Groin Flap Design and Versatility - Semantic Scholar · essary. During microvascular anastomosis,...
8
Groin Flap Design and Versatility David C. C. Chuang, M.D., L. H. Colony, M.D., Iq[. C. Chert, M.D., and F. C. Wei, M.D. Taipei, Taiwan,and East Lansing, Mich. The groin flap is a reliable and well-established recon- structive option for pedicled or free-tissue transfer. Con- cern regardingits variable vascular origin and caliber has limited its use. To overcome this, a simplified guideline based on the transverse diameter of the patient’s index and long fingers at the distal interphalangeal level has been developed. Thus "rule of two finger widths" posi- tions the origin of the vascular pedicle from the femoral vessels two,finger widths below the inguinal ligament, the upper flap border two finger widths above the in- guinal ligament, the lower flap border two finger widths below the vascular origin, and both parallel to the flap axis, which lies along a line from the vascular origin to the anterosuperioriliac spine. This new groin flap design provides the necessaryguidelines for vascular identifica- tion, accommodates pediatric and adult stature, and en- sures primary donor-site closure if flap dimensions are within the prescribed boundaries. In addition, a new sartorius-cutaneous groin flap is presented. This combinesthe cutaneous groin flap with the proximal sartorius muscle (up to 15 cm), which supplied by the deepvessels of the superficial circumflex iliac system. The sartorius-cutaneous groin flap further emphasizes the concept of singleopedicle compound or combined flaps and additionally enhancesthe extensive. reconstructive versatility of previously described groin flaps. Over 200 pedicled and free groin flaps have been performed according to the "rule of two finger widths" over the past 5 years. There have been no complications related to flap design, such as difficulty with flap eleva-. tion, marginal necrosis, or donor-site closure. Fourcase.,; of free sartorius-cutaneous groin, flaps have been per-. formed, with complete survival of the skin flap as well as the skin graft on the sartorius muscle in each patient. Since first described by McGregor andJacksor~ in 1972,1’2 the pedicled groin flap modificatior~ of the Wood 3’4 and Shaw 5’6 abdominal flaps ha.,; been widely used in reconstructive surgery. Ir~ 1973, Daniel and Taylor 7 and O’Brien et al. 8 expanded the usefulness of this donor site by successfully employing free groin flaps for Ic~ extremity reconstruction. Although initiall popular form of free-tissue transfer, the flap has subsequently been used less fiequel as other donor sites have emerged. Reason this decline in popularity may include the .able origin, limited length, and inconsistent ber of the vascular pedicle, as well as exce bulk in obese patients. Despite these disad tages, the groin flap remains a solidly method of reconstruction for pedicled or transfer. 9-~ The purpose of this paper is line techniques that improve groin flap ness and demonstrate the versatility of groin reconstruction. Specifically, a simple method for groin flap design, the "rule of; finger widths," will be presented, and sartorius-cutaneous groin flap will be that emphasizes the principle of corn combined flaps from the groin region. MATERIALS AND METHODS During the 5-year period from 1983 through January of 1988, over 200 cled and free groin flaps have been perfc at Chang Gung Memorial Hospital. The and elevation of many of these flaps have facilitated by the use of the "rule of two widths." The two-finger-widths rule is the transverse diameter of the patie~at’s it and long fingers at the distal interphal level. This principle allows for simplified safe dissection, and primary donor-site The relative consistency of the width of the two fingers among adults (3.5 to 4.0 cm) the operator’s fingers to serve as the template after initial comparison with the From the Department of Plastic and Reconstructive Surgery at the Chang GungIVlemorial Hospital and Chang Gung the Departmentof Surgery, Division of Plastic and Reconstructive Surgery, at Michigan State University College of Human for publication February 19, 1988; revised July 21, 1988. 100
Transcript of Groin Flap Design and Versatility - Semantic Scholar · essary. During microvascular anastomosis,...

Groin Flap Design and VersatilityDavid C. C. Chuang, M.D., L. H. Colony, M.D., Iq[. C. Chert, M.D., and F. C. Wei, M.D.Taipei, Taiwan, and East Lansing, Mich.
