Guidance of Cardiovascular Tissue Regeneration via Novel...
102
Guidance of Cardiovascular Tissue Regeneration via Novel Synthetic & Natural Matrix Approaches by Jeffrey Justin David Henry A dissertation submitted in partial satisfaction of the requirements for the degree of Joint Doctor of Philosophy with University of California, San Francisco in Bioengineering in the Graduate Division of the University of California, Berkeley Committee in charge: Professor Song Li, Chair Professor Tejal Desai Professor Ting Xu Spring 2013
Transcript of Guidance of Cardiovascular Tissue Regeneration via Novel...

Guidance of Cardiovascular Tissue Regeneration via Novel Synthetic & Natural Matrix Approaches
by
Jeffrey Justin David Henry
A dissertation submitted in partial satisfaction of the
requirements for the degree of
Joint Doctor of Philosophy with University of California, San Francisco
in
Bioengineering
in the
Graduate Division
of the
University of California, Berkeley
Committee in charge:
Professor Song Li, Chair Professor Tejal Desai
Professor Ting Xu
Spring 2013


1
Abstract
Guidance of Cardiovascular Tissue Regeneration via Novel Synthetic & Natural
Matrix Approaches
By
Jeffrey Justin David Henry
Doctor of Philosophy in Bioengineering
University of California, Berkeley
Professor Song Li, Chair
Cardiovascular diseases remain the leading cause of mortality in many countries. Devices such as stents, vascular grafts, and heart valves have been developed to treat such diseases. However, many of these devices fail due to thrombotic complications. Recently, the fields of cardiovascular tissue engineering and regenerative medicine have begun to focus on treatments that not only replace diseased tissue, but also aid in the recovery and growth of new healthy tissue. Providing the appropriate matrix for tissue growth is essential to achieving effective tissue engineering solutions. Natural matrix materials can be advantageous as they have high biocompatibility, and are most similar to the native extracellular environment. Additionally, synthetic matrix materials may also provide advantages, since they are easily customizable and provide scalability. This dissertation will discuss work aimed to guide cardiovascular tissue regeneration, using both synthetic and natural approaches. Since non-thrombogenicity is a key concern, a comprehensive review of nonthrombogenic approaches in cardiovascular bioengineering will be presented first. Next, a novel approach, known as in situ vascular tissue engineering is presented and explored as a treatment for replacing clogged blood vessels. Specifically, we investigated the efficacy of small-diameter vascular grafts composed of electrospun nano-to-microscale fibers with immobilized heparin and vascular endothelial growth factor (VEGF). Finally, we discuss the development and efficacy of a naturally derived, injectable amniotic membrane scaffold for treatment of myocardial infarction.

I
Acknowledgements
THIS DISSERTATION IS DEDICATED TO MY BROTHER,
DAREN RAMON HENRY
The most vivid images from my childhood are often of my autistic brother
Daren, and the constant struggles he endured as a result of his mental disability. At that time (early 1980’s), knowledge on autism was very limited, and it took several years until my brother was properly diagnosed. My family and I used to travel all over the country from specialist to specialist, trying to get answers about my brother’s condition. At one particular specialist in New Jersey, I remember staring at odd shaped images on a computer screen. I was six years old and probably unable to really understand what an MRI was, but I stood there in awe as the doctor explained that those images were of my brother’s brain. As technology and medicine advanced, Daren began to receive better treatment for his condition. His quality of life has significantly improved and now our family enjoys a warm, loving relationship with him. The struggle of growing up with a mentally disabled brother forever instilled in me, the heartfelt desire to help improve the lives of people with diseases or disabilities. It also showed me how advances in science and engineering could drastically affect those with medical needs. My brother is a constant reminder of this, and a constant source of motivation in my life.
In addition, I would like to give my heartfelt appreciation and thanks, for the many individuals who have helped me during my doctoral journey. First and foremost, I must thank my parents Arthur & Linda Henry for their constant support, love, and wisdom. They have been and will always be my rock and I am forever grateful to them. I also have to thank my other brother Arthur Hodari Henry for being a great friend, and for pushing me to be a more confident, yet humble, and balanced individual.
Next, I must thank my advisor, Dr. Song Li for giving me the opportunity to join his lab. I thank him for taking a young mechanical engineer in under his tutelage, and providing me with a basis and foundation to conduct scientific research in bioengineering. I am exceptionally grateful for the countless hours of support, mentorship he has offered. Dr. Li’s mentorship instilled confidence, and also taught me to not be afraid to think big.
I also thank the National Institute of Health, Ford Foundation and the Siebel Scholars program for providing, financial support, as well as academic and professional support.

II
I would also like to thank all of my co-authors, lab colleagues and collaborators; Julia Chu, Nikita Derugin, Sze Yue Wong, Lawrence Delrosario, Dr. Danielle An-Chi Tsou, Dr. Kyle Kurpinski, Dr. Craig Hashi, Timothy L. Downing, Dr. Randall Janairo, Dr. Yiquan “Eugene” Zhu, Dr. Aijun Wang, Dr Roykaya Diop, Dr. Hayley Lam, Dr. Lance Yu, Benjamin Lee, Dr. Shyam Patel, Dr. Dong Wang, Julia Chang and Falei Yuan and Dr. Zhenyu Tang and Dr. Randall Lee.
I am especially grateful for the dillegent work of my undergraduate researchers, Surya Kotha, Kellen Chen and Jesse Lou. The opportunity to mentor such talented students has been amazing and especially gratifying. I wish them all the best as they now begin to embark upon their own doctoral journey.
I also thank the many close friends who have been there throughout my journey. Some of whom also told me “you’re crazy, why would you want to spend the next 6 years in school?”. Lastly, I especially thank Ms. Akilah Huguley for her constant patience, love, understanding and support.

III
Table of Contents
Chapter 1: Nonthrombogenic Approaches to Cardiovascular Bioengineering
INTRODUCTION ............................................................................................. 2
• Vascular Disease
• Vascular Grafts
• Stents
• Heart Valves
• Vascularized Tissues
MECHANISMS OF THROMBOSIS ................................................................. 4
• Platelet Adhesion and Activation
• Blood Coagulation
THE ENDOTHELIUM: NATURAL REGULATOR OF THROMBOSIS ............. 6
• Endothelial Cell Regulation of Coagulation
• Endothelial Cell Regulation of Platelet Adhesion and Activation
• Endothelial Cell Regulation of Fibrinolysis
NONTHROMBOGENIC MODIFICATION OF SURFACES ............................. 9
• Modifications Using Anticoagulants
• Modifications to Prevent Platelet Adhesion and Activation
NONTHROMBOGENIC APPROACHES USING ENDOTHELIAL CELLS AND STEM CELLS................................................................................................. 16
• In Vitro Endothelialization
• In Situ Endothelialization
• Nonthrombogenic Surfaces Seeded With Bone Marrow Mesynchymal Stem Cells

IV
SUMMARY ..................................................................................................... 20
Chapter 2 – Development and Characterization of Nano/Micro-fibrous Grafts with VEGF for In Situ Vascular Tissue Engineering
INTRODUCTION ........................................................................................... 22
MATERIALS & METHODS ............................................................................ 23
• Fabrication of Electrospun Scaffolds
• Fabrication of Tubular Scaffolds for Vascular Grafts Implantation
• Mechanical Characterization of Electrospun Scaffolds
• Heparin Modification of Electrospun Scaffolds
• Antithrombogenic Activity of Heparin-Modified Scaffolds
• VEGF Immobilization
• Characterization of VEGF Immobilization and Release
RESULTS ...................................................................................................... 26
• Fabrication of Blended Electrospun Scaffolds
• Mechanical Properties of Blended Electrospun Scaffolds
• Heparin Immobilization
• Antithrombogenic Activity of Immobilized Heparin
• VEGF Immobilization and Release
DISCUSSION ................................................................................................. 33
Chapter 3 – In Vivo Performance of VEGF in Nano/Micro-fibrous Vascular Grafts INTRODUCTION ............................................................................................... 35 MATERIALS & METHODS ................................................................................ 36
• Animal Studies
• Histological Analysis

V
• En Face Immunofluorescence Staining for ECs
• Statistical Analysis
RESULTS .......................................................................................................... 37
• Patency of Bioactive Nano/Micro-fibrous Vascular Grafts
• Endothelialization, Cellular infiltration and Matrix Remodeling
DISCUSSION ..................................................................................................... 44
Chapter 4 - Conclusions and Future Directions .............................................................................................................. 45 Chapter 5 - Development of Injectable Human Amniotic Membrane Matrix for Post-Myocardial Infarction Tissue Repair. INTRODUCTION ............................................................................................... 49
• Motivation: Myocardial Infarction and Cardiac Scar Formation
• Amniotic Membrane: Function & Current Usage
METHODS ......................................................................................................... 49
• Decellularization of Human Amniotic Membrane (hAM)
• Preparation of Injectable hAM Matrix
• Biochemical Characterization of Injectable hAM Matrix
• In Vitro Characterization of Injectable hAM Matrix Cytotoxicity
• Acute, Sub-Acute and Chronic Myocardial Infarction (MI)
Models
• Preliminary hAM Matrix Injection Studies
• Functional Recovery of LV function after hAM Matrix Injection
RESULTS .......................................................................................................... 53

VI
• Characterization of injectable human amniotic membrane (hAM)
matrix
• In vitro studies using bovine aortic endothelial cells (BAECs)
• Acute MI and recovery of LV function following hAM Matrix
Injection
• Sub-Acute MI and recovery of LV function following hAM Matrix
Injection
• Chronic MI and recovery of LV function following hAM Matrix
Injection
CONCLUSIONS & FUTURE DIRECTIONS ........................................................ 63
Chapter 6 - Supplemental Experiments
• Release of SDF-1 from Micro-Fibrous Vascular Grafts
under Flow ................................................................................. 66
• Modification of Nano/Micro-Fibrous Vascular Grafts using
Thrombin Aptamers .................................................................. 70
• Impantation of Nano/Micro-Fibrous Vascular Grafts in a Porcine
Model ........................................................................................ 74
REFERENCES…………………………………………………………………………81

1
Chapter 1 Nonthrombogenic Approaches to Cardiovascular Bioengineering
Portions of this chapter appear in: Li S, Henry JJ. Nonthrombogenic approaches to cardiovascular bioengineering. Annu Rev Biomed Eng. 2011;13:451-75.

2
1. INTRODUCTION
Cardiovascular diseases are a leading cause of mortality in many countries[1, 2].Cardiovascular devices such as vascular grafts, stents, and heart valves have been developed to treat these diseases; however, thrombus formation remains a problem. In the past few decades, antithrombogenic surface modifications have been employed to improve the performance of cardiovascular devices. In addition to biochemical modifications, endothelial cells (ECs) and nonthrombogenic stem cells are used to cover the surface of devices and engineered tissues. A fast-growing area of tissue engineering is to build nonthrombogenic vascularized tissues and organs that can be perfused and integrated into the host upon implantation. In this regard, a nonthrombogenic microvascular network is essential for the function of tissue-engineered vascular tissues and organs. This chapter focuses on the advances in nonthrombogenic surface modifications for cardiovascular tissue engineering and discusses the challenges and barriers that need to be met in order to achieve success. For general reviews on cardiovascular tissue engineering, the reader is referred to previous publications[3-9].
1.1. Vascular Disease
Atherosclerosis, which causes narrowing of the vessel wall, is one of the most severe forms of cardiovascular disease. Bypass surgery is a common surgical intervention to treat atherosclerosis; more than 500,000 vascular bypass grafts are implanted in the United States each year. Additionally, patients experiencing chronic kidney disease or acute renal failure undergo hemodialysis. A non-thrombogenic access graft is necessary to prevent complications associated with hemodialysis. Autologous vessels, such as the saphenous vein and internal mammary artery, are currently the optimal conduits for vascular bypass[10, 11]. However, autologous grafts still have a 35% failure rate, and for many patients, use of an autologous graft is not a viable option. It is estimated that nearly 30% of patients lack a suitable vessel because of size mismatch, preexisting disease, or previous surgery[12].
1.2. Vascular Grafts
Synthetic grafts, which are typically made from materials such as expanded polytetrafluoroethylene (ePTFE) or Dacron, can be used with relatively high success for bypass of large arteries[13-15].
Figure 1.1: Gore-TEX Stretch Vascular Graft. Image taken from goremedical.com

3
When the graft diameter is smaller than 6 mm, as is the case for coronary and infrapopliteal bypass, these grafts are prone to clogging due to thrombosis[10, 16-18]. The development of a nonthrombogenic small-diameter vascular graft could satisfy a large clinical need and thus has been one of the most-pursued goals within the field of cardiovascular bioengineering for many years. Current approaches include antithrombogenic modifications with biomolecules or cells for synthetic vascular grafts and the development of tissue-engineered vascular grafts (TEVGs). In addition to nondegradable polymers such as ePTFE, Dacron, and polyurethane, biodegradable polymers such as poly(lactic acid), poly(caprolactone), and poly(glycolic acid) and their copolymers also are used as graft or scaffold materials
1.3. Stents Another frequently used treatment for vascular clogging is percutaneous angioplasty followed by stent placement.
Figure 1.2: Purcutaneous Angioplasty with Stent Placement. Image taken from heartsurgeons.com
However, the placement of metal stents in the blood vessels often results in significant in-stent restenosis and reocclusion, which involves thrombosis, inflammatory responses, the proliferation of smooth muscle cells (SMCs), and neointima formation. To prevent early thrombogenesis on the stent surface, anticoagulants such as warfarin (an activated Factor IX inhibitor), aspirin (a cyclooxygenase-1 inhibitor), and clopidogrel (an antagonist of platelet ADP-receptor P2Y12) are administered in blood circulation[19]. To suppress SMC proliferation, polymers—such as poly(lactide-co-σ-caprolactone), poly-n-butyl methacrylate and polyethylene–vinyl acetate copolymer, and chondroitin sulfate/gelatin—have been used to coat stents and deliver antiproliferative drugs such as paclitaxel and sirolimus[20-24]. However, owing to the nonspecific effects of these drugs on multiple cell types and the inflammatory responses to polymers, endothelial healing and function are compromised, which may cause late stent thrombosis[25, 26]. Further investigations are needed to select appropriate polymers for stent coating and polymer stents and to develop antithrombogenic modifications of stent surfaces.

4
1.4. Heart Valves Heart valve replacements are widely used to treat valve defects, with more than 100,000 heart valve replacement surgeries performed each year in the United States[8].
Figure 1.3: Aortic Valve Prostheis. Image taken from www.medtronic.com
The current options for valve
replacements include mechanical valves and bioprosthetic valves. Similar to small-diameter synthetic grafts, mechanical valves also incur a high risk of thrombosis. However, patients receiving mechanical heart valves can take oral anticoagulants that significantly reduce the risk
of thrombotic events [27]. Although there is an increased risk of bleeding complications, mechanical valves are still expected to remain viable for the duration of a patient's life. Bioprosthetic valves are relatively nonthrombogenic, and bleeding risk is minimized because lifelong administration of anticoagulants is not needed. Bioprosthetic valves are typically fabricated from decellularized and preserved xenogeneic valves or pericardial tissue. Bioprosthetic valves are not as durable as mechanical valves, and failure occurs by tissue degeneration and calcification. The development of a living tissue-engineered heart valve (TEHV) capable of self-remodeling has been pursued as a strategy to address the limitations of mechanical and bioprosthetic valves. Nonetheless, bioprosthetic valves can now last up to 20 years[28, 29]; thus, the current standard for success in TEHV applications is very high. Although mechanical and bioprosthetic valves dominate over TEHVs in clinical usage, pediatric valve replacements require prosthesis capable of remodeling with the growth of cardiac tissues, and thus still present a need to pursue the development of nonthrombogenic TEHVs. 1.5. Vascularized Tissues and Organs
A big hurdle in tissue engineering is the diffusional limit of oxygen and nutrient transport within three-dimensional (3D) tissues. To grow 3D tissues and organs with thicknesses of more than a few hundred micrometers, perfusion through a microvascular network is needed for the mass transfer in the tissues. Upon implantation of the tissues and organs, their survival and function depend on the blood supply and the integration of the existing vascular network into the host circulation system. To date, decellularization of organs, microfabrication techniques, 3D printing, and coculture of ECs with fibroblasts have been explored to create prevascularized tissues and organs (e.g., liver, heart, and lung)[30-37]. To make these approaches work in vivo, a nonthrombogenic vascular network is one of the essential requirements, and the integration of the vascular network with the host vessels is needed.
2. MECHANISMS OF THROMBOSIS

5
The blood circulatory system is a closed-loop system responsible for the distribution of vital nutrients throughout the body. Injury to the vessel wall results in rapid thrombus (clot) formation to seal the damaged site and prevent blood leakage. Thus, the process of thrombus formation is an essential mechanism for maintaining circulation integrity. Thrombus formation involves the accumulation of circulating platelets at the injury site, as well as the coagulation system that produces thrombin and ultimately fibrin to stabilize the clot.
2.1. Platelet Adhesion and Activation
In the native vasculature, platelet aggregation ensues upon vessel injury through the adhesion of exposed collagen in the subendothelial matrix. This initial adhesion of platelets is mediated by glycoprotein VI and glycoprotein Ib, the membrane receptors that bind to collagen and collagen-bound von Willebrand factor, respectively[38, 39]. Platelet adhesion is also mediated by integrins α2β1 and αIIbβ3, which bind to collagen and fibrinogen/fibrin, respectively[40-42]. Therefore, it is likely that the adsorption of these proteins to blood-contacting surfaces initiates platelet adhesion on the surface of cardiovascular devices and engineered tissues.
The activation of platelets is also a complex subject, especially in the context of biomaterials. The individual factors known to cause activation are numerous and have been discussed previously[39, 43-45]. In some cases, platelet adhesion to a surface alone, including the binding of glycoprotein VI or integrin α2β1 to collagen and the binding of integrin αIIbβ3 to fibrinogen/fibrin, can cause platelet activation. Alternatively, some soluble factors can activate platelets by binding to their receptors. For example, activation of the tissue factor (TF) pathway leads to thrombin production, and thrombin can cleave protease-activated receptor 1 (Par-1) on the platelet surface and activate platelets; thromboxane A2 (TXA2) and ADP can bind to their respective receptors and activate platelets[40, 46-48]. Both mechanisms, platelet adhesion and the exposure to soluble agonists, are believed to be capable of independently initiating platelet activation[40, 48]. However, the relative contribution of each mechanism is still not clearly understood. In general, platelet activation is signified by a drastic change in platelet geometry[49] and by the release of platelet granules containing a variety of potent chemical agonists that amplify the activation and aggregation of platelets[43, 44, 48]. The specific consequences of platelet activation include thrombus formation, inflammatory responses, the stimulation of cardiovascular cells, and the changes of material surfaces.
2.2. Blood Coagulation
Blood coagulation is a series of cascading events that produce thrombin and ultimately fibrin material that stabilizes the thrombus. Blood coagulation is composed of two separate pathways: the intrinsic pathway (or contact-phase

6
pathway) and the extrinsic pathway. Each pathway leads to a common pathway for thrombin generation.
The intrinsic pathway is a series of reactions that occur during the first 100–200 s of initial contact between blood and a surface. Primary components in the intrinsic pathway include Factor XII, kallikrein, high-molecular-weight kininogen, and Factor XI [46, 50, 51]. The intrinsic pathway may not play a significant role during coagulation in the native vasculature. Patients deficient in activated Factor XII still produce elevated levels of thrombin during vascular bypass procedures, suggesting that the intrinsic pathway is not required for thrombus formation on tissue-engineered surfaces[52].
The extrinsic pathway of coagulation is initiated by the exposure of TF to blood. Classically, TF is thought to reside primarily in the adventitial and medial tissue layers of blood vessels[53]. However, there is an increasing amount of evidence that suggests the presence of circulating TF in blood, secreted by monocytes and neutrophils[48, 54, 55]. Thus, TF in blood also may play a prominent role in biomaterial-related thrombus formation[15, 16]. Once exposed, TF activates and interacts with Factor VII to form the activated TF-Factor VIIa complex (also known as the tenase complex). The tenase complex cleaves Factor X to produce activated Factor X (Factor Xa). Factor Xa is then able to activate and interact with Factor V. This action leads to the formation of the Factor Xa–Factor Va complex, also known as the prothrombinase complex, which converts prothrombin to thrombin [46, 48, 54].
Thrombosis is a potent and self-amplifying response necessary for the maintenance of hemostasis. However, to maintain the function of cardiovascular implants such as vascular grafts, stents, heart valves, and vascularized tissues and organs, we need to prevent thrombosis on implant surfaces. Endothelium constitutes an effective cellular layer to inhibit the adhesion and activation of platelets, block the coagulation process, and mediate clot dissolution. With the understanding of these molecular mechanisms, one can design bioactive surfaces to mimic the natural antithrombogenic properties locally or systemically.
3. THE ENDOTHELIUM: NATURAL REGULATOR OF THROMBUS FORMATION
The endothelium serves as a physical barrier that separates circulating blood from thrombogenic tissue components within the vascular wall. More importantly, the endothelium also plays a multifaceted role in hemostasis and actively regulates thrombotic events. Developments in nonthrombogenic cardiovascular tissue engineering have largely focused on achieving EC coverage and/or mimicry of specific antithrombotic elements inherent to ECs. Thus, for the purpose of this review, it is important to give a brief overview of the key mechanisms of EC regulation of thrombus formation. More extensive reviews can be found elsewhere[56-58]. In summary, healthy ECs exert antithrombotic activity

