
Granulomatous diseases in ENT
99
Granulomatous conditions in ENT
-
Upload
sarita-pandey -
Category
Health & Medicine
-
view
17 -
download
2
Transcript of Granulomatous diseases in ENT

Granulomatous conditions in ENT
Granuloma formation
• Response of immune system to an indigestible agent• Usually neutrophils remove agents by phagocytosis &
digestion• Macrophages phagocytose indigestible agents, loose their
mobility & accumulate at site of injury• Undergo structural changes: Larger with more cytoplasm
epitheloid cells• Epitheloid cells fuse Multinucleated giant cells• Nuclei arrange in horse shoe pattern Langerhans giant
cells• All these cells are surrounded by a collar of lymphocytes

Granuloma

Granuloma
• Noncaseating or Caseating– Central area of necrosis– “Cheese-like” appearance– Often visible macroscopically
Granulomatous diseases
• Infective• Inflammatory• Neoplastic
• Forms part of a spectrum of conditions in which vasculitides play a role
• Many are systemic conditions– Preferentially target or present in the upper respiratory
tract
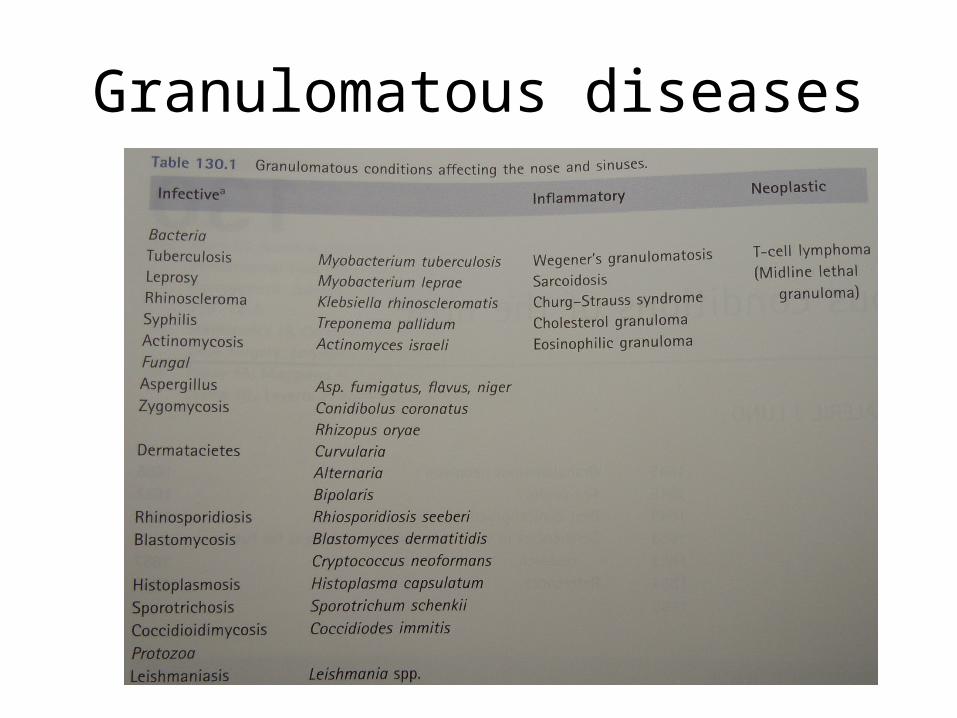
Granulomatous diseases
INFLAMMATORY CONDITIONS

Wegener’s Granulomatosis• Relatively common disease of upper airway• Friedrick Wegerner– 1939: Necrotizing granulomas and vasculitis of upper & lower
airway, occurring either together or as separate components
• Coexistence of vasculitis & granulomas• Classically involves triad: – Airway– Lung– Renal disease
Wegener’s Granulomatosis
• Aetiology = unknown• Hypersensitivity reaction to an unknown
stimulus• Affects all ages and both males & females

• 3 main forms of WG– Type 1
• Limited form• Symptoms of URTI persisting for weeks & not responding to
A/b• Pain over the dorsum of the nose• Epistaxis & variable degree of nasal obstruction• Very large crusting of the nasal cavities & nasopharynx
bilaterally• When crusts are removed – mucosa is very friable• Septal perforations & eventual nasal collapse in advanced
disease
Wegener’s Granulomatosis
Wegener’s Granulomatosis
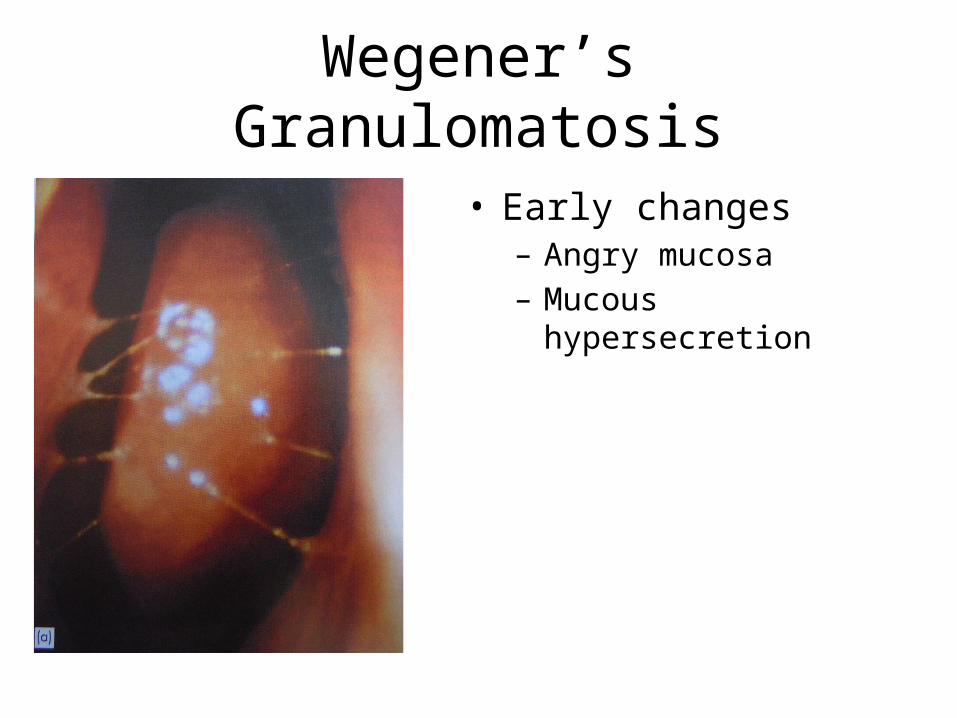
• Early changes– Angry mucosa– Mucous hypersecretion

