
Health and Medical Subpanel Pan Flu Advisory Committee Karen Remley, MD, MBA, FAAP State Health...
64
Health and Medical Subpanel Pan Flu Advisory Committee Karen Remley, MD, MBA, FAAP State Health Commissioner Mark J. Levine, MD, MPH Deputy Commissioner, Emergency Preparedness January 12, 2010 Virginia Housing Center The 2009 H1N1 influenza pandemic in Virginia
-
Upload
beryl-curtis -
Category
Documents
-
view
216 -
download
1
Transcript of Health and Medical Subpanel Pan Flu Advisory Committee Karen Remley, MD, MBA, FAAP State Health...

Health and Medical SubpanelPan Flu Advisory Committee
Karen Remley, MD, MBA, FAAPState Health CommissionerMark J. Levine, MD, MPHDeputy Commissioner, Emergency
Preparedness
January 12, 2010Virginia Housing Center
The 2009 H1N1 influenza pandemic in Virginia

U.S. Department of Health and Human Services H1N1 Response Pillars
• Surveillance• Communication • Vaccination• Mitigation
Virginia addition• Direct Medical Care / Surge

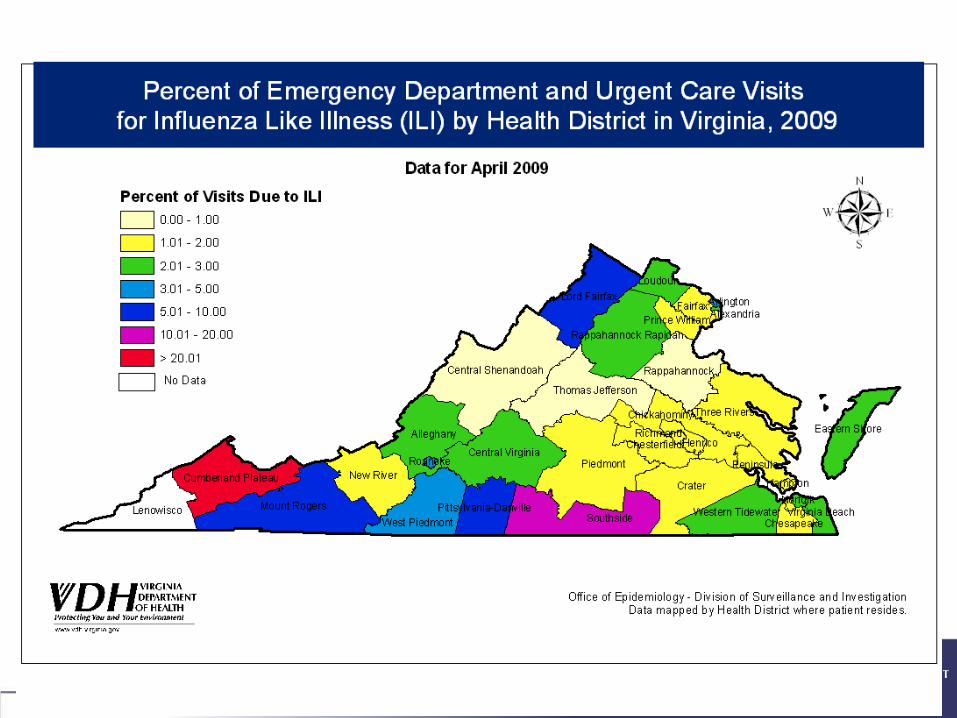
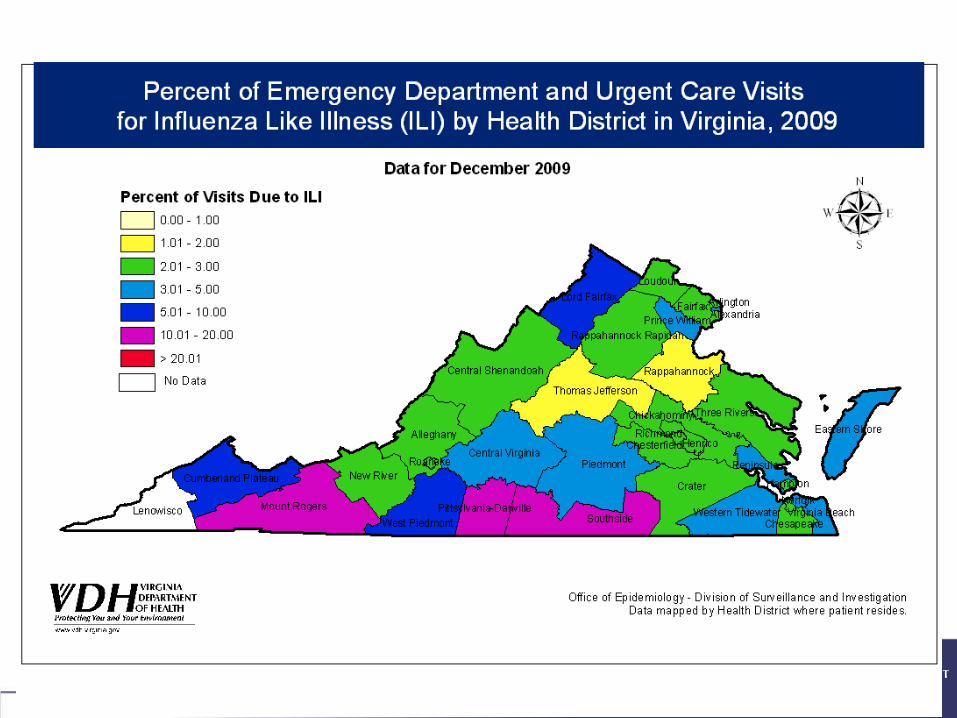
Surveillance:Monitoring Flu Activity in Virginia
ED/UC visits for flu-like illness (ILI)• By age group, region
Lab surveillanceOutbreaks reportedDeaths confirmed*School absences*School and day care closures*
* New for 2009 H1N1

