Genetic, immunological and clinical risk factors for biliary strictures following liver...
9
CLINICAL STUDIES Genetic, immunological and clinical risk factors for biliary strictures following liver transplantation Speranta Iacob 1,2,3,* , Vito R. Cicinnati 1,2,* , Alexander Deche ˆ ne 1 , Monika Lindemann 4 , Falko M. Heinemann 4 , Vera Rebmann 4 , Stanislav Ferencik 5 , Georgios C. Sotiropoulos 2 , Irinel Popescu 3 , Peter A. Horn 4 , Guido Gerken 1 , Andreas Paul 2 and Susanne Beckebaum 1,2,6 1 Departments of Gastroenterology and Hepatology, University Hospital Essen, Essen Germany 2 Department of General, Visceral and Transplantation Surgery,University Hospital Essen, Essen Germany 3 Fundeni Clinical Institute of Digestive Diseases and Liver Transplantation, Bucharest Romania 4 Institute for Transfusion Medicine University Hospital Essen, Essen Germany 5 Institute for Immunology University Hospital Essen, Essen Germany 6 Present address: Department of Transplant Medicine, University Hospital Mu ¨ nster Albert-Schweitzer-Campus 1, Geba ¨ ude A14, 48149, Mu ¨ nster, Germany Keywords anastomotic biliary strictures – CCR5D32 – chemokine – CX3CR1 – ischaemic type biliary lesions – liver transplantation Abbreviations AB, antibodies; ALF, Acute liver failure; AS, anastomotic strictures; AST, aspartate aminotransferase; BSA, bovine serum albumin; CCL, CC chemokine ligand; CCR5D32, CC chemokine receptor 5 delta32 loss-of-function mutation; CCR, CC chemokine receptor; CIT, cold ischaemia time; CX3CL1, fractalkine; CX3CR1, fractalkine receptor; ELISA, enzyme linked immunosorbent assay; HLA, human leucocyte antigen; IFN-c, interferon-gamma; Ig, immune globuline; IL, interleukin; ITBL, ischaemic type biliary lesion(s); LT, liver transplantation; mAB, monoclonal antibodies; MICA, major-histocompatibility complex classI-related chain A; MICB, major- histocompatibility complex class I-related chain B; PBS, phosphate buffer saline; PCR, polymerase chain reaction; PCR-SSP, polymerase chain reaction using sequence Abstract Background: Biliary strictures after liver transplantation (LT) are a major cause of morbidity and reduced graft survival. Aims: The purpose of this study was to investigate genetic, immunological and clinical risk factors for the occur- rence of post-LT ischaemic type biliary lesions (ITBLs) and biliary anasto- motic strictures (AS). Methods: Clinical and laboratory data, chemokine receptor (CCR) genotypes, chemotactic cytokines and anti-major-histo- compatibility complex antibodies in serum were investigated in 162 LT patients. Results: In the univariate analysis, older donor and recipient age, par- tial LT, high peak aspartate aminotransaminase (AST) levels and CC chemokine receptor 5 delta32 loss-of-function mutation (CCR5D32) were associated with ITBL, whereas LT for acute liver failure (ALF), ABO-compatible non-identical LT, presence of donor-specific anti-human leucocyte antigen (HLA) class II anti- bodies and fractalkine receptor (CX3CR1)-249II allele were associated with AS. In the multivariate analysis, CCR5D32 was an independent risk factor for ITBL, whereas LT for ALF, ABO-compatible non-identical LT, and CX3CR1-249II allele remained predictive for AS. Serum levels of interferon-gamma and inter- leukin (IL)-6 as well as IL-10 were significantly increased in patients with biliary strictures. Conclusion: Specific chemokine receptor polymorphisms of the reci- pient are associated with development of post-LT biliary strictures. Altered cyto- kine profile may contribute to enhanced fibrotic tissue remodelling and biliary stricture formation. Screening of anti-HLA antibodies might be useful for early identification of at-risk patients who could benefit from closer surveillance and tailored immunosuppressive regimen. Our findings may have relevance for pre- diction and management of post-LT biliary strictures. specific primers; sMICA, soluble major- histocompatibility complex class I-related chain A; sMICB, soluble major- histocompatibility complex class I-related chain B; sULBP2, soluble UL16 binding protein 2; Th1, T helper type 1; Th2, T helper type 2; TNF-a, tumour necrosis factor-alpha. Biliary complications after liver transplantation (LT) still represent a major source of morbidity, impaired quality of life and graft loss despite advances in surgical techniques and interventional endoscopic treatment Correspondence Susanne Beckebaum, University Hospital Essen, Hufelandstr. 55, 45122 Essen, Germany Tel: + 49 251 8357935 Fax: + 49 251 8357771 e-mail: [email protected] DOI:10.1111/j.1478-3231.2012.02810.x *S.I. and V.R.C. have contributed equally to this work Parts of the results were orally presented at the 15th Congress of the European Society for Organ Transplantation, Glasgow, United King- dom, 4–7 September 2011 Liver International (2012) © 2012 John Wiley & Sons A/S 1 Liver International ISSN 1478-3223
-
Upload
speranta-iacob -
Category
Documents
-
view
215 -
download
1
Transcript of Genetic, immunological and clinical risk factors for biliary strictures following liver...