Wegener’s Granulomatosis
• End result of advanced disease

Wegener’s Granulomatosis
• End result of advanced disease

Wegener’s Granulomatosis
• End result of advanced disease– Infiltration of orbit– Sclerosis and opacification of
nasal cavity– Septal erosion

Wegener’s Granulomatosis
• End result of advanced disease– Infiltration of orbit– Septal destruction– Hyperostosis– Opacification of sinuses
• 3 main forms of WG– Type 2• Sicker patient with more systemic symptoms• Pulmonary involvement
– Cough & pleuritic pain– Haemoptysis & cavitating lesions on CXR– Encapsulated lung abscess
Wegener’s Granulomatosis
• 3 main forms of WG– Type 3
• Widely disseminated with involvement of multiple organs– Airway
» Short segment of subglottic/upper tracheal stenosis– Pulmonary– Renal
» Hematuria & abn urinary sediment & segmental/diffuse glomerulonephritis
– Cutaneous» Tick-bite like lesions on the distal limbs
– Oral» Hyperplastic granular lesion of gingiva; ulcerative stomatitis
– Otological» OME ± mastoiditits & profound SNHL
– Eye» Conjunctivitis; Dacrocystitis; Episcleritis; Orbital pseudotumour
Wegener’s Granulomatosis

Wegener’s Granulomatosis

Wegener’s Granulomatosis
• Diagnosis– cANCA• 95% sensitive in generalized disease• 60% sensitive in localized disease
– FBC, ESR, CRP, CXR, Urine analysis for casts– Histology: Tissue from septum & all turbinates– CT nose & paranasal sinuses• Non-specific mucosal thickening; bony destruction; new
bone formation

Wegener’s Granulomatosis
Wegener’s Granulomatosis
• Main histological features:– Vasculitis involving medium & small vessels– Granulomatous necrosis (can be non-necrotic);
Large epitheloid cells; lined with histiocytes– Scattered multinucleated giant cells

Wegener’s Granulomatosis
• Treatment:– Prednisone 1mg/kg/day + Cyclophosphamide 2mg/kg/day x 1/12
• Prednisone tapered to alternate days x 2/12 & then discontinued once complete response achieved
• Cyclophosphamide continued x 6/12 to 1 year & then tapered over a few months
– Other• Azathioprine• Methotrexate• Plasma exchange Ig infusion
– Nose• Topical steroids, nasal douching & irrigation
– Surgical reconstruction• Wait until disease has been in remission for some time

Sarcoidosis
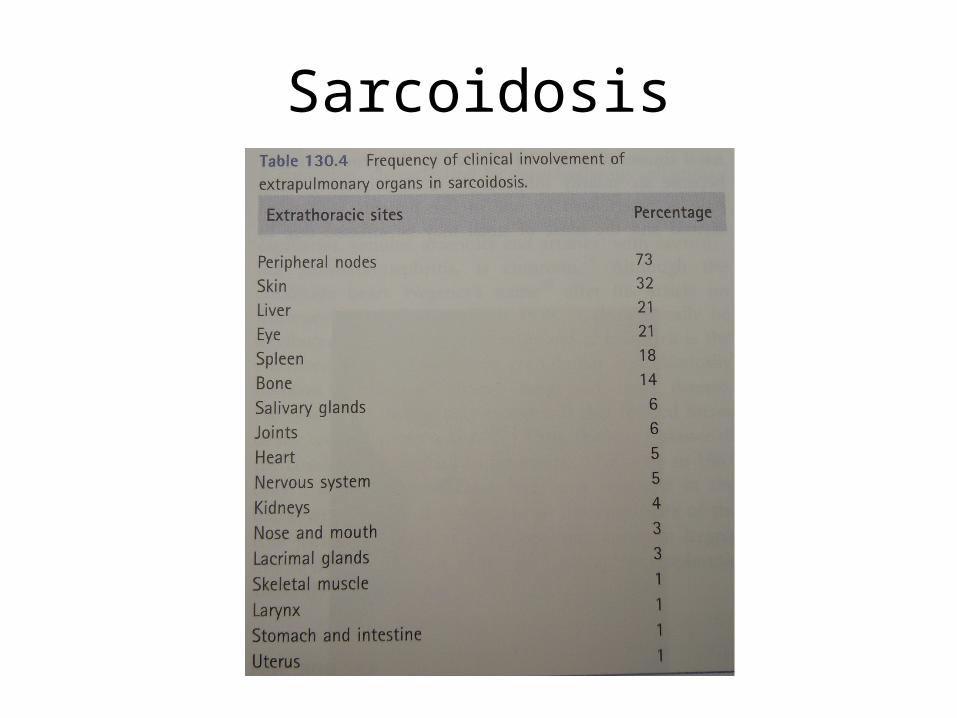
• Systemic condition of unknown aetiology• Can involve any organ including many H&N structures
• Incidence = 64/100,000 in Scandinavia• Condition of young adults between 3rd & 5th decade• Female preponderance = 2:1• Ratio of black to Caucasian = 12:1
• Nasal manifestation almost always part of multisystem sarcoid which have been present for some years
Sarcoidosis
Sarcoidosis
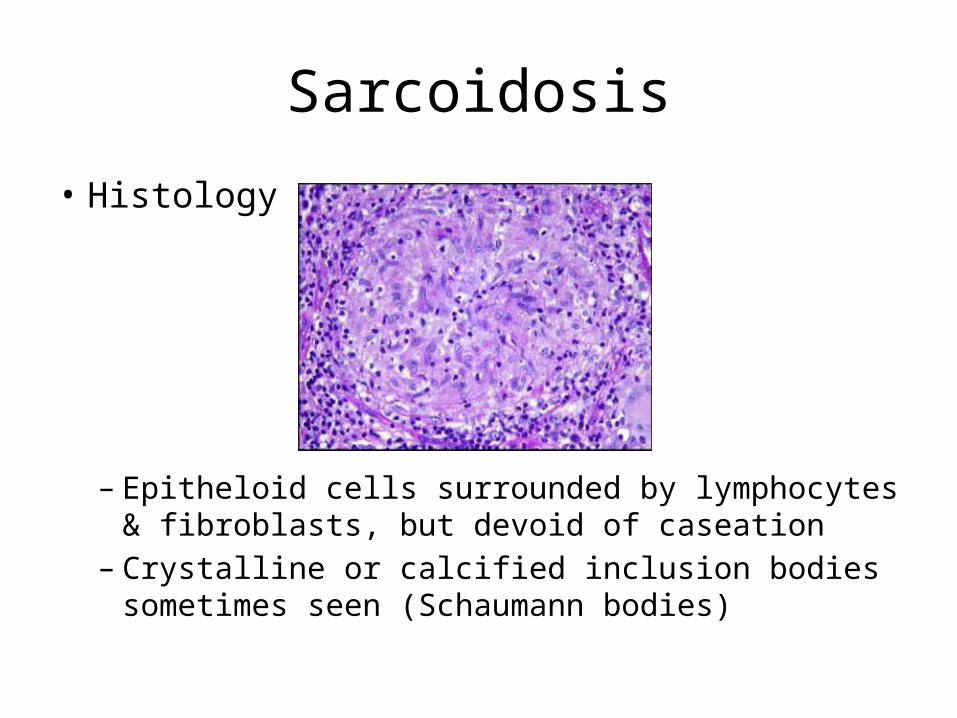
• Histology
– Epitheloid cells surrounded by lymphocytes & fibroblasts, but devoid of caseation
– Crystalline or calcified inclusion bodies sometimes seen (Schaumann bodies)