7
by inhibiting coagulation, suppressing platelet aggregation, and stimulating fibrinolysis (Fig 1.4).
3.1 Endothelial Cell Regulation of Coagulation
ECs synthesize several key molecules to counteract blood coagulation events. Heparan sulfate proteoglycan (HSPG), which is expressed on the EC surface, serves as a cofactor of antithrombin- III (AT-III) to facilitate thrombin inhibition [59, 60]. ECs also express thrombomodulin (TM), a functional thrombin receptor on the EC surface. Upon binding to TM, thrombin converts protein C to its active form, activated protein C (APC), which in turn inhibits Factor Va and Factor VIIa[61]. ECs are also responsible for synthesizing TF pathway inhibitor (TFPI), which binds to both Factor VIIa and Factor Xa. As a result, TFPI limits TF-induced activation of the extrinsic coagulation pathway[62, 63]. EC-derived protein S acts as a cofactor for TFPI, increasing TF inhibition by a factor of ∼10 [64] (Fig 1.4).
Figure 1.4 Endothelial cell (EC) regulation of coagulation. Heparan sulfate proteoglycans (HSPGs) are expressed on the EC surface and serve as cofactors for antithrombin-III (AT-III) to facilitate thrombin inhibition.Thrombomodulin is a functional thrombin receptor present on the EC surface. Binding of thrombin to thrombomodulin leads to activated protein C (APC)-induced inhibition of Factor Va and Factor VIIa, which thus limits thrombin production. ECs also secrete tissue factor pathway inhibitor (TFPI). TFPI inhibits the coagulation pathway by binding to both Factor VIIa and Factor Xa. EC-derived protein S acts as a cofactor for TFPI to enhance the inhibition of tissue factor (TF).
Extracellular Matrix

8
3.2. Endothelial Cell Regulation of Platelet Adhesion and Activation
ECs synthesize and release nitric oxide (NO) and prostacyclin (PGI2), both of which suppress platelet adhesion and activation (Fig 1.5)[65, 66]. NO and prostacyclin are constitutively expressed by ECs, and their levels of expression can be modulated in response to fluid shear stress and chemical stimuli[67, 68]. The EC surface also can bind ectonucleotidases that hydrolyze ADP, an agonist of platelet activation[56, 69]. The EC surface has a brush-like layer (0.4–0.5 µm in thickness) of glycocalyx (see Reference[70] for a comprehensive review). The glycocalyx layer consists of proteoglycans with glycosaminoglycan (GAG) side chains and glycoproteins bearing acidic oligosaccharides. GAGs such as HSPGs, chondroitin/dermatan sulfate proteoglycans, and hyaluronic acid/hyaluronan (HA) are expressed by ECs, with heparan sulfate accounting for 50%–90% of side chains. These macromolecules in glycocalyx are negatively charged, which effectively retain water and form a lubrication layer on the EC surface. There is evidence that HSPGs can resist platelet adhesion[71]. In addition, glycocalyx plays an important role in mechanotransduction[72-74]. For example, degradation of heparan sulfate in glycocalyx inhibits shear stress–induced NO production [75].
Figure 1.5: Endothelial cell (EC) regulation of platelet adhesion and activation. ECs synthesize and release nitric oxide (NO) and prostacyclin (PGI2) to suppress platelet adhesion and activation. HSPGs mediate fluid shear stress–induced NO production. The EC surface also can bind ectonucleotidases that hydrolyze ADP, an agonist of platelet activation.
Extracellular Matrix

9
3.3. Endothelial Cell Regulation of Fibrinolysis
ECs produce and release agents that degrade fibrin material and allow dissolution of the clot. Tissue-type plasminogen activator (t-PA), a major initiator of fibrin degradation[76, 77], is constitutively released by ECs. The activity of t-PA is modulated by the expression of plasminogen activator inhibitor type-1 (PAI-1) by ECs[78-80]. Overall, fibrinolytic activity is thus largely dependent on the relative balance between t-PA and PAI-1 expression. Urokinase release from ECs can also initiate fibrin degradation; however, urokinase production is dependent on the state of EC activation due to inflammatory stimuli[81] (Fig 1.6).
Figure 1.6: Endothelial cell (EC) stimulation of fibrinolysis. Tissue-type plasminogen activator (t-PA) is constitutively released by ECs and is the major initiator of fibrin degradation. ECs also secrete plasminogen activator inhibitor type-1 (PAI-1) to modulate the activity of t-PA. Urokinase release from ECs can also initiate fibrin degradation.
4. NONTHROMBOGENIC MODIFICATION OF SURFACES
Nonthrombogenic modifications take advantage of existing knowledge of thrombogenesis. Most strategies have been developed to inhibit the coagulation cascade and prevent platelet adhesion and activation. Strategies utilizing fibrinolytic mechanisms to degrade clots also have been explored, but to a much lesser extent. For example, urokinase immobilization on several biomaterials has been performed, although fibrinolytic activity of immobilized urokinase is significantly lost within 24 h [82, 83], possibly due to the presence of
Extracellular Matrix

10
plasminogen activator inhibitors in circulating plasma. Therefore, this section focuses on biochemical modifications of implant surfaces to inhibit coagulation and prevent platelet adhesion and activation. The use of ECs and stem cells for the modification of surfaces and the construction of vascular network is discussed in the next section.
4.1. Surface Modification Using Anticoagulants
The development of materials with anticoagulant function has been actively pursued for many years. Incorporation of heparin, the most common anticoagulant used clinically, seemingly has been a central focus in the development of such material.
4.1.1. Heparin
Heparin is a natural polysaccharide of heterogeneous composition and has close structural and functional similarities to heparan sulfate. Similar to heparan sulfate, heparin binds to AT-III and causes a conformational change in the reactive center of AT-III to allow the inhibition of thrombin (Fig 1.7). To a lesser extent, heparin-AT-III complexes also can enable the inhibition of other coagulation factors including Factors XIa, Xa, and IXa[84]. The first report on biomaterial modification with heparin involved heparin modification to graphite, a material for mechanical heart valves[85]. This early report revealed that heparin modification could substantially reduce thrombus formation, both in vitro and in vivo. However, clinical success of heparinized implant surfaces has been rather limited, and several studies have debated the degree of in vivo improvement in blood compatibility when compared with several non-heparin-coated surfaces.
Variations in the strategy of heparin immobilization, in addition to differences in bulk material compositions, may result in different efficacy and clinical outcomes. Immobilization of heparin has been performed through ionic bonding, physical adsorption, bulk material incorporation, and covalent linkage. Ionic bonding of heparin can be accomplished by the adsorption of a cationic agent, such as benzalkonium chloride, which can then bind to anionic portions of heparin molecules. One study used the heparin benzalkonium chloride complex (HBAC) to treat acellular collagen vascular grafts derived from decellularized subintestinal mucosa. Thrombus formation on the HBAC-treated grafts after 90 days was significantly lowered when implanted as rabbit carotid artery interposition grafts[12]. Heparinized ePTFE vascular grafts with tridodecylmethylammonium chloride (TDMAC)-heparin coating had improved 1-month patency in a rat bypass model[86]. Heparin coating on ePTFE and polyurethane grafts also improved the patency of vascular grafts[87].
Stability of heparin coatings is much higher when a covalent grafting strategy is employed. Covalent grafting can be done through cross-linking reactions involving one of several functional groups such as hydroxyls, carboxyls,

11
or amines, which reside on the heparin chain. Maintaining the biological activity of heparin is a key concern, as the AT-III binding region should remain available. The use of a hydrophilic spacer such as poly(ethylene glycol) (PEG) has been shown to effectively enhance the AT-III binding activity of heparin[88, 89] and maintain the patency of vascular grafts for 3 months in a canine model[90]. This enhancement in activity when using a PEG spacer likely arises from a reduction in steric hindrance. Reduced protein adsorption and platelet adhesion to the material surfaces is an additional antithrombogenic effect of PEG (see Section 4). Another strategy to better preserve the bioactivity of bound heparin is to use end-point immobilization[91] [92]. During end-point immobilization, aldehyde groups are introduced at the reducing termini of heparin chains. Aldehyde groups then can be reacted with surface amines, thereby binding heparin through a single linkage that allows the chain to extend freely and interact with AT-III. Stents coated with polyamine and end-point-conjugated heparin were shown to prevent acute stent thrombosis [93, 94]. In addition, tri-block copolymers such as poly(dimethylsiloxane)(PDMS)–poly(ethylene oxide) (PEO)–heparin have been produced to incorporate heparin into polymer chains [95].
Clinical studies have shown that heparin-conjugated ePTFE grafts have 68% (above-knee) and 81% (below-knee) patency for peripheral bypass procedure at 2 years[96] and that heparin-bonded Dacron grafts have a 46% patency rate at 5 years[97]; these rates are improved over those of untreated grafts. Despite its widespread use to coat blood-contacting materials, heparin immobilization does have a few limitations, one of which is the inability of heparin to inhibit fibrin-bound thrombin. Heparin also relies on the local presence of AT-III to exert its activity. Additionally, heparin's ability to bind various bioactive molecules such as growth factors and matrix proteins could lead to other side effects[98-100]. There are also reports that heparin-coated stents could induce neointima formation due to inflammatory responses caused by heparin or polymer coating [101, 102].
4.1.2. Hirudin
Owing to the limitations of heparin, many groups have explored modifications using substances that inhibit thrombin or thrombin production directly. Among the available direct inhibitors of thrombin, hirudin is the most potent natural inhibitor. Hirudin is a small protein (only 65 amino acids) originally derived from the medicinal leech. Hirudin forms a tight bivalent complex with thrombin; this binding blocks both the active site and the fibrinogen binding exosite[103, 104]. Consequently, hirudin is capable of inhibiting soluble thrombin as well as fibrin-bound thrombin (Fig 1.7). Recombinant hirudin (r-hirudin) has been covalently attached to several materials for use in cardiovascular tissue engineering applications. Immobilized r-hirudin on the biodegradable polymer poly(d,l-lactide-co-glycolide) resulted in a significant reduction in thrombus formation in vitro[105]. Dacron patches modified with covalently linked r-hirudin showed an overall reduction in short-term thrombus formation after implantation

12
in canine aorta [106, 107]. However, direct conjugation of hirudin has resulted in significantly reduced bioactivity relative to soluble hirudin. This is especially the case when the primary attachment is done using the N terminus. Selective attachment using the ε-amino acids has been shown as an alternative to better preserve the bioactivity of conjugated hirudin[108]. Recently, our group has used PEG as a spacer to covalently link the C terminus of r-hirudin to a biodegradable microfibrous vascular graft prepared from electrospun poly(l-lactide) (PLLA). The PEG-treated and PEG-hirudin-treated grafts showed an overall reduction in adherent and activated platelets. In vivo performance of the PEG-hirudin-treated vascular graft also was improved, as there was a significant increase in patency at 6 months after implantation into rat carotid arteries [109]. Poly(lactic acid) also has been used to coat stents and release pegylated hirudin to reduce neointima formation[110]. An in vitro study showed that hirudin conjugated to paracyclophane-coated stents decreased thrombogenicity and platelet adhesion[111]. The effect of immobilized hirudin on late stent thrombosis remains to be investigated.
4.1.3. Other thrombin inhibitors
As alternatives to hirudin, several other direct thrombin inhibitors are available or in development[112, 113]. For example, aptamers with DNA sequences specific for thrombin binding may be used to inhibit thrombin activity[114, 115]. An advantage of this approach is the highly stable nature of aptamers. As with the immobilization of hirudin, attachment density and overall activity should remain key design criteria for immobilizing any alternative direct thrombin inhibitor. To be effective, direct thrombin inhibitors must be presented in amounts capable of inhibiting thrombin levels within the microenvironment. Determining this critical density may prove challenging and will likely depend on the specific cardiovascular application and location.
4.1.4. Thrombomodulin and Tissue Factor Pathway Inhibitor.
In addition, immobilized TM and TFPI have been explored as a method to limit thrombin production and further enhance the nonthrombogenic properties of tissue-engineered implants (Fig 1.7). A few studies have validated the in vitro effectiveness of immobilized TM in reducing thrombogenicity. Covalent attachment of recombinant TM has been shown to prolong plasma recalcification times and reduce thrombin-induced platelet aggregation on poly(ether urethane urea)[116]. Another in vitro study of surfaces dip-coated with lipid vesicles containing TM also demonstrated a reduction in thrombogenicity. Interestingly, a study showed an even greater reduction in thrombogenicity when heparin and TM were coimmobilized to the surface[117], demonstrating additive enhancements in antithrombogenic effect. To date, however, relatively little work has been done to study the in vivo effectiveness of immobilized TM in cardiovascular applications. One study showed that in vivo coagulation was prolonged when TM was conjugated to cellulose fibers and subsequently

13
implanted into canine vessels[118]. Another more recent study investigated the in vivo effectiveness of TM-modified ePTFE stent grafts in porcine carotid arteries[119]. Results demonstrated reduced early neointimal hyperplasia, an effect that the authors attribute to a reduction in thrombin-stimulated SMC proliferation[120]. Similarly, immobilization of TFPI on Dacron vascular grafts was shown to maintain patency for 3 months and reduce neointima thickness[121]. More studies are needed to determine how the modification of the surfaces with TM and TFPI influences long-term patency.
Figure 1.7: Modification of surfaces using anticoagulant. Immobilized heparin binds to antithrombin-III to facilitate thrombin inhibition. Direct thrombin inhibitors such as hirudin can be immobilized to circumvent the dependence of antithrombin-III for thrombin inhibition. Thrombomodulin and tissue factor pathway inhibitor (TFPI) are linked to surfaces to inhibit coagulation. Spacers, such as poly(ethylene glycol) (PEG) and others, can be used to decrease steric hindrance and increase activity of anticoagulant molecules.
4.2. SURFACE MODIFICATIONS TO PREVENT PLATELET ADHESION & ACTIVATION
Prevention of platelet adhesion and activation is critical for the production of nonthrombogenic implants. The use of material surface modifications to block such platelet responses has been an active area of cardiovascular bioengineering.
4.2.1. Nitric oxide
Under normal conditions, platelet adhesion to the vessel wall is a localized activity and EC-derived NO acts to inhibit platelet adhesion. NO also has been reported to help maintain the nonproliferative phenotype of vascular SMCs, thus

14
limiting intimal hyperplasia. Biomaterials that mimic this mechanism by incorporating NO donor groups can be used to limit platelet adhesion and thrombus formation on the surfaces of cardiovascular implants (Fig 1.8). Numerous NO-donor-containing compounds have been identified and can be selected according to their release rate, mechanism of NO liberation, and toxicity[122-124]. Incorporation of these compounds into polymeric materials also can be achieved using various techniques including blending, covalent grafting to pendant groups, and synthesis into the polymer backbone.
Diazeniumdiolates are one particular class of NO donor compounds that are formed through the complexation of NO and nucleophilic amines. Diazeniumdiolates can decompose in solutions at physiological pH to release NO[123, 125]. Polyurethanes can be synthesized to include diazeniumdiolate segments and are capable of sustained NO production and the accompanied reduction of platelet adhesion up to 2 months[126]. Coatings containing similar NO donor groups have successfully reduced in vivo platelet adhesion on ePTFE vascular grafts[125]. In addition to limiting platelet adhesion, NO-producing polyurethanes also have been shown to limit SMC proliferation, which contributes to neointimal hyperplasia. NO-releasing polyurethane also seemingly promotes EC migration and proliferation, which could also contribute to long-term patency[126].
4.2.2. Poly(ethylene glycol)
The adsorption of serum proteins is the initial response upon contact between blood and the material surface. Protein adsorption is likely a driving force in platelet adhesion and thrombus formation on tissue-engineered surfaces. The creation of material surfaces that resist protein adsorption is a potential strategy to reduce platelet adhesion to tissue-engineered cardiovascular implants. The hydrophilic polymer PEG (or PEO) was first identified for its unique ability to resist protein adsorption[127-129]. PEG/PEO surface coatings have been widely used to create “nonfouling” materials, which resist protein adhesion (Fig 1.8). PEG/PEO layers can be developed using various techniques, such as passive adsorption, covalent grafting, and bulk modification. Using in vitro and in vivo studies, several groups have proved the effectiveness of PEG/PEO layers in significantly reducing platelet adhesion to cardiovascular materials such as Nitinol stents, ePTFE, Dacron, and polyurethane heart valves[88, 130-132]. However, most in vivo studies of PEG/PEO-modified implants have been unsuccessful in proving a significant improvement in limiting thrombus formation[88, 133, 134]. One explanation is that the PEG/PEO layer may be modified by plasma proteins; alternatively, PEG/PEO layers limit only individual platelet adhesion but may not resist the adhesion from platelet aggregates that might form in blood away from the material surface[88]. Nevertheless, PEG/PEO can be used as a molecular linker/spacer for antithrombogenic molecules such as heparin and hirudin.

15
4.2.3. Glycosaminoglycans
Because GAGs on an EC surface can resist platelet adhesion, several groups have explored the use of GAG molecules to modify the surfaces of cardiovascular devices (Fig 1.8). To prevent platelet adhesion, photocurable chondroitin sulfate and HA are used for the luminal surface coating of vascular grafts[135]. HA conjugated to the polyethylenimine branch on a copolymerized polyurethane backbone was shown to be more effective than either PEG-grafted or heparin-grafted surfaces with respect to limiting protein adsorption and platelet adhesion. Interestingly, confluent, morphologically healthy cultures of ECs were achieved on surfaces grafted with only low-molecular-weight HA but not high-molecular-weight HA[136]. Because GAG coating provides a low adhesion layer mimicking the EC surface, further studies are needed to verify the biological function in vivo.
4.2.4. Phosphorylcholine
Phosphorylcholine (PC) is a phospholipid found in the cell membrane. To mimic the property of PC in resisting protein adsorption and platelet adhesion, PC is immobilized on the surface of biomaterials by cross-linking, polymerization, and peptide bonding[137-139] (Fig 1.8). Although there is evidence that PC coating on ePTFE grafts and stents reduces neointima formation in vivo[137, 140-142], there are also conflicting results showing that PC coating has no effect[143]. Nevertheless, PC coating exhibits biocompatibility and stability in vivo [139, 144, 145] and could be used for local drug delivery.
4.2.5. Albumin.
Albumin has been associated with significantly lower platelet adhesion when compared with other plasma proteins. For this reason, some have used covalently coupled albumin as an attempt to reduce thrombogenicity of cardiovascular implants (Fig 1.8). Although in vitro studies showed a significant reduction in platelet adhesion with albumin coating, clinical outcomes have not been able to establish a clear advantage when albumin-coated grafts were implanted [134].

16
Figure 1.8: Modifications of surfaces to prevent platelet adhesion and activation. Nitric oxide (NO) donors can be incorporated into materials to prevent platelet adhesion and activation for extended durations. PEG, glycosaminoglycans (GAGs), phosphorylcholine (PC), and albumin can be used to decrease protein deposition and platelet adhesion. APC, activated protein C.
5. ANTITHROMBOGENIC APPROACHES USING ENDOTHELIAL CELLS AND STEM CELLS 5.1. In Vitro Endothelialization
The native endothelium is inherently nonthrombogenic and plays a pivotal role in mediating thrombosis. Therefore, it is widely accepted that ideal tissue-engineered cardiovascular implants must contain a confluent, mature, and healthy endothelium. Complete endothelial coverage is necessary for nonthrombogenicity because platelet thrombus formation is extremely sensitive to exposed surfaces. TEVGs can be fabricated through the use of collagen matrix, synthetic matrix, and cell sheets[146-148]. To maintain the patency of the grafts, an EC monolayer on the luminal surface of the grafts is required. A clinically relevant issue is the source of ECs. Because ECs are generally immunogenic, an autologous EC source is desirable. For example, ECs can be isolated from progenitors in circulating blood and bone marrow, or isolated from soft tissues such as adipose tissue.
In addition to large vessels, endothelialization of microvessels is essential to prevent thrombus formation and clogging when vascularized tissue and organs are implanted. A recent exciting approach to the construction of complicated tissue and organ structure is to decellularize harvested tissues and organs and then to repopulate functional cells into the decellularized matrix. To prevent the clogging of the vascular network, ECs were perfused into the vascular network to

17
cover the luminal surface of large vessels and microvessels. This approach is promising, as shown in a few recent publications on the reconstruction and short-term in vivo function of heart, liver, and lung[33-36]. However, to keep these organs functioning for longer time periods, further optimization is needed to keep the vascular network unclogged.
For engineered tissues, capillary network can form in the 3D microenvironment via the coculture of ECs and fibroblasts or mesenchymal cells. Although this capillary network is not functional and mature in vitro, it accelerates the formation of functional anastomosis with host vasculature upon the implantation of the engineered tissues [37]. If desired, the structure and distribution of the capillary network can be designed and constructed by using the microfabrication technique and 3D printing method [30-32].
Early attempts to tissue-engineer synthetic cardiovascular implants involved seeding the implants with autologous ECs. In most cases, EC retention under in vivo flow conditions has been relatively low and has led to poor outcomes. In the case of some ePTFE grafts, the majority of seeded ECs are lost within 24 h after exposure to physiological shear stress[149]. Long-term outcomes have varied in success depending on the type of seeding protocol used as well as the synthetic material used. In the case of EC-seeded ePTFE grafts for femoropopliteal bypass, patency after 30 months remained significantly less when compared with that of vein grafts[150]. To enhance EC retention on the surface of vascular grafts under flow conditions, researchers have explored preconditioning ECs with fluid shear stress. In response to shear stress, ECs are able to adapt in that their cytoskeletons, focal adhesions, and underlying extracellular matrices (ECMs) are reorganized and strengthened [151, 152]. Vascular grafts can be connected with a circulation system in vitro, and shear stress is ramped up gradually to induce the remodeling of an EC monolayer and thus to increase cell adhesion strength[153-155].
Some recent attempts to produce nonthrombogenic cardiovascular implants using EC seeding have aimed to promote stronger and more specific EC adhesions. Incorporation of adhesion peptides derived from ECM molecules has been explored as a potential strategy to increase EC retention on tissue-engineered cardiovascular surfaces. Studies utilizing the RGD peptide sequence immobilized on ePTFE grafts have been able to increase the level of EC attachment and retention under flow significantly. In most cases, nonetheless, RGD-coated grafts still have been unsuccessful in achieving and maintaining confluent EC coverage[149, 153].Additionally, RGD is a fibronectin-derived peptide recognized by platelets and ECs with similar affinitySuch affinity for platelet recognition could potentiate thrombus formation if ECs are detached. Alternatively, the laminin-derived YIGSR peptide is more specific for EC adhesion. Studies of polyurethane grafts containing YIGSR and PEG exhibited increased EC adhesiveness while showing minimal signs of platelet adhesion[156]. Other sequences including the REDV peptide [157, 158] and