CL IN ICAL STUDIES
Genetic, immunological and clinical risk factors for biliary stricturesfollowing liver transplantationSperanta Iacob1,2,3,*, Vito R. Cicinnati1,2,*, Alexander Dechene1, Monika Lindemann4, Falko M. Heinemann4,Vera Rebmann4, Stanislav Ferencik5, Georgios C. Sotiropoulos2, Irinel Popescu3, Peter A. Horn4, Guido Gerken1,Andreas Paul2 and Susanne Beckebaum1,2,6
1 Departments of Gastroenterology and Hepatology, University Hospital Essen, Essen Germany
2 Department of General, Visceral and Transplantation Surgery,University Hospital Essen, Essen Germany
3 Fundeni Clinical Institute of Digestive Diseases and Liver Transplantation, Bucharest Romania
4 Institute for Transfusion Medicine University Hospital Essen, Essen Germany
5 Institute for Immunology University Hospital Essen, Essen Germany
6 Present address: Department of TransplantMedicine,UniversityHospitalMunster Albert-Schweitzer-Campus 1, GebaudeA14, 48149, Munster,
Germany
Keywords
anastomotic biliary strictures – CCR5D32 –
chemokine – CX3CR1 – ischaemic type biliary
lesions – liver transplantation
Abbreviations
AB, antibodies; ALF, Acute liver failure; AS,
anastomotic strictures; AST, aspartate
aminotransferase; BSA, bovine serum
albumin; CCL, CC chemokine ligand;
CCR5D32, CC chemokine receptor
5 delta32 loss-of-function mutation; CCR, CC
chemokine receptor; CIT, cold ischaemia
time; CX3CL1, fractalkine; CX3CR1,
fractalkine receptor; ELISA, enzyme linked
immunosorbent assay; HLA, human leucocyte
antigen; IFN-c, interferon-gamma; Ig,
immune globuline; IL, interleukin; ITBL,
ischaemic type biliary lesion(s); LT, liver
transplantation; mAB, monoclonal
antibodies; MICA, major-histocompatibility
complex classI-related chain A; MICB, major-
histocompatibility complex class I-related
chain B; PBS, phosphate buffer saline; PCR,
polymerase chain reaction; PCR-SSP,
polymerase chain reaction using sequence
AbstractBackground: Biliary strictures after liver transplantation (LT) are a major causeof morbidity and reduced graft survival. Aims: The purpose of this study wasto investigate genetic, immunological and clinical risk factors for the occur-rence of post-LT ischaemic type biliary lesions (ITBLs) and biliary anasto-motic strictures (AS). Methods: Clinical and laboratory data, chemokinereceptor (CCR) genotypes, chemotactic cytokines and anti-major-histo-compatibility complex antibodies in serum were investigated in 162 LTpatients. Results: In the univariate analysis, older donor and recipient age, par-tial LT, high peak aspartate aminotransaminase (AST) levels and CC chemokinereceptor 5 delta32 loss-of-function mutation (CCR5D32) were associated withITBL, whereas LT for acute liver failure (ALF), ABO-compatible non-identicalLT, presence of donor-specific anti-human leucocyte antigen (HLA) class II anti-bodies and fractalkine receptor (CX3CR1)-249II allele were associated with AS.In the multivariate analysis, CCR5D32 was an independent risk factor for ITBL,whereas LT for ALF, ABO-compatible non-identical LT, and CX3CR1-249IIallele remained predictive for AS. Serum levels of interferon-gamma and inter-leukin (IL)-6 as well as IL-10 were significantly increased in patients with biliarystrictures. Conclusion: Specific chemokine receptor polymorphisms of the reci-pient are associated with development of post-LT biliary strictures. Altered cyto-kine profile may contribute to enhanced fibrotic tissue remodelling and biliarystricture formation. Screening of anti-HLA antibodies might be useful for earlyidentification of at-risk patients who could benefit from closer surveillance andtailored immunosuppressive regimen. Our findings may have relevance for pre-diction andmanagement of post-LT biliary strictures.
specific primers; sMICA, soluble major-
histocompatibility complex class I-related
chain A; sMICB, soluble major-
histocompatibility complex class I-related
chain B; sULBP2, soluble UL16 binding
protein 2; Th1, T helper type 1; Th2, T helper
type 2; TNF-a, tumour necrosis factor-alpha.
Biliary complications after liver transplantation (LT)still represent a major source of morbidity, impairedquality of life and graft loss despite advances in surgicaltechniques and interventional endoscopic treatment
Correspondence
Susanne Beckebaum, University Hospital Essen,
Hufelandstr. 55, 45122 Essen, Germany
Tel: + 49 251 8357935
Fax: + 49 251 8357771
e-mail: [email protected]
DOI:10.1111/j.1478-3231.2012.02810.x
*S.I. and V.R.C. have contributed equally to this workParts of the results were orally presented at the 15th Congress of theEuropean Society for Organ Transplantation, Glasgow, United King-dom, 4–7 September 2011
Liver International (2012)© 2012 John Wiley & Sons A/S 1
Liver International ISSN 1478-3223

options (1). Post-LT biliary complications occurring in10–35% of patients comprise leaks, strictures and for-mation of biliary cast, sludge, and stones (2, 3). Earlyanastomotic strictures (AS) are usually related to techni-cal reasons, whereas later appearing strictures have amultifactorial origin. Nonanastomotic strictures with-out underlying hepatic artery thrombosis are commonlyreferred to as ischaemic-type biliary lesions (ITBL). Sev-eral risk factors for ITBL have been identified, includingpreservation-induced injury, prolonged cold and warmischaemia times, altered bile composition and immuno-logical injury (3–5). Cytokines and chemokines are keymediators of hepatobiliary inflammation (6). Pro-inflammatory cytokines, such as interleukin (IL)-6,tumour necrosis factor-alpha (TNF-a) and interferon-gamma (IFN-c), may sustain cell-mediated immuneresponses, thereby promoting hepatobiliary injury.Locally increased levels of chemokines such as CCchemokine ligand (CCL)2, CCL5 as well as fractalkine(CX3CL1) induce chemotaxis and transendothelialmigration of inflammatory leucocytes expressing therespective receptors, thereby sustaining the inflamma-tory cascade (7). Genetic polymorphisms of chemokinereceptors (CCR), which mediate leucocyte traffickingalter their expression and function, and thus may influ-ence hepatobiliary inflammation after LT (8). Forinstance, an association between CC chemokine recep-tor 5 delta32 loss-of-function mutation (CCR5D32) anddevelopment of ITBL has been reported (9, 10). Theimpact of human leucocyte antigen (HLA) mismatchesand the presence of anti-HLA antibodies (AB) on liverallograft survival is still an issue of debate (11–13). Inthis study, we assessed the association of distinctchemokine receptor polymorphisms on ITBL and ASdevelopment after LT. Furthermore, we aimed to iden-tify immunological and clinical risk factors for theoccurrence of post-LT biliary strictures.
