Free Range Acupuncture (NYC) Intake Form p.1-5
7
Free Range Acupuncture Confidential Intake Form Name______________________________ Date________________Email_________________________________ Recommendations: 1 Why are you here today? How are you feeling compared to the last time you were here? How does your body feel ? Draw it! Notes!
-
Upload
tabitha-silver -
Category
Documents
-
view
212 -
download
0
description
It's your Story, and your Body. Everything we do with our bodies and everything that happens to us is written - like the grain of a tree - in our connective tissue, deep in our muscles and stored in our bones. Life & living - reverberates throughout our nervous systems - like waves - and affects our future ability to live and practice well. Unwind! Acupuncture can unwind you from the holding patterns that stress, accidents, hard work and family history have bound & contorted you into. Life is in our bodies and living is through our bodies - sometimes we get stuck. Come get unstuck. Reconnect with your body and the story that is within it. Come feel how to thrive wherever life takes you!
Transcript of Free Range Acupuncture (NYC) Intake Form p.1-5
Free Range Acupuncture Confidential Intake Form
Name______________________________ Date________________Email_________________________________
� � � �
Recommendations:!�1
Why are you here today? How are you feeling compared to the last time you were here? !
How does your body feel ?
Draw it!
Notes!

Free Range Acupuncture Confidential Intake Form
Energy & Emotions I have been having trouble with: (Circle all that apply) !
Anger Irritability Sensitivity Outbursts Worry Racing or-Repeating Thoughts Poor Memory Hyperactivity Anxiety Difficulty Concentrating Fatigue Sadness Depression Grief Boredom Isolation !
Sleep I sleep____hours per night.
I have difficulty w/: Vivid Dreams Falling sleep / Staying asleep/Getting up !
!• What do you do to Relax & Have Fun? !!!• What Practice, Image or Story calms & centers you? !!!• How’s your Energy? Too little/Enough/Too Much/ Uneven !!! !• What is your Primary Concern today - the main
thing that you want to work on improving?
Recommendations:!�2
Free Range Acupuncture Confidential Intake Form Please circle all of the following symptoms that apply: This / That !Headaches What are they like? !Recent / Recurrent & Chronic Sharp / Dull / Throbbing/Dizziness