18
other designer sequences identified through phage display also may be candidates for increasing the specificity of EC adhesion. However, platelet activation and thrombus formation is an extremely robust and self-reinforcing mechanism, and even low levels of platelet adhesion can contribute to platelet activation. Consequently, surfaces that display even a minimal level of platelet recognition may still be prothrombogenic. The copresentation of cell-adhesive domains along with molecules such as NO donors that actively decrease platelet activity may represent a promising strategy for increasing EC adhesion while simultaneously preventing platelet activation[159].
5.2. In Situ Endothelialization
EC seeding of vascular constructs requires vessel biopsies followed by long harvesting periods. In situ self-endothelialization of vascular implants is an approach that could circumvent the need for autologous cell harvesting. In the case of synthetic vascular grafts and stents in humans, complete endothelial coverage is never attained solely from transanastomotic migration[160]. Achieving in situ endothelialization undoubtedly will require a stimulus capable of increasing EC recruitment from more than one source. In addition to transanastomotic EC migration, other potential sources for in situ endothelialization include transmural migration via capillary ingrowth and the recruitment of endothelial progenitors (EPCs) present in circulation.
It has been shown that directional EC migration can be controlled by micropatterned parallel matrix strips [161]. To increase transanastomotic EC migration, micro- and nanotopography of the luminal surface of vascular grafts can be engineered. For example, longitudinal aligned nanofibers on the luminal surface of vascular grafts can be made by electrospinning, which promotes EC migration and endothelialization in vitro and in vivo (R. Janairo & S. Li, unpublished observation). Microgrooves also can be used to limit SMC proliferation and enhance EC organization and migration[162, 163]. Other microfeatures such as micropores on a Nitinol surface also have been shown to promote endothelialization in vitro[164].
Homing of EPCs represents a possible strategy for promoting in situ self-endothelialization of cardiovascular constructs. EPCs are bone-marrow-derived mononuclear cells that are found in circulating blood. The concentration of circulating EPCs is generally very low; however, treatment with several chemical factors—such as granulocyte colony-stimulating factor (G-CSF) [165], SDF-1[166, 167],VEGF[168, 169], MMP-9[170], and statin [171]—may be able to increase circulating EPC concentrations and/or differentiation into mature ECs. Future studies that elucidate the exact underlying mechanisms of chemical factors and EPC mobilization will be critical.
Presentation of homing molecules on the implant surface that recognize EPC-specific markers and selectively capture these cells is another potential strategy

19
to increase in situ endothelialization. EPCs are characterized by the expression of several surface markers, such as CD34, CD133, and vascular endothelial growth factor rector-2 (VEGFR-2). Upon entry into circulation from bone marrow, EPCs begin to lose the expression of CD133 but are positive for CD34 and VEGFR-2. Grafts coated with monoclonal antibodies to recognize these early EPC expression markers have been explored as a means to capture EPCs. Reports of vascular grafts coated with a monoclonal antibody against CD34 demonstrated that nearly complete endothelialization could be achieved within 3 days. However, it was also noted that graft intimal hyperplasia was significantly increased in parallel, leading to occlusion and failure[172]. Several theories have been used to explain the increase in intimal hyperplasia that is associated with grafts and stents coated with antibodies against CD34. One explanation is that some populations of CD34+ cells have the capability to differentiate into vascular SMCs and other proinflammatory cells[173, 174], which thus would account for the increased intimal hyperplasia. In fact, one study suggests that less than 1% of the total circulating CD34+ progenitors are actually EPCs (as defined by the coexpression of CD133, CD34, and VEGFR-2) [174]. Nonetheless, for EPC capture technology to be successful for vascular tissue engineering applications, further development of highly specific capture molecules is needed. Aptamers, which are short oligonucleotides capable of target recognition, have been suggested as a possible alternative for capturing EPCs[175]. Researchers also will require a better understanding of the commitment and identity of attracted progenitor populations in vivo. It is also worth noting that the cell sources of ECs found in vascular grafts are controversial.
5.3. Nonthrombogenic Surfaces Seeded with Bone Marrow Mesenchymal Stem Cells
Traditionally, ECs are considered to be the only possible cell type with hemocompatibility and antithrombogenic property. EPCs are a potential source for obtaining autologous ECs. Upon EPC differentiation and their maturation into ECs, these cells can be used to coat surfaces and form vascular network. In addition to the isolation of ECs from adult vascular tissues, ECs can be derived from pluripotent stem cells such as induced pluripotent stem cells and embryonic stem cells. The cell-reprogramming technology makes it possible to convert somatic cells into induced pluripotent stem cells and thus ECs for autologous transplantation.
Recently, mesenchymal stem cells (MSCs) derived from bone marrow have been used to construct vascular grafts[71, 176]. Bone marrow MSCs are derived from the stromal cells in bone marrow, are compatible with blood cells including platelets, have low immunogenic properties, and can differentiate into SMCs (see[177] for a review); these traits make MSCs an ideal cell source to construct the mesenchymal layer of TEVGs. Interestingly, MSCs exhibit similar hemocompatibility and antiplatelet properties as ECs. For example, MSCs resist platelet adhesion, which requires HSPGs on the cell surface[71]. Although MSCs

20
cannot differentiate into ECs and do not express some EC genes such as NO synthase, whether MSCs express other antithrombogenic EC genes awaits further investigation. In addition, MSCs could stabilize the blood vessels as pericytes and secrete soluble factors for EC recruitment. MSCs likely can be an alternative cell source to ECs for some of the cardiovascular tissue engineering applications.
6. SUMMARY POINTS AND FUTURE ISSUES 1. Nonthrombogenic modifications are necessary for cardiovascular devices
and engineered tissues such as vascular grafts, stents, heart valves, and vascularized tissues and organs.
2. Several strategies and biomolecules have been used for nonthrombogenic biochemical modifications: anticoagulation, prevention of platelet adhesion and activation, and fibrinolytic modification.
3. The EC can inhibit coagulation, prevent platelet adhesion and activation, and induce fibrinolysis, and it is an ideal cell type for nonthrombogenic modifications; other cell types such as bone marrow MSCs are also compatible with blood cells and can resist platelet adhesion.
4. ECs can be used to cover cardiovascular devices, tissue-engineered biological equivalents, and microvessels in vascularized tissues and organs to form nonthrombogenic monolayer.
5. Strategies to promote in situ endothelialization include engineering the micro- or nanotopography of surfaces to promote transanastomotic cell migration and immobilizing biomolecules to recruit circulating ECs and EPCs.
FUTURE ISSUES 1. There is significant difference between the in vitro and in vivo
environments; the cross-talk between thrombogenesis and inflammatory responses and the effect of new therapeutic approaches need further investigation.
2. To address the multifaceted and self-enforcing characteristics of platelet activation and coagulation cascade, the combination of surface modifications should be explored to produce a nonthrombogenic surface.
3. Understanding the molecular structure and the interaction of biomolecules with the surface and targets is necessary to facilitate the rational design of more effective surface modification.
4. Research is needed to explore the use of micro- and nanomaterials and stem cells to promote in situ endothelialization.
5. To obtain sufficient quantities of nonthrombogenic cells (e.g., ECs, MSCs) from human tissues, the protocols for autologous cell isolation and expansion should be developed; alternatively, nonthrombogenic cells may be reprogrammed from other autologous cells.

21
Chapter 2 Development and Characterization of Electrospun Vascular Grafts with VEGF for In Situ Vascular Tissue Engineering

22
1. INTRODUCTION
Cardiovascular disease remains the leading cause of mortality in many countries. The replacement of diseased blood vessels is a common treatment with more than 500,000 vascular graft surgeries performed in the U.S. each year. Still, more than 30% of patients needing arterial replacement lack a suitable autologous vein graft for surgery[178]. Synthetic grafts are available but are prone to clogging by thrombosis and cannot be used for the replacement of small diameter vessels (<6 mm inner diameter) [179, 180]. Thus, there has been a large need to develop small-diameter tissue engineered vascular grafts for arterial replacement. Several cellular approaches utilizing in-vitro tissue engineering have been reported and explored for the development of arterial replacements [181-184]. In vitro cellular approaches hold much promise; however, their extensive cultivation periods and current necessity for autologous cell sources could be prohibitive toward widespread implementation. In situ tissue engineering represents an alternative approach, whereby a temporary scaffold without cells is implanted and provides stimulatory cues to guide the remodeling of a functional vascular graft within the host. To be successful, the development of biomaterials that mimic natural features of the extracellular matrix (ECM) and provide appropriate biochemical cues for vascular tissue formation is necessary.
Since endothelial Cells (ECs) are potent inhibitors of thrombosis, it is widely accepted that an ideal tissue engineered artery requires a functional and confluent endothelium to prevent failure. Therefore, stimulatory cues to guide endothelium formation are critical for in situ vascular tissue engineering. Additionally, scaffolds for in-situ vascular tissue engineering should support cellularization and natural matrix deposition. Cellularization and matrix deposition within electrospun materials has often been limited due to the relatively small pore sizes between fibers. Heparin coating has been shown to enhance the cellular infiltration within electrospun materials during dermal wound healing [185]. However, it is unclear whether heparin can influence cellular infiltration of electrospun materials in other applications. Additionally, vascular endothelial growth factor (VEGF), which has heparin binding ability, is a potent mitogen for ECs. Together, heparin and VEGF could act to simultaneously suppress thrombosis and stimulate endothelialization, vascular cellularization and matrix synthesis.
Electrospun fibrous scaffolds are a promising platform for in-situ vascular tissue engineering due to their structure similarity to native ECM and potential to guide cellular processes [186]. Aliphatic polyesters like poly(lactide) (PLA), poly(glycolic acid) (PGA) and poly(caprolactone) (PCL) are bioresorbable and can be electrospun into nano/micro-fibrous materials that serve as temporary matrices for in situ tissue morphogenesis. However, PLA, PGA, PCL and the copolymers thereof, all lack modifiable functional groups along their backbone and thus, have limited capacity for biomolecule coupling. Functionality can be

23
substantially increased through copolymerization with other monomers that contain modifiable groups (e.g. poly(lysine))[187]. However, copolymerization methods can often be expensive and labor intensive. Here, we present a simple and effective method to increase the density of chemically modifiable end groups within a bioresorbable fibrous scaffold by blending similar high and low molecular weight polymers prior to electrospinning. The blending method is simple yet versatile and can be used in numerous applications where a higher capacity for stable biomolecule attachment is needed.
In this study, we use the method to increase the binding and stability of conjugated heparin and VEGF on electrospun fibrous scaffolds for in situ vascular tissue engineering. This chapter will present the methods used for graft fabrication, as well as the characterization of several physical and chemical properties.
2. MATERIALS & METHODS
2.1 Fabrication of Electrospun Scaffolds
Electrospun scaffolds were fabricated from the biodegradable polymers poly(L-Lactide) (PLLA), and poly(caprolactone) (PCL). To increase the number of end groups available for biomolecule attachment, low molecular weight PCL (LMW-PCL; MW= 2,000 kDa) (Polysciences, Warrington, PA) or low molecular weight PLLA (LMW-PLLA; MW = 2,000) (Polysciences, Warrington, PA) was blended with a high molecular weight PLLA (HMW-PLLA; MW=100,000) (Lactel Absorbable Polymers, Pelham, AL). Four polymer solutions were prepared with final concentrations of 19% (w/v) HMW-PLLA (PLLA), 19%(w/v) HMW-PLLA/5% (w/v) LMW-PLLA (PLLA/5%PLLA), 19% (w/v) HMW-PLLA/5%(w/v) LMW-PCL (PLLA/5%PCL), and 19%(w/v) HMW-PLLA/10% LMW-PCL (PLLA/10%PCL) (See Table 2.1)
Poly(L-Lactide) MW= 100,000 (w/v)
Poly(L-Lactide) MW = 2000 (w/v)
Poly(caprolactone) MW = 2000 (w/v)
1) PLLA 19% ----- -----
2) PLLA/5%PLLA 19% 5%
3) PLLA/5%PCL 19% ----- 5%
4) PLLA/10%PCL 19% ----- 10%
Table 2.1: Summary of polymer blend compositions

24
All polymers were dissolved in 1,1,1,3,3-hexafluoro-2-propanol (HFIP) via sonication for 45 minutes or until fully dissolved. Electrospinning was performed to make membrane scaffolds for the in vitro testing as previously described [186]. Polymer solutions were delivered at a flow rate of 1ml/hr using a programmable syringe pump (Cole-Parmer, Vernon Hills, IL). A positive voltage of 12.5 kV was applied to a spinneret using a high voltage generator (Gamma High Voltage, Ormond Beach, FL). Fibers were collected on a rotating (speed =200 rpm) stainless steel drum (diameter = 10 cm). Electrospinning continued until the scaffold thickness reached 150 µm. Scaffolds were then removed from the drum and placed into a vacuum desiccator for 24 hours to remove any residual HFIP. Scaffolds were cut into rectangular sections and fiber quality and dimensions were inspected using a Hitachi TM-1000 scanning electron microscope.
2.2 Fabrication of Tubular Scaffolds for Vascular Graft Implantation
Tubular grafts were fabricated by using electrospinning similarly as described above with minor modifications[188]. Fibers were collected onto a rotating stainless steel mandrel (diameter = 1 mm) (speed = 20 rpm, same linear speed as rotating drum). Electrospinning was performed until the graft wall thickness reached 150 µm. Grafts were then removed from the mandrel and placed into a vacuum desiccator for 24 hours to remove any residual HFIP.
2.3 Mechanical Characterization of Electrospun Scaffolds
Fibrous scaffolds were cut into 1 cm x 4 cm rectangular segments and subjected to uniaxial tensile testing by using an Instron machine (Model 5544, Instron, Norwood, MA). All Scaffolds (n=6 for all groups) were stretched by using a strain rate of 0.1 mm/s until fracture or a strain of 75 percent (whichever was first). Force/displacement data was recorded using a sampling rate of 1 Hz. Elastic Modulus, ultimate tensile strength (UTS) and strain at failure were computed for each of the scaffold groups. Results from mechanical characterization were compared to previously reported values of ePTFE and native arteries. Ultimately, this comparison was used to identify an appropriate electrospun scaffold for vascular graft implantation during animal studies.
2.4 Heparin Modification of Electrospun Scaffolds
Covalent attachment of heparin was performed as described previously [188]by using 1-ethyl-3-(3 dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxysulfosuccinimide (sulfo-NHS) (Pierce Biotechnology, Rockford, IL) as crosslinkers and di-amino-poly(ethylene glycol) (di-NH2-PEG) (Sigma Aldrich, St Louis, MO) as a spacer. The density of surface carboxyl groups was increased by briefly hydrolyzing the material in sodium hydroxide

25
(NaOH, 0.01N) for 10 minutes. Scaffolds were rinsed thoroughly in phosphate buffered saline (PBS), followed by rinsing using deionized water. Scaffolds were then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10mg/ml sulfo-NHS and 20 mg/ml di-NH2-PEG at room temperature. Scaffolds were rinsed in PBS and then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10 mg/ml sulfo-NHS and 20 mg/ml unfractionated heparin sodium salt (Sigma Aldrich, St. Louis, MO). Following heparin modification, scaffolds were thoroughly washed in PBS and remaining reactive sites were quenched using 10 mg/ml glycine in PBS for 30 minutes.
The presence of heparin on fibrous scaffolds was verified and measured by using toluidine blue (Sigma Aldrich, St. Louis, MO) as described previously [189]. Briefly, untreated, PEGylated, and heparin-modified electrospun scaffolds were placed in 0.0005% w/v Toluidine Blue solution and vortexed for 10 minutes. Standard heparin solutions ranging from 0 µg/ml to 250 µg/ml were also prepared in 0.0005% (w/v) toluidine blue solution and vortexed for 10 minutes. After vortexing, 3 ml of n-hexane was added to all samples and standard heparin solutions to extract the remaining unbound toluidine blue. To determine the concentration of remaining toluidine blue, the absorbance was measured at 631nm by using a spectrophotometer (BioRad, Model 550). The concentration of immobilized heparin on each piece of scaffold was thus determined by comparing their absorbance values of unbound toluidine blue to those obtained from the standard heparin solutions.
2.5 Antithrombogenic Activity of Heparin-Modified Scaffolds The antithrombogenic activity of heparin-modified grafts was determined
by measuring the level of thrombin inhibition in the presence of antithrombin-III. As described previously [190],, the chromogenic substrate for thrombin, S-2238 (Diapharma, West Chester, OH), was used to detect thrombin activity. Briefly, untreated, PEGylated and heparin-modified grafts were placed in a 50 mM Tris buffer containing 0.08 NIH units of human antithrombin-III (Sigma Aldrich, St. Louis, MO), and shaken for 5 minutes at 37°C. Standard solutions containing 0 to 400 units of heparin were similarly prepared in Tris buffer and 0.08 NIH units of human antithrombin-III. Afterwards, 0.08 NIH units of human thrombin (Sigma Aldrich, St. Louis, MO) were added to each sample and standard solution, and shaken for 30 seconds at 37°C. Subsequently, 5 mM S-2238 was added, and samples were incubated with shaking for 10 minutes at 37° C. All reactions were stopped by the addition of 40% acetic acid. Remaining thrombin activity was quantified by measuring the absorbance of the sample supernatants and standard solutions at 405nm (BioRad, Model 550). The heparin activity for all samples was determined by comparing to those obtained for the standard heparin solution 2.6 VEGF Immobilization
Many isoforms of VEGF have high affinity with heparin molecules naturally found in the ECM. For this reason, heparin was used as an adaptor molecule to

26
immobilize VEGF to PLLA and PLLA/5%PCL scaffolds. Following heparin modification, scaffolds were incubated in PBS solutions containing 0,1, 2 and 4 µg/ml human recombinant VEGF-165 (Peprotech Inc., Rocky Hill, NJ) on a shaker for 16 hours at 4°C. PLLA scaffolds without heparin modification were subjected to the similar VEGF treatment and used for comparison purposes during characterization of VEGF immobilization and release. After VEGF attachment, scaffolds were rinsed repeatedly in PBS for 30 minutes.
2.7 Characterization of VEGF Immobilization and Release
Immunofluorescent staining was performed to confirm VEGF attachment and visualize its distribution. In brief, the scaffolds with and without VEGF were incubated in 10% goat serum (Sigma Aldrich, St. Louis, MO) for 1 hour, with the rabbit antibody against VEGF for 2 hours and with Alexa Fluor 488 conjugated goat anti-rabbit IgG (Invitrogen) for 30 minutes. The density of immobilized VEGF was also quantified directly using an enzyme-linked immunosobent assay (ELISA) (Peprotech Inc., Rocky Hill, NJ). Prior to ELISA analysis, rectangular scaffold segments (1 cm x 0.5 cm each) were completely digested by using sodium hydroxide (0.1 N, 24h), followed by immediate pH neutralization using hydrochloric acid (0.1 N). The amount of immobilized VEGF was quantified by ELISA in comparison to the ELISA measurements of standard VEGF solutions containing 0-1 ng/ml VEGF in PBS. An additional set of VEGF standards containing non-treated graft segments was prepared in sodium hydroxide (0.1 N, 24h) and neutralized with hydrochloric acid (0.1 N). Base/acid treatment and the presence of digested graft material did not affect the accuracy of VEGF measurement by ELISA (data not shown).
For VEGF release studies, VEGF was immobilized to scaffolds by using 1.0 µg/ml VEGF in PBS. The incubation media for each scaffold was 2 ml of PBS, which was removed and replenished every 24 hours. Scaffolds were shaken moderately and kept at 37°C during the study. At various intervals, scaffolds were digested and the amount of immobilized VEGF remaining was measured by using ELISA.
2.8 Statistical Analysis The data was presented as mean ± standard deviation. All data were analyzed with one-way ANOVA tests. Holm’s t test was performed to evaluate significant differences between pairs. A p-value of less than 0.05 was considered statistically significant.
3. RESULTS
3.1 Fabrication of Blended Electrospun Scaffolds
Electrospun fibrous scaffolds were successfully fabricated by using each of the chosen polymer compositions: PLLA, PLLA/5%PLLA, PLLA/5%PCL, and

27
PLLA/10%PCL (Fig. 2.1 A-D). For all polymer groups, uniform fiber formation without beading was achieved using identical electrospinning parameters (i.e. voltage, flow rate and needle-to-collector distance). Fiber diameters were 866 ± 150 nm, 961 ± 265 nm, 926 ± 215 nm, and 982 ± 175 nm for PLLA, PLLA/5%PLLA, PLLA/5%PCL and PLLA/10%PCL scaffolds respectively. Fiber diameters for all groups had a similar distribution with an approximate range of 500 nm to 1.5 µm.
3.2 Mechanical Properties of Blended Electrospun Scaffolds
Uniaxial tensile testing of electrospun scaffolds was performed to investigate how the incorporation of a low molecular weight polymer would affect the bulk mechanical properties such as elastic modulus, UTS, and strain at failure (Fig 2.1 F). The elastic modulus of the electrospun scaffolds was 170 ± 7.6 MPa, 180 ± 10.1MPa, 68 ± 8.7 MPa, and 33 ± 7.0 MPa for PLLA, PLLA/5%PLLA, PLLA/5%PCL and PLLA/10%PCL polymer compositions respectively. There was no difference between the modulus of PLLA and PLLA/5%PLLA scaffolds, suggesting that the addition of 5% LMW-PLLA into the polymer blend had no significant effect on elastic modulus. The addition of LMW-PCL resulted in a significant decrease in elastic modulus. Reduction in elastic modulus was more evident when the amount of blended LMW-PCL was increased from 5% (w/v) to 10%(w/v) (p<0.001). From physical examination, grafts became more flexible and kink-resistant with the addition of LMW-PCL.
The UTS was 3.7 ± 0.2 MPa, 3.8 ± 0.3 MPa, 1.8 ± 0.1 MPa, and 1.0 ± 0.1 MPa for PLLA, PLLA/5%PLLA, PLLA/5%PCL and PLLA/10%PCL polymer compositions respectively. There was no difference in UTS between PLLA and PLLA/5%PLLA scaffolds. However, addition of 5% (w/v) LMW-PCL reduced UTS by nearly 50% relative to PLLA. When the concentration of LMW-PCL was increased to 10% (w/v), UTS decreased by approximately 75%.
PLLA scaffolds had a strain-at-failure of approximately 40% elongation. Addition of LMW-PLLA significantly reduced strain-at-failure, and the abrupt fracture of PLLA/5%PLLA scaffolds occurred at less than 10% elongation. Since abrupt fracture at low levels of strain is highly undesirable for a vascular graft design, PLLA/5%PLLA scaffolds were excluded from the remaining experiments. The addition of LMW-PCL increased strain-to-failure of PLLA/5%PCL and PLLA/10%PCL to more than 75% elongation.
PLLA/5%PCL scaffolds had an elastic modulus similar to expanded polytetrafluoroethylene (ePTFE) and a UTS in the range of native arteries (Fig. 2.1 G). Thus, PLLA/5%PCL was chosen for the fabrication of tubular grafts for vascular implantation (Fig. 2.1 E). It is also worth mentioning, that since PLLA/10%PCL had a UTS similar to the lower limit of that found in native arteries, as a factor of safety, PLLA/5%PCL was used instead.

