
Acupuncture in Physiotherapy TM Acupuncture in ... - AACP
124
Acupuncture in Physiotherapy TM Journal of the Acupuncture Association of Chartered Physiotherapists Autumn 2018 Volume 30, Number 2 ISSN 2058-3281 Acupuncture in Physiotherapy Volume 30, Number 2, Autumn 2018
Transcript of Acupuncture in Physiotherapy TM Acupuncture in ... - AACP
Acupuncture in PhysiotherapyTM
Journal of the Acupuncture Associationof Chartered Physiotherapists
Autumn 2018 Volume 30, Number 2
ISSN 2058-3281
Acupuncture in Physiotherapy
TMVolum
e 30, Num
ber 2, Autum
n 2018
ACUPUNCTURE & MOXA TREATMENT ROOM
SPORTREHAB & EXERCISE
TAPING MASSAGE
SUPPORTS & BRACESCUPPING
© M
artin
mar
k | D
ream
stim
e
Sports & Physical Therapiesincluding Acupuncture, Moxibustion
Cupping, Magnetic and much more...
www.harmonymedical.co.ukt: +44 (0)208 5187337 e: [email protected]

Save The Date!DATE: Saturday 18th May 2019TIME: 9:00am - 5:00pm
DoubleTree by Hilton,London Docklands,London,SE16 5HW
4-for-3 GROUP DISCOUNTS
AACP ANNUAL CONFERENCE
2 0 1 9Celebrating our...
#AACP35
Join us in London for our biggest conference yet. We will also be celebrating our 35th anniversary on Friday 17th May with an evening of fun, food and festivities...with a few surprises! We are offering complimentary tickets to the anniversary celebrations for a limited number of conference delegates. Full speaker line-up to be announced soon. Join us on Facebook, Twitter and LinkedIn to make sure you don’t miss any announcements.
www.aacp.org.uk


© 2018 Acupuncture Association of Chartered Physiotherapists 3
Acupuncture in Physiotherapy
www.aacp.org.ukAcupuncture in Physiotherapy is printed twice a year for the membership of AACP. It aims to provide information for members that is correct at the time of going to press. Articles for inclusion should be submitted to the clinical editor at the address below or by email. All articles are reviewed by the clinical editor, and while every effort is made to ensure validity, views given by contributors are not necessarily those of the Association, which thus accepts no responsibility.
Editorial addressDr Val Hopwood18 Woodlands CloseDibden PurlieuSouthampton SO45 4JGUK
email: [email protected]
The AssociationThe British association for the practice of Western research-based acupuncture in physiotherapy, AACP is a professional network affiliated with the Chartered Society of Physiotherapy. It is a member-led organization, and with around 6000 subscribers, the largest professional body for acupuncture in the UK. We represent our members with lawmakers, the public, the National Health Service and private health insurers. The organization facilitates and evaluates postgraduate education. The development of professional awareness and clinical skills in acupuncture are founded on research-based evidence and the audit of clinical outcomes.
AACP LtdSefton House, Adam Court, Newark Road, Peterborough PE1 5PP, UK
Tel: 01733 390007
Printed in the UK by Henry Ling Ltd at the Dorset Press, Dorchester DT1 1HD
ContentsAutumn 2018
Editorial .................................................................................... 5Chairman’s report ................................................................... 7Chief Executive Officer’s report ......................................... 9AACP Annual Conference .................................................. 11
Literature reviewMechanisms and dose parameters of electric needle stimulation: clinical considerations – Part I by T. Perreault, S. O. Flannagan, M. T. Grubb & R. Grubb ......................... 17
ParadigmThe interaction and outcomes of acupuncture, both traditional Chinese medicine and intra- muscular stimulation, with Deep Oscillation® Treatment: a case study- based discussion by C. Boynes ................................... 27Practical applications of meridian theory in pain management – the meridian wave approach by A. Ziv & I. Levi ....................................................................................... 35
ResearchTypes of control in acupuncture clinical trials might affect the conclusion of the trials: a review of acupuncture on pain management by H. Chen, Z. Ning, W. L. Lam, W.- Y. Lam, Y. K. Zhao, J. W. F. Yeung, B. F.- L. Ng, E. T.- C. Ziea & L. Lao ................................. 45How placebo needles differ from placebo pills by Y. Chae, Y.- S. Lee, P. Enck ................................................... 55
Case reportsAcupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study by A. Manso.................................................................. 67Left elbow lateral epicondylalgia, treated successfully with acupuncture combined with typical physiotherapy intervention by Justin Walsh.................................................. 77The use of Seirin Pyonex indwelling needles in the treatment of non- traumatic low back pain – a case study by D. Giura .............................................................................. 83Acupuncture for pain relief in a patient following hip arthroscopic surgery by D. Atkinson .................................. 87Acupuncture for the treatment of whiplash associated disorder by Suzanne Cronin ................................................... 95
OpinionElectricity and electroacupuncture – a quick overview by L. Pearce ................................................................................ 105
ReviewsProduct review .................................................................... 109Book reviews ....................................................................... 111News, views and interviews .............................................. 115Guidelines for authors ....................................................... 117
The greatest Chinese medicine resource in the English language
three print issues a year
exclusive 24/7 online access to over 2000
articles and abstracts
exclusive online access to full 2000+ item JCM Research
Archive
Special offer - one month free access to the entire JCM online archives
1. Register on the website (jcm.co.uk) if you haven’t already done so
2. Send an email to [email protected] with ‘Special offer’ in the subject line (offer valid until December 31st 2018)
3. Wait for an email from us explaining how to access our vast 40-year archive of articles, abstracts and research news
Prices per year UK Europe
Practitioner £43 £46
Student £33 £36
Student group* £28 £31*(minimum ten subscriptions mailed to a single address) How to subscribe
Online at www.jcm.co.uk/subscribe
© 2018 Acupuncture Association of Chartered Physiotherapists 5
Acupuncture in Physiotherapy
www.aacp.org.uk
Journal Committee
Clinical EditorDr Val Hopwood FCSP
Corporate EditorBethan Griffiths(email: [email protected])
Book Review EditorWendy Rarity(email: [email protected])
News EditorRosemary Lillie(email: [email protected])
Public Relations and Marketing OfficerJennifer Clarkson(email: [email protected])
AACP Office ManagerLisa Stephenson(email: [email protected])
AACP Ltd Board Members
Chairman: Jon HobbsLesley PattendenPaul BattersbyDiana GiuraSuzanne NittaChris Collier MBEWendy RarityCaspar van Dongen Chief Executive Officer: Caspar van DongenAuditor: Rawlinsons, PeterboroughCompany Secretary: Michael Tolond
Editorial
Welcome to the Autumn 2018 edition of Acupuncture in Physiotherapy. After our long hot summer, now it’s time to concentrate on the interesting cases and current research in our chosen field. As usual we have a varied selec-tion. In this issue we have included three papers previously published in other journals. On the research front we offer Chen et al. (“Types of control in acupuncture clinical trials might affect the conclusion of the trials: a review of acupuncture on pain management”) (pp. 45–53), a really good look at some of the problems and also some of the solutions.
In the same vein we have offered Chae et al. (“How placebo needles differ from placebo pills?”) (pp. 55–66), which originates in the field of psychiatry and provides an overview of the characteristics of placebo needles and how they differ from placebo pills in two aspects: (1) physiological response and (2) blinding efficacy. The authors discuss alternative control strategies for the placebo effects in acupuncture therapy.
Amos Ziv has allowed republication of his article “Practical applications of meridian theory in pain management – the meridian wave approach” (pp. 35–43), which previously featured in the Journal of Chinese Medicine (October 2017).
We also have an opinion piece on electro-acupuncture by Lynn Pearce (pp. 105–107) and an excellently comprehensive introduction to dry needling from Dr Thomas Perreault (pp. 17–26).
As usual, our members have provided an absorbing collection of case studies: • André Manso on trochanteric bursitis
• Justin Walsh on epicondylalgia
• Suzanne Cronin on whiplash associated disorder
• Daniel Atkinson on hip arthroscopic surgery
• Diana Giura on low back pain.
Additionally, we also have some short sum-maries (compiled by Robert Millett) of the contributions from the speakers at the May conference, including John Cross, Lynn Pearce, Thomas Perreault, Johnny Wilson and Cheryl Mason.

Editorial
© 2018 Acupuncture Association of Chartered Physiotherapists6
Finally, you’ll find a selection of book reviews, an equipment review and some exciting news regarding Helene Langevin.
Dr Val Hopwood FCSP, FAACPClinical Editor, Acupuncture in Physiotherapy
© 2018 Acupuncture Association of Chartered Physiotherapists 7
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 7–8
Chairman’s report
Welcome to the latest edition of the Acupuncture Association of Chartered Physiotherapists (AACP) journal Acupuncture in Physiotherapy, in autumn 2018. Even through the long hot summer, the team at the AACP office has been working diligently to ensure the latter half of 2018 is as productive as the former was. Following on from the success of the AACP’s annual conference held on 19 May in Reading, we had two other key dates for the AACP diary in the autumn: 13 October for the AACP’s conference in Leeds, and 3 November for the AACP’s Scotland study day in Edinburgh. These are part of the continuing efforts of the AACP to reach members across the country and to improve access to ever expanding knowledge in research and approaches in clinical practice.
Notable speakers in Leeds included Dr Giovanna Franconi, Dr Daniel Keown and Dr Amali Lokugamage. Dr Giovanna Franconi is assistant professor of Internal Medicine at Tor Vergata University in Rome, and a member of the editorial board of the European Journal of Integrative Medicine. Dr Franconi presented the intriguing topic of “Traditional Chinese Medicine (TCM) and Acupuncture in the Omics Era.” Making a welcome return to the AACP conference stage was Dr Daniel Keown, author of the critically acclaimed book What God Forgot To Tell Surgeons. Following in the theme of this popular treatise, Dr Keown informed those in attendance why “Qi Exists!” Also presenting was internationally renowned consultant obstetrician and gynaecologist, and fellow of the Royal College of Obstetricians and Gynaecology, Dr Amali Lokugamage. Dr Lokugamage has been lauded for her work in promoting respectful care, dignity and autonomy in maternity services as well as lecturing on the origins of compassionate behaviour and social cohesion. Dr Lokugamage is a member of the board of directors of the UN- recognized International Motherbaby Childbirth Organization and sits on the advisory board of Human Rights in Childbirth, as well as
being on the editorial board for the International Journal of Childbirth. Dr Lokugamage presented an insightful talk exploring “Why Women Seek Acupuncture and Complementary Medicine for Women’s Health.” Another speaker of note was Chris Nortley. Chris brings 30 years of experience to the AACP stage, first as a clini-cal specialist nurse in psychiatry, and then as an acupuncturist treating inpatients and outpatients with a range of mental health and general medi-cal conditions in the National Health Service (NHS). A clinician of considerable standing, Chris was presented with an award by HRH The Prince of Wales for his work in integrating acupuncture into the NHS in 2003; in 2004 he was featured in the Independent on Sunday as one of the ten leading acupuncturists in the UK, and in 2011 he received an ‘Acupuncture Hero’ award from the British Acupuncture Council. Chris presented “an Introduction to Traditional Chinese Medicine.” Other speakers included the ever popular Andy Harrop presenting the rela-tionship of “the Adrenal Glands in Diagnosis and Treatment,” and AACP Fellow, David Mayor, who was “Exploring Amplitude in Transcutaneous Electroacupuncture Stimulation (TEAS).”
The Scotland study day in Edinburgh wel-comed four practicing clinicians to the stage to share their wealth of knowledge and clinical experience which informed their approaches to a variety of clinical scenarios. Subjects vary from “Acupuncture, Pain and the Emotional Mind” presented by John Wood, to “Acupuncture Within Sport” with Johnny Wilson, to “Acupuncture in Neurology” with Caroline McGuire. The day opened with Lynne Pearce’s insightful reflections on “Fascial Connections” and their relationship and influence within acu-puncture. Further information on the Leeds and Edinburgh events can be found on the AACP website.
This summer saw the appointment of a new AACP clinical advisor in the person of

Chairman’s report
© 2018 Acupuncture Association of Chartered Physiotherapists8
longstanding AACP tutor and acupuncture BSc lecturer, Paul Battersby. Paul has taken up the reins and has relished the new challenge of dealing with members’ enquiries in addition to reviewing research and supporting the devel-opment of a variety of AACP projects and member benefits. For support with your clinical queries please contact Paul directly at [email protected].
Following a recent update in IT services, the AACP has also opened up the archives and now the last ten years of the journal of the AACP is searchable online for members. Log in as an AACP member and search Acupuncture in Physiotherapy with a keyword, subject or author name. The system is updated every six months and forms a great research aid and another use-ful AACP member benefit.
There is also now more continuing profes-sional development (CPD) available than ever this year with one- and two- day courses cover-ing a variety of topics, from brushing up on basic skills to advanced needling techniques and concepts. Included within the CPD portfolio this year is the addition of another “Anatomy for Acupuncture” day. Now in its third year, this CPD event gives members the opportunity to work with Luke Welsh, Anatomy Teaching Fellow at Keele School of Medicine, and use state- of- the- art technology and cadavers to explore in intimate detail the human anatomy beneath the acupuncture points. From 2018 there will now be two events per year, one in May and one in November. This course is unique for the UK and has already attracted attendees from across the world who have an interest in expanding their knowledge of anatomy related to clinical application of acupuncture. If you are interested in attending any of the courses listed on the AACP website, or even hosting
one and obtaining free places, then please con-tact course administrator Claire Buckingham at [email protected].
The AACP’s public relations and marketing officer Jennifer Clarkson ([email protected]) has been busy this year across a number of media platforms promoting the skills and expe-rience of AACP members to the general public. Recent statistics show that over 9 million media contacts have been made in the last 12 months with potential patients of AACP members via a variety of print and electronic publications. Feel free to contact Jennifer directly to discuss promotional and media queries further.
This summer, the AACP team has also been working on the development of a significant new member benefit that is set for launch soon. Watch out for updates in the monthly e- newsletter on this great new resource free to AACP members.
Thank you as ever for your ongoing support for the AACP. Thanks to you, the AACP is approaching another milestone anniversary, with 2019 seeing its 35th year! Thirty- four years on, and the AACP administrative and management team continues to work hard to support mem-bers and deliver the best member experience possible. If, however, you feel there are issues the AACP need to be addressing or you have any ideas on how you would like to see the AACP develop or improve, particularly as we reach another landmark together, then please feel free to get in touch with the office or me directly ([email protected]). As ever, I look forward to catching up with you in person at an AACP event somewhere soon.
Jonathan HobbsAACP Chairman