!When are they? !Morning / Noon / Evening
!Where? !Back of Head/ Neck Forehead/ Temples Sides of head/ Top of head Whole head/ Behind Eyes
!
Aches, Pains or Numbness
Where is the primary area? Type: Ache/Pain / Numbness Whole Body Chest / Abdomen / Ribs/ Hips Shoulders /Hands/Arms/Elbows/ Hips/Knees/Feet Back: Upper/ Mid/ Lower
!What’s the pain like? !Sharp / Stabbing / Dull Throbbing/ Cramping Heavy / Swollen/ Radiating Feel to touch: Hot / Cold/ Numb
!Rate Discomfort 1-10:_______ !What makes the pain better?
Pressure / Heat / Cold Rest / Activity / Eating
!
Digestion, Food & Tastes
My relationship with food: !No appetite / Excessive Appetite Bingeing/ Cravings for - Sugar? Salt?/ Other:_________________
!I have trouble with: !Indigestion /Belching / Bloating / Gurgling Nausea / Vomiting / Ulcers Acid regurgitation / Heartburn Hernia / Severe Stomach Pain
!After Eating I feel:
My Best / Bad / Tired Pain !Taste in Mouth: Bitter/ Sweet / Sour / Salty / Pungent / Spicy
Recommendations:!�3
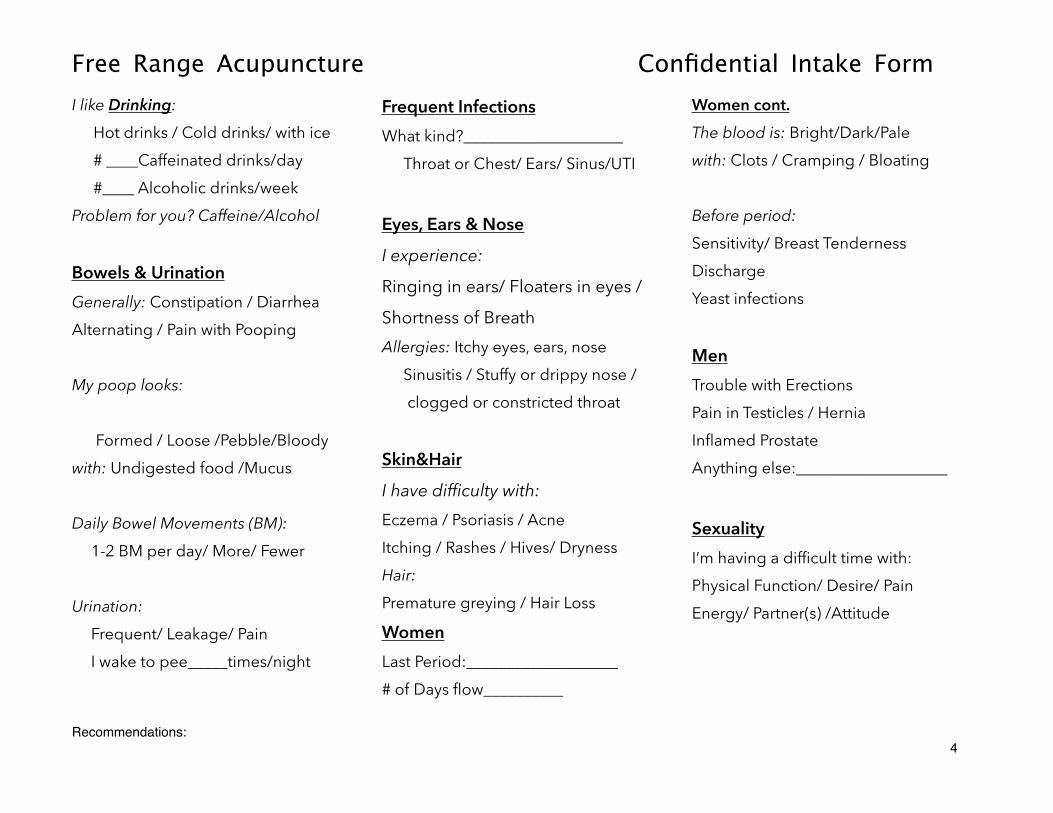
Free Range Acupuncture Confidential Intake Form I like Drinking:
Hot drinks / Cold drinks/ with ice # ____Caffeinated drinks/day #____ Alcoholic drinks/week
Problem for you? Caffeine/Alcohol !Bowels & Urination
Generally: Constipation / Diarrhea Alternating / Pain with Pooping !My poop looks: !Formed / Loose /Pebble/Bloody
with: Undigested food /Mucus !Daily Bowel Movements (BM):
1-2 BM per day/ More/ Fewer !Urination:
Frequent/ Leakage/ Pain I wake to pee_____times/night
!
Frequent Infections What kind?____________________
Throat or Chest/ Ears/ Sinus/UTI
!Eyes, Ears & Nose
I experience:
Ringing in ears/ Floaters in eyes /
Shortness of Breath Allergies: Itchy eyes, ears, nose
Sinusitis / Stuffy or drippy nose / clogged or constricted throat
!Skin&Hair
I have difficulty with: Eczema / Psoriasis / Acne Itching / Rashes / Hives/ Dryness Hair: Premature greying / Hair Loss
Women Last Period:___________________ # of Days flow__________
Women cont. The blood is: Bright/Dark/Pale with: Clots / Cramping / Bloating !Before period: Sensitivity/ Breast Tenderness Discharge Yeast infections !Men Trouble with Erections Pain in Testicles / Hernia Inflamed Prostate Anything else:___________________
!Sexuality I’m having a difficult time with: Physical Function/ Desire/ Pain Energy/ Partner(s) /Attitude !!!
