New York Headache Center Headache Update Alexander Mauskop, MD.
Upload
damir-zagrebCategory
view
212download
0description

European Interactive Pain Course03.-07.09.07
Wednesday
Headache – Symptoms and
treatment

European Interactive Pain Course03.-07.09.07
Headache and facial pain: diagnosis
History
Location
of pain
Character
of pain
First onset
Duration
of pain
Pain-free
intervals
Reasons
for
increase
or decrease
in symptoms
Triggering
factors
Concomitant
symptoms
Analgesic
history
Family
history
Family
stress
Social
history

European Interactive Pain Course03.-07.09.07
Examples of patterns of pain for various types of headache
Migraine
Cluster headache
Chronic
tension
headache
Trigeminal
neuralgia
M D M D F S S M D M D F S S M D M D F S SM D M D F S S
M D M D F S S M D M D F S S M D M D F S SM D M D F S S
0
10
0
10
M D M D F S S M D M D F S S M D M D F S SM D M D F S S0
10
Attackendauer ~ 30 min/d
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 240
10
NRS
NRS
NRS
NRS

European Interactive Pain Course03.-07.09.07
Headache and facial pain
Keeping a headache diary
Determine
the
type, frequency
and severity
of headache
Monitoring
of treatment
Download Kopfschmerzkalender: www.dmkg.de

European Interactive Pain Course03.-07.09.07
Pathogenesis of migraine
Congenital
tendency towards
reaction
Congenital
tendency towards
reaction
Triggers:StressLight and noiseFoodstuffs, alcoholEffects
of weather
Hormone fluctuationsChanges
in sleeping-waking-rhythm
Triggers:StressLight and noiseFoodstuffs, alcoholEffects
of weather
Hormone fluctuationsChanges
in sleeping-waking-rhythm
Crossing
migraine
thresholdCrossing
migraine
threshold
Abnormal cerebral activityAbnormal cerebral activity
Abnormal vascular activity
Abnormal vascular activity
HeadacheHeadache
Aura symptomsAura symptoms
Vomiting
center disorder
Vomiting
center disorder
Central sensitization
Central sensitization

European Interactive Pain Course03.-07.09.07
Migraine
Therapeutic regimen in acute migraine
ASA (1 g) or paracetamol (1 g) or ibuprofen (600 mg) or dipyrone (1 g)
After onset of effect of the anti-emeticgive ASA, paracetamol, ibuprofen or dipyrone
Metoclopramide or domperidone 20 mg orally or rectally
Start medicinal therapywith anti-emetic
treatmentafter 20 minutes
Orally: e.g. sumatriptan subcutaneously: 6 mg or25-100 mg rectally: 25 mg or
nasally: 20 mg
If pain relief is inadequate:administration of sumatriptan
No effect Side-effect:vomiting
Recurrence of headache
Repeat after 4 hours at the earliest (max.
300 mg/day)
Repeat after 2 hours at the earliest (max. 12 mg s.c./day or max.
50 mg supp./day or max. 40 mg nasally/day)
On recurrence of headacherepeat sumatriptan
administration
Source: DMKG 2000 Guidelines

European Interactive Pain Course03.-07.09.07
Triptans – Onset of effect
Source: SPCs
SubstanceSubstance TrademarkTrademark FormulationFormulation DosesDoses Onset
of effectOnset
of effect
SumatriptanSumatriptan Imigran®Imigran®
s.c.orallynasallyrectally
s.c.orallynasallyrectally
6 mg50 –
100 mg
10 –
20 mg25 mg
6 mg50 –
100 mg
10 –
20 mg25 mg
10 –
15 min30 min15 min30 min
10 –
15 min30 min15 min30 min
ZolmitriptanZolmitriptan Asco
Top®Asco
Top®
Asco
Top®Asco
Top®
orally
(SL tab.)nasallyorally
(SL tab.)
nasally2.5 mg
2.5 –
5 mg2.5 mg
2.5 –
5 mg60 min15 min60 min15 min
RizatriptanRizatriptan Maxalt
lingua®Maxalt®Maxalt
lingua®
Maxalt®orally
(SL tab.)
orallyorally
(SL tab.)
orally10 mg10 mg10 mg10 mg
30 min30 min30 min30 min
NaratriptanNaratriptan Naramig®Naramig® orallyorally 2.5 mg2.5 mg 60 min60 min
AlmotriptanAlmotriptan Almogran®Almogran® orallyorally 12.5 mg12.5 mg 30 min30 min
EletriptanEletriptan Relpax®Relpax® orallyorally 40 mg40 mg 30 min30 min
FrovatriptanFrovatriptan Allegro®Allegro® orallyorally 2.5 mg2.5 mg 2 h2 h

