GI and Hepatobiliary lecture
91
THE GASTROINTESTI NAL AND HEPATOBILIARY SYSTEMS Barry University NUR 313
-
Upload
michelle-harris -
Category
Education
-
view
392 -
download
3
Transcript of GI and Hepatobiliary lecture

THE
GASTROINTESTI
NAL AND
HEPATOBILIARY
SYSTEMS
Barry University NUR 313
Objectives
At the completion of this lecture, the students will
be able to:
Describe the structure and function of the
gastrointestinal system
Verbalize the difference between the upper,
middle and lower GI tract.
Understand various disorders of the GI system
such as GERD, peptic ulcer disease, hepatitis,
pancreatitis, and gastroenteritis.
Describe diagnostic tests and treatments related
to various disorders of the GI system.
2
Structure and Function
Major Physiological Functions of the GI
system
Digestion of food
Absorption of nutrients into the blood stream
Motility, Secretion, Digestion, absorption
3
Structure and Function
GI tract is divided into 3 parts:
Upper: mouth, esophagus and stomach
Intake source
Middle: duodenum, jejunum and ileum
Digestion and absorption
Lower: cecum, colon, rectum
Storage and elimination
4
Structure and Function
Esophagus: straight, tube about 10 inches in
length
Smooth muscle layers with peristaltic movements
to move food
Connects oropharynx to stomach
Upper Pharyngoesophageal sphincter keeps air
from entering esophagus and stomach during
breathing
Lower Gastroesophageal Sphincter prevents
reflux of gastric contents
5
Stucture and Function
Stomach
Pouch-like structure on left side of
abdomen serves as food storage
Pyloric sphincter controls rate of
stomach emptying and prevents
regurgitation of intestinal contents back
into stomach
6

7
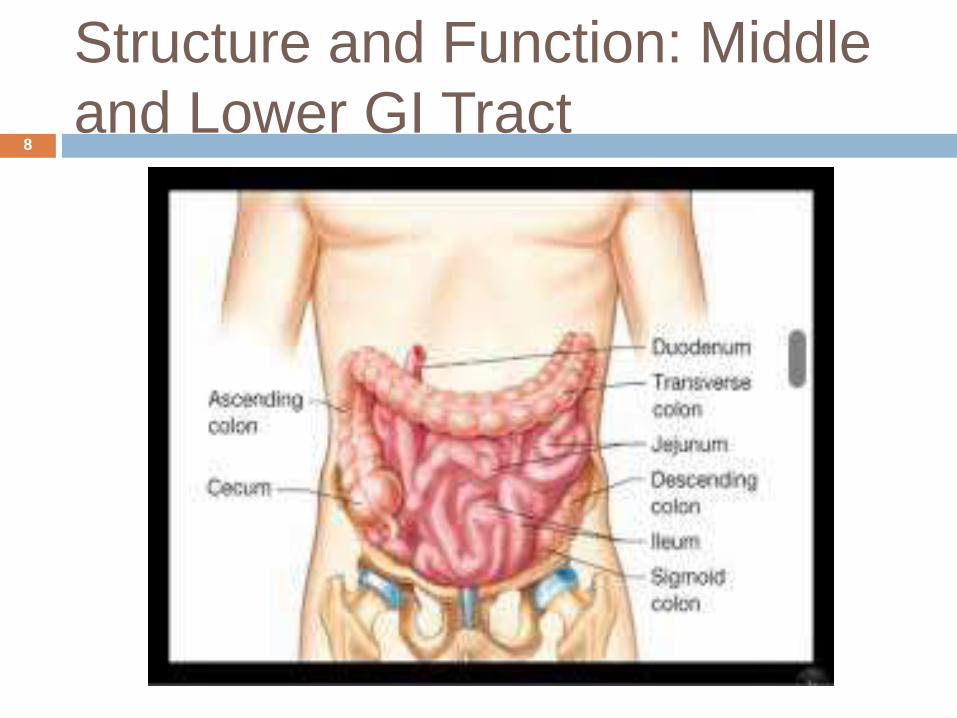
Structure and Function: Middle
and Lower GI Tract8
Structure and Function: Motility
Rhythmic intermittent contractions – mixing
and moving food
Esophagus, upper stomach, small intestines
Tonic movements is a constant contractions
Lower esophagus, ileocecal valve, anal sphincter
Autonomic nervous system
SNS
PNS
9
Structure and Function
Hormones:
Gastrin: stimulates gastric acid, blood flow
Cholecystokinin (CCK): Contraction of gallbladder
and secretion of pancreatic enzymes
Secretin: inhibits gastric acid secretion; stimulates
secretion of water from the pancreas
Ghrelin: peptide hormone stimulates food intake
and digestive function (appetite)
10
Digestion and Absorption
Digestion: The process of dismantling
food into parts
Requires hydrolysis, enzyme
cleavage, fat emulsification
Absorption: moving nutrients from
external intestinal lumen to internal
environment.
11
Disorders of the GI and Hepatobiliary
systems
Gastroesophageal
Reflux Disease
(GERD)
Peptic Ulcer
Disease
Gastroenteritis
IBD – Crohn’s &
Ulcerative Colitis
Diverticular Disease
Appendicitis
Intestinal
Colorectal CA
Peritonitis
Hepatitis
Cirrhosis
Liver Failure
Cholecystitis
Pancreatitis
12

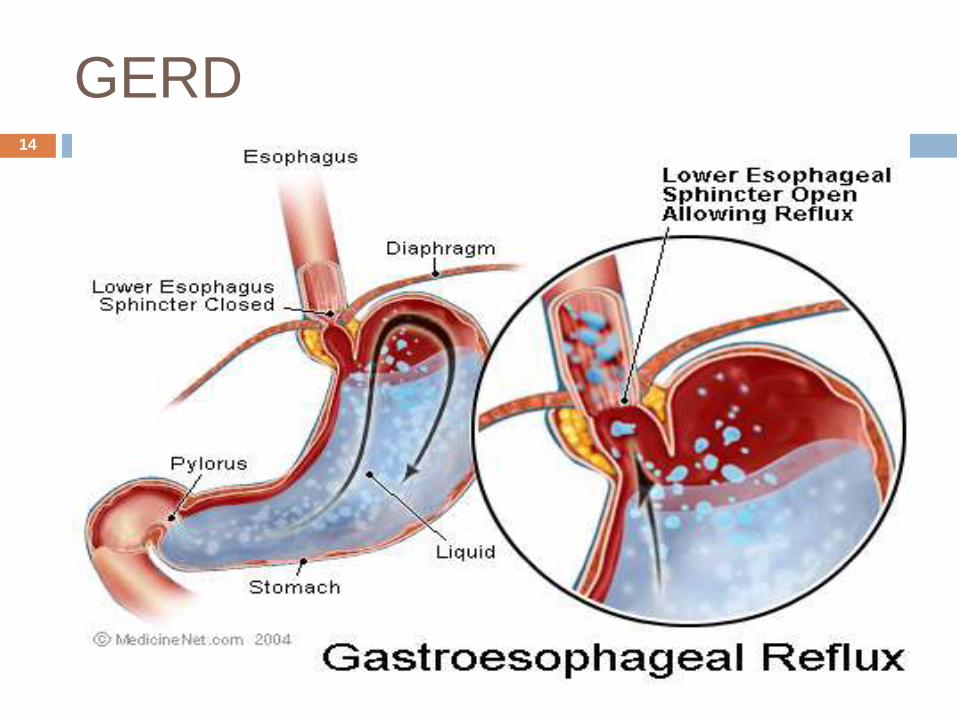
Gastroesophageal Reflux Disease
Reflux of gastric contents into esophagus