The groin flap is a reliable and well-established recon-structive option for pedicled or free-tissue transfer. Con-cern regarding its variable vascular origin and caliber haslimited its use. To overcome this, a simplified guidelinebased on the transverse diameter of the patient’s indexand long fingers at the distal interphalangeal level hasbeen developed. Thus "rule of two finger widths" posi-tions the origin of the vascular pedicle from the femoralvessels two,finger widths below the inguinal ligament,the upper flap border two finger widths above the in-guinal ligament, the lower flap border two finger widthsbelow the vascular origin, and both parallel to the flapaxis, which lies along a line from the vascular origin tothe anterosuperior iliac spine. This new groin flap designprovides the necessary guidelines for vascular identifica-tion, accommodates pediatric and adult stature, and en-sures primary donor-site closure if flap dimensions arewithin the prescribed boundaries.
In addition, a new sartorius-cutaneous groin flap ispresented. This combines the cutaneous groin flap withthe proximal sartorius muscle (up to 15 cm), which supplied by the deep vessels of the superficial circumflexiliac system. The sartorius-cutaneous groin flap furtheremphasizes the concept of singleopedicle compound orcombined flaps and additionally enhances the extensive.reconstructive versatility of previously described groinflaps.
Over 200 pedicled and free groin flaps have beenperformed according to the "rule of two finger widths"over the past 5 years. There have been no complicationsrelated to flap design, such as difficulty with flap eleva-.tion, marginal necrosis, or donor-site closure. Four case.,;of free sartorius-cutaneous groin, flaps have been per-.formed, with complete survival of the skin flap as well asthe skin graft on the sartorius muscle in each patient.
Since first described by McGregor andJacksor~in 1972,1’2 the pedicled groin flap modificatior~of the Wood3’4 and Shaw5’6 abdominal flaps ha.,;been widely used in reconstructive surgery. Ir~1973, Daniel and Taylor 7 and O’Brien et al.8
expanded the usefulness of this donor site by
successfully employing free groin flaps for Ic~extremity reconstruction. Although initiallpopular form of free-tissue transfer, theflap has subsequently been used less fiequelas other donor sites have emerged. Reasonthis decline in popularity may include the.able origin, limited length, and inconsistentber of the vascular pedicle, as well as excebulk in obese patients. Despite these disadtages, the groin flap remains a solidlymethod of reconstruction for pedicled ortransfer. 9-~ The purpose of this paper isline techniques that improve groin flapness and demonstrate the versatility of groinreconstruction. Specifically, a simplemethod for groin flap design, the "rule of;finger widths," will be presented, andsartorius-cutaneous groin flap will bethat emphasizes the principle of corncombined flaps from the groin region.
MATERIALS AND METHODS
During the 5-year period from1983 through January of 1988, over 200cled and free groin flaps have been perfcat Chang Gung Memorial Hospital. Theand elevation of many of these flaps havefacilitated by the use of the "rule of twowidths." The two-finger-widths rule isthe transverse diameter of the patie~at’s itand long fingers at the distal interphallevel. This principle allows for simplifiedsafe dissection, and primary donor-siteThe relative consistency of the width of thetwo fingers among adults (3.5 to 4.0 cm) the operator’s fingers to serve as thetemplate after initial comparison with the
From the Department of Plastic and Reconstructive Surgery at the Chang Gung IVlemorial Hospital and Chang Gungthe Department of Surgery, Division of Plastic and Reconstructive Surgery, at Michigan State University College of Humanfor publication February 19, 1988; revised July 21, 1988.
100

84, No. 1 / GROIN FLAP DESIGN
t’S. In clinical practice, the usual operator-iient variability of less than 0.5 cm can be
adjusted for during marking and has littleon final flap design. Moreover, no design
terations have been necessary for patients withmsualtv broad or slender digits. However, pe-
p~ttients do require strict attention to ra-finger width assessment and accurate flap
but still conform to the two-finger-
~[dths rule.