Visits for ILI, Virginia
0
2
4
6
8
10
12
14
16
Week Ending Date
Pe
rce
nt
of
Vis
its
fo
r IL
I
2007-08 2008-09 2009-10
Percent of Emergency Department and Urgent Care Visits for Influenza-like Illness (ILI) by Week, Virginia, 2009-10 Influenza Season Compared with the Previous Two Seasons

0.0
5.0
10.0
15.0
20.0
25.0
30.0
Week Ending Date
Pe
rce
nt
of
Vis
its
fo
r IL
I
0-4 5-24 25-49 50-64 65+ All Ages
Percent of Emergency Department and Urgent Care Visits for Influenza-like Illness (ILI)by Age Group, Virginia, 2008-09 and 2009-10 Influenza Seasons
ILI Visits by Age Group

Laboratory Surveillance
Reports to VDH from all sources• DCLS• Private laboratories• Sentinel providers (ED, hospital, MD practice)
3428 positive flu results have been reported since August 1, 2009
3418 (99.7%) are 2009 H1N1 or A/unknown
The other 10 were: one H3 in October, 2 seasonal H1 in August, 3 seasonal A in Oct and 1 in December, and 2 B in August and 1 in October.
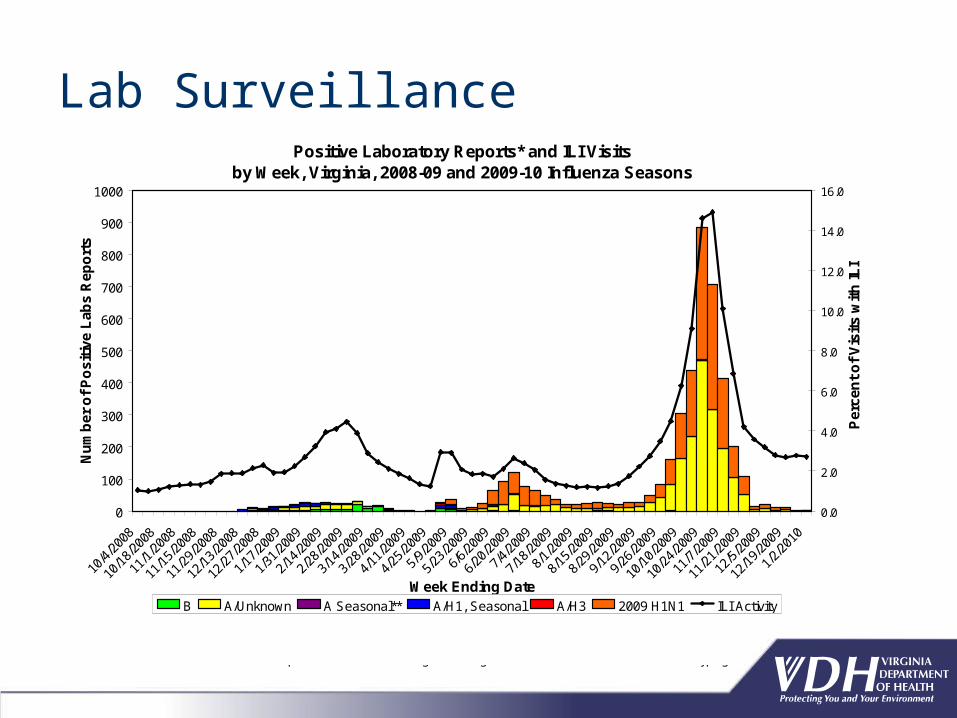
Lab SurveillancePositive Laboratory Reports* and ILI Visits
by Week, Virginia, 2008-09 and 2009-10 Influenza Seasons
0
100
200
300
400
500
600
700
800
900
1000
10/4
/200
8
10/1
8/20
08
11/1
/200
8
11/1
5/20
08
11/2
9/20
08
12/1
3/20
08
12/2
7/20
08
1/17
/200
9
1/31
/200
9
2/14
/200
9
2/28
/200
9
3/14
/200
9
3/28
/200
9
4/11
/200
9
4/25
/200
9
5/9/
2009
5/23
/200
9
6/6/
2009
6/20
/200
9
7/4/
2009
7/18
/200
9
8/1/
2009
8/15
/200
9
8/29
/200
9
9/12
/200
9
9/26
/200
9
10/1
0/20
09
10/2
4/20
09
11/7
/200
9
11/2
1/20
09
12/5
/200
9
12/1
9/20
09
1/2/
2010
Week Ending Date
Nu
mb
er o
f P
osi
tive
Lab
s R
epo
rts
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
Per
cen
t o
f V
isit
s w
ith
ILI
B A/Unknown A Seasonal** A/H1, Seasonal A/H3 2009 H1N1 ILI Activity