© 2018 Acupuncture Association of Chartered Physiotherapists 9
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 9
Chief Executive Officer’s report
Musings on membership mutualityAs we approach the AACP’s 35th anniversary year in 2019, I would like to thank all AACP members, past and present, for their support of the Association through all those years. This has made us and kept us by far the longest established and largest organization represent-ing acupuncture in the UK.
At the AACP’s inaugural meeting in the autumn of 1984, its very first chairman, Mr Neville Greaves, couldn’t have imagined that someday the AACP would represent around 6000 acupuncture- physiotherapists.
Thirty- five years after its conception, as a mature organization, the AACP is going strong in representing your interests and promoting your acupuncture services to the British public at large. In turn, we wouldn’t be able to do this without the continued support of you, our members. For many years now you have helped us to be the largest acupuncture association in the country, and our size and clout is important in offering you the best possible support. This mutuality, this circularity of support, is the basis of our success: yours and AACP’s.
This mutuality expresses itself also in our organizational structure. As a company limited by guarantee, we are owned by and operate only for the benefit of our members. The AACP is run by a board of directors elected by the membership at the annual general meeting. And
a clear majority of board members are drawn from the membership. All income generated by the organization is spent for the benefit of AACP members now or in future years.
How much you are able to influence the AACP and what we do depends very much on your involvement with the organization. AACP committees regularly have a vacancy that needs to be filled. It isn’t necessary to wait for that, though; we are always open to ideas from members and sometimes a simple email may be sufficient to influence direction. Just let me know via [email protected] if there is anything you would like to share or discuss. It might be that one idea that makes the difference!
We may be 35 soon, but we will never stop innovating. In the coming few months we will be able to present some new technological developments that will be available to AACP members only. These new developments to sup-port you in your application of acupuncture in physiotherapy are in turn only possible through your continued membership of, and support for, your AACP.
The continuation of this synergetic mutuality for another 35 years will strengthen the founda-tions of the AACP, ensuring that we are able to improve and enhance the support for our members for many years to come.
Caspar van DongenChief Executive Officer

© 2018 Acupuncture Association of Chartered Physiotherapists 11
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 11–15
AACP Annual Conference, 19 May 2018
IntroductionThis year’s annual conference took place at the Hilton Hotel in Reading, where delegates were presented as usual with a wide range of informative and thought provoking material to develop their professional understanding and incorporate into their daily practice.
Summaries of the majority of these presenta-tions follow below, while Chris Boynes’ personal and clinical perspectives on the interaction and outcomes of Deep Oscillation® Therapy with acupuncture can be found in his article on pp. 27–34 in this issue of Acupuncture in Physiotherapy.
Acupuncture in women’s healthCheryl Mason A key question for delegates at the confer-ence was whether acupuncture could provide relief from pelvic girdle and low back pain in pregnancy. It was posed by Cheryl Mason, an acupuncturist with a private clinic in Leeds who has experience of working in NHS nurs-ing, midwifery and pain management teams. In her presentation, she outlined research findings which indicate that acupuncture can provide relief to pregnant women with these types of pain.
“A 2006 study (Van de Pol et al.) showed that acupuncture did appear to reduce low back pain and pelvic girdle pain during pregnancy, increas-ing people’s capacity to exercise and carry out daily activities,” she said. “Another study in 2009 (Wang et al.), using one week of continu-ous auricular acupuncture on the ears, showed a significant reduction in pain compared to sham acupuncture control groups.” She also cited the findings of a 2016 feasibility study and pilot randomized controlled trial which evaluated acupuncture and standard care for pregnant women with back pain. It was led by Chartered Society of Physiotherapy member Nadine Foster from Keele University. The study
compared three groups of pregnant women with back pain. One group received standard care that included two to four sessions of one- to- one physiotherapy and a self- management booklet. The second group received standard care, plus six to eight sessions of acupuncture. The third group received standard care, plus non- penetrating sham acupuncture.
“At the eight- week follow- up they found that 74% of participants favoured the addition of acupuncture,” said Ms Mason. She told delegates there were three possible ways acupuncture may ease pain: via a mechanical local action, a neurological action or a hormonal one. “The needles create a local trauma response – a flood of antihistamines, a mast cell response. And they have an influence on the muscle spindle, which is great if you are treating pelvic girdle pain, because you can treat local points and get results with the muscles, tissues and fascia. We also know acupuncture produces a neurological effect. For instance, there is the work of Hugh McPherson, who featured on the BBC’s ‘Trust Me I’m a Doctor’ in October 2014, using MRI scanners to show that pain modification centres in the brain light up during acupunc-ture. A lot of scientific research shows it’s not placebo. There are real effects produced by the needles.”
Delegates also heard that acupuncture could also have an effect on hormones, so it was important not to needle contraindicated points when treating pregnant women. “We know acupuncture can stimulate serotonin and oxytocin production, as well as other neuro-transmitters,” said Ms Mason. “In pregnancy the nervous system and endocrine system are quite delicate and predisposed for labour. If we are stimulating oxytocin production by insert-ing needles into certain points we could theo-retically stimulate labour. We need to be aware which points are safe to use.” She referred to a Cochrane Database review into acupuncture or
Conference 2018
© 2018 Acupuncture Association of Chartered Physiotherapists12
acupressure for induction of labour, published in October 2017. The review highlighted that acupuncture showed some benefit in improving cervical maturity, making it more favourable for labour. Therefore, using the wrong points could potentially result in this effect.
Ms Mason said there had been more than 8000 randomized controlled trials into acupunc-ture in the last eight years. “But there is still some confusion over its effectiveness, so we need more quality research,” she said. “What we do know, however, is that acupuncture has a good safety profile and is especially relevant for pregnancy and the treatment of pelvic girdle pain and other pregnancy- related conditions.” She added that, if attendees were planning a treatment protocol for women with pregnancy- related pelvic girdle and low back pain, research by Matthew Bauer (2016) indicated that 16 or more treatments of acupuncture lead to the greatest success rates.
Robert Millett
Acupuncture- physiotherapy in sports Johnny WilsonProfessional football players often experience low back pain which can be challenging and complex to treat, but acupuncture can help as part of a multimodal approach.
This was the message at the conference from Johnny Wilson, clinical director of Athlete Rebuild and former head physiotherapist for professional football clubs Notts County, Scunthorpe and Chesterfield. He shared his experience of how acupuncture could improve the outcomes of injuries in professional sport. Mr Wilson said: “In professional football we deal, on a day- to- day basis, with what are com-monly known as ‘the big four’, because they carry quite a high burden of injury. They are hamstring, ankle, knee and groin injuries. But what is less well known is the prevalence of low back pain, which is what I spend the majority of my time dealing with. Players come to the clinic and have a lot of mobilization and manual therapy on their lumbar spines. It’s generally
self- limiting, but I’ve had two players over the last nine years whose careers have ended due to low back pain.”
Mr Wilson, who has worked in professional sport for 17 years, said the high incidence of low back pain was down to the extreme physi-cal demands of the sport. He explained that professional footballers usually played in at least 60 games and 160 training sessions over a 10- month season. In addition, while sprinting, play-ers can reach top speeds of 32.8 km per hour and often cover in excess of 10 km per game. “Because of these demands we incorporate as many strategies as we can to keep the guys on the pitch.”
He also told delegates that low back pain often presented a “conundrum” because there was a lack of consensus about how to provide the best care. This had led to what he described as a “management vacuum”. However, he said several research groups have suggested that longstanding low back pain can be generated and maintained at the local tissues (the site of pain), as well as in the corresponding spinal segment and at a cortical level. As a result, he regularly offers acupuncture to athletes who complain of low back pain, as research has conclusively shown it can inhibit the sensation of pain locally, segmentally and cortically.
Mr Wilson said he advocated integrating acupuncture into a multimodal sports medicine approach and provided details of a case study of how this had worked with a young profes-sional footballer. The player had complained of an intermittent dull ache at rest. This rose to a high pain level (8 out of 10) whenever he ran or engaged in extension- based exercises in the gym. He also experienced stiffness, discomfort in sustained postures and could only maintain a neutral pelvic tilt in any position. Adding to this, he had high anxiety levels as the pain was preventing him from playing or training at full intensity. He feared he might lose his place on the team. No red flags were identified and nothing remarkable was found on examination. In addition, an MRI scan showed no structural abnormalities. ‘So we hypothesized that it must be neurophysiological and tested him using Peter O’Sullivan’s movement and functional

Conference 2018
© 2018 Acupuncture Association of Chartered Physiotherapists 13
impairment system for assessing low back pain,” Mr Wilson said. “We did a lot of education with him, which was important, and his anxiety settled down. We talked about pain and tissue damage and possible neurophysiological drivers, which he thought were plausible. After that, he was keen to try acupuncture, which he’d never had before.”
A multimodal approach was implemented, which included eight 20- min sessions of acu-puncture and the outcomes were “very good . . . The sports medicine department was happy to advocate acupuncture as part of his programme because it kept him in training and helped to increase his levels of participation in terms of intensity of running and gym training,” said Mr Wilson. “He also did other things as well, such as practising mindfulness. But post- acupuncture, he told us something had changed for him. He felt looser and we could all see a difference in him.”
Delegates heard that it was common for athletes to report reduced pain levels, improved lumbar range and improved function on poste-rior chain strength tests after acupuncture. Mr Wilson uses it in conjunction with an extensive running, strength, power, neuromuscular con-trol and lumbo- pelvic- hip complex stability and education programme. “I also offer it as an option to players to help modulate pain levels, help them carry out their rehab and return to training and competing in a timely and safe manner.”
Robert Millett
Acupressure for neurological conditionsJohn R. CrossAcupressure is not a diluted version of acu-puncture, as some people mistakenly believe, and has the advantage of providing non- invasive treatment. This was one of the messages from Chartered Society of Physiotherapists Fellow John Cross. Mr Cross, a retired physiotherapist who has used acupressure for almost 40 years, was the first chartered physiotherapist to become a registered acupuncturist.
During his presentation, which focused on the use of clinical acupressure for neurological conditions, Mr Cross said: “Why do we use acupressure? Because it’s non- invasive, which is great for patients and also, sometimes, for practitioners – because not all of us like nee-dles. Also, I found that acupressure allows you to have a greater rapport and oneness with your client, because you receive constant feed-back and confirmation about how treatment is progressing. Patients tend to relax more easily and it allows you to teach self- help procedures, which you can show them after a session and which they can use between treatments.”
Mr Cross said there were many types of acu-pressure, and shared his theory that acupressure and reflexology are synonymous, citing examples of their similarity. “Every acupressure- point on the body is a reflex of something. A reflex is a reflected point or pathway, and every reflex point can be touched, massaged or needled. And there is a misconception that reflexology is just concerned with the feet and hands. Reflex points and areas are all over the body, not just on the feet and hands.”
He described how therapists could use acupressure and reflexology to ease symptoms associated with neurological conditions, includ-ing stress, thermal imbalance, flaccidity, spasms, fatigue, incoordination and pain.
With the aid of pictures, he showed delegates relevant acupressure points and described their therapeutic uses. Mr Cross also highlighted how the spine, brain, cranial nerves and autonomic nervous system are thought, by some cultures and branches of traditional medicine, to be ‘reflected’ on other regions of the body.
Robert Millett
Temporomandibular disordersDr Thomas PerreaultDr Thomas Perreault, clinical specialist physical therapist from the US, presented “Dry Needling for Myofascial Temporomandibular Disorders: Case Study and Review of the Literature.”
Dr Perreault opened by defining tempo-romandibular disorder (TMD) as pathologies

Conference 2018
© 2018 Acupuncture Association of Chartered Physiotherapists14
of the temporomandibular joint, masticatory muscles, and related anatomical structures. Presenting a review of the current literature, he stated that myofascial TMD is prevalent in patients with orofacial pain and is strongly linked to central sensitization. He proposed that trigger point dry needling and acupuncture are widely accepted therapies used in the treatment of myofascial pain syndromes (MPS) which include myofascial TMD. He outlined several studies that showed that needling to trigger points of the temporalis, masseter, and lateral pterygoid can help to alleviate TMD pain and improve function.
Based on these opening statements, Dr Perreault went on to present a case study of a 13- year- old female with intermittent left- sided jaw and facial pain that had been ongoing for two months. The outcome of her case dem-onstrated the positive benefits of needling to trigger points within the masticatory muscles with subacute myofascial TMD. The needling techniques chosen included direct needling of the masseter and lateral pterygoid. Dr Perreault supported the outlined needling protocols with direct evidence from the literature that con-firmed the positive effects of accurate and direct needling into the involved masticatory muscles. Discussing other interventions for TMD, he proposed that needling was selected as the primary intervention as literature reviews now conclude the lateral pterygoids are inaccessible to intraoral palpation, thus rendering manual therapy to this muscle ineffective. Describing the specifics of needling technique, he discussed empirical evidence that suggests that eliciting a local twitch response (LTR) during needling is essential. He then, however, highlighted a recent review of more up- to- date studies showing that eliciting a LTR does not necessarily correlate with positive changes in pain and disability but is linked to increased pain and inflammation. He went on to state that restoration of normal mandibular movement, function, and rapid relief of pain was observed at the conclusion of treatment. Treatment consisted of four sessions using manual needle winding to trigger points without inducing a LTR, as this approach was well supported in the literature.
In summary, Dr Perreault’s presentation gave an insight into the clinical application of needl-ing for TMD supported by relevant published literature. With reference to an example case study, he discussed the practical application of needling regarding angle of insertion, depth of needling, safety aspects and the accurate and effective location of target structures. Overall, he drew together the integral aspects of evidence- based practice; namely the integra-tion of individual clinical expertise and experi-ence blended with the best available published evidence, whilst considering patient preference to obtain a positive outcome. His style of presentation was fluid, engaging and informa-tive throughout and raised several interesting clinically- related questions which he answered directly following his session.
Jonathan HobbsAACP Chairman
It’s all in the anatomy – the merging worlds of fascia and meridian theory Lynn PearceLynn Pearce has been working with her acu-puncture and physiotherapy skills and slowly moving towards a place of integration of the reality of anatomy which is our baseline as physiotherapists and the sometimes more eso-teric concepts of meridians. She freely admitted that this talk was still a work in progress as there are so many avenues to try and pull together, but hoped there might be some new ideas and ways of looking at the body as a whole.
Starting with the anatomy, Ms Pearce outlined where we are with the study of fascia and the development of new ideas on its functional and sensory role, making it more than just a mechani-cal tissue. The ‘new organ’ – the interstitium, as suggested by Neil Thiese – adds another dimension to fascial anatomy that deserves enquiry. Challenging where people actually place their needles, the idea was to think about how techniques within superficial fascia can seem to have a widespread effect by relating that back to the nature of fascia itself.