Patients and methods
Patients
This study was designed as a cross-sectional study at theDepartment of General, Visceral and TransplantationSurgery at the University Hospital in Essen, Germany.Patients transplanted with an ABO blood groupidentical or compatible primary deceased orliving-related LT were prospectively enrolled at theirregular follow-up visit in the LT outpatient unitbetween June 2009 and June 2010. Adult LT patientswere eligible for the study if they (a) had received a pri-mary deceased or living-related LT � 3 months prior tostudy entry. Diagnosis of ITBL and AS was based onmagnetic resonance cholangiopancreaticography andendoscopic retrograde cholangiopancreaticography orpercutaneous transhepatic cholangiography. Patientswere excluded if they (a) had any clinical and/or bio-chemical signs of acute infection including cholangitis;
(b) had undergone endoscopic or surgical intervention<1 week from inclusion; (c) had a history of chronicductopenic rejection (d) were diagnosed with hepaticartery thrombosis.
Although recurrent PBC is characterized by progres-sive destruction of small bile ducts, biliary injuries inITBL may additionally be triggered by autoimmune-mediated causes of the underlying cholestatic disease.Moreover, in recipients transplanted for PSC, there isno diagnostic tool for clearly distinguishing betweenITBL and recurrent PSC. We therefore excluded patientstransplanted for cholestatic liver diseases.
At enrolment, blood was taken for genotyping,chemokine and cytokine analysis, and recipient anddonor data were extracted from medical records. Thisstudy was conducted in accordance with the Declarationof Helsinki 2000, approved by the Institutional ReviewBoard of the University of Duisburg-Essen (IRB 09-4272), and all patients provided written informed con-sent before study entry. Graft failure was defined as his-tologically proven liver cirrhosis or allograft dysfunctionrequiring relisting for LT or leading to death.
Genotype analysis
For analysis of CCR2, CCR5 and CX3CR1 genotype,genomic DNA was prepared from 200lL buffy coatusing the QIAamp® DNA Blood Kit (Qiagen, Hilden,Germany). The CCR2-V64I, CX3CR1-V249I andCX3CR1-T280M polymorphisms were analysed throughpolymerase chain reaction (PCR) followed by restrictionfragment length polymorphism (Table 1). Polymerasechain reaction products of CCR5 and restriction frag-ments of CCR2 and fractalkine receptor (CX3CR1) wereanalysed by 3% agarose gel electrophoresis and stainedwith ethidium bromide.
Cytokine and chemokine quantification in serum
Cytokines were assessed by flow cytometry using the‘BD Cytometric Bead Array Human Th1/Th2/Th17Cytokine Kit’ (BD Biosciences, San Jose, CA, USA). Theconcentrations of CCL3/MIP-1a, CCL5/RANTES andCX3CL1/Fractalkine were measured by enzyme-linkedimmunosorbent assay technique (ELISA) (R&D SystemsEurope, Abingdon, England) according to the manufac-turer’s protocol.
Human leucocyte antigen typing and antibody testing
HLA-A and HLA-B antigens were typed by serology orPCR using sequence-specific primers (PCR-SSP).HLA-DR and DQ antigens were analysed using PCR-SSP methodology or sequencing-based typing (14).Screening for anti-HLA class I, class II, or major-histo-compatibility complex class I-related chain (MIC)A ABwas performed using Luminex technology (LuminexCorporation, Austin, TX, USA) according to the
Liver International (2012)© 2012 John Wiley & Sons A/S2
Post–LT biliary strictures Iacob et al.

manufacturer’s instructions (LABScreen assay, OneLambda Inc., Canoga Park, CA, USA) (15). Discrimina-tion of HLA specificities in LABScreen Mixed positivesamples was performed using LABScreen Single Antigenbeads (One Lambda Inc.). LABScreen Mixed positivesamples were also tested for the presence of lymphocy-totoxic AB using complement-dependent cytotoxicityassays with the addition of dithiothreitol to excludelymphocytotoxic autoantibodies of the immune globu-line (Ig)M type.
Assessment of soluble MICA (sMICA), soluble MICB(sMICB) and soluble UL16 binding protein 2 (sULBP2)by ELISA
Capture of sMICA and sULBP2 molecules wasperformed with monoclonal AB (mAB) AMOI andmAB BUM01, both used in a final concentration of25 ng/ml (BAMOMAB, Munich, Germany). The detec-tion of bound sMICA or sULBP2 molecules was per-formed with biotin-coupled polyclonal goat anti-humanMICA or goat anti-human ULBP-2 (R&D SystemsGmbH) diluted to 400 ng/ml in phosphate buffer saline(PBS), supplemented with 1% bovine serum albumin(BSA), and 2% inactivated goat serum. Bound detectionAB were recognized by streptavidin conjugated withhorseradish peroxidase (R&D Systems GmbH) beingdiluted 1:200 in PBS with 1% BSA. 3,3′,5,5′-tetrame-thybenzidine (Sigma-Aldrich Chemie GmbH, Munich,Germany) served as a substrate solution. Absorbancewas measured at 450 nm (Biotek Instruments, Winoo-ski, VT, USA). Assessment of sMICB was performedwith commercial ELISA kits (R&D Systems GmbH)according to the protocols of the manufacturer. Recom-binant MICA, MICB and ULBP2 protein fused with Fcportion of human IgG (R&D Systems GmbH) were usedas standard reagents. Determination of sNKG2D ligandplasma levels was performed by a four-parameter curvefitting.
Statistical analysis
Continuous data are expressed as mean ± standard devi-ation (SD) unless otherwise indicated. Categorical dataare described as frequencies of the subjects with a spe-cific characteristic. Chi-square or Fischer’s exact test wasused for comparing categorical data and Student’s t-testor Mann–Whitney U test, when appropriate, was usedfor comparing continuous variables. Multivariate logis-tic regression analysis was performed to identify inde-pendent risk factors for development of biliarycomplications after LT. Patient and graft survivalaccording to different variables were evaluated using theKaplan Meier method. Survival curves were comparedusing the log rank test. Two-tailed p values <0.05 wereconsidered statistically significant. Statistical analysiswas performed using SPSS software (SPSS Inc., Chicago,IL, USA).T
able
1.Po
lymerasechainreaction(PCR)an
dPC
R-restrictionfrag
men
tlength
polymorphism
(PCR-RFLP)
Position
Mutation
Nucleo
tide
chan
ge*
Forw
ardprimer
(5′?
3′)
Reverse
primer
(5′?
