
Gadolinium: MRI Contrast Agent
6
Safety Concerns for Gadolinium: MRI Contrast Agent The medical field has for nearly 30 years regarded gadolinium based contrast agents used in MRI scans as safe and nontoxic, believing that gadolinium is rapidly and completely cleared from the body by the kidneys. However, in 2007, the FDA issued safety warnings for patients with kidney disease in whom gadolinium (Gd) was linked to Nephrogenic Systemic Fibrosis (NSF) [Parazella 2009]. NSF is a scleroderma-like condition with skin plaques that resemble “orange peel,” typically appearing symmetrically on the arms and legs and trunk. The fibrosis can progress to affect muscles, lung, liver, heart and kidneys. Despite the warning, gadolinium-based contrast agents (GBCA) continued to be considered extremely safe and without major adverse effects in people with normal kidney function. This belief has now been called into question with the discovery that gadolinium (Gd) is deposited in brain, bone, liver and skin, even in patients with normal kidney function [Kanda et al., 2016, 2015; Kanal et al., 2016; Murata et al., 2016; Ramalho et al., 2016, 2015]. The journal Magnetic Resonance Imaging published a special issue on gadolinium bioeffects and toxicity in December 2016. Our goal in sharing this information with you is to help you manage the risks associated with receiving MRI scans with contrast and any steps you may be able to take to help reduce those risks. What are the potential effects, both immediate and long-term? Acute reactions that have been reported include itching, rash, hives, skin discoloration, increased sweating, respiratory distress and acute kidney injury. Destruction of WBCs and RBCs (hemolysis) is also possible. Studies have not been systematically conducted to determine the optimal dose and best imaging time in patients with impaired kidney function, renal failure, in the elderly or in children. The long-term, cumulative effects of retained gadolinium in the body are not yet understood. Patients who report suffering from chronic symptoms related to Gd exposure have created online Gadolinium Toxicity support groups. Frequently reported symptoms [Burke et al., 2016; Semelka et al., 2016b; Ramalho et al., 2016; Broome et al., 2007] include: • Headache • Brain fog or difficulty concentrating • Central Pain Syndrome. Believed to be caused by CNS injury, Central Pain can affect a large portion of the body or be restricted to the hands or feet. Pain is typically constant, moderate to severe in intensity, and may be made worse by touch, movement, emotions, and temperature changes, usually cold temperatures. It is described as burning, "pins and needles" sensations, pressing or aching pain, often with brief bursts of sharp pain. Some people also experience numbness and loss of touch sensations on the feet or hands. • Bone pain deep in hip bones or ribs • Joint stiffness, swelling or pain • Difficulty moving or straightening arms, hands, legs or feet • Skin changes: burning or itching, red or dark patches, swelling, tightening or hardening of the skin • Edema in the skin, muscles and connective tissue of legs • Changes in vision or hearing • Muscle weakness The onset of symptoms is reported to be immediately following GBCA administration in 66% of cases, and within 6 weeks in 32% [Burke et al., 2016]. ______________________________________________________________________ © 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053 Physicians have been lulled into the belief that gadolinium based MRI contrast agents are “biologically inert.” Yet in it’s free, unbound state (Gd3+), it is a highly toxic heavy metal. Jeanne M. Wallace, PhD, CNC & Michelle Gerencser, MS Evidence-based cancer nutrition consulting since 1997. www.Nutritional-Solutions.net • [email protected] • (435) 563-0053