Conference 2018
© 2018 Acupuncture Association of Chartered Physiotherapists 15
Ms Pearce pointed to The Fascia Research Society – a group including Helene Langevin, Robert Schliep, Tom Myers, Siegfried Mense and many more – which is pushing the boundaries as to our understanding of the most interesting tissue of the day. Dan Keown, author of the book The Spark in the Machine, also outlines a fascinating view of the spaces within fascia as meridians and the concept that surgeons use these spaces to get round the body, not realising they may be using the meridian network.
Through works by Leonardo da Vinci, whose anatomical studies show us clearly the ‘valleys and grooves’ of the body/meridians, as explained in the Huangdi Neijing, Ms Pearce explored the placement of needles, and what you feel for as therapists, in longitudinal planes as opposed to transverse. She highlighted how Langevin’s work shows that tissue displacement along fascial planes is more effective if a needle is placed in a ‘groove’ – i.e. within the inter- muscular tissue as opposed to intra- muscular tis-sue. This may also account for the bidirectional report of sensation some people get when having acupuncture. The effect of stress on the sympathetic system is well known, and Ms Pearce drew attention to Mense’s work which shows a proportionally high number of free nerve endings within superficial fascia which are
responsive to changes in the autonomic nervous system (ANS). This could provide some expla-nation as to how emotional stress can cause an increase in nociceptive pain and far flung signs and symptoms.
Looking at the combined pictures of main meridians, musculoskeletal meridians, trigger points and their referral, or Tom Myers’ anat-omy trains, Ms Pearce showed that if we pick key acupuncture points based on anatomical intersections, those points will readily transpose from one system to another, occurring in the same place and yet having different effects dependent on the therapist’s belief systems. Regardless of those belief systems, the place-ment of an acupuncture needle will have far reaching effects, partly described by the role and structure of the fascial network that we needle into. Whether Qi, or current, or fluid, or all of them, flow through that target region, that is the mental struggle of definition that we face as scientific therapists who also play with energy in its raw form. We all like to have an answer, but sometimes there isn’t just the one answer, and merging worlds just explain things in different ways.
Robert Millett


© 2018 Acupuncture Association of Chartered Physiotherapists 17
Correspondence: Thomas Perreault, Physical Therapy Department, Wentworth- Douglass Hospital, 789 Central Avenue, Dover, New Hampshire 03820, USA (email: [email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 17–26
lITErATurE rEvIEw
Mechanisms and dose parameters of electric needle stimulation: clinical considerations – Part I
T. PerreaultNorthern New England Spine Center, Department of Physical Therapy, Wentworth- Douglass Hospital, Dover, New Hampshire, USA
S. O. FlannaganFounder One Accord Physical Therapy, Phoenix, Arizona, USA
M. T. GrubbThe University of Tennessee, Chattanooga, Tennessee, USA
r. GrubbThe University of Tennessee, Chattanooga, Tennessee, USA
AbstractRecent studies support that electric needle stimulation (ENS) provides superior analgesic effects compared to manual needle stimulation alone, making it preferable for the clinical management of chronic pain. An electronic database search was performed with the aim of completing a narrative review of the literature to explore the neuronal mechanisms trig-gered by ENS from a clinical standpoint. The majority of studies on ENS mechanisms support the use of strong, noxious needle stimuli for greater pain inhibition at the spinal and supraspinal levels. Multiple studies support that noxious ENS enhances spinal serotonin (5- HT) and noradrenaline (NA) levels by activating supraspinal neurons that project down to the level of the spine, and that both NA and 5- HT have an overall effect of creating anti- nociception. Further, arginine vasopressin (AVP) is released due to noxious ENS leading to amplified effects of the descending pain inhibitory systems. Various studies supported the use of lower frequency ENS for inducing a potent anti- nociceptive effect in the periphery by enhancing anandamide levels, increasing the availability of its target receptor, and up- regulating the endogenous opioid system in the periphery. Additionally, longer durations of electric stimulation (between 15 to 30 min) resulted in longer lasting analgesic effects and increased pressure pain thresholds in human subjects. A multitude of analgesic mechanisms are triggered with electric needle stimulation; however intensity of stimulation, needle place-ment within the segmental distribution of pain and duration of ENS seem to be the most important dose parameters for greater anti- nociceptive effects.
Keywords: acupuncture, analgesia, needle, pain, stimulation.
IntroductionDry needling and acupuncture are routinely administered treatments for the management of chronic pain conditions (Zhou et al. 2015).

Mechanisms and dose parameters of electric needle stimulation – Part I
© 2018 Acupuncture Association of Chartered Physiotherapists18
Both procedures use needle stimulation to trigger endogenous mechanisms that are advantageous for altering sensory perception (Baeumler et al. 2014) and decreasing pain in neuromusculoskeletal (NMSK) disorders (Yuan et al. 2016). According to a recent review, the analgesic effects following a course of needling treatments in patients with chronic pain have been reported to last for up to a 1- year period (MacPherson et al. 2017). Fundamentally, manual stimulation occurs when needles are inserted into the body and positioned to the desired depth; however, manipulation of the indwelling needle is required for the activation of local (Yin et al. 2018), spinal (Kagitani et al. 2010, Huang et al. 2018) and supraspinal (Niddam et al. 2007) analgesic effects. It is currently unknown what an optimal needling dosage is for any musculoskeletal condition, however, strength of needle manipulation (Choi et al. 2013), increas-ing the number of needles used (MacPherson et al. 2013) and administering repeated needling sessions (Vickers et al. 2018) are dosage param-eters that have been shown to enhance clinical outcomes. Clinically, electrical stimulation of needles is added to enhance or even replace the therapeutic effects of manual needling due to the elicitation of unique biological effects (Langevin et al. 2015). Recent studies support that electric needle stimulation (ENS) provides a greater analgesic effect making it preferable to manual stimulation alone (Manheimer et al. 2010; Baeumler et al. 2015), and that repeated application of strong ENS can be safely used with other therapies for both reducing pain and opioid medication usage (Zheng et al. 2018). The aim of this narrative review is to explore the neuronal mechanisms triggered by ENS from a clinical perspective. More specifically, this review will summarize relevant literature focusing on dosage and stimulation parameters of ENS that best contribute to analgesic effects in patients with painful NMSK conditions.
Materials and methodsLiterature researchLiterature for this narrative review was sought that investigated mechanisms and/or dosage
parameters of electric needle stimulation for anti- nociception. With the intent of perform-ing a narrative review, included articles were not limited to randomized controlled trials, systematic reviews or meta- analyses, nor were they limited to studies only on human subjects. An electronic database search of PubMed, MEDLINE, Science Direct and Google Scholar was performed using the following terms: dry needling, acupuncture, electroacupuncture, electric AND needle stimulation, dry needling AND segmental, acupuncture AND segmental, acupuncture AND analgesia. No restrictions were placed on date of article publication and only articles written in English were reviewed. Additionally, the reference lists of included studies were also hand searched to identify any articles relevant to the selected topic. Irrelevant articles were discarded.
Discussion ENS effects are intensity dependentThe neural pain inhibitory mechanism that is activated via ENS is dependent on the intensity of stimulation. Whether the intensity parameter is noxious or non- noxious will govern which afferent fibres are stimulated and also if local, spinal segmental, or more systemic analgesic effects are triggered. According to Xin et al. (2016), segmental analgesia is triggered by applying ENS of low intensity (i.e. below pain threshold) to a local point on the side of pain. Applied at higher intensities (i.e. at or above the noxious level), ENS was shown to increase thermal and mechanical pain thresholds within and beyond the segmental distribution of needle stimulation on the ipsilateral and con-tralateral sides, respectively (Xin et al. 2016). In an earlier study on human subjects, depression of the nociceptive reflex and pain sensation was achieved using ENS applied at and beyond pain thresholds, reaching depression levels of 58.8% and 60.7% respectively (Xu et al. 2003). Taken together these studies support the use of strong, noxious needle stimuli for greater segmental pain inhibition. However, according to both studies, ENS had no effect on pain or reflex inhibition when low intensity ENS was applied

T. Perreault et al.
© 2018 Acupuncture Association of Chartered Physiotherapists 19
to a contralateral acupoint within the same segmental level. Zhu et al. (2004) reported that at the segmental level, analgesia was enhanced in an intensity- dependent manner with ENS and strongest when applied to homo- segmental locations. More specifically, as the strength of needle stimulation increased, thereby reaching and surpassing activation range of Aδ and/or C- fibres, it resulted in greater and longer last-ing depression of the C- fibre reflex response. In addition, contralateral stimulation to the same acupoint also produced potent inhibi-tory effects in an intensity dependent manner. However, only noxious contralateral stimulation to the same point was effective in inducing segmental effect; while innocuous stimuli was ineffective (Zhu et al. 2004). Additionally, strong stimulus to a remote heterotopic acupoint (i.e. remote to the side of pain) in the forelimb was shown to produce trans- segmental anal-gesia through involvement of diffuse noxious inhibitory controls (DNIC) and induced a clear depression of the C- fibre reflex response on the ipsilateral hind limb. It is known that Aβ afferent fibres, which mediate light touch, are preferentially stimulated with innocuous ENS (Kagitani et al. 2010), resulting in the activa-tion of GABAergic inhibitory interneurons in the superficial laminae of the dorsal horn that inhibit Aδ and C- fibre input, which leads to pain relief within the stimulated segment (Baeumler et al. 2015). Noxious stimulation also triggers a release of endogenous opioids and inhibitory neurotransmitters (GABA and glycine) in the spinal cord (SC). Several studies show ENS induces a release of spinal endogenous opioids (Zhao 2008), up- regulates the release of GABA (Qiao et al. 2017), and potentially leads to a release of glycine in the SC (Zhou et al. 2008; Butts et al. 2016). Accordingly, this contributes to spinal segmental inhibition and suppression of glutamate activity in post- synaptic dorsal horn neurons. It is proposed that inhibition will also occur in ascending spinal neurons that project to the basal forebrain, leading to activa-tion (i.e. dis- inhibition) of a spino- supraspinal opioid- dependent mechanism in the nucleus accumbens (Tambeli et al. 2002; Tambeli et al. 2003). That is, endogenous neuromodulators
released by noxious ENS suppress ascending nociceptive activity, triggering a potent supra-spinal mechanism that induces trans- segmental or global pain inhibition.
ENS induces segmental inhibitionPain inhibition occurs in a pattern relative to the spinal segmental distribution of the patient’s symptoms when needles are inserted (and elec-trically stimulated) within that same distribution (i.e. segmental inhibition). Using non- painful electrical stimuli, Baeumler et al. (2015) con-cluded that short term increases in pain pressure threshold (PPT) were confined to a sensory region of the L4- L5 segment in close proximity to the needling sites. This was noted on both the treated limb and contralateral lower leg. In comparison to manual acupuncture, electrical stimulation provided a more robust improve-ment in PPT, however, no changes in pressure sensitivity were observed heterosegmentally when measured at the C6 segment with either modality (Baeumler et al. 2015). Similarly, Lang et al. (2010) reported using non- noxious electric stimuli to four needles in the anterior lower leg and found a bilateral increase in PPT over the sensory region of the peroneal nerve within the L4 segment. Manual needle stimulation was similar in effect for providing bilateral increases in PPT with unilateral stimulation (Lang et al. 2010). Collectively, the above studies support the concept of a segmental needling approach that can be complemented with ENS. A limitation in the above studies is that they were performed on healthy volunteers and not on patients with pain. However, a recent meta- analysis of 85 studies reported significant short- term and long- term effects of acupuncture on PPT in patients with painful musculoskeletal disorders. Additionally, it was concluded that ipsilateral needling close to the measurement sites elicited the strongest effects on sensory thresholds than remote or contralateral needling (Baeumler et al. 2014). This supports the concept that seg-mental inhibition is dependent on stimulation of primary afferents that carry noxious and non- noxious input to the spinal level, thereby assisting with analgesia in the same segment of the needle stimulus. Thus, there do appear to be

