Global Health: What Does it Mean for ENT?
14
1 Name: Declan Murphy Word count: 2998 Global Health: What Does it Mean for ENT? Introduction Global health is a term to describe the conduction of transnational research to identify variables that influence health, and the use of information gathered to inform evidence-based decisions which aim to improve health across the world. (1) In 2007, the World Health Organisation (WHO) outlined the main threats to global human health in the 21 st Century. (2) These include a rise in epidemic-prone diseases, foodborne diseases, accidental or deliberate outbreaks of infectious disease, toxic chemicals and radionuclear materials, and finally environmental disasters which influence health through multiple avenues. (2) An acute threat to global health is climate change. (3,4) Research demonstrates its direct and indirect influence on health. The greatest effect on health will arise from limited access to safe food and water, and dirtier air. Climate change is estimated to contribute to an additional 12.6 million death each year. (5) Otorhinolaryngology and Global health Ear, Nose and Throat (ENT) surgery, also called Otorhinolaryngology, is the surgical specialty concerned with the diagnosis, evaluation and management of head, neck, ear, nose and throat diseases. (6) ENT encompasses a vast disease spectrum, much of which is treatable through manoeuvres and medical management but equally, surgical intervention is often indicated. ENT disease prevalence, risk factors and treatment vary between developed and developing countries. Health provision, particularly surgery, in developing countries is poor and their healthcare systems are unstable. (7) Technological advances provide ENT surgery with novel diagnostic and treatment opportunities, however new technology is inaccessible to developing countries which further contributes to the great difference in ENT practice between the developed and developing world. (2,8) The American Academy of Otolaryngology has outlined the main ENT diseases requiring intervention in low- and middle-income countries (LMIC). These include thyroid and parathyroid disease, hearing loss, chronic ear disease, tracheostomy care and paediatric airway pathologies. (8) In this essay, I will outline key global health concerns in otorhinolaryngology, discuss why discrepancies in ENT services between developed and developing countries exist, provide an insight into future challenges for global otorhinolaryngology, and finally suggest methods to minimise ENT’s global burden. Hearing Loss In 2012 it was estimated that 5.3% of the world’s population were living with disabling hearing loss (DHL), defined as a hearing impairment greater than 40db when 15years or older, or greater than 30dB when younger than 15years. (9) The burden of hearing loss predominates in LMICs, particularly
Transcript of Global Health: What Does it Mean for ENT?

1
Name: Declan Murphy Word count: 2998
Global Health: What Does it Mean for ENT?
Introduction
Global health is a term to describe the conduction of transnational research to identify variables that
influence health, and the use of information gathered to inform evidence-based decisions which aim
to improve health across the world.(1)
In 2007, the World Health Organisation (WHO) outlined the main threats to global human health in
the 21st Century.(2) These include a rise in epidemic-prone diseases, foodborne diseases, accidental or
deliberate outbreaks of infectious disease, toxic chemicals and radionuclear materials, and finally
environmental disasters which influence health through multiple avenues.(2)
An acute threat to global health is climate change.(3,4) Research demonstrates its direct and indirect
influence on health. The greatest effect on health will arise from limited access to safe food and water,
and dirtier air. Climate change is estimated to contribute to an additional 12.6 million death each
year.(5)
Otorhinolaryngology and Global health
Ear, Nose and Throat (ENT) surgery, also called Otorhinolaryngology, is the surgical specialty
concerned with the diagnosis, evaluation and management of head, neck, ear, nose and throat
diseases.(6) ENT encompasses a vast disease spectrum, much of which is treatable through
manoeuvres and medical management but equally, surgical intervention is often indicated.
ENT disease prevalence, risk factors and treatment vary between developed and developing countries.
Health provision, particularly surgery, in developing countries is poor and their healthcare systems are
unstable.(7) Technological advances provide ENT surgery with novel diagnostic and treatment
opportunities, however new technology is inaccessible to developing countries which further
contributes to the great difference in ENT practice between the developed and developing world.(2,8)
The American Academy of Otolaryngology has outlined the main ENT diseases requiring intervention
in low- and middle-income countries (LMIC). These include thyroid and parathyroid disease, hearing
loss, chronic ear disease, tracheostomy care and paediatric airway pathologies.(8)
In this essay, I will outline key global health concerns in otorhinolaryngology, discuss why
discrepancies in ENT services between developed and developing countries exist, provide an insight
into future challenges for global otorhinolaryngology, and finally suggest methods to minimise ENT’s
global burden.