28
Figure 2.1 Structural and mechanical properties of electrospun materials. (A-D) Scanning electron microscopic (SEM) images of the electrospun scaffolds with PLLA (A), PLLA/5%PLLA (B), PLLA/5%PCL (C), PLLA/10%PCL (D). (E) Representative SEM image of an electrospun vascular graft with PLLA/5%PCL. (F) Stress-strain curves of electrospun scaffolds. (G) Mechanical properties of the electrospun scaffolds. The scale bar indicates 30 µm (A through D), and 300 µm (E). *Properties for ePTFE [191] and native carotid artery [192] taken from previous literature.

29
3.3 Heparin Immobilization
To investigate the effect of low molecular weight polymer addition on biomolecule coupling capacity, we measured the density of immobilized heparin in PLLA, PLLA/5%PCL and PLLA/10%PCL scaffolds (Fig. 2.2 A). The amount of immobilized heparin in PLLA, PLLA/5%PCL and PLLA/10%PCL scaffolds was 8.4, 22.2 and 57.7 µg/cm3 respectively. Thus, a significant increase in immobilized heparin density could be achieved when LMW-PCL was blended into the polymer solution prior to electrospining. The density of heparin immobilization continued to increase as the concentration of LMW-PCL was increased from 5% (w/v) (PLLA/5%PCL) to 10% (w/v) (PLLA/10%PCL).
3.4 Antithrombogenic Activity of Immobilized Heparin
The thrombin binding activity of immobilized heparin was assessed for PLLA, PLLA/5%PCL, and PLLA/10%PCL scaffolds (Fig. 2.2 B). The activity of immobilized heparin on PLLA, PLLA/5%PCL and PLLA/10%PCL scaffolds was 27.3, 69.6, and 112.6 NIH Units/cm3 respectively. No significant difference in activity was found among any of the non-heparin-modified scaffolds (data not shown). This result confirmed that immobilized heparin retained anti-thombogenic activity. PLLA/5%PCL and PLLA/10%PCL scaffolds exhibited an increase in anti-thrombogenic activity, which was consistent with the increase in heparin density in these scaffolds.

30
Figure 2.2: Characterization of immobilized heparin on materials. (A) Density of immobilized heparin in electrospun scaffolds with PLLA, PLLA/5%PCL and PLLA/10%PCL. (B) Anticoagulant activity of immobilized heparin in the electrospun scaffolds with PLLA, PLLA/5%PCL and PLLA/10%PCL.
3.5 VEGF Immobilization and Release
VEGF was immobilized to non-heparin-modified PLLA (PLLA), heparin-modified PLLA (PLLA-Heparin) and heparin-modified PLLA/5%PCL (PLLA/5%PCL-Heparin) scaffolds. Heparin specific immobilization of VEGF to electrospun scaffolds was confirmed by immunostaining, as exemplified in Fig. 2.3 A.
We also determined the density of immobilized VEGF in PLLA, PLLA-Heparin and PLLA/5%PCL-Heparin scaffolds as a function of initial VEGF loading concentration (Fig. 2.3 B). The density of immobilized VEGF was significantly greater on PLLA/5%PCL-Heparin scaffolds than PLLA-Heparin scaffolds for all loading concentrations of VEGF (p<0.05). The amount of immobilized VEGF was significantly greater on both heparin-modified scaffolds

31
than on untreated PLLA scaffolds at all loading concentrations. The amount of VEGF on untreated PLLA and PLLA/5%PCL scaffolds was similar, thus only untreated PLLA is shown.
Release of VEGF from PLLA, PLLA-Heparin and PLLA/5%PCL-Heparin was measured over a time period of 7 days (Fig. 2.3 C). Approximately 83% of the immobilized VEGF was lost from untreated PLLA scaffolds after 1 day. Heparin modification of PLLA reduced the initial burst release of VEGF to 60% after 1 day. The burst release of VEGF from PLLA/5%PCL-Heparin scaffolds, which contained approximately 3-times more bound heparin, was further reduced to approximately 40% of the initial concentration. After 7 days, all VEGF had been released from untreated PLLA scaffolds, while PLLA-Heparin scaffolds retained approximately 15% of the initially bound VEGF. Retention of VEGF on PLLA/5%PCL scaffolds was significantly greater after 7 days, with nearly 50% of the initially bound VEGF still remaining. Release of VEGF from untreated PLLA and PLLA/5%PCLL was similar at all time points, thus only release information for PLLA is shown.

32
Figure 2.3. VEGF immobilization and release from electrospun scaffolds. (A) Immunostaining of bound VEGF on heparin modified electrospun fibers. (B) Density of immobilized VEGF vs input VEGF concentration for the electrospun scaffolds with untreated PLLA, heparin-modified PLLA and heparin modified PLLA/5%PCL. (C) Release of VEGF over 7 days from the electrospun scaffolds with untreated PLLA, heparin-modified PLLA and heparin-modified PLLA/5%PCL. Results for untreated PLLA and PLLA/5%PCL were similar, and thus only untreated PLLA is shown.

33
4. DISCUSSION
Our objective was to create bioactive vascular grafts using electrosnpun fibers with the capability to accelerate endothelializaton and direct vascular cellularization in situ. In this study, we also established a method to significantly increase the surface conjugation capacity of an electrospun biodegradable polymer, HMW-PLLA, by blending with a low molecular weight polymer prior to electrospinning. Covalent attachment of biomolecules to PLLA or PCL is accomplished by conjugation to end groups. The addition of LMW-PCL increases the density of available end groups and results in the increased heparin conjugation capacity observed in this study. Also, the morphology of electrospun HMW-PLLA fibers was not affected by the addition of LMW-PCL or LMW-PLLA. In this study, we also found that the addition of either low molecular weight polymer (LMW-PCL or LMW-PLLA) did not affect the ability of blended polymers to form fibers under identical electrospinning conditions, which makes this technique simple and versatile. After, investigating the mechanical and chemical properties of 3 different polymer blends, the material composed of High-MW PLLA and Low-MW PCL was chosen for in-vivo implantation.
Heparin modification reduced the initial burst release of VEGF from electrospun PLLA scaffolds. PLLA/5%PCL scaffolds, which had significantly greater heparin conjugation capacity, further reduced the initial burst of VEGF. One explanation is that the increase of heparin on the surface of electrospun fibers provides more stable binding sites for VEGF. This heparin dependent effect on burst release of VEGF is consistent with previous reports on the growth factor release from heparin modified materials [193, 194].
The next chapter (Chapter 3),will discuss the implantation of small-diameter electrospun vascular grafts with VEGF using a rodent model. The formation of a confluent endothelial cell layer, vascular cell infiltration, and natural matrix deposition are all critical success factors for in situ vascular tissue engineering. As such, these features will be a focus in the study presented in Chapter 3.

34
Chapter 3 Implantation of Electrospun Vascular Grafts with VEGF for in situ Tissue Engineering

35
1. INTRODUCTION In Chapter 2, we investigated the mechanical and chemical properties of 3
different polymer blends containing a high-MW Poly(L-Lactide), two low-MW polymers; Poly(L-Lactide) and Polycaprolactone (PCL). Ultimately, a blend containing high-MW PLLA and Low-MW PCL was selected for future implantation. The addition of Low-MW PCL provided additional end groups for biomolecule attachment. This approach was able to significantly increase the density of immobilized heparin and VEGF. Additionally, the addition of Low-MW PCL enhanced the retention of VEGF to electrospun grafts after 7 days. Now, we move forward toward the goal of creating a viable small-diameter vascular graft through in situ tissue engineering.
Since endothelial Cells (ECs) are potent inhibitors of thrombosis, it is widely accepted that an ideal tissue engineered artery requires a functional and confluent endothelium to prevent failure. Therefore, stimulatory cues to guide endothelium formation are critical for in situ vascular tissue engineering. Additionally, scaffolds for in-situ vascular tissue engineering should support cellularization and natural matrix deposition. Cellularization and matrix deposition within electrospun materials has often been limited due to the relatively small pore sizes between fibers. Heparin coating has been shown to enhance the cellular infiltration within electrospun materials during dermal wound healing [185]. However, it is unclear whether heparin can influence cellular infiltration of electrospun materials in other applications. Additionally, vascular endothelial growth factor (VEGF), which has heparin binding ability, is a potent mitogen for ECs. Together, heparin and VEGF could act to simultaneously suppress thrombosis and stimulate endothelialization, vascular cellularization and matrix synthesis.
In this chapter, we will discuss the performance of electrospun vascular grafts with VEGF after implantation using a rat carotid artery model. In addition to overall patency, critical features for in situ tissue engineering, such as endothelium formation, cellular infiltration and matrix production will also be examined.

36
2. MATERIALS & METHODS
2.1 Fabrication of Electrospun Vascular Grafts
Electrospun vascular grafts were fabricated from the biodegradable polymers poly(L-Lactide) (PLLA; MW=100,000) (Lactel Absorbable Polymers, Pelham, AL) and poly(caprolactone) (PCL; MW=2,000) Polysciences, Warrington, PA). The polymers were combined to make a solution with final concentration of 19% (w/v) PLLA and 5% (w/v) PCL. The polymers were dissolved in the solvent 1,1,1,3,3-hexafluoro-2-propanol (HFIP) via sonication for 45 minutes or until fully dissolved. Electrospinning was performed to make vascular grafts for implantation as previously described[186]. Polymer solutions were delivered at a flow rate of 1ml/hr using a programmable syringe pump (Cole-Parmer, Vernon Hills, IL). A positive voltage of 12.5 kV was applied to a spinneret using a high voltage generator (Gamma High Voltage, Ormond Beach, FL). [188]. Fibers were collected onto a rotating stainless steel mandrel (speed = 20 rpm, diameter = 1 mm, same linear speed as 10cm drum). Electrospinning was performed until the graft wall thickness reached 150 µm. Grafts were then removed from the mandrel and placed into a vacuum desiccator for 24 hours to remove any residual HFIP.
Covalent attachment of heparin was performed as described previously [188]by using 1-ethyl-3-(3 dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxysulfosuccinimide (sulfo-NHS) (Pierce Biotechnology, Rockford, IL) as crosslinkers and di-amino-poly(ethylene glycol) (di-NH2-PEG) (Sigma Aldrich, St Louis, MO) as a spacer. The density of surface carboxyl groups was increased by briefly hydrolyzing the material in sodium hydroxide (NaOH, 0.01N) for 10 minutes. Grafts were rinsed thoroughly in phosphate buffered saline (PBS), followed by rinsing using deionized water. Grafts were then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10mg/ml sulfo-NHS and 20 mg/ml di-NH2-PEG at room temperature. Grafts were rinsed in PBS and then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10 mg/ml sulfo-NHS and 20 mg/ml unfractionated heparin sodium salt (Sigma Aldrich, St. Louis, MO). Following heparin modification, grafts were thoroughly washed in PBS and remaining reactive sites were quenched using 10 mg/ml glycine in PBS for 30 minutes. Following heparin modification, grafts were incubated in PBS solutions containing 1 µg/ml human recombinant VEGF-165 (Peprotech Inc., Rocky Hill, NJ) on a shaker for 16 hours at 4°C. After VEGF attachment, scaffolds were rinsed repeatedly in PBS for 30 minutes. Following PBS rinsing, grafts were stored in sterile PBS at 4°C , for no more than 24 hours prior to implantation during animal studies.
2.2 Animal Studies

37
All procedures were approved by the Institutional Review Board Service and Institutional Animal Care and Use Committee at the University of California, San Francisco and the University of California, Berkeley. Male Athymic rats (6-8 weeks old, 200–240 grams) were purchased from the National Cancer Institute Animal Facility. Rats were anesthetized with 2% isoflurane and placed in the supine position. Using aseptic techniques, a midline ventral incision was made exposing the right common carotid artery (CCA). The right CCA was then clamped, ligated, and a 6-mm long PLLA/5%PCLvascular graft (either untreated, heparin-modified or VEGF-modified) was sutured end-to-end by using interrupted 10-0 sutures. For 2-week studies, 6 animals were used in each experimental group. For 1-month studies, 11 animals were used in each experimental group. No additional heparin or other anti-coagulant was used at any time during these animal studies. At 2 weeks or 1 month following implantation, rats were euthanized and vascular grafts were explanted and washed with saline to remove remaining blood. Prior to euthanization and explantation at 1 month, graft patency was examined by using necropsy.
2.3 Histological Analysis Explanted grafts were either cut longitudinally for luminal en face staining,
or cryopreserved at -20ºC in optimal cutting temperature (OCT) compound (Sigma Aldrich) and cryosectioned into 10-µm thick sections for cross-sectional staining. Immunohistochemical staining for CD31 (BD Biosciences, San Jose, CA) and smooth muscle-myosin heavy chain (SM-MHC) (Santa Cruz Biotechnology) was performed to visualize the presence of ECs and smooth muscle cells (SMCs) respectively. Verhoeff’s stain was used to visualize collagen and elastin content within the graft. Nuclei were stained with DAPI to visualize the distribution of cells within the graft wall and surrounding tissue. The density of cells within the graft wall after 1-month was quantified from DAPI-stained sections by using image analysis software (NIH Image J). 2.4 En Face Immunofluorescence Staining for ECs
Endothelial coveage was assessed at 2 weeks post-implantation. Freshly explanted grafts were transected longitudinally and fixed with 4% paraformaldehyde for 20 minutes. Samples were washed with PBS, blocked with 5% goat serum and incubated with the mouse anti-rat CD31 primary antibody and Alexa-Fluor 488 secondary antibody. The samples were washed and mounted on slides with the inner luminal surface of the graft in-contact with the coverslip. Immunofluorescent Images of CD31+ cells were captured along the entire length of both the inner luminal surface and outer surface of the grafts by using a Zeiss confocal microscope. Images were stitched together using Adobe Photoshop to visualize the entire inner and outer surface of the graft. Computed histomorphometry was performed using Image J software. Endothelial coverage of the lumen was quantified by measuring the length of endothelial cell layer on the lumen surface, and is expressed as the percentage of total graft length.

38
2.5 Statistical Analysis
The data is presented as mean ± standard deviation. All data were analyzed with one-way ANOVA tests. Holm’s t test was performed to evaluate significant differences between pairs. A p-value of less than 0.05 was considered statistically significant. 3. RESULTS 3.6 Patency of Bioactive Electrospun Vascular Grafts
Using PLLA/5%PCL, untreated, heparin-modified and VEGF-modified scaffolds were fabricated and implanted into rats as vascular grafts. VEGF significantly increased the patency of vascular grafts after 1-month. After 1-month, 6 of 11 (55%) untreated grafts, 7 of 11 (64%) heparin-modified grafts, and 10 of 11(88%) VEGF-modified grafts were patent.
3.7 Endothelialization, Cellular infiltration and Matrix Remodeling of Vascular Grafts
Electrospun vascular graft explants were stained for the EC surface marker CD31 to assess the degree of endothelialization after 2-weeks (Fig. 3.1 A-C). VEGF immobilization significantly increased endothelialization on the inner surface. VEGF-modified grafts had 82% EC coverage after 2-weeks, which was approximately twice as much coverage found on both untreated and heparin modified grafts which had 39% and 40% EC coverage respectively (Fig. 3.1 G).
In addition to having more luminal coverage at 2-weeks, ECs on VEGF-modified grafts were more elongated and had morphology similar to that normally observed in the native endothelium (Fig. 3.2 A-I). After 2-weeks, substantial angiogenesis was observed in the outer layer of all grafts (Fig 3.1 D-F & Fig 3.2 J-L). The presence of newly formed microvessels suggests that the implanted grafts had been effectively integrated with the host tissues. After 1-month, ECs on VEGF-modified grafts retained a more elongated morphology, similar to that found in native arteries (Fig. 3.3 A-C).

39
Figure 3.1. Endothelialization and angiogenesis in vascular grafts at 2 weeks post-implantation. The grafts were stained for EC marker CD31. (A-C) EC coverage on the inner surface (lumen) of the grafts: (A) untreated, (B) heparin-modified, and (C) VEGF-modified. (D-F) ECs of microvessels on the outer surface of the grafts: (D) untreated, (E) heparin-modified, and (F) VEGF-modified. (G) Quantification of EC coverage on the inner surface of grafts at 2 weeks post-implantation. Scale Bar = 0.5 mm.

40
Figure 3.2. High magnification images of ECs on the inner surface of the vascular grafts, and microvessel formation on the outer surface of the vascular grafts, at 2 weeks post implantation. The samples were stained for EC surface marker CD31.
(A-I) ECs on inner surface. Representative inner layer images were taken from proximal, middle and distal graft segments. (J-L) Microvessel formation on outer surface. Scale Bar = 50 µm.
The contribution of SMCs in the remodeling of vascular grafts after 1-month was also analyzed (Fig. 3.3 G-I). MHC+ SMCs were found within the walls of heparin-modified and VEGF-modified grafts. MHC+ cells were also present within the neotissue that surrounded most but not all grafts. Small traces of Intimal hyperplasia were observed in a few untreated grafts at 1-month, as demonstrated by the presence of SMCs in the neointima.
The extent of matrix deposition (collagen and elastin) within the graft was assessed 1-month after the implantation (Fig. 3.3 J-L). Untreated grafts had minimal matrix deposition within the graft. In contrast, extensive matrix deposition was found within both heparin-modified and VEGF-modified grafts at 1-month. All grafts, untreated, heparin-modified and VEGF-modified, were surrounded by an outer layer of neotissue. The thickness of surrounding

41
neotissue varied and did not appear to be dependent on the type of graft treatment used in this study.
The effect of heparin and VEGF treatment on total cellular infiltration into electrospun grafts after implantation was assessed at 1-month (Fig. 3.4). Cellular infiltration was significantly greater for heparin-modified and VEGF-modified grafts, compared to untreated grafts. Some of the cells found within the wall of heparin-modified and VEGF-modified grafts are positive for MHC, suggesting that SMCs contributed to the population of infiltrating cells (Fig 3.3 G-I).

42
Figure 3.3. Endothelialization, SMCs and collagen/elastin deposition in electrospun vascular grafts at 1 month post-implantation. (A-C) En-face staining of CD31 for ECs on the inner surface of vascular grafts. (D-F) Cross-sectional staining of CD31 for ECs in the vascular grafts. (G-I) Cross-sectional staining of SM-MHC for SMCs in the vascular grafts. (J-L) Collagen and elastin deposited in the grafts were examined by using Verhoeff’s stain. Collagen is shown in pink, Elastin is shown in black. The scale bar indicated is 50 µm (A through C), 75 µm (D through F) and 200 µm (G through I), and 75 µm (J through L).

43
Figure 3.4. Cell infiltration into electrospun vascular grafts at 1 month post-implantation. Nuclei are stained by DAPI. (A) Cell density within the graft was quantified. (B-D) Cross-sections of explanted electrospun vascular grafts 1 month post-implantations. The boundary of the graft is marked by dashed lines. Scale bar = 150 µm.

44
4. DISCUSSION
VEGF modification enhanced endothelialization of electrospun vascular grafts at 2-weeks, and also improved graft patency at 1-month. Endothelialization may have occurred through a combination of proposed mechanisms including trans-anastomotic migration, capillary in growth and adhesion/differentiation/proliferation of circulating EC progenitors [195] . In this study, a small number of ECs were found dispersed within the wall of VEGF modified grafts. This finding suggests that circulating ECs and EC progenitors may have contributed to endothelialization. Achieving full endothelialization has been an extensive pursuit within the field of vascular tissue engineering. Interestingly, very few studies have explored the use of VEGF modification to direct endothelium formation. Of the few studies, most have shown VEGF treated grafts to enhance endothelialization but also at the cost of increasing inward remodeling from intimal hyperplasia [196, 197]. In contrast, the presence of intimial hyperplasia was not observed in our study of VEGF treated grafts. Electrospun fibrous materials have been reported to direct vascular SMCs toward a contractile phenotype, as opposed to the synthetic phenotype associated with intimal hyperplasia [198]. Heparin has been also shown to inhibit vascular SMC proliferation and possibly prevent initimal hyperplasia associated with VEGF [197, 199, 200]. Therefore, the presence of immobilized heparin in conjunction with electrospun fibers and VEGF may have acted together to reduce intimal SMC proliferation.
Heparin treatment also improved cellular infiltration into electrospun fibrous scaffolds. This result supports previous studies on heparin treatment and the effect on cellular infiltration into electrospun scaffolds [185]. Although we did not find a difference in total cellular infiltration between heparin-modified and VEGF grafts, CD31+ cells were only seen within VEGF grafts. This finding provides evidence that it may be possible to more effectively guide the specificity of infiltrating cells through combined immobilization of heparin and other biomolecules, such as VEGF.
Future studies should investigate the presence of intimal hyperplasia after long-term implantation of VEGF treated grafts. Additionally, recent publications have highlighted the role calcifications may play in vascular graft failure[201]. Future studies on VEGF-treated vascular grafts should also investigate the presence of calcifications after long-term implantation. Previous reports on VEGF treated materials have implicated the importance of dose dependency of VEGF on vascular tissue response[202]. Likewise, future studies should also investigate the influence of growth factor dose on the endothelialization, cellularization and patency of VEGF grafts. To further translate these findings into human environment, long-term foreign body response and implantation into large animals should be investigated.