3′)
Annea
ling
temperature
(°C)
Restriction
enzyme†
Size
(bp)
CCR2Exon1
V64I
G190A
CAACATG
CTG
-CTC
ACATC
TCCCCACAATG
GG-AGAGTA
ATA
A52.5
FokI
299
CCR5Exon1
D32
–CAAAAAGAAGG-TCTTCATTACACC
CCTG
TGCCTC
TT-CTTCTC
ATTTC
G56.6
–189(w
t)157
(D32)
CX3CR1
Exon2
V249IT280M
G745AC839T
AGCCATTAAAC-TGATC
CTTCTG
AGAACACTTC-CATG
CCTG
C53.7
AclIB
ccI
270+60330
*Numberingfrom
ATG
inmRNA.
†Enzymes
from
New
EnglandBioLabs,Ipsw
ich,MA,USA
.
bp,basepair;wt,wild-type.
Liver International (2012)© 2012 John Wiley & Sons A/S 3
Iacob et al. Post–LT biliary strictures

Results
Study population
A total of 586 LT recipients (n = 102 with AS or ITBLand n = 484 without biliary strictures) were screened foreligibility criteria. Of those, n = 37 patients with ITBL,n = 40 with AS and n = 85 controls were enrolled in thestudy. Twenty-five patients with AS or ITBL and 399controls did not qualify for the study (n = 2 and n = 26of patients were transplanted <3 months after LT, n = 4and n = 73 were transplanted due to cholestatic liver dis-ease, n = 1 and n = 18 had chronic ductopenic rejection,n = 18 and n = 117 presented with clinical and/or labo-ratory signs of acute infection, n = 78 controls hadincomplete data records, n = 3 controls were diagnosedwith hepatic artery thrombosis) and n = 84 controls didnot give informed consent. The median time from LT toITBL and AS occurrence was 5.1 months (range 3.6–141.4 months) and 6.3 months (range 4.5–191 months),respectively. The proportion of patients with blood typeA, B, AB and O was 50, 14.8, 9.3 and 25.9% respectively.All patients were treated with tacrolimus (77.2%) orcyclosporine A (22.8%)-based immunosuppression. Ofthose, 24.1% received additional low dose (2.5–5 mg)steroid therapy, 35.2% mycophenolate mofetil and 6.1%sirolimus therapy. Patients’ characteristics in the studygroups at evaluation are shown in Table 2.
Genotype and allele distribution among livertransplantation recipients
The distribution of CCR2, CCR5 and CX3CR1 geno-types was not significantly different among patients withbiliary complications and controls. All patients withCX3CR1-280T/M or M/M alleles harboured concomi-tant presence of CX3CR1-249V/I or I/I alleles.
Risk factors for development of post-transplant biliarycomplications
Genetic, immunological and clinical risk factors forboth types of post-transplant biliary strictures includedin the univariate analysis are shown in Tables 3 and 4.In the univariate analysis, ITBL was associated withdonor age >50 years (P = 0.001), older recipient age atLT (P = 0.009), partial LT (P = 0.03), CCR5D32hetero/homozygosity (P = 0.01) and high peak aspartataminotransferases (AST) (P = 0.03). For AS, thefollowing risk factors were identified: CX3CR1-249IIallele (P = 0.03), LT for acute liver failure (ALF)(P = 0.03), ABO-compatible non-identical LT(P = 0.03), presence of donor-specific anti-HLA classII AB (P = 0.02). Independent variables associated withAS and ITBL were identified by multivariate logisticregression analysis (Table 5). CCR5D32 hetero/homo-zygosity (P = 0.03) was an independent risk factor forITBL, whereas ABO-compatible non-identical LT(P = 0.03), ALF as LT indication (P = 0.03) andCX3CR1-249II allele (P = 0.03) were independent riskfactors for AS.
Association of genetic variants with allograft outcome
There was no difference in graft survival between LTrecipients heterozygous or homozygous for theCCR5D32 allele in comparison with recipients with theCCR5 wild type homozygous allele (log rank P = 0.52)or between those with CX3CR1-249I homozygous allelecompared with CX3CR1-249V/I or V/V alleles (log rankP = 0.69). Furthermore, there was no associationbetween CCR2, CCR5 and CX3CR1 genotype polymor-phisms and graft survival in ITBL or AS subgroups (logrank test, P = NS).
Table 2. Patient characteristics in the study groups at evaluation
VariableControl group(n = 85)
AS group(n = 40) P value*
ITBL group(n = 37) P value†
Age at evaluation (years) 53.5 ± 10.1 50.8 ± 12.8 0.49 55.4 ± 13.5 0.12Time period LT – enrolment (days) 2590.3 ± 177.4 2179.8 ± 223.9 0.22 2029.5 ± 233.9 0.06HCV-related liver disease‡ 29 (34.1%) 13 (32.5%) 0.85 7 (18.9%) 0.09Advanced fibrosis (F3-F4) 18 (21.2%) 13 (32.5%) 0.17 14 (37.8%) 0.054Disease recurrence (HCV and AIH) 34 (40%) 14 (35%) 0.59 7 (18.9%) 0.02At least one episode of cholangitis§ 17 (20%) 24 (60%) <0.0001 19 (51.4%) 0.0004Recurrent (� 3) episodes of cholangitis 0 (0%) 13 (32.5%) <0.0001 14 (37.8%) <0.0001
Values are expressed as mean ± SD or numbers (percentages).*P value for comparison of AS group vs control group.
†P value for comparison of ITBL group vs control group.
‡Other indications included: alcohol-related liver disease (n = 29, 17.9%), hepatitis B (n = 25, 15.4%), autoimmune hepatitis (n = 15, 9.3%), acute
liver failure (ALF) (n = 11, 6.7%), Wilson disease (n = 8, 4.9%), cryptogenic cirrhosis (n = 7, 4.3%) and others (n = 18, 11.3%).
§Episodes of acute cholangitis were diagnosed according to the diagnostic criteria of Tokyo guidelines (48).
AS, anastomotic stricture; ITBL, ischaemic type biliary lesion; LT, liver transplantation; HCV, hepatitis C virus; AIH, autoimmune hepatitis.
Liver International (2012)© 2012 John Wiley & Sons A/S4
Post–LT biliary strictures Iacob et al.

Chemokine and cytokine patterns in patients with biliarycomplications
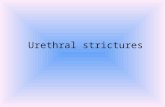
Levels of IFN-c, IL-10, IL-6 were significantly higher inthe ITBL group compared with control groups(P = 0.01, P = 0.007, P = 0.0003, respectively; Fig. 1A).IL17, IL-2, IL-4, TNF-a, CCL3, CCL5 and CX3CL1serum concentrations did not differ between bothgroups. There was a significantly higher IL-10/IFN-cratio in the ITBL group (0.93 ± 0.10 vs 0.71 ± 0.10,P = 0.02), as well as a higher IL-10/IL-2 ratio(0.77 ± 0.09 vs 0.6 ± 0.11, P = 0.03).