Hearing Loss
In 2012 it was estimated that 5.3% of the world’s population were living with disabling hearing loss
(DHL), defined as a hearing impairment greater than 40db when 15years or older, or greater than
30dB when younger than 15years.(9) The burden of hearing loss predominates in LMICs, particularly

2
Sub-Saharan Africa (SSA), south Asia, and the Asian pacific.(9) The prevalence of hearing loss decreases
exponentially as gross national income (GNI) increases, both for adults and children.(10)(figure 1) 48%
of adults over 65years in south Asia have DHL, compared with 18% of those from high-income
countries (HIC).(10,11)
Figure 1: The prevalence of Disabling hearing loss (<15yrs) decreases as GNI increases.(11)
Why does hearing loss matter?
Whether from a developed or underdeveloped country, chronic hearing loss in children impairs
speech and language development.(12) Disability and handicap results, for example through poor
educational and vocational attainment. Unemployment rates are higher in deaf adults, and those that
do achieve employment, usually receive a lower grade than the general population.(12) Children whose
hearing is impaired are more prone to experiencing emotional, sexual and physical abuse, including
murder.(12,13)
WHO estimates that unaddressed hearing loss has a global cost of 750 billion international dollars.(10)
Many causes of DHL are preventable and owing to its negative consequences, prevention is
paramount.
Hearing loss in developing countries
The prevalence of childhood DHL is higher in developing countries. 2.4% of children under 15 years of
age have DHL in South Asia, a low-income country, compared with 0.5% in HICs.(11) 80% of the world’s
deaf population receive no education, particularly skewed towards LMICs where almost all deaf
people don’t, causing devastating consequences for deaf childrens’ futures.(14)
Causes of hearing loss in children and adolescents

3
60% of DHL in children under 15yrs is preventable with a disproportionately high burden in LMICs
where 75% are preventable, compared with 49% in HICs.(10)
Infections are the main preventable cause.(15) They occur antenatally (rubella and syphilis) or during
infancy (mumps, measles and rubella). Persistent middle ear infections cause chronic suppurative
otitis media (CSOM), a condition affecting 330 million people worldwide. It is more common in LMICs,
accounting for roughly 25% of the ENT workload, where it is associated with higher complication rates
too.(10,15–17) Secondly, complications from childbirth may cause sensorineural hearing loss, usually
secondary to cerebral damage, which may result from birth asphyxia and hyperbilirubinaemia;
complications more commonly affect premature neonates.(10) Finally, ototoxicity is the third main
cause, most commonly arising from medication use in babies or pregnant mothers.(10)
Figure 2: Disabling hearing loss in adults 65yrs+.(11)
Hearing loss in adults
Although the proportional difference between LMICs’ and developed countries’ DHL prevalence is
largest in those under 15yrs old, adult populations differ too.(figure 2) Adult DHL is usually due to
disease originating from childhood, degenerative changes, and noise-induced DHL.
Noise-induced hearing loss is particularly prevalent in LMICs. Many LMICs are experiencing rapid
urbanisation and therefore increased noise exposure with minimal regulation.(18) Residents and
workers are exposed to high noise levels which contributes to the high prevalence of noise-induced
DHL.(12)
How can we minimise preventable causes of hearing loss in LMICs?
As many DHL cases in LMICs are preventable, we can intervene in various ways to reduce its incidence.
Self- and herd-immunity can be induced through providing childhood immunisations, particularly
against measles, mumps, rubella and bacterial meningitis.(10,12) Contraceptive access in LMICs is poor.
Therefore immunising women of reproductive age against rubella, screening pregnant females for

4
syphilis, and improving antenatal care all help reduce neonatal DHL.(10,12) HIV prevention would reduce
its influence on CSOM complication rates (OR 4.3, 95% CI; 1.17–15.6; p=0.028).(17) Implementing
newborn hearing screening programmes in LMICs would improve the early diagnosis and treatment
of sensorineural hearing loss. High quality ENT training for professionals, accessible primary health
care services, and up-to-date technology could prevent unsafe prescribing of ototoxic medication and
would allow disease to be identified at an early stage. Early disease identification would reduce the
prevalence of CSOM-associated complications that occur at an increased rate in prolonged and
untreated disease (OR 1.03, 95% CI; 1.007–1.05; p=0.01).(17)
Minimising noise exposure is essential. In the UK, The Control of Noise at Work Regulations 2005
ensures that employers reduce occupational noise to prevent it impairing their employees’ hearing.(19)
Pressure must be put on LMIC governments to create similar legislation, which often is lacking. If
environments and occupations cannot be altered, personal protective equipment must be available.