-
Upload
jeanne-m-wallace-phd -
Category
Health & Medicine
-
view
64 -
download
1
Transcript of Gadolinium: MRI Contrast Agent
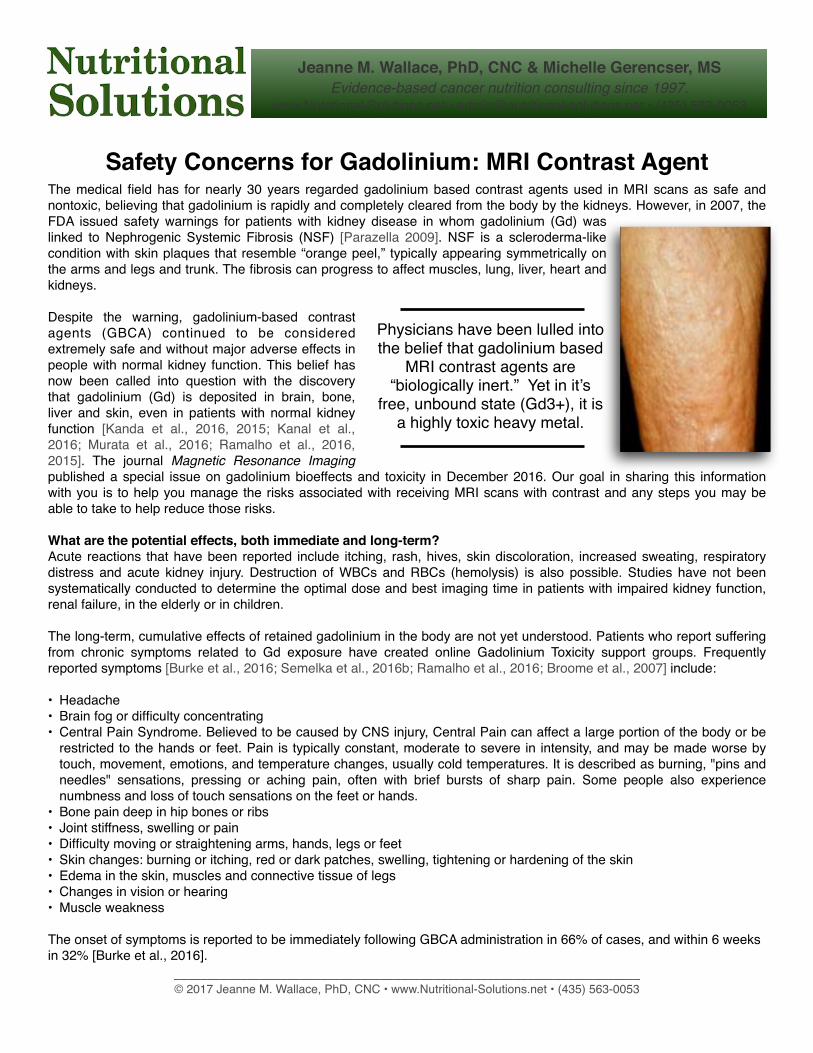
Safety Concerns for Gadolinium: MRI Contrast AgentThe medical field has for nearly 30 years regarded gadolinium based contrast agents used in MRI scans as safe and nontoxic, believing that gadolinium is rapidly and completely cleared from the body by the kidneys. However, in 2007, the FDA issued safety warnings for patients with kidney disease in whom gadolinium (Gd) was linked to Nephrogenic Systemic Fibrosis (NSF) [Parazella 2009]. NSF is a scleroderma-like condition with skin plaques that resemble “orange peel,” typically appearing symmetrically on the arms and legs and trunk. The fibrosis can progress to affect muscles, lung, liver, heart and kidneys.
Despite the warning, gadolinium-based contrast agents (GBCA) continued to be considered extremely safe and without major adverse effects in people with normal kidney function. This belief has now been called into question with the discovery that gadolinium (Gd) is deposited in brain, bone, liver and skin, even in patients with normal kidney function [Kanda et al., 2016, 2015; Kanal et al., 2016; Murata et al., 2016; Ramalho et al., 2016, 2015]. The journal Magnetic Resonance Imaging published a special issue on gadolinium bioeffects and toxicity in December 2016. Our goal in sharing this information with you is to help you manage the risks associated with receiving MRI scans with contrast and any steps you may be able to take to help reduce those risks.
What are the potential effects, both immediate and long-term?Acute reactions that have been reported include itching, rash, hives, skin discoloration, increased sweating, respiratory distress and acute kidney injury. Destruction of WBCs and RBCs (hemolysis) is also possible. Studies have not been systematically conducted to determine the optimal dose and best imaging time in patients with impaired kidney function, renal failure, in the elderly or in children.
The long-term, cumulative effects of retained gadolinium in the body are not yet understood. Patients who report suffering from chronic symptoms related to Gd exposure have created online Gadolinium Toxicity support groups. Frequently reported symptoms [Burke et al., 2016; Semelka et al., 2016b; Ramalho et al., 2016; Broome et al., 2007] include:
• Headache • Brain fog or difficulty concentrating• Central Pain Syndrome. Believed to be caused by CNS injury, Central Pain can affect a large portion of the body or be
restricted to the hands or feet. Pain is typically constant, moderate to severe in intensity, and may be made worse by touch, movement, emotions, and temperature changes, usually cold temperatures. It is described as burning, "pins and needles" sensations, pressing or aching pain, often with brief bursts of sharp pain. Some people also experience numbness and loss of touch sensations on the feet or hands.