Patients with AS had significantly higher serum con-centrations of IFN-c (P = 0.02), IL-10 (P = 0.002) andIL-6 (P = 0.003) compared with the control groups(Fig. 1B). There was also a significantly higher IL-10/IFN-c ratio in the AS group compared with those in thecontrol groups (1.53 ± 0.23 vs 0.71 ± 0.10, P = 0.0002).Subgroups of patients with AS and controls, both carry-ing the CX3CR1-249II allele, had comparable CX3CL1serum concentrations (P = 0.51).
Discussion
Biliary strictures represent a major complication affect-ing both short- and long-term outcome of LT patients.In concordance with other studies (16–21), increasedpreservation allograft injury, as reflected by high post-operative peak levels of serum AST and older donor agewere associated with a higher prevalence of ITBL. Inaddition, in our study, we found that older recipient agewas associated with ITBL occurrence. A possible expla-nation might be sought in the concept of immunosenes-
cence, which is characterized by a disrupted immunebalance with a latent systemic pro-inflammatory statusand augmented anti-inflammatory cytokine response(22).
Consistent with two previous reports (9, 10) and incontrast to another report (23) presence of loss-of-func-tion CCR5D32 mutation was associated with anincreased risk of ITBL development. The expression ofchemokines in transplanted organs is complex and regu-lated by specific tissue as well as by time after transplan-tation (24). CCR5, which appears to be preferentiallyexpressed on T helper cells type 1 (Th1) (25), has a criti-cal role for migration of alloreactive T cells in hepatictissue (26). In case of a non-functional receptor in Th1cells, a T helper type 2 (Th2) pattern of T-cell activationis supposed to prevail, leading to dysregulation of allo-reactive AB responses (27). For instance, it has beenshown that donor-specific AB produced in CCR5-defi-cient heart and renal allograft recipients are sufficient todirectly mediate humoural graft rejection (28, 29).
Several clinical risk factors for AS have been reportedin the literature, including post-operative bile leakage,female donor/male recipient combination and right-lobe living-donor LT (2). None of these factors was rele-vant in our study, whereas LT for ALF was identified asan independent risk factor for development of AS. Dys-regulated systemic cytokine expression in the course ofALF may lead to increased inflammatory infiltrate anddamage of the allograft, which then results in a fibrogen-ic healing process (30).
ABO-blood group incompatible LT has long beenrecognized to be associated with inferior graft survivalrates (20, 31). A putative pathomechanism might be
Table 3. Results of univariate analysis of immunological risk factors for AS and ITBL development following LT
VariableControl group(n = 85)
AS group(n = 40) P value*
ITBL group(n = 37) P value†
CCR2-V64I (VI+II) 22.4% 17.5% 0.53 18.9% 0.67CCR5-D32 (wt/D32 + D32/D32) 14.1% 10% 0.52 32.4% 0.01CX3CR1-V249I (II) 7.1% 20% 0.03 10.8% 0.48CX3CR1-T280M (MM) 3.5% 5% 0.65 0% 0.55ABO compatible, not identical LT‡ 2.4% 12.5% 0.03 5.4% 0.58HLA AB class I positive 34.1% 30% 0.64 21.6% 0.16Donor-specific AB class I positive 3.5% 5% 0.69 2.7% 0.99HLA AB class II positive 31.8% 32.5% 0.93 35.1% 0.71Donor-specific AB class II positive 8.2% 22.5% 0.02 16.2% 0.18History of acute rejection episode(s) 20% 27.5% 0.34 18.9% 0.89MICA AB positive 25.9% 22.5% 0.68 18.9% 0.40Soluble MICA (ng/ml) 0.27 ± 0.04 0.42 ± 0.10 0.34 0.38 ± 0.07 0.14Soluble MICB (ng/ml) 0.011 ± 0.004 0.013 ± 0.007 0.89 0.017 ± 0.007 0.31Soluble ULBP2 (ng/ml) 0.053 ± 0.01 0.092 ± 0.03 0.50 0.057 ± 0.02 0.78
Values are expressed as mean ± SD or percentages.
*P value for AS group vs control group
†P value for ITBL group vs control group.
‡All ABO-compatible LT were realized with donor blood type O, except for one with donor type B for an AB positive recipient.
AS, anastomotic stenosis; ITBL, ischaemic type biliary lesions; LT, liver transplantation; AB, antibodies; sMICA/MICB, soluble major histocompatibility
complex class I-related chain A/B; soluble ULBP2, soluble UL16 binding protein 2.
Liver International (2012)© 2012 John Wiley & Sons A/S 5
Iacob et al. Post–LT biliary strictures

related to immune-mediated injury, given that bloodgroup-related antigens are physiologically expressed oncholangiocytes in larger bile ducts and, in pathological
conditions, also on smaller intrahepatic bile ductules(32). There are conflicting results in the literature withrespect to ABO-compatible non-identical LT indicatingeither a similar (33) or an inferior (34) outcome. Inter-estingly, LT across the Rhesus blood group barrier hasalso been reported to increase the risk of biliary compli-cations (35). Our study is the first showing that ABO-compatible non-identical LT bears an increased risk fordevelopment of AS. The potential clinical relevance andimpact of anti-HLA AB on allograft outcome has beenwell established in kidney transplantation (36, 37),whereas its role in allograft outcome and biliary strictureformation is unclear in the LT setting (11, 38, 39). Inthis study, we found that occurrence of AS was associ-ated with the presence of donor-specific AB. If thesepreliminary observations are confirmed in large pro-spective studies, screening of anti-HLA AB might proveuseful for early detection of at-risk LT patients whocould benefit from increased surveillance and intensifiedimmunosuppressive therapy.