Sarcoidosis
• Nasal involvement– Presenting complaints

Sarcoidosis
• Nasal involvement– External
• Lupus pernio • Predilection for cold
sensitive areas, such as tip of nose

Sarcoidosis
• Lupus pernio of the cervical skin

Sarcoidosis
• Nasal involvement– Mucosa• Granular appearance (“Strawberry skin”)
– Tiny pale granulomas against a erythematous mucosa
• Very friable mucosa• Crusting, nasal congestion, mucopurulent discharge• Anterior septal perforation & later nasal bridge collapse• Paranasal sinus involvement & infection
Sarcoidosis
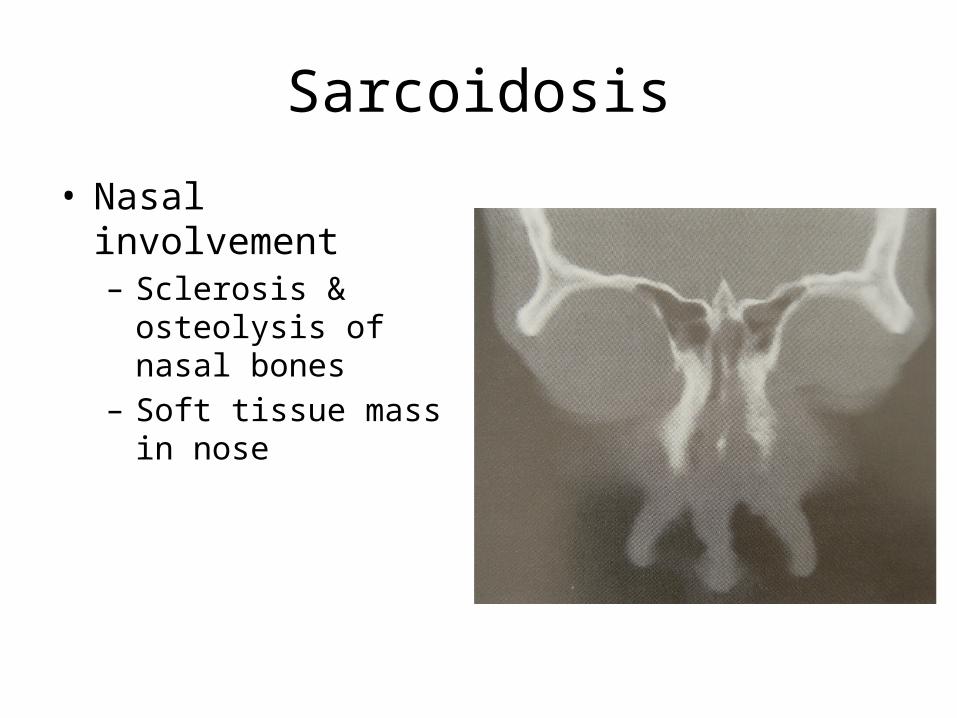
• Nasal involvement– Sclerosis & osteolysis of
nasal bones– Soft tissue mass in nose

Sarcoidosis
• Salivary glands– Bilateral non-tender, firm, smooth parotid swelling
• Lymphoid hyperplasia– Adenoids – OSA; OME
• Supraglottic larynx– Dyspnoea; dysphonia– Sub sites• Epiglottis arytenoid aryepiglottic folds false cords

Sarcoidosis
• Laryngeal involvement

Sarcoidosis
• Laryngeal involvement

Sarcoidosis
• Diagnosis– Combination of histology, imaging & haematology– Exclude other causes for non-caseating
granulomatous changes– ↑ serum ACE (83% of patients with active sarcoid)• Also in TB, Leprosy, 1ᴼ biliary cirrhosis
– ESR, CRP & urinary calcium– Mild anaemia, leucopenia, thrombocytopenia,
eosinophilia

