HEADACHE - smbs.buffalo.edu · u “Headache genes” u Migraine, tension-type, cluster, and other...
74
HEADACHE: Diagnosis and Treatment Melissa Rayhill, MD, FAHS Assistant Professor of Neurology/Headache Specialist Jacobs School of Medicine and Biomedical Sciences
Transcript of HEADACHE - smbs.buffalo.edu · u “Headache genes” u Migraine, tension-type, cluster, and other...

HEADACHE:Diagnosis and Treatment
Melissa Rayhill, MD, FAHS
Assistant Professor of Neurology/Headache Specialist
Jacobs School of Medicine and Biomedical Sciences

Disclosures
u I have no financial disclosures

Objectives: (aka *WHAT TO STUDY*)
u Know the proposed pathophysiologic mechanisms for migraine
u Be familiar with the diagnostic criteria for the major primary headache disorders
u Understand the therapeutic approach to primary headache disorders (both abortive and preventive therapies) and when to start them
u Identify dangerous causes of secondary headache that are not to be missed

How many of you get headaches?

Do I need to know this? …. YES.
u 1 in 4 households in the US has someone with migraine1
u Lifetime prevalence of tension-type headache is about 78%2
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41(7):646-657
2. Rasmussen BK. et. al. J Clin Epidemiology. 1991.

The Great Divide…
u Primary
Headache
u “Headache genes”
u Migraine, tension-type, cluster, and other headache
types
u Secondary
Headache
u Headache as a result of…
u tumors, blood in the brain, etc.
Beware… people with a history of migraine can also get brain tumors!

Headache History:
u Occurrence – hyperacute, acute, subacute, chronic
u Location, Duration, Severity, Character
u Frequency (how often are they headache-free?)
u Associated symptoms (nausea, photophobia, etc.)
u Don’t forget:u Sleep
u Psychiatric comorbidities
u Medication use (or overuse?)

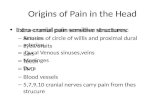
The brain feels no pain!
What can cause pain in the head?
u ….Everything else!
u Especially large vessels and the dura.
u Innervation includes:
u CN V – intracranial structures in anterior
and middle fossa of skull, above the
cerebellar tentorium
u CN IX and X – part of posterior fossa
u Upper cervical roots – infra-tentorial and
cervical structures

Physical Exam
u Altered mental status
u Papilledema (high intracranial pressure)
u Nuchal rigidity/fever (with meningitis)
u Focal neurologic deficits
u Vast majority of patients with chronic
headache have normal neuro exam

Primary HeadachesWhen was the very first headache you ever had?

Primary Headaches:
u Migraine
u Tension-type Headache
u Cluster Headache
u MANY others!

When in doubt, use ICHD:International Classification of Headache Disorders
Version 3
www.ichd-3.org
BILLS FAN
JOKE!

Diagnosing Migraine
without aura
A. At least five attacks fulfilling criteria B–D…
B. Headache attacks lasting 4-72 hours
C. At least 2 of the following 4 characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravation by or causing avoidance of routine physical activity (e.g. walking or climbing stairs)
D. During headache at least 1 of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not better accounted for by another ICHD-3 diagnosis.

Wait. What’s an aura?
Scintillating
Scotoma

She’s having a stroke! ……
…never mind, it’s language aura!

Diagnosing Migraine
with aura (~30% of migraineurs)
A. At least 2 attacks fulfilling criteria B and C
B. One or more of the following fully reversible aura symptoms:1. Visual2. Sensory3. Speech and/or language4. Motor5. Brainstem6. Retinal
C. At least 2 of the following four characteristics:1. At least one aura symptom spreads gradually over 5 minutes, and/or
two or more symptoms occur in succession2. Each individual aura symptom lasts 5-60 minutes3. At least one aura symptom is unilateral4. The aura is accompanied, or followed within 60 minutes, by headache
D. Not better accounted for by another ICHD-3 diagnosis, and transient ischemic attack has been excluded.

