H. ZAGHOUANI, N. EZZAIRI, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA, L. BEN CHRIFA,H. AMARA,...
33
H. ZAGHOUANI, N. EZZAIRI, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA, L. BEN CHRIFA,H. AMARA, D. BEKIR, CH. KRAIEM Departement of radiology, Hospital of Farhat Hached, Sousse, Tunisia NR37
-
Upload
marvin-russell -
Category
Documents
-
view
215 -
download
0
Transcript of H. ZAGHOUANI, N. EZZAIRI, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA, L. BEN CHRIFA,H. AMARA,...

H. ZAGHOUANI, N. EZZAIRI, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA, L. BEN CHRIFA,H. AMARA, D. BEKIR, CH.
KRAIEMDepartement of radiology, Hospital of Farhat Hached, Sousse,
Tunisia
NR37

Rathke’s cleft cysts (RCCs) are benign congenital, non-
neoplastic sellar and/ or suprasellar lesions originating
from epithelial remnants of Rathke’s pouch .
These cysts are extremely common, found during
routine autopsies in 13% to 22% of normal pituitaries.

In 1913, Goldzieher described the first case of RCC
as an incidental postmortem finding.
The description of RCC has expanded since the
advent of computed tomography (CT) scanning and
magnetic resonance imaging (MRI), showing that
the incidence of this disease wich discovery was
only by autopsy, was underestimated.

The aim of this work is to emphasize the value of MRI in
the positive and differential diagnosis of this disease
through a retrospective study of 5 cases of Rathke’s
cleft cyst with a literature review.

We retrospectively analyzed the records of five patients
with Rathke’s cleft cysts collected in the service of
radiology in the hospital of Farhat Hached Sousse.
A brain MRI was performed for all patients. All the
cysts were discovered incidentally.

There were two female and three male patients ranging
in age from 14 to 48 years.
MR examinations were performed using 1.5-T
imagers.
Axial and coronal T1-weighted images were obtained
without administration of gadolinium.
With axial and coronal FSE T2-weighted images.
Section thickness was 4 mm, with intersection spacing
of 0%.

The signal, shape, size, seat and reports of the lesions were
analyzed.
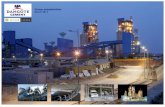
It showed in all cases a cystic formation of the sellar
region with variable signals and sizes.
The localization of the cysts was strictly intrasellar in 4
cases and extended to the suprasellar region in one case.
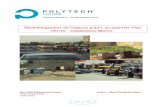
Of the five MR scans reviewed, the lesions were of low
signal intensity in T1-weighted images, there was no
enhancement in post-gadolinium sequences .They were
recorded to be of high intensity T2-weighted images.


Coronal T1 MR image Coronal T1 MR image Coronal T2 MR image Coronal T2 MR image
Coronal postcontrast T1 MR image
Coronal postcontrast T1 MR image
Sagittal post contrast T1-weighted MR image
Sagittal post contrast T1-weighted MR image

Rathke’s cleft cyst (RCC) was first incidentally reported
by Lushka in 1860 as ‘an epithelial area in the capsule
of the human hypophysis resembling oral mucosa’.
The first symptomatic RCC case was described by
Goldzieher in 1913.

RCCs have been referred to by a variety of names
including pituitary cyst, mucoid epithelial cyst,
intrasellar epithelial cyst, Rathke’s pouch cyst, and
colloid cyst of the pituitary.
Not until 1934 did Frazier and Alpers propose its
contemporary name of tumor of Rathke’s cleft.

As Voelker and colleagues have stated, the most common
theory about the origin of RCCs is that the cysts are derived
from true remnants of the embryologic Rathke pouch.
On or about the 24th day of embryonic life, the Rathke pouch
arises as a dorsal diverticulum from the stomodeum; it is
lined with epithelial cells of ectodermal origin.

At approximately the same time, the infundibulum forms
as a downgrowth of the neuroepithelium from the
diencephalon.
By the fifth week, the Rathke pouch comes into contact
with the infundibulum, and the neck of the pouch
becomes occluded at the buccopharyngeal junction.
During the sixth week, the Rathke pouch separates from
the oral epithelium. Subsequently, the pars distalis of the
pituitary gland develops from the anterior wall of the
pouch.

The posterior wall does not proliferate and remains as the
poorly defined pars intermedia.
The residual lumen of the pouch is reduced to a narrow
Rathke cleft, which generally regresses. The persistence
and enlargement of this cleft is considered to be the cause
of the RCC.
Other authors have different theories regarding the
formation of RCCs, suggesting instead that the cells of
origin are derived from the neuroepithelium or the
endoderm, or that they come from metaplastic anterior
pituitary cells.

Rathke cleft cysts are smoothly marginated cysts that vary in
size from a few millimeters to 1–2 cm.
The contents vary from clear CSF-like fluid to thick mucoid
material.
Microscopically, they are similar to other endodermal cysts
(neurenteric and colloid). They are lined by pseudostratified
or single-layered columnar or cuboidal epithelium.

Cilia and scattered mucin-secreting goblet cells are
common. Many cysts have squamous differentiation,
and cornified squamous pearls are occasionally
identified.
The intracystic nodule consists of mucinous material at
histologic examination. Biochemical analysis of this
material is consistent with cholesterol and protein.

Forty percent are completely intrasellar, while 60%
have some suprasellar extension through the cleft of the
diaphragma sella .
Completely suprasellar cysts are rare .