Table 4. Results of univariate analysis of recipient, donor and surgical risk factors for AS and ITBL development following LT
VariableControl group(n = 85)
AS group(n = 40) P value*
ITBL group(n = 37) P value**
Recipient FactorsRecipient age at LT (years) 47.3 ± 9.4 45.7 ± 13.5 0.96 50.9 ± 12.9 0.009Donor-recipient gender mismatch 30.6% 40% 0.29 48.6% 0.056MELD score at LT 17.7 ± 8.2 19.3 ± 8.8 0.24 20.9 ± 9.3 0.06Child-Pugh C classification 42.4% 40% 0.80 45.9% 0.71Acute liver failure (LT indication) 2.4% 12.5% 0.03 10.8% 0.06Partial LT (living related or split) 22.4% 35% 0.13 5.4% 0.03CMV infection 15.3% 17.5% 0.75 16.2% 0.89Presence of diabetes mellitus 30.6% 37.5% 0.44 27% 0.69Duct to duct biliary anastomosis 92.9% 85% 0.15 100% 0.17Bile leakage 15.3% 17.5% 0.75 5.4% 0.14Peak AST (U/L) 683.9 ± 97.8 830.4 ± 123.9 0.06 1061.2 ± 230.4 0.03Peak ALT (U/L) 609.7 ± 67.1 753.9 ± 117.9 0.33 786.4 ± 132.6 0.28Peak total bilirubin (mg/dl) 5.4 ± 4.4 6.6 ± 7.1 0.55 5.8 ± 4.4 0.52
Donor FactorsDonor age >50 years 29.4% 22.5% 0.41 59.5% 0.001Donor BMI (kg/m2) 24.8 ± 3.3 24.7 ± 4.1 0.52 25.0 ± 4.1 0.80Donor AST (U/L) 52.7 ± 75.2 42.6 ± 50.9 0.30 56.2 ± 61.0 0.34Donor ALT (U/L) 40.9 ± 44.6 34.5 ± 28.3 0.74 46.5 ± 44.9 0.46Donor c-GT (U/L) 64.6 ± 98.4 48.3 ± 83.8 0.80 74 ± 95.4 0.32Donor total bilirubin (mg/dl) 0.8 ± 1.0 0.6 ± 0.3 0.45 0.7 ± 0.3 0.52Donor sodium (mmol/L) 146.4 ± 8.1 144.8 ± 6.3 0.31 149.7 ± 8.3 0.051Cerebrovascular accident in donor 42.4% 30% 0.18 56.8% 0.14
Surgical FactorsCold ischaemia time (minutes) 474.6 ± 181.5 425.8 ± 184.7 0.33 425.1 ± 182.9 0.17Warm ischaemia time (minutes) 39 ± 15.0 36.8 ± 12.4 0.72 40.2 ± 14.7 0.68UW preservation solution‡ 57.6% 50% 0.42 54.1% 0.71
Values are expressed as mean ± SD or percentages.
*P value for AS group vs control group.
†P value for ITBL group vs control group.
‡Organ procurement was performed according to standard techniques by using the University of Wisconsin preservation solution or histidine-trypto-
phane-ketoglutarate solution.
AS, anastomotic stenosis; ITBL, ischaemic type biliary lesions; LT, liver transplantation; MELD, model of end stage liver disease; CMV, cytomegalovirus;
AST, aspartate aminotransferase; ALT, alanine aminotransferase, BMI, body mass index; c-GT, gamma-glutamyl-transferase; UW preservation solu-
tion, University of Wisconsin preservation solution.
Table 5. Results of multivariate analysis of AS and ITBL develop-ment following LT
Regressioncoefficient
Standarderror
v2
(b=0) P value
Variables as risk factors for ASABO compatibility 1.85 0.89 4.31 0.03Acute liverfailure at LT
1.85 0.89 4.31 0.03
CX3CR1-V249I (II) 1.30 0.60 4.69 0.03Variable as risk factor for ITBLCCR5-D32(wt/D32 + D32/D32)
1.09 0.51 4.58 0.03
AS, anastomotic stricture; ITBL, ischaemic type biliary lesion, LT, liver
transplantation; wt, wild type.
Liver International (2012)© 2012 John Wiley & Sons A/S6
Post–LT biliary strictures Iacob et al.

This study is the first showing an association betweenpolymorphisms of CX3CR1 and AS occurrence. Fractal-kine is a chemokine with both chemoattractant andcell-adhesive functions. The V249I and T280M poly-morphisms modulate the CX3CR1 receptor expressionand function (40). It has been reported that monocytes/macrophages lacking CX3CR1 undergo increased celldeath following liver injury, which then perpetuatesinflammation and results in enhanced liver fibrosis (41).The probable genetic association of CX3CR1 with ASoccurrence is also supported by other studies showing acorrelation between alterations of this gene and fibro-proliferative disorders such as systemic sclerosis (42),fibrostenosing Crohn’s disease (43), and advanced liverfibrosis in chronic hepatitis C (44).
Patients with ITBL and AS presented significantlyhigher levels of inflammatory cytokines (IFN-c and IL-6) and IL-10 compared with controls. In addition, wefound increased IL-10/IFN-c and IL-10/IL-2 serumratios in ITBL patients as well as increased IL-10/IFN-c
serum ratios in AS patients. IL-10 is a known inhibitorof cell-mediated inflammatory reactions and has beenshown to have considerable pro-fibrotic activity viainduction of pro-fibrotic mediator transforming growthfactor-beta 1 (45, 46). It has been suggested that IL-10acts as an anti-inflammatory factor at early inflamma-tory processes, whereas fibrotic activity predominates atlater more chronic stages and upon repair responses(47). However, IL-10 has complex effector propertiesand its exact role in the fibrotic reaction still remainscontroversial (45).