as a result of
Reduction in lower esophageal sphincter
tone
Delayed gastric emptying
Increase gastric acid secretion
Irritation of esophageal mucosa
13
GERD
GERD14
Risk Factors
Factors which reduce LES tone
Aging
Obesity
Pregnancy
High fat meals
15
Signs and Symptoms
Pyrosis (heartburn) cardinal symptom
Belching
Atypical Symptoms
Esophageal pain referred to the neck,
mid-back, upper abdomen
Chest pain
Chronic cough, wheezing, Hoarseness
Chronic sore throat, dysphagia
16
Diagnosis
History and physical alone if symptoms
are typical
Endoscopy and biopsy if symptoms are
atypical
Complications
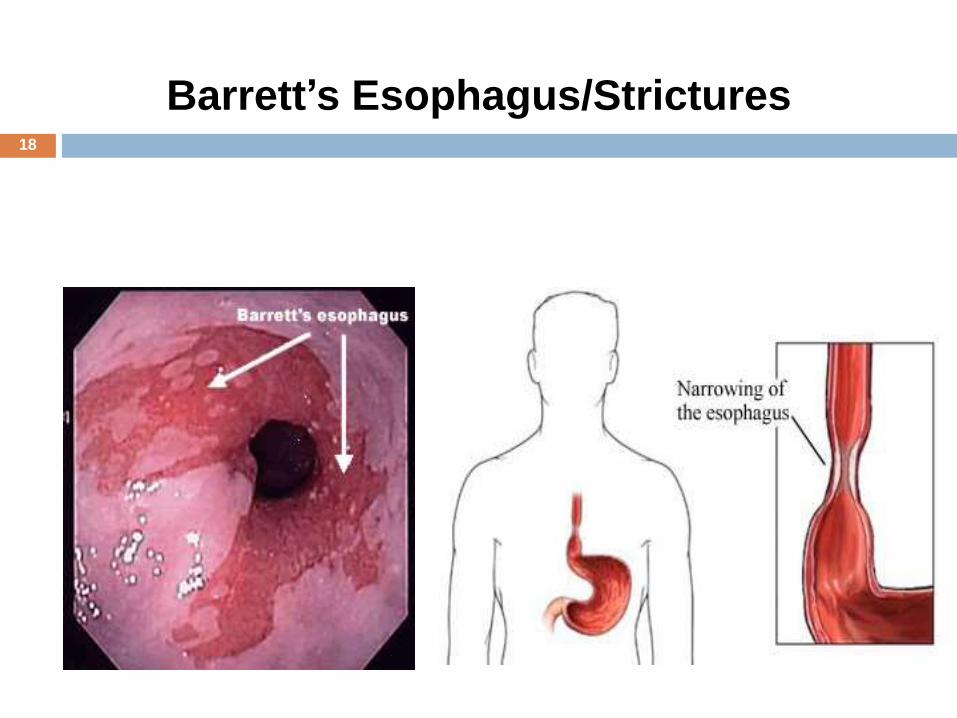
Barrett’s esophagus
Strictures
17
18
Barrett’s Esophagus/Strictures
Treatment
Medication
Avoid recumbence after eating
Elevate head of bed when sleeping
Reduce size of meals
Reduce fat, acid, spices, caffeine, sweets,
peppermints, chocolate, and alcohol
Avoid constrictive garments
19
Peptic Ulcer Disease
A group of ulcerative disorders that occur in
areas of the upper gastrointestinal tract that
are exposed to acid-pepsin secretions
Erosion of the gastric membrane
Gastric ulcers
Duodenal ulcers
Stress ulcers- Curling’s ulcer
20

Gastric Ulcer21
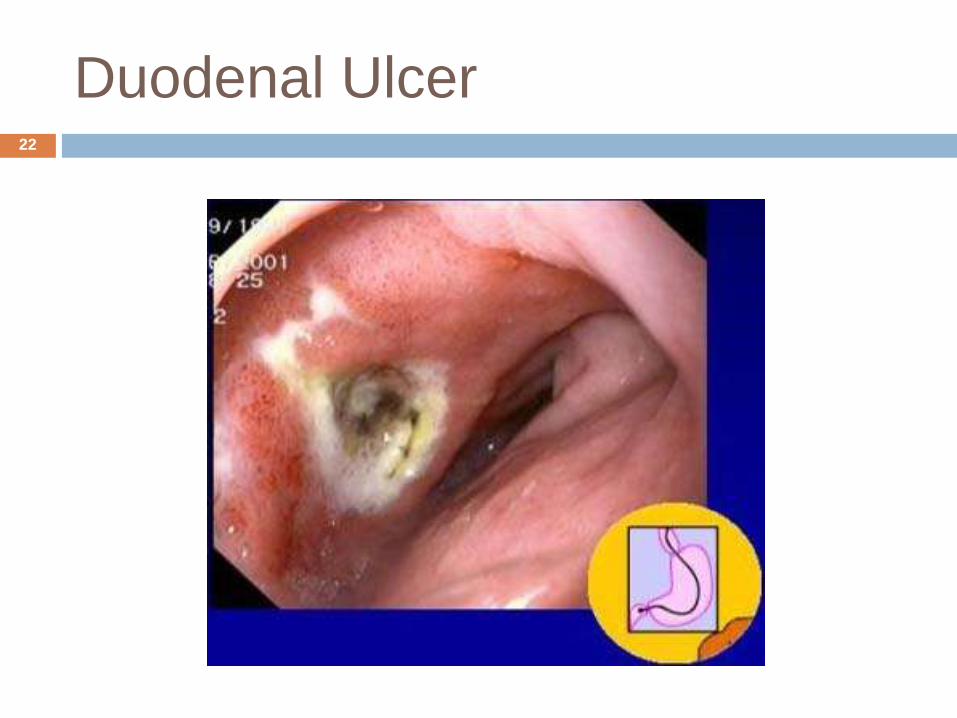
Duodenal Ulcer22
Risk Factors
Helicobacter pylori (H-Pylori) infection
90-95% of patients with duodenal
ulcers
60-70% of patients with gastric
ulcers
NSAIDs
aspirin
23
Signs and Symptoms
Pain
Burning, gnawing, cramp-like
Frequently when stomach empty
Midline epigastric, near xiphoid…may
radiate to back or right shoulder
Relieved by foods or antacids
Periodicity: daily for weeks, then remits
until next occurrence
24
Complications
Bleeding
Hematemesis
Coffee ground emesis
Hematochezia
Melena
Occult bleeding
Gastric Outlet Obstruction
Caused by edema, spasm, scar tissue
Perforation
Peritonitis
25
TREATMENT
Antibiotics for H-Pylori
Proton pump inhibitors (protonix), H2 Blockers
(pepcid)
Bismuth (Maalox, pepto bismol)
Avoid symptom triggers
Alcohol
High fat
Tobacco
Spicy food
26
Infectious Enterocolitis
Acute infection causing inflammation of the
intestinal linings resulting in vomiting, diarrhea,
and fever.
Etiology
Infection is by fecal-oral route.
Risk Factors
Improper hand washing and food preparation
Day care center attendance (children)
Recent use of antibiotics
27
Infectious Agents
Rotavirus
Clostridium difficile (C-diff)
pseudomembraneous colitis→ toxic
megacolon!
Staphylococcus aureus
Escherichia coli (E-coli)
Shigella
Salmonella
Campylobacter
Giardia lamblia
28
Symptoms
Diarrhea and abdominal pain
Treatment
Supportive for 48 hours
Avoid anti-diarrheal agent
Rehydrate! – especially in pediatric and geriatric population
Stool for WBC, stool cultures, stool for ova, cysts, and parasites
Monitor hydration with BUN, urine specific gravity, electrolytes.
29
INFLAMMATORY BOWEL
DISEASE (IBD)
Idiopathic chronic disorders of the GI
tract distinguished by the recurrent
inflammatory involvement of intestinal
segments.