• Bone pain deep in hip bones or ribs • Joint stiffness, swelling or pain• Difficulty moving or straightening arms, hands, legs or feet• Skin changes: burning or itching, red or dark patches, swelling, tightening or hardening of the skin• Edema in the skin, muscles and connective tissue of legs• Changes in vision or hearing• Muscle weakness
The onset of symptoms is reported to be immediately following GBCA administration in 66% of cases, and within 6 weeks in 32% [Burke et al., 2016].
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053
Physicians have been lulled into the belief that gadolinium based
MRI contrast agents are “biologically inert.” Yet in it’s
free, unbound state (Gd3+), it is a highly toxic heavy metal.
Jeanne M. Wallace, PhD, CNC & Michelle Gerencser, MSEvidence-based cancer nutrition consulting since 1997.
www.Nutritional-Solutions.net • [email protected] • (435) 563-0053
These emerging reports have led the U.S. FDA in July 2015 to announce an investigation into the risks of gadolinium brain deposits in people with normal kidney function.
What is Gadolinium?Gadolinium is a rare earth mineral with magnetic properties when exposed to magnetic fields. This property permits it to enhance the detail and clarity of diagnostic MRI and MRA scans. Medical imaging is the only known route of exposure in humans. The gadolinium ion is highly toxic so it must be chemically bonded (chelated) to a stable carrier molecule, a ligand. Properly chelated gadolinium is believed to remain in the extracellular space between cells—rather than being taken up by cells—thereby enhancing its rapid clearance by the kidneys [Mann 1993]. Reports suggest it is eliminated from the body within 2-4 hrs. In patients with impaired renal function, clearance may exceed 30 hrs, contributing to its toxicity. Animals studies have shown Gd present in skin biopsies 2-12 months after exposure [Pietsch et al., 2009], and human case reports find persistent Gd in skin and bone biopsies 3-8 years after last exposure [Darrah et al., 2009; Thakral et al., 2007].
So how does a so-called stable, chelated agent become toxic? It’s an problem of chelate stability. Reports suggest that once in the body, current gadolinium formulations become unchelated, exposing tissues to the toxic form, Gd3+ [Greenberg 2010; Mann 1993]. This process is called transmetallation and describes the dissociation of a metal from its chelating agent (ligand) in the presence of other competing metals. Minerals in the body—copper, calcium, iron and zinc—appear to compete with gadolinium for binding sites on the chelating agent, displacing Gd3+ [Thakral et al., 2007; Mann 1993]. Free, unbound gadolinium causes tissue injury via inflammation and fibrosis (scarring). Transmetallation is more likely to occur when Gd remains in the body for longer time periods, such as in those with poor kidney function. With this key mechanism of action revealed, it is hoped that the industry will develop GBCA with greater stability and reduced toxicity.