the two-finger-widths rule, easy and~id intraoperative or bedside flap design is
line. The bony landmarks of the anterosu-riot iliac spine (ASIS) and pubic tubercle are
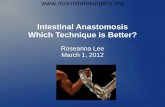
and the course of the inguinal ligament(Fig. 1, dashed line). The femoral ar-
i (FA) is then palpated and marked. Its course~resents the medial flap border. Point 1 (Fig.the origin of the superficial circumflex iliac
~ (SCIA) from the femoral artery, is locatedthin two finger widths below the junction of
inguinal ligament and the femoral artery.rative exploration has confirmed the or-the superficial circumflex iliac artery
this interval in all cases of free or islandThe course of this artery, also the
flap, is then drawn from its origin onartery (point 1) to the anterosuperior
spine. The superficial circumflex iliac artery[es into a superficial and deep branch medial~ sartorius within the femoral triangle.9’12-16
2 (Fig. 1), two finger widths medial
1. The rule of two finger widths (ASIS = anterosu-iliac spine; dashed line = inguinal ligament; FA =artery; SCIA = superficial circumflex iliac artery;
= SCIA origin" Point 2 ~ superficial SCIA branch-*uperficial course).
101
the anterosuperior iliac spine, the superficialbranch of the superficial circumflex iliac arteryemerges from beneath the deep fascia to con-tinue a more superficial course, while the deepbranch of the superficial circumflex iliac arteryenters the sartorius to supply the proximal endof the muscle. The upperflap border is identifiedmedially two finger widths above the inguinalligamen~t parallel to the superficial circumflexiliac artery course. The lower flap border is alsoparallel to the superficial circumflex iliac arterycourse and is marked two finger widths belowthe superficial circumflex iliac artery origin(point 1). The position of the lateralflap borderis usually determined by recipient-site require-ments. Flap length-to-width ratio beyond the an-terosuperior iliac spine is usually kept at 1:1 forsafety. Once markings are complete (Fig. ~),specific flap configuration along the central axiscan be outlined depending on donor-site require-ments. If drawn within the identified boundaries,direct donor-site closure is ensured. Based on apatient’s two finger widths of up to 4 cm, a flap1~ cm wide can be harvested. In flaps so de-signed, sufficient undermining and hip flexionhave allowed primary closure in 100 percent ofpatients.
Dissection
The bidirectional dissection plan outlined byDaniel and Terzis~ and others~2-~4 is .helpful be-cause laterally the superficial circumflex iliac ar-tery course is constant and medially its origin isvariable (from the common femoral, profundafemoral, external pudendal, or superficial epi-gastric, arteries). This allows for a rapid lateral-to-medial dissection and a slow, meticulous me-dial-to-lateral dissection. Flap elevation is corn-
FIG. 2. Patient outline of the rule of two finger widths.

102
Femoral vein
PLASTIC AND RECONSTRUCTIVE SURGERY, July
, i
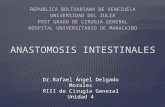
FIG. 3. (A) Cross section of groin region with lateral sartorius fascia incised. (SCIA superficial circumflex iliac artery). (B) Cutaneous groin flap elevation with the superficialcircumflex iliac artery and the anterior ~,~artorius fascia. (C) Sartorius-cutaneous groin flapelevation with the deep superficial circumflex ilia c artery above the posterior sartorius fascia.
pleted as the lateral and medial dissections pro-gress toward one another.
The conventional groin flap is based on thesuperficial branch of the superficial circumflexiliac artery, which begins its superficial coursetwo finger widths medial to the anterosuperioriliac spine as it exits the femoral triangle (point2 in Fig. 1). This vessel is best protected byharvesting the anterior sartorius fascia with thecutaneous groin flap, even though this may riskinjury to the lateral femoral cutaneous nerve(Fig. 3, A and B). The fascia is incised longitudi-nally along the lateral muscle border and ele-vated from lateral to medial. Prior to incising themedial muscle fascia from beneath, the superfi-cial branch is visualized through the fascia andprotected, while the deep superficial circumflexiliac artery branch penetrating the fascia is li-gated. This deep vessel originates within thefemoral triangle at the superficial circumflex iliacartery bifurcation and courses deep and lateralllybeneath the anterior sartorius fascia supplyingthe muscle.
