS
Routine for all patients with possible nosocomial pneumonia?
Targeted use of invasive diagnosis Critically ill Immunocompromised patient (esp. T-cell defect) Deterioration on empiric therapy Failure to respond to empiric therapy Other therapeutic consideration (e.g., foreign-body)


PROTECTED SPECIMEN BRUSH

BRONCHOALVEOLAR LAVAGE

Meta-analysis of Invasive Strategies for the Diagnosis of Ventilator-Associated Pneumonia & their Impact on Mortality*
Odds Ratio for Mortality
*Random effects model; Test of heterogeneity p=0.247, for Odds ratio p=0.620
0.13 1 7.84
Study % Weight Odds Ratio
(95% CI)
2.42 (0.75,7.84) Sanchez-Nieto, et al. 13.0 0.71 (0.28,1.77) Ruiz, et al. 19.5 0.71 (0.47,1.06) Fagon, et al. 50.9 1.08 (0.39,2.98) Violan, et al. 16.5
0.89 (0.56,1.41) Overall (95% CI)
Favors InvasiveApproach
Favors Non-InvasiveApproach
Shorr A, Kollef. MH Crit Care Med 2005;33:46.

Morrow LE, Kollef MH. Crit Care Med 2010;38[suppl]:S352-352

EMPIRIC THERAPY: GENERAL RULES
Know the flora and susceptibilities of the pathogens causing nosocomial pneumonia at your own institution
Obtain history of antibiotic-allergies from all patients (adjust regimen appropriately)
Choose empiric therapy to minimize drug interactions Dose adjust (when appropriate) in patients with renal and/or hepatic
failure Consider specific contraindications or precautions (e.g., pregnancy,
neuromuscular disease) All other things being equal use the least expensive therapy Provide appropriate non-antibiotic care

IMPACT OF ANTIMICROBIALSIMPACT OF ANTIMICROBIALS
0
10
20
30
40
50
60
Hospital Mortality
%
All Cause Infection-related
Inadequate Therapy n = 169
Adequate Therapy n = 486
Kollef Chest 115:462, 1999

HAP: The Importance of Initial Empiric Antibiotic Selection
Alvarez-Lerma F. Intensive Care Med 1996 May;22(5):387-394. Rello J, Gallego M, Mariscal D, et al. Am J Respir Crit Care Med 1997 Jul;156(1):196-200.Luna CM, Vujacich P, Niederman MS, et al. Chest 1997;111(3):676-685.Kollef MH and Ward S. Chest 1998 Feb;113(2):412-20.Sanchez-Nieto JM, Torres A, Garcia-Cordoba F, et al. Am J Respir Crit Care Med. 1998;157:371-376.Ruiz M, Torres A, Eqig, S, et al. Am J Respir Crit Care Med. 2000;162:119-125.Dupont H, Mentec H, Sollet, JP, et al. Intensive Care Med. 2001;27(2):355-362 61
16.2
41.538
33.3
25
39
47.3
24.7
63
91
61.4
4350
60.7
0
20
40
60
80
100
Alvarez-Lerma
Rello Luna Kollef Sanchez-Nieto
Ruiz Dupont
% m
ort
ality
Adequate init. antibiotic Inadequate init. antibiotic
P=NS P=NSP=NSP=NSP=0.001P<0.001P=0.06

ATS/IDSA. Am J Respir Crit Care Med 2005;171:388-416

ATS/IDSA. Am J Respir Crit Care Med 2005;171:388-416

Vincent J-L, et al. Drugs 2010;70:1927-1944

ATS/IDSA. Am J Respir Crit Care Med 2005;171:388-416
DURATION OF THERAPY: STUDY DESIGN
Authors: Chastre J, et al. JAMA 2003;290:2988 Study goal: Compare 8 vs 15 days of therapy for VAP Design: Prospective, randomized, double-blind (until day 8),
clinical trial VAP diagnosed by quantitative cultures obtained by bronchoscopy
Location: 51 French ICUs (N=401 patients) Outcomes: Assessed 28 days after VAP onset (ITT analysis)
Primary measures = death from any cause Microbiologically documented pulmonry infection recurrence Antibiotic free days

DURATION OF THERAPY: RESULTS
Primary outcomes (8 vs 15 days) Similar mortality, 18.8% vs 17.2% Similar rate of recurrent infection, 28.9% vs 26.0%
MRSA, 33.3% vs 42.9% Nonfermenting GNR, 40.6% vs 25.4% (p<0.05)
More antibiotic free days, 13.1% vs 8.7% (p<0.001) Secondary outcomes (8 vs 15 days)
Similar mechanical ventilation-free days, 8.7 vs 9.1 Similar number of organ failure-free days, 7.5 vs 8.0 Similar length of ICU stay, 30.0 vs 27.5 Similar frequency death at day 60, 25.4% vs 27.9% Multi-resistant pathogen (recurrent infection), 42% v 62% (p=0.04)