LMICs carry a larger proportion of DHL than developed countries but care is minute in
comparison.(20,21) Although small, progress has been made over the last decade, particularly primary
care health service expansion in LMICs with a focus on educating local people in the effective
management of ear diseases.(20–22)
Disease of the Nose, Pharynx and Larynx
A prospective cohort study assessed the burden of ENT disease in LMICs. Roughly 2600 patients were
assessed and followed-up for three years, all of whom presented to secondary care outpatient
departments and healthcare camps in an Indian farming community with high poverty rates.(21) All
diagnoses were made by trained professionals who decided whether ENT referral was indicated.
Roughly 8% had a nasal disorder, 50% attributable to acute rhinitis, likely due to working in masonry,
with paint, and around dust.(21)(figure 3) Seasonality showed an increasing incidence in winter.
8% had recurrent sinusitis, becoming chronic in all patients after three years or less.(21) Nasal polyposis
requiring surgery affected 10% of patients.(21)
19% of those with swallowing difficulty or hoarseness had chronic laryngitis and tonsillitis caused 49%
of throat pain.(21) Iron deficiency is epidemic in many LMICs due to diet, worm infections, malaria and
poor antenatal care.(23) As a result, Plummer Vinson’s syndrome - a triad of iron deficiency, atrophic
glossitis and oesophageal webs or strictures - was diagnosed in 23% of those with swallowing
difficulty.(21)

5
Figure 3: Nasal diseases in Vellore District of Tamil Nadu.(21)
Air pollution and LMICs
Air pollution is the contamination of any environment by substances (chemical, biological or physical)
that modify its natural characteristics.(24) With in-depth knowledge of the adverse impacts of air
pollution, developed countries have made successful efforts to reduce levels.(25) This is not the case in
LMICs. As industry has expanded, air pollution has remained high, and efforts have either minimally
reduced levels or they have remained static.(25)
Previous research has demonstrated a positive correlation between disease incidence and air
pollution concentrations. Respiratory and cardiovascular diseases particularly are associated, with
morbidity and mortality rates increasing.(25) NO2 and SO2, affect the upper airway and middle ear
causing inflammation, irritation and infection.(26,27) Higher levels of air pollution is associated with
increased incidence of head and neck cancer, which is discussed later.(28,29)
A study in Beijing evaluated the influence of air pollution on otolaryngology outpatient attendance.(27)
NO2 and SO2 concentrations showed positive associations with outpatient attendance.(27) Exposure to
air pollution early in life increases the risk to both upper and lower respiratory tract infections in
children, including middle ear infection.(30,31) Exposure to a combination of pollutants accelerates the
onset of allergic rhinitis, particularly inducing exacerbations.(27) These findings are consistent with
other studies.(30–32)
Data on air pollution’s influence on ENT disease is limited. Higher air pollutant concentrations in
developing countries may suggest that LMICs suffer greater air pollution associated ENT disease
burden than HICs. Further research is required for confirmation.

6
Head and Neck Cancer
Head and neck cancers (HNC) are the sixth most common cancer worldwide.(33) Two thirds of the
global burden of HNCs occur in LMICs, and the Indian subcontinent alone is responsible for one third
of lip and oral cavity cancers.(29)
The incidence of HNCs is increasing globally, particularly among women, likely due to increased alcohol
and tobacco use, and improved diagnostic capabilities.(29,34) Alcohol and tobacco use remain the
greatest risk factors for laryngeal cancer. Tobacco primarily influences disease at the vocal cords and
glottis, and alcohol mainly in the supraglottic region. Synergism is evident between HNC risk factors,
particularly tobacco use (smoking and smokeless), Gutka chewing as it contains Areca nut, alcohol
consumption, and oral Human papillomavirus (HPV) infections.(35)
Smoking
Over the last 10yrs tobacco use has been increasing by 2-3% per year in India, and is expected to be
responsible for 13% of all deaths there by 2020.(36) In LMICs, cancer of the oral cavity and throat is one
of the commonest causes of death; the Aizawl district has the highest incidence of pharyngeal and
tongue cancer in the world, 11.5/100,000 and 7.6/100,000 respectively.(33)
Alcohol
In most LMICs, alcohol is consumed infrequently but heavily.(37) Moderate and heavy alcohol use
increases the risk to cancers, including cancer of the larynx, with a systematic review demonstrating a
risk-ratio of 1.44 (95% CI 1.25–1.66) for moderate consumption and 2.65 (95% CI 2.19–3.19) for heavy
consumption.(37,38) Through lack of education, LMIC inhabitants are less aware of alcohol’s negative