European Interactive Pain Course03.-07.09.07
Ferrari MD et al (THE LANCET 2001)
Large metaanalysis
of 53 randomised
double-blind controlled studies
in a total of 24,089 patients
The
parameters
analysed
included: Pain relief
at 2 hours
RecurrenceTolerability
versus
100mg sumatriptan
Oral triptans in acute migraine treatment

European Interactive Pain Course03.-07.09.07
The differences between triptans
are small, but relevant for the
individual patient
Compared with placebo, the response rate of all triptans
is 79-89%
Oral triptans in the treatment of acute migraine
Ferrari MD et al (THE LANCET 2001)

European Interactive Pain Course03.-07.09.07
Sumatriptan:Long-standing
experience, well tolerated, good effect
(variety
of
formulations)Zolmitriptan:A good alternative in many
patients; no weaknesses; well tolerated
Rizatriptan (10mg):Somewhat
shorter
time to Cmax
Naratriptan: Very
well tolerated, but
weaker
and slower
Almotriptan:Good effect
and well tolerated
Eletriptan (80mg): Good effect, less
recurrence, less
well tolerated
Frovatriptan*:Long elimination
half-life
Orale triptans in acute migraine treatment
*) not
in the
Ferrari protocol
(THE LANCET 2001) Ferrari MD et al (THE LANCET 2001)

European Interactive Pain Course03.-07.09.07
Pharmacological treatment of migraine attacks Triptan contraindications
Vascular disease
Coronary arteries, brain arteries, peripheral blood vessels
Pregnancy and lactation
Dangerous interactions with ergotamines
are possible; comedication must therefore be avoided
Age <18 (except sumatriptan) or >65
Basilar migraine, familial hemiplegic migraine
Limitations on use:
Comedication
with SSRIs

European Interactive Pain Course03.-07.09.07
Pharmacological treatment of migraine attacks Triptans
Side effects:
Fatigue, exhaustion
Vertigo
Flush, pressure, tightness
neck and chest
Tingling / paresthesia
involving the head or extremities
Heaviness in the limbs

European Interactive Pain Course03.-07.09.07
A – No riskB – No evidence of increased
riskC – Risk cannot be ruled outD – Definite evidence of
increased riskX - Absolute risk
Drugs for treating headache during pregnancy
Active drug substance CategoryParacetamol
B
Caffeine
BMetoclopramide
B
Metoprolol
BMagnesium
B
Fluoxetine
BIbuprofen
and NSAIDs
B/D in 3rd trimester
Aspirin
C/D in 3rd trimesterTriptans
C
Flunarizine
COther
beta-blockers
C
Amitriptyline
CValproate
D/X
Ergotamines
XFrom
Evers

European Interactive Pain Course03.-07.09.07
Migraine prophylaxis
Drug therapy – key drugs:
Metoprolol
or propranolol
Flunarizine
Valproic
acid
Amitriptyline
Topiramate
Naproxen premenstrually

European Interactive Pain Course03.-07.09.07
Migraine prophylaxis
Non-pharmacological therapy
Antistress techniques
Relaxation
techniques
Biofeedback
Endurance
sports
Acupuncture

European Interactive Pain Course03.-07.09.07
Part 1: The primary headaches
Migraine
Tension-type headache
Cluster headache and other trigeminal autonomic cephalalgias
Other primary headache disorders
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Part 1: The primary headaches
Migraine
Tension-type headache
Cluster headache and other trigeminal autonomic cephalalgias
Other primary headache disorders
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Tension-type headache
Lifetime prevalence of 80%
Headache duration: 30 min –
7 days
2 characteristics:Bilateral location
pressing/tightening
(non- pulsating) quality
mild or
moderate intensity
not
aggravated
by
routine physical
activity
such as
walking
or
climbing
stairs
2 characteristics:no nausea
or
vomiting
(anorexia
may
occur)
no more
than
one
of photophobia
or
phonophobia
2 + 2 = Tension-type headache

European Interactive Pain Course03.-07.09.07
Tension-type headache
Episodic TTH:At least 10 episodes
occurring
on <15 days
per month
for
at
least 3 months
Chronic TTH:Headache
occurring
on ≥15 days
per month
on average
for
more
than
3 months

European Interactive Pain Course03.-07.09.07
Congenital
predisposition
Poor
physical
posture Psychosocial
triggers:Everyday
stressInterpersonal conflictChronic
feeling
of inability
to cope
Tense
muscles
Disorder
of brain
metabolismCentral sensitization
Headache
Tension-type headache model
Travell/Simons. Trigger
Point Flip Chart. Lippincott
Williams & Wilkins (1996)

European Interactive Pain Course03.-07.09.07
Tension-type headache
Treatment of acute tension-type headache
Paracetamol, conventional NSAIDs
or metamizole
Combination of 250 mg acetylsalicylate, 250 mg paracetamol und 65 mg caffeine
Flupirtine
100-300 mg
Topical application of peppermint oil