THERAPY: SUMMARY I
Negative lower respiratory tract cultures can be used to stop antibiotic therapy if obtained in the absence of an antibiotic change in past 72 hours
Early, appropriate, broad spectrum therapy, antibiotic therapy should be prescribed with adequate doses to optimize antimicrobial efficacy
An empiric therapy regimen should include agents that are from a different antibiotic class than the patient is currently receiving
De-escalation of antibiotic should be considered once data are available on the results of the patient’s cultures and clinical response
A shorter duration of therapy (7-8 days) is recommended for patients with uncomplicated HAP, VAP, or HCAP who have had a good clinical response

THERAPY: SUMMARY III
High risk patients Multiple-drug regimens required Combine beta-lactam with aminoglycoside (preferred)
or quinolone (levo or cipro) Consider need for coverage of oxacillin-resistant S.
aureus, Legionella

THERAPY: SUMMARY IV
Bronchoscopy directed therapy May improve outcome
Demonstrated by a randomized study Several cohort studies have failed to demonstrated benefit
Mortality reduced by initial use of appropriate antibiotics Duration of therapy, in general, should be 7-8 days

Kollef M. Chest 2004;32:1396

Morrow LE, Kollef MH. Crit Care Med 2010;38[suppl]:S352-352

Morrow LE, Kollef MH. Crit Care Med 2010;38[suppl]:S352-352

STRENGTH OF RECOMMENDATIONSAND QUALITY OF EVIDENCE

STRATEGIES TO PREVENT VAPIN ACUTE CARE HOSPITALS
Surveillance Definition of VAP most subjective of all device associated HAIs Significant intra-observer variability exists Use active surveillance (not administrative data alone) Ideally perform semiquantitative culture of endotracheal
secretions or quantitative culture of BAL fluid Prevention
Follow CDC guidelines to prevent VAP Interrupt most common mechanisms by which VAP develops
Aspiration of secretionsColonization of the aerodigestive tractUse of contaminated equipment
Coffin SE, et al. ICHE 2008;29 (suppl 1):S31-S40

STRATEGIES TO PREVENT VAPIN ACUTE CARE HOSPITALS
Prevention: General strategies Conduct active surveillance Adhere to hand hygiene recommendations Use non-invasive ventilation whenever possible Minimize the duration of ventilation Perform daily assessments of readiness to wean Educate personnel regarding prevention
Prevention: Strategies to prevent aspiration Maintain patients in a semirecumbent position (30o-45o
elevation) Use a cuffed ET tube with in-line or subglottic suctioning
Coffin SE, et al. ICHE 2008;29 (suppl 1):S31-S40

STRATEGIES TO PREVENT VAPIN ACUTE CARE HOSPITALS
Prevention: Strategies to reduce colonization Orotracheal intubation preferred to nasotracheal intubation Avoid acid suppressive therapy Perform oral care with an antiseptic solution
Prevention: Strategies to minimize contamination Use sterile water to rinse reusable respiratory equipment Remove condensate from the ventilatory circuit Change the ventilatory circuit only when visibly soiled or
malfunctioning Store and disinfect respiratory equipment properly
Coffin SE, et al. ICHE 2008;29 (suppl 1):S31-S40

STRATEGIES TO PREVENT VAPIN ACUTE CARE HOSPITALS
Special approached for the prevention of VAP Use an ET tube with in-line and subglottic suctioning
Approaches that should not be routinely used Do not routinely administer IVIG, GM-CSF, or chest physiotherapy Do not routinely use rotational therapy with kinetic or continuous
lateral rotational therapy beds Do not routinely administer prophylactic aerosolized or systemic
antimicrobials Unresolved issues
Selective digestive tract decontamination Avoidance of H2 antagonists or proton pump inhibitors Use of antiseptic-impregnated ET tubes
Coffin SE, et al. ICHE 2008;29 (suppl 1):S31-S40

IHI GUIDELINE: VAP BUNDLE
Elevation of the head of the bed to between 30 and 45 degrees
Daily “sedation vacation” and daily assessment of readiness to extubate
Peptic ulcer disease (PUD) prophylaxis Deep venous thrombosis (DVT) prophylaxis (unless
contraindicated)

CONCLUSIONS I
Nosocomial pneumonia remains an important cause of patient morbidity and mortality in the US
Nosocomial pneumonia results in a more prolonged hospital stay and increased cost
Local epidemiology of pathogens and antibiograms are critical to empiric and directed chemotherapy
Determining the etiologic agent(s) of nosocomial pneumonia is problematic even with new invasive diagnostic techniques
CONCLUSIONS II
Use of empiric, broad-spectrum regimens remain critical to favorable patient outcomes
Single-drug regimens may be appropriate for some low-risk patients, but two-drug regimens with broad spectrum (including P. aeruginosa) are necessary for high-risk patients
Prevention is superior to treatment


