Recommendations:!�4
Free Range Acupuncture Confidential Intake Form
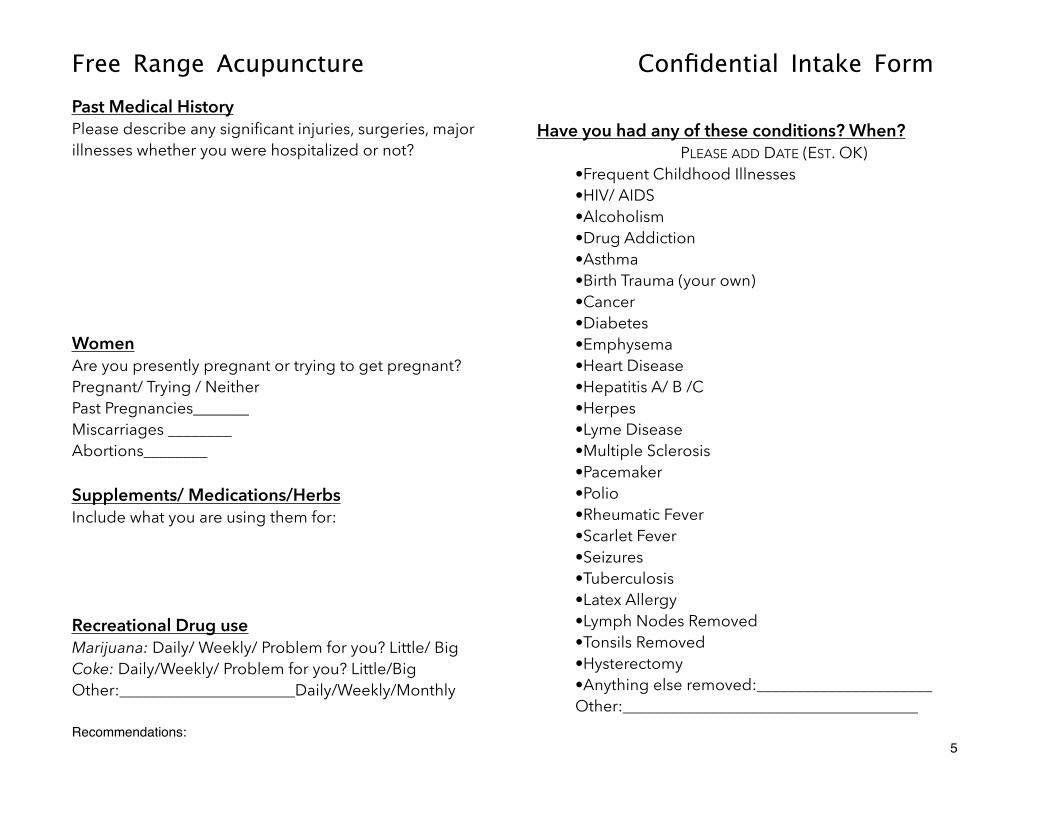
Past Medical History Please describe any significant injuries, surgeries, major illnesses whether you were hospitalized or not? !!!!!!!!Women Are you presently pregnant or trying to get pregnant?Pregnant/ Trying / Neither Past Pregnancies_______ Miscarriages ________ Abortions________ !Supplements/ Medications/Herbs Include what you are using them for: !!!!Recreational Drug use Marijuana: Daily/ Weekly/ Problem for you? Little/ Big Coke: Daily/Weekly/ Problem for you? Little/Big Other:______________________Daily/Weekly/Monthly
!Have you had any of these conditions? When?
PLEASE ADD DATE (EST. OK) •Frequent Childhood Illnesses •HIV/ AIDS •Alcoholism •Drug Addiction •Asthma •Birth Trauma (your own) •Cancer •Diabetes •Emphysema •Heart Disease •Hepatitis A/ B /C •Herpes •Lyme Disease •Multiple Sclerosis •Pacemaker •Polio •Rheumatic Fever •Scarlet Fever •Seizures •Tuberculosis •Latex Allergy •Lymph Nodes Removed •Tonsils Removed •Hysterectomy •Anything else removed:______________________ Other:_____________________________________
Recommendations:!�5

Free Range Acupuncture Confidential Intake Form
ATTUNMENT NOTES NAME:__________________________________ DATE:________________
Recommendations:!�6

Free Range Acupuncture Confidential Intake Form
� � TONGUE Pulse ! HT/SI LU/LI ! LV/GB SP/ST ! KD/UB PC/TH
!Circuit & Elements
Pattern of Fatigue LU LI ST SP` Spinal Irritation HT SI UB KD Diaphragm Constriction PC TH GB LV Cardiac Alarm Pelvic Collapse Fire Next Steps: Wood Earth Treatment Principle ! Metal ! Water
Points Muscles
Recommendations:!�7
!Palpation