Sarcoidosis
• Treatment– Oral steroids, Methotrexate ± Hydroxychloroquine– Topical intranasal steroids (spray/drops)– Nasal douching/irrigation
– Surgery contraindicated for both cosmetic & functional indications

Churg-Strauss Syndrome
• 1st described 1951 by Churg & Strauss– Syndrome of systemic vasculitis & asthma
• Eosinophil-rich & granulomatous infl involving the resp tract & necrotizing vasculitis affecting small to medium sized vessels & associated with asthma & eosinophilia

Churg-Strauss Syndrome
• 3 phases– Prodromal phase• May persist for years• Allergic disease (allergic rhinitis, nasal polyposis,
asthma)
– Peripheral blood & tissue eosinophilia• Chronic eosinophilic pneumonia & eosinophilic
gastroenteritis
– Life threatening systemic vasculitis
Churg-Strauss Syndrome
• Histo
– Necrotizing giant cell vasculitis, interstitial granulomas & eosinophilic pulmonary infiltrates
Churg-Strauss Syndrome
• Nasal involvement– Usual polyposis– May also have crusting & septal perforation
– Doesn’t display diffuse mucosal destruction like with WG

Churg-Strauss Syndrome
• Treatment– Oral steroids
– Polyposis• Topical steroids ± surgery
Giant cell Granuloma
• “giant cell reparative granuloma” or “giant cell reaction of bone”
• Benign condition of jaws & other craniofacial sites
• Commonly occur in children & young adults
Giant cell Granuloma
• Clinical features– Maxilla & mandible most commonly affected– sphenoid bone temporal bone
– Pain & swelling over affected bone– Diplopia; frontal headache; hearing loss; vertigo;
tinnitus
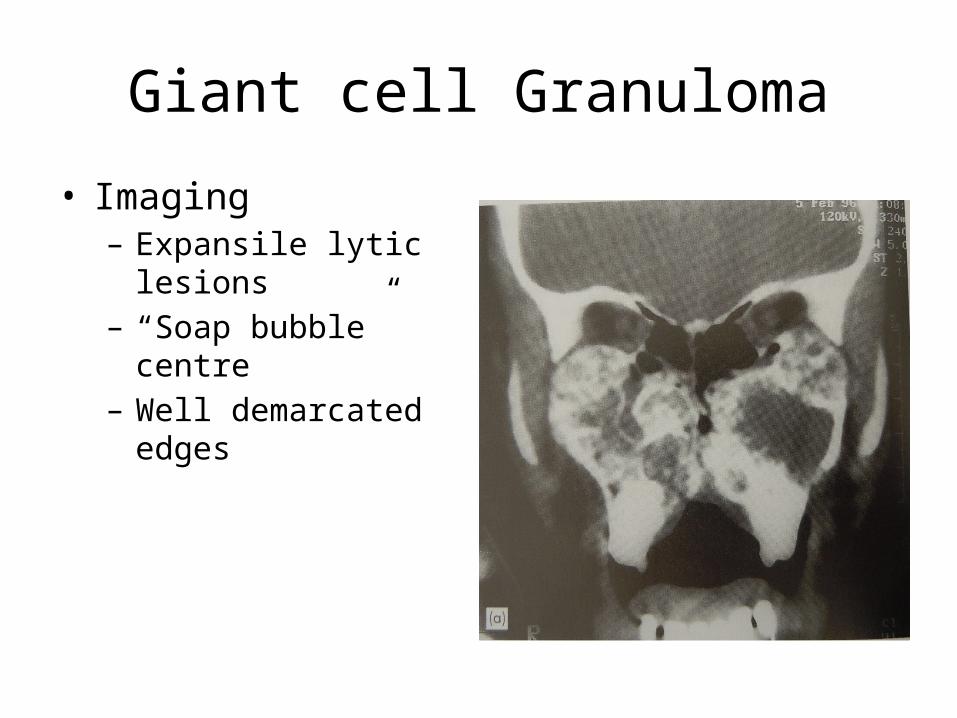
Giant cell Granuloma
• Imaging– Expansile lytic lesions– “Soap bubble” centre– Well demarcated edges

Giant cell Granuloma
• Cherubism– Bilateral symmetrical
involvement of jaws
– Rare inherited childhood condition

Giant cell Granuloma
• Cherubism– Bilateral symmetrical
involvement of jaws
– Rare inherited childhood condition
Cholesterol granuloma
• Granulomatous reaction to cholesterol crystals precipitated in tissues
• Presumed 2ᴼ to haemorrhage and/or trauma
• Lesions may affect maxilla, frontal sinus, temporal bone
• Produce expansion of bone, cosmetic deformity & displacement of adjacent structures

Cholesterol granuloma
• Imaging– Cyst-like expansion of bone/sinus– Opaque on CT & not contrast enhancing
• Histo– Granulation tissue of giant cells surrounding clefts
created by cholesterol granulation
• Treatment– Surgical excision & complete removal of granulation