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053
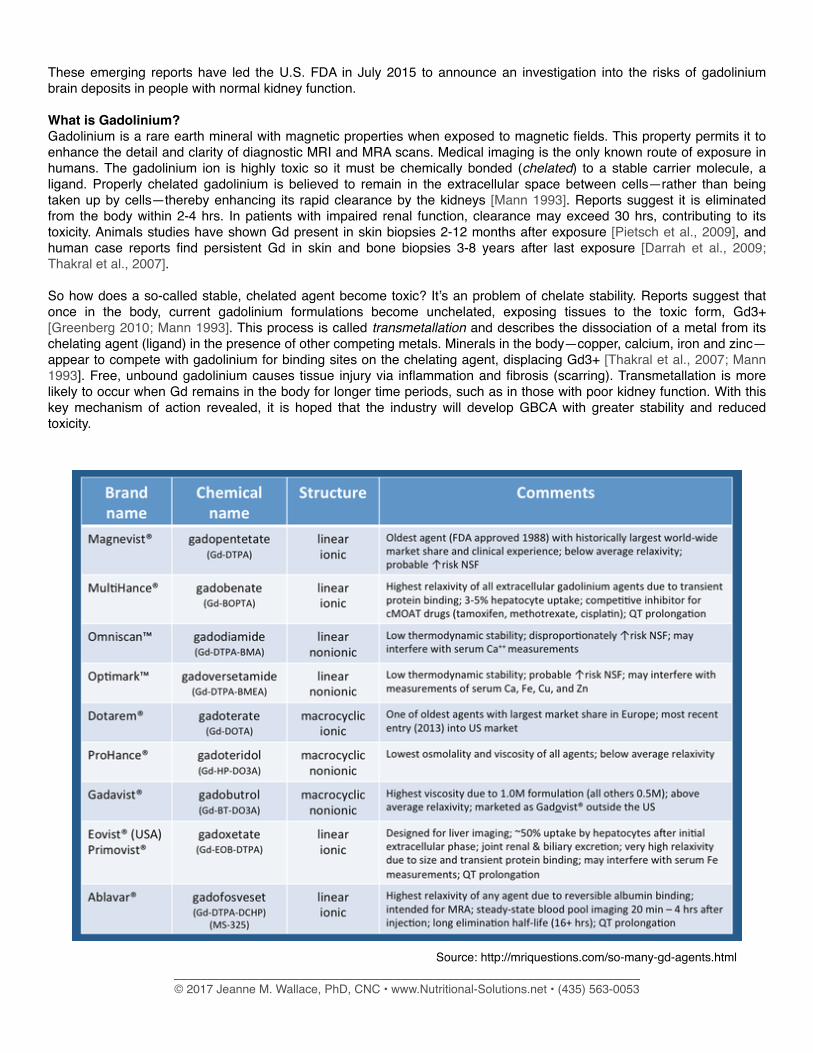
Source: http://mriquestions.com/so-many-gd-agents.html

Different Forms of Gadolinium
Nine different GBCA formulations are currently available (see chart above). They fall into 2 categories: linear and macrocyclic molecules. The latter has a ring structure where the Gd3+ is caged inside the chelated ligand, apparently providing a more stable molecule with improved safety [Radbruch et al., 2015; Runge 2001]. Nonionic linear GBCAs are reported to have the highest risk for NFS [Hasebroock & Serkova 2009]. Gd has been found deposited in tissues with both forms [Murata et al., 2016], but linear forms had deposition at 2.5-fold greater amounts [Gibby et al., 2004].
It might be worth noting which contrast agent you are given when you get your scan. You can also study the chart, and discuss with your doctor which agents are least likely to be harmful. This might be especially protective in long-term survivors who are a heightened risk of gadolinium accumulation from multiple ongoing scans.
How Does Gadolinium Harm the Body?CALCIUM: The Gd molecule very closely matches the size and structure of calcium. Gadolinium can bind to enzymes that usually require calcium as a co-factor such as the cell’s calcium channel. This inhibits the normal function of these enzymes.
IRON: A key mechanism that drives gadolinium toxicity is its interaction with iron. Gd prompts tissue resident macrophages, whose job it is to recycle iron, to release labile iron. This released, free iron causes injury, inflammation and fibrosis to the affected tissues [Swaminathan 2016]. Iron-rich structures of the brain appear to be most affected by Gd retention.
While not yet proven, this may mean that individuals with excess iron (high ferritin, for example) may be at higher risk. Noticing a drop in RBC levels, a sign of hemolysis, may key you in to this effect. Dietary and nutritional strategies to chelate iron may be relevant.
• Test ferretin and discuss with Your Nutrition Team self-care strategies to modulate excess iron• Use caution with iv Vitamin C! It can interact with iron in a fenton reaction, leading to further damage• Watch your RBC levels on your blood work decoder following your MRI scans
ZINC: When studies are done on the toxicity of Gd, the symptoms mimic zinc deficiency. It is likely that by binding zinc, Gd creates a relative or functional deficit of zinc.
ENZYMES: Gadolinium blocks a number of enzymes that are important for health.
Who may be at risk?While there are some reports of people having reactions to Gd after their first exposure, other studies suggest Gd accumulations become concerning after 6 scans. The dose given and form of Gd are also factors influencing risk.
• Long-term cancer survivors who, due to the high number of MRI scans over time, may bioaccumulate gadolinium
• Those who have on-going active disease being monitored with frequent, regular MRIs
• Anyone with reduced kidney function may develop increased gadolinium body burden. Symptoms of poor kidney function often do not appear until 80% of renal function is impaired. Be sure to have your kidney function has been tested before each MRI!