consequences and alcohol cessation strategies tend to fail.(37)
Air pollution and HNC
High levels of air pollution is associated with an increased risk to developing HNC.(28) 74% of the Indian
population relies on solid fuels, greatly contrasting that of HICs, where in April 2017 Britain generated
all electricity without using any coal.(39) India is using increasing quantities of coal, rising at a rate of
2.8% each year.(28,40)
A retrospective case-control study investigated how exposure to air pollution from solid fuels affects
the incidence of laryngeal and hypopharyngeal cancer.(28) Exposure to burning coal indoors for over
50yrs increased the risk of developing hypopharyngeal (OR 3.47, CI 0.95–12.69) and laryngeal (OR
3.65, CI 1.11–11.93) cancers.(28) Other solid fuels such as wood increased the risk to hypopharyngeal
cancer too (OR 1.62, CI 1.14–2.32) but not in never-smokers.(28)
Human Papillomavirus (HPV) and HNC
HPV is present in 50% of Squamous cell carcinomas (SCC) of the head and neck, particularly affecting
the tongue and tonsils.(33) Changing oral sexual practices and the presence of high-risk HPV genotypes
increase the frequency of HPV-associated HNCs in LMICs. These particularly affect younger patients
and aren’t sex-specific.(33) HPV is present in 16% of oral and laryngeal cancers in HICs; this is fewer than
in LMICs, especially India where prevalence ranges from 33.6% to 67%.(41)
By understanding the biology of HPV-associated cancers, there is no reason to suggest that the HPV
vaccine’s protective properties would differ in efficacy between HNC and anogenital cancer.(42) HPV

7
vaccinations for genotypes 16 and 18 could prevent over 90% of HPV-associated oropharyngeal
cancers, supporting the argument that males should be vaccinated too, owing to their higher risk for
HPV-associated HNC.(42,43)
HPV vaccines are widely available in high-income and some middle-income countries. Although one
of the most-cost effective methods for disease prevention, vaccines are rarely available in low-income
countries.(44,45) For vaccines to become widely available, substantial financial subsidies must be
provided. Recently, Ministries of Health and non-governmental organisations (NGO) have used
donated vaccinations to try and improve conditions.(44) Although a good effort, governmental and
international projects are essential otherwise HPV-associated HNC rates are unlikely to fall.
HNC care improvements in the developing world
Steps must be taken to both prevent and manage HNC in LMICs. Primary preventative initiatives such
as international media campaigns to raise awareness of the current HNC crisis, taxing tobacco and
alcohol use, designating smoke-free areas, vaccinations, ventilation for buildings, and safe-sex
programmes are essential. Secondary prevention by appropriately training professionals to manage
HNCs and encouraging smoking cessation would help too.
Climate change and ENT
With the beginning of the industrial revolution, humans have released gases into the lower
atmosphere that trap energy and contribute to global warming by amplifying the Earth’s natural
greenhouse effect.(46) As the Earth continues to warm our climate changes, and its effect on human
life and health already is evident.
Climate change has been referred to as one of the greatest risks to human health, and between 2030
and 2050 is predicted to cause around 250000 deaths per year.(47) Figure 4 outlines how climate
change affects human health.
Climate change’s health impact will be felt across the globe, most prominently however, in LMICs.
LMICs already have weak health infrastructures, particularly for ENT services, and damage for example
through loss of land and overcrowding, will impair its ability to cope.(47) Changes in air pollution and
aeroallergen concentrations will affect otorhinolaryngeal disease, and changes in the distribution of
vector organisms will predispose to infectious disease, including those of the nasopharynx, ear, and
paediatric airway.(3,46,48)

8
Figure 4: Diagrammatic depiction of the mechanisms through which climate change can affect human
health.(46)
How can we improve ENT Global Health for the future?
The ENT disease burden predominates in developing countries, unfortunately being a prime example
of the inverse care law in action. Although not to the same extent as in developed countries, the
population in LMICs is ageing. Along with ageing comes an increased disease burden, increasing
demands on health services, rationing of treatment, and longer waiting times. Although interventions
such as an ENT training programme established in SSA showed promise, there was minimal
improvement in the population’s ENT health as the community’s population grew at a rate that
overwhelmed new services after just six years.(49) It seems that improved education and
communication, humanitarian efforts, and introducing self-sustaining healthcare infrastructures are
necessary approaches to reduce the global burden of ENT diseases.