Mechanisms and dose parameters of electric needle stimulation – Part I
© 2018 Acupuncture Association of Chartered Physiotherapists20
compelling clinical precedents for using a spinal segmental approach to needling for painful musculoskeletal disorders.
ENS local analgesic effectsENS can help to relieve inflammatory pain via down- regulation of nociceptive ion channels. Manual needle manipulation has been shown to mechanically activate pain channels that induce anti- nociceptive effects (Wu et al. 2014). The aim with ENS, however, is to reduce influx of cation currents to sensory receptors to inhibit pain related action potentials. More specifically, ENS has been shown to target and suppress transient receptor potential vanilloid- 1 (TRPV1), a channel that is involved in detection of mechanical, thermal, and acid- induced pain in the periphery, dorsal root ganglion (DRG), and SC level (Yang et al. 2017). TRPV1 activation occurs under inflammatory conditions, leading to both increased nociceptive action potentials and enhanced expression of the TRPV1 recep-tor in neurons of the DRG and spinal dorsal horn. A novel study reported that low frequency ENS to a point segmentally related to the area of pain induction decreased inflammatory pain in an animal model by reducing the expression of TRPV1 and TRPV4 receptors in ipsilateral DRG neurons projecting to the L3- L5 seg-ments (Chen et al. 2012). Additionally, non- local ENS applied contralaterally but within the spinal segment of inflammatory- induced pain can similarly decrease TRPV1 expression and decrease sodium current influx at the DRG and SC dorsal horn neurons respectively (Lu et al. 2016). A recent study reported that strong low frequency ENS triggers release of adenosine to activate A1 receptors (A1R) and opioids to act on the μ- receptors, resulting in suppression of nociceptive ion channels in DRG neurons. More specifically, A1R activation may lead to decreased adenylyl cyclase activity and inhibi-tion of protein kinase A (PKA), resulting in receptor down- regulation by limiting receptor phosphorylation (Chen et al. 2011; Liao et al. 2017). Taken together, these studies suggest that low frequency ENS can treat inflammatory pain detected by primary afferents by reduc-ing synaptic transmission in DRG neurons
and the dorsal horn of the SC to alter pain sensation.
ENS reduces inflammatory painENS has been shown to reduce pain from inflamed tissue through activating the endo-cannabinoid and endogenous opioid systems. Anandamide is an endogenous cannabinoid that activates two receptor types (CB1 and CB2) that inhibit nociceptive input to the SC dorsal horn. CB1 receptors are localized on primary afferent neurons, within the spinal dorsal horn, and the Central Nervous System (CNS). CB2 receptors are located primarily on immune cells to include mast cells, macrophages, keratinocytes, and T- lymphocytes. Application of low or high fre-quency ENS can elevate anandamide levels in the periphery by promoting its synthesis and release from epidermal keratinocytes. Importantly, the anti- nociceptive effects of ENS are correlated with the subsequent increase in peripheral anan-damide levels that rely on activation of local CB2 receptors (Chen et al. 2009). Additionally, ENS of high or low frequency can up- regulate the expression of CB2 receptors on resident immune cells and leukocytes that are recruited to areas of inflamed tissue (Zhang et al. 2010). By activating CB2 receptors, anandamide can stimulate opioid- containing leukocytes to release β- endorphin and contribute to analgesia by binding to peripheral opioid receptors (Su et al. 2011). Additionally, contralateral ENS applied pre- treatment away from the site of pain was effective at reducing inflammatory pain and involves specific μ- opioid receptor activation at the spinal level (Yang et al. 2011). Taken together, these studies show that ENS induces a potent anti- nociceptive effect in the periphery by enhancing anandamide levels, increasing the availability of its target receptor, and up- regulating the endogenous opioid system in the periphery.
At the spinal level, cannabinoids have an inhibitory effect on primary afferents and at the substantia gelatinosa of the dorsal horn by decreasing glutamate release from primary afferent terminals through CB1 receptor activa-tion. Several studies show that low concentra-tions of anandamide are sufficient to activate