Because donor vessels are often small, prior totransection of the vascular pedicle, careful as-sessment of the required vascular caliber is nec-essary. During microvascular anastomosis, mostvascular discrepancies can be overcome by tra-ditional methods of instrument dilation, obliquesectioning, fish-mouthing, and end-to-side tech-niques. In the case of the groin flap, additionalterminal vascular diameter can be obtained byharvesting a wedge or cuff (Fig. 4, A) of femo’.ral
A
FIG. 4. Gaining additional terminal Vascular diameter.Harvesting a cuff of femoral artery. (B) Longication splitting.
artery and vein with the vascular pedicle.9
femoral vessels may be closed directly orvein patch if required. A more practical te{nique can be employed when the superficialcumflex iliac artery and superficial epigastrictery have a common trunk or proximallytioned side branches (even if small). Thebifurcation is split and opened by incising lot
tudinally the inner V portion of thefrom the open vessel ends. This maneuver dmatically increases the diameter availableanastomosis and provides a smooth transit~between larger recipient and smallervessels~4 (Fig. 4, B).
SARTORIUS-CUTANEOUS GROIN FLAP
Previously described groin flap anatomydocumented the superficial circumflex iliac

Vol. 84, No. 1 / GROIN FLAP DESIGN
FIG. 5. Sartorius-cutaneous groin flap.
tery course and its division into superficial anddeep branches. Clinically, as noted in the preced-
ing section, the deep superficial circumflex iliaclrtery branch and accompanying vein run deep
the sartorius fascial This pedicte enters and)plies the proximat sartorius muscle and is the
Isis for a newly devised sartorius-cutaneousIroin flap (Fig. 5). Frequently, a more medially
located smaller pedicle from the superficial cir-~mflex iliac artery also supplies the proximal
and should be preserved. The type IVvascular supply of the sartorius gen-
prohibits muscle transfer. ~7 However, the)roximal 15 cm has been reliably transferi’ed infour patients (from January of 1986 throughDecember of 1987) based on the deep vessels ofthe superficial circumflex iliac system. The!ength of proximal sartorius transferred in thismanner should not extend beyond 15 cm andIsually requires division of two distal segmental
Beyond this level, muscle viability isuestionable. In clinical cases, active bleeding
the cut muscle edge and the distally dividedpedicles is mandatory to provide as-
surance of adequate muscle vascularity. Initialmuscle coverage with porcine skin followed bydelay<:d split-thickness skin grafting is recom-
Dissection of this new flap begins identically tothat of cutaneous groin flap elevation (Fig. 3, A).
lateral sartorius fascia is similarly incisedmgitudinally during the lateral to medial dissec-
The muscle may then be safely elevatedits posterior fascia beginning posteriorly
and inferiorly away from the deep vessels previ-described (Fig. 3, C). Once mobilized, the
muscle is divided distally at the selected level and
lly at its anterosuperior iliac spine origin,the medial muscle fascia is divided from
after the pedicle is visualized. This flap
103
incorporates both the superficial and deepbranches of the superficial circumflex iliac ar-tery, and no direct exploration of the deepbranch is necessary. As the muscle is raised fromits posterior fascia, ligation of two or more me-dially located segmental pedicles may be re-quired. The remaining medial groin flap dissec-tion within the femoral triangle follows.
CASE REPORTS
Case 1
A 20-year-old man suffered a severe nonreplantablecrushing amputation of the radial border of his nondominantleft hand.. The amputation level extended obliquely throughthe base of the first and midpoint of the second metacarpalsand through the distal phalanges of the long and ring fingers(Fig. 6, above, left). A salvaged portion of the distal indexmetacarpal was used acutely as a conventional bone graft toelongate the thumb metacarpal (Fig. 6, above, right). Becausewell-vascularized muscle coverage of the bone graft wassought, the proximal sartorius was elevated with the groinflap being raised for wound coverage. The muscle demon-strated excellent viability and was wrapped around the bonegraft (Fig. 6, center, left). The cutaneous portion of thesartorius-cutaneous groin flap was then employed to coverthe muscle and remaining open wound (Fig. 6, center, right).Following uncomplicated pedicle division at 4 weeks, excel-lent primary healing was achieved in preparation for toe-to-thumb transfer (Fig. 6, below).
