Gynecology 5th year, 7th lecture (Dr. Muhabat Salih Saeid)
25
ECTOPIC PREGNANCY Dr. Muhabat Salih Saeid MRCOG LONDON UK
-
Upload
college-of-medicine-sulaymaniyah -
Category
Health & Medicine
-
view
2.566 -
download
2
description
The lecture has been given on Dec. 20th, 2010 by Dr. Muhabat Salih Saeid.
Transcript of Gynecology 5th year, 7th lecture (Dr. Muhabat Salih Saeid)

ECTOPIC PREGNANCY
Dr Muhabat Salih Saeid
MRCOG LONDON UK
WHEN A WOMAN PRESENTS WITH AN EARLY PREGNANCYhellip Ask yourself two questionshellip
Where is this pregnancy
Is it viable
WHERE IS THIS PREGNANCY
In a woman with an early pregnancy you must determine if the pregnancy is intrauterine or an ectopic because her life could depend on it
Ectopic Pregnancy 1048708 Pregnancy anywhere outside uterine cavity 1048708 Fallopian tube most common location 1048708 Second leading cause of maternal mortalityRisk Factors 1048708 Pelvic inflammatory disease Age Previous Ectopic Previous tubal ligationSymptoms 1048708 Abdominal pain vaginal bleeding syncope amenorrhea 1048708 Occurs 5-8 weeks after last menstrual period
ECTOPIC PREGNANCY 95 are in the fallopian tube (70 ampulla 12 isthmus 11 fimbria 2 interstitialcornual) Ovarian occurs about 3 of the time abdominal 1 of the time cervical lt1 of the time
Seeber 2006
HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
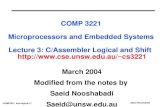
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

WHEN A WOMAN PRESENTS WITH AN EARLY PREGNANCYhellip Ask yourself two questionshellip
Where is this pregnancy
Is it viable
WHERE IS THIS PREGNANCY
In a woman with an early pregnancy you must determine if the pregnancy is intrauterine or an ectopic because her life could depend on it
Ectopic Pregnancy 1048708 Pregnancy anywhere outside uterine cavity 1048708 Fallopian tube most common location 1048708 Second leading cause of maternal mortalityRisk Factors 1048708 Pelvic inflammatory disease Age Previous Ectopic Previous tubal ligationSymptoms 1048708 Abdominal pain vaginal bleeding syncope amenorrhea 1048708 Occurs 5-8 weeks after last menstrual period
ECTOPIC PREGNANCY 95 are in the fallopian tube (70 ampulla 12 isthmus 11 fimbria 2 interstitialcornual) Ovarian occurs about 3 of the time abdominal 1 of the time cervical lt1 of the time
Seeber 2006
HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

WHERE IS THIS PREGNANCY
In a woman with an early pregnancy you must determine if the pregnancy is intrauterine or an ectopic because her life could depend on it
Ectopic Pregnancy 1048708 Pregnancy anywhere outside uterine cavity 1048708 Fallopian tube most common location 1048708 Second leading cause of maternal mortalityRisk Factors 1048708 Pelvic inflammatory disease Age Previous Ectopic Previous tubal ligationSymptoms 1048708 Abdominal pain vaginal bleeding syncope amenorrhea 1048708 Occurs 5-8 weeks after last menstrual period
ECTOPIC PREGNANCY 95 are in the fallopian tube (70 ampulla 12 isthmus 11 fimbria 2 interstitialcornual) Ovarian occurs about 3 of the time abdominal 1 of the time cervical lt1 of the time
Seeber 2006
HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Ectopic Pregnancy 1048708 Pregnancy anywhere outside uterine cavity 1048708 Fallopian tube most common location 1048708 Second leading cause of maternal mortalityRisk Factors 1048708 Pelvic inflammatory disease Age Previous Ectopic Previous tubal ligationSymptoms 1048708 Abdominal pain vaginal bleeding syncope amenorrhea 1048708 Occurs 5-8 weeks after last menstrual period
ECTOPIC PREGNANCY 95 are in the fallopian tube (70 ampulla 12 isthmus 11 fimbria 2 interstitialcornual) Ovarian occurs about 3 of the time abdominal 1 of the time cervical lt1 of the time
Seeber 2006
HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

ECTOPIC PREGNANCY 95 are in the fallopian tube (70 ampulla 12 isthmus 11 fimbria 2 interstitialcornual) Ovarian occurs about 3 of the time abdominal 1 of the time cervical lt1 of the time
Seeber 2006
HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