45
Chapter 4 Conclusions & Future Directions

46
Conclusions & Future Directions
To date, the pursuit of a small-caliber vascular conduit remains one of the most challenging goals within the field of vascular tissue engineering. After nearly 30 years of research, there still is no surface coating capable of thwarting long-term thrombus formation. Many of the advancements in nonthrombogenic surface treatments have been able to prove effectiveness in vitro, but a major gap separates in vitro outcomes from in vivo implementation. The cause of this gap is likely a lack of understanding of the specific mechanisms involved in biomaterial-related thrombus formation in vivo [203]. For example, some in vitro studies that have been able to show significant reduction in platelet adhesion and activation have not necessarily been correlated with a reduction of the similar parameters in vivo. The influence of inflammation and its relationship with thrombus formation also has not been fully elucidated. Recently, inflammatory cells present in circulation have been discovered to be capable of expressing TF, one of the key enzymes involved in coagulation and platelet activation. Inflammatory responses and the toxicity of delivered drugs also may affect other cell types such as ECs and SMCs to inhibit endothelialization or stimulate SMC proliferation, resulting in complications such as late stent thrombosis. The nature of cross-talk between inflammatory responses and thrombosis warrants further investigation.
Aside from this, the mechanisms that lead to thrombus formation are multifaceted and self-enforcing, and surface treatments aimed to prevent a single mechanism of thrombus formation may not be sufficient. Recent studies that deal with both platelet adhesion and coagulation pathway, such as studies using PEG and hirudin, have shown some promise. Thus, the combination of surface modifications may further improve the efficacy.
Additionally, the orientation, conformation, and stability of the immobilized molecules on the surface should be further characterized. For example, direct thrombin inhibitors need to be presented on surfaces in the optimal configurations and at the optimal surface densities that inhibit thrombin at a rate equal to or likely greater than the rate of thrombin production. Computational modeling has been able to help the overall understanding of how levels of specific coagulation enzymes contribute to overall coagulation. New models that can allow researchers to gain more insight into the molecular structure and function of antithrombogenic molecules will be needed. This information can be combined with nanotechnologies to design and optimize the surface modification.
Many of the attempts to circumvent the need for nonthrombogenic coatings have moved toward creating EC-coated devices or completely biological equivalents. Owing to the immunological constraints inherent to ECs, it is now widely accepted that fabrication of endothelial layers requires autologous cells. This constraint still raises issues about EC sourcing and the difficulties of harvesting enough ECs from hosts. Circulating blood, bone marrow, and adipose tissues are

47
potential sources of ECs in adult. At least tens of millions of ECs are needed for surface coating or re-endothelialization of decellularized tissue and organs. The isolation and expansion of scalable autologous stem cells and progenitor cells for EC derivation or antithrombogenic treatment will need further investigation. Alternatively, with the advancement of cell-reprogramming technologies[204, 205], ECs can be either derived from autologous induced pluripotent stem cells or directly reprogrammed from autologous cells. Stem cell technologies that may be able to replicate suitable EC populations eventually may be able to reduce construction times of EC-coated devices, TEVGs, and vascularized tissues and organs.
Antithrombogenic modifications with biomolecules provide short-term nonthrombogenic surfaces, and endothelialization provides long-term protection from thrombosis. However, in situ endothelialization is attractive and may be needed to maintain the long-term nonthrombogenic property of implants without relying on the presence of anticoagulation, antiplatelet drugs in the blood circulation, or in vitro cell seeding. A major difference between human models and most of the animal models is that endothelialization of vascular grafts is hardly achieved in human, which could account for the different results in animal and clinical studies. The incapability to achieve complete endothelialization in humans can be attributed to long vascular grafts (>5 cm), limited transanastomotic endothelial migration, and inefficient capture of circulating ECs and EPCs. To address this issue, both biophysical and biochemical modifications are needed. For example, the micro- and nanotopography of the luminal surface in vascular grafts can be designed with microgrooves or aligned nanofibers in the longitudinal direction to promote transanastomotic EC migration. Biochemical modification with ligands or antibodies for circulating ECs and EPCs will also facilitate endothelialization.
In chapters 2 & 3, we began investigating in situ vascular tissue engineering approaches. Our objective was to create bioactive vascular grafts using electrosnpun fibers with the capability to accelerate endothelializaton and direct vascular cellularization in situ. In doing so, we investigated the effectiveness of an electrospun vascular graft with combined heparin and VEGF. VEGF modification enhanced endothelialization of electrospun vascular grafts at 2-weeks, and also improved graft patency at 1-month. Endothelialization may have occurred through a combination of proposed mechanisms including trans-anastomotic migration, capillary in growth and adhesion/differentiation/-proliferation of circulating EC progenitors . Future studies should aim to elucidate the specific mechanism by which endothelialization via VEGF signaling may have occurred. The presence of intimal hyperplasia, and calicification after long-term implantation(6-12 months) of VEGF treated grafts should also be explored.

48
Chapter 5 Development of Injectable Amniotic Membrane Matrix for Post-Myocardial Infarction Tissue Repair

49
1. INTRODUCTION
Myocardial Infarction (MI) associated heart failure is the leading cause of death in the U.S[206]. MI occurs when blood flow to the heart from coronary arteries is temporarily blocked, causing ischemia and subsequent myocardial tissue death. Myocardial tissue is unable to effectively regenerate following MI, thus leading to left ventricular remodeling, scar formation, and eventual heart failure[207-209]. Cardiac tissue engineering strategies that promote regeneration of healthy myocardial tissue and prevent scarring are critical for preventing post-MI heart failure. A variety of scaffolds have been explored to direct cardiac tissue growth. However, the biochemical compositions of these scaffolds are not optimal and fail to reduce scarring. As a result, the restoration of cardiac tissue function is prevented.
In contrast, decreased scar formation has been identified as a characteristic associated with the early fetal wound healing environment. For this reason, fetal membranes such as the amniotic membrane (AM) have been extensively studied and have been shown to exert anti-scarring and anti-immflammatory effects[210-212]. For years, human amniotic membrane (hAM) tissue has been used to repair corneal defects and reduce scarring during healing[211, 213, 214]. Due to its anti-scarring, and potential regenerative properties, materials derived from hAM could serve beneficial in restoring cardiac function following MI. Moreover, development of an injectable form of hAM matrix would allow for non-invasive delivery, which would help enhance the potential benefits.
In this chapter, a method for isolating hAM matrix through decellularization is discussed, as well as a processing methods to yield an injectable formulation of hAM matrix. Characterization of decellularization efficiency, matrix composition and in vitro cytotoxicity is also presented. Lastly, preliminary in vivo animal studies which investigate the efficacy of injectable hAM matrix delivery on the restoration cardiac function following various stages of myocardial infarction (acute, subacute, & chronic) are presented.
2. METHODS
2.1 Decellularization of Human Amniotic Membrane (hAM)
Full term human placentas with intact amniotic membrane (hAM) were obtained from healthy donors undergoing caesarean section at the University of California, San Francisco or University of California, Davis Hospital. The hAM was then identified and separated from the placenta and weighed. The tissue was subsequently frozen at -80C for 48 hours and thawed prior to decellularization. The membrane was thoroughly rinsed with water and soaked in 1N saline for 15 minutes. Membranes were then treated in a solution containing 8mM CHAPS

50
[3-[3-Cholamidopropyl]dimethylammonio]-1-propanesulfonate], 25mM EDTA, and 1M NaCl at room temperature with moderate shaking. The CHAPS solution was removed and replenished every 2 hours, for 6 hours total. For comparison purposes, 8mM SDS (sodium dodecyl sulfate) was used instead of CHAPS. Following CHAPS or SDS treatment, all membranes were subsequently washed with TBS (3 times, 20 minutes each). To remove remaining nucleic acid material, membranes were incubated in a 90 U/ml benzonase solution (Sigma Aldrich Inc.) for15 hours at 37°C. To enhance nuclease activity, benzonase was prepared in 50mM Tris-HCL pH 8.0, with 0.1 mg/ml BSA, and 1mM MgCl2. Following benzonase treatment, hAMs were washed repeatedly in TBS, followed by repeated washes with distilled water. hAMs were further decellularized and disinfected using a 0.1% peracetic acid,4% ethanol and water. After repeated washing in TBS, and distilled water, hAMs were dialyzed against water at 4°C for 4 days to remove excess reagents.
Following dialysis, portions of the decellularized hAM were snap frozen in OCT compound and sectioned for histological analysis. Intact and unteated hAM was also frozen and sectioned for comparison. Sections were stained with DAPI or Hematoxylin & Eosin to visualize nuclei and matrix components respectively.
2.2 Preparation of Injectable hAM Matrix
Decellularized hAMs were lyophilized overnight, and subsequently ground into a dry powder using a motorized grinder. The decellularized hAM powder was solubilized by digesting in 0.2 mg/ml pepsin and 0.1N HCL for 48 hours at room temperature. A ratio of 20mg hAM Matrix per 200µg per 1ml 0.1N HCL was used. After 48 hours, the solution pH was adjusted to 8.0 using 10N NaOH and 10x PBS. The pH adjusted matrix was then re-lyophilized overnight, ground into powder form, and stored at 4°C. Prior to experiments, the hAM matrix sterilized in ethylene oxide gas overnight. To induce gelation, hAM matrix was dissolved in PBS (20mg/ml) and allowed to gel at 37°C.
2.3 Characterization of Injectable hAM Matrix
Remaining DNA content in the injectable hAM matrix was quantified using a Quant-iT™ PicoGreen® Assay (Invitrogen, Grand Island, NY). A DNeasy Blood & Tissue Kit® (Qiagen, Valencia, CA) was used to isolate DNA prior to quantification using the assay. The DNA content of CHAPS processed hAM matrix, and SDS processed hAM matrix is presented as a percentage of native, untreated hAM tissue.
Glycosoaminoglycans (GAGs) are often reported be lost following decellularization of tissue. For this reason, we quantified the GAG content of both CHAPS processed hAM matrix and SDS processed hAM matrix. GAG content was quantified using a colorimetric 1,9 dimethylmethylene blue (DMMB) assay as described previously[215]. This reagent specifically binds to the sulfate

51
and carboxyl groups of sulfated GAGs to cause a metachromatic shift. This shift in absorption can then be quantified via spectroscopy at 530 nm . Lyophilized powder native and decellularized hAM tissue was first digested using proteinase K (1mg proteinase K/ 80mg hAM matrix). DMMB reagent (16µg/mL) was then allowed to react with the samples. GAG content in each sample was then immediately quantified by measuring the absorbance at 530nm and comparing to values obtained using known GAG concentrations. Final GAG content is given as a percentage of GAG content in the native tissue. The hAM matrix processed using CHAPS contained the highest amount of preserved GAG content. For this reason, the CHAPS hAM matrix was used in all in vitro and in vivo experiments.
Mass spectrometry was also performed in order survey the overall protein composition of the injectable hAM matrix. Samples were digested with trypsin and desalted with C18 spec tips prior to analysis. Identification of proteins was done at the Vincent J. Coates Proteomics/Mas Spectrometry Laboratory, was performed using 2-dimension (“MudPit”) HPLC separation with tandem mass spectrometry. Peptide identification and data analysis and was performed using SEQUEST.
2.4 In Vitro Characterization of Injectable hAM Matrix Cytotoxicity
Cytoxicity was examined by investigating the effect of injectable hAM matrix on bovine arterial endothelial cells (BAECs). BAECs were harvested from fresh bovine aortas as previously described using collagenase and gentle scrapping with a policeman[216]. All cells were cultured in Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% fetal bovine serum (FBS) and 1% penicillin/streptomycin antibiotic mix. Cell culture was maintained in a humidified incubator at 37°C.
For proliferation experiments, the surfaces of a 24-well tissue culture plate were coated with either 1mg/ml rat tail collagen type-1 (BD Biosciences) or 5mg/ml injectable hAM matrix. BAEC were seeded on coated surfaces at low density (1000 cells/cm2), medium density (5,000 cells/cm2), and high density (10,000 cells/cm2). BAEC proliferation on hAM matrix and collagen type-1 surfaces after 48 hours was then measured and compared using a Click-iT® EdU Alexa Fluor® 488 Detection Kit (Life Technologies Inc). Samples were counterstained using DAPI. Cell proliferation is given as the percent of EdU positive cells. Proliferation data is presented as mean ± standard deviation. All data were compared with one-way ANOVA tests. Holm’s t test was performed to evaluate significant differences between pairs. A p-value of less than 0.05 was considered statistically significant.
2.5 Acute, Sub-Acute and Chronic Myocardial Infarction (MI) Models

52
All surgical procedures were approved by the Committee for Animal Research of the University of California San Francisco. The ischemia-reperfusion model used in this study has been previously used extensively as a model for myocardial infarction (MI)[217, 218]. Female Sprague-Dawley rats (225–250 g) were anesthetized with ketamine (90 mg/kg) and xylazine (10 mg/kg). The chest was opened by a median sternotomy, and a single stitch of 7-0 Ticron suture (United States Surgical division of Tyco Healthcare, Norwalk,CT) was introduced around the left anterior descending (LAD) coronary artery and tightened to occlude for 30 min before reperfusing the vessel. In the acute MI studies, animals were allowed to recover for 2 days prior to treatment. In the sub-acute MI studies, animals were allowed to recover for 2 weeks prior to treatment. Lastly, in the chronic MI studies, animals were allowed to recover for 4 weeks prior to treatment.
2.6 Preliminary hAM Matrix Injection Studies
At 2 days post-MI, rats in the acute study group were randomized into hAM matrix (n=5) or PBS control group (n=3). At 2 weeks post-MI, rats in the sub-acute study group were randomized into hAM matrix (n=3) or PBS control group (n=3). At 4 weeks post-MI, rats in the chronic study group were randomized into hAM matrix (n=2) or PBS control group (n=3). The animals were anesthetized and the abdomen was opened. The LV apex was exposed via a subdia-phragmatic incision, leaving the chest wall and sternum intact. For each treatment group, 0.1ml was injected into the infarcted LV of each heart using a 27-G needle and echocariographical guidance.
2.7 Functional Recovery of LV function after hAM Matrix Injection
Transthoracic echocarography was performed immediately prior to injection, and 4 weeks after injection. Echocardiograms were used to calculate ejection fraction and fractional shortening before and after treatment. Ejection fraction was calculated as described previously. A parasternal long axis B-mode image was acquired in order to identify the maximum LV length.. Three short axis B-mode images were also acquired at basal, midventricular, and apical LV levels. Results are presented as the percent change in ejection fraction and percent change in fractional shortening. Using frames from the long axis images, as well as maximum and minimum cross sectional areas in the heart cycle, LV end-systolic volume (LVESV) and LV end-diastolic volume were calculated. LV Ejection fraction (LVEF) was calculated as follows, LVEF = [(LVEDV – LVESV)/LVEDV] x 100. Results are given as the percent change in LVEF 1- month post injection. Left ventricular inner dimensions at systole (LVIDs) and diastole (LVIDd) were calculated using the leading edge method, as prescribed by the American Society of Echocardiography. Fractional shortening, FS was calculated as follows, [(LVIDd – LVIDs)/LVIDd] x 100. Results are presented as the percent change in FS 1-month post injection

53
3. RESULTS
3.1 Characterization of injectable human amniotic membrane (hAM) matrix
An injectable hAM matrix was prepared through decellularization of hAM tissue (Fig. 5.1). Using a series of chemical treatments, which included the use of either CHAPS or SDS detergent, hAM tissue was successfully decellularized.
The solubilized hAM matrix remained a viscous liquid while on ice or at room temperature. Gelation could be induced when placed at 37°C, as the resulting material became a soft gel that required gentle handling (Fig 5.1D).
Figure 5.1: Physical appearance of hAM during various stage of processing. A) Untreated hAM prior to decellularization. B)Decellularized hAM tissue. C) Lyophilized and ground soluble hAM matrix. D) Solubilized hAM matrix after 1-hour of gelation at 37C. hAM gel is shown at top of tube. For contrast, non-gelled DMEM liquid is shown residing on bottom..

54
The decellularized tissue was sectioned and stained for nuclei using either DAPI or hemotoxylin & eosin (H&E) stain. Both CHAPS and SDS decellularization processes were successful, as both tissues groups appeared devoid of cells (Fig 5.2). General matrix structure of native,CHAPS decellularized and SDS decellularized hAM was visualized using H&E staining(Fig. 5.2 A-C). The matrix structure of CHAPS decellularized hAM appears to be minimally altered in comparison to native hAM. However, the matrix structure of SDS decellularized hAM appears significantly altered when compared to the structure of native hAM.
In order to quantify the efficiency of decellularization protocols, remaining DNA content within decellularized hAM matrix was quantified (Fig 5.3A). The amount of DNA/mg of both SDS and CHAPS processed tissue was measured as a percentage of the amount of DNA/mg of untreated hAM tissue. Following CHAPS decellularization, only 3.4% of the native hAM DNA content remained. Similarly, only 4.1% of the native DNA content remained following decellularization using SDS. No significant difference in DNA content was observed between SDS and CHAP hAM matrix.
Glycosoaminoglycans (GAGs) are a critical component of the extracellular matrix, and also a component commonly lost after decellularization. For this reason, the GAG content within CHAPS and SDS decellularized hAM was measured (Fig. 5.3B). GAG content was measured as a percentage of the GAG content found within native, untreated hAM. After CHAPS decellularization, GAGs were relatively conserved, as 85.6% of the native GAG in hAM was retained. In contrast however, only 10.1% of native GAG content was retained following decellularization using SDS. Since effective decellularization could be achieved using CHAPS, and GAG/matrix components were preserved, CHAPS processed hAM was used in all in vitro and in vivo experiments.
Mass spectrometry analysis of the injectable hAM matrix revealed a complex mixture of over 1100 proteins. Table 5.1 summarizes the major matrix components and proteins of interest that were identified. A complete summary of the analysis can be found in the appendix.

55
111 111111 Protein 1 Collagen I 2 Collagen III 3 Collagen IV 4 Collagen V 5 Collagen VI 6 Collagen VII 7 Collagen XII 8 Collagen XIV 9 Collagen XVIII 10 Collagen XXVII 11 Fibronectin 12 Laminin 13 Keratin 14 Fibrillin-1 15 Fibrillin-2 16 Insulin-like Growth Factor Binding Protein 17 Latent TGF-β Binding Protein-1 15 FGF Receptor-III 15 VEGF Receptor-I
Table 5.1: Summary of major matrix proteins in injectable hAM matrix, identified using 2D-Mud-Pit Mass Spectrometry Analysis.

56
Figure 5.2: Histological characterization of CHAPS and SDS decellularized hAM tissue. (A-C) H&E staining of untreated, CHAPS decellularized and SDS decellularized hAM. (D-F) DAPI staining of nuclei present in untreated, CHAPS decellularized, and SDS decellularized hAM. Scale bar = 150µm.

57
Figure 5.3: Biochemical Characterization of DNA and GAG content in decellularized hAM. A) Percentage of native DNA content remaining after CHAPS or SDS decellularization. B) Percentage of native glycosoaminoglycan (GAG) content remaining after CHAPS or SDS decellularization.
3.2 In vitro studies using bovine aortic endothelial cells (BAECs)
To assess the preliminary biocompatibility and cytotoxicity of the injectable hAM matrix, the proliferation of BAECs on hAM matrix was measured. As a positive control of biocompatiblity, the proliferation of BAECs on type-1 collagen was also measured. At low, medium and high cell densities, there was no significant difference in proliferation on hAM surfaces, when compared to proliferation on Collagen-1 surfaces with similar cell densities (Fig 4). Thus, no decline in proliferation was observed, suggesting the absence of cytotoxicity from the hAM matrix.

58
Figure 5.4: Proliferation of bovine aortic endothelial cells on hAM matrix. BAECs were seeded at low, medium, and high density on either hAM ECM or collagen-1. Proliferation was measured using EdU and is presented as the percentage total DAPI stained cells expressing positive EdU staining.
3.3 Acute MI and recovery of LV function following hAM Matrix Injection
Using an acute rat model of MI, a preliminary investigation on the efficacy hAM matrix injection was performed. Two days after MI, hAM matrix or PBS was injected. The change in ejection fraction and fractional shortening was then measured 1-month after injection B. For hAM ECM group, 5 of 5 animals experienced an improvement in ejection fraction. After PBS injection, 2 of 3 animals experienced a decline in ejection fraction. On average, the percentage change in ejection fraction for hAM ECM and PBS injection groups was +8.8% and -9.7% respectively (Fig. 5). Fractional shortening also improved for animals receiving hAM ECM following acute MI. Improvements in fractional shortening were observed in 5 of 5 animals received hAM injection. A decline in franctional shortening following acute MI was observed for all animals receiving PBS injection. On average, animals receiving hAM ECM injection experienced a 10.5% increase in fractional shortening, while animals receiving PBS injection experienced a 8.4% decline in fractional shortening (Fig. 6).

59
Figure 5.5: Effect of ECM injection on LV ejection fraction following acute MI. A)Average change in ejection fraction for animals receiving either hAM ECM or PBS injection. B)Summary of changes in ejection fractions by animal and treatment type.

60
Figure 5.6: Effect of ECM injection on LV fractional shortening following acute MI. (A)Average change in fractional shortening for animals receiving either hAM ECM or PBS injection. (B)Summary of changes in fractional shortening by animal and treatment type.
3.4 Sub-Acute MI and recovery of LV function following hAM Matrix Injection
Using a sub-acute rat model of MI, a preliminary investigation on the efficacy hAM matrix injection was performed. Two weeks after MI, hAM matrix or PBS was injected. The change in ejection fraction and fractional shortening was then measured 1-month after injection (Fig 7 & Fig 8). For hAM ECM group, 3 of 3 animals experienced an improvement in ejection fraction. After PBS injection, 2 animals experienced an improvement in ejection fraction, while 1 animal experienced a decline. On average, the percentage change in ejection fraction for hAM ECM and PBS injection groups was 8.8% and -9.7% respectively. SImilar trends were observed in fractional shortening. Improvements in fractional shortening were observed in 3 of 3 animals receiving hAM injection. A decline in fractional shortening following sub-acute MI was observed in 1 animal receiving PBS injection, while an improvement was observed in 2 animals receiving PBS. On average, animals receiving hAM ECM injection experienced a 12% increase in fractional shortening, while animals receiving PBS injection experienced a 9.7% decline in fractional shortening.