Case 2
A 27-year-old man sustained a punch-press injury to thewrist area of his dominant right upper extremity (Fig. 7,above, left). Damage to deep structures included open frac-ture dislocation of the carpus and first two metacarpals,multiple flexor and extensor tendon ruptures, and transec-tion of the radial and ulnar arteries and ulnar nerve. Follow-ing removal of devitalized tissue, fracture fixation, revascu-larization, and tendon and nerve repair, additional debride-ment of nonviable skin and soft tissue dorsally was necessary(Fig. 7, above, right). This resulted in a 5-cm-wide volar soft-tissue defi~ct with exposed vascular, nerve, and tendon re-pairs. Dorsally and radially, extensor tendons over the first,second, and third metacarpals were exposed from the wristto the metacarpophalangeal joints. Wound coverage in twoplanes was required, both volar and dorsal.
Recon..struction was accomplished acutely with a free sar-torius-cutaneous groin flap. This included the proximal 10cm of the sartorius muscle and a 6 x 14 cm cutaneous groinflap on a single vascular pedide. Following transfer andrevascularization, the groin flap was positioned over the rawvolar wrist surface, and the muscle portion was rotated tocover the dorsal-radial defect and initially dressed with por-cine skin followed by delayed split-thickness skin grafting(Fig. 7, center, left). The donor site was closed primarily, andthe patient’s postoperative course was uncomplicated. Theoverall reconstructed appearance and functional recoverywere excellent (Fig. 7, center, right, and below).
DISCUSSION
Numerous anatomic and clinical studies havebeen published regarding groin flap anatomy

104 PLASTIC AND RECONSTRUCTIVE SURGERY, Ju[ 3, 19~
FIG. 6. Pedicled sartorius-cutaneous groin flap. (Above, left) A 20-year-old man with radial left hand amputation.right) Acute thumb metacarpal bone graft. (Center, left) Positioning of sartorius muscle. (Center, right) Pedicledportion of flap. (Below) Primary healing prior to toe-to-thumb transfer.
and application since the flap was first describedin 1972.~’2’7-16’~8-z5 These studies have demon-strated general agreement that the flap axis over-lies the superficial circumflex iliac artery course.This axis is consistently directed from the pointof superficial circumflex iliac artery origin to theanterosuperior iliac spine. In spite of their con-stant course, the superficial circumflex iliac ves-
sels have a variable point and pattern of oriThe level of vascular origin has beenas between 2.5 cm~6 and 5 cm~4 below theguinal ligament, and four potential vascularterns have been found at this site by Harii
Unfortunately, because of thisanatomy, pinpoint localization of the groinpedicle is not possible preoperatively. This

Vol. ,~4, No. 1 / GROIN FLAP DESIGN 105
Free sartorius-cutaneous groin flap. (Above, l@) A 27-year-e, ld man with right wrest punch-press injury. (Above, right)d~lsal-radial skin and soft-tissue debridement. (Center, left) Flap inset. (Center, right, and below) Primary healing at 3
variability may direct some surgeons toreconstructive alternatives with more de-anatomy, although it need not be a deter-
to .utilizing this most easily concealed of allsttes. The "rule of two finger widths" can
-qP Smgeons overcome concerns regarding an-variation in the groin region. It provides
necessary guidelines for proper flap design
and vascular origin identification within two fin-ger’ widths below the inguinal ligament. The two-finger-widths rule simply positions key points,accommodates pediatric and adult stature, andensures primary donor-site closure if the flapdimensions are within the prescribed boundaries.Employing this new groin flap design with pre-viously described dissection plans facilitates time-

106
saving flap harvest while emphasizing the appro-priate caution and flexibility necessary to pre-serve the vascular pedicle.
While the outlined design format can helpeliminate concern regarding vascular variations,the microvascular techniques described can over-come anastomotic size discrepancies due to po-tentially limited donor-vessel caliber. However,the remaining disadvantage of flap bulkiness inobese patients remains largely unanswered. Po-sitioning the flap more laterally, as in Acland’siliac free flap,21 only partially improves the situ-ation. The only documented potential solutionhas been DeHaan et al.’s case report of rapidgroin flap expansion (11 days). In addition providing a large, well-vascularized flap with lim-ited donor-site deformity, the .transferred tissuewas noted to be dramatically thinned and sur-prisingly supple.26 The precise indications forrapidly expanded groin flaps and whether flapbulkiness can reliably be eliminated in obese pa-tients await further application.