HOW TO YOU DETERMINE LOCATION OF THE PREGNANCY First determine dating by LMP Then perform ultrasound If you can see location of the pregnancy
you are done If you cannothellipit becomes more
complicatedhellip
EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

EARLY PREGNANCY WITH UNKNOWN LOCATION Check a serum BHCG If it is above the discriminatory zone
(DZ)mdash(this is different at every hospital) an intrauterine pregnancy should be seen
Then do an ultrasound to see if you see the pregnancy
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGgtDZ and pregnancy seen in the
uterus you are done If BHCGgtDZ and no pregnancy seen in
the uterus it is an ectopic until proven otherwise
EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

EARLY PREGNANCY WITH UNKNOWN LOCATION If BHCGlt DZ and you do not see the
pregnancy on the ultrasound consider your patienthellip
Is shehellipUnstable or stableHave pain Have risk factors for ectopicYour differential diagnosis is intrauterine
pregnancy just too small to see on ultrasound vs ectopic
EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

EARLY PREGNANCY WITH UNKNOWN LOCATIONbull Generally BHCG will double in 48 hoursbull If the patient is stable you can have her
return in 48 hours for repeat BHCGbull If is doubling appropriately likely normal
intrauterine pregnancy and can order ultrasound when gtDZ
bull If not doubling appropriately consider treatment for ectopic (methotrexate or surgery)
USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

USS FINDINGS Empty uterus Adnexal mass
+- FHRRing of blood flow on dopplerTenderness on probe pressure over mass
Free fluid especially POD TV scan ideally if available
ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

ECTOPIC WITH FHR
Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Tubal Ectopic Pregnancy
Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Ectopic Pregnancy Management-determine hemodynamic stability Medical Methotrexate-unruptured small no cardiac activity compliant patient Surgical Laparoscopy
bull Salpingostomybull Salpingectomy
Laparotomy
Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Medical therapy Medical therapy involving methotrexate
The patient must be hemodynamically stable
no signs or symptoms of active bleeding or hemoperitoneum
she must be reliable compliant and able to return for follow-up
size of the gestation which should not exceed 35 cm at its greatest dimension on ultrasound (US) measurement
She should not have any contraindications to the use of methotrexate
Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Contraindications to Methotrexate
A bhCG level of greater than 15000 IUL fetal cardiac activity and free fluid in the cul-de-sac on US (presumably representing tubal rupture) documented hypersensitivity to methotrexate breastfeedingimmunodeficiencyalcoholismalcoholic liver disease or any liver diseaseblood dyscrasiasleukopeniathrombocytopeniaanemia active pulmonary diseasepeptic ulcer diseaserenal hepatic or hematologic dysfunction
Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Surgical therapy
Laparoscopy has become the recommended approach in most cases
Laparotomy is usually reserved for patients
who are hemodynamically unstable
patients with cornual ectopic pregnancies
for surgeons inexperienced in laparoscopy and in patients where laparoscopic approach is difficult (eg secondary to the presence of multiple dense adhesions obesity or massive hemoperitoneum)
Total salpingectomy is the procedure of choice In a patient who has completed childbearing and no longer desires fertility in a patient with a history of an ectopic pregnancy in the same tube in a patient with severely damaged tubes
Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Expectant management
Candidates for successful expectant management are asymptomatic and have no evidence of rupture or hemodynamic instability Furthermore they should portray objective evidence of resolution such as declining bhCG levels They must be fully compliant and must be willing to accept the potential risks of tubal rupture
Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Ectopic Pregnancy- Unusual Variants Heterotopic Pregnancy Simultaneous IUP and
ectopic gestations Rare- 1 in 30000 pregnancies
Abdominal Pregnancy-can occur anywhere in peritoneal cavity (1 in 3000)
Cervical Pregnancy (1 in 10000) May need hysterectomy
Ovarian Pregnancy (1 in 7000) Oophorectomy usually required
Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-

Prognosis for Subsequent Fertility
Overall subsequent pregnancy rate is 60 other 40 are infertile
One-third of pregnancies after an ectopic pregnancy are another ectopic pregnancy one-sixth are spontaneous abortions
Only 33 of women with ectopic pregnancy will have a subsequent live birth
- Ectopic pregnancy
- When a woman presents with an early pregnancyhellip
- Where is this pregnancy
- Slide 4
- Slide 5
- Ectopic Pregnancy
- How to you determine location of the pregnancy
- Early pregnancy with unknown location
- Early pregnancy with unknown location (2)
- Early pregnancy with unknown location (3)
- Early pregnancy with unknown location (4)
- USS findings
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Ectopic with FHR
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
-