*Positive laboratory reports are presented by week of specimen collection. Data are added as new test results become available; therefore, information for the most recent week will always be incomplete.
** 'A Seasonal' indicates a positive Influenza A finding that is negative for Novel H1N1 with no further subtyping.
Deaths
35 deaths confirmed to have 2009 H1N1 influenza• Ages 6-83
• 32 adults• 3 children
• 1 pregnant or post-partum• 34 with underlying medical conditions*
*chronic lung, metabolic, renal, cardiovascular disease; obesity; immunosuppression

School AbsencesDaily Public School Absenteeism
by School Type, Virginia, 2009-10 School Year
0
2
4
6
8
10
12
14
16
18
Date
Pe
rce
nt
Ab
se
nt
Elementary Middle High
*
*
*Day before holiday

Special Studies
VDH is also participating in special data collection projects led by CDC:• Death case series• Hospitalized patient case series• Severely ill pregnant women• Peramivir recipients• Guillian-Barre syndrome









Influenza other than H1N1
Rare reports of seasonal influenza A and B so far in 2009-2010 • Very few seen in Virginia• No sustained transmission in U.S. to date• WHO has no reports of seasonal influenza
activity to date during 2009-2010 flu season

H5N1 (Avian Flu)- Cumulative data
2009 activity seen in:Cambodia (2 cases), China (8 cases, 2 deaths)Egypt (40 cases, 5 deaths)Indonesia (24 cases, 22 deaths)Vietnam (6 cases, 5 deaths)
Dec 2008 Dec 2009
387 cases 467 cases
245 deaths 282 deaths
15 countries 15 countries

H1N1 Communications:A critical pillar with three key components
Prepare Respond
Prevent

H1N1 Communications:Audiences
CDCState Agencies and Local Governments Governor and Senior LeadershipMaryland and DC Health LeadershipHealthcare facilitiesClinical CommunitySchools and UniversitiesPrisons and Jails PressPublic High Priority Groups
Vulnerable Populations