T. Perreault et al.
© 2018 Acupuncture Association of Chartered Physiotherapists 21
CB1 receptors, significantly reduce calcitonin gene- related peptide (CGRP) release in the spinal dorsal horn, and reduce neuronal excit-ability (Morisset et al. 2001). This modulation of neuropeptide release in the dorsal horn likely occurs through a reduction in adenylyl cyclase. In contrast, high concentrations of anandamide will elicit excitatory nociceptive input to dorsal horn neurons by activating the TRPV1 receptor that enhances the release of substance P (SP) and CGRP (Ahluwalia et al. 2003a; Ahluwalia et al. 2003b). Thus, anandamide has a regulatory effect on neurotransmitter release at the spinal level and the subsequent effect is concentration dependent (Tognetto et al. 2001).
ENS duration parametersENS activates all afferent nerve fibre groups according to nerve conduction velocity measures in animal models (Kagitani et al. 2010). ENS has an initial pain modulatory effect through either noxious Aδ or innocuous Aβ fibre stimulation that results in segmental inhibition. A supraspi-nal mechanism may also be triggered with longer time durations of ENS, shifting away from pain inhibition that is spinally mediated to a form of descending pain inhibition that is much more potent and global in effect. In a study by Leung et al. (2008), bilateral increases in sensory thresholds were confined to the L4 dermatome of the lower leg and correlated to the areas of unilateral needle insertion that received brief electrical stimulation. However, a longer duration of electric stimulation (between 15 to 30 min) resulted in longer lasting analgesic effects and increased pressure pain thresholds that extended beyond just the segmental levels of the needling sites (Leung et al. 2008). In contrast, even a short stimulation time of 5 min with ENS is sufficient to deliver strong and fast onset analgesia compared to manual needling but the effect is limited to only a few minutes duration (Schliessbach et al. 2011).
ENS and descending pain inhibitionENS triggers descending pain inhibition by activating neurons in the rostral- ventral region of the medulla and the locus coeruleus of the pons. These regions contain supraspinal
nuclei that extend fibres down the dorsolateral funiculus (DLF), delivering serotonin (5- HT) and NA to superficial laminae of the SC dorsal horn to inhibit pain when activated. Li et al. (2007) reported that creating a spinal lesion on the DLF in an inflammatory pain model eradicates the pain inhibition ENS created by eliminating the delivery of 5- HT and NA at the spinal level (Li et al. 2007). The authors also reported low ENS intensity was sufficient to increase ipsilateral (but not contralateral) pain thresholds, indicating that the SC on the side of pain is hyper- responsive to the needle stimulus compared to the contralateral uninvolved side at the same level. Zhang et al. (2012) concluded that ENS alleviates pain in part through 5- HT1A receptors on post- synaptic dorsal horn neurons resulting in modulation of the NMDA receptor. Additionally, the authors provided supporting evidence that ENS enhances spinal serotonin levels by activating supraspinal serotonin- containing neurons that project to the level of the spine. Furthermore, ENS increased spinal release of norepinephrine by activating noradrenergic- spinal projection neurons in the locus coeruleus. NA preferentially activates the alpha- adrenergic receptors (α2A) on primary afferent nerve fibres (Aδ fibres specifically), leading to pre- synaptic reduction of glutamate release to the SC (Zhang et al. 2012). Both NA and 5- HT have an overall effect of anti- nociception. Both also produce membrane hyperpolarization in neurons of the substantia gelatinosa of the dorsal horn, decrease excita-tory neurotransmitter (glutamate) release from primary Aδ and C- fibres pre- synaptically, and increase inhibitory neurotransmitter release (GABA and glycine) from interneurons (Yoshimura & Furue 2006).
Importantly, noradrenergic descending inhibi-tory system activation can enhance the opioid effects at the SC level during periods of inflam-mation. When the opioid effect is not strong enough to induce anti- nociception, the effects are enhanced by spinal adrenergic mechanisms. Thus, painful stimulation applied ipsilater-ally can stimulate the noradrenergic system (or even serotonergic system) to provide this effect. One study reported that ENS applied at
Mechanisms and dose parameters of electric needle stimulation – Part I
© 2018 Acupuncture Association of Chartered Physiotherapists22
noxious levels stimulated α2A receptor activa-tion via spinal NA, promoting analgesic effect in the SC. This may perhaps be more power-ful than the opioid effect, as α2A receptor anatagonists abolished ENS effects whereas opioid receptor antagonists did not (Koo et al. 2008). Mechanistically, α2A receptor activa-tion increases K+ conductance in dorsal horn neurons, causing hyperpolarization, decreased neuron excitability, and decreased glutamate release in the dorsal horn leading to analgesia. This is mainly brought about through Aδ- fibre stimulation that leads to adrenergic system acti-vation. Furthermore, the analgesic actions of opioid receptors are enhanced under inflamma-tory conditions and thereby more potent on the affected side of inflammation (Stein & Kuchler 2013), thus demonstrating why α2A receptor agonists exhibit enhanced effects at the level of the SC during inflammation.
ENS has also been shown to restore descending pain inhibitory system function in chronic pain situations. Low frequency and moderate intensity (2 Hz and 1 mA) ENS has also been shown to enhance CB1 receptor levels on GABAergic neurons in the midbrain periaqueductal gray (PAG). Activation of the CB1 receptor will inhibit GABA release from PAG neurons, disinhibit serotonin release from neurons in the PAG and Rostral Ventromedial Medulla (RVM) and promote restoration of and improved function to diffuse noxious inhibi-tory controls (DNIC) and the descending pain inhibitory systems by reversal of the reduced CB1 receptor expression in situations of chronic pain. (Yuan et al. 2018).
ENS induces supraspinal analgesic effectsAt the level of the brain, there are potent mechanisms triggered with ENS that originate and act centrally and then transport spinally to inhibit pain. Noxious electric needle stimulation has been shown to trigger the release of argi-nine vasopressin (AVP) from the hypothalamic paraventricular nucleus (PVN) and promote its transport via nerve fibres and ventricles in the brain to the PAG, nucleus raphe magnus (NRM) of the medulla, and caudate nucleus in the basal
ganglia (Deng et al. 2015). AVP is synthesized in selected neurons of the hypothalamus, mainly in the PVN and supraoptic nucleus (SON). Painful stimulation has been shown to increase noradrenaline (NA) that interacts with PVN neurons to promote synthesis and secretion of AVP that can assist in pain modulation (Zhou et al. 2010). AVP also enhances descending pain inhibition by stimulating the synthesis and secretion of the endogenous opioids enkephalin and β- endorphin in the PAG (Yang et al. 2007b), stimulating the serotonergic system in the NRM (Yang et al. 2009) that leads to 5- HT release in the dorsal horn, and the subsequent spinal release of endogenous opioids via activation of serotonin receptors (Pan et al. 2012). Thus, ENS of noxious intensity can trigger release of AVP and has a potent effect on analgesia at the spi-nal level leading to increased pain thresholds. In the treatment of primary sciatica, a positive cor-relation between pain relief and levels of AVP in the cerebrospinal fluid (CSF) was observed after a session of bilateral ENS to segmentally- related acupuncture points. More specifically, 60 min of low frequency and low intensity ENS induced larger increases in AVP levels than a 30- min duration (Zhao et al. 2015). AVP levels in the CSF increased dose- dependently when treatment duration was the dosage parameter.
A recent review supports that needling inhib-its pain via supraspinal increase of oxytocin lev-els, resulting in transport to oxytocin receptors on spinal neurons, interneurons, and primary afferents at the dorsal horn (Butts et al. 2016). Several studies suggest oxytocin acts to inhibit inflammatory pain by modulating acid sensing ion channel (ASIC) function through activation of vasopressin receptors and up- regulation of calcineurin to decrease current amplitudes on sensory receptors (Yang et al. 2007a; Qiu et al. 2014). ENS has been shown to promote release of oxytocin from the SON of the hypo-thalamus and facilitate the transfer of oxytocin to the PAG, NRM, and spinal cord, thereby resulting in analgesia through its influence on endogenous opioid release in neurons of the DRG. Interestingly, AVP was able to induce the same ASIC regulation and analgesic effect as oxytocin by activating the same V1a receptor
T. Perreault et al.
© 2018 Acupuncture Association of Chartered Physiotherapists 23
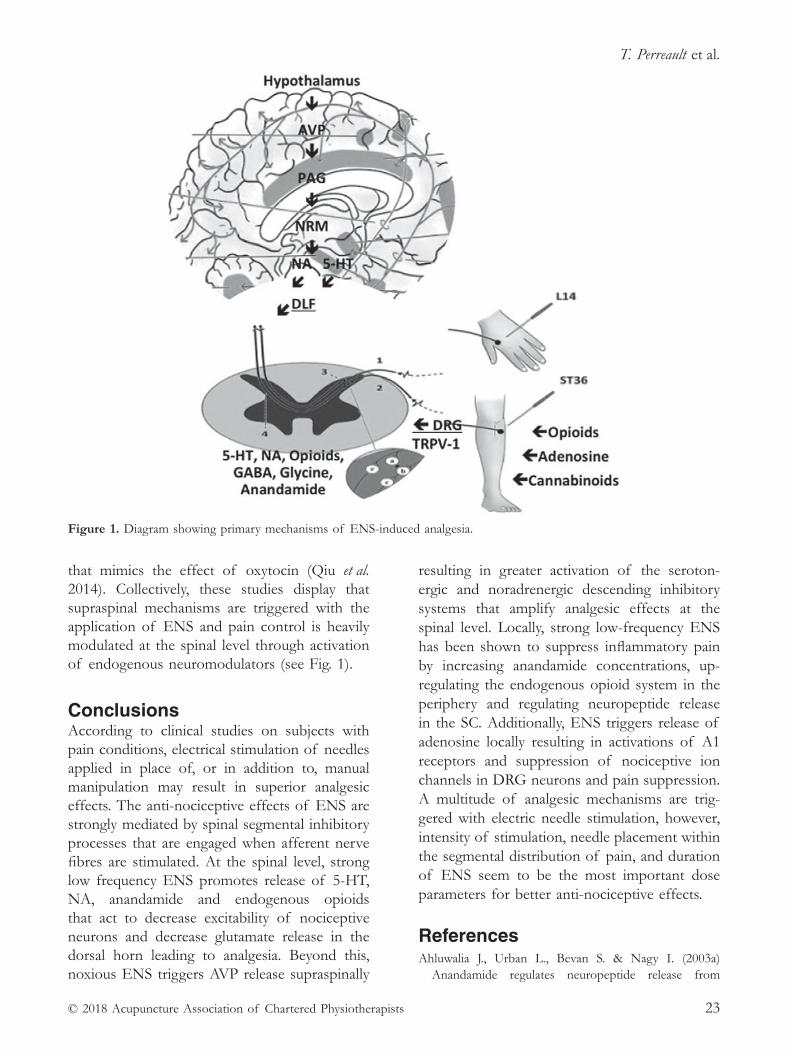
that mimics the effect of oxytocin (Qiu et al. 2014). Collectively, these studies display that supraspinal mechanisms are triggered with the application of ENS and pain control is heavily modulated at the spinal level through activation of endogenous neuromodulators (see Fig. 1).
Conclusions According to clinical studies on subjects with pain conditions, electrical stimulation of needles applied in place of, or in addition to, manual manipulation may result in superior analgesic effects. The anti- nociceptive effects of ENS are strongly mediated by spinal segmental inhibitory processes that are engaged when afferent nerve fibres are stimulated. At the spinal level, strong low frequency ENS promotes release of 5- HT, NA, anandamide and endogenous opioids that act to decrease excitability of nociceptive neurons and decrease glutamate release in the dorsal horn leading to analgesia. Beyond this, noxious ENS triggers AVP release supraspinally
resulting in greater activation of the seroton-ergic and noradrenergic descending inhibitory systems that amplify analgesic effects at the spinal level. Locally, strong low- frequency ENS has been shown to suppress inflammatory pain by increasing anandamide concentrations, up- regulating the endogenous opioid system in the periphery and regulating neuropeptide release in the SC. Additionally, ENS triggers release of adenosine locally resulting in activations of A1 receptors and suppression of nociceptive ion channels in DRG neurons and pain suppression. A multitude of analgesic mechanisms are trig-gered with electric needle stimulation, however, intensity of stimulation, needle placement within the segmental distribution of pain, and duration of ENS seem to be the most important dose parameters for better anti- nociceptive effects.
referencesAhluwalia J., Urban L., Bevan S. & Nagy I. (2003a)
Anandamide regulates neuropeptide release from
Figure 1. Diagram showing primary mechanisms of ENS- induced analgesia.
Mechanisms and dose parameters of electric needle stimulation – Part I
© 2018 Acupuncture Association of Chartered Physiotherapists24
capsaicin- sensitive primary sensory neurons by activat-ing both the cannabinoid 1 receptor and the vanilloid receptor 1 in vitro. European Journal of Neuroscience, 17 (12), 2611–8.
Ahluwalia J., Yaqoob M., Urban L., et al. (2003b) Activation of capsaicin- sensitive primary sensory neurones induces anandamide production and release. Journal of Neurochemistry 84 (3), 585–91.
Baeumler P. I., Fleckenstein J., Benedikt F., et al. (2015) Acupuncture- induced changes of pressure pain thresh-old are mediated by segmental inhibition – a random-ized controlled trial. Pain 156 (11), 2245–55.
Baeumler P. I., Fleckenstein J., Takayama S., et al. (2014) Effects of acupuncture on sensory perception: a systematic review and meta- analysis. PLoS One 9 (12): e113731.
Butts R., Dunning J., Perreault T., et al. (2016) Peripheral and spinal mechanisms of pain and dry needling medi-ated analgesia: a clinical resource guide for health care professionals. International Journal of Physical Medicine & Rehabilitation 4 (327).
Chen L., Zhang J., Li F., et al. (2009) Endogenous anandamide and cannabinoid receptor- 2 contribute to electroacupuncture analgesia in rats. Journal of Pain 10 (7), 732–9.
Chen W. H., Tzen J. T., Hsieh C. L., et al. (2012) Attenuation of TRPV1 and TRPV4 expression and function in mouse inflammatory pain models using electroacupuncture. Evidence- Based Complementary Alternative Medicine 2012: 636848.
Chen Y., Yang C. & Wang Z. J. (2011) Proteinase- activated receptor 2 sensitizes transient receptor potential vanil-loid 1, transient receptor potential vanilloid 4, and tran-sient receptor potential ankyrin 1 in paclitaxel- induced neuropathic pain. Neuroscience 193, 440–51.
Choi Y. J., Lee J. E., Moon W. K. & Cho S. H. (2013) Does the effect of acupuncture depend on needling sensation and manipulation? Complementary Therapies in Medicine 21 (3), 207–14.
Deng X.- H., Wang Y.- L., Yuan Y., et al. (2015) The roles of vasopressin in acupuncture analgesia. Journal of Pharmaceutical Medicine 3, 11–16.
Huang M., Wang X., Xing B., et al. (2018) Critical roles of TRPV2 channels, histamine H1 and adenosine A1 receptors in the initiation of acupoint signals for acupuncture analgesia. Scientific Reports 8: 6523.
Kagitani F., Uchida S. & Hotta H. (2010) Afferent nerve fibers and acupuncture. Autonomic Neuroscience 157 (1–2), 2–8.
Koo S. T., Lim K. S. Chung K., et al. (2008) Electroacupuncture- induced analgesia in a rat model of ankle sprain pain is mediated by spinal α- adrenoceptors. Pain 135 (1–2), 11–19.
Lang P. M., Stoer J., Schober G. M., et al. (2010) Bilateral acupuncture analgesia observed by quantitative sensory testing in healthy volunteers. Anesthesia and Analgesia 110 (5), 1448–56.
Langevin H. M., Schnyer R., MacPherson H., et al. (2015) Manual and electrical needle stimulation in acupunc-ture research: pitfalls and challenges of heterogeneity. Journal of Alternative and Complementary Medicine 21 (3), 113–28.
Leung A. Y., Kim S. J., Schulteis G. & Yaksh T. (2008) The effect of acupuncture duration on analgesia and peripheral sensory thresholds. BMC Complementary and Alternative Medicine 8 (18).
Li A., Wang Y., Xin J., et al. (2007) Electroacupuncture suppresses hyperalgesia and spinal Fos expression by activating the descending inhibitory system. Brain Research 1186, 171–9.
Liao H. Y., Hsieh C. L., Huang C. P. & Lin Y. W. (2017) Electroacupuncture attenuates CFA- induced inflam-matory pain by suppressing Nav1.8 through S100B, TRPV1, opioid, and adenosine pathways in mice. Scientific Reports 7: 42531.
Lu K. W., Hsu C. K., Hsieh C. L., et al. (2016) Probing the effects and mechanisms of electroacupuncture at ipsi-lateral or contralateral ST 36- ST 37 acupoints on CFA- induced inflammatory pain. Scientific Reports 6: 22123.
MacPherson H., Maschino A. C., Lewith G., et al. (2013). Characteristics of acupuncture treatment associated with outcome: an individual patient meta- analysis of 17,922 patients with chronic pain in randomised con-trolled trials. PLoS One 8 (10): e77438.
MacPherson H., Vertosick E. A., Foster N. E., et al. (2017) The persistence of the effects of acupuncture after a course of treatment: a meta- analysis of patients with chronic pain. Pain 158 (5), 784–793.
Manheimer, E., Cheng, K., Linde, K., et al. (2010) Acupuncture for peripheral joint osteoarthritis. Cochrane Database of Systematic Reviews CD001977.
Morisset V., Ahluwalia J., Nagy I. & Urban L. (2001) Possible mechanisms of cannabinoid- induced antinociception in the spinal cord. European Journal of Pharmacology 429 (1–3), 93–100.
Niddam D. M., Chan R. C., Lee S. H., et al. (2007). Central modulation of pain evoked from myofascial trigger point. Clinical Journal of Pain, 23 (5), 440–8.
Pan Y.- J., Yin Z.- K., Yang J., et al. (2012) Serotonin influ-ences the endogenous opiate peptides in the rat spinal cord to participates in pain modulation. Open Journal of Anesthesiology 2 (2), 29–35.
Qiao L. N., Liu J. L., Tan L. H., et al. (2017) Effect of electroacupuncture on thermal pain threshold and expression of calcitonin- gene related peptide, sub-stance P and gamma- aminobutyric acid in the cervical dorsal root ganglion of rats with incisional neck pain. Acupuncture in Medicine 35 (4), 276–283.
Qiu F., Qiu C. Y., Cai H., et al. (2014) Oxytocin inhibits the activity of acid- sensing ion channels through the vasopressin, V1A receptor in primary sensory neurons. British Journal of Pharmacology 171 (12), 3065–76.
Schliessbach J., van der Klift E., Arendt- Nielsen L., et al. (2011) The effect of brief electrical and manual
T. Perreault et al.
© 2018 Acupuncture Association of Chartered Physiotherapists 25
acupuncture stimulation on mechanical experimental pain. Pain Medicine 12 (2), 268–75.
Stein C. & Küchler S. (2013) Targeting inflammation and wound healing by opioids. Trends in Pharmacological Sciences 34 (6), 303–12.
Su T. F., Zhang L. H., Peng M., et al. (2011) Cannabinoid CB2 receptors contribute to upregulation of β- endorphin in inflamed skin tissues by electro-acupuncture. Molecular Pain 7: 98.
Tambeli C. H., Parada C. A., Levine J. D. & Gear R. W. (2002) Inhibition of tonic spinal glutamatergic activity induces antinociception in the rat. European Journal of Neuroscience 16 (8), 1547–53.
Tambeli C. H., Quang P., Levine J. D. & Gear R. W. (2003) Contribution of spinal inhibitory receptors in heterosegmental antinociception induced by noxious stimulation. European Journal of Neuroscience 18 (11), 2999–3006.
Tognetto M., Amadesi S., Harrison S., et al. (2001) Anandamide excites central terminals of dorsal root ganglion neurons via vanilloid receptor- 1 activation. Journal of Neuroscience 21 (4), 1104–9.
Vickers A. J., Vertosick E. A., Lewith G., et al. (2018) Acu- puncture for chronic pain: update of an individual patient data meta- analysis. Journal of Pain 19 (5), 455–474.
Wu S. Y., Chen W. H., Hsieh C. L. & Lin Y. W. (2014) Abundant expression and functional participation of TRPV1 at Zusanli acupoint (ST 36) in mice: mecha-nosensitive TRPV1 as an “acupuncture- responding channel”. BMC Complementary and Alternative Medicine 14 (96).
Xin J., Su Y., Yang Z., et al. (2016) Distinct roles of ASIC3 and TRPV1 receptors in electroacupuncture- induced segmental and systemic analgesia. Frontiers in Medicine 10 (4), 465–472.
Xu W. D., Zhu B., Rong P. J., et al. (2003) The pain- relieving effects induced by electroacupuncture with different intensities at homotopic and heterotopic acu-points in humans. American Journal of Chinese Medicine 31 (5), 791–802.
Yang E. J., Koo S. T., Kim Y. S., et al. (2011) Contralateral electroacupuncture pretreatment suppresses carrageenan- induced inflammatory pain via the opioid- mu receptor. Rheumatology International 31 (6), 725–30.
Yang J., Hsieh C. L. & Lin Y. W. (2017) Role of transient receptor potential vanilloid 1 in electroacupuncture analgesia on chronic inflammatory pain in mice. Biomed Research International 2017: 5068347.
Yang J., Yang Y., Chen J. M., et al. (2007a) Effect of oxy-tocin on acupuncture analgesia in the rat. Neuropeptides 41 (5), 285–92.
Yang J., Yang Y., Xu H. T., et al. (2007b) Arginine vasopressin induces periaqueductal gray release of enkephalin and endorphin relating to pain modulation in the rat. Regulatory Peptides 142 (1–2), 29–36.
Yang J., Yuan H., Chu J., et al. (2009) Arginine vasopres-sin antinociception in the rat nucleus raphe magnus is
involved in the endogenous opiate peptide and seroto-nin system. Peptides 30 (7), 1355–61.
Yin N., Yang H., Yao W., et al. (2018). Mast cells and nerve signal conduction in acupuncture. Evidence- Based Complementary and Alternative Medicine 2018: 3524279.
Yoshimura M. & Furue H. (2006) Mechanisms for the anti- nociceptive actions of the descending noradrener-gic and serotonergic systems in the spinal cord. Journal of Pharmacological Sciences 101 (2), 107–17.
Yuan Q. L., Wang P., Liu L., et al. (2016) Acupuncture for musculoskeletal pain: a meta- analysis and meta- regression of sham- controlled randomized clinical trials. Scientific Reports 6: 30675.
Yuan X. C., Zhu B., Jing X. H., et al. (2018) Electroacupuncture potentiates cannabinoid receptor- mediated descending inhibitory control in a mouse model of knee osteoarthritis. Frontiers in Molecular Neuroscience 11: 112.
Zhang J., Chen L., Su T., et al. (2010) Electroacupuncture increases CB2 receptor expression on keratinocytes and infiltrating inflammatory cells in inflamed skin tis-sues of rats. Journal of Pain 11 (12), 1250–8.
Zhang Y., Zhang R. X., Zhang M., et al. (2012) Electroacupuncture inhibition of hyperalgesia in an inflammatory pain rat model: involvement of distinct spinal serotonin and norepinephrine receptor subtypes. British Journal of Anaesthesia 109 (2), 245–52.
Zhao X. Y., Zhang Q. S., Yang J., et al. (2015) The role of arginine vasopressin in electroacupuncture treat - ment of primary sciatica in human. Neuropeptides 52, 61–5.
Zhao Z. Q. (2008) Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology 85 (4), 355–75.
Zheng Z., Gibson S., Helme R. D., et al. (2018) Effects of electroacupuncture on opioid consumption in patients with chronic musculoskeletal pain: a multicenter ran-domized controlled trial. Pain Medicine [Epub ahead of print.] doi: 10.1093/pm/pny113.
Zhou H.- Y., Zhang H.- M., Chen S.- R. & Pan H.- L. (2008) Increased C- fiber nociceptive input potentiates inhibi-tory glycinergic transmission in the spinal dorsal horn. Journal of Pharmacology and Experimental Therapeutics 324 (3), 1000–1010.
Zhou K., Ma Y. & Brogan M. S. (2015) Dry needling versus acupuncture: the ongoing debate. Acupuncture in Medicine 33 (6), 485–90.
Zhou X. J., Yang J., Yan F. L., et al. (2010) Norepinephrine plays an important role in antinociceptive modulation of hypothalamic paraventricular nucleus in the rat. International Journal of Neuroscience 120 (6), 428–38.
Zhu B., Xu W. D., Rong P. J., et al. (2004) A C- fiber reflex inhibition induced by electroacupuncture with different intensities applied at homotopic and heterotopic acu-points in rats selectively destructive effects on myeli-nated and unmyelinated afferent fibers. Brain Research 1011 (2), 228–37.