INFECTIOUS SYSTEMIC DISEASES
BACTERIAL

Rhinoscleroma
• Chronic granulomatous disease of the resp tract– Nose; larynx; trachea & bronchi
• Klebsiella rhinoscleromatis
• Occur @ any age in either sex– > common in middle aged females
• Central & South-eastern Europe; North Africa; Indian subcontinent; Indonesia; South America
Rhinoscleroma
• 3 stages– Catarrhal stage
• Foul-smelling purulent rhinorrhoea (weeks – months)
– Atrophic stage• Large, foul-smelling nasal plaques or crusts• Same as lesions in atrophic rhinitis
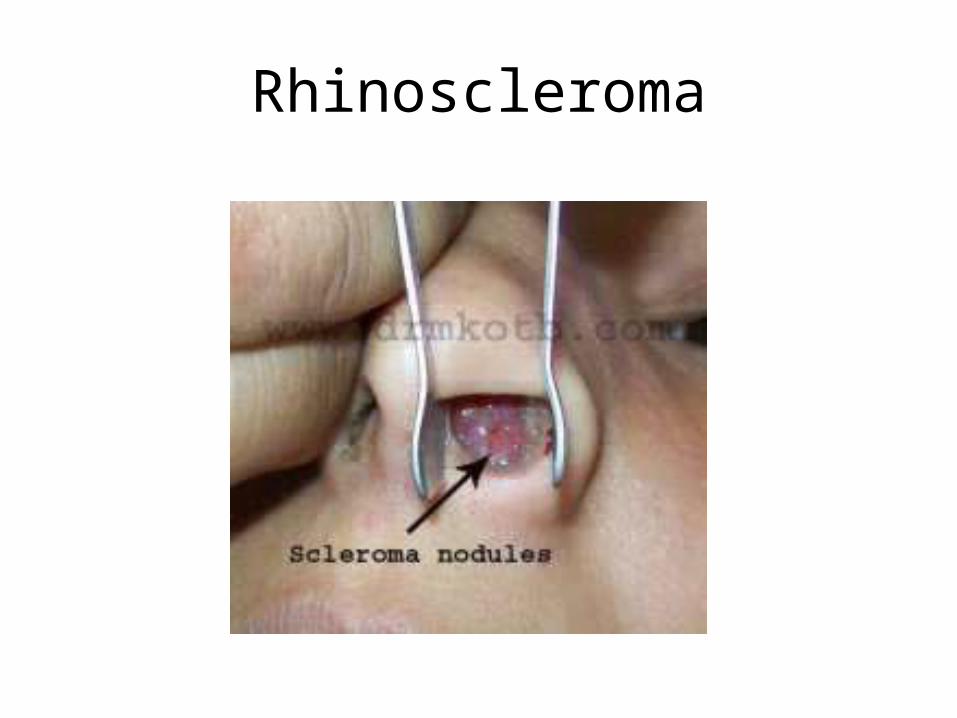
– Granulomatous or proliferative stage• Multiple granulomatous, non-ulcerative nodules throughout
nose, pharynx, larynx, trachea & bronchi• Bluish red & rubbery and later paler & harder
– Cicatrizing stage• Scaring, adhesions, stenosis & distortion of normal anatomy
Rhinoscleroma
Rhinoscleroma
• Histo– Scattered large foam cells (Mikulicz cells)• Vacuolated cells with a central nucleus• Contain the indigestible bacilli & Russel bodies
• Diagnosis– Clinical features– Microbiology– Histological features

Rhinoscleroma
• Treatment– Treatment must be intense & prolonged– Streptomycin 1g/day + Tetracycline 2g/day x 4/52– Continued till 2 x consecutive negative cultures
– Rifampicin, Bactrim & Ciprofloxacin
– Surgical debridement prior to A/b in granulomatous stage
– Surgery to “core out” scar tissue in Cicatrizing phase
Tuberculosis
• Mycobacterium tuberculosis• Uncommon in nose• More common in cervical LN, pharynx, larynx
& ear
Tuberculosis
• Nasal involvement– Lupus Vulgaris • Begins in vestibule, then extends to adjoining skin &
mucosa• Apple jelly nodules (Does not blanch)• May form ulcers with undermined edges

Tuberculosis
• Lupus vulgaris
Tuberculosis
• Nasal involvement– Lupus Vulgaris
• Begins in vestibule, then extends to adjoining skin & mucosa• Apple jelly nodules (Does not blanch)• May form ulcers with undermined edges
– Ulcerative form• Involves cartilaginous nasal septum or inferior turbinate• Nasal floor is spared• Nasal obstruction, pain, discharge, crusting, epistaxis• Septal perforation, but not dorsal saddling
– Sinus granuloma• Soft tissue mass with/without bone destruction

Tuberculosis
• Sinus granuloma– Sino-nasal mass– Surrounding infiltration– Bone destruction

Tuberculosis
• Laryngeal involvement– Occurs in association with pulm TB– Dysphonia, Dysphagia, Otalgia
– Diffusely oedematous & reddened larynx• Predominantly affects post ⅓ of larynx• May have ulceration (confused with Sq cell CA)

Tuberculosis
• Laryngeal involvement

Tuberculosis
• Diagnosis– Histology (AFB)– CXR– PCR & BACTEC
• Treatment– As other TB

Nontuberculous Mycobacteria
• Mycobacterium fortuitum• Mycobacterium scrofulaceum• Mycobacterium szulgai• Mycobacterium xenopi• Mycobacterium bovis
Syphilis
• Spirochaete: Treponema pallidum• Can affect all ages and both sexes equally
• Primary– Infectious!!– Chancre / hard non-painful ulcerated nodule– Self limiting (6 – 10 weeks)– Diff: furunculosis / malignant neoplasm

Syphilis
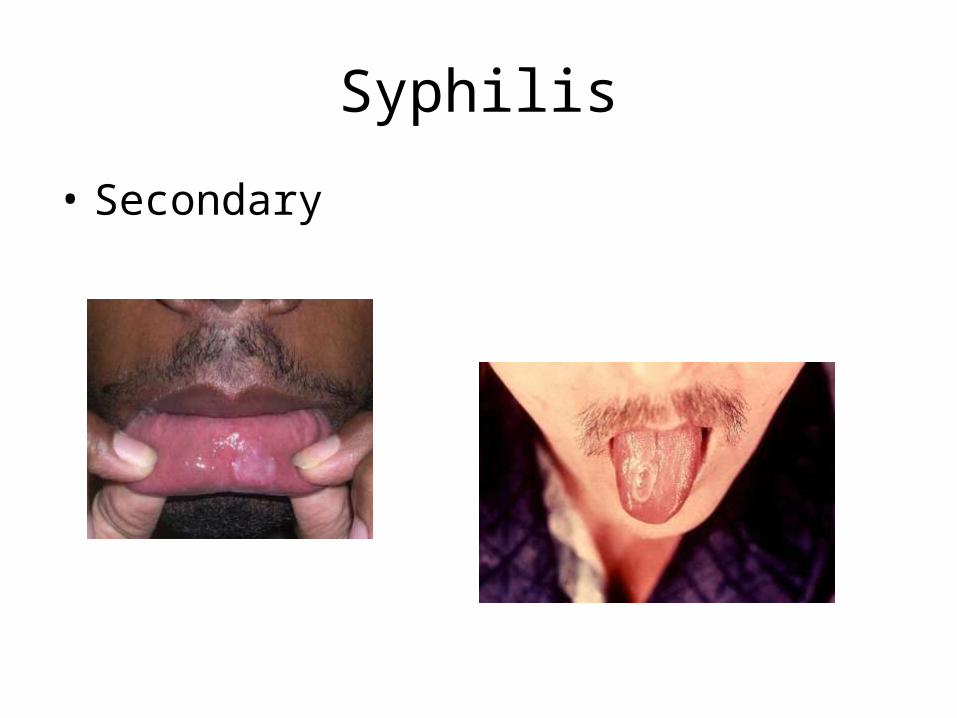
• Secondary– Most infectious!!– Persistent catarrhal rhinitis– Persistent crusting or fissuring of vestibule– Mucous patches on tongue, gingiva, pharynx– Rarely larynx• Diffuse erythematous papules on larynx
– Epiglottis & aryepiglottic folds
Syphilis
• Secondary