Two main types
Crohn’s disease
Ulcerative colitis (UC)
30
Incidence
Peak age of onset 20-30’s (Crohn’s), and
30’s(UC)
Family history
Genetic predisposition – triggered by dietary
antigen or microbial agent
31
Crohn’s Disease
Definition Granulomatous inflammatory lesions of the GI tract.
Location Mouth to anus. Mostly small intestine & proximal colon.
Pattern “cobblestone” inflammatory appearance of submucosal
layer Skip lesions if multiple
Manifestations Intermittent diarrhea, steatorrhea, colicky pain, weight loss,
F/E imbalances, nutritional deficiencies, malaise, low-grade fever.
Complications: anal & perianal fistulas, abscesses, intestinal obstruction
32

33

Crohn’s Disease34
Diagnosis
H&P
Sigmoidoscopy & Colonoscopy with biopsy:
inflammation; biopsy often reveals
granulomatous inflammation
X-rays
CT scan
Sedimentation rate: elevated
CBC: possible anemia
Electrolytes: imbalances
35
TREATMENT
Gastroenterologist referral
Corticosteroids
Immunosuppressants
Antibiotics- Metronidazole (Flagyl)
Nutritious diet; residue free/bulk free to allow
bowel rest
36
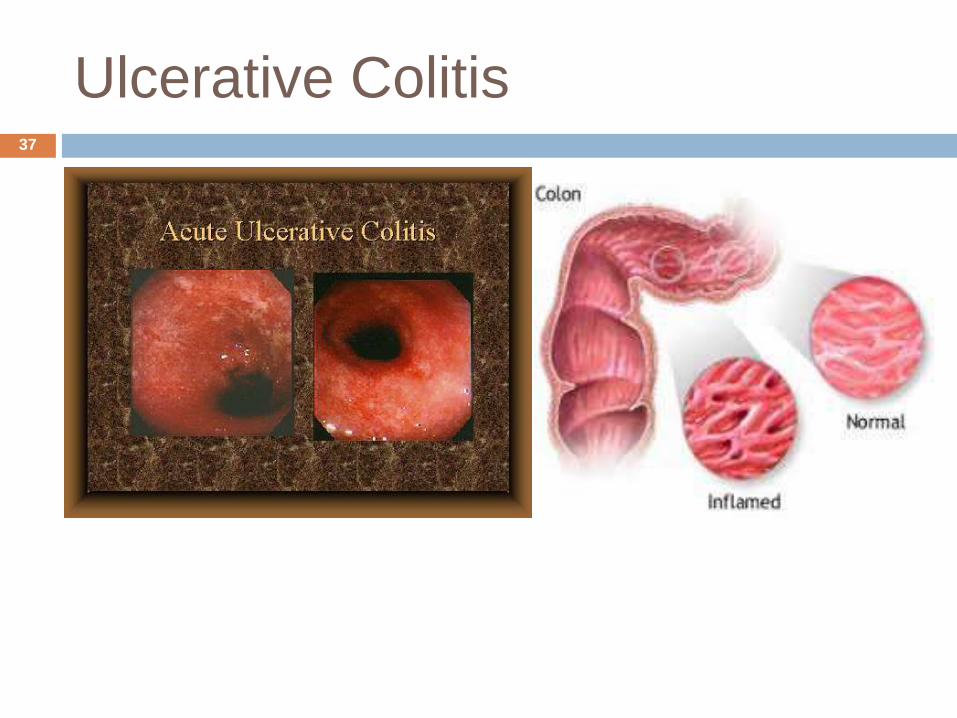
Ulcerative Colitis37
Ulcerative Colitis
Definition Inflammatory condition confined to the mucosal layer of the
rectum and colon
Location Starts in rectum and spreads proximally through colon
Pattern Confluent inflammatory pattern (no “skip” lesions)
Lead to pinpoint mucosal hemorrhages; may develop into crypt abscesses; may become necrotic & ulcerate
Pseudopolyps of mucosal layer
Manifestations Bloody diarrhea, nocturnal diarrhea, mild abdominal
cramping
Complications: Colon cancer risk; toxic megacolon in severe fulminant type
38
Ulcerative Colitis
Diagnosis
H&P
Colonoscopy
Treatment
Diet modifications Fiber reduces diarrhea
Avoid caffeine, lactose, spicy, and gas-producing foods
Corticosteroids
Immunosuppressants
Surgery
39
DIVERTICULAR DISEASE
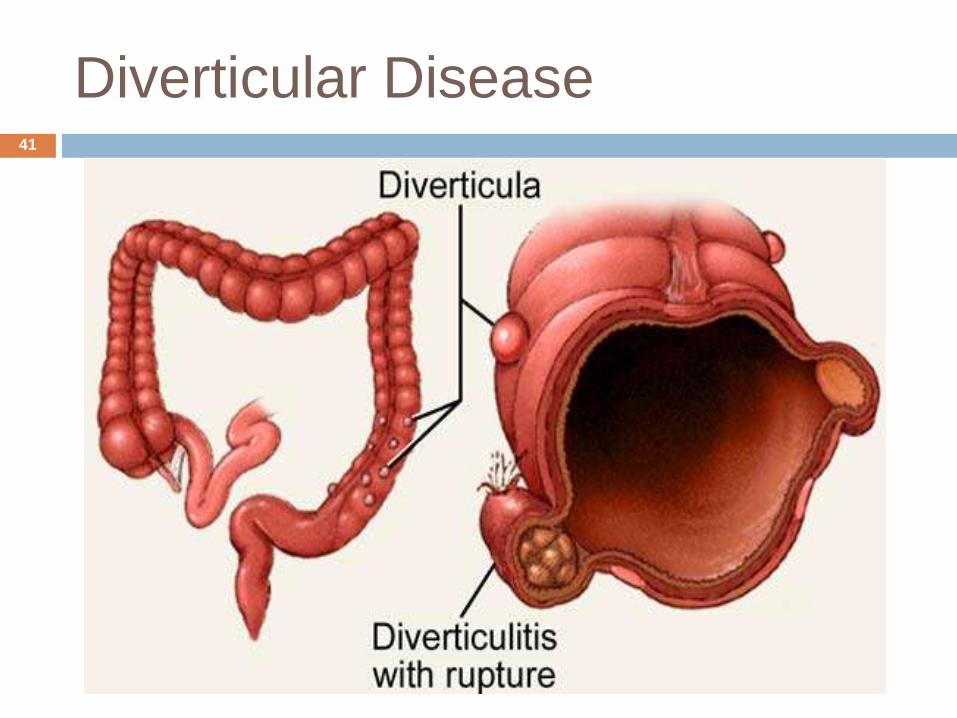
Diverticulum – saclike protrusions of the
mucous membrane that herniates outward
through muscular layer. (outpouches or
outpocketings)
Diverticula – plural for diverticulum
Diverticulosis – the presence of diverticula
Diverticulitis – diverticula become inflamed
and may perforate (undigested food, fecal
matter, and bacteria become trapped forming
fecalith)
40
Diverticular Disease41
DIVERTICULAR DISEASE
Increases dramatically with age
More common in North America, Australia, and
Europe
Affects men and women equally
Risk Factors
Low fiber diet
↓strength of colon musculature
↓physical activity
Poor bowel habits
42
ACUTE DIVERTICULITIS
LLQ ABDOMINAL PAIN (93-100%)
Tender palpable mass in LLQ
Fever
Mild to moderate leukocytosis
Nausea, vomiting, and anorexia
Constipation/Diarrhea
43
DIAGNOSIS
Diverticulosis
Usually no symptoms – picked up on routine
colonoscopy or plain X-ray
Vague abd discomfort, change in bowel habits,
bloating, flatulence
Flat and Upright abdominal films
CT scan**
Colonoscopy
Barium enema—not for acute diverticulitis!