Mechanisms and dose parameters of electric needle stimulation – Part I
© 2018 Acupuncture Association of Chartered Physiotherapists26
Part II of this Literature Review will appear in the Spring 2019 issue of Acupuncture in Physiotherapy.
Dr Thomas Perreault graduated with a BSc in Kinesiology from The University of Maine in 2004 and earned his doctoral degree in Physical Therapy from Franklin Pierce University in 2008. Dr Perreault is a graduate of the Institute of Orthopedic Manual Therapy Clinical Fellowship in Woburn, Massachusetts and he is a Board Certified Orthopedic Specialist through the American Physical Therapy Association. He is also a member of the Acupuncture Association of Chartered Physiotherapists and has practiced in the
outpatient orthopedic setting for 10 years. Dr Perreault is currently a Clinical Specialist at Wentworth Douglass Hospital in Dover, New Hampshire for the Northern New England Spine Center with a focus on dry needling for chronic spinal pain, temporomandibular disorders and headache. He lectures internationally on dry needling for the management of musculoskeletal dis-orders. Dr Perreault is also lead author of “The local twitch response during trigger point dry needling: is it necessary for successful outcomes?” which was published in 2017 in the ever popular Journal of Bodywork and Movement Therapies.

© 2018 Acupuncture Association of Chartered Physiotherapists 27
Correspondence: Chris Boynes, Corner House, 3 The Street, Helhoughton, Nr Fakenham, Norfolk, NR21 7AH (email: [email protected])
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 27–34
PArADIGM
The interaction and outcomes of acupuncture, both traditional Chinese medicine and intra- muscular stimulation, with Deep Oscillation® Treatment: a case study- based discussion
C. Boynes Private Practice, Norfolk, UK
AbstractThis article first explains what Deep Oscillation® Treatment (DOT) is and how it works, then focuses on four case studies in which the author has used acupuncture and DOT together effectively as part of overall patient treatment and management.
Keywords: Electrostatics, lymphatics, oscillation, pain reduction, tissue response.
IntroductionDOT is an internationally- patented electro-mechanical therapy method based on the Johnsen- Rahbek effect in physics. It supplements and intensifies all types of connective tissue work without pressure, and reaches to a depth of 8 cm as proven by a burns study by Tápanes et al. (2010) and in a diagnostic ultrasound visual verification test by Medina Cabezas.
Research into the therapeutic uses of this effect on tissue was first carried out by two German physiotherapists, Wolfgang Walder and Hans Seidl, in the early 1980s. It works on the theory that if a semi- conductor is put between two electrodes and a voltage is applied, it creates an electrostatic force similar to rub-bing a balloon on your clothes and holding it over your head so your hair stands up. This generates a minimal electrostatic field, and with a semiconductor layer this force can be trans-ferred to human tissue without heat or the use of electrical stimulation. If we transfer this to deep oscillation, the membrane of the applica-tor or gloves of the therapist are the vinyl layer
(semiconductor); the adhesive electrodes as well as the metal plate, the applicator, and the titanium element held by the patient perform as the electrodes. It is a biphasic application in microampere range, thus metal implants are not contraindicated. To explain the working electrostatic field, the circuit is in the Deep Oscillation® machine. As the circuit changes polarity, the tissue is dropped and the circuit stopped temporarily through an active discharge device in the machine, which is part of the therapy’s patented circuitry. There is no prob-lem using the oscillator all day by the therapist or patient. Studies conducted in 1988 saw no adverse effects to therapist (Portnov & Zabelina 2002). The Deep Oscillation® machine can produce an electrostatic field at a low, medium or high frequency ranging from 5 Hz to 250 Hz. This alternating current is able to pick up treated tissue and then drop it at a variable speed, depending on the selected frequency. For example, at 5 Hz this occurs at 5 times a second, and at 250 Hz it occurs at 250 times a second. In treatment, this deep oscillation massage penetrates a depth of 8 cm through the skin, connective tissue, fat tissue and muscle, to reach its sphere of activity (Fig. 1).
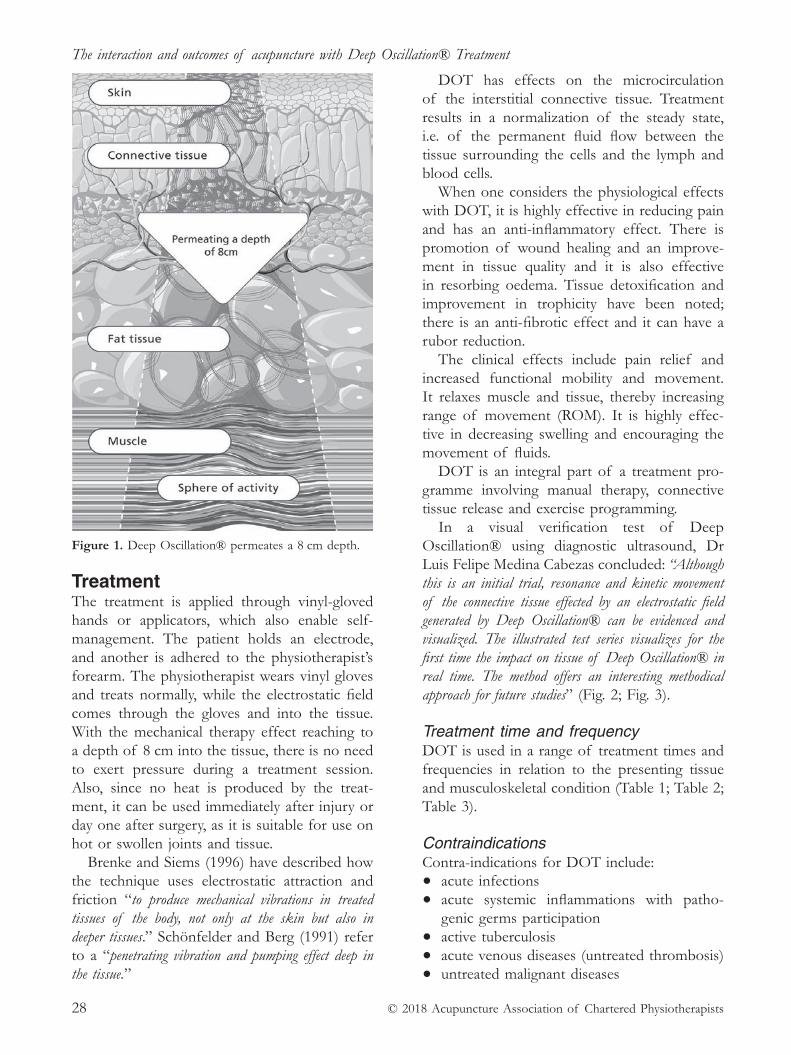
The interaction and outcomes of acupuncture with Deep Oscillation® Treatment
© 2018 Acupuncture Association of Chartered Physiotherapists28
TreatmentThe treatment is applied through vinyl- gloved hands or applicators, which also enable self- management. The patient holds an electrode, and another is adhered to the physiotherapist’s forearm. The physiotherapist wears vinyl gloves and treats normally, while the electrostatic field comes through the gloves and into the tissue. With the mechanical therapy effect reaching to a depth of 8 cm into the tissue, there is no need to exert pressure during a treatment session. Also, since no heat is produced by the treat-ment, it can be used immediately after injury or day one after surgery, as it is suitable for use on hot or swollen joints and tissue.
Brenke and Siems (1996) have described how the technique uses electrostatic attraction and friction “to produce mechanical vibrations in treated tissues of the body, not only at the skin but also in deeper tissues.” Schönfelder and Berg (1991) refer to a “penetrating vibration and pumping effect deep in the tissue.”
DOT has effects on the microcirculation of the interstitial connective tissue. Treatment results in a normalization of the steady state, i.e. of the permanent fluid flow between the tissue surrounding the cells and the lymph and blood cells.
When one considers the physiological effects with DOT, it is highly effective in reducing pain and has an anti- inflammatory effect. There is promotion of wound healing and an improve-ment in tissue quality and it is also effective in resorbing oedema. Tissue detoxification and improvement in trophicity have been noted; there is an anti- fibrotic effect and it can have a rubor reduction.
The clinical effects include pain relief and increased functional mobility and movement. It relaxes muscle and tissue, thereby increasing range of movement (ROM). It is highly effec-tive in decreasing swelling and encouraging the movement of fluids.
DOT is an integral part of a treatment pro-gramme involving manual therapy, connective tissue release and exercise programming.
In a visual verification test of Deep Oscillation® using diagnostic ultrasound, Dr Luis Felipe Medina Cabezas concluded: “Although this is an initial trial, resonance and kinetic movement of the connective tissue effected by an electrostatic field generated by Deep Oscillation® can be evidenced and visualized. The illustrated test series visualizes for the first time the impact on tissue of Deep Oscillation® in real time. The method offers an interesting methodical approach for future studies” (Fig. 2; Fig. 3).
Treatment time and frequencyDOT is used in a range of treatment times and frequencies in relation to the presenting tissue and musculoskeletal condition (Table 1; Table 2; Table 3).
ContraindicationsContra- indications for DOT include:• acute infections
• acute systemic inflammations with patho-genic germs participation
• active tuberculosis
• acute venous diseases (untreated thrombosis)
• untreated malignant diseases
Figure 1. Deep Oscillation® permeates a 8 cm depth.
C. Boynes
© 2018 Acupuncture Association of Chartered Physiotherapists 29
• erysipelas or cellulitis
• patients with cardiac pacemakers or other electronic implants
• untreated heart complaints and diseases
• pregnancy
• hypersensitivity to electrostatic fields
• infectious skin diseases.
Deep Oscillation® therapy and acupunctureThe following question was asked of Dr Jens Reinhold, CEO of Physiomed, the manufacturer
of Deep Oscillation®: “Why does DOT pre- needling make the needles go in more easily?” According to Dr Reinhold, there are four possibilities:(1) The fact that acupuncture points are more
sensitive to thermal or mechanical stimuli, involving a higher temperature, might be due to an increased number of TRPV1 pain receptors on the cells. A study by Boisnic and Branchet (2013) showed DOT led to a significant reduction in the number of TRPV1 pain receptors represented on keratinocyte cells which is an explanation for the statistically significant pain alleviat-ing potential DOT.
(2) The mechanical resonance vibrations of DOT and their effects on afferent neurons might simply have analgesic effect by influ-encing the gate control mechanism.
(3) Kuti- visceral or somato- visceral effects resulting from DOT could have effects on pain reception, resulting in ‘tissue softening’.
(4) Depending on the overall physiological and psychological condition of the patient, it may be the case that DOT just relaxes the patient who ‘lets go’ and tolerates the needles better.
Practitioner feedbackA questionnaire was sent out to medical profes-sionals in the UK who are currently utilizing Deep Oscillation® as part of their treatment protocols. Responses to the questions asked were as follows:
Question: Do you use Deep Oscillation® pre- or post- acupuncture? What is the effect on tissue; does it help needling?Answers:
• Pre-acupuncture:
• “Helps ease muscles, relaxes patient”
• “Needle insertion more comfortable after using DOT”
• Post- acupuncture:
• “Lessens the discomfort of needling”
• “Generally used to enhance physiological changes brought on by needle insertion”
• “Good for pain and spasm”
Figure 2. Still image from video of verification test of Deep Oscillation® by Dr Luis Felipe Medina Cabezas.
Figure 3. Still image from video of verification test of Deep Oscillation® by Dr Luis Felipe Medina Cabezas.
Table 1. Deep Oscillation®: treatment time and frequency range in relation to tissue condition.
ConditionTreatment time Duration Frequency range
acute short approx. 8–10 minapprox. 5 min
high frequencylow frequency
subacute long approx. 10–20 minapprox. 5 min
high frequencylow frequency
chronical
long
approx. 5 min approx. 15 min approx. 10 min
medium frequency high frequency low frequency
The interaction and outcomes of acupuncture with Deep Oscillation® Treatment
© 2018 Acupuncture Association of Chartered Physiotherapists30
• “Use a combination of DOT and acupuncture for stubborn injuries”
• “Positive changes with acupuncture and DOT on lymphatic presentations”
Question: Do you feel that using acupuncture and Deep Oscillation® has reduced treatment times? If so, by how much?Answers:
• “Not sure if it has reduced treatment times, but result is more effective”
• “Each treatment is longer but I’m seeing faster results in fewer sessions”
• “DOT has helped with pain and movement in 85–90% of patients”
• “Patients see results in probably 25% fewer sessions”
• “Not treatment times, but perhaps the frequency of treatments”
Question: What do you feel DOT does to help/interact with acupuncture?Answers:
• “Decreases tissue tension so needles insert easier”
• “Increased ROM with DOT and needles”
• “It softens tissue in areas where manual massage is difficult”
• “Each treatment complements each other; it offers a calming and soothing effect on clients”
• “Encourages relaxation prior to needling; relaxation both of the patient mentally, and of the tissues physically”
Question: What do your patients feel about your use of DOT; what feedback do you regularly get?Answers:
• “Players generally comment that they feel that have come back more quickly than they expected and feel a lot more mobile following treatment”
• “They love it. They are surprised it is effective as it feels so comfortable”
• “Reduction in pain, feels less tight and looser”
• “Most patients respond favourably to DOT and are quite intrigued by its concept. Most have found relief of symptoms when applied to painful neck and shoulders”
Case studiesUsed in conjunction with acupuncture as part of the treatment protocol, the author has found that the use of DOT prior to (and post- ) nee-dling helps the tissue feel softer, allowing the needles to go in better, particularly with intra- muscular stimulation (IMS).
Table 2. Examples of different frequencies used to treat musculoskeletal (MSK) presentations.
MSK presentation Treatment
an arthritic setting 160 Hz × 10 min followed by 85 Hz × 5 mintennis elbow/golfer’s elbow 160 Hz – 180 Hz followed by 85 Hz × 5 minsciatica setting 170 Hz – 200 Hz × 10 min followed by 28 Hz – 40 Hz × 5 minmixed tissue response 250 Hz × 20 min, then 60 Hz × 20 min (considering what the different frequencies do to the
tissue – a ‘pain’ setting initially followed by a more ‘pumping’ effect)adhesive capsulitis 25 Hz – 80 Hz × 5 min then 80 Hz – 250 Hz × 15 min then 5 Hz – 25 Hz × 10 min
Table 3. The effect of different Deep Oscillation® frequencies.
Frequency Effect
high frequencies (80–250 Hz) • pain significantly reduced• lymphatic drainage pathways opened and activated• trapped cellular metabolic waste/abnormal fluid build- up broken down• hardened fibrotic tissue & scar tissue dispersed
medium frequencies (25–80 Hz) • microcirculation in the interstitial spaces of the connective tissue is boosted• tissue layers are relaxed• biological waste products move out to the lymph system for removal
low frequencies (5–25 Hz)
• vasodilation causes slight lowering of blood pressure. • a powerful, gentle, pumping action causes strong movement in the tissue. • re- instigation of flowing fluids encourages essential nutrients back to the tissue