European Interactive Pain Course03.-07.09.07
Tension-type headache
Treatment of chronic tension-type headache
Keeping a headache calendar
(www.dmkg.de
or www.americanheadachesociety.org)
Pharmacological
prevention
Non-pharmacological
prevention
Combination
of pharmacological
and non-pharmacological strategies
(Holroyd
et al. 2001)

European Interactive Pain Course03.-07.09.07
Tension-type headache
Pharmacological prevention
Tricyclic
Antidepressants (amitriptyline, doxepin, imipramine,…)
Other antidepressants (mirtazapine, venlafaxine,…)
Valproate, gabapentin, topiramate
Tizanidine
Botulinum
toxin injections are ineffective in the therapy of
chronic TTH (Evers et al. 2002)

European Interactive Pain Course03.-07.09.07
Tension headache
Non-pharmacological prevention
Regular
physical
activity/sports
Avoid/stop
smoking/caffeine
abuse
Adopt
a regular
lifestyle
(sleep, regular
meals, etc.)
Relaxation
techniques
/ biofeedback
Stress mangement
training
Intractable
cases:
Multimodal headache
program

European Interactive Pain Course03.-07.09.07
Multimodal treatment program for patients with chronic headache
Erlangen program:
8 patients
in a group
Duration: 8 weeks
(twice
weekly, 3 –
9 pm)
Neurologist, psychologist, exercise
therapist
Particular
treatment
elements:
stress management
training, education,
exercise
sessions, PMR-training, biofeedback therapy

European Interactive Pain Course03.-07.09.07
Multimodal treatment program for patients with chronic headache
B. Gunreben et al.: Effectiveness of an intensive multidisciplinary treatment programme for headache. Headache (2009)
A 20h-programm is
not superior
to standard
care
The
intensive (96h)- therapy is
highly
effective
for
patients
with
chronic headaches
and succeeds
the
20h-programm and standard
care

European Interactive Pain Course03.-07.09.07
Part 2: The secondary headaches
Headache attributed to trauma
Headache attributed to vascular disease
…
Headache attributed to a substance or its withdrawal
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Part 2: The secondary headaches
Headache attributed to trauma
Headache attributed to vascular disease
…
Headache attributed to a substance or its withdrawal
Medication-overuse headache (MOH)
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Medication-overuse headache
IHS- Criteria
Headache
present
on 15 or
more
days/ month
Regular
overuse
for
≥3 months
of one
or
more
drugs
that
can
be taken
for
acute
treatment
of headache
Headache
has developed
or
markedly
worsened
during
medication overuse
Headache
resolves
or
reverts
to its
previous
pattern
within
2
months
after
discontinuation
of overused
medication

European Interactive Pain Course03.-07.09.07
Medication-overuse headache
Prevalence
of 1 -1,5% (2,6% in women
in 0,2% in men)
First periodic (e.g. migraine), then permanent
“chameleon”, characteristics
shifting
from
migraine-like
to those
of
tension-type
headache
Overuse
is
defined
in terms
of duration
(≥3 months
and treatment days
per week
(on 2 or
more
day
each
week)
MOH can
occur
in headache-prone
patients
when
acute
headache medications
are
taken
for
other
indications

European Interactive Pain Course03.-07.09.07
Medication-overuse headache
Pathogenesis (presumed)
Genetic
predisposition?
Medication induces changes in serotonergic/dopaminergic
synapses
Disinhibition
of the supraspinal
and trigeminal nociceptive
system

European Interactive Pain Course03.-07.09.07
DMKG recommendation
Do not
take
any
headache
or
migraine
medicine
for
longer
than
3 days
in succession
or
on more
than
10 days
per month

European Interactive Pain Course03.-07.09.07
Treatment
Abrupt substance
withdrawal
for
at least 14 days
(opioids, benzodiazepines, barbiturates
must
be
tapered)
During
withdrawal: prednisone
100 mg for
5 days, adequate hydration, long
lasting
NSAIDs
(Naproxen
500 mg)
Concurrent
pharmacological
treatment
of causative
headache disorder
(amitriptyline, topiramate)
Supportive
behavioural
therapy
(high rate of relapse
-
38% in the
first
year)
Medication-overuse headache

European Interactive Pain Course03.-07.09.07
Take-Home Messages Headache
The
IHS-Classification
distinguishes
between primary and secondary headaches (headache
as a symptom
of an underlying
disease)
Göbel. Die Kopfschmerzen. Springer (2004)
A thorough
history and examination is
needed for
an accurate
headache
diagnosis
The
most
common
headache
dignoses
are migraine, tension-type headache and
medication-overuse headache