The sartorius-cutaneous groin flap presentedis a new reconstructive option from a familiardonor region. It is not a true musculocutaneousflap because the cutaneous portion of the flap isnot supplied by direct musculocutaneous perfo-rating vessels. This muscle-cutaneous type of do-nor tissue can have the added flexibility of recon-structing defects at differing levels or depths, aswell as in two different planes. It may be em-ployed for upper extremity coverage as a pedi-cled flap or have broader indications as a freeflap.
The concept of compound or combinationflaps, such as the sartorius-cutaneous groin flap,is not new and has been widely applied in otherregions. Familiar examples include the fibularosteoseptocutaneous flap combined with the lat-eral soleus and latissimus dorsi combinations withscapular, parascapular, axillary, and serratus an-terior. In addition to these naturally occurringflap combinations, artificial single-pedicle flapssuch as the free latissimus dorsi and fibular com-bination also have been devised,e7 The principleof compound or combined tissue transfer on asingle pedicle not only increases the area of flapcoverage, but also enhances the overall useful-ness of existing donor sites.
Nowhere has the concept of compound orcombined flaps been so widely applied as in thegroin region. Following description of the pedi-cled and free cutaneous flaps in 1972 and 1973,respectively, 1’~’7’8 Taylor and Watson~8 devel-
PLASTIC AND RECONSTRUCTIVE SURGERY, july 1989
oped the osteocutaneous flap in 1978. and Tay-lor et al.~9’3° documented its deep vascular supplyin 1979. This same vascular pedicle was utilizedwhen Ramasastry et al. 31’~2 outlined the internaloblique muscle and myo-osseous flaps in 1984.:Wei et al. ~ later outlined the fasciocutaneot(with external oblique aponeurosis) and osteofas.ciocutaneous (external oblique aponeurosis and:iliac crest) groin flaps for Achilles tendon reostruction with or without associated bony defects,The sartorius-cutaneous groin flap serves tophasize the concept of compound or combin.flaps and additionally highlight the reconstru,tive flexibility of the groin region.versatility and applicability of the groin flap andits limited donor-site deformity continue to makit an excellent reconstructive option.
David C. C. Chuang, M.D.Department of Plastic and Reconstructive SurChang Gung Memorial Hospital199, Tung Hwa North RoadTaipei, Taiwan
REFERENCES
1. McGregor, I. A., and Jackson, I.T. The groinBr.J. Plast. Surg. 25: 3, 1972.
2. Lister, G. D., McGregor, I. A., and Jackson, I. T.groin flap in hand injuries, lnjury 4: 229, 1973.
3. Wood, J. Case of extreme deformity of the neckforearm from the cicatrices of a burn cured b’sion, excision and transplantation of skin,and remote. Medico-chir. Trans. 46 149, 1863.
4. Boo-Chai, Khoo. John Wood and his contributionplastic surgery: The first groin flap. Br. J. Plast.30: 9, 1977.
5. Shaw, D.T. Open abdominal flaps for repmr offace defects of the upper extremity. Surg.Am. 24: 293, 1944.
6. Shaw, D. T., and Payne, R. L. One stage tubeddominal flaps: Single pedicle tubes. Surg.Obstet. 83: 205, 1946.
7. Daniel, R. K., and Taylor, G.I. Distant transfer of:island flap by microvascular anastomoses: Atechnique. Plast. Reconstr. Surg. 52:111, 1973.
8. O’Brien, B. M., McLeod, A. M., Hayhurst, J. W.,al. Successful transfer of a large island flap frotgroin to the foot by microvasculmReconstr. Surg. 52: 271, 1973.
9. Daniel, R. K., and Terzis, J. K. Free-Tissueby Microvascular Anastomoses. In R. K. DanielJ. K. Terzis, Reconstructive Microsurgery.tle, Brown, 1977. Pp. 214-221.
10. Chow, J. A., Bilos, Z.J., Hui, P., Hall, R. E., Seyfer,E., and Smith, A.C. The groin flap in resurgery of the hand. Plast. Reconstr. Surg.1986.
11. Wood, M. B., and Iron, G.B. Upper-extremityskin flap transfer: Results and utility aswith conventional distant pedicle skin flaps.

Vol. 84, No. 1 / GROIN FLAP DESIGN
Plast. Surg. 11: 523, 1983.‘2. Harii, K., Obmori, K., Torii, S., et al. Free groin skin
flaps. Br. J. Plast. Surg. ’28: 225, 1975.