C. Boynes
© 2018 Acupuncture Association of Chartered Physiotherapists 31
Case study 1Fifty- eight- year- old Ms C. first came to see the therapist having had problems with her neck, left- sided shoulder girdle pain and left- sided facial pain. Her previous medical history included 15 years of neck pain; diagnosis with left- sided facial neuralgia in the summer of 2016; and diagnosis in 2017 with left- sided temporomandibular (TMJ) problems.
Her problem list included a lack of neck movement with both rotations and side flexions along with a loss of cervical spine extension and combined rotation with extension. She was stiff in the thoracic spine from the cervico-thoracic junction (CTJ) to T8- T9 and had stiffer first ribs bi- laterally. She was also having regular neuralgic type left- sided neck and cheek pain which was sharp most of the time and had not cleared since some dental work in 2014.
Treatment included manual therapy for joint work, including sustained natural apophyseal glides (SNAGs); posterior- anterior (P–A) and anterior- posterior (A–P) joint mobilizations; rotational mobilizations plus adjustments at the cervical spine and thoracic spine; and connec-tive tissue releases for soft tissue on the anterior, lateral and posterior neck and shoulders. DOT was used for stiffness, pain and tissue ‘soften-ing’ with frequencies of 200 Hz and 60 Hz for 20 min each or more in a session.
Further treatment included IMS to the neck, shoulders and thoracic spine for tissue changes. Notably the upper trapezius, levator scapulae, splenius capitas and cervices, and sternocleido-mastoid (SCM) and further into the rhomboids and the thoracic spine. Traditional Chinese medicine (TCM) points for the neuralgic- type pain (mostly upper cervical spine) were given, also for symptoms of headache and migraine, which included Gall Bladder (GB) 20, GB 21, Bladder (BL) 10, Large Intestine (LI) 4, BL 60 and Kidney (KI) 3, plus manual therapy for joint range of movement (ROM) improvement at C1/C2 to C3/C4. Also, left- sided points were used for the neuralgic- type pain affected by the upper cervical points such as Governor Vessel (GV) 20, BL 7, BL 9, BL 10 and BL 11. Specific home exercises were given for the
upper cervical spine rotation and neck/shoulder ROM.
After eight 1- h sessions, the patient felt the pain had reduced significantly and was 98% improved. She was no longer suffering from the neuralgic- type constant pain.
Clinical reasoning: Firstly the TCM points abolished the neuralgic- type problem. Secondly, the IMS changed the tissue pain/tension. Thirdly, the DOT helped the tissue stiffness and ‘pain,’ and encouraged ROM and ultimately daily function. An important point here to note was that when needling post- DOT, the tissue was softer and less ‘crampy’ then pre- DOT treatment.
Case study 2Seventy- three- year- old Mr P. attended the clinic with severe migraine and blurred vision. His previous medical history included suffering with headaches and migraines since his twenties. His past treatment included drug therapy which had helped, although he did feel that when he was on beta blockers it had made things worse. He also had longstanding stiffness with his neck and shoulders.
After initial assessment, his problem list included joint and connective tissue tightness, and a reduced ROM with both shoulder joints, but there was no neural referral or signs and symptoms of such. The migraines were in an area that suggested the GB channel, with pain in the area of GB 14 and GB 20 in the neck.
Initial treatment included Mulligan’s headache SNAG at C0/C1 and rotation at C1/C2, but this only made small changes for the better. TCM points were then applied at GB 20 initially, then at BL 10, GB 41, LI 4 and Stomach (ST) 8, and IMS at the upper trapezius, levator scapulae, rhomboids, infraspinatus (IS) and pectoral major and minor, subscapularis, deltoids/splenius capitas and cervices. Further manual therapy involved SNAGs, mobilizations and adjustments to the CTJ and thoracic spine. DOT was added at 200 Hz and 60 Hz between 20 and 40 min in a session for pain and tissue softening. This always left the patient’s neck moving more easily and it was even more comfortable with warmth applied after the treatment sessions.
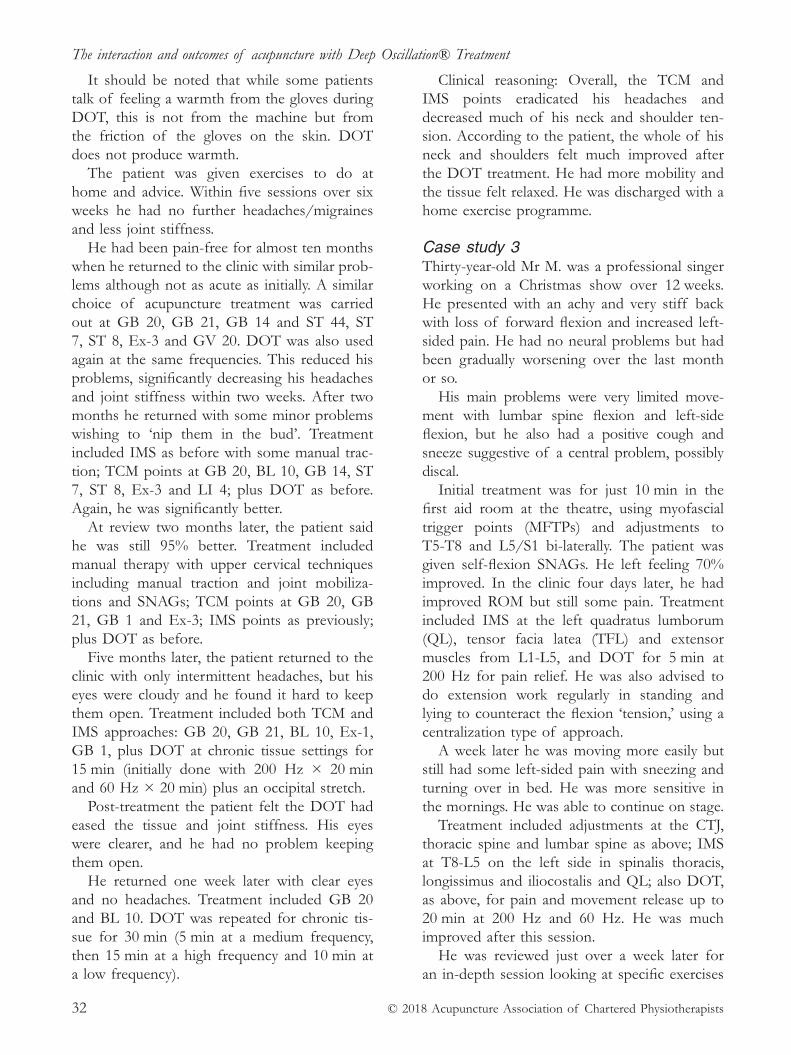
The interaction and outcomes of acupuncture with Deep Oscillation® Treatment
© 2018 Acupuncture Association of Chartered Physiotherapists32
It should be noted that while some patients talk of feeling a warmth from the gloves during DOT, this is not from the machine but from the friction of the gloves on the skin. DOT does not produce warmth.
The patient was given exercises to do at home and advice. Within five sessions over six weeks he had no further headaches/migraines and less joint stiffness.
He had been pain- free for almost ten months when he returned to the clinic with similar prob-lems although not as acute as initially. A similar choice of acupuncture treatment was carried out at GB 20, GB 21, GB 14 and ST 44, ST 7, ST 8, Ex- 3 and GV 20. DOT was also used again at the same frequencies. This reduced his problems, significantly decreasing his headaches and joint stiffness within two weeks. After two months he returned with some minor problems wishing to ‘nip them in the bud’. Treatment included IMS as before with some manual trac-tion; TCM points at GB 20, BL 10, GB 14, ST 7, ST 8, Ex- 3 and LI 4; plus DOT as before. Again, he was significantly better.
At review two months later, the patient said he was still 95% better. Treatment included manual therapy with upper cervical techniques including manual traction and joint mobiliza-tions and SNAGs; TCM points at GB 20, GB 21, GB 1 and Ex- 3; IMS points as previously; plus DOT as before.
Five months later, the patient returned to the clinic with only intermittent headaches, but his eyes were cloudy and he found it hard to keep them open. Treatment included both TCM and IMS approaches: GB 20, GB 21, BL 10, Ex- 1, GB 1, plus DOT at chronic tissue settings for 15 min (initially done with 200 Hz × 20 min and 60 Hz × 20 min) plus an occipital stretch.
Post- treatment the patient felt the DOT had eased the tissue and joint stiffness. His eyes were clearer, and he had no problem keeping them open.
He returned one week later with clear eyes and no headaches. Treatment included GB 20 and BL 10. DOT was repeated for chronic tis-sue for 30 min (5 min at a medium frequency, then 15 min at a high frequency and 10 min at a low frequency).
Clinical reasoning: Overall, the TCM and IMS points eradicated his headaches and decreased much of his neck and shoulder ten-sion. According to the patient, the whole of his neck and shoulders felt much improved after the DOT treatment. He had more mobility and the tissue felt relaxed. He was discharged with a home exercise programme.
Case study 3Thirty- year- old Mr M. was a professional singer working on a Christmas show over 12 weeks. He presented with an achy and very stiff back with loss of forward flexion and increased left- sided pain. He had no neural problems but had been gradually worsening over the last month or so.
His main problems were very limited move-ment with lumbar spine flexion and left- side flexion, but he also had a positive cough and sneeze suggestive of a central problem, possibly discal.
Initial treatment was for just 10 min in the first aid room at the theatre, using myofascial trigger points (MFTPs) and adjustments to T5- T8 and L5/S1 bi- laterally. The patient was given self- flexion SNAGs. He left feeling 70% improved. In the clinic four days later, he had improved ROM but still some pain. Treatment included IMS at the left quadratus lumborum (QL), tensor facia latea (TFL) and extensor muscles from L1- L5, and DOT for 5 min at 200 Hz for pain relief. He was also advised to do extension work regularly in standing and lying to counteract the flexion ‘tension,’ using a centralization type of approach.
A week later he was moving more easily but still had some left- sided pain with sneezing and turning over in bed. He was more sensitive in the mornings. He was able to continue on stage.
Treatment included adjustments at the CTJ, thoracic spine and lumbar spine as above; IMS at T8- L5 on the left side in spinalis thoracis, longissimus and iliocostalis and QL; also DOT, as above, for pain and movement release up to 20 min at 200 Hz and 60 Hz. He was much improved after this session.
He was reviewed just over a week later for an in- depth session looking at specific exercises
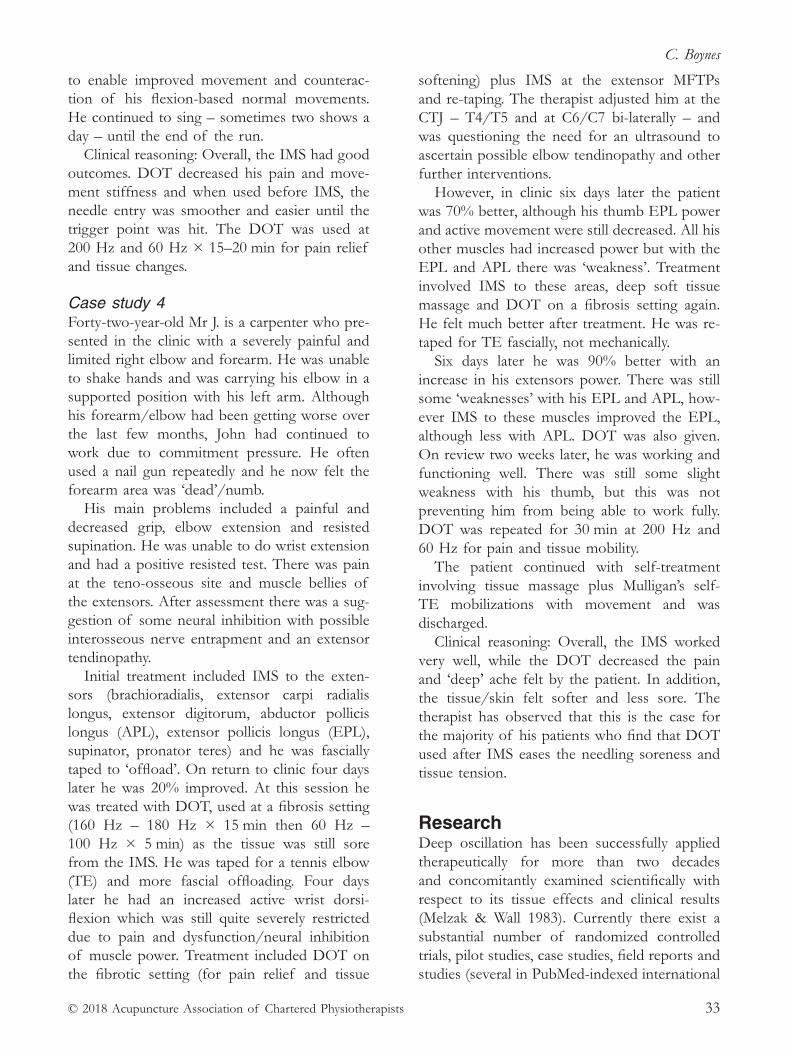
C. Boynes
© 2018 Acupuncture Association of Chartered Physiotherapists 33
to enable improved movement and counterac-tion of his flexion- based normal movements. He continued to sing – sometimes two shows a day – until the end of the run.
Clinical reasoning: Overall, the IMS had good outcomes. DOT decreased his pain and move-ment stiffness and when used before IMS, the needle entry was smoother and easier until the trigger point was hit. The DOT was used at 200 Hz and 60 Hz × 15–20 min for pain relief and tissue changes.
Case study 4Forty- two- year- old Mr J. is a carpenter who pre-sented in the clinic with a severely painful and limited right elbow and forearm. He was unable to shake hands and was carrying his elbow in a supported position with his left arm. Although his forearm/elbow had been getting worse over the last few months, John had continued to work due to commitment pressure. He often used a nail gun repeatedly and he now felt the forearm area was ‘dead’/numb.
His main problems included a painful and decreased grip, elbow extension and resisted supination. He was unable to do wrist extension and had a positive resisted test. There was pain at the teno- osseous site and muscle bellies of the extensors. After assessment there was a sug-gestion of some neural inhibition with possible interosseous nerve entrapment and an extensor tendinopathy.
Initial treatment included IMS to the exten-sors (brachioradialis, extensor carpi radialis longus, extensor digitorum, abductor pollicis longus (APL), extensor pollicis longus (EPL), supinator, pronator teres) and he was fascially taped to ‘offload’. On return to clinic four days later he was 20% improved. At this session he was treated with DOT, used at a fibrosis setting (160 Hz – 180 Hz × 15 min then 60 Hz – 100 Hz × 5 min) as the tissue was still sore from the IMS. He was taped for a tennis elbow (TE) and more fascial offloading. Four days later he had an increased active wrist dorsi- flexion which was still quite severely restricted due to pain and dysfunction/neural inhibition of muscle power. Treatment included DOT on the fibrotic setting (for pain relief and tissue
softening) plus IMS at the extensor MFTPs and re- taping. The therapist adjusted him at the CTJ – T4/T5 and at C6/C7 bi- laterally – and was questioning the need for an ultrasound to ascertain possible elbow tendinopathy and other further interventions.
However, in clinic six days later the patient was 70% better, although his thumb EPL power and active movement were still decreased. All his other muscles had increased power but with the EPL and APL there was ‘weakness’. Treatment involved IMS to these areas, deep soft tissue massage and DOT on a fibrosis setting again. He felt much better after treatment. He was re- taped for TE fascially, not mechanically.
Six days later he was 90% better with an increase in his extensors power. There was still some ‘weaknesses’ with his EPL and APL, how-ever IMS to these muscles improved the EPL, although less with APL. DOT was also given. On review two weeks later, he was working and functioning well. There was still some slight weakness with his thumb, but this was not preventing him from being able to work fully. DOT was repeated for 30 min at 200 Hz and 60 Hz for pain and tissue mobility.
The patient continued with self- treatment involving tissue massage plus Mulligan’s self- TE mobilizations with movement and was discharged.
Clinical reasoning: Overall, the IMS worked very well, while the DOT decreased the pain and ‘deep’ ache felt by the patient. In addition, the tissue/skin felt softer and less sore. The therapist has observed that this is the case for the majority of his patients who find that DOT used after IMS eases the needling soreness and tissue tension.
research Deep oscillation has been successfully applied therapeutically for more than two decades and concomitantly examined scientifically with respect to its tissue effects and clinical results (Melzak & Wall 1983). Currently there exist a substantial number of randomized controlled trials, pilot studies, case studies, field reports and studies (several in PubMed- indexed international