44
TREATMENT
Increase dietary fiber
Bowel retraining/ regular defacation
Complications – Hospitalization
NPO
Nasogastric tube
TPN
Broad spectrum antibiotics
Surgery
45
APPENDICITIS46
APPENDICITIS
Inflammation of the vermiform appendix
Can lead to gangrene and perforation
Cause: Intraluminal obstruction w/ fecalith
Signs and Symptoms
Initially: vague epigastric or periumbilical pain
Nausea, vomiting, anorexia
Follow onset of pain
RLQ McBurney’s point rebound tenderness
75% have leukocytosis 10-18,000/mm3
Fever
Psoas sign/ Obturator test
47

48
DIAGNOSIS/TREATMENT
Emergency Department
History & Physical
CT scan** (or U/S)
Appendectomy (surgical)
IV Antibiotics
Complications
Peritonitis
Abscess formation
Septicemia
49

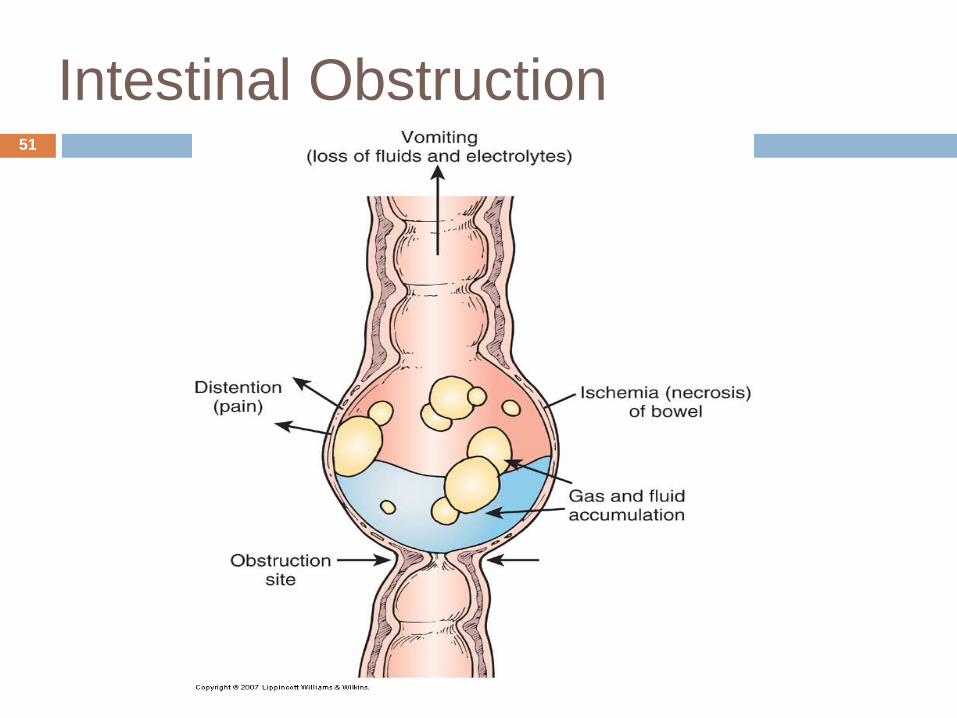
Intestinal Obstruction
Mechanical vs. Paralytic Mechanical:
Hernias, adhesions, strictures, tumors, foreign bodies, intussusception, volvulus
Severe colicky pain Borborygmy
Paralytic: “adynamic” Neurogenic or muscular impairment of peristalsis Paralytic ileus Absent bowel signs
S/S: Abdominal distention, pain, constipation, vomiting, F&E
disturbances.
50
Intestinal Obstruction51
Diagnosis
Abdominal X-ray
CT
U/S
52
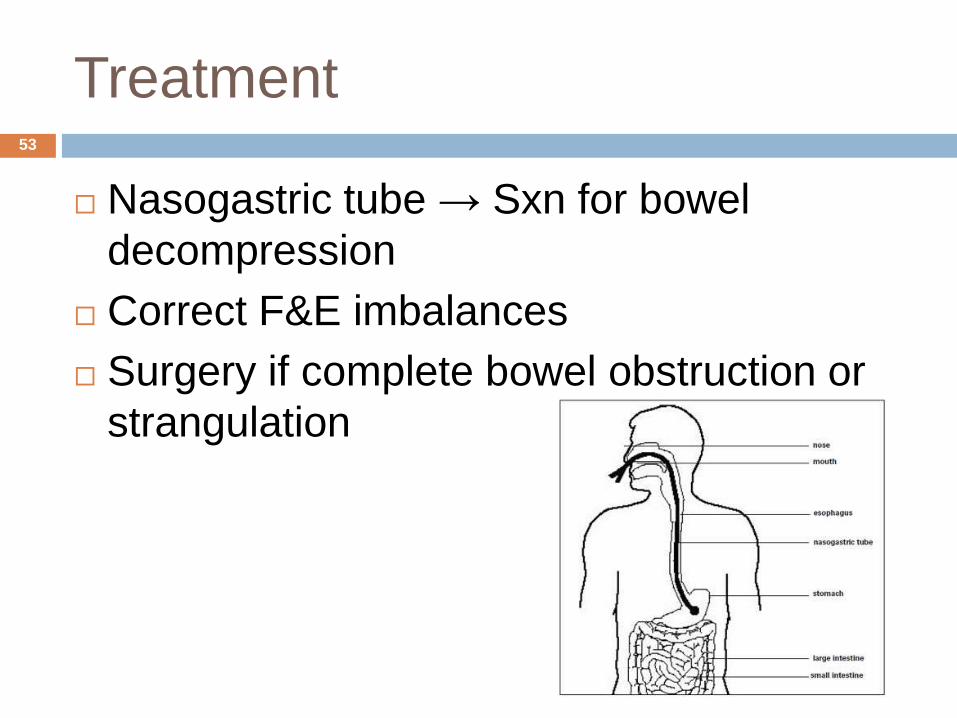
Treatment
Nasogastric tube → Sxn for bowel
decompression
Correct F&E imbalances
Surgery if complete bowel obstruction or
strangulation
53
COLORECTAL CANCER
Uncontrolled growth of malignant cells in the
large intestine
Risk Factors - >40, polyps, family history, DM,
Tobacco, diets rich in fats and red meats,
ethnicity
S/S – Change in bowel habits, occult blood,
bloating, anorexia, weight loss
Pain is a LATE sign!