Chronic Migraine:Must have at least 3 months of the following:
Occurs > 15 days a month
Lasts > 4 hours a day
Migrainous > 8 days month
features

Migraine Pathogenesis:
u “A genetic susceptibility” that’s always there
u “A dysfunction of brain-stem nuclei that are
involved in the sensory/nociceptive
modulation of craniovascular afferents.”
u Goadsby et al, NEJM 2002

Migraine Pathogenesis:
u Activation of trigeminal nucleus
caudalisàu Releases vasoactive peptides (calcitonin
gene-related peptide (CGRP) and
substance P among others)à
u Stimulates further inflammatory response
of the trigeminovascular system
u This nociceptive activation can cause
central and peripheral sensitization

Migraine Pathogenesis:

Migraine Pathogenesis:
u May begin with a wave of
neuronal excitation in cortical
gray matter, with local blood
flow changes, followed by
spreading cortical depression
(CSD)
u Probably bidirectional activation
occurs (cortex to brainstem, and
brainstem to cortex)
u CSD spreads predictably across
the cortex at 2 – 6 mm/minute

Migraine Pathogenesis:
u In the setting of a genetic susceptibility to migraine the following may worsen or trigger headache:
u Skipping meals/fasting, inadequate hydration
u Changes in sleep patterns and/or poor quality sleep
u Stress
u Menses, ovulation, or irregular cycles (hormonal therapies, etc. )
u Head trauma
u Depression and anxiety commonly co-occur with (but do not cause) headache.

Primary Headaches:Migraine Treatment

Primary Headaches:Migraine Treatment
u Abortive medication
u Taken at the time of headache to relieve that headache episode
u “Preventive” medication
u Taken daily, whether headache present or not, to decrease overall frequency and severity of headaches on average
u Does not actually “prevent all headaches”

So, when should you start a
migraine preventive therapy?
u Frequency of headaches ≥ 1-2 days/week, with disability ≥ 3 days/month
u Recurring migraines that, in the patient’s
opinion, significantly interfere with daily routines
u Use of acute medications more than 2 times
per week
u Acute medications are contraindicated, not
tolerated, or ineffective

Primary Headaches:Migraine Abortive Therapy
u NSAIDs:
u Naproxen, ibuprofen, combination analgesics (Excedrin)
u Anti-emetics:
u Prochlorperazine (Compazine) or metoclopramide (Reglan)
u These 2 have migraine-specific actions in addition to treating nausea (dopamine antagonists AND serotonin receptor antagonists)
u Dihydroergotamine (DHE), used intranasal or IV
u Triptans… and many more! …
u Don’t forget about non-oral options!
u Ketorolac IV, anti-emetics IV/PR, triptan nasal spray/IM/patch

Migraine Abortive Therapy:Triptans
u Triptan Mechanism
u Selective serotonin 1B,1D receptor agonists (5-HT agonists)
u Acts at the trigeminal nucleus caudalis and peripherally on blood vessels.
u Causes neuronal inhibition and blockade of release of CGRP
u Work best if adequate HIGH dose taken early in the attack
u Take effect within 20-60 minutes
u Can be combined with NSAIDS and antiemetics
u Avoided in patients with CAD, PVD, and pregnancy

Migraine Abortive Therapy:Sumatriptan (Imitrex)
u Oral
u Nasal spray
u Subcutaneous injection

Migraine Abortive Therapy:
Triptans
u All 7 are about the same in studies… but different
among patients
u *sumatriptan*, naratriptan, zolmitriptan, and rizatriptan
are generic (most insurances cover sumatriptan first)
u Long-acting triptans are best for menstrually
related migraine (twice daily for 4 days may be
helpful)
u Non-oral therapies can be helpful!

Primary Headaches:Migraine Preventive Therapy
u Choice of agent will depend on co-morbid conditions and acceptable side effects
u Must be consistently taken for 2 - 3 months to adequately judge effectiveness
u Start with low dose, increase slowly
u Can continue use of abortive treatments

Primary Headaches:Migraine Preventive Therapy
u Antidepressants– tricyclic antidepressants, SNRIs
u Beta-blockers
u Anticonvulsants
u ACE inhibitors
u Requires trials of other agents first, $$$
u Botulinum toxin A (Botox)
u CGRP monoclonal antibodies

AHS/AAN Guidelines (2012) on Preventive Therapies:Loder, Burch, and Rizzoli. Headache, 2012. J
u Beta blockers: propranolol, metoprolol, timolol (A)
u AEDS: divalproex sodium (Depakote), topiramate (A)
u Antidepressants: amitriptyline, venlafaxine (B)
u Supplements: riboflavin, magnesium (trimagnesium dicitrate) (B)
u Others: cyproheptadine, candesartan, lisinopril (C)
u Level A: Established efficacy; Level B: Probably effective; Level C: Possibly effective; Level U: Inadequate or conflicting data to support or refute medication use

31 injections? Are you crazy, doc?
http://www.allergan.com/assets/pdf/botox_pi.pdf

Chronic Migraine Prevention:
Onabotulinum toxin A (Botox)
u The recommended dose for treating chronic migraine is
155 Units administered intramuscularly (IM) as 0.1 mL (5
Units) injections per each site
u Given by provider in the office every 12 weeks
u No data in pregnancy