• Those who take medications that impair renal function or increase the risk of acute kidney injury (see box at right)
• This with excess iron or copper• Those who are given nonionic linear forms of Gd: Omniscan, Optimark, Magnevist
Should I stop getting scans?With new information about the potential risks associated with GBCAs, it can be tempting to avoid getting scanned. This may not be the best option! Instead, discuss with your doctor the benefits vs risks involved. For most people, obtaining
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053
Drugs that can Exacerbatethe Risk of Kidney Injury
AvastinPlatin-based chemotherapyDiureticsNSAIDsACE inhibitorsAngiotensin II receptor blockersStatinsFluoroqunolonesTetracyclines

essential medical information about their tumor far outweighs the risks. At the same time, you can ask that the frequency and interval of MRI scans be reduced to that which is truly medically necessary. If you have compromised renal function, you may need to discuss alternate means of imaging with your doctor.
Protective Steps to ConsiderOur office has worked with many long-term survivors who have had numerous scans, and we have not noted these toxicity symptoms among our clients. Our lead clinician, Michelle Gerencser, MS, notes that there are several reasons why our clients may be more protected:
• They chelate copper with molybdenum, which is neutral with regard to gadolinium.• They avoid iron and take steps to chelate iron when it’s level is excessive.• They avoid taking isolated calcium supplements, and mobilize circulating calcium into bone with vitamin K2 when it is
elevated in serum.• Clients who actively work with us have maintained healthy kidney function, even those with one kidney and those on
kidney-toxic medications. We teach them how to monitor and support kidney function.• Our clients have high sulfur diets (including high quality red meat, cruciferous vegetables and alliums like garlic and
onion), and this may help bind gadolinium.• Our clients sometimes use MSM, a type of sulfur, as part of their copper chelation protocol.• Our clients support their glutathione levels with whey protein powders and with low or very low glycemic diets.
BEFORE YOUR SCAN• Ensure you have been properly screened for kidney function [GFR > 60, tested within last 6 weeks], and if impaired
discuss alternate scanning options with your medical team. You may wish to consult with us regarding diet/nutritional support for kidney health.
• Drink adequate water prior to and immediately following your MRI screen. Let your medical team know if you think you may be dehydrated.
• Discuss the risks with your physician if you know you have excessively high levels of copper, iron, calcium and/or zinc (zinc toxicity leading to Gd retention has been reported in persons using denture creams that contain zinc [Greenberg 2010].
• Refer to our Caring for Your Kidneys program for diet and lifestyle strategies to improve renal health.• Avoid metabolic acidosis (when the blood and tissue pH falls below 7.35-7.45) which can increase the rate of Gd
retention [Peak & Sheller 2007]. You can check your Blood Work Decoder for these signs: high chloride and potassium with low calcium and CO2.
• Be aware that recent inflammatory events—injuries, infections, surgery, vascular procedures and blood clots—can increase your risk of retaining gadolinium from the administered GBCA [Sadowski et al., 2007; Peak & Sheller 2007]. You can check your most recent Blood Work Decoder for elevated hsCRP and D-dimer or Fibrinogen. Diet, nutrition and lifestyle strategies can help you resolve these issues.
AFTER YOUR SCANS• Boost glutathione levels. The precursor to GSH, N-acetyl cysteine or NAC, helps protect against the renal toxicity of
Gd3+ [Pereira et al., 2012]. However, NAC can have some negative effects. Therefore, lipoic acid, selenium and/or stabilized glutathione are better choices. Discuss dose, duration, frequency with us.
• Consider keeping a record of the number of MR scans with contrast you have had, together with their dates and which Gadolinium agent you were given.
• TESTING: you can test your gadolinium levels
Chelation therapy to remove gadolinium from the body is currently being researched by Drs. Jay, Semelka and Prybylski at the University of NC School of Medicine [Prybylski et al., 2016] but the best therapeutic plan and efficacy have not yet been reported. Reports from integrative medicine practitioners and environmental naturopaths in online forums have not reported much success using the typical oral chelation protocols with DMSA or EDTA, though iv chelation with Ca-EDTA (calcium-EDTA) has a few promising reports.