We acknowledge the limitations of our study. Forinstance, lacking investigation of chemokine receptorgene expression in the liver allograft might be viewed asa potential drawback. This, however, should be of minorrelevance as leucocytes constituting the inflammatoryinfiltrate are exclusively derived from the recipient anddonor CCR5 genotype has been shown not to be associ-ated with ITBL (10). It has also to be considered thatmultifactorial diseases, such as biliary strictures, are
25
15
20
P = 0.0003
5
10
pg/m
lpg
/ml
P = 0.01 P = 0.007
IFN-γITBL (–)
IFN-γITBL (+)
IL-10ITBL (–)
IL-10ITBL (+)
IL-17ITBL (–)
IL-17ITBL (+)
IL-6ITBL (–)
IL-6ITBL (+)
IL-4ITBL (–)
IL-4ITBL (+)
IL-2ITBL (–)
IL-2ITBL (+)
TNF-αITBL (–)
TNF-αITBL (+)
0
25
15
20
5
10
P = 0.002
P = 0.003
0
IFN-γAS (–)
IFN-γAS (+)
IL-10AS (–)
IL-10AS (+)
IL-17AS (–)
IL-17AS (+)
IL-6AS (–)
IL-6AS (+)
IL-4AS (–)
IL-4AS (+)
IL-2AS (–)
IL-2AS (+)
TNF-αAS (–)
TNF-αAS (+)
P = 0.02
(A)
(B)
Fig. 1. Box plots of serum cytokine levels in patients with ischaemic type biliary lesions (ITBL), anastomotic strictures (AS), and controls. Thetop and bottom of the boxes represent the first and third quartiles, respectively. The boxes enclose the interquartile range, with the medianvalue denoted by the horizontal line. Concentrations of IFN-c, IL-10 and IL-6 were significantly higher in the ITBL (A) and AS (B) groups com-pared with the control group. IFN, interferon; IL, interleukin.
Liver International (2012)© 2012 John Wiley & Sons A/S 7
Iacob et al. Post–LT biliary strictures

unlikely to exclusively depend on single gene polymor-phisms, thus revealing the necessity to investigate andidentify additional genetic factors. Moreover, our find-ings about increased cytokine levels in blood of ITBLand AS patients have to be interpreted cautiously as sys-temic inflammatory responses may not necessarilyreflect to the same extent ongoing intrahepatic inflam-matory events. Finally, our results might be biased dueto the large number of patients excluded during theselection process and the cross-sectional study design.Thus, our results need to be confirmed in larger pro-spective trials.
In conclusion, we expanded on previous workemphasizing the role of loss-of-function CCR5D32mutation for risk of ITBL development. Moreover, thisis the first study showing that AS occurrence is associ-ated with a single nucleotide polymorphism in theCX3CR1 gene as well as presence of donor-specific AB.Our findings may have relevance for predicting the riskof occurrence of biliary lesions post-LT and developingpreventive as well as therapeutic strategies to improveallograft survival.
References
1. Sharma S, Gurakar A, Jabbour N. Biliary strictures follow-ing liver transplantation: past, present and preventivestrategies. Liver Transpl 2008; 14: 759–69.
2. Verdonk RC, Buis CI, Porte RJ, et al. Anastomotic biliarystrictures after liver transplantation: causes and conse-quences. Liver Transpl 2006; 12: 726–35.
3. Verdonk RC, Buis CI, van der Jagt EJ, et al. Nonanasto-motic biliary strictures after liver transplantation, part 2:management, outcome, and risk factors for disease pro-gression. Liver Transpl 2007; 13: 725–32.
4. Buis CI, Geuken E, Visser DS, et al. Altered bile composi-tion after liver transplantation is associated with the devel-opment of nonanastomotic biliary strictures. J Hepatol2009; 50: 69–79.
5. Op Den Dries S, Sutton ME, Lisman T, Porte RJ. Protec-tion of bile ducts in liver transplantation: looking beyondischemia. Transplantation 2011; 92: 373–9.
6. Strazzabosco M, Fabris L, Spirli C. Pathophysiology ofcholangiopathies. J Clin Gastroenterol 2005; 39: S90–102.
7. Isse K, Harada K, Zen Y, et al. Fractalkine and CX3CR1are involved in the recruitment of intraepithelial lympho-cytes of intrahepatic bile ducts. Hepatology 2005; 41: 506–16.
8. Kruger B, Schroppel B, Murphy BT. Genetic polymor-phisms and the fate of the transplanted organ. TransplantRev (Orlando) 2008; 22: 131–40.
9. Moench C, Uhrig A, Lohse AW, Otto G. CC chemokinereceptor 5delta32 polymorphism-a risk factor for ische-mic-type biliary lesions following orthotopic liver trans-plantation. Liver Transpl 2004; 10: 434–9.
10. Op Den Dries S, Buis CI, Adelmeijer J, et al. The combina-tion of primary sclerosing cholangitis and CCR5-Delta32in recipients is strongly associated with the developmentof nonanastomotic biliary strictures after liver transplanta-tion. Liver Int 2011; 31: 1102–9.
11. Castillo-Rama M, Castro MJ, Bernardo I, et al. Preformedantibodies detected by cytotoxic assay or multibead arraydecrease liver allograft survival: role of human leukocyteantigen compatibility. Liver Transpl 2008; 14: 554–62.
12. Muro M, Marin L, Miras M, et al. Liver recipients har-bouring anti-donor preformed lymphocytotoxic antibod-ies exhibit a poor allograft survival at the first year aftertransplantation: experience of one centre. Transpl Immu-nol 2005; 14: 91–7.
13. Neumann UP, Guckelberger O, Langrehr JM, et al. Impactof human leukocyte antigen matching in liver transplanta-tion. Transplantation 2003; 75: 132–7.
14. Oudshoorn M, Horn PA, Tilanus M, Yu N. Typing ofpotential and selected donors for transplant: methodologyand resolution. Tissue Antigens 2007; 69(Suppl. 1): 10–2.
15. Heinemann FM. HLA genotyping and antibody character-ization using the luminex multiplex technology. TransfusMed Hemother 2009; 36: 273–8.
16. Li S, Stratta RJ, Langnas AN, et al. Diffuse biliary tractinjury after orthotopic liver transplantation. Am J Surg1992; 164: 536–40.
17. Pirenne J, Monbaliu D, Aerts R, et al. Biliary stricturesafter liver transplantation: risk factors and prevention bydonor treatment with epoprostenol. Transplant Proc 2009;41: 3399–402.
18. Nakamura N, Nishida S, Neff GR, et al. Intrahepatic bili-ary strictures without hepatic artery thrombosis after livertransplantation: an analysis of 1,113 liver transplantationsat a single center. Transplantation 2005; 79: 427–32.
19. Moench C, Moench K, Lohse AW, Thies J, Otto G. Pre-vention of ischemic-type biliary lesions by arterial back-table pressure perfusion. Liver Transpl 2003; 9: 285–9.
20. Heidenhain C, Pratschke J, Puhl G, et al. Incidence of andrisk factors for ischemic-type biliary lesions following ortho-topic liver transplantation.Transpl Int 2010; 23: 14–22.