Phases1. Crisis Communications- credible, timely, accurate 2. Disease education and prevention campaign3. Vaccination campaign
Overarching theme of education, collaboration and partnerships
Establish VDH as trusted source of information
H1N1 Communications:

Information Sources:H1N1GET1 website
Phone line 877-1-ASK-VDH3Opened 4/0989% of calls were from the general public88% phone, 12% emailVolume peak >700 calls/day84% in reference to vaccine

Information Sources
Press Conferences> 15Press Releases- >15Media Briefings by phone- >15Meetings/Lectures to various groups > 90
local and state levelSchool nurses, PTA, local government,
Grand RoundsAARP- magazine and Internet

Targeted communications- over 400Schools- parentsEmployersExecutive, Legislative and Judicial Branch of
State GovernmentVirginia Federal Congressional DelegationOther state agenciesTribal leadersHome school community Private SchoolsConstituent responses

Internal Communications
Local Health Director Conference callsPolycom with relevant staffDaily Senior Leadership meetingsWeekly Governor’s report

“Dear Colleague” Letters
Forum for sharing actionable information using four pillars approach including CDC updates
DHP emergency contact information- over 120,000 providers
MD, other clinical specialty organizations distribute23 letters to date
Positive Laboratory Isolates and ILI Reports by Week in Virginia,2008-2009 Influenza Season
0
20
40
60
80
100
120
Week Ending Date
Nu
mb
er o
f P
osi
tive
Lab
s
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Per
cen
t IL
I
2009 H1N1
A/H3
A/H1, Seasonal
A/Unknown
B
ILI Activity

Health Commissioner’s Infectious Disease Advisory Committee
Frederick G. Hayden, MDProfessor of Internal Medicine and Pathology, Division of Infectious DiseasesUniversity of Virginia Health Systems
Thomas M. Kerkering, MDChief of Infectious DiseasesVirginia Tech, Carilion School of Medicine
Edward C. Oldfield, III, MDChief of Division of Infectious Disease Eastern Virginia Medical School
Donald Poretz, MD, FACP, IDSA Clinical Professor of Medicine, MCV School of MedicineAnd Georgetown University School of Medicine
Richard P Wenzel, MD, MSc Chair of Internal MedicineVirginia Commonwealth University School of Medicine Michael B. Edmond, MD, MPH, MPAChair of the Division of Infectious Disease Virginia Commonwealth University Health System
James L. Pearson, DPh, BCLD Director, Division of Consolidated LaboratoriesDepartment of General Services
Ronald B. Turner, MDProfessor of PediatricsAssociate Dean for Clinical ResearchDepartment of PediatricsUniversity of Virginia School of Medicine
Mark J. Levine, MD, MPHDeputy Commissioner of Emergency Preparedness & Response ProgramsVirginia Department of Health
Diane Helentjaris, MD, MPHDeputy Director, Office of EpidemiologyVirginia Department of Health
James E. Burns, MD, MBADeputy Commissioner of Public HealthVirginia Department of Health
Karen Remley, MD, MPH, FAAPCommissionerVirginia Department of Health

Health Commissioner’s Primary Care Advisory GroupAlfred Abuhamad EVMS
Alice Ackerman Carilion
David Ascher Inova
Mike AshbyMartha Jefferson Hospital
Bob Chevalier University of Virginia
Tom Cleary Emergency Med
David Davidow Psy Solutions
Phil Dawson West End Pediatrics
Diane Dubinsky Fairfax Pediatrics
Tom EppesCentral VA Family Physicians
Bob Gunther
President, VA Chap. Of AAP; Augusta Pediatrics
Fred Hayden University of Virginia
Jon KatzVirginia Hospital Center
Tom Kayrouz Carilion PICU
William Koch MCVH-VCU
Donald LewisChildren's Hospital Kings Daughters
Doug MitchellChildren's Hospital Kings Daughters
Wade Neiman OB/GYN
Wayne Reynolds Sentara Medical Group
Mark Ryan VCU Medical Group
Sofia Teferi Bon Secours
Ron Turner University of Virginia
Arno ZarnitskyChildren's Hospital Kings Daughters