Education and communication
Both public and staff in LMICs are insufficiently educated in the prevention, diagnosis, treatment, and
rehabilitation of ENT disease. Public behaviours increase the population’s risk to disease and health
care is of insufficient quality and quantity.(50) This is due to poor local training and the migration of
professionals.(50) Therefore, LMICs become dependent on the importation of external practitioners
who they cannot afford.(50) International bodies must help to fund training programmes for local
people, as done rather successfully in Malawi by Mulwafu et al.(22) Being trained to deliver
preventative healthcare, such as vaccinations and contraception, is essential.
Innovative low-cost methods for training are needed. Clark et al(51) developed an ear trainer for low-
resource settings which recently has been validated as a realistic representation of the ear for
microsurgical training. GoogleGlass is a company that has streamed live surgical operations online
using a camera attached to spectacles.(52) In 2014, its first operation was live-streamed to 13000

9
surgical students from 115 different countries. Students had their questions answered by the surgeon
in real-time, representing a cornerstone in transnational education and providing promise for future
training in LMICs.(53)
Telemedicine, the use of electronic information and technology to provide healthcare when distance
separates the patient from the professional, should be utilised as an affordable way to communicate
with, and provide care to, LMICs which often have limited transport opportunities.(54,55)
Humanitarian efforts
Although most aid is provided vertically, when trying to establish a sustainable healthcare system,
horizontal aid should predominate.(56) Financial cooperation from multiple bodies is required to
establish a sustainable healthcare system in LMICs. Independent donors, universities, ministries, and
both governmental and NGOs must contribute so healthcare professionals can be recruited and
resources made available.(57)
Healthcare infrastructure
A sustainable health system requires robust financing, a well-trained workforce who are paid
appropriately, an evidence-base to assist in decision-making, technology sufficient to diagnose and
treat disease, and a system to deliver medicine and technology to patients.(50) Most LMIC’s healthcare
systems underachieve in all of these categories for various reasons.(50)
Healthcare systems operate in numerous ways. To maximise the population’s health for the lowest
cost, most funding should target high-quality primary care service provision with a focus on disease
prevention.(58) This is difficult to implement however as privately-run services often provide treatment
for established disease and thus prevention strategies are of little interest. The role of NGOs is not
simply to ‘fill gaps’ in health care; they can provide large-scale innovative health programmes.(59) NGOs
face challenges. They are dependent on donors, often lack a strategic plan and often have conflicting
political governance. Governments are often focused on short-term public popularity with short-term
objectives. Along with other political motives such as pressure from big businesses (pharmaceutical,
tobacco and alcohol), convincing governments to prioritise the long-term commitment towards
establishing an effective disease prevention strategy is challenging.

10
References:
1. Beaglehole R, Bonita R. What is global health? Glob Health Action. 2010 Apr 6;3:
10.3402/gha.v3i0.5142.
2. World Health Organization. World Health Report: Global Public Health Threats in the 21st
Century. WHO; 2013
3. CDC. Climate Change and Public Health - Climate Effects on Health. Centers for Disease
control and Prevention. 2016. Available from:
https://www.cdc.gov/climateandhealth/effects/default.htm [cited 2017 Aug 24]
4. Balbus J, Crimmins A, Gamble JL. Human health the impacts of climate change on in the united
states. U.S. Global Change Research Program. 2016
5. World Health Organization. Climate change and human health: Protecting health from climate
change. World Health Organization; 2017
6. NHS Careers. Otorhinolaryngology (ear, nose and throat surgery, ENT) Health Careers.
Available from: https://www.healthcareers.nhs.uk/explore-roles/surgery/ear-nose-throat-
surgery. [cited 2017 Aug 24]
7. Chao TE, Mandigo M, Opoku-Anane J, Maine R. Systematic review of laparoscopic surgery in
low- and middle-income countries: benefits, challenges, and strategies. Surgical endoscopy.
2016 Jan;30(1):1-10. doi: 10.1007/s00464-015-4201-2.
8. American Academy of Otolaryngology. Otolaryngology in Global Health. American Academy
of Otolaryngology - Head and Neck Surgery. 2017. Available from:
http://www.entnet.org/content/otolaryngology-global-health [cited 2017 Aug 24]
9. World Health Organisation. Prevention of Blindness and Deafness: Estimates. World Health
Organization; 2012. Available from: http://www.who.int/pbd/deafness/estimates/en/ [cited
2017 Aug 13].
10. World Health Organisation. Deafness and hearing loss. WHO. 2017. Available from:
http://www.who.int/mediacentre/factsheets/fs300/en/ [cited 2017 Aug 24]
11. World Health Organisation. WHO Global estimates on prevalence of hearing loss: mortality and
Burden of Diseases and Prevention of Blindness and Deafness, WHO. 2012
12. Olusanya BO, Neumann KJ, Saunders JE. The global burden of disabling hearing impairment: a
call to action. WHO; 2014;92:367-373.
