Funduscopy Ho
29
What is funduscopy? And… Why is it important to you?
-
Upload
saadah-munawaroh-hd -
Category
Documents
-
view
216 -
download
2
description
Funduscopy Ho
Transcript of Funduscopy Ho

What is funduscopy?And…
Why is it important to you?

Web sites of interest:
Welch Alleyn www.panoptic.welchallyn.com http://www.welchallyn.com/medical/ go to
“optometry student” menu drop down
Red Atlashttp://www.redatlas.com

Review of ocular anatomy

Retinal Layers

Optic Nerve Anatomy

Choroidal Vessels

Funduscopy Techniques/instruments
Direct Ophthalmoscopy
Indirect Ophthalmoscopy
Fundus Biomicroscopy
Fundus Contact Lens

Why do we dilate pupils?

Direct OphthalmoscopyAdvantages Portable Easy to use Upright image Magnification 15x Can use w/o dilation
Disadvantages Small field of view Lack of stereopsis Media opacities can degrade
image
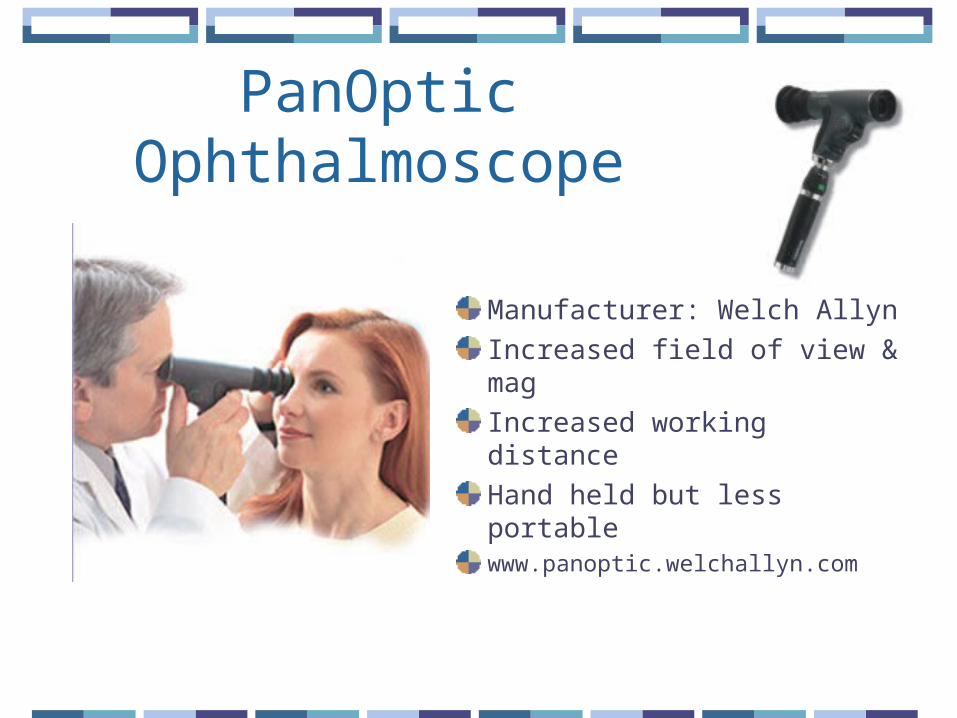
PanOptic Ophthalmoscope
Manufacturer: Welch Allyn
Increased field of view & mag
Increased working distance
Hand held but less portablewww.panoptic.welchallyn.com

Indirect Ophthalmoscopy
Monocular or binocularAdvantages: Wide field of view Binocular instruments
provide stereopsis
Disadvantages: Requires more skill Decreased magnification
(3x) Requires dilation Inverted image

Indirect Ophthalmoscopy

Fundus Biomicroscopy
Field of View & Mag: FOV <indirect but
>direct varies w/lens & slit
lamp mag
Inverted imageStereopsisDilated pupilRequires skill

Fundus Biomicroscopy

Fundus Contact LensRequires physical contact w/eye
Viewed w/Biomicroscope
Advanced dx & surgery
Field of view & Mag vary w/lens design

Direct Ophthalmoscopy: Basic skills
Optics: Illumination system Magnifier
Hyperopes myopes
Observation system Lens wheel Apertures