How Can I Tell if I have Gadolinium Toxicity?Genova Diagnostics offers urine testing for Gadolinium (and other heavy metals). The “Toxic Elements Clearance Profile” tests for 20 different heavy metals including gadolinium, and costs about $170 if ordered at www.DirectLabs.com [under the “Order Tests” tab choose “Specialty Labs”].
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053
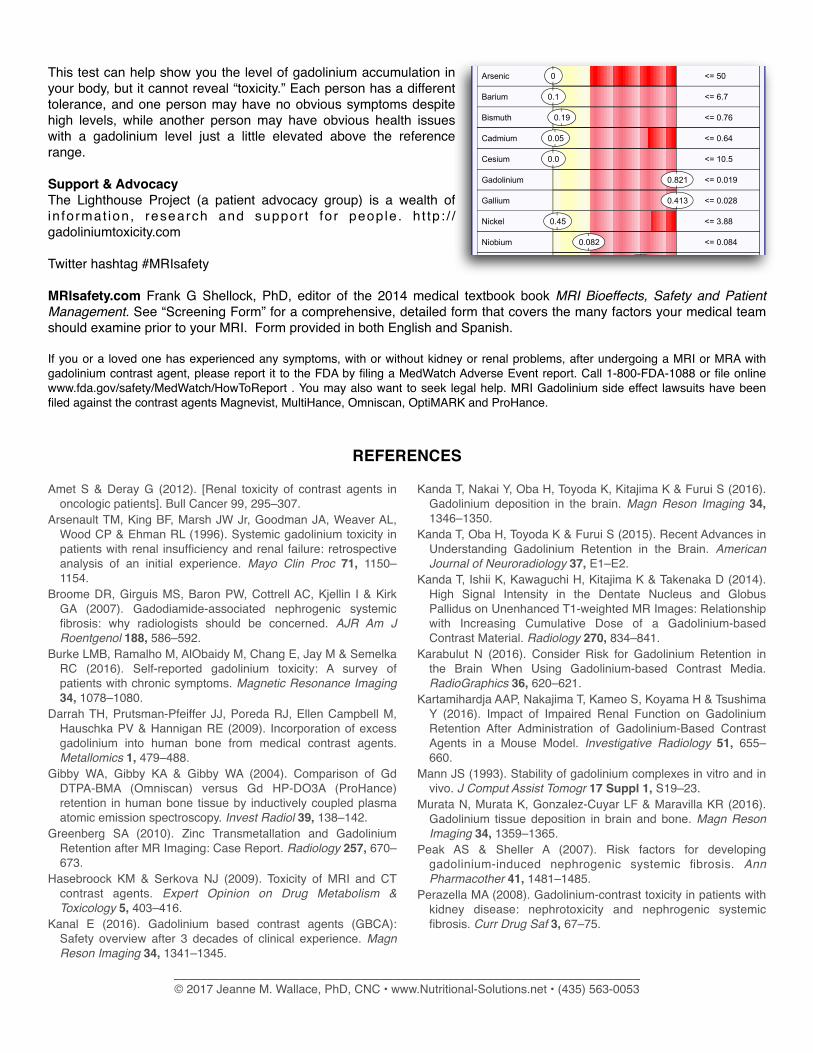
This test can help show you the level of gadolinium accumulation in your body, but it cannot reveal “toxicity.” Each person has a different tolerance, and one person may have no obvious symptoms despite high levels, while another person may have obvious health issues with a gadolinium level just a little elevated above the reference range.
Support & AdvocacyThe Lighthouse Project (a patient advocacy group) is a wealth of in format ion, research and suppor t for people . h t tp : / /gadoliniumtoxicity.com
Twitter hashtag #MRIsafety
MRIsafety.com Frank G Shellock, PhD, editor of the 2014 medical textbook book MRI Bioeffects, Safety and Patient Management. See “Screening Form” for a comprehensive, detailed form that covers the many factors your medical team should examine prior to your MRI. Form provided in both English and Spanish.
If you or a loved one has experienced any symptoms, with or without kidney or renal problems, after undergoing a MRI or MRA with gadolinium contrast agent, please report it to the FDA by filing a MedWatch Adverse Event report. Call 1-800-FDA-1088 or file online www.fda.gov/safety/MedWatch/HowToReport . You may also want to seek legal help. MRI Gadolinium side effect lawsuits have been filed against the contrast agents Magnevist, MultiHance, Omniscan, OptiMARK and ProHance.