13. Jones L, Bellis MA, Wood S, Hughes K, McCoy E, Eckley L.. Prevalence and risk of violence
against children with disabilities: a systematic review and meta-analysis of observational
studies. Lancet; 2 2012 Sep 8;380(9845):899-907.
14. WFD, Human Rights. World federation of the deaf. 2016. Available from:
https://wfdeaf.org/human-rights/ [cited 2017 Aug 24]
15. DeAntonio R, Yarzabal J-P, Cruz JP, Schmidt JE, Kleijnen J. Epidemiology of otitis media in
children from developing countries: A systematic review. International Journal of Pediatric

11
Otorhinolaryngology; 85;2016; 65–74.
16. Orji F. A survey of the burden of management of chronic suppurative otitis media in a
developing country. Annals of Medical and Health Sciences Research; 2013 Oct;3(4):598-601.
17. Mushi MF, Mwalutende AE, Gilyoma JM, Chalya PL, Seni J, Mirambo MM. Predictors of disease
complications and treatment outcome among patients with chronic suppurative otitis media
attending a tertiary hospital, Mwanza Tanzania. BMC Ear, Nose and Throat Disorders. 2016 Jan
7;16:1
18. Schwela D, Finegold LS, Stewart J. A strategic approach on environmental noise management
in developing countries. 9th International Congress on noise as a Public health Problem. 2008
19. HSE. The Control of Noise at Work Regulations. Health and Safety Executive. 2005. Available
from: http://www.hse.gov.uk/noise/regulations.htm [cited 2017 Aug 24]
20. Harris MS, Dodson EE. Hearing health access in developing countries. Current Opinion in
Otolaryngology and Head and Neck Surgery. 2017; Jul 3.
21. Emerson LP, Job A, Abraham V. A model for provision of ENT health care service at primary and
secondary hospital level in a developing country. Biomed Research International;
2013;2013:562643
22. Mulwafu W, Nyirenda TE, Fagan JJ, Bem C, Mlumbe K, Chitule J. Initiating and developing
clinical services, training and research in a low resource setting: the Malawi ENT experience.
Tropical doctor. 2014 Jul;44(3):135-9.
23. World Health Organisation. Micronutrient deficiencies: Iron Deficiency Anaemia. WHO. 2015.
Available from: http://www.who.int/nutrition/topics/ida/en/ [cited 2017 Aug 24]
24. World health organisation. Air pollution. WHO. 2016. Available from:
http://www.who.int/topics/air_pollution/en/ [cited 2017 Aug 24]
25. Chen B, Kan H. Air pollution and population health: a global challenge. Environmental Health
and Preventative Medicine;2008 Mar;13(2):94-101.
26. Njoroge GN, Bussmann RW. Traditional management of ear, nose and throat (ENT) diseases in
Central Kenya. Journal of Ethnobiology and Ethnomedicine; 2006; 2: 54.
27. Zhang F, Xu J, Zhang Z, Meng H, Wang L, Lu J. Ambient air quality and the effects of air pollutants
on otolaryngology in Beijing. Environmental Monitoring and Assessment. 2015, 187:495.
28. Sapkota A, Gajalakshmi V, Jetly DH, Roychowdhury S, Dikshit RP, Brennan P. Indoor air pollution
from solid fuels and risk of hypopharyngeal/laryngeal and lung cancers: a multicentric case-
control study from India. International Journal of Epidemiology. 2008 Apr;37(2):321-8
29. Gupta B, Johnson NW, Kumar N. Global Epidemiology of Head and Neck Cancers: A Continuing
Challenge. Oncology. 2016;91:13-23.
30. Aguilera I, Pedersen M, Garcia-Esteban R, Ballester F, Basterrechea M, Esplugues A. Early-Life
Exposure to Outdoor Air Pollution and Respiratory Health, Ear Infections, and Eczema in Infants
from the INMA Study. Environmental Health Perspectives. 2012 Dec 5;121(3).