European Interactive Pain Course03.-07.09.07
Take-Home Messages Headache
Migraine
attacks
can
be
treated
with
a combination
of antiemetics and
classical analgetics in an adequate dose. If
pain
is
not
reliefed properly, triptans should
be
administered
TTH can
be
treated
with
classical
analgetics
in an adequate dose
Drug treatment
should
not
exceed
10 days/month
For chronic
headache: combination of pharmacological and non-
pharmacological strategies

European Interactive Pain Course03.-07.09.07
The International Classification of Headache Disorders
Headache Classification Subcommittee of the International Headache Society
2nd Edition 2003Cephalalgia 2004; 24 (Suppl 1): 1-160.
www.ihs-classification.org

European Interactive Pain Course03.-07.09.07
Part 1
Primary headache disorders
Part 2
Secondary headache disorders
Part 3
Cranial
neuralgias, central
and primary
facial
pain
and other headaches
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Part 1: The primary headaches
Migraine
Tension-type headache
Cluster headache and other trigeminal autonomic cephalalgias
Other primary headache disorders
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Part 1: The primary headaches
Migraine
Tension type headache
Cluster headache and other trigeminal autonomic cephalalgias
Other primary headache disorders
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Concomitant symptomsConjunctival
injection, miosis,
ptosis, lacrimation, rhinorrhoea
Concomitant symptomsConjunctival
injection, miosis,
ptosis, lacrimation, rhinorrhoea
CharacteristicsVery painful, restlessness,unilateral, periorbital, temporal
CharacteristicsVery painful, restlessness,unilateral, periorbital, temporal
AttacksDuration: 15-180 min1–8 / 24 h, at night, same time
AttacksDuration: 15-180 min1–8 / 24 h, at night, same time
Clusters1-3 months (episodic CH)
No remission (chronic CH)
Clusters1-3 months (episodic CH)
No remission (chronic CH)
Cluster Headache

European Interactive Pain Course03.-07.09.07
Cluster Headache
Trigger factors
Alcohol
Nitroglycerin
Histamine
Relaxation, but also physical strain
High altitudes
Flickering lights

European Interactive Pain Course03.-07.09.07
Cluster Headache
Pathogenesis (presumed)
Genetic component?
Activation
of the
posterior
hypothalamic
grey
matter
Non-septic inflammation
in the cavernous sinus and
in the region of the superior ophthalmic vein
Chronobiologic
disease?
Symptomatic: process of midline-structures

European Interactive Pain Course03.-07.09.07
Cluster Headache
Treatment of attacks
Inhalation of 100% oxygen (10l/min for 20 min via face mask)
Triptans
(Sumatriptan
s.c./nasal spray, Zolmitriptan
nasal spray)
Intranasal lidocaine
Treatment

European Interactive Pain Course03.-07.09.07
Cluster Headache
Prophylactic treatment
Verapamil
(>320 mg daily)
Steroids (Prednisone 100 mg daily, tapered over 10 to 12 days)
Lithium, Topiramate, Gabapentin, Valproat, Melatonin, Triptans
Occipital nerve block (steroids and anaesthetics)
Implantation of an occipital nerve stimulator
Deep brain stimulation of the hypothalamus

European Interactive Pain Course03.-07.09.07
Part 1
Primary headache disorders
Part 2
Secondary headache disorders
Part 3
Cranial
neuralgias, central
and primary
facial
pain
and other headaches
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
Part 1
Primary headache disorders
Part 2
Secondary headache disorders
Part 3
Cranial neuralgias, central
and primary
facial
pain
and other headaches
The International Classification of Headache Disorders

European Interactive Pain Course03.-07.09.07
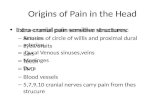
Trigeminal neuralgia
SymptomsVery intense painStrictly unilateral in the region of one or several branches of the trigeminal nerveSudden attacks of shooting, electric shock-like painDuration of the attacks: seconds to minutesUp to 200 attacks/dayTypical trigger mechanisms such as swallowing, talking, chewing, cleaning teeth, etc.Develops usually in mid to late life

European Interactive Pain Course03.-07.09.07
Trigeminal neuralgia
Classical trigeminal neuralgiaNot attributed to another disordercompression
of the
trigeminal
root
by
tortuous
or
aberrant
vessels
Symptomatic trigeminal neuralgiaLesions of brainstem, neoplasm (neurinoma
of the acoustic
nerve), inflammation (e.g. multiple sclerosis)

European Interactive Pain Course03.-07.09.07
Trigeminal neuralgia
MedicationAnticonvulsants (carbamazepine, oxcarbazepine, gabapentin,…)NSAIDs
and opioids
are ineffective
SurgeryMicrovascular
decompression of the trigeminal nerve
Gamma-knife
radiosurgery
(radiation
of the
nerve root)Percutaneous
treatment
(destruction
of the
gasserian
ganglion)