REFERENCES
Amet S & Deray G (2012). [Renal toxicity of contrast agents in oncologic patients]. Bull Cancer 99, 295–307.
Arsenault TM, King BF, Marsh JW Jr, Goodman JA, Weaver AL, Wood CP & Ehman RL (1996). Systemic gadolinium toxicity in patients with renal insufficiency and renal failure: retrospective analysis of an initial experience. Mayo Clin Proc 71, 1150–1154.
Broome DR, Girguis MS, Baron PW, Cottrell AC, Kjellin I & Kirk GA (2007). Gadodiamide-associated nephrogenic systemic fibrosis: why radiologists should be concerned. AJR Am J Roentgenol 188, 586–592.
Burke LMB, Ramalho M, AlObaidy M, Chang E, Jay M & Semelka RC (2016). Self-reported gadolinium toxicity: A survey of patients with chronic symptoms. Magnetic Resonance Imaging 34, 1078–1080.
Darrah TH, Prutsman-Pfeiffer JJ, Poreda RJ, Ellen Campbell M, Hauschka PV & Hannigan RE (2009). Incorporation of excess gadolinium into human bone from medical contrast agents. Metallomics 1, 479–488.
Gibby WA, Gibby KA & Gibby WA (2004). Comparison of Gd DTPA-BMA (Omniscan) versus Gd HP-DO3A (ProHance) retention in human bone tissue by inductively coupled plasma atomic emission spectroscopy. Invest Radiol 39, 138–142.
Greenberg SA (2010). Zinc Transmetallation and Gadolinium Retention after MR Imaging: Case Report. Radiology 257, 670–673.
Hasebroock KM & Serkova NJ (2009). Toxicity of MRI and CT contrast agents. Expert Opinion on Drug Metabolism & Toxicology 5, 403–416.
Kanal E (2016). Gadolinium based contrast agents (GBCA): Safety overview after 3 decades of clinical experience. Magn Reson Imaging 34, 1341–1345.
Kanda T, Nakai Y, Oba H, Toyoda K, Kitajima K & Furui S (2016). Gadolinium deposition in the brain. Magn Reson Imaging 34, 1346–1350.
Kanda T, Oba H, Toyoda K & Furui S (2015). Recent Advances in Understanding Gadolinium Retention in the Brain. American Journal of Neuroradiology 37, E1–E2.
Kanda T, Ishii K, Kawaguchi H, Kitajima K & Takenaka D (2014). High Signal Intensity in the Dentate Nucleus and Globus Pallidus on Unenhanced T1-weighted MR Images: Relationship with Increasing Cumulative Dose of a Gadolinium-based Contrast Material. Radiology 270, 834–841.
Karabulut N (2016). Consider Risk for Gadolinium Retention in the Brain When Using Gadolinium-based Contrast Media. RadioGraphics 36, 620–621.
Kartamihardja AAP, Nakajima T, Kameo S, Koyama H & Tsushima Y (2016). Impact of Impaired Renal Function on Gadolinium Retention After Administration of Gadolinium-Based Contrast Agents in a Mouse Model. Investigative Radiology 51, 655–660.
Mann JS (1993). Stability of gadolinium complexes in vitro and in vivo. J Comput Assist Tomogr 17 Suppl 1, S19–23.
Murata N, Murata K, Gonzalez-Cuyar LF & Maravilla KR (2016). Gadolinium tissue deposition in brain and bone. Magn Reson Imaging 34, 1359–1365.
Peak AS & Sheller A (2007). Risk factors for developing gadolinium-induced nephrogenic systemic fibrosis. Ann Pharmacother 41, 1481–1485.
Perazella MA (2008). Gadolinium-contrast toxicity in patients with kidney disease: nephrotoxicity and nephrogenic systemic fibrosis. Curr Drug Saf 3, 67–75.
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053
<= 50 Arsenic 0
<= 6.7 Barium 0.1
<= 0.76 Bismuth 0.19
<= 0.64 Cadmium 0.05
<= 10.5 Cesium 0.0
<= 0.028 Gallium 0.413
<= 3.88 Nickel 0.45
<= 0.084 Niobium 0.082
<= 0.019 Gadolinium 0.821

Perazella MA (2009). Current Status of Gadolinium Toxicity in Patients with Kidney Disease. Clinical Journal of the American Society of Nephrology 4, 461–469.