12
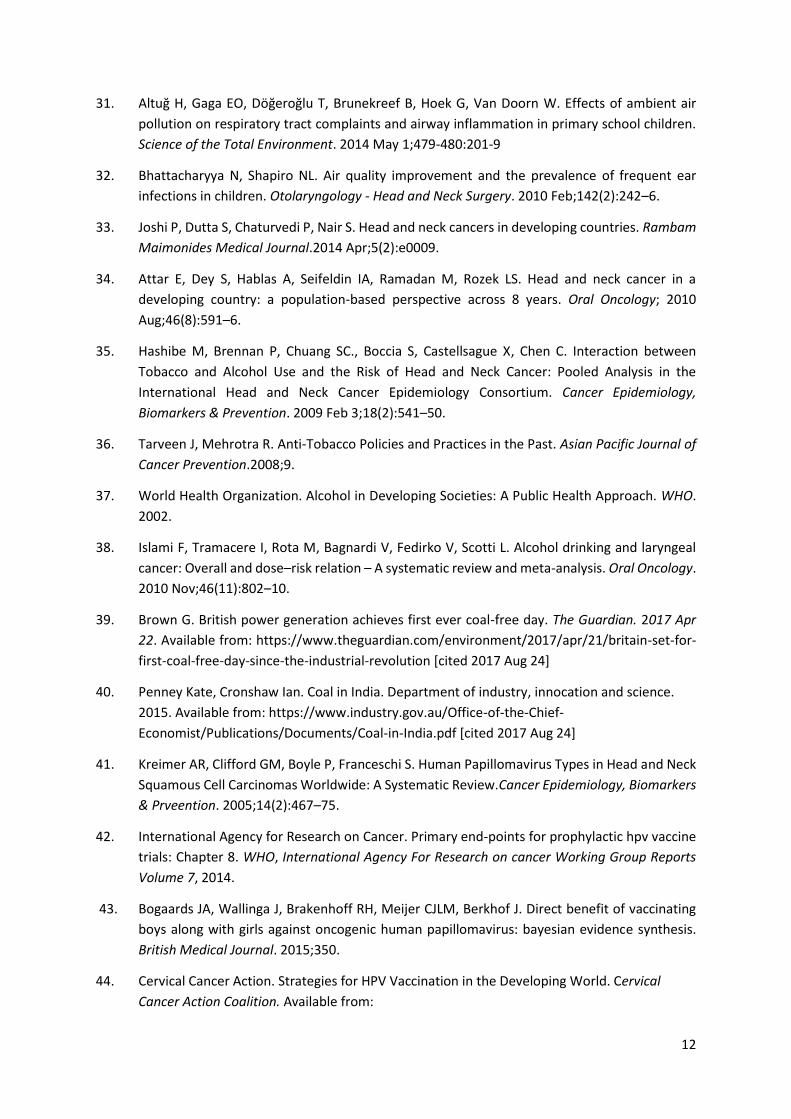
31. Altuğ H, Gaga EO, Döğeroğlu T, Brunekreef B, Hoek G, Van Doorn W. Effects of ambient air
pollution on respiratory tract complaints and airway inflammation in primary school children.
Science of the Total Environment. 2014 May 1;479-480:201-9
32. Bhattacharyya N, Shapiro NL. Air quality improvement and the prevalence of frequent ear
infections in children. Otolaryngology - Head and Neck Surgery. 2010 Feb;142(2):242–6.
33. Joshi P, Dutta S, Chaturvedi P, Nair S. Head and neck cancers in developing countries. Rambam
Maimonides Medical Journal.2014 Apr;5(2):e0009.
34. Attar E, Dey S, Hablas A, Seifeldin IA, Ramadan M, Rozek LS. Head and neck cancer in a
developing country: a population-based perspective across 8 years. Oral Oncology; 2010
Aug;46(8):591–6.
35. Hashibe M, Brennan P, Chuang SC., Boccia S, Castellsague X, Chen C. Interaction between
Tobacco and Alcohol Use and the Risk of Head and Neck Cancer: Pooled Analysis in the
International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiology,
Biomarkers & Prevention. 2009 Feb 3;18(2):541–50.
36. Tarveen J, Mehrotra R. Anti-Tobacco Policies and Practices in the Past. Asian Pacific Journal of
Cancer Prevention.2008;9.
37. World Health Organization. Alcohol in Developing Societies: A Public Health Approach. WHO.
2002.
38. Islami F, Tramacere I, Rota M, Bagnardi V, Fedirko V, Scotti L. Alcohol drinking and laryngeal
cancer: Overall and dose–risk relation – A systematic review and meta-analysis. Oral Oncology.
2010 Nov;46(11):802–10.
39. Brown G. British power generation achieves first ever coal-free day. The Guardian. 2017 Apr
22. Available from: https://www.theguardian.com/environment/2017/apr/21/britain-set-for-
first-coal-free-day-since-the-industrial-revolution [cited 2017 Aug 24]
40. Penney Kate, Cronshaw Ian. Coal in India. Department of industry, innocation and science.
2015. Available from: https://www.industry.gov.au/Office-of-the-Chief-
Economist/Publications/Documents/Coal-in-India.pdf [cited 2017 Aug 24]
41. Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human Papillomavirus Types in Head and Neck
Squamous Cell Carcinomas Worldwide: A Systematic Review.Cancer Epidemiology, Biomarkers
& Prveention. 2005;14(2):467–75.