Monoclonal antibodies against CGRP:
New Preventive options!
u Erenumab (4/2018)
u Fremanezumab (9/2018)
u Galcanezumab (9/2018)
u Eptinezumab (pending)

CGRP: What we know…and What we don’t know…
u Calcitonin Gene Related Peptide is a widely distributed,
vasodilatory neuropeptide
u About 3 years of clinical trial data on erenumab
u Nothing terrible happened when erenumab was given IV to
people with stable angina!
u Depre, et al. A Randomized, Double-Blind, Placebo-Controlled
Study to Evaluate the Effect of Erenumab on Exercise Time During
a Treadmill Test in Patients With Stable Angina. Headache2018;58:715-723.
u Not studied in pregnancy/lactation!

Primary Headaches:Migraine in Pregnancy
u Pregnancy related decrease in migraine commonly seen, ? related to estrogen levels
u 5-30% have no improvement or worsening of migraines
u Beware of secondary headaches!!
u Dissection, pituitary apoplexy, venous sinus thrombosis, pre-eclampsia, reversible cerebral vasoconstrictive syndrome (RCVS)

Migraine in Pregnancy:
FDA Risk Categories
u Category A: Controlled human studies show no risk
u Category B: No evidence of risk in humans but
there are no controlled human studies
u Category C: Risk to humans has not been ruled out
u Category D: Positive evidence of risk in human or
animal studies
u Category X: Contraindicated in pregnancy

Migraine in Pregnancy:
When a medication is required…
u Abortive medications:
u Acetaminophen
u Caffeine (<200mg/day)1
u Metoclopramide
u Nerve blocks (lidocaine)
u Preventive medications:
u Magnesium gluconate
u Magnesium oxide
u Propranolol (former FDA Cat. C)
1. ACOG Committee Opinion No. 462: Moderate caffeine consumption during pregnancy. Obstet Gynecol. 2010 Aug;116(2 Pt 1):467-8. doi: 10.1097/AOG.0b013e3181eeb2a1.

Caution in Pregnancy:
Abortive Meds
Drug Associated risks
Butalbital-containing
analgesics
Medication overuse headache common, severe
neonatal withdrawal syndrome if prolonged use
NSAIDs – 3rd trimester Decreased amniotic fluid volume, inhibit labor,
cause bleeding close to term, premature closure of
ductus arteriosus (some studies say after 20 weeks
gestation)
Caffeine >300mg/day Increased risk spontaneous abortion, low birth
weight
Triptans (C)/
Dihydroergotamine (X)
?Placental blood flow changes

Caution in Pregnancy:
Preventive MedsDrug Important to know FDA Safety Category
Amitriptyline Uncertain, similar to
SSRIs? organogenesis
C
Atenolol Associated with perinatal
beta blockade and
growth retardation
D
Topiramate Facial clefts D
Valproic acid (Depakote) neural tube defects,
?verbal IQ
Contraindicated in
migraine
(D in epilepsy)

Medication Overuse Headache:A secondary headache!
u Limit abortives to no more than 2 days
per week!
u Occurs in patients with pre-existing headache
u Symptomatic and preventive treatments become less effective over time
u Medication use gives transient relief with overall escalation of headache sensitivity

Principles of MOH therapy
u Taper/stop medications implicated. Usually:u NSAIDs
u **Opiates (tramadol, oxycodone, etc.)
u Triptans
u **Barbituates (Fioricet/Fiorinal)
u Caffeine! (Excedrin)
u Generally limit caffeine 1-2 cups before 1pm, consistency!
u Substitute acute meds and start good preventive meds
u **BEWARE OF WITHDRAWAL SYNDROMES

Primary Headaches:Tension-Type HeadacheA. Lasting from 30 minutes to 7 days
B. At least two of the following four characteristics:
A. Bilateral location
B. Pressing or tightening (non-pulsating) quality
C. Mild or moderate intensity
D. Not aggravated by routine physical activity such as walking or climbing stairs
C. Both of the following:A. No nausea or vomiting
B. No more than one of photophobia or phonophobia
D. Not better accounted for by another ICHD-3 diagnosis.

Primary Headaches:Tension-Type Headache (TTH)
u Can occur with or without pericranial tenderness
u Episodic and chronic forms
u The most common headache type!
Loder E, Rizzoli P. Tension-type Headache.
BMJ 2008;336:88-92.