61
Figure 5.7: Effect of ECM injection on LV ejection fraction following sub-acute MI. A)Average change in ejection fraction for animals receiving either hAM ECM or PBS injection. B)Summary of changes in ejection fractions by animal and treatment type.
Figure 5.8: Effect of ECM injection on LV fractional shortening following sub-acute MI. (A)Average change in fractional shortening for animals receiving either hAM ECM or PBS injection. (B)Summary of changes in fractional shortening by animal and treatment type.
3.5 Chronic MI and recovery of LV function following hAM Matrix Injection
Using a chronic rat model of MI, a preliminary investigation on the efficacy hAM matrix injection was performed. Four weeks after MI, hAM matrix or PBS was injected. The change in ejection fraction and fractional shortening was then measured 1-month after injection. For hAM ECM group, all animals experienced an improvement in ejection fraction. In contrast, after PBS injection, all animals experienced a decline in ejection fraction. On average, the percentage change in ejection fraction for hAM ECM and PBS injection groups was 9.6% and -12.1% respectively. Similar trends were observed in fractional shortening. All animals receiving hAM injection experienced an improvements in fractional shortening. In contrast, all animals receiving PBS injection experienced a small decline in fractional shortening. On average, animals receiving hAM ECM injection

62
experienced a 12% increase in fractional shortening, while animals receiving PBS injection experienced a -2.9% decrease in fractional shortening.
Figure 5.9: Effect of ECM injection on LV ejection fraction following chronic MI. A)Average change in ejection fraction for animals receiving either hAM ECM or PBS injection. B) Summary of changes in ejection fractions by animal and treatment type.
Figure 5.10: Effect of ECM injection on LV fractional shortening following chronic MI. (A)Average change in fractional shortening for animals receiving either hAM ECM or PBS injection. (B)Summary of changes in fractional shortening by animal and treatment type.

63
4. CONCLUSIONS AND FUTURE DIRECTIONS
The goal of this study was to develop an injectable ECM derived from human amniotic tissue, and investigate its potential to promote recovery following myocardial infarction. To date, this study is the first to report the development of a injectable scaffold derived from decellularized amniotic membrane. Previous studies have utilized decellularization methods to fabricate injectable scaffolds from urinary bladder matrix, myocardial matrix, and lipoaspirate matrix. Our hypothesis, is that our human amniotic membrane matrix takes advantage of unique anti-scarring properties that are specific and unique to fetal membrane tissue.
The composition of extracellular matrix is unique to the organ/tissue from which it is derived. Likewise, decellularization methods must be tailored and made unique according to the tissue of interest. Through experimentation of various decellularization techniques, we have identified a process that is capable of preserving extracellular components, most specifically, the natural glycosoaminoglycans, from amniotic membrane. This process is highly efficient in removing cellular contents, as seen in the removal of >96% of native DNA content. For future studies, it will be helpful to determine if higher levels of decellularization are needed to yield non-immunogenic matrix products.
Through in vitro cell studies on bovine aortic endothelial, we found that the injectable hAM matrix was non-cytotoxic, and did not affect cell proliferation. In the future, it will be helpful to determine the effects on cell proliferation, attachement, and migration for other cardiac specific cell lines. In addition, it will be helpful to determine if the extracted hAM matrix is capable of affecting myofibroblast differentiation, an event central to the process of scar formation.
Lastly, we sought to perform a preliminary set of in vivo animal studies to investigate the effect of hAM injection on functional LV recovery following myocardial infarction. Heart failure following MI is a progressive process, consisting of several stages. During the acute phase, cardiomyocyte death occurs, and is following my macrophage, monocyte and neutrophil migration. The inflamation response continues through the subacute phase, until cellular components begin to be replaced by dense collagen fibrils. During the chronic phase, infarct expansion occurs, leading to dilation and continued LV remodeling. Due to the diversity in physiological response across various of stages MI, we chose to do preliminary studies on the effects of hAM matrix injection on cardiac function different stages of MI.
In the acute model, hAM matrix injection appears contribute to an improvement in LV function, as ejection fraction and fractional shortening both increased significantly following treatment. Although the improvement was statistically significant, sample sizes will need to be increased in order reach a higher power of analysis. In the subacute studies, there does not appear to be a

64
preliminary trend toward an improvement in LV function following hAM injection. Interestingly however, results from the chronic MI study show consistent improvements in LV function following hAM matrix injection. If future studies are able to confirm this result, it would suggest that hAM matrix injection is capable of reversing the effects of advance LV remodeling, and potentially infarct scar formation.
Future studies will obviously need to focus on increasing the sample sizes across all groups. In addition, histological analysis must be performed to investigate the effects of hAM injection of fibrotic tissue formation, angiogenesis, and the presence of inflammatory cells. In addition, elucidation of the potential mechanism of LV functional improvement from hAM matrix injection will require a comparison to the effects of other matrix materials. By adding additional matrix groups to the study, it can be confirmed whether LV functional improvement from hAM matrix injection is due to the unique biochemical environment of the amniotic membrane, or if LV improvement is due to a mechanical constrainment of LV dilation. To further elucidate the mechanism of action, additional in vitro studies should be performed which analyze the effects on myofribroblasts, and other cardiac specific stem cell populations.

65
Chapter 6 Supplemental Experiments
• Stability of immobilized SDF-1α from Micro-Fibrous Vascular Grafts under Flow
• Modification of Nano/Micro-Fibrous Vascular Grafts using Thrombin Binding Aptamers
• Impantation of Nano/Micro-Fibrous Vascular Grafts in a Porcine Model

66
Stability of immobilized SDF-1α from Micro-Fibrous Vascular Grafts under Flow
1. INTRODUCTION
In the past decade, significant progress has been made to construct tissue-engineered blood vessels (TEBV) in vitro by using vascular cells with or without scaffolds[178, 179, 182, 184, 219, 220].In addition, adult stem cells such as bone marrow mesenchymal stem cells or mixed cell populations have been used to make TEBV[183, 184, 221-223]. However, constructing cellular grafts involves extensive manipulation of cells in vitro and is time consuming, which limits the application to individualized and non-urgent therapies.
An interesting finding from the studies on stem cell-seeded grafts is that the stem cells in TEBVs are replaced by endogenous cells within days to weeks[182, 222],,suggesting that the regeneration potential of endogenous cells could be harnessed for blood vessel regeneration. However, adult vascular cells, including endothelial cells (ECs) and smooth muscle cells (SMCs), have limited expansion capability. Therefore, it will be highly desirable to develop vascular grafts that can recruit endogenous stem cells or progenitor cells of both ECs and SMCs. CD34+ endothelial progenitor cells (EPCs) are present in circulating blood, and can differentiate into ECs[224, 225].
Many biochemical factors are able to influence EPC mobilization and homing to ischemic tissues[220, 226, 227] In particular, stromal cell-derived factor-1α (SDF-1α) is a potent factor for EPC homing as well as neovascularization[228, 229]. The immobilization of such factors to the vascular graft surface is a promising strategy toward achieving in situ vascular regeneration. In doing so, the stability of immobilized factors is a key feature for concern. In contrast to several other applications, the vascular grafts surface is exposed to fluid shear stress from blood flow. The condition of flow is likely to accelerate release of immobilized factors from the graft surface.
In this section, microfibrous vascular grafts with attached SDF-1 and heparin were fabricated. The stability of attached SDF-1 was investigated by measuring the release of SDF-1 over time under static and flow conditions.
2. METHODS & MATERIALS
2.1 Fabrication of vascular grafts

67
Microfiber scaffolds were fabricated by using poly(l-lactic acid) (PLLA) (Mw 67,400, Sigma–Aldrich) and polycaprolactone (PCL, Mw 2000, Polysciences). The polymer blends (e.g., 19% PLLA and 5% PCL; w/v) were completely dissolved in 1,1,1,3,3,3-hexafluoro-2-propanol (HFIP, Aladdin). Microfibrous grafts were made by electrospinning polymer fibers onto a rotating stainless steel mandrel (1-mm diameter and 300 rpm). The negative voltage of 4.5 kV was applied to the mandrel, and a positive voltage of 4 kV was applied to the spinneret by using a high-voltage generator (Gamma High Voltage, Ormond Beach, FL). The electrospinning process was allowed to proceed until an approximately 200-µm wall thickness was achieved. The structure of the scaffolds was characterized by using a scanning electron microscope (Hitachi TM-1000). The half-life of the degradation of PLLA, the major component in the grafts, is about one year.
2.2 Heparin conjugation and SDF-1α immobilization
Heparin-functionalized microfibers were fabricated by using di-NH2–PEG as a linker molecule [24]. Briefly, the density of reactive carboxylic groups on the microfibers was increased by briefly treating the scaffolds with 0.01 N NaOH (Sigma–Aldrich). Di-NH2–PEG molecules (Mw 3400, Sigma) were then covalently attached to the carboxylic groups on the microfibers by using EDC and Sulfo-NHS (Pierce Biotechnology). Heparin was conjugated to the free amines on the di-NH2–PEG molecules via EDC and Sulfo-NHS. Following heparin conjugation, SDF-1α (R&D Systems) in PBS (500 ng/mL) were incubated with the scaffolds over night at 4 °C to allow for its binding to heparin and its immobilization on the scaffolds. For comparison, same concentration of SDF-1α was passively adsorbed onto microfibers of untreated grafts as control.
2.3 Stability and In Vitro Release of Immobilized SDF-1 α under flow and static conditions
The stability and in vitro release of immobilized SDF-1α was evaluated over a period of 7 days under both static and flow conditions. For static release experiments, 1 mL of PBS was used as incubation medium for each graft. PBS was removed and replenished every 24 h. For release experiments under flow, silicon tubing was used to connect grafts to a large reservoir (100 L) containing PBS. The reservoir was placed at height above the graft to supply PBS at a flow rate of 476 ± 6 mL/h, which corresponded to a physiologically relevant shear stress of ∼13 dyn/cm2. A peristaltic pump was used to pump PBS back into the reservoir to maintain the circulation of PBS. Grafts were collected on days 0, 1, 3 and 7 followed by complete digestion in 0.1 N NaOH for 36 h. Following digestion, samples were neutralized with 0.1 N HCl. The amount of immobilized SDF-1α remaining was then directly quantified using an ELISA kit (R&D System).

68
Figure A.1: Schematic of vascular graft flow loop. Silicon tubing is used to deliver PBS from reservoir #1, through attached graft, and into reservoir #1. Peristaltic pump returns displaced fluid back into reservoir #1. Multiple grafts with attached tubing were run in parallel (n=4 for each group)
3. RESULTS
To suppress thrombogenic events, microfibers were functionalized with heparin by using di-amino-poly (ethylene glycol) (di-NH2–PEG) as a linker molecule. Di-NH2–PEG was covalently attached to the carboxylic groups on the microfibers by using 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxysulfosuccinimide (Sulfo-NHS) .Heparin was then covalently attached to the free amines on the di-NH2–PEG molecules via carbodiimide chemistry. Since heparin binds to and stabilizes SDF-1α, we used heparin as a molecular linker to sequester recombinant SDF-1α.
The stability and in vitro release of immobilized SDF-1α was evaluated by ELISA and the results were normalized and shown. The amount of SDF-1α at Day 0 in the control and in the heparin-bound group was 87.2 ± 3.7 ng/cm3 and 268.3 ± 13.8 ng/cm3 (n = 6), respectively. It showed that SDF-1α was stably immobilized on the microfibrous scaffolds and a slow release of SDF-1α was achieved for more than a week in vitro (Fig A.2). In contrast, passively adsorbed SDF-1α on microfibers was not stable and was released rapidly. This was further accelerated by flow as the passively adsorbed SDF-1α was completely washed off within a week. However, after 1 week, 40% and 20% of heparin-bound SDF-1α remained on the grafts under static and flow conditions respectively.

69
Figure A.2: The time course of SDF-1α release from grafts. The release kinetics of the control group (passively adsorbed SDF-1α) and heparin-bound SDF-1α. SDF-1α under static and flow conditions was compared. The amount of SDF-1α remaining on the grafts is shown (n = 4 for each group).
0
20
40
60
80
100
0 5 10
Perc
enta
ge o
f Im
mob
ilize
d SD
F-1α
Rem
aini
ng
Time (Days)
Control (Static)
Control (Flow)
Heparin (Static)
Heparin (Flow)

70
Modification of Nano/Micro-Fibrous Vascular Grafts using Thrombin Binding Aptamers
1. INTRODUCTION
Aptamers are short sequences of nucleic acids that are capable of 3-dimensonal recognition, binding and inhibition of target proteins[230, 231]. We have created a method for modifying vascular grafts using aptamer based anticoagulants. The use of aptamers to bind and inhibit thrombogenic factors could prevent occlusion of vascular grafts and has several advantages over previously used anticoagulants. Heparin is currently the standard anticoagulant used clinically. Heparin is typically isolated from bovine or porcine tissues, which can present several risks including the transmission of viruses. Oversulfated heparin contamination has also led to severe illness and even death. Since aptamers are comprised of short nucleic acid sequences (15-100 bases), they can be readily made with high quality control and high yields at a substantially lower cost.
In this study, thrombin binding aptamers are conjugated to electrospun nano-fibrous vascular grafts. Results from a preliminary animal study to evaluate the efficacy nanofibrous grafts with conjugated thrombin aptamers is also presented.
2. METHODS & MATERIALS
2.1 Fabrication of Electrospun Vascular Grafts with immobilized TBA
Nanofibrous vascular grafts were fabricated using poly(l-lactic acid) (PLLA) (Mw 67,400, Sigma–Aldrich) and polycaprolactone (PCL, Mw 2000, Polysciences). The polymer blends (e.g., 19% PLLA and 5% PCL; w/v) were completely dissolved in 1,1,1,3,3,3-hexafluoro-2-propanol (HFIP, Aladdin). Microfibrous grafts were made by electrospinning polymer fibers onto a rotating stainless steel mandrel (1-mm diameter and 300 rpm). The negative voltage of 4.5 kV was applied to the mandrel, and a positive voltage of 4 kV was applied to the spinneret by using a high-voltage generator (Gamma High Voltage, Ormond Beach, FL). The electrospinning process was allowed to proceed until an approximately 200-µm wall thickness was achieved.
The known thrombin binding aptamer (TBA) sequence 5’ GGTTGGTGTGGTTGG-3’ was immobilized to electrospun vascular grafts.

71
Aptamers sequences were ordered from Integrated DNA Technologies Inc. For immobilization purposes, the aptamer was customized with a 5’ modification containing an amine terminated standard C12 spacer to yield NH2-C12-5’ GGTTGGTGTGGTTGG-3’.
Covalent attachment of aptamers was performed using 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxysulfosuccinimide (sulfo-NHS) (Pierce Biotechnology, Rockford, IL). Briefly, grafts were treated briefly with 0.1N NaOH for 10 min and rinsed with PBS. Subsequently, grafts were allowed to react for 3 hours in MES buffer containing 10 µM, NH2-C12-5’ GGTTGGTGTGGTTGG-3’ 20mg/ml EDC and 10mg/ml Sulfo-NHS.
Visualization of covalently attached TBA was achieved by using a biotinylated sequence NH2-C12-5’ GGTTGGTGTGGTTGG-3-Biotin, followed by labeling using streptavidin-conjugated Alexa 488 (Life Technologies Inc.). As negative controls, non-conjugated Aptamer scaffolds (passively absorbed), and conjugated non-biotinylated grafts were stained.
2.2 Animal Studies
All procedures were approved by the Institutional Review Board Service and Institutional Animal Care and Use Committee at the University of California, San Francisco and the University of California, Berkeley. Male Athymic rats (6-8 weeks old, 200–240 grams) were purchased from the National Cancer Institute Animal Facility. Rats were anesthetized with 2% isoflurane and placed in the supine position. Using aseptic techniques, a midline ventral incision was made exposing the right common carotid artery (CCA). The right CCA was then clamped, ligated, and a 6-mm long graft (either untreated,or TBA-modified) was sutured end-to-end by using interrupted 10-0 sutures. 3 rats were used for each experimental group.
Patency was observed using necropsy 1-month following implantation. At 1-month, animals were sacrificed and grafts were removed. Grafts were then snap-frozen in OCT and sectioned for histological analysis. Hematoxylin staining was performed to visualize the presence of thrombosis, occlusion and neointima formation.
3. RESULTS
3.1 Fabrication of Electrospun Vascular Grafts with immobilized TBA
The thrombin binding aptamer sequence was successfully conjugated to electrospun vascular grafts. Fluorescent visualization of the immobilized biotinylated aptamer demonstrated specific and stable conjugation (Fig A.3). An increase in conjugated TBA was observed when the input TBA concentration

72
was increased from 1µM to 10µM. Positive staining was not observed on grafts with onlyypassively adsorbed TBA (both 1µM and10µM), which further confirmed that stable conjugation of TBA was achieved.
3.2 Animal Studies
Electrospun vascular grafts (untreated and TBA-modified) were implanted into rats for 1-month using a carotid artery superposition model. After 1-month, 1 of 3 (33%) of untreated grafts were patent, and 1 of 3 (33%) of TBA-modified grafts were patent. Although, it is not possible to reach a conclusion given the small sample size, it appears that there is no significant difference in patency among untreated and TBA-modified vascular grafts. H&E staining of explanted grafts does not show a significant difference among occluded and non-accluded grafts for both groups (Fig A.4).
Figure A.3: Fluorescent staining of immobilized thrombin binding aptamer (TBA).
4. Conclusions
This study demonstrated the ability to successfully conjugate a thrombin binding aptamer sequence to the surface of an electrospun vascular graft. Immunostaining for immobilized aptamer sequence revealed stable and specific attachment. However, preliminary in-vivo studies did not appear to show a significant improvement from the immobilization of the TBA sequence.

73
Figure A.4: H&E staining of TBA-modified vascular grafts 1-month after implantation.
Possible explanations may be related to the mechanism by which the TBA sequence neutralizes thrombin. It has recently been shown that TBA sequence used in this study, does not bind to the same thrombin exosite as heparin, hirudin or other similar anticoagulants. For this reason, it is possible that the TBA used does not irreversibly neutralize thrombin. Additionally, the TBA in this study may also have background levels of reactivity with other blood proteins, in addition to thrombin. Interactions with these proteins may have indirected triggered thrombosis and subsequently, graft occlusion. Potential Interactions with other blood proteins should be fully explored in the future. Lastly, other aptamers sequences with known thrombin binding ability should be included in these studies as well.

74
Impantation of a Nano/Micro-Fibrous Vascular Graft in a Large Animal Porcine Model
1.INTRODUCTION
To better approximate the human anatomy, in vivo vascular graft studies should eventually be performed using large animal models[232]. Porcine models have widely been used for large animal vascular graft studies[233]. In this study, a heparin modified electrospun vascular graft is implanted into the pig carotid artery for 4 weeks. Doppler Ultrasound is used to assess patency, after which, histological analysis is performed to assess luminal occlusion, graft cellularity and matrix organization. The results represent the start of a preliminary study to investigate the efficacy of heparin-modified electrospun vascular grafts using a large animal model.
2. METHODS & MATERIALS
2.1 Vascular Graft Fabrication
Electrospun vascular grafts were fabricated from the biodegradable polymers poly(L-Lactide) (PLLA; MW=100,000) (Lactel Absorbable Polymers, Pelham, AL) and poly(caprolactone) (PCL; MW=2,000) Polysciences, Warrington, PA). The polymers were combined to make a solution with final concentration of 19% (w/v) PLLA and 5% (w/v) PCL. The polymers were dissolved in the solvent 1,1,1,3,3-hexafluoro-2-propanol (HFIP) via sonication for 45 minutes or until fully dissolved. Electrospinning was performed to make vascular grafts for implantation as previously described[186]. Polymer solutions were delivered at a flow rate of 1ml/hr using a programmable syringe pump (Cole-Parmer, Vernon Hills, IL). A positive voltage of 12.5 kV was applied to a spinneret using a high voltage generator (Gamma High Voltage, Ormond Beach, FL). [188]. Fibers were collected onto a rotating stainless steel mandrel (speed = 100 rpm, diameter = 4.7 mm). Electrospinning was performed until the graft wall thickness reached 150 µm. Grafts were then removed from the mandrel and placed into a vacuum desiccator for 24 hours to remove any residual HFIP.
Covalent attachment of heparin was performed as described previously [188]by using 1-ethyl-3-(3 dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxysulfosuccinimide (sulfo-NHS) (Pierce Biotechnology, Rockford, IL) as crosslinkers and di-amino-poly(ethylene glycol) (di-NH2-PEG) (Sigma Aldrich, St Louis, MO) as a spacer. The density of surface carboxyl groups was increased by briefly hydrolyzing the material in sodium hydroxide (NaOH, 0.01N) for 10 minutes. Scaffolds were rinsed thoroughly in phosphate

75
buffered saline (PBS), followed by rinsing using deionized water. Scaffolds were then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10mg/ml sulfo-NHS and 20 mg/ml di-NH2-PEG at room temperature. Scaffolds were rinsed in PBS and then allowed to react for 3 hours in MES buffer (pH 5.5) containing 20 mg/ml EDC, 10 mg/ml sulfo-NHS and 20 mg/ml unfractionated heparin sodium salt (Sigma Aldrich, St. Louis, MO). Following heparin modification, grafts were thoroughly washed in PBS and remaining reactive sites were quenched using 10 mg/ml glycine in PBS for 30 minutes.
2.2 Porcine Model
Care and maintenance of animals were performed in accordance with the National Institutes of Health guidelines and with the rules of the UCSF committee on animal research. 1 pig weighing 50-55 kg was pre-medicated with ketamine (20 mg per kilogram of body weight; Parke-Davis, East Leigh, Hampshire, England), xylazine (2 mg/kg; Spectrum Chemicals and Laboratory Products, Gardera, Calif), and atropine (0.04 mg/kg; Abbott Laboratories, North Chicago, Ill). After intubation, the animal received a gas mixture of 1.5%–2.5% isoflurane (Abbott Laboratories) and 2–3 L/min of oxygen. A midline incision was made to expose the right common carotid artery (CCA). The right CCA was then clamped, ligated, and a 12-mm long heparin treated PLLA/5%PCL graft was sutured end-to-end by using uninterrupted 7-0 sutures.
Prior to removal, duplex ultrasonography was used to observe the patency grafts at 1-month. Grafts were explanted and immediately transected longitudinally to visualize the luminal surface. Graft segments were then snap frozen in OCT compound and later sectioned into 10µm slices for histological analysis.
2.3 Histological Analysis
Frozen sections were fixed in 4% PFA and blocked using 5% normal goat serum (Sigma Aldrich Inc.). Immunohistochemical staining was performed using an anti-CD31 primary antibody (from Abcam Inc.). DAPI was to used stain nuclei and to visualize the distribution of cells throughout the vascular graft wall. The density of cells within the vascular graft wall was computed using image J analysis software. Hemotoxylin & eosin staining was performed to visualize the distribution of cells and matrix. Native pig carotid arteries were used as a control for all staining.
3. RESULTS
A heparin-modified electrospun vascular graft was implanted into the pig carotid artery for 1-month. Immediately following surgery, the porous structure of the graft was immediately filled with red blood cells and other cellular components, and the color of the graft changed. The Uninterrupted suture

76
technique did not result in any bleeding or leakage at the anastomotic sites. Good blood flow was immediately observed at both the proximal and distal ends of the graft (Fig A.5 A). After 1-month implantation, significant scar tissue was observed surrounding the graft (Fig A.5 B). Following longitudinal transection, the luminal surface was very clean, with only few small streaks of blood showing.
Figure A.5: Implantation of heparin-modified vascular graft using a porcine model. A)Implanted vascular graft immediately following anastomosis and return of blood flow. B) Vascular graft and associated scar tissue 1-month following implantation. C) Lumnal surface of graft at 1-month.
After 1-month implantation, excellent patency was observed from ultrasonography. Excellent blood flow was seen at both proximal and distal ends of the grafts. A small but not substantial region of turbulent blood flow was observed near the proximal anastomosis (Fig A.6).