Syphilis
• Tertiary– Luckily much less infective….
– Nose• Pain (always worse @ night), swelling & obstruction• Tenderness over nasal bridge (characteristic sign)• Gumma
– Begins as a subcut nodule punched out destructive ulcer
• Bony portion of septum most comonly involved

Syphilis
• Tertiary– Ulcerated gumma– Cicatrization of bony
nasal dorsum
Syphilis
• Tertiary– Luckily much less infective….
– Larynx• Nodular infiltrates coalescing to painless ulcers
– Epiglottis & aryepiglottic folds
• Appearance = similar to TB & CA
– Ear• SNHL, OM, Meniere’s symptoms

Syphilis
• Diagnosis– TPHA/VDRL / RPR– Biopsy in doubtful cases
• Treatment– Parenteral Penicillin
Leprosy
• Hansen’s disease• AFB: Myrobacterium leprae
• Epidemiology– 12 – 15 million people affected world wide– Brazil, India, Indonesia, Myanmar, Nigeria: 82% of
cases– Commonly manifests ages 10-20 years– Nasal d/c = principal route of transmission

Leprosy
• 7th WHO Expert Committee on Leprosy– Hypopigmented or reddish skin lesion w definite
loss of sensation– Involvement of peripheral nerves (thickening or
loss of sensation– Skin smear + for AFB,s
Leprosy
• 2 distinct polar forms of disease w spectrum in between– Tuberculoid Leprosy:• Strong host resistance• Non-infective• Localized
– Lepromatous Leprosy• Poor host resistance• Infective• Systemic with widespread involvement of tissues
Leprosy
• Nasal involvement– Tuberculoid Leprosy• Solitary skin lesion w cutaneous anaesthetic patches• Vestibule skin involvement, but no mucosal involvement
– Lepromatous Leprosy• Skin, nerve & mucosal involvement• Nasal obstruction, crust formation & blood-stained d/c
– Nasal d/c contain AFB’s
• Advanced: Atrophic Rhinitis, septal perforation & dorsal saddling

Leprosy
• Laryngeal involvement– Only with concurrent systemic illness– Principal area = supraglottis• Epiglottis – nodular oedema & ulceration
– Present w dysphonia (muffled voice)

Leprosy
• Diagnosis– Clinical– Bacteriological examination: Nasal d/c or scrapings
of nasal mucosa– Histology
• Treatment– Dapsone (Single drug treatment resistance)– Rifampicin & clefozamine – acts rapidly– Triple therapy = best results

Actinomycosis
• Anaerobes: Actinomycoses bovis / israeli• Chronic suppurative disease• Poor dental hygiene• Soft tissue involvement of submandibular or
cervical regions– Abscess & sinus tract formation
• Secondary laryngeal involvement– Erythematous, swollen wooden larynx

Actinomycosis
• Diagnosis:– Microbiology– Classic “Sulphur
Granules” on biopsy
• Treatment– Penicillin– Tetracycline

INFECTIOUS SYSTEMIC DISEASES
FUNGAL
Histoplasmosis
• Histoplasmosis capsulatum• Granulomatous fungal disease• Soil from chicken houses / bat & bird faeces
• Extremes of ages• Mostly Larynx & tongue, but also nose &
paranasal sinuses