13. O’Brien, B. M., Morrison, W. A., Ishida, H., etal. Free-flap transfers with microvascular anasto-moses. Br. J. Plast. Surg. 27: 220, 1974.
14. Serafin, D., and Buncke, K.J. (Eds.) Groin Flap. In T. Jackson (Ed.), Microsurgical Composite Tissue Trans-plantation. St. Louis: Mosby, 1979. Pp. 231-243.
Taylor, G. I., and Daniel, R. K. The anatomy ofseveral free-flap donor sites. Plast. Reconstr. Surg. 56:243, 1975.
:16. Ohmori, K., and Harii, K. Free groin flaps: Theirvascular basis. Br. J. Plast. Surg. 28: 238, 1975.
Mathes, S. J., and Nahai, F. Clinical Applications forMuscle and Musculocutaneous Flaps. St. Louis: Mosby,1982.
Daniel, R. K., and Williams, H.B. The free transferof skin flaps by microvascular anastomoses. Plast.Reconstr. Surg. 52: 16, 1973.
Smith, P.J. The vascular basis of axial-pattern flaps.Br.J. Plast. Surg. 26: 150, 1973.
McGregor, I.A. Flap reconstruction in hand surgery:The evolution of presently used methods. J. HandSurg. 4: I, 1979.
~1. Acland, R.D. The’ free iliac flap: Lateral modification;: ) of the free groin flap. Plast. Reconstr. Surg. 64: 30,
1979.Schlenker, J. D., and Averill, R. M. The iliofemoral
(groin) flap for hand and forearm coverage. Orthop.Rev. 9: 57, 1980.
May, J. w., and Bartlett, S. P. Staged groin flap inreconstruction of the pediatric hand. J. Hand Surg.6: 163, 1981.
Wray, R. C., Wise, D. M., Young, V. L., and Weeks, P.M. The groin flap in severe hand injuri.es. Ann.
! Plast. Surg. 9: 459, 1982.~.’ Harii, K., lwaya, T., and Kawaguchi, N. Combination
107
myocutaneous flap and microvascular free flap. Plast.Reconstr. Surg. 68: 700, 1981.
26. DeHaan, M. R., et al. Pedicled Groin Flap Expansion:A Case Report. Presented at Midwest Plastic SurgerySociety Annual Meeting, Springfield, Illinois, 1987.
27. Donski, P. K., Buchler, U., and Ganz, R. Combinedosteocutaneous microvascular flap procedure for ex-tensive bone and soft-tissue defects in the tibia. Ann.Plast. Surg. 16: 386, 1986.
28. Taylor, G. I., and Watson, N. One-stage repair ofcompound leg defects with free revascularized flapsof groin skin and iliac bone. Plast. Reconstr. Surg. 61:494, 1978.
29. Taylor, G. I., Townsend, P., and Corlett, R. Super-iority of the deep circumflex iliac vessels as the supplyfor free groin flaps: Experimental work. Plast. Re-constr. Surg. 64: 595, 1979.
30. Taylor, G. I., Townsend, P., and Corlett, R. Super-iority of the circumflex iliac vessels as the supply forfree groin flaps: Clinical work. Plast. Reconstr. Surg.64: 745, 1979.
31. Ramasastry, S. S., Tucker, J. B., Swartz, W. M., andHurwitz, D.J. The internal oblique muscle flap: Ananatomic and clinical study. Plast. Reconstr. Surg. 73:721, 1984.
32. Ramasastry, S. S., Futrell, J. W., Williams, S. L., andHurwitz, D.J. Internal oblique muscle pedicle flapfor coverage of a major soft-tissue defect of the groin.Ann. Plast. Surg. 15: 57, 1985.
33. Wei, F.-C., Chen, H.-C., and Chuang, C.-C., etal. Reconstruction of Achilles tendon and calca-neous defects with skin-aponeurosis-bone compositefree tissue from the groin region. Plast. Reconstr.Surg. 81: 579, 1988.
34. Chen, Z. W., Yang, D. Y., and Chang, D.S. Free SkinFlap Transfer. In Z. W. Chen (Ed.), Microsurgery.Berlin: Springer-Verlag, Shanghai Scientific andTechnical Publishers, 1982. P. 220.