Primary Headaches:TTH Treatments
u Abortive therapy:
u Mostly NSAIDs
u Over-the-counter combination medications (Excedrin)
u Preventive therapy:
u Tricyclic antidepressants (amitriptyline has the strongest evidence by far)
u Venlafaxine (an SNRI)
u ?Muscle relaxants (tizanidine, cyclobenzaprine)
u Consider biofeedback, physical therapy, cognitive behavioral therapy

Primary Headaches:Cluster Headache
u Prevalence 0.1%
u Predominantly seen in males
u Relatively short duration
u Unilateral, periorbital
u Ipsilateral lacrimation, nasal stuffiness, conjunctival injection, Horner’s syndrome commonly associated
u High association with SUICIDE. Take it seriously!

Cluster Headache:
A. At least five attacks fulfilling criteria B–D
B. Severe or very severe UNILATERAL orbital, supraorbital and/or temporal pain lasting 15–180 minutes (when untreated)
C. At least one of the following symptoms or signs, ipsilateral to the headache:
Conjunctival injection and/or lacrimation, nasal congestion and/or rhinorrhea, eyelid edema, forehead and facial sweating, forehead and facial flushing, sensation of fullness in the ear, miosis and/or ptosis
AND/OR A sense of restlessness or agitation
D. Attacks have a frequency between one every other day and eight per day for more than half of the time when the disorder is active

Primary Headaches:Cluster Headache
u Chronic and episodic forms
u Occur in clusters lasting weeks-months
u Between cluster periods, headache free for months-years
u During cluster, get multiple headaches/day, usually at the same time each day
u Headaches triggered by alcohol during cluster period
u The headache is SIDE-LOCKED on only one side

Cluster Headache:
u Functional MRI shows activation of ipsilateral posterior hypothalamic gray matter during attack (central pacemaker regions, near parasympathetic outflow)

Cluster Headache:Abortive Therapy
u Sumatriptan-- SUBCUTANEOUS!
u 100% oxygen, 12-15 L/min USING A NON-REBREATHER MASK

Cluster Headache:Preventive Therapy
u Verapamil
u Lithium carbonate
u Bridge Therapies:
u Greater occipital nerve block w/ steroid
u Prednisone taper

Secondary Headaches: The scary kind

Adapted from Silberstein SD et al., eds. Headache in Clinical Practice. 2nd. August 2002.
Diagnostic Evaluation

Secondary Headaches:Red Flags
HISTORYu “First or Worst”
u Cancer, HIV, immunocompromised
u >50yo, new onset
u Seizures
u Focal symptoms
u Change over time
EXAMu Papilledema
u Cognitive impairment
u Fever, stiff neck
u Focal signs on exam

Secondary Headaches:Blood where it shouldn’t be
1. Intra-parenchymal hemorrhage
u Due to HTN (cocaine/amphetamines), vascular malformation, trauma, anticoagulation, amyloid angiopathy
2. Intra-ventricular hemorrhage
u Can cause obstructive hydrocephalus
3. Epidural hematoma “lens shaped” (lentiform)
u Usually arterial, associated with linear skull fracture which crosses/tears middle meningeal artery
4. Subdural hemorrhage “crescent shaped”
u Usually shearing of bridging veins in subdural space
u More common in the young, elderly, alcoholism
u Associated with anticoagulation or closed head trauma
5. Subarachnoid hemorrhage

Subdural or Epidural?
A B

Secondary Headaches:Subarachnoid hemorrhage (SAH)
u Spontaneous (usually due to rupture of aneurysm) or traumatic
u Presents with “the worst headache of my entire life”, altered mental status, vomiting, nuchal rigidity
u CT scan of brain demonstrates blood in >90% if done within the first 24 hours. If CT negative → lumbar puncture
u Delayed onset of vasospasm → focal neurological deficits (usually 7-14 days after bleed)

Xanthochromia: “SAH wuz here”
u Blood in CSF pink for first 24 hours, then CSF
turns yellow due to enzymatic breakdown of
hemoglobin after subarachnoid hemorrhage

Secondary Headaches:Problems w/ arteries + veins
1. Carotid artery dissection
u Causes headache and facial pain ipsilateral to the dissecting artery,
and can be complicated by arterial infarction in anterior circulation
2. Vertebral artery dissection
u Causes headache and neck pain ipsilateral to the dissecting artery,
and can be complicated by arterial infarction in posterior circulation
3. Venous Sinus Thrombosis
u Hypercoaguable states (oral contraceptives) increase risk
u Can cause lethal venous infarction from not allowing tissue to drain
properly, restricting arterial inflow eventually
4. Temporal Arteritis