77
Figure A.6: Duplex Ultrasonography of implanted graft at 1-month. A) Longitudinal view showing excellent flow of blood through the graft. B) Axial view showing excellent blood leaving the distal end of the graft.
After 1-month, significant cellular infiltration into the graft wall was observed. The density of nuclei with the graft wall was similar to that observed in the native pig carotid artery(Fig A.7). Hematoxylin & eosin staining revealed dense layers of scar tissue surrounding the graft wall (Fig A.8). After 1-month, endothelium formation was not observed at either end of the graft, proximal or distal.
Figure A.7: Cellularzation of heparin-modified vascular graft at 1 month. A) Native porcine common carotid artery (CCA), B) Heparin-modified graft (Proximal End). C) Heparin-modified graft (Distal End). D)Quantification of cell density

78
Figure A.7: Tissue deposition around heparin-modified graft at 1-month. A) Native CCA. B)Heparin-modified graft (Distal). C)Heparin-modifed graft (Proximal).

79
Figure A.7: Endothelialization of heparin-modified graft at 1-month. A) Native CCA. B)Heparin-modified graft (Distal). C)Heparin-modifed graft (Proximal)

80
4. DISCUSSION
This preliminary study provides a foundation for future large animal studies of electrospun vascular grafts. After 1-month in vivo, the graft remained patent and showed excellent blood flow. Interestingly, a small turbulent region of blood flow was observed near the entrance of the graft. Attempts to minimize turbulence in this region should me made in the future, as changes in hemodynamic stresses may effect local cell behavior and remodeling. Dense regions of scar tissue were observed surrounding the graft after 1-month in vivo. This is a drastic contrast to the rodent studies discussed during the earlier chapters. Long-term studies should be performed to investigate whether the presence of the surrounding neotissue has an effect on graft patency. After 1-month, the graft showed excellent cell infiltration and was similar to the density observed in the native pig carotid. This result is also consistent results previously described in chapter 3, on heparin-modified grafts implanted using rat carotid models. It is also worth discussing the lack of graft endothelialization after 1-month. In rodent models, nearly complete endothelialization occurs in some heparin and untreated grafts. The lack of graft endothelialization in pigs is likely due to the larger graft area (i.e. further EC migration distance), and possibly due to a reduced mitogenecity of endothelial cells in pigs. This provides additional evidence that stimulation from biological signaling cues, such as VEGF or SDF-1α, are required to achieve full endothelialization. In addition to a larger sample size, future pig studies should include electrospun grafts with VEGF or SDF-1α modification.

81
References
[1] R. R. Atherosclerosis—an inflammatory disease. N Engl J Med.340:115.1999 [2] R. R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature.362:801.1993 [3] RY K, HJ S, K S, P B, AM S. The roles of tissue engineering and vascularisation in the development of micro-vascular networks: a review. Biomaterials.26:1857.2005 [4] N LH, N D, A M, S G, L dlF, T M. Technology insight: the evolution of tissue-engineered vascular grafts—from research to clinical practice. Nat Clin Pract Cardiovasc Med.4:389.2007 [5] M L, K L, A E, DL K. Vascularization strategies for tissue engineering. Tissue Eng Part B Rev.15:353.2009 [6] RM N, D S. Vascular tissue engineering. Annu Rev Biomed Eng.3:225.2001 [7] MS S, FJ S, JE M. Bioengineering challenges for heart valve tissue engineering. Annu Rev Biomed Eng.11:289.2009 [8] I. V. Heart valve tissue engineering. Circ Res.97:743.2005 [9] LE N, RS L. Advances in tissue engineering of blood vessels and other tissues. Transpl Immunol.5:303.1997 [10] FJ V, SK G, E A, S W-F, RH S. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg.3:104.1986 [11] B L, F L, D C, N R, K E, P T. Long-term (5 to 12 years) serial studies of internal mammary artery and saphenous vein coronary bypass grafts. J Thorac Cardiovasc Surg.89:248.1985 [12] T H, G A, J M, K B, P H, S S. Remodeling of acellular collagen graft into a physiologically responsive neovessel. Nat Biotechnol.17:1083.1999 [13] F A, JO B, R-G R, TC S, M T. Ruptured abdominal aortic aneurysm with aorto-caval fistula. J Vasc Surg.40:582.2004 [14] JB R, C M, JP N, E M, J C, G F. Prosthetic carotid bypass grafts for atherosclerotic lesions: a prospective study of 198 consecutive cases. Eur J Vasc Endovasc Surg.37:272.2009 [15] LP J, M L, JE F, OC R, BS J. Dacron or PTFE for above-knee femoropopliteal bypass: a multicenter randomised study. Eur J Vasc Endovasc Surg.34:44.2007 [16] Y. T. Vascular prostheses for aortocoronary bypass grafting: a review. Artif Organs.19:39.1995 [17] RE P, WD S, FJ V, LA S, RT L. Polytetrafluoroethylene bypasses to infrapopliteal arteries without cuffs or patches: a better option than amputation in patients without autologous vein. J Vasc Surg.23:347.1996 [18] RB C, DC J, GR N, TB C. Aorta-coronary bypass grafting with polytetrafluoroethylene conduits: early and late outcome in eight patients. J Thorac Cardiovasc Surg.94:132.1987 [19] A S, J L, TS L, M H. Coronary stents and chronic anticoagulation. Circulation.119:1682.2009

82
[20] DE D, ER E, P S, AR G, DA B. Neointimal thickening after stent delivery of paclitaxel: change in composition and arrest of growth over six months. J Am Coll Cardiol.36:2325.2000 [21] A F, PF H, S S, L C, FD K. Pathological analysis of local delivery of paclitaxel via a polymer-coated stent. Circulation.104:473.2001 [22] MC M, PW S, JE S, J F, E BH. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med.346:1773.2002 [23] JE S, MA C, A A, AS A, F F. Lack of neointimal proliferation after implantation of sirolimus-coated stents in human coronary arteries: a quantitative coronary angiography and three-dimensional intravascular ultrasound study. Circulation.103:192.2001 [24] T S, G K, S H, LR B, G L. Stent-based delivery of sirolimus reduces neointimal formation in a porcine coronary model. Circulation.104:1188.2001 [25] EP M, E S, E R, E C, AT O. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet.364:1519.2004 [26] R V, G G, A F, G M, N G. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation.109:701.2004 [27] S C, F R, E B. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation.89:635.1994 [28] M M, M A, R N, I G, L P. Fifteen-year experience with the mitral Carpentier-Edwards PERIMOUNT pericardial bioprosthesis. Ann Thorac Surg.71:S236.2001 [29] S. R. Choice of prosthetic heart valve for adult patients. J Am Coll Cardiol.41:893.2003 [30] KM C, DR P, J T. Formation of perfused, functional microvascular tubes in vitro. Microvasc Res.71:185.2006 [31] S K, J B, R K, S L, ER O. Silicon micromachining to tissue engineer branched vascular channels for liver fabrication. Tissue Eng.6:105.2000 [32] V M, T B, T T, G F, RR M. Organ printing: computer-aided jet-based 3D tissue engineering. Trends Biotechnol.21:157.2003 [33] HC O, B C, C C, C S, I P. Regeneration and orthotopic transplantation of a bioartificial lung. Nat Med.16:927.2010 [34] HC O, TS M, SK G, LD B, SM K. Perfusion-decellularized matrix: using nature's platform to engineer a bioartificial heart. Nat Med.14:213.2008 [35] TH P, EA C, L Z, EJ L, L G. Tissue-engineered lungs for in vivo implantation. Science.329:538.2010 [36] BE U, A S-G, H Y, ML I, MA G. Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix. Nat Med.16:814.2010 [37] X C, AS A, CM G, CK G, AJ P. Prevascularization of a fibrin-based tissue construct accelerates the formation of functional anastomosis with host vasculature. Tissue Eng Part A.15:1363.2009 [38] ZM. R. Role of von Willebrand factor in platelet thrombus formation. Ann Med.32:2.2000

83
[39] ZM. R. Mechanisms initiating platelet thrombus formation. Thromb Haemost.78:611.1997 [40] N. M. Triggers, targets and treatments for thrombosis. Nature.451:914.2008 [41] OJT M, Y Z, N A, LM M, D S. Evaluation of the role of platelet integrins in fibronectin-dependent spreading and adhesion. J Thromb Haemost.2:1823.2004 [42] JS B, BW B, PC B. The structure and function of platelet integrins. J Thromb Haemost.7:200.2009 [43] D B, H D, J V. Platelet actuation. Blood Rev.9:143.1995 [44] ZM. R. Platelet adhesion under flow. Microcirculation.16:58.2009 [45] MB G, MV S. Biomaterial-associated thrombosis: roles of coagulation factors, complement, platelets and leukocytes. Biomaterials.25:5681.2004 [46] EW D, K F, W K. The coagulation cascade: initiation, maintenance, and regulation. Biochemistry.30:10363.1991 [47] Sherwood L. Human Physiology:From Cells to Systems. 6 ed: Thompson Brooks/Cole; 2007. [48] B F, BC F. Mechanisms of thrombus formation. N Engl J Med.359:938.2008 [49] K P, F M, H P. Morphological characterization of surface-induced platelet activation. Biomaterials.11:24.1990 [50] AH. S. Contact activation: a revision. Thromb Haemost.78:101.1997 [51] AH. S. Plasma kallikrein/kinin system: a revised hypothesis for its activation and its physiologic contributions. Curr Opin Hematol.7:261.2000 [52] J. B. Role of factor XII in thrombin generation and fibrinolysis during cardiopulmonary bypass. Lancet.344:1192.1994 [53] JN W, KM S, SM S, D G. Localization of tissue factor in the normal vessel wall and in the atherosclerotic plaque. Proc Natl Acad Sci USA.86:2839.1989 [54] SR. C. Thrombin signaling and protease-activated receptors. Nature.407:258.2000 [55] PL G, U R, B B, D K, M R. Blood-borne tissue factor: another view of thrombosis. Proc Natl Acad Sci USA.96:2311.1999 [56] C. M. Endothelial cell functions. J Cell Physiol.196:430.2003 [57] KK W, P T. Role of endothelium in thrombosis and hemostasis. Annu Rev Med.47:315.1996 [58] VW vH. The endothelium: vascular control of haemostasis. Eur J Obstet Gynecol Reprod Biol.95:198.2001 [59] M B, R K, M K, MT H, J S. Biology of the syndecans: a family of transmembrane heparan sulfate proteoglycans. Annu Rev Cell Biol.8:365.1992 [60] M B, M G, PW P, O R, ML F. Functions of cell surface heparan sulfate proteoglycans. Annu Rev Biochem.68:729.1999 [61] DJ S-K, S K, JS M, GL F, CT E. The endothelial cell protein C receptor augments protein C activation by the thrombin-thrombomodulin complex. Proc Natl Acad Sci USA.93:10212.1996 [62] GJ. B. Tissue factor pathway inhibitor. Thromb Haemost.74:90.1995 [63] Hackeng TM, Maurissen LF, Castoldi E, Rosing J. Regulation of TFPI function by protein S. J Thromb Haemost.7 Suppl 1:165-8.2009

84
[64] TM H, KM S, G T, J R. Protein S stimulates inhibition of the tissue factor pathway by tissue factor pathway inhibitor. Proc Natl Acad Sci USA.103:3106.2006 [65] LC B, TJ M, RG R, FE P. Prostacyclin increases cyclic AMP levels and adenylate cyclase activity in platelets. Nature.267:850.1977 [66] JC dG, JD B, S M, RM P, PG dG, JJ S. Nitric oxide functions as an inhibitor of platelet adhesion under flow conditions. Circulation.85:2284.1992 [67] MW R, P V, G W, N F, S M. Platelet adhesion to human vascular endothelium is modulated by constitutive and cytokine induced nitric oxide. Cardiovasc Res.27:1380.1993 [68] HL K, JA F. Role of cytoskeleton in shear stress-induced endothelial nitric oxide production. Am J Physiol.273:H347.1997 [69] JD P, JS C, JL G. Metabolism of adenine nucleotides by ectoenzymes of vascular endothelial and smooth-muscle cells in culture. Biochem J.190:421.1980 [70] S W, JM T, ER D. The structure and function of the endothelial glycocalyx layer. Annu Rev Biomed Eng.9:121.2007 [71] CK H, Y Z, GY Y, WL Y, BS H. Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proc Natl Acad Sci USA.104:11915.2007 [72] S. C. Molecular and mechanical bases of focal lipid accumulation in arterial wall. Prog Biophys Mol Biol.83:131.2003 [73] JJ M, M M, S P, L L, JL G, S L. Role of cell surface heparan sulfate proteoglycans in endothelial cell migration and mechanotransduction. J Cell Physiol.203:166.2005 [74] S W, X Z, Y H, H V, SC C. Mechanotransduction and flow across the endothelial glycocalyx. Proc Natl Acad Sci USA.100:7988.2003 [75] JA F, JR K, K A, Z P, RO D, JM T. Heparan sulfate proteoglycan is a mechanosensor on endothelial cells. Circ Res.93:e136.2003 [76] H M, O K, M N, S U, O M. Differential role of components of the fibrinolytic system in the formation and removal of thrombus induced by endothelial injury. Thromb Haemost.81:601.1999 [77] WP F, N G, M S. Vascular functions of the plasminogen activation system. Arterioscler Thromb Vasc Biol.27:1231.2007 [78] J S, MS S, MR K, GM B, EF B. Increased type 1 plasminogen activator inhibitor gene expression in atherosclerotic human arteries. Proc Natl Acad Sci USA.89:6998.1992 [79] K B, A N, RD G, V M, N B. Absence of host plasminogen activator inhibitor 1 prevents cancer invasion and vascularization. Nat Med.4:923.1998 [80] WP. F. Plasminogen activator inhibitor 1, fibrin, and the vascular response to injury. Trends Cardiovasc Med.14:196.2004 [81] VW vH, EA vdB, W F, G D. Tumor necrosis factor induces the production of urokinase-type plasminogen activator by human endothelial cells. Blood.75:1991.1990 [82] T O, G K. Urokinase immobilized on medical polymeric materials: fundamental and clinical studies. Artif Organs.4:58.1980

85
[83] S W, Y S, T T, T M, T H. The in vitro and in vivo behavior of urokinase immobilized onto collagen-synthetic polymer composite material. J Biomed Mater Res.15:553.1981 [84] E H, K K, G S. The molecular-weight dependence of the rate-enhancing effect of heparin on the inhibition of thrombin, factor Xa, factor IXa, factor XIa, factor XIIa and kallikrein by antithrombin. Biochem J.193:395.1981 [85] VL G, JD W, RC D. Heparin bonding on colloidal graphite surfaces. Science.142:1297.1963 [86] EF R, MM F, AM R, B K. Heparin bonding increases patency of long microvascular prostheses. Plast Reconstr Surg.101:142.1998 [87] BH W, R R, E T, S G, T S. Improvement of patency rate in heparin-coated small synthetic vascular grafts. Circulation.98:II319.1998 [88] K P, HS S, MK D, NL E. In vitro and in vivo studies of PEO-grafted blood-contacting cardiovascular prostheses. J Biomater Sci Polym Ed.11:1121.2000 [89] S T, E M, E S, J L. Activity toward thrombin-antithrombin of heparin immobilized on two hydrogels. Biomaterials.10:11.1989 [90] C N, KD P, DW G, HA J, T O. In vivo nonthrombogenicity of heparin immobilized polymer surfaces. ASAIO Trans.36:M168.1990 [91] O L, R L, P O. A new non-thrombogenic surface prepared by selective covalent binding of heparin via a modified reducing terminal residue. Biomater Med Devices Artif Organs.11:161.1983 [92] P O, J S, TE M, J R. On the blood compatibility of end-point immobilized heparin. J Biomater Sci Polym Ed.11:1261.2000 [93] PA H, HM vB, HU E, SH H, PA A. Reduction in thrombotic events with heparin-coated Palmaz-Schatz stents in normal porcine coronary arteries. Circulation.93:423.1996 [94] PW S, H E, W vdG, AC L, F K. Heparin-coated Palmaz-Schatz stents in human coronary arteries: early outcome of the Benestent-II Pilot Study. Circulation.93:412.1996 [95] DW G, T O, SW K, DG C, BD R. Poly(dimethylsiloxane)-poly(ethylene oxide)-heparin block copolymers. III: Surface and bulk compositional differences. J Biomed Mater Res.24:547.1990 [96] KP W, S B, M B, J C. Infrainguinal ePTFE vascular graft with bioactive surface heparin bonding: first clinical results. J Cardiovasc Surg.46:425.2005 [97] C D, C M. Heparin-bonded Dacron or polytetrafluoroethylene for femoropopliteal bypass: five-year results of a prospective randomized multicenter clinical trial. J Vasc Surg.40:924.2004 [98] WJ F, MA C, HW C, BA K, MA S. Solution structure of the heparin-binding domain of vascular endothelial growth factor. Structure.6:637.1998 [99] G N, T C, S G, Z P. Vascular endothelial growth factor (VEGF) and its receptors. FASEB J.13:9.1999 [100] S. S-E. Development of fibrin derivatives for controlled release of heparin-binding growth factors. J Control Release.65:389.2000 [101] De Scheerder I, Wang K, Wilczek K, Meuleman D, Van Amsterdam R. Experimental study of thrombogenicity and foreign body reaction induced by heparin-coated coronary stents. Circulation.95:1549-53.1997

86
[102] SC G, HC Y, G C, P A-S, MM C. Intense inflammatory reaction to heparin polymer coated intravascular Palmaz stents in porcine arteries compared to uncoated Palmaz stents. Cardiovasc Interv Radiol.26:158.2003 [103] MG G, JP P, J R, H G, W B. Crystal structure of the thrombin-hirudin complex: a novel mode of serine protease inhibition. EMBO J.9:2361.1990 [104] T S, M R, J D. Mechanism of the inhibition of α-thrombin by hirudin-derived fragments hirudin(1-47) and hirudin(45-65). Eur J Biochem.195:251.1991 [105] B S, P R, T G. Covalent immobilization of hirudin improves the haemocompatibility of polylactide-polyglycolide in vitro. Biomaterials.18:1495.1997 [106] MD P, SA B, MJ B, WC Q, FW L. Covalent linkage of recombinant hirudin to poly(ethylene terephthalate) (Dacron): creation of a novel antithrombin surface. Biomaterials.18:755.1997 [107] MC W, MD P, EM R, MA C, FW L, WC Q. In vivo assessment of a novel Dacron surface with covalently bound recombinant hirudin. Cardiovasc Pathol.8:153.1999 [108] J L, W P, D K, H-G G, H H. Immobilization of the thrombin inhibitor r-hirudin conserving its biological activity. J Mater Sci Mater Med.12:807.2001 [109] CK H, N D, RRR J, R L, D S. Antithrombogenic modification of small-diameter microfibrous vascular grafts. Arterioscler Thromb Vasc Biol.30:1621.2010 [110] E A, I H, C B, K P, D P. Inhibition of neointima formation after experimental coronary artery stenting: a new biodegradable stent coating releasing hirudin and the prostacyclin analogue iloprost. Circulation.101:1453.2000 [111] J L, D K, W P, H H. Bioactive immobilization of r-hirudin on CVD-coated metallic implant devices. Biomaterials.22:817.2001 [112] M DN, S M, HR B. Direct thrombin inhibitors. N Engl J Med.353:1028.2005 [113] JM M, P B, J J, KL R, JW F. Design and characterization of hirulogs: a novel class of bivalent peptide inhibitors of thrombin. Biochemistry.29:7095.1990 [114] W L, A K, G G, J T, L L. A novel nucleotide-based thrombin inhibitor inhibits clot-bound thrombin and reduces arterial platelet thrombus formation. Blood.83:677.1994 [115] B P, L M, A R, C G. Stability and binding properties of a modified thrombin binding aptamer. Biophys J.94:562.2008 [116] A K, Y A, M Y, T A, I M, M A. In vivo and ex vivo evaluation of the antithrombogenicity of human thrombomodulin immobilized biomaterials. ASAIO J.41:M369.1995 [117] P-Y T, SS R, X-L S, EL C. Membrane-mimetic films containing thrombomodulin and heparin inhibit tissue factor-induced thrombin generation in a flow model. Biomaterials.27:2637.2006 [118] A K, Y U, N F, E Y, I M, M A. Immobilization of human thrombomodulin onto poly(ether urethane urea) for developing antithrombogenic blood-contacting materials. Biomaterials.15:848.1994 [119] J L, MJ S, PR N, GM H, M I. Immobilization of human thrombomodulin to expanded polytetrafluoroethylene. J Surg Res.105:200.2002