Vaccination media campaign
• Television and Cable- >10,000 plays• Radio- >4,750 plays• Internet 3,7 million impressions • Bus and Rail boards- 185• Movie theaters- 260• Media Buy share with DC/MD for NOVA

Vaccine information - Google Flu Vaccine Locator
Allows users to find vaccination locations by ZIP code

H1N1 Vaccine Development

CDC- Advisory Committee on Immunization Practices- September 2009
H1N1 Vaccine Planning- High Priority Groups
Pregnant womenHousehold contacts and caregivers of infants <6 mo
of ageHealthcare and EMS personnelAll persons 6 mo – 24 years of agePersons 25 – 64 years of age who have health
conditions associated with higher risk of medical complications from influenza
Up to 4.1 million Virginians in these categories

Vaccine free in all settingsAll supplies providedPrivate Providers can charge administration feeStates to determine allocation and documentation
process
H1N1 Vaccine Planning
Established 2006August 2009 75 users including MDs, HospitalsJanuary 2010 2,732 users including MDs,
Hospitals and Pharmacies

Vaccination Campaign Tenets
• Combined Public/Private • Focus on priority groups with special attention
pregnant women• Local Health Departments- School age large scale
vaccination plans • Documentation to occur through VIIS with
minimal information- Name, DOB, vaccine type and lot number

Vaccine Manufacturers
National Distributor (McKesson)
Internal Distributor
(GIV)
Vaccinators
Vaccinators
Orders ≥100 doses
Orders < 100 doses
Vaccine Distribution Process

VDH Guiding principles for vaccine allocation
strive to be fair and ethical throughout the vaccination campaign.
focus on CDC’s target groups. partner with thousands of public and private
vaccinators in communities throughout the Commonwealth.
rely on the judgment of the vaccine providers in the healthcare community to help it reach CDC’s target groups.

VDH Guiding principles for vaccine allocation
Local health departments (LHs) will work with these partners to assure that all persons have an opportunity to be vaccinated.
There will be no charges for any H1N1 vaccinations administered by or under the supervision of LHDs.
All persons, regardless of whether they live in Virginia or not, will be provided H1N1 vaccine by any LHD once the vaccine is available to the general public through pharmacies and other retail outlets.
The specific focus of LHD’s vaccination efforts will include their own patients and staff, CDC’s target groups, as well as assuring that vulnerable populations have access to the vaccine.

Variables affecting allocation process
Flow of vaccine from manufacturers and CDC Formulation of available vaccine Reliability of the distribution process from
manufacturer to patient Provider preferences (patient population,
formulation, storage capacity, staff capacity)

Guiding principles for reaching target groupsFocus on:
• High-risk for hospitalization and death from flu• Act as source for outbreaks in high-risk group settings • Easily accessible through specific providers
Target group High-risk Outbreak prevention
Easily accessible
Pregnant women X X
Healthcare workers X X
Parents of infants <6mo By proxy
Children 6mo-4y/o X X (daycare) X
Children 5-18y/o X X (schools) X
Young adults 19-24y/o X X (colleges) +/-
25-64y/o with medical conditions X