Histoplasmosis
• Always accompanied pulm involvement– Cough, chest pain, hoarseness
Diffuse miliary Chronic cavitating
Histoplasmosis
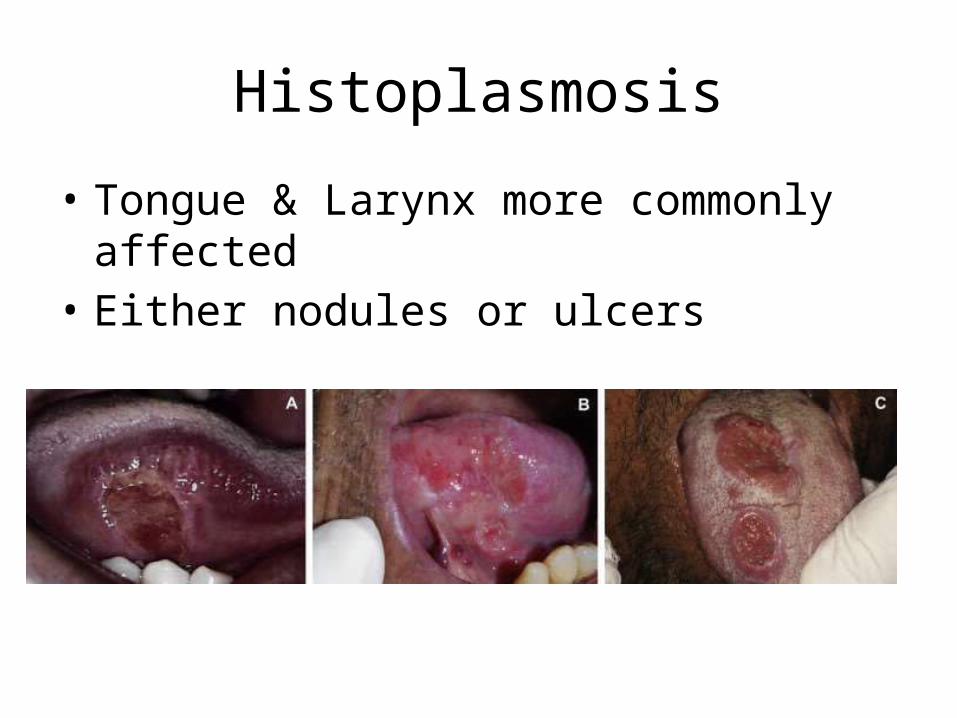
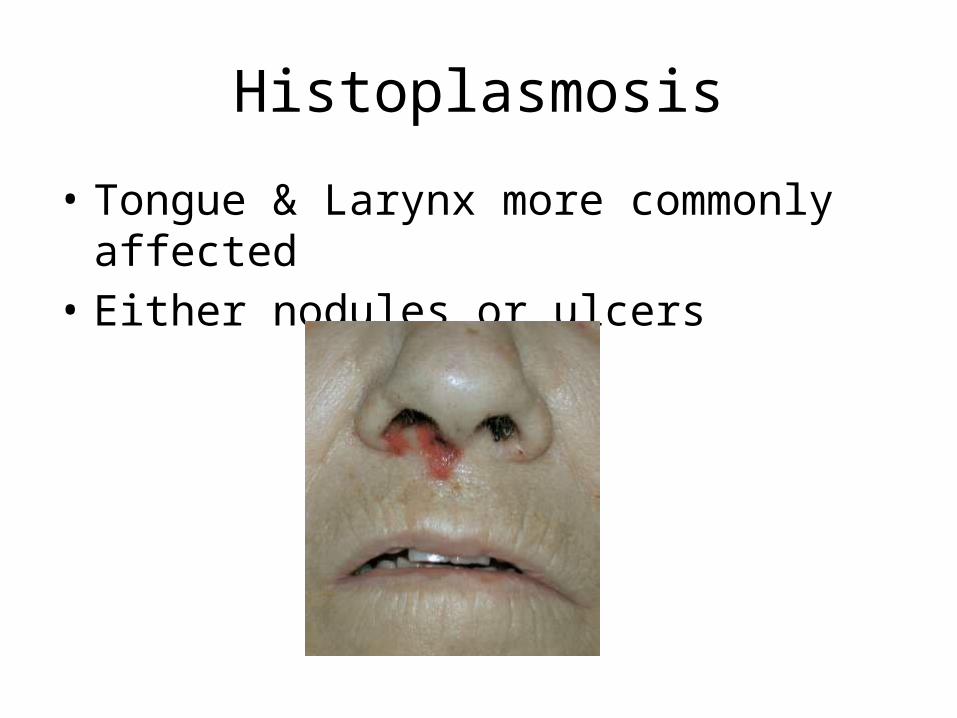
• Tongue & Larynx more commonly affected• Either nodules or ulcers
Histoplasmosis
• Tongue & Larynx more commonly affected• Either nodules or ulcers

Histoplasmosis
• Diagnosis– Biopsy• Epitheloid / histiocytic granuloma• Organism seen with methenamine silver nitrate stain
• Treatment– Amphotericin B
Rhinosporidiosis
• Rhinosporidium seeberi• Asia & Africa• Immersion in contaminated waters
• Nasal mucosal lesions– Initial: flat & sessile lesion– Later: Painless polypoid growth filling the nasal
cavity

Rhinosporidiosis
• Clinical manifestation– Painless slow growing nasal mass• Friable, polypoid and vascular• Strawberry appearance
– Nasal obstruction, watery rhinorrhoea

Rhinosporidiosis
• Diagnosis– Histology• Pseudoepitheliomatous squamous metaplasia overlying
multiple globular cysts (sporangia)• Prominent accompanied granulomatous reaction of
fibrosis tissue
• Treatment– No medical management– Complete surgical excision
Aspergillus/Mucor
• Fungal Rhinosinusitis• Usually in immune-compromised individuals
• Non-invasive fungal sinusitis / rhinosinusitis• Invasive fungal rhinosinusitis

Aspergillus/Mucor
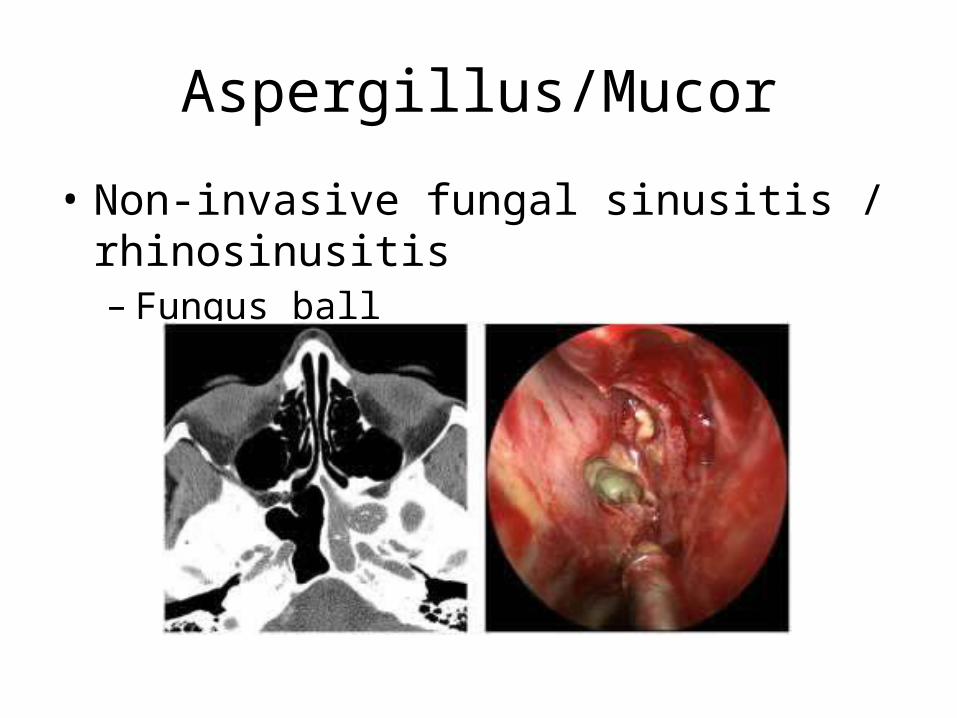
• Non-invasive fungal sinusitis / rhinosinusitis– Fungus ball
• Only described in adults in the literature• Immunocompetent patients• Aspergillus most common• Tangled mats of hyphae in one or more sinuses• Extramucosal disease• Maxillary sinus sphenoid sinus other sinuses• Symptom = Post-nasal d/c , asymptomatic• CT: heterogeneous opacification• Surgical removal by endonasal under endoscopic guidance
Aspergillus/Mucor
• Non-invasive fungal sinusitis / rhinosinusitis– Fungus ball