87
[120] G W, J-M L, G H, MH E, MJ R, BS C. Inhibition of experimental neointimal hyperplasia by recombinant human thrombomodulin coated ePTFE stent grafts. J Vasc Surg.47:608.2008 [121] LB S, J U, S M, H T, K O, N K. Pretreatment of a Dacron graft with tissue factor pathway inhibitor decreases thrombogenicity and neointimal thickness: a preliminary animal study. ASAIO J.47:325.2001 [122] PG W, M X, X T, X W, Z W. Nitric oxide donors: chemical activities and biological applications. Chem Rev.102:1091.2002 [123] LK K, JE S. Nitrogen-based diazeniumdiolates: versatile nitric oxide–releasing compounds for biomedical research and potential clinical applications. J Chem Educ.79:1427.2002 [124] LJ I, C N, J L. Nitric oxide donors and cardiovascular agents modulating the bioactivity of nitric oxide: an overview. Circ Res.90:21.2002 [125] DJ S, D C, S P, ML S, JA H. Nitric oxide–releasing polymers containing the [N(O)NO]− group. J Med Chem.39:1148.1996 [126] H-W J, LJ T, JL W. Nitric oxide–producing polyurethanes. Biomacromolecules.6:838.2005 [127] WR G, GH W, TA H, AS H. Protein adsorption to poly(ethylene oxide) surfaces. J Biomed Mater Res.25:1547.1991 [128] P H, M G, R D, GM W, PE L. Molecular conformation in oligo(ethylene glycol)-terminated self-assembled monolayers on gold and silver surfaces determines their ability to resist protein adsorption. J Phys Chem B.102:426.1998 [129] S S, V P, E M. Poly(ethylene oxide) grafted to silicon surfaces: grafting density and protein adsorption. Macromolecules.31:5059.1998 [130] GM B, MJ G, R W, DJ W. In vitro blood compatibility of surface-modified polyurethanes. Biomaterials.19:1151.1998 [131] CR D, P P, PC J, EJ B, AJ R, WR W. Molecular barriers to biomaterial thrombosis by modification of surface proteins with polyethylene glycol. Biomaterials.19:1885.1998 [132] DK H, KB L, KD P, CS K, SY J. In vivo canine studies of a Sinkhole valve and vascular graft coated with biocompatible PU-PEO-SO3. ASAIO J.39:M537.1993 [133] C N, T O, HA J, KD P, SF M. Blood compatibility of PEO grafted polyurethane and HEMA/styrene block copolymer surfaces. J Biomed Mater Res.24:1151.1990 [134] J. H. Pharmacologic modification of materials. Cardiovasc Pathol.2:121.1993 [135] H K, T M. Biocompatible coatings for luminal and outer surfaces of small-caliber artificial grafts. J Biomed Mater Res.30:321.1996 [136] TW C, KS M. Regulation of polyurethane hemocompatibility and endothelialization by tethered hyaluronic acid oligosaccharides. Biomaterials.30:5341.2009 [137] SW J, KM F, JM C, RP A, SS R. Fabrication of a phospholipid membrane-mimetic film on the luminal surface of an ePTFE vascular graft. Biomaterials.27:3473.2006

88
[138] K K, CP S. Cell mimetic lateral stabilization of outer cell mimetic bilayer on polymer surfaces by peptide bonding and their blood compatibility. J Biomed Mater Res A.79:23.2006 [139] AL L, JD F, S S, JD R, BJ H. Long-term stability of a coronary stent coating post-implantation. J Biomed Mater Res.63:699.2002 [140] E A, I H, K A, S A, K O. Effects of stent coating on platelets and endothelial cells after intracoronary stent implantation. Clin Cardiol.24:159.2001 [141] C C, AB L, JC O, B N, EJ C. Phosphorylcholine coating of ePTFE grafts reduces neointimal hyperplasia in canine model. Ann Vasc Surg.11:74.1997 [142] R C, L G, S S, R V, AJ C. Stent-based delivery of ABT-578 via a phosphorylcholine surface coating reduces neointimal formation in the porcine coronary model. Catheter Cardiovasc Interv.65:227.2005 [143] KK K, KA R, NA C, J C, SJ P, JE N. Phosphorylcholine-coated metallic stents in rabbit iliac and porcine coronary arteries. Scand Cardiovasc J.32:261.1998 [144] N M, J G, L S, DC C, DC C, CM H. Phosphorylcholine-coated stents in porcine coronary arteries: in vivo assessment of biocompatibility. J Invasive Cardiol.13:193.2001 [145] H Z, P B, T C, JB S, X F. Clinical experience with a new biocompatible phosphorylcholine-coated coronary stent. J Invasive Cardiol.11:608.1999 [146] N LH, N D, G K, B V, P K. Human tissue-engineered blood vessels for adult arterial revascularization. Nat Med.12:361.2006 [147] LE N, J G, WM A, KK H, S H. Functional arteries grown in vitro. Science.284:489.1999 [148] CB W, E B. A blood vessel model constructed from collagen and cultured vascular cells. Science.231:397.1986 [149] KP W, G S, S K, A H. Improved endothelial cell attachment on ePTFE vascular grafts pretreated with synthetic RGD-containing peptides. Eur J Vasc Endovasc Surg.12:321.1996 [150] M H, J S, M D, J G, R C. Endothelial seeding of polytetrafluoroethylene femoral popliteal bypasses: the failure of low-density seeding to improve patency. J Vasc Surg.20:650.1994 [151] CG G, R S, S C. Shear stress induces spatial reorganization of the endothelial cell cytoskeleton. Cell Motil Cytoskelet.40:317.1998 [152] S L, M K, YL H, S J, DD S. Fluid shear stress activation of focal adhesion kinase: linking to mitogen-activated protein kinases. J Biol Chem.272:30455.1997 [153] JG M, JC S, H S, M G, JA H. Enhanced endothelial cell retention on shear-stressed synthetic vascular grafts precoated with RGD-cross-linked fibrin. Tissue Eng.11:887.2005 [154] M B, D M, HJ S, B F, G H. Shear-stress preconditioning and tissue-engineering-based paradigms for generating arterial substitutes. Biotechnol Appl Biochem.39:151.2004 [155] MJ O, BJ B. Shear stress–conditioned, endothelial cell–seeded vascular grafts: improved cell adherence in response to in vitro shear stress. Surgery.117:334.1995

89
[156] M P, K T, B M, M G, G M. Selective recognition of cyclic RGD peptides of NMR defined conformation by alpha αIIbβ3, αVβ3, and α5β1 integrins. J Biol Chem.269:20233.1994 [157] S M, J H. Vascular endothelial cell adhesion and spreading promoted by the peptide REDV of the IIICS region of plasma fibronectin is mediated by integrin α4β1. J Biol Chem.267:14019.1992 [158] J H, R R, R T, S B. Fibronectin peptides mediate HMEC adhesion to porcine-derived extracellular matrix. Biomaterials.23:1841.2002 [159] LJ T, P Y, H-W J, JL W. Nitric oxide–releasing polyurethane-PEG copolymer containing the YIGSR peptide promotes endothelialization with decreased platelet adhesion. J Biomed Mater Res B.84:108.2008 [160] P Z, D B, P H. Prosthetic vascular grafts: wrong models, wrong questions and no healing. Biomaterials.28:5009.2007 [161] S L, S B, YL H, YT S, YS L. Effects of morphological patterning on endothelial cell migration. Biorheology.38:101.2001 [162] RG T, F H, NF H, D L, S L. Regulation of vascular smooth muscle cells by micropatterning. Biochem Biophys Res Commun.307:883.2003 [163] P U, A P, M L, P P, SJ S. Micropatterning of three-dimensional electrospun polyurethane vascular grafts. Acta Biomater.6:4229.2010 [164] Y S, G W, L C, H L, P Y. Investigation of surface endothelialization on biomedical nitinol (NiTi) alloy: effects of surface micropatterning combined with plasma nanocoatings. Acta Biomater.5:3593.2009 [165] Q S, V B, M H-DW, LR S. Utilizing granulocyte colony-stimulating factor to enhance vascular graft endothelialization from circulating blood cells. Ann Vasc Surg.16:314.2002 [166] K S, H L, K D, T S, A G. Platelet-derived stromal cell–derived factor-1 regulates adhesion and promotes differentiation of human CD34+ cells to endothelial progenitor cells. Circulation.117:206.2008 [167] K-i H, M I, K O, S I, Q Z. Gene transfer of stromal cell–derived factor-1α enhances ischemic vasculogenesis and angiogenesis via vascular endothelial growth factor/endothelial nitric oxide synthase–related pathway: next-generation chemokine therapy for therapeutic neovascularization. Circulation.109:2454.2004 [168] C K, H M, T T, R G, O T. Vascular endothelial growth factor165 gene transfer augments circulating endothelial progenitor cells in human subjects. Circ Res.86:1198.2000 [169] C K, H T, B L, PR V, JM I. VEGF gene transfer mobilizes endothelial progenitor cells in patients with inoperable coronary disease. Ann Thorac Surg.70:829.2000 [170] PE S, PWM F, RD W, DJ S, MJB K, S V. Endothelial progenitor cells: new hope for a broken heart. Circulation.107:3093.2003 [171] S D, A A, M V, C M-R, K A. HMG-CoA reductase inhibitors (statins) increase endothelial progenitor cells via the PI 3-kinase/Akt pathway. J Clin Investig.108:391.2001 [172] JI R, JMM H, HJM V, E V, MM N. In vivo cell seeding with anti-CD34 antibodies successfully accelerates endothelialization but stimulates intimal

90
hyperplasia in porcine arteriovenous expanded polytetrafluoroethylene grafts. Circulation.112:12.2005 [173] D. S. Smooth muscle progenitor cells in human blood. Circulation.106:1199.2002 [174] HP W, M A-A, G Z. Endothelial progenitor cell capture stents—hype or hope? Int J Cardiol.145:115.2009 [175] J H, A P, M H, J G, T R. Immobilized DNA aptamers used as potent attractors for porcine endothelial precursor cells. J Biomed Mater Res A.84:614.2008 [176] MP B, A D, N H, JD R, GN N. Tissue-engineered vascular grafts demonstrate evidence of growth and development when implanted in a juvenile animal model. Ann Surg.248:370.2008 [177] NF H, S L. Mesenchymal stem cells for vascular regeneration. Regen Med.3:877.2008 [178] Huynh T, Abraham G, Murray J, Brockbank K, Hagen P, Sullivan S. Remodeling of acellular collagen graft into a physiologically responsive neovessel. Nature Biotechnology.17:1083-6.1999 [179] Nerem RM, Seliktar D. VASCULAR TISSUE ENGINEERING. Annual Review of Biomedical Engineering.3:225-43.2001 [180] Tomizawa Y. Vascular prostheses for aortocoronary bypass grafting: a review. Artificial organs.19:39-45.1995 [181] Weinberg C, Bell E. A blood vessel model constructed from collagen and cultured vascular cells. Science.1986 [182] L'Heureux N, Dusserre N, Konig G, Victor B, Keire P, Wight TN, et al. Human tissue-engineered blood vessels for adult arterial revascularization. Nat Med.12:361-5.2006 [183] Gong Z, Niklason LE. Small-diameter human vessel wall engineered from bone marrow-derived mesenchymal stem cells (hMSCs). The FASEB Journal.22:1635-48.2008 [184] Hashi CK, Zhu Y, Yang GY, Young WL, Hsiao BS, Wang K, et al. Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proceedings of the National Academy of Sciences.104:11915.2007 [185] Kurpinski KT, Stephenson JT, Janairo RRR, Lee H, Li S. The effect of fiber alignment and heparin coating on cell infiltration into nanofibrous PLLA scaffolds. Biomaterials.31:3536-42.2010 [186] Patel S, Kurpinski K, Quigley R, Gao H, Hsiao BS, Poo MM, et al. Bioactive nanofibers: synergistic effects of nanotopography and chemical signaling on cell guidance. Nano Lett.7:2122-8.2007 [187] Barrera DA, Zylstra E, Lansbury PT, Langer R. Copolymerization and degradation of poly(lactic acid-co-lysine). Macromolecules.28:425-32.1995 [188] Hashi CK, Derugin N, Janairo RRR, Lee R, Schultz D, Lotz J, et al. Antithrombogenic modification of small-diameter microfibrous vascular grafts. Arteriosclerosis, Thrombosis, and Vascular Biology.30:1621-7.2010

91
[189] Smith PK, Mallia AK, Hermanson GT. Colorimetric method for the assay of heparin content in immobilized heparin preparations. Anal Biochem.109:466-73.1980 [190] Chandler WL, Solomon DD, Hu CB, Schmer G. Estimation of surface-bound heparin activity: a comparison of methods. J Biomed Mater Res.22:497-508.1988 [191] Catanese J, Cooke D, Maas C, Pruitt L. Mechanical properties of medical grade expanded polytetrafluoroethylene: The effects of internodal distance, density, and displacement rate. Journal of Biomedical Materials Research.48:187-92.1999 [192] Fung YC. Biomechanics Circulation. 2nd ed: Springer; 1996. [193] Pike DB, Cai S, Pomraning KR, Firpo MA, Fisher RJ, Shu XZ, et al. Heparin-regulated release of growth factors in vitro and angiogenic response in vivo to implanted hyaluronan hydrogels containing VEGF and bFGF. Biomaterials.27:5242-51.2006 [194] Sakiyama-Elbert S. Development of fibrin derivatives for controlled release of heparin-binding growth factors. Journal of Controlled Release.65:389-402.2000 [195] Li S, Henry JJD. Nonthrombogenic Approaches to Cardiovascular Bioengineering. Annual Review of Biomedical Engineering.13:451-75.2011 [196] Walpoth BH, Zammaretti P, Cikirikcioglu M, Khabiri E, Djebaili MK, Pache J-C, et al. Enhanced intimal thickening of expanded polytetrafluoroethylene grafts coated with fibrin or fibrin-releasing vascular endothelial growth factor in the pig carotid artery interposition model. J Thorac Cardiovasc Surg.133:1163-70.2007 [197] Luong-Van E, Grøndahl L, Chua KN, Leong KW, Nurcombe V, Cool SM. Controlled release of heparin from poly(epsilon-caprolactone) electrospun fibers. Biomaterials.27:2042-50.2006 [198] Hu J, Sun X, Ma H, Xie C, Chen YE, Ma PX. Porous nanofibrous PLLA scaffolds for vascular tissue engineering. Biomaterials.31:7971-7.2010 [199] Kang Ss Fau - Gosselin C, Gosselin C Fau - Ren D, Ren D Fau - Greisler HP, Greisler HP. Selective stimulation of endothelial cell proliferation with inhibition of smooth muscle cell proliferation by fibroblast growth factor-1 plus heparin delivered from fibrin glue suspensions. [200] Weatherford DA, Sackman JE, Reddick TT, Freeman MB, Stevens SL, Goldman MH. Vascular endothelial growth factor and heparin in a biologic glue promotes human aortic endothelial cell proliferation with aortic smooth muscle cell inhibition. Surgery.120:433-9.1996 [201] de Valence S, Tille JC, Mugnai D, Mrowczynski W, Gurny R, Möller M, et al. Long term performance of polycaprolactone vascular grafts in a rat abdominal aorta replacement model. Biomaterials.33:38-47.2012 [202] Davies N, Dobner S, Bezuidenhout D, Schmidt C, Beck M, Zisch AH, et al. The dosage dependence of VEGF stimulation on scaffold neovascularisation. Biomaterials.29:3531-8.2008 [203] SP. J. The growing complexity of platelet aggregation. Blood.109:5087.2007

92
[204] S Y, HM B. Nuclear reprogramming to a pluripotent state by three approaches. Nature.465:704.2010 [205] JH H, K S, R J. Pluripotency and cellular reprogramming: facts, hypotheses, unresolved issues. Cell.143:508.2010 [206] MEMBERS WG, Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, et al. Heart Disease and Stroke Statistics—2009 Update: A Report From the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation.119:e21-e181.2009 [207] Christman KL, Lee RJ. Biomaterials for the Treatment of Myocardial Infarction. Journal of the American College of Cardiology.48:907-13.2006 [208] Hayakawa K, Takemura G, Kanoh M, Li Y, Koda M, Kawase Y, et al. Inhibition of Granulation Tissue Cell Apoptosis During the Subacute Stage of Myocardial Infarction Improves Cardiac Remodeling and Dysfunction at the Chronic Stage. Circulation.108:104-9.2003 [209] Pfeffer MD, Ph.D, Marc A. Left ventricular remodeling after acute myocardial infarction. Annual Review of Medicine.46:455-66.1995 [210] Niknejad H, Peirovi H, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian A. Properties of the amniotic membrane for potential use in tissue engineering. European Cells & Materials.15:88-99.2008 [211] Shimmura S, Shimazaki J, Ohashi Y, Tsubota K. Antiinflammatory effects of amniotic membrane transplantation in ocular surface disorders. Cornea.20:408-13.2001 [212] Talmi Y, Sigler L, Inge E, Finklestein Y, Zohar Y. Antibacterial properties of human amniotic membranes. Placenta.12:285-8.1991 [213] Dua HS, Gomes JAP, King AJ, Maharajan VS. The amniotic membrane in ophthalmology. Survey of Ophthalmology.49:51-77.2004 [214] Tosi G, Massaro-Giordano M, Caporossi A, Toti P. Amniotic membrane transplantation in ocular surface disorders. Journal of Cellular Physiology.202:849-51.2005 [215] Farndale RW, Buttle DJ, Barrett AJ. Improved quantitation and discrimination of sulphated glycosaminoglycans by use of dimethylmethylene blue. Biochim Biophys Acta.883:173-7.1986 [216] Li S, Kim M, Hu Y-L, Jalali S, Schlaepfer DD, Hunter T, et al. Fluid Shear Stress Activation of Focal Adhesion Kinase: LINKING TO MITOGEN-ACTIVATED PROTEIN KINASES. Journal of Biological Chemistry.272:30455-62.1997 [217] Christman K, Fok H, Sievers R, Fang Q, Lee R. Fibrin glue alone and skeletal myoblasts in a fibrin scaffold preserve cardiac function after myocardial infarction. Tissue Engineering.10:403-9.2004 [218] Huang NF, Sievers RE, Park JS, Fang Q, Li S, Lee RJ. A rodent model of myocardial infarction for testing the efficacy of cells and polymers for myocardial reconstruction. Nat Protocols.1:1596-609.2006 [219] Isenberg B, Williams C, Tranquillo R. Small-diameter artificial arteries engineered in vitro. Circulation Research.2006 [220] Li S, Henry JJ. Nonthrombogenic approaches to cardiovascular bioengineering. Annu Rev Biomed Eng.13:451-75.2011

93
[221] Olausson M, Patil PB, Kuna VK, Chougule P, Hernandez N, Methe K, et al. Transplantation of an allogeneic vein bioengineered with autologous stem cells: a proof-of-concept study. Lancet.380:230-7.2012 [222] Roh JD, Sawh-Martinez R, Brennan MP, Jay SM, Devine L, Rao DA, et al. Tissue-engineered vascular grafts transform into mature blood vessels via an inflammation-mediated process of vascular remodeling. Proceedings of the National Academy of Sciences of the United States of America.107:4669-74.2010 [223] Shin'oka T, Matsumura G, Hibino N, Naito Y, Watanabe M, Konuma T, et al. Midterm clinical result of tissue-engineered vascular autografts seeded with autologous bone marrow cells. J Thorac Cardiovasc Surg.129:1330-8.2005 [224] Hirschi KK, Goodell MA. Hematopoietic, vascular and cardiac fates of bone marrow-derived stem cells. Gene Ther.9:648-52.2002 [225] Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med.9:702-12.2003 [226] Asahara T, Takahashi T, Masuda H, Kalka C, Chen D, Iwaguro H, et al. VEGF contributes to postnatal neovascularization by mobilizing bone marrow-derived endothelial progenitor cells. EMBO J.18:3964-72.1999 [227] Landmesser U, Engberding N, Bahlmann FH, Schaefer A, Wiencke A, Heineke A, et al. Statin-induced improvement of endothelial progenitor cell mobilization, myocardial neovascularization, left ventricular function, and survival after experimental myocardial infarction requires endothelial nitric oxide synthase. Circulation.110:1933-9.2004 [228] De Falco E, Porcelli D, Torella AR, Straino S, Iachininoto MG, Orlandi A, et al. SDF-1 involvement in endothelial phenotype and ischemia-induced recruitment of bone marrow progenitor cells. Blood.104:3472-82.2004 [229] Yamaguchi J, Kusano KF, Masuo O, Kawamoto A, Silver M, Murasawa S, et al. Stromal cell-derived factor-1 effects on ex vivo expanded endothelial progenitor cell recruitment for ischemic neovascularization. Circulation.107:1322-8.2003 [230] Hermann T, Patel DJ. Adaptive recognition by nucleic acid aptamers. Science.287:820-5.2000 [231] Patel DJ, Suri AK, Jiang F, Jiang L, Fan P, Kumar RA, et al. Structure, recognition and adaptive binding in RNA aptamer complexes. J Mol Biol.272:645-64.1997 [232] Rashid ST, Salacinski HJ, Hamilton G, Seifalian AM. The use of animal models in developing the discipline of cardiovascular tissue engineering: a review. Biomaterials.25:1627-37.2004 [233] Narayanaswamy M, Wright KC, Kandarpa K. Animal models for atherosclerosis, restenosis, and endovascular graft research. Journal of vascular and interventional radiology : JVIR.11:5-17.2000












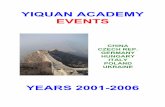


![INDEX.* [digitalassets.lib.berkeley.edu]digitalassets.lib.berkeley.edu/anthpubs/ucb/text/ucp006...Buckingham's island, 206. Bucknell ranch, 188. Buckner creek, 143, 259; moun-tains,](https://static.fdocuments.net/doc/165x107/5afedb927f8b9a864d8f89bb/index-s-island-206-bucknell-ranch-188-buckner-creek-143-259-moun-tains.jpg)