Diagnosis – Colonoscopy, CEA
Treatment – Surgery, chemo, radiation
Screening recommendations
54
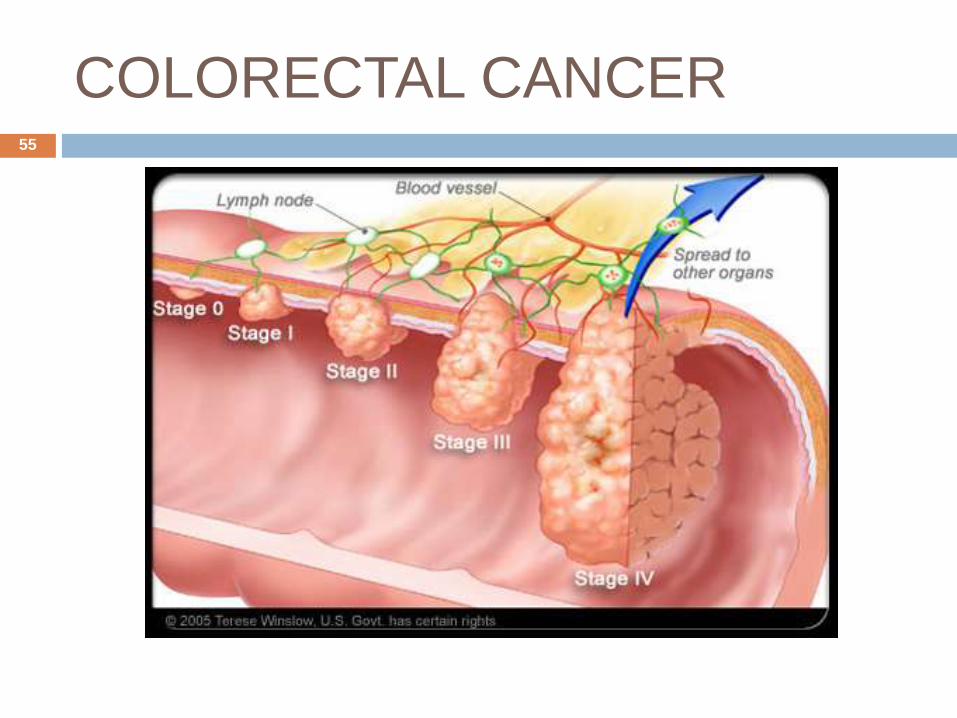
COLORECTAL CANCER55
Peritonitis
Inflammatory response of the peritoneal
membrane
Causes:
Bacterial or chemical irritation
Perforated ulcers, diverticulum, appendix
Gangrenous bowel or gallbladder
56
Signs & Symptoms
Pain & tenderness
Rigid/board-like, distended, guarded abdomen
Shallow respirations
N/V
Fluid losses; Dehydration
Fever
↑WBC count
Tachycardia
Hypotension
57

58
Complications
Paralytic ileus
Hypovolemia
Sepsis
Shock
60
Treatment
Correction of underlying cause
Correction of F&E imbalances
Surgery if indicated
NPO
NGT for decompression
Antibiotics
Analgesics
61
VIRAL HEPATITIS
Viral infection affecting the liver
Five viral causative agents: A,B,C,D,E
Hepatitis B,C, and D can cause chronic infections
Risk Factors:
HAV & HEV
Transmitted via fecal-oral route
Travel to endemic areas
Ingestion of contaminated food, water, milk, or shellfish
IgM anti-HAV, IgG anti-HAV
Hep A vaccine available
62
RISK FACTORS B&C
HBV, HCV –blood/body fluids
Shared needles
Multiple sexual partners
Tattoo recipients; body piercings
Health care workers
Can cause chronic hepatitis & cirrhosis
All adolescents are considered high-risk for HBV
Risk for hepatocellular CA w/ HCV
HBV vaccine available
63
SIGNS AND SYMPTOMS
Many are asymptomatic
Nausea, vomiting, anorexia, RUQ abdominal
pain, liver enlargement
Malaise, fever
Sclera become yellow (icteric)
Jaundice, dark urine, clay-colored stools
Elevated ALT, AST, bilirubin levels
64
DIAGNOSIS
Liver function tests
ALT, AST – hepatic injury
ALT – Think Hepatitis B
AST – Alcohol, Statins, Tylenol
PT/albumin – measure synthetic activity of
liver
Bilirubin – measure of excretory function of
liver
65
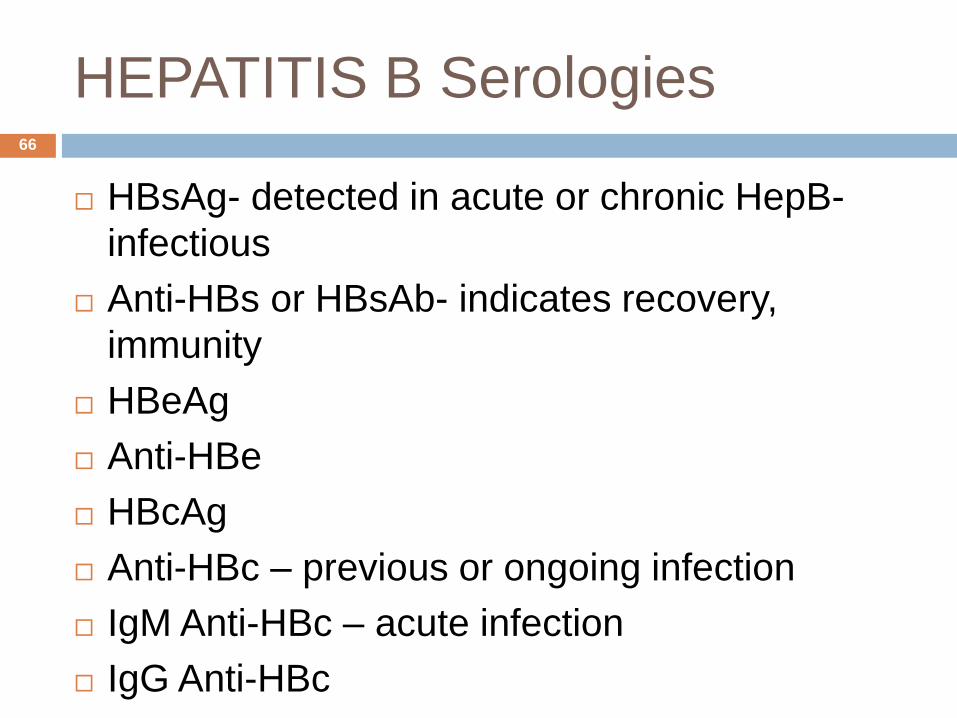