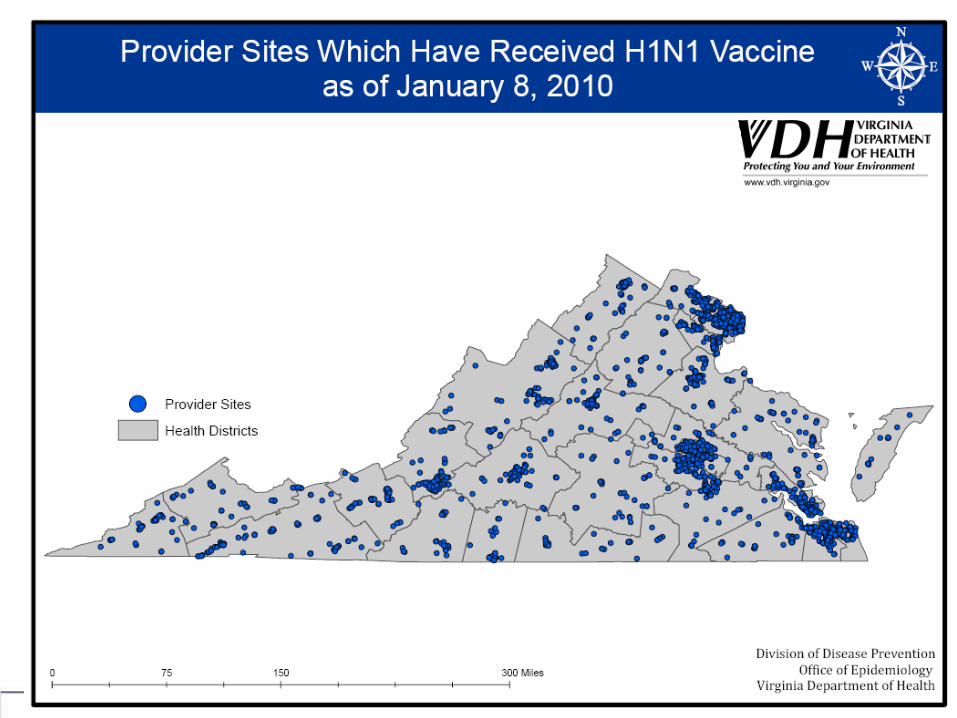
Vaccine Administration sites
MD officesLocal Health Depts.Schools HospitalsMallsStoresZooEtc…….





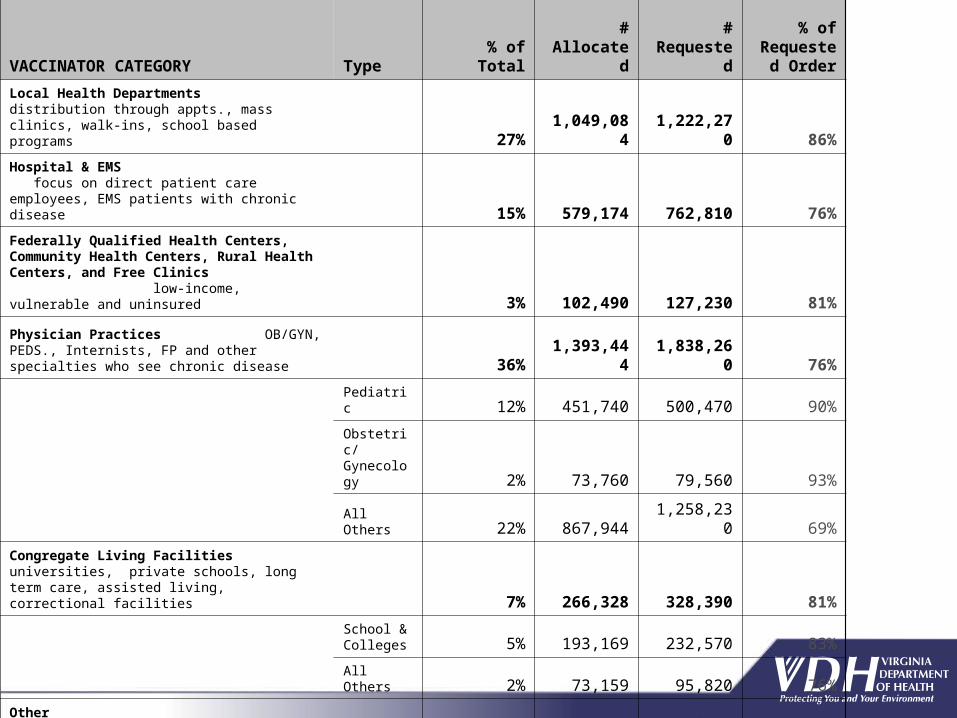
VACCINATOR CATEGORY Type % of Total#
Allocated
# Requeste
d
% of Requeste
d Order
Local Health Departments distribution through appts., mass clinics, walk-ins, school based programs 27%
1,049,084
1,222,270 86%
Hospital & EMS focus on direct patient care employees, EMS patients with chronic disease 15% 579,174 762,810 76%
Federally Qualified Health Centers, Community Health Centers, Rural Health Centers, and Free Clinics low-income, vulnerable and uninsured 3% 102,490 127,230 81%
Physician Practices OB/GYN, PEDS., Internists, FP and other specialties who see chronic disease 36%
1,393,444
1,838,260 76%
Pediatric 12% 451,740 500,470 90%
Obstetric/Gynecology 2% 73,760 79,560 93%
All Others 22% 867,944 1,258,230 69%
Congregate Living Facilities universities, private schools, long term care, assisted living, correctional facilities 7% 266,328 328,390 81%
School & Colleges 5% 193,169 232,570 83%
All Others 2% 73,159 95,820 76%
Other Occupational Health, Retail Pharmacy 12% 478,310
1,476,750 32%
Misclassification 0% 650 4,900 13%
Total 100%3,869,48
05,760,61
0