RCCs often produce no symptoms and so are usually
discovered incidentally, when radiographic or necropsy
findings are reviewed.
Symptomatic RCCs are uncommon, but cysts can
enlarge and cause symptoms secondary to compression
of the pituitary gland, pituitary stalk, optic chiasm, or
hypothalamus.
Symptomatic RCCs vary in presentation: headache,
visual and/or endocrine disturbance.

MRI is the modality of choice in the detection of RCCs.
It is superior to CT scanning for evaluating RCC mass
extension.
Sagittal and coronal MRI scans provide reliable
information concerning the relationship of the mass to
the optic nerves, optic chiasm, and hypothalamus.

Coronal MRI is also helpful in the evaluation of the
lateral extension of the sellar cyst and its relationship to
the internal carotid arteries and cavernous sinuses. MRI
also has superior multiplanar capabilities and contrast
resolution compared with those of CT scanning.
The advantage of CT scanning is that it is superior to
MRI in depicting small amounts of calcium.

This advantage can be important, because the presence
of calcification tends to indicate an alternative
diagnosis, such as craniopharyngioma, although small
calcifications are observed in some cases of RCC. CT
scanning is also superior to MRI in the evaluation of
associated bony remodeling.

Rathke cleft cysts (RCCs) frequently appear as well-
circumscribed, hypo-attenuating, cystic sellar masses
that may have suprasellar extension.As a result of the
different cystic contents, RCCs may appear iso-
attenuating or hyperattenuating relative to the brain
parenchyma.
RCCs usually have a thin wall that may enhance.

Variability in CT scan contrast enhancement among
individual cysts may reflect squamous metaplasia in the
wall or a peripherally displaced rim of pituitary tissue.
Extravasation of cystic contents may inflame nearby
structures, resulting in enhancement.
Calcification characteristically is not depicted on CT
scans, although Shin and colleagues have described this
finding in a number of cases.Complex cysts may have
septations.
Large cysts may cause bony remodeling.

The best imaging clue is a non enhancing non calcified
intra- and/or suprasellar cyst with an intracystic nodule .
While this is the typical picture, the imaging
characteristics vary widely.
Approximately half are hyperintense on T1- weighted
images, while half are hypointense. On T2-weighted
images, 70% are hyperintense and 30% are iso- or
hypointense.

Although no characteristic MRI features have been
identified, many RCCs are in 1 of the following 2
groups:
• Rathke cleft cysts (RCCs) with low signal intensity on
T1-weighted images and high signal intensity on T2-
weighted images.
• RCCs with high signal intensity on T1-weighted images
and variable signal intensity on T2-weighted images.
The cystic contents of the first group resemble those of
cerebrospinal fluid (CSF). In the second group, an
increase in the signal on T1-weighted images has been

related to the high content of mucopolysaccharides, which is
believed to result from an increase in the number of mucin-
secreting cells in the cyst wall, as well as from an increase
in the activity of these cells.
Uncommon cases with high signal intensity on T1-weighted
images and low signal intensity on T2-weighted images
have been suggested to result from a combination of
factors, including the presence of mucopolysaccharides,
chronic hemorrhage, a high cholesterol content, and
cellular debris from the cyst wall.

A small nonenhancing intracystic nodule is considered a
virtually pathognomonic sign of a Rathke cleft cyst.
These nodules show high signal intensity on T1-
weighted images and low signal intensity on T2-
weighted images, and they do not enhance.
Rathke cleft cysts do not enhance after contrast material
administration, although an enhancing rim of displaced
compressed pituitary gland is present in approximately
half of the cases.

The report's authors went on to conclude that, with
regard to RCCs, DWI-SSFSE with apparent diffusion
co-efficient (ADC) values provides objective
information for differentiation from other sellar cysts.
DWI-SSFSE with ADC values can also be employed in
the differentiation of RCCs from craniopharyngiomas
and hemorrhagic pituitary adenomas. All the RCCs are
hypo-intense relative to the normal brain parenchyma
(restricted diffusion) .

The differential diagnosis for Rathke cleft cysts includes
craniopharyngioma, cystic pituitary adenoma, or other
non neoplastic cysts (arachnoid cysts or
epidermoids) .
Unlike Rathke cleft cysts, craniopharyngiomas typically
demonstrate calcification and approximately 90% have
nodular, globular, or rim enhancement.

The presence of solid enhancing nodules in the cyst wall
also favors the diagnosis of craniopharyngioma.
The rare noncalcified cystic nonenhancing
craniopharyngioma, a finding more common in adults
than in children, may be impossible to distinguish from
Rathke cleft cyst with imaging findings alone.

The most common approach in the treatment of RCCs is
transsphenoidal surgery, in which the cyst is partially
excised and drained.
This method is effective and helps to preserve pituitary
function.
Radical excision can cause additional and unnecessary
pituitary damage; therefore, it is not the treatment of choice.
In transsphenoidal surgery, the cyst is opened, a biopsy
specimen is obtained from the wall, and the cyst is drained
into the sphenoid sinus.

An interesting aspect of treatment is the decrease in the
size of the cyst after high-dose steroid therapy.
Although the pathophysiologic mechanism is not clear,
the steroids are assumed to have an effect on the
secretion or absorption of cystic fluid. This finding
suggests that steroid therapy may be useful in some
patients with an RCC and inflammatory changes.
Further study in this area is needed to gauge its
effectiveness is the treatment of RCCs.

The MRI is effecticient in the positive and especially
the differential diagnosis of these cysts, and to guide the
therapeutic decision.Once the diagnosis
is considered, a spaced clinical and MRI monitoring is
adopted in cases of asymptomatic cyst, while a surgical
treatment is proposed for the rare symptomatic cysts.