HEPATITIS B Serologies
HBsAg- detected in acute or chronic HepB-
infectious
Anti-HBs or HBsAb- indicates recovery,
immunity
HBeAg
Anti-HBe
HBcAg
Anti-HBc – previous or ongoing infection
IgM Anti-HBc – acute infection
IgG Anti-HBc
66
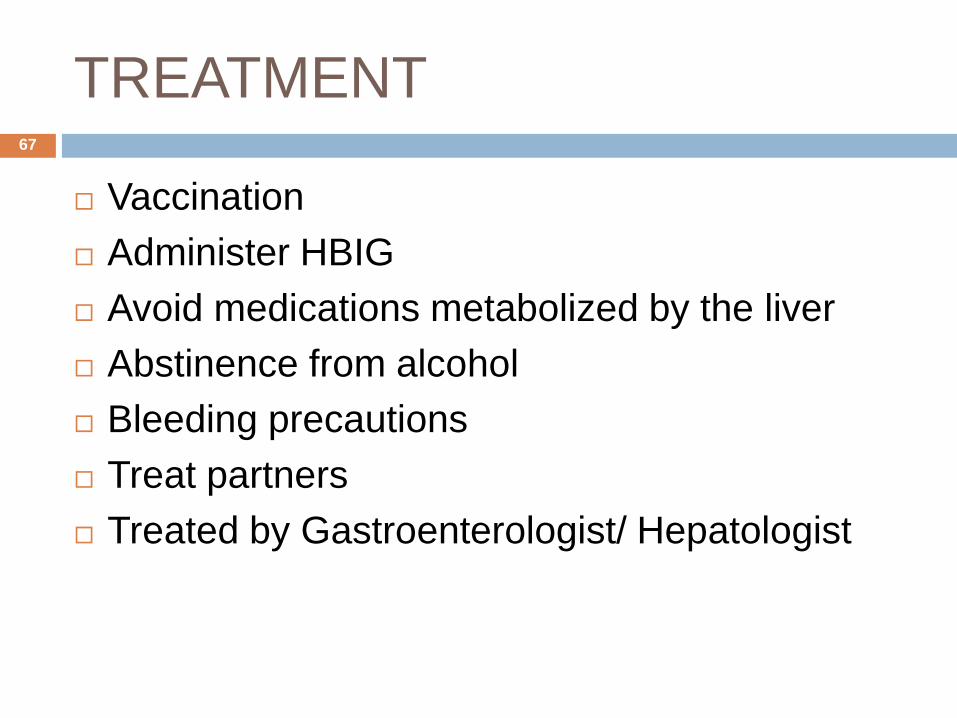
TREATMENT
Vaccination
Administer HBIG
Avoid medications metabolized by the liver
Abstinence from alcohol
Bleeding precautions
Treat partners
Treated by Gastroenterologist/ Hepatologist
67

CIRRHOSIS
End stage chronic liver disease
Irreversible inflammatory disease
Disrupts liver structure and function
Inflammation causes structural fibrotic
changes
Disruption of blood flow…portal HTN
Obstruction of biliary system…jaundice
68
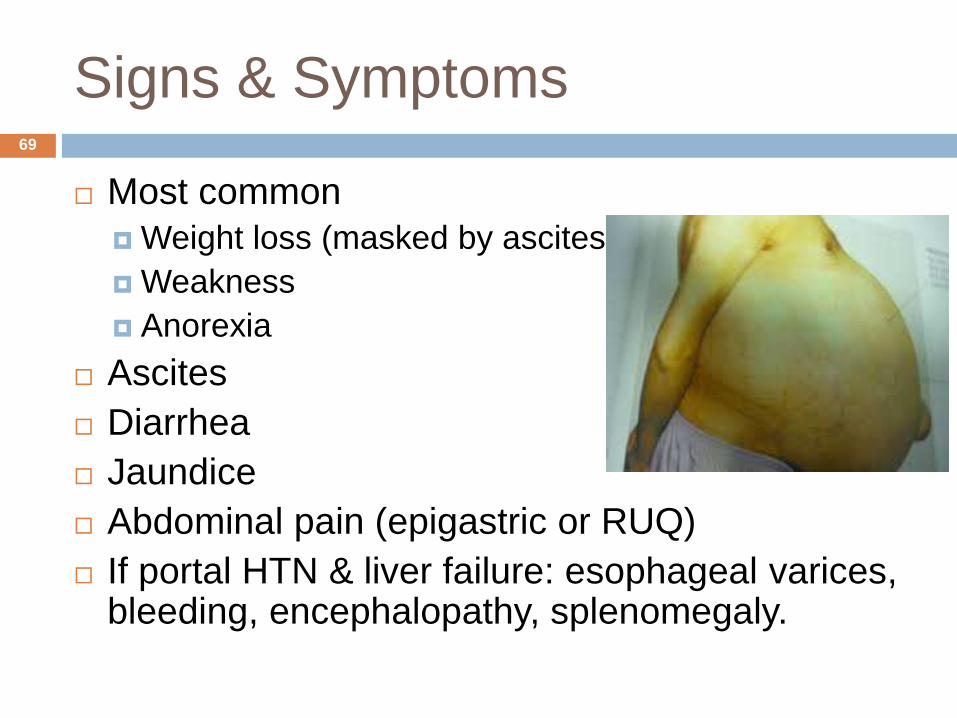
Signs & Symptoms
Most common
Weight loss (masked by ascites)
Weakness
Anorexia
Ascites
Diarrhea
Jaundice
Abdominal pain (epigastric or RUQ)
If portal HTN & liver failure: esophageal varices, bleeding, encephalopathy, splenomegaly.
69
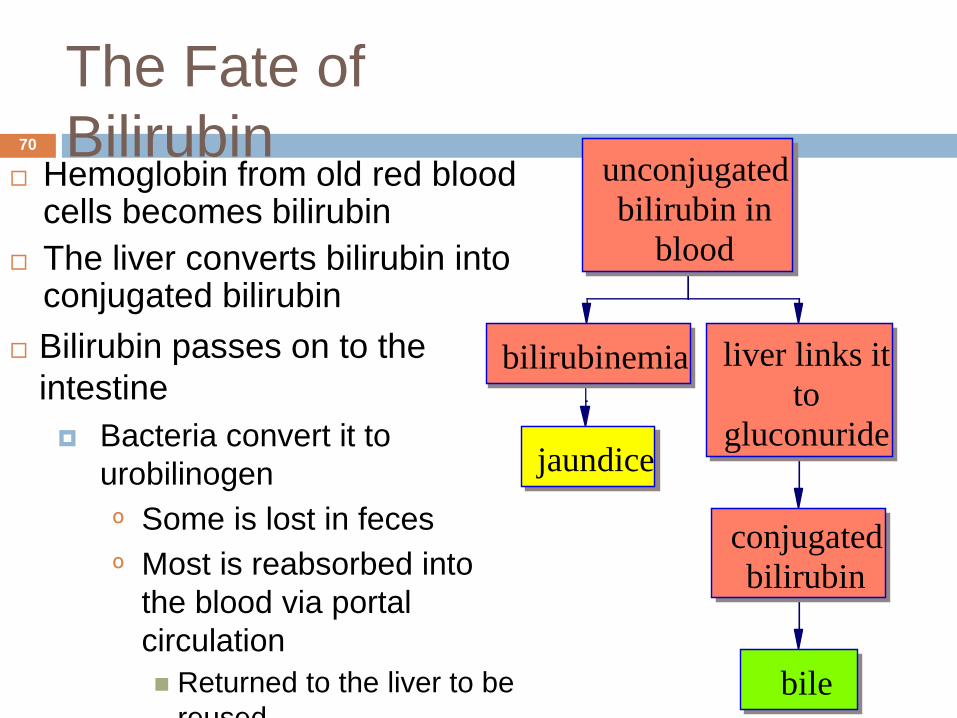
The Fate of
Bilirubin Hemoglobin from old red blood
cells becomes bilirubin
The liver converts bilirubin into conjugated bilirubin
Bilirubin passes on to the
intestine
Bacteria convert it to
urobilinogen
º Some is lost in feces
º Most is reabsorbed into
the blood via portal
circulation
Returned to the liver to be
reused
unconjugated
bilirubin in
blood
bilirubinemia
jaundice
liver links it
to
gluconuride
conjugated
bilirubin
bile
70
The Fate of Bilirubin…
Why would a man with liver failure
develop jaundice?
71
Liver Failure Leads To …
Hematologic disorders
Anemia, thrombocytopenia (low platelet),
coagulation defects, leukopenia (WBC)
Metabolic disorders
Fluid retention, hypokalemia, disordered
sexual functions
Which hormones would cause these
endocrine disorders?
72
Liver Failure Leads To …(cont.)