Direct Ophthalmoscopy: Basic skills
Viewing ocular media Observe red reflex Look for media
opacities Cataracts Corneal scars Large floaters

Direct Ophthalmoscopy: Basic skills
Proper position for central fundus viewing
Right eye to right eye
Left eye to left eye
Don’t rub noses…

Direct Ophthalmoscopy: Basic skills
Proper position for peripheral fundus viewing

Direct Ophthalmoscopy: Exam technique
Be systematicStart at optic disc & work radiallyObserve:Optic disc: C/D ratioVessels: course & caliber, AV ratio, light
reflex, crossings/bankingMaculaPeripheral fundus
Direct Ophthalmoscopy: Basic skills
Clinical pearlsFOV incr. when closer to Pt. Larger pupil increases FOV Contact lensesCheck lens wheel– watch accommodation

Normal Fundus

Viewing the Optic Nerve Head
Observe:SizeShapeColorMarginsCup to disc ratio (C/D) horiz & Vert
Blood Vessel Evaluation
Observe:Vessel diameterShape/tortuosityColorCrossingsLight reflexArtery/Vein (A/V) ratio: after 2nd bifurcation

Hypertensive Retinopathy
Scheie classification:I: Thinning of retinal arterioles relative
to veinsII: Obvious arteriolar narrowing w/focal areas
of attenuationIII: Stage II + cotton wool spots, exudates &
hemesIV: Stage III + swollen optic disk (similar to
papilledema)
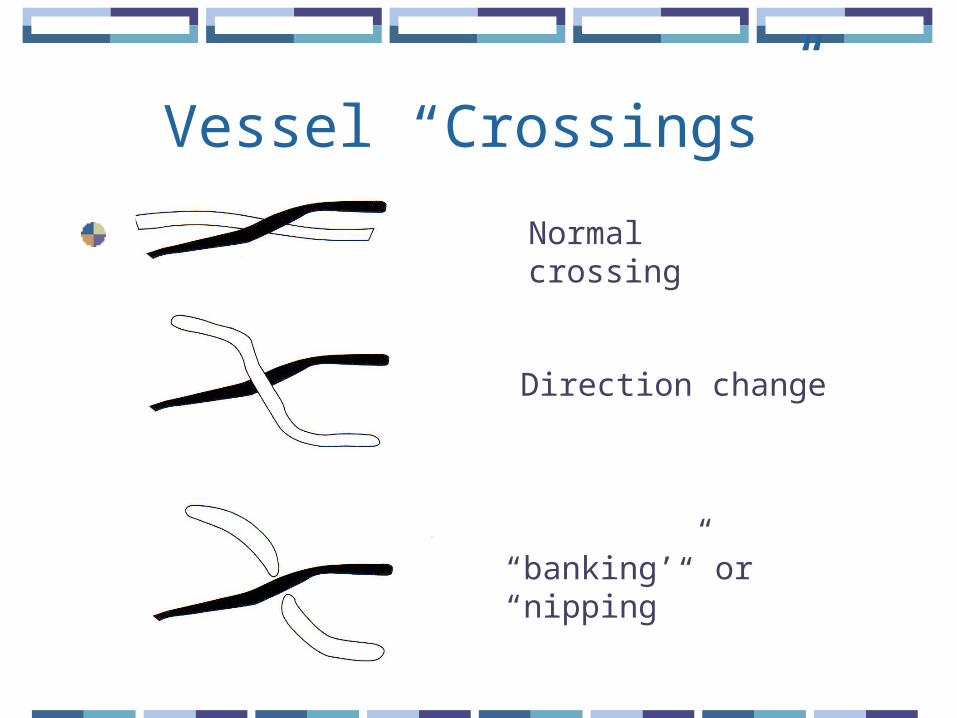
Vessel “Crossings”
Normal crossing
Direction change
“banking’” or “nipping”
Arteriolosclerosis
Increased light reflex (1/2)
“Copper wire” arterioles
“Silver wiring” arterioles whitish appearance w/continuing sclerosis
Increased A/V crossings

Macula
Lies about 2DD (disc diameters) temporal to the optic disc
Should be avascular
May appear darker red than surrounding retina
Should see bright foveal reflex on younger pts