42. International Agency for Research on Cancer. Primary end-points for prophylactic hpv vaccine
trials: Chapter 8. WHO, International Agency For Research on cancer Working Group Reports
Volume 7, 2014.
43. Bogaards JA, Wallinga J, Brakenhoff RH, Meijer CJLM, Berkhof J. Direct benefit of vaccinating
boys along with girls against oncogenic human papillomavirus: bayesian evidence synthesis.
British Medical Journal. 2015;350.
44. Cervical Cancer Action. Strategies for HPV Vaccination in the Developing World. Cervical
Cancer Action Coalition. Available from:

13
http://www.rho.org/files/CCA_HPV_vaccination_strategies.pdf [cited 2017 Aug 24]
45. Lahariya C. Vaccine epidemiology: A review. Journal of Family medicine and Primary Care.
2016;5(1):7–15.
46. Mcmichael AJ, Campbell-Lendrum DH, Corvalán CF, Ebi KL, Githeko AK, Scheraga JD. Climate
change and human health. WHO. 2003. Available from:
http://www.who.int/globalchange/publications/climchange.pdf [cited 2017 Aug 24]
47. World Health Organization. Climate change and health. WHO. 2017. Available from:
http://www.who.int/mediacentre/factsheets/fs266/en/ [cited 2017 Aug 24]
48. Ebi KL, McGregor G. Climate Change, Tropospheric Ozone and Particulate Matter, and Health
Impacts. Environmental Health Perspectives. 2008 Jul 10;116(11):1449–55. A
49. Mulwafu W, Ensink R, Kuper H, Fagan J. Survey of ENT services in sub-Saharan Africa: little
progress between 2009 and 2015. Global Health Action. 2017 Jan 9;10(1):1289736.
50. EPRS. Strengthening Health Systems In Developing Countries [Internet]. European
Parliamentary Research Service Blog. 2015; Available from:
epthinktank.eu/2015/02/10/strengthening-health-systems-in-developing-countries/ [cited
2017 Aug 24]
51. Clark MPA, Westerberg BD, Mitchell JE. Development and validation of a low-cost microsurgery
Ear Trainer for low-resource settings. The Journal of Laryngology and Otology;.2016 Oct
24;130(10):954–61.
52. Developers G. Glass at Work. GoogleGlass. 2017; Available at: https://www.x.company/glass/
[cited 2017 Aug 24]
53. Smith R. First operation streamed live with surgeon wearing Google glass. The Telegraph. 2014.
Available from: http://www.telegraph.co.uk/news/health/news/10851116/First-operation-
streamed-live-with-surgeon-wearing-Google-glass.html [cited 2017 Aug 24]
54. Field MJ. Telemedicine: A Guide to Assessing Telecommunications on Health Care. Institute of
Medicine (US) Committee on Evaluating Clinical Applications of Telemedicine; 1996
55. Combi C, Pozzani G, Pozzi G. Telemedicine for Developing Countries A Survey and Some Design
Issues. Application of Clinical Infectious Diseases. 2016;718518(7):1025–50.
56. World Health Organization. Vertical–horizontal synergy of the health workforce. WHO.
Available from: http://www.who.int/bulletin/volumes/83/4/editorial10405/en/ [cited 2017
Aug 24]
57. Maeseneer J De, Weel C van, Egilman D, Mfenyana K, Kaufman A, Sewankambo N, et al.
Funding for primary health care in developing countries. British Medical Journal. 2008
;336(7643).
58. World health Organization. What are the advantages and disadvantages of restructuring a
health care system to be more focused on primary care services? WHO. 2004; Available from:
http://www.euro.who.int/__data/assets/pdf_file/0004/74704/E82997.pdf [cited 2017 Aug
24]

14
59. Mercer A, Khan MH, Daulatuzzaman M, Reid J. Effectiveness of an NGO primary health care
programme in rural Bangladesh: evidence from the management information system. Health
Policy and Planning;2004;19(194):187–98.


![Education Matters. School related words What are books divided into? What does [ / ] mean? What does [ - ] mean? What does [ * ] mean? What are English,](https://static.fdocuments.net/doc/165x107/56649e575503460f94b4fc24/education-matters-school-related-words-what-are-books-divided-into-what-does.jpg)