Skin disorders
Jaundice, red palms, spider nevi
Hepatorenal syndrome
Azotemia, increased plasma creatinine,
oliguria
Hepatic encephalopathy
Asterixis, confusion, coma, convulsions
Ammonia not converted to urea
73

Veins Draining into the Hepatic
Portal System
Portal hypertension causes pressure in these veins to increase
Varicosities and shunts develop
Organs engorge with blood
74
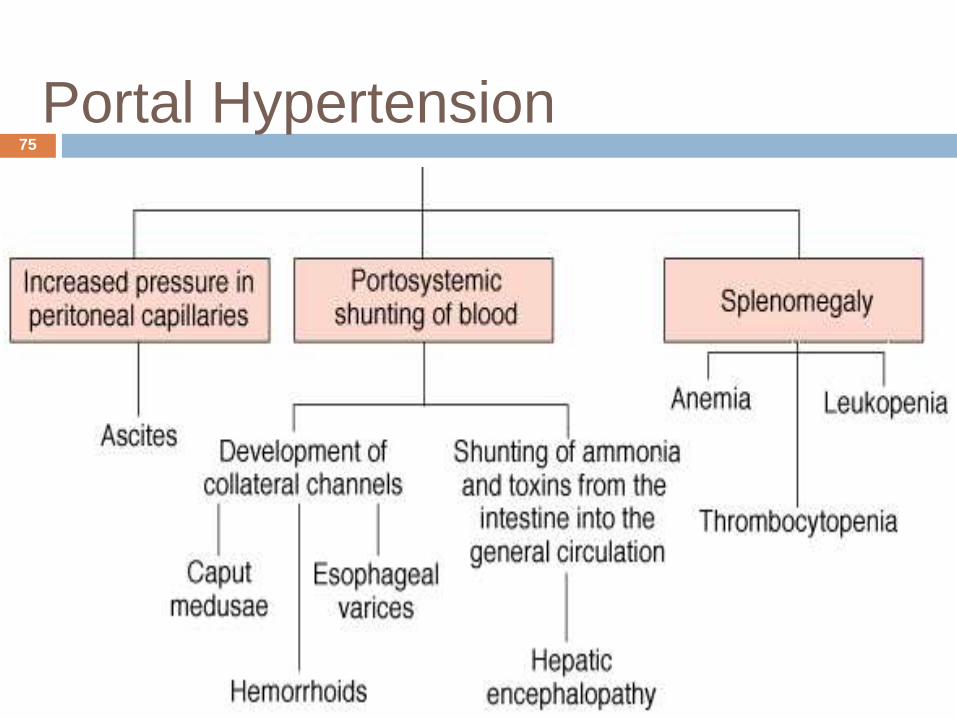
Portal Hypertension75
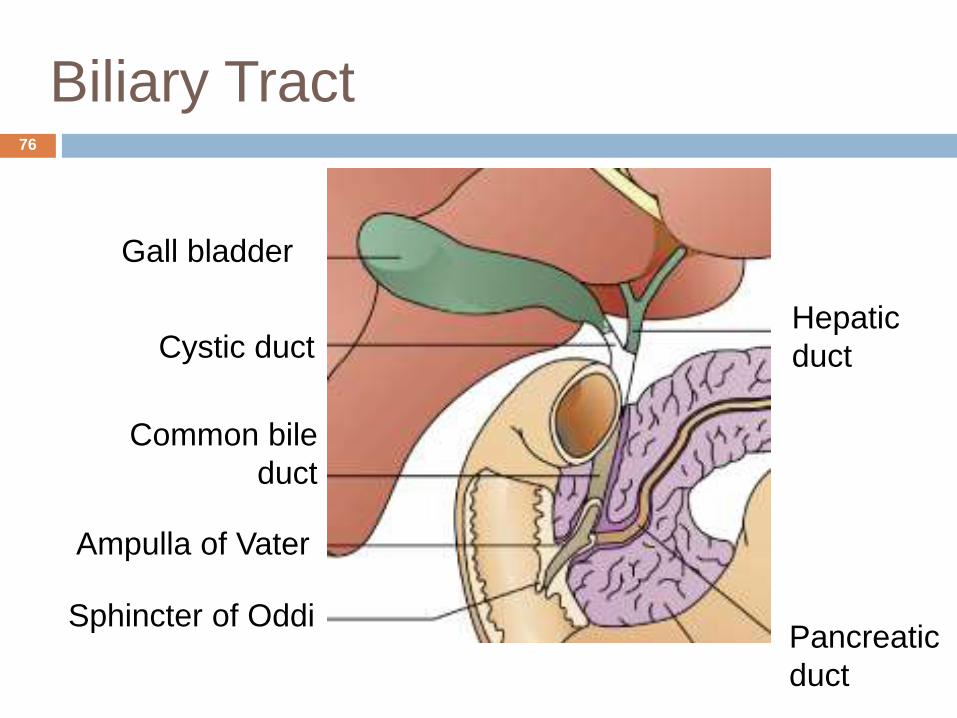
Biliary Tract
Hepatic
duct
Pancreatic
duct
Gall bladder
Cystic duct
Common bile
duct
Ampulla of Vater
Sphincter of Oddi
76
Disorders of the Gallbladder
Cholelithiasis (gallstones) Cholesterol, calcium salts, or mixed
Acute and chronic cholecystitis Inflammation caused by chemical
irritation due to concentrated bile. Can result in ischemia from mucosal swelling
Choledocholithiasis Stones in the common bile duct
Cholangitis Inflammation of the common bile duct
77
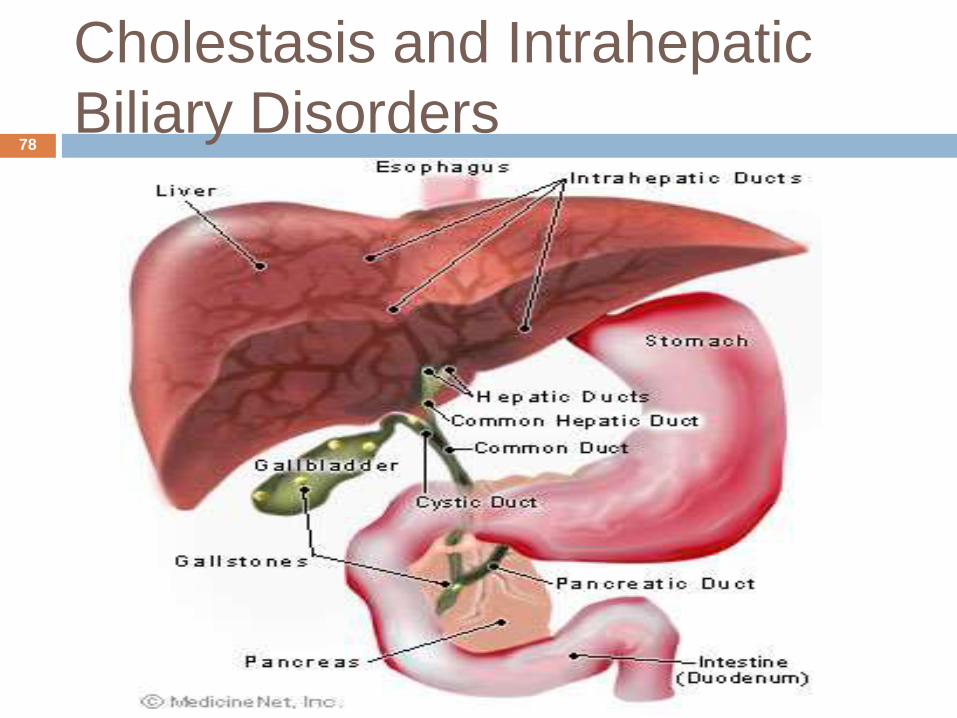
Cholestasis and Intrahepatic
Biliary Disorders78

Gall Stones79
Cholecystitis
Gall bladder disease
Acute – Complete or partial obstruction of the
cystic or common bile ducts.
Inflammation caused by chemical irritation
from the concentrated bile, mucosal swelling
and ischemia.
Bacterial infection
Mucosal necrosis gangrene perforation
Risk Factors
The Five F’s
80
SIGNS AND SYMPTOMS
RUQ pain that radiates to the tip of the right
scapula
Murphy’s sign
Excessive belching
Flatus
Nausea and vomiting
Low-grade fever
Elevated WBC count
Worsening symptoms after ingesting fried
foods.