Mitigation - Protecting Healthcare Workers
Distribution of PPE from State SNS Stockpile 57 Free Clinics & 27 Community Health Centers
60,000 surgical masks122,000 N-95 respirators10,000 face shields Gloves & Gowns

Mitigation - EMS Agencies
PPE Distributed to 520 EMS Agencies245,000 N-95 respirators120,000 surgical masks
Augmented hospital PPE as requested from the remaining 25% of the SNS allocation
810,000 additional respirators and 1 million surgical masks purchased with Federal grant funds; now stocked at the Virginia Distribution Center for distribution as needed

Direct Medical Care /Surge
State antiviral stockpile• Oseltamivir
Surge

State Antiviral Stockpile release
VDH Stockpile Tamiflu Rx ClaimsWeekly summary
050
100150200250300350400
10/2
4/20
09
11/7
/200
9
11/2
1/20
09
12/5
/200
9
12/1
9/20
09
Date
Rx
Cla
ims
Suspension Claims
75 mg Tab Claims

Hospital Surge
Hospitals coped with heavy ER traffic - near normal diversion incidents
Signage and physical barriers to divert ILI patients to appropriate triage area
Establishment of triage and treatment sites outside of ER area
Use of PPE to protect hospital staff and patients

Hospital Surge (con’t)
ICUs moderately stressedHigher than normal occupancy ratesDid not exceed capacity
Scarce, Specialized Equipment and Trained StaffIsolated incidents of serious respiratory cases and
limited equipment/staff Identified need to continue efforts to develop scarce
resource allocation protocols.

Situational Awareness
Hospital bed-tracking/status system
Provided timely and accurate information on healthcare system status
Effective means of sharing information
Information provided weekly to National hospital bed-tracking and status system (HAvBED)

CMS Waiver for EMTALA and HIPAASection 1135 of the Social Security Act permits
the HHS Secretary to waive certain regulatory requirements for healthcare facilities in response to emergencies provided that:
1) the President has declared an emergency or disaster under the Stafford Act or the National Emergencies Act and
2) the HHS Secretary has declared a Public
Health Emergency (PHE)

CMS Waiver for EMTALA and HIPAA (con’t)
HHS Secretary exercised her waiver authority effective October 23, 2009. CMS was delegated the authority to determine the waiver for each case justified by necessity and extent.
Waived certain provisions including EMTALA & HIPAA for healthcare providers who are unable to comply with these requirements as a result of the H1N1 influenza pandemic
Hospitals were notified of the process for applying for a 1135 waiver, either directly to CMS via the regional CMS office or via the State Survey Agency (our VDH OLC)
Next Steps

Targeted Vaccination and After Action Analysis
Vaccination Strategy
First of Regular Shipments (Bolus)
Pre-campaign shipments for most at risk
School Based Clinics
LHD Clinics
Private Providers
and Pharmacies
Community Mass Vax EventsVac
cine
Dos
es
Adm
inis
tere
d
Targeted Outreach to Specific Groups
The most at risk
Children 6 months to 18 years; their caregivers
General Public
1st Drip Phase I Phase IIApprox. Date
Healthcare Providers

ResourcesVirginia Department of Health Web site:
www.vdh.virginia.gov; www.H1N1Get1.com Toll-free VDH Inquiry Center:
1-877-ASK-VDH3 (1-877-275-8343)Google Flushot Locator
www.google.com/flushot
CDC H1N1 Web site:www.cdc.gov/h1n1flu
U.S. Dept. of Health & Human Services Flu center:www.flu.gov


