21. Buis CI, Verdonk RC, van der Jagt EJ, et al. Nonanasto-motic biliary strictures after liver transplantation, part 1:radiological features and risk factors for early vs. late pre-sentation. Liver Transpl 2007; 13: 708–18.
22. Licastro F, Candore G, Lio D, et al. Innate immunity andinflammation in ageing: a key for understanding age-related diseases. Immun Ageing 2005; 2: 8.
23. Heidenhain C, Puhl G, Moench C, Lautem A, Neuhaus P.Chemokine receptor-5delta32 mutation is no risk factorfor ischemic-type biliary lesion in liver transplantation.J Transplant 2009; 2009: 436515.
24. Colvin BL, Thomson AW. Chemokines, their receptors,and transplant outcome. Transplantation 2002; 74: 149–55.
25. Bonecchi R, Bianchi G, Bordignon PP, et al. Differentialexpression of chemokine receptors and chemotacticresponsiveness of type 1 T helper cells (Th1s) and Th2s.J Exp Med 1998; 187: 129–34.
26. Murai M, Yoneyama H, Harada A, et al. Active participa-tion of CCR5(+)CD8(+) T lymphocytes in the pathogene-sis of liver injury in graft-versus-host disease. J Clin Invest1999; 104: 49–57.
27. Andres PG, Beck PL, Mizoguchi E, et al. Mice with a selec-tive deletion of the CC chemokine receptors 5 or 2 areprotected from dextran sodium sulfate-mediated colitis:lack of CC chemokine receptor 5 expression results in aNK1.1 + lymphocyte-associated Th2-type immuneresponse in the intestine. J Immunol 2000; 164: 6303–12.
Liver International (2012)© 2012 John Wiley & Sons A/S8
Post–LT biliary strictures Iacob et al.

28. Nozaki T, Amano H, Bickerstaff A, et al. Antibody-medi-ated rejection of cardiac allografts in CCR5-deficientrecipients. J Immunol 2007; 179: 5238–45.
29. Bickerstaff A, Nozaki T, Wang JJ, et al. Acute humoralrejection of renal allografts in CCR5(-/-) recipients. Am JTransplant 2008; 8: 557–66.
30. Streetz KL, Wustefeld T, Klein C, Manns MP, TrautweinC. Mediators of inflammation and acute phase response inthe liver. Cell Mol Biol (Noisy-le-grand) 2001; 47: 661–73.
31. Wu J, Ye S, Xu X, et al. Recipient outcomes after ABO-incompatible liver transplantation: a systematic reviewand meta-analysis. PLoS One 2011; 6: e16521.
32. Nakanuma Y, Sasaki M. Expression of blood group-relatedantigens in the intrahepatic biliary tree and hepatocytes innormal livers and various hepatobiliary diseases. Hepatolo-gy 1989; 10: 174–8.
33. Aladag M, Gurakar A, Camci C, et al. Compatible ABOmismatch and liver transplantation: a single center’s expe-rience. Exp Clin Transplant 2006; 4: 467–9.
34. Barone M, Avolio AW, Di LA, Burra P, Francavilla A.ABO blood group-related waiting list disparities in livertransplant candidates: effect of the MELD adoption.Transplantation 2008; 85: 844–9.
35. Busquets J, Castellote J, Torras J, et al. Liver transplanta-tion across Rh blood group barriers increases the risk ofbiliary complications. J Gastrointest Surg 2007; 11: 458–63.
36. Cardarelli F, Pascual M, Tolkoff-Rubin N, et al. Prevalenceand significance of anti-HLA and donor-specific antibod-ies long-term after renal transplantation. Transpl Int 2005;18: 532–40.
37. Terasaki PI, Ozawa M, Castro R. Four-year follow-up of aprospective trial of HLA and MICA antibodies on kidneygraft survival. Am J Transplant 2007; 7: 408–15.
38. Fontana M, Moradpour D, Aubert V, Pantaleo G, PascualM. Prevalence of anti-HLA antibodies after liver trans-plantation. Transpl Int 2010; 23: 858–9.
39. Ge X, Ericzon BG, Nowak G, et al. Are preformed anti-bodies to biliary epithelial cells of clinical importance inliver transplantation? Liver Transpl 2003; 9: 1191–8.
40. Faure S, Meyer L, Costagliola D, et al. Rapid progressionto AIDS in HIV+ individuals with a structural variant ofthe chemokine receptor CX3CR1. Science 2000; 287: 2274–7.
41. Karlmark KR, Zimmermann HW, Roderburg C, et al. Thefractalkine receptor CXCR1 protects against liver fibrosisby controlling differentiation and survival of infiltratinghepatic monocytes. Hepatology 2010; 52: 1769–82.
42. Marasini B, Cossutta R, Selmi C, et al. Polymorphism ofthe fractalkine receptor CX3CR1 and systemic sclerosis-associated pulmonary arterial hypertension. Clin DevImmunol 2005; 12: 275–9.
43. Brand S, Hofbauer K, Dambacher J, et al. Increasedexpression of the chemokine fractalkine in Crohn’s diseaseand association of the fractalkine receptor T280M poly-morphism with a fibrostenosing disease Phenotype. Am JGastroenterol 2006; 101: 99–106.
44. Wasmuth HE, Zaldivar MM, Berres ML, et al. The fractal-kine receptor CX3CR1 is involved in liver fibrosis due tochronic hepatitis C infection. J Hepatol 2008; 48: 208–15.
45. Wynn TA. Fibrotic disease and the T(H)1/T(H)2 para-digm. Nat Rev Immunol 2004; 4: 583–94.
46. Lee CG, Homer RJ, Cohn L, et al. Transgenic overexpres-sion of interleukin (IL)-10 in the lung causes mucusmetaplasia, tissue inflammation, and airway remodelingvia IL-13-dependent and -independent pathways. J BiolChem 2002; 277: 35466–74.
47. Barbarin V, Arras M, Misson P, et al. Characterization ofthe effect of interleukin-10 on silica-induced lung fibrosisin mice. Am J Respir Cell Mol Biol 2004; 31: 78–85.
48. Wada K, Takada T, Kawarada Y, et al. Diagnostic criteriaand severity assessment of acute cholangitis: Tokyo Guide-lines. J Hepatobiliary Pancreat Surg 2007; 14: 52–8.
Liver International (2012)© 2012 John Wiley & Sons A/S 9
Iacob et al. Post–LT biliary strictures