Secondary Headaches:Arterial Dissection
u A common cause of stroke in patients <40yrs old
u ~50% of patients with carotid dissection have ipsilateral Horner’s syndrome (ptosis, miosis, anhydrosis) due to stretching or compression of sympathetic fibers traveling with the vessel

Secondary Headaches:Temporal Arteritis
u aka– “Giant cell arteritis”: an indicator of granulomatous inflammation

Secondary Headaches:Temporal arteritis
u Subacute granulomatous inflammation most prominent along the internal elastic lamina of arterial wall
u Usually affects branches of the external carotid artery (superficial temporal artery)
u May have malaise, fever, weight loss, myalgias, arthralgias
u May have jaw claudication/stiffness, scalp tenderness due to decreased blood flow
u Ophthalmic artery involvement can result in visual changes or sudden loss of vision, leading to blindness in 60%!!!

Revised Criteria Amer. College of Rheumatology
Temporal Arteritis
N/A Age at onset ≥50 years old
Domain I
1
1
2
1
2
New onset localized headache
Sudden onset of visual disturbances
Polymyalgia Rheumatica (PMR)
Jaw Claudication
Abnormal temporal artery (tenderness, decr. pulsation)
Domain II
1
1
2
Unexplained fever and/or anemia
ESR ≥50 mm/hour
Compatible pathology

Secondary Headaches:Temporal Arteritis
u ACR Criteria are highly sensitive and specific
u Treatment → High dose steroids… Don’t wait for biopsy results!

Secondary Headaches:High Pressure Problems
1. Headache attributed to arterial hypertension
u Seen with hypertensive emergency and conditions causing sudden elevation of BP
2. Intracranial Hypertension (of CSF):
u Morning-predominant headaches, N/V
u Elevated CSF pressure due to mass/tumor/abscess
u Idiopathic: “previously called pseudotumor cerebri”, now called IIH (idiopathic intracranial hypertension)....

Secondary Headaches: IIH(Idiopathic Intracranial Hypertension)
u Risk Factors:u Affects young obese women (or w/ recent weight
gain)u Pregnancy, oral contraceptives, steroidsu Hypervitaminosis A u Tetracyclineu Obstruction of intracranial venous drainage
u Venous sinus thrombosis (Diagnosis of idiopathic IH requires venous imaging w/ MRV or CTV!)
u polycythemia, thrombocytosis

Secondary Headaches:IIH
u Increased resistance to CSF reabsorption at the arachnoid granulations, ?role of hormones
u Opening pressure elevated on LP àPapilledema usually seen on exam
u Other symptoms:u Blurry vision, horizontal diplopia (CN VI compressed),
“pulsatile tinnitus”, N/V
u Pressure on the optic nerve can result in optic atrophy/blindnessà MUST follow with an ophthalmologist
u CT/MRI may show “slit-like” ventriclesu Treatment – acetazolamide, repeated LPs or lumbo-
peritoneal shunt, optic nerve sheath fenestration

Idiopathic intracranial hypertension
Radiopaedia.org

Secondary Headaches:Low pressure problems
u Intracranial HYPOtension

Secondary Headaches:Intracranial HYPOtension
1. Post-LP headache (or “wet” epidural after delivery)u Caused by persistent spinal subarachnoid fluid leak causing
traction on pain sensitive structures at base of brain
u Meningeal contrast enhancement, “sagging brain” w/ pontine flattening
2. Spontaneous intracranial hypotensionu Usually due to small trauma, small tear in dura around spine
u Having some connective tissue disorders is a risk
u Occipital-predominant headache u Precipitated by standing, relieved by laying down (worse at
end of day)
u Most improve on their own or with caffeine u Blood patch may help some patients with lingering
symptoms

Other noteworthy headaches
u “Thunderclap headache”: THINK BADNESS until proven otherwise (need brain/vessel imaging), sometimes occurs w/ sexual activity
u Occipital neuralgia (shooting electric pains from the back of the head up to the front)
u Headache attributed to sinusitis (Not as common as you think!!)
u Post-traumatic headache (with or without post-concussive syndrome; acute or chronic)
u Cervicogenic headache (related to cervical arthritis/arthropathy)
u Trigeminal Neuralgia
u …AND MORE!!

At the end of the talk…
u Know the proposed pathophysiologic mechanisms
for migraine
u Be familiar with the diagnostic criteria for the
major primary headache disorders
u Understand the therapeutic approach to primary
headache disorders (both abortive and preventive
therapies) and when to start them
u Identify dangerous causes of secondary headache
that are not to be missed

Hope I didn’t give anyone a headache with all of this!
www.americanheadachesociety.org