Headache
29
NUR AINA BINTI AB KADIR
-
Upload
ainakadir -
Category
Health & Medicine
-
view
270 -
download
0
Transcript of Headache

NUR AINA BINTI AB KADIR

GENERAL PRINCIPLES
• Associated features are the disorders itself
PRIMARY
• Exogenous disordersSECONDARY

COMMON CAUSES OF HEADACHE

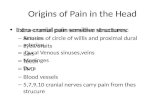
ANATOMY&PHYSIOLOGY
• Peripheral nociceptors are stimulated tissue
injury,visceral distension
• Pain producing pathways of the peripheral/ CNS are
damaged/activated inappropiately
• Cranial structures(pain producing): scalp, middle
meningeal artery, dural sinuses, falx cerebri, proximal
segments of the large pial arteries

CLINICAL EVALUATION OF ACUTE, NEW ONSET HEADACHE
• New& severe VS recurrent over many years• Probability of finding a potentially serious cause & need
prompt evaluation, proper treatment• 1st step: complete neurologic examination• Abnormal examination/history of recent-onset headache
CT/MRI study• General evaluation of acute headache might include the
investigation of CVS & renal status by BP monitoring & urine examination

Cont..
• Psychological state : relationship exist between head pain and depression
• Underlying recurrent headache disorders may be activated by pain follows otologic/ endodontic surgical procedures.

HEADACHE SYMPTOMS THAT SUGGEST A SERIOUS UNDERLYING DISORDER
• “WORST” headache ever• 1st severe headache• Subacute worsenig over days/weeks• Abnormal neurologic examination• Fever/unexplained systemic signs• Vomiting that precedes headache• Pain induced by bending,lifting,cough• Pains that disturbs sleep/presents immediately upon awakening
• Known systemic illness• Onset after age 55• Pain associated with local tenderness eg.: region of temporal artery

MIGRAINE• Second most common cause of headache
• Episodic headache with certain features such as sensitivity to light, sound, and movement
• Headache often accompanied by nausea and vomiting
• A benign and recurring syndrome of headache associated with other symptoms of neurologic dysfunction in varying admixtures.
• Sensitive to environmental and sensory stimuli

PATHOPHYSIOLOGY1) Vascular theory

2) Cortical spreading depression
• Activation of cells in the trigeminal vasoactive neuropeptides,
calcitonin gene–related peptide (CGRP), at vascular terminations of the
trigeminal nerve and within the trigeminal nucleus.
• Centrally, the second-order trigeminal neurons cross the midline and
project to ventrobasal and posterior nuclei of the thalamus for further
processing.
• Other brainstem region : nucleus locus coeruleus in the pons and the
rostroventromedial medulla.


PATHOPHYSIOLOGY
3) Involvement of neurotransmitter 5-hydroxytryptamine- methysergide : first drug capable of preventing migraine attacks- triptans : potent agonists of 5-HT1B, 5-HT1D, 5-HT1F


PATHOPHYSIOLOGY
4) Role of dopamine- migraine symptoms can be induced by dopaminergic stimulation- dopamine receptor antagonists are effective especially when given parenterally or concurrently with other antimigraine agents

PATHOPHYSIOLOGY
• Migraine has a strong genetic component5) Familial hemiplegic disorders
- rare type of migraine with aura
FHM MUTATIONS
FHM1 CAY2.1 (P/Q)-type voltage-gated calcium channel CACNA1A gene
FHM2 Na+-K+ATPase ATP1A2 gene
FHM3 Neuronal voltage gated sodium channel SCN1A

• Hormonal influences – usually occur during menstruation
• Contraceptive pill - exacerbate migraine in many patients
• Dietary precipitants - cheese, chocolate, red wine
• Psychological stress - pt tend to have attacks at
weekends/beginning of a holiday (may be associated with
vasodilatation of extracranial vessels, but may be due to
disturbed neuronal activity in the hypothalamus

DIAGNOSIS & CLINICAL FEATURESRepeated attacks of headache lasting 4-72 hours in patients with a normal physical examination, no other reasonable cause for the headache and:At least 2 of the following features
Plus at least 1 of the following features
Unilateral pain Nausea/vomiting
Throbbing pain Photophobia and phonophobia
Aggravation by movement
Moderate or severe intensity