Aspergillus/Mucor
• Non-invasive fungal sinusitis / rhinosinusitis– Allergic fungal sinusitis
• Immunocompetent patients• Younger patient group < 30years• Hypersensitivity to fungus residing in mucous• Dematiaceous species• “allergic mucin” – eosinophilic mucin with or without fungus• Unilateral/Bilateral polyps with complete opacification of sinus cavity on
CT– Frequently bony expansion
• Diagnosis– Presence of hyphae in mucin
• Treatment– Prednisone, nasal steroids & removal of all mucin

Aspergillus/Mucor
• Non-invasive fungal sinusitis / rhinosinusitis– Allergic fungal sinusitis
Aspergillus/Mucor
• Invasive fungal rhinosinusitis– Chronic or indolent invasive fungal rhinosinusitis• Rare• Mostly in immuno-competent patients• Aspergillus most frequent• Pain = Main symptom• Chronic headache, proptosis, cranial nerve deficits• Maxillary sinus most commonly affected• Bony erosion extending to orbit or skull base

Aspergillus/Mucor
• Invasive fungal rhinosinusitis– Acute fulminant fungal rhinosinusitis• Immuno-compromised patients• Fatal outcome without prompt treatment• Mycotic infiltration of mucosa & sinuses• Initially: Fever of unknown origin or rhinorrhoea• Later: Proptosis, opthalmoplegia, CN palsies• Most common site: near middle turbinate, septum• Thrombosis & necrosis

Aspergillus/Mucor
• Invasive fungal rhinosinusitis– Acute fulminant fungal rhinosinusitis
NEOPLASTIC
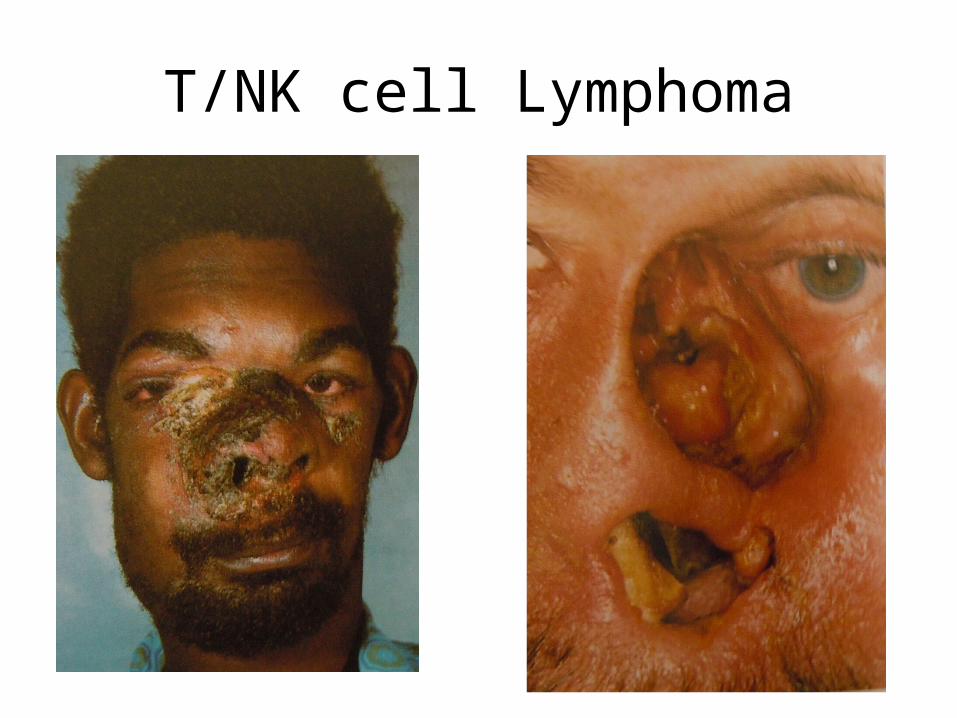
T/NK cell Lymphoma
• “midline destructive granuloma”• Classical destruction of the midface• Similar appearance of aggressive midfacial
destruction by cocaine abuse
• All decades of life (mean = 50years)• Both sexes• Association with EBV
T/NK cell Lymphoma
• 3 stages:– Prodromal• Persistent nasal obstruction & rhinorrhoea
– Second stage• Necrosis around nasal cavity• Purulent nasal d/c, crusting, tissue loss
– Terminal stage• Haemorrhage & gross mutilation of face• Eventually lead to death
T/NK cell Lymphoma

T/NK cell Lymphoma
• Diagnosis– Good quality representative biopsy beneath the slough &
crusts
• Imaging– Dramatic destruction of midline soft tissue & bone without
a gross tumour mass
– Treatment• Radical full course radiotherapy 55 Gy• Wide field coverage incl nose, sinuses & palate


