81

DIAGNOSIS/ TREATMENT
Ultrasound
Gallbladder scan
Treatment
Bowel rest, intravenous hydration, analgesia, and
intravenous antibiotics. For mild cases of acute
cholecystitis, antibiotic therapy with a single
broad-spectrum antibiotic is adequate
Laparoscopic cholecystectomy (“Lap Chole”)
82
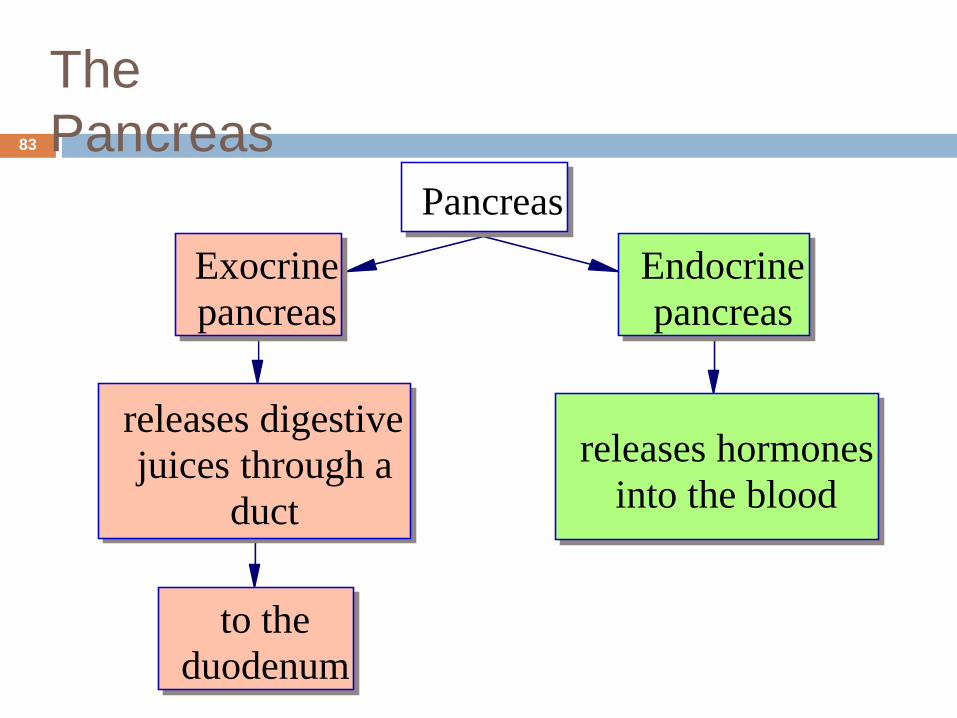
The
Pancreas
Pancreas
Exocrine
pancreas
releases digestive
juices through a
duct
to the
duodenum
Endocrine
pancreas
releases hormones
into the blood
83
Exocrine Pancreas
Acini produce: Inactive digestive
enzymes
Trypsin inactivator
These are sent to the duodenum
In the duodenum, the digestive enzymes are activated
84
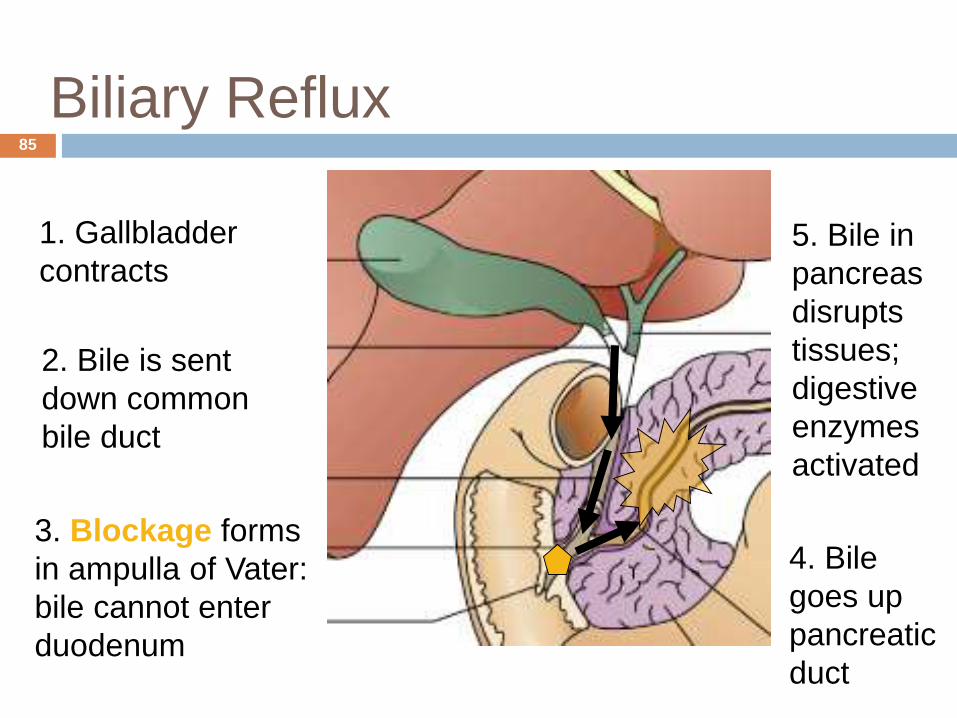
Biliary Reflux
5. Bile in
pancreas
disrupts
tissues;
digestive
enzymes
activated
4. Bile
goes up
pancreatic
duct
1. Gallbladder
contracts
2. Bile is sent
down common
bile duct
3. Blockage forms
in ampulla of Vater:
bile cannot enter
duodenum
85
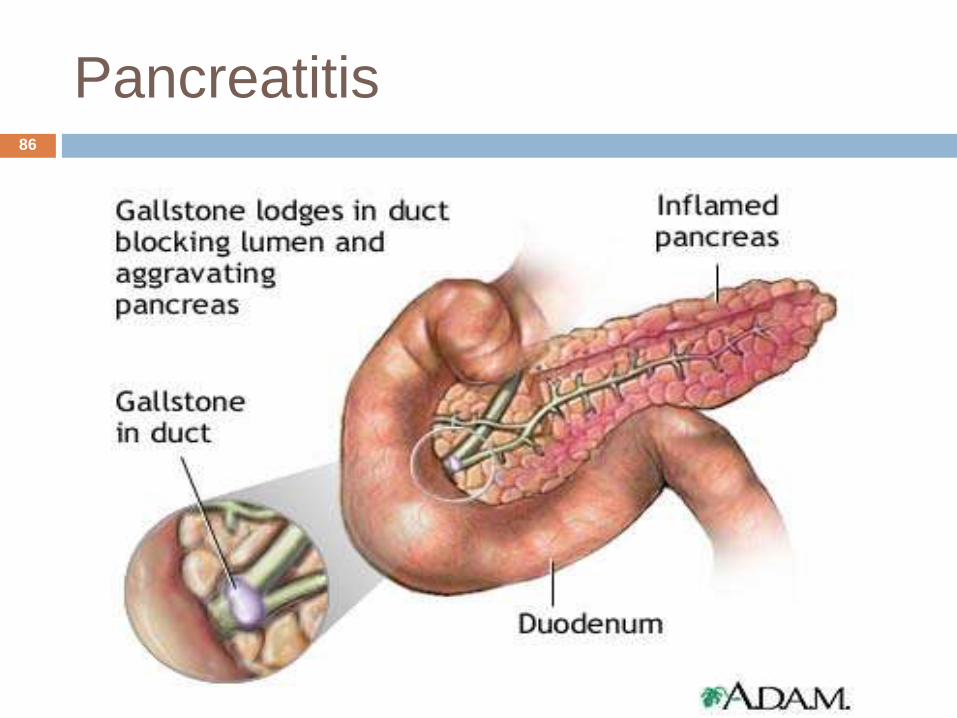
Pancreatitis86
ACUTE PANCREATITIS
Rapidly developing, potentially fatal,
inflammatory disease of the pancreas
Escape of pancreatic enzymes cause
autodigestion of the pancreas and fat necrosis
Causes:
Gall stones/Alcohol/GI surgery
87
Autodigestion of the Pancreas
Activated enzymes begin to digest the
pancreas cells
Severe pain results
Inflammation produces large volumes of serous
exudate hypovolemia
Elevated enzymes (amylase, lipase) appear in
the blood
Areas of dead cells undergo fat necrosis
Calcium from the blood deposits in them
º Hypocalcemia
88
Acute Pancreatitis
Signs & Symptoms
Severe abrupt abdominal pain that may radiate to the back.
Pain worse in supine position
N/V
Hyperglycemia
Hypotension & tachycardia
Fever
Elevated pancreatic enzymes – Amylase, Lipase,
Tx – aggressive hydration, antibiotics, NPO, NGT, pain management, surgery
89
Chronic Pancreatitis and Pancreatic
Cancer
Have signs and symptoms similar to acute
pancreatitis
MOST common cause: ETOH
Permanent destruction of exocrine function and
later stages also endocrine fxn destruction
Often have:
Digestive problems because of inability to deliver
enzymes to the duodenum
Glucose control problems because of damage to islets
of Langerhans
Signs of biliary obstruction because of underlying bile
tract disorders or duct compression by tumors
90
91