Pereira LVB, Shimizu MHM, Rodrigues LPMR, Leite CC, Andrade L & Seguro AC (2012). N-acetylcysteine protects rats with chronic renal failure from gadolinium-chelate nephrotoxicity. PLoS ONE 7, e39528.
Pietsch H, Lengsfeld P, Jost G, Frenzel T, Hütter J & Sieber MA (2009). Long-term retention of gadolinium in the skin of rodents following the administration of gadolinium-based contrast agents. European Radiology 19, 1417–1424.
Prybylski JP, Semelka RC & Jay M (2016). Can gadolinium be re-chelated in vivo? Considerations from decorporation therapy. Magn Reson Imaging 34, 1391–1393.
Radbruch A, Weberling LD, Kieslich PJ, Eidel O, Burth S, Kickingereder P, Heiland S, Wick W, Schlemmer H-P & Bendszus M (2015). Gadolinium Retention in the Dentate Nucleus and Globus Pallidus Is Dependent on the Class of Contrast Agent. Radiology 275, 783–791.
Ramalho J, Ramalho M, Jay M, Burke LM & Semelka RC (2016). Gadolinium toxicity and treatment. Magnetic Resonance Imaging 34, 1394–1398.
Ramalho J, Semelka RC, Ramalho M, Nunes RH, AlObaidy M & Castillo M (2015). Gadolinium-Based Contrast Agent Accumulation and Toxicity: An Update. American Journal of Neuroradiology 37, 1192–1198.
Rogosnitzky M & Branch S (2016). Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals 29, 365–376.
Runge VM (2001). Safety of magnetic resonance contrast media. Top Magn Reson Imaging 12, 309–314.
Sadowski EA, Bennett LK, Chan MR, Wentland AL, Garrett AL,
Garrett RW & Djamali A (2007). Nephrogenic systemic fibrosis: risk factors and incidence estimation. Radiology 243, 148–157.
Semelka RC, Commander CW, Jay M, Burke LMB & Ramalho M (2016a). Presumed Gadolinium Toxicity in Subjects With Normal Renal Function. Investigative Radiology 51, 661–665.
Semelka RC, Ramalho J, Vakharia A, AlObaidy M, Burke LM, Jay M & Ramalho M (2016b). Gadolinium deposition disease: Initial description of a disease that has been around for a while. Magn Reson Imaging 34, 1383–1390.
Semelka RC, Ramalho M & Jay M (2016c). Summary of special issue on gadolinium bioeffects and toxicity with a look to the future. Magnetic Resonance Imaging 34, 1399–1401.
Swaminathan S (2016). Gadolinium toxicity: Iron and ferroportin as central targets. Magnetic Resonance Imaging 34, 1373–1376.
Thakral C, Alhariri J & Abraham JL (2007). Long-term retention of gadolinium in tissues from nephrogenic systemic fibrosis patient after multiple gadolinium-enhanced MRI scans: case report and implications. Contrast Media & Molecular Imaging 2, 199–205.
Thomsen HS (2008). Is NSF only the tip of the “gadolinium toxicity” iceberg? Journal of Magnetic Resonance Imaging 28, 284–286.
Todd DJ & Kay J (2008). Nephrogenic systemic fibrosis: an epidemic of gadolinium toxicity. Curr Rheumatol Rep 10, 195–204.
White GW, Gibby WA & Tweedle MF (2006). Comparison of Gd(DTPA-BMA) (Omniscan) Versus Gd(HP-DO3A) (ProHance) Relative to Gadolinium Retention in Human Bone Tissue by Inductively Coupled Plasma Mass Spectroscopy. Investigative Radiology 41, 272–278.
______________________________________________________________________© 2017 Jeanne M. Wallace, PhD, CNC • www.Nutritional-Solutions.net • (435) 563-0053

















![Diagnostic and treatment modalities for patients with ...gadolinium contrast-enhanced MRI with superior soft tissue resolution [43]. In case of a cervical lymph node metastasis, the](https://static.fdocuments.net/doc/165x107/60ef0b4b1967d215f7539337/diagnostic-and-treatment-modalities-for-patients-with-gadolinium-contrast-enhanced.jpg)