TREATMENT
• NON PHARMACOLOGIC MANAGEMENT– Identify and avoid of specific headache triggers– Change of lifestyles– Reduce stress

TREATMENT
• ACUTE ATTACK THERAPIES FOR MIGRAINE– Mild migraine : oral agents– Severe attacks : parenteral therapy – Drugs : • 5-HT1B/1D receptor agonists• Ergot alkaloids• NSAIDs• Dopamine receptor antagonists

•Simple Analgesics•Acetaminophen, aspirin, caffeine : Two tablets or caplets q6h (max 8 per day)
•NSAIDs•Naproxen :220–550 mg PO bid
•5-HT1 Agonists•Oral•Ergotamine One 2 mg sublingual tablet at onset
•Nasal•Dihydroergotamine •Prior to nasal spray, the pump must be primed 4 times; 1 spray (0.5 mg) is administered, followed in 15 min by a second spray

Cont..
• Parenteral• Dihydroergotamine : 1 mg IV, IM, or SC at onset and q1h • Sumatriptan:6 mg SC at onset • Dopamine Antagonists• Oral• Metoclopramide :5–10 mg/d• Parenteral• Chlorpromazine 0.1 mg/kg IV at 2 mg/min; max 35
mg/d

OTHER• Other• Oral• Acetaminophen, 325 mg, plus dichloralphenazone, 100 mg,
plus isometheptene, 65 mg• Two capsules at onset followed by 1 capsule q1h (max 5
capsules)• Nasal• Butorphanol 1 mg (1 spray in 1 nostril), may repeat if
necessary in 1–2 h• Parenteral• Narcotics

TREATMENT
• PREVENTIVE TREATMENT
– Frequency of attacks is >2 per month
– Duration of attacks is >24 hours
– Disturb patient's lifestyle, with significant disability
that lasts 3 or more days
– Acute attack therapies fails or is overused

DRUGS DOSES
Antiepileptic drugs : valproate
400-600 mg bid
Beta blockers : propranolol 40-120mg bid
Tricyclic antidepressants :amitriptyline
10-75 mg at night
Serotonergic drugs:methysergide
1-4 mg qd
Pizotifen 0.5-2 mg qid

SECONDARY HEADACHE
MENINGITIS
INTRACRANIALHEMORRHAGE
BRAIN TUMOR
TEMPORALARTERITIS
GLAUCOMA

• MENINGITIS• Acute,severe headache
with neck stiff, fever• Lumbar puncture is
mandatory• Striking accentuation of
pain with eye movement
• INTRACRANIAL HEMORRHAGE
• Acute,severe headache with stiff neck,no fever suggest subarachnoid hemorrhage

• BRAIN TUMOR• Chief complaints of headache-
30%• Pain: intermittent deep, dull
aching of moderate intensity• Disturb sleep:10%• Vomitingheadcahe by weeks:
posterior fossa brain tumors• h/o amenorrhea& galactorrhea
prolactin-secreting pituitary adenoma/PCOS
• Head pain appear abruptly after bending, lifting,coughing posterior fossa mass, a Chiari malformation, low CSF volume
• GLAUCOMA• Prostrating headache with
nausea& vomiting• Starts with severe eye pain• On P/E: eye is often red with a
fixed,moderately dilated pupil

TEMPORAL ARTERITIS
• Inflammatory disorder of arteries(extracranial carotid circulation)• Common disorder of elderly• Half of the patient with untreated TA blindness • Symptoms: headache, polymyalgia rheumatica, jaw claudication,
fever and weight loss • Pain usually appears gradually over a few hours before peak
intensity is reached; occasionally, it is explosive in onset. • The quality of pain:throbbing; it is almost invariably described as
dull and boring, with superimposed episodic stabbing pains

REFERENCE
• Harrison’s Principle of Internal Medicine, 18th Edition, Volume 1
• Davidson’s Principles and Practice of Medicine, 22nd Edition
• http://emedicine.medscape.com/article/1142556