The interaction and outcomes of acupuncture with Deep Oscillation® Treatment
© 2018 Acupuncture Association of Chartered Physiotherapists34
journals) to provide a medical evidence base for deep oscillation.
Full references for Deep Oscillation® research and studies can be obtained via the website https://www.physiomed.de/en/products/deep-oscillation-evident-clinics/#bibliography and in Reinhold (2017).
references Boisnic S. & Branchet M.- C. (2013) Anti- inflammatory
and draining effect of the Deep Oscillation® device tested clinically and on a model of human skin maintained in a survival condition. European Journal of Dermatology 23 (1), 59–63.
Brenke R. & Siems W. (1996) Adjuvante therapie beim lym-phödem [Adjuvant therapy in lymphedema]. Zeitschrift fur Lymphologie 20 (1), 31–35.
Medina Cabezas L. F. Visual verification of deep oscil-lation with diagnostic ultrasound. [Online video.] https://youtu.be/LiiiktcNENM
Portnov V. & Zabelina Y. (2002) New method for deep mas-sage of tissues: first results of Hivamat 200 system clinical application in Russia. President Affairs Department of the Russian Federation Medical Center Central Clinical Hospital, Moscow, Russia.
Reinhold J. (2017) Mechanisms of deep oscillation. The Journal: Manual Lymphatic Drainage UK [WWW
document.] http://www.physiopod.co.uk/assets/images2017/2017- MLD- 6pp- web.pdf
Schönfelder G. & Berg D. (1991) Nebenwirkungen nach brusterhaltender therapie des mammakarzinoms. erste ergebnisse mit Hivamat® 200. [Therapy for a carci-noma of the breast followed by early treatment with Deep Oscillation® therapy] Gynaekologische Praxis 15, 109–122.
Tápanes S. H., Suárez A., Acosta T. B., et al. (2010) Value of deep oscillation therapy in the healing of AB burns. Cuban Journal of Physical Medicine & Rehabilitation RNPS 2244, Folio 148.
Chris Boynes is a chartered physiotherapist, manual and sports specialist, and acupuncture practitioner. He has thirty years of experience treating musculoskeletal conditions, has practised acupuncture for over twenty years, and has worked in professional rugby and other elite sports. At the May 2018 AACP Conference, Mr Boynes discussed his use of acupuncture with Deep Oscillation® Treatment, both of which he uses as an interactive tool with all his physiotherapy skills, and gave his personal observations on how effective they had been in helping with pain relief, muscle and tissue relaxation and improving functional mobility and movement.

© Journal of Chinese Medicine 35
Correspondence: Amos Ziv, Heaven and Earth TCM specialty clinic, Rehovot, Israel (email: aaziv10@ netvision.net.il)
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 35–44
PArADIGM
Practical applications of meridian theory in pain management – the meridian wave approach
A. ZivHeaven and Earth TCM specialty clinic, Rehovot, Israel
I. leviHeaven and Earth TCM specialty clinic, Rehovot, Israel
AbstractMeridian theory serves as a fundamental concept in classical Chinese medicine. Yin yang and five phase theory, zang fu internal organ theory and channel theory comprise a theoreti-cal foundation often described as the ‘Three Pillars’ of Chinese medicine. Meridian wave acupuncture is an effective, evidence- based system for pain management based on classical channel theory. This article outlines the basic theory and main techniques of this system for clinical application in pain management. A key element discussed involves the arrangement of the channel system into six pairs of functional physiological units. These six channels act as connecting pathways between the external environment and the internal environment of the internal organs. Each channel resonates with a distinct wave quality. By tapping into the correct channel with acupuncture treatment, a strong wave- like movement of Qi can be induced in order to vigorously resolve obstruction. Three main actions are performed dur-ing the acupuncture session and include a ripple ‘wave initiation’ through bleeding jing- well points, a channel Qi- leveraging ‘wave propagation’ through needling distal ends of the same channel, and immediate assessment of the result that is described as ‘wave effect’. Although many additional elements support this system, the key aspects presented here serve as an immediately applicable and effective tool for pain management. Much of the work and theory described in this article is based on the teachings of the late Professor Dr Wang Ju Yi, a contemporary master of channel theory- based acupuncture.
Keywords: acupuncture, bleeding, channels, injury, leverage, meridians, meridian wave, musculo-skeletal, obstruction, pain, Qi, wave.
Authors’ noteThe use of the term ‘channel’ rather than ‘meridian’ has been debated by modern scholars of Chinese medicine (Ellis et al. 1989). ‘Channel’ is often preferred as a term that better describes their concept and function. Nevertheless, the authors use the term ‘meridian’ in this article as it includes the notions of spatial direction
and accuracy, which help to convey the practical essence of this acupuncture system.
Preface Meridian theory forms a fundamental aspect of classical Chinese medicine. Together with yin yang and five phase theory, and zang fu theory, it comprises the foundational theory known as the ‘Three Pillars’ of Chinese medicine as described in the Nei Jing (Inner Classic). For historical reasons beyond the scope of this arti-cle, meridian theory has been less emphasized

Practical applications of meridian theory in pain management – the meridian wave approach
© Journal of Chinese Medicine36
in the teachings of modern traditional Chinese medicine (TCM). Practising acupuncture with-out a thorough understanding of meridian theory undermines the theoretical framework of classical Chinese medicine, and may lead to a significant reduction in therapeutic effectiveness.
Understanding meridian theory provides insight into the classical Chinese medicine perspective of how the body works internally, and how it interacts with the outer world and universe. Because of this, meridian theory- based acupuncture often produces significantly improved outcomes in practice. This article outlines an effective and practical application of meridian theory- based acupuncture. Specifically focused on the treatment of pain and move-ment limitation, the meridian wave acupuncture system is rooted in classical Chinese medicine meridian theory. It has been used on thousands of patients in China, Europe, the United States and Israel. This pain management acupuncture system has been validated successfully in a randomized controlled trial of acupuncture for acute back or neck pain in the emergency (A&E) room of a major hospital in Israel (Ziv et al. 2012). Compared to sham acupuncture and no treatment control, results showed a decrease in total pain of more than 40% and an increase in spinal flexion- extension of more than 26%.
IntroductionAs described in the Nei Jing, Chinese medicine is based on three theories that form a funda-mental organizational framework, collectively referred to as the ‘Three Pillars’ of Chinese medicine (Wang & Robertson 2008).
Yin yang and five phase theoryThese two theories form a basic language or code that can be used to describe all phenomena in the universe, including the human body. With this language all existence and events, including disease and healing, can be categorized and described. With analogy to Western science, these theories can be likened to the mathemati-cal formulae that describe the workings of the universe.
Zang fu theory Zang fu (internal organ) theory is a major subject of discussion in the classic texts of Chinese medicine. It refers to the physiology and pathology in the body as governed by functional organ systems, whose major role is the production, preservation and storage of the vital substances: Qi, blood, jing- essence and body fluids. With analogy to Western science, zang fu theory has parallels with the subjects of anatomy, physiology and pathology.
Meridian theory While the rules of the outer universe and climates are conveyed by the language of yin yang and the five phases, and physiology and pathology are mainly categorized according to zang fu functions, meridian theory is the con-necting pathway between these theories. The meridians represent the connection between the inner physiology of the body and the climates of the outer universe. With analogy to Western science, meridian theory has parallels with phys-ics and chemistry, through which we see the mathematical laws of the universe manifesting in physiology and pathology. That is, physical and chemical laws such as thermodynamics and biochemistry, are at the basis of all physiological and pathological processes in the living body. Likewise, from a Chinese medicine perspective the meridian system is the basis of all physio-logical and pathological processes in the living body.
The emergence of meridian theoryScholars of the Nei Jing formed their holistic view of the universe and the human body by observing nature. These theorists of classi-cal Chinese sciences strove to understand the relationship between the human body and its environment, between the microcosm and the macrocosm. The meridians are a key concept in actualising this holistic nature. According to this view, the meridians have distinct pathways which connect the organs internally, and are involved in processes through which the body

A. Ziv & I. Levi
© Journal of Chinese Medicine 37
interacts with the environment. Understanding the unifying role of the meridians is what gives life to the concept of holism in Chinese medicine: “Without channel theory the principle of ‘holism’ in Chinese medicine makes little sense ” (Wang Ju Yi).
It is important to emphasise that in the clas-sics the meridians are not described as ‘hollow pipes’ but as a physiologically active units that act as networks (wang lou), pathways (tong dao) and communication systems (tu jing) (Wang 1999). Thus the meridians are a living network that bind yin and yang, external to internal, and conduct necessary external influences into the internal environment and vice versa. They thus facilitate healthy physiological activity and, in case of dysfunction, actively participate in rebalancing pathology. Information about the state of the organs and their surroundings (the inner ‘climate’) is continuously commu-nicated by the meridians in order to facilitate physiological balance. For example, a state of excess dampness in the Tai Yin Spleen may be communicated to the Yang Ming system in order to promote a response of increasing dry-ness. Dryness is the inner climate of the Yang Ming, which is regulated by the Large Intestine absorbing excess fluids from the intestines. This explains the rationale behind needling Zusanli Stomach (ST) 36 for Spleen damp- related diar-rhoea. Thus the meridians are referred to in the early classics as an integral part of the organs themselves, yet contain functions that surpass the general function of the organs due to their role in inter acting with the outer environment and climate (Wang 2000).
Meridian theory and external climates – the six QiThe meridians connect the Qi of the body to the Qi of the external environment. The exter-nal climatic influences are also referred to as the six Qi. These are cold, summer- heat/fire, damp-ness, dryness, fire and wind. It is important to note that the six Qi are functional climatic forces which are necessary for the function of the internal organs and are therefore not necessarily ‘evil’ factors. The six Qi may become the six
‘evil’ Qi if the meridian system is impaired and unable to maintain balance with the climates or if the climatic influences are excessively strong and invade the body. The climate- meridian rela-tionships are specific, and the meridians bond each of the six Qi to a specific organ system:
Tai Yang (Small Intestine, Bladder) – coldShao Yang (San Jiao, Gall Bladder) –
summer- heat Yang Ming (Large Intestine, Stomach) – drynessTai Yin (Lung, Spleen) – dampnessShao Yin (Heart, Kidney) – fireJue Yin (Pericardium, Liver) – windThe meridian system has both external and
internal functions. The external role is to bal-ance and regulate the movement of the six Qi into and out of the body. The meridians may allow the climates to enter, or else push them away, thus regulating the internal climate. As extensions of the organs, the internal role of the meridians is to balance and regulate the functions of the zang fu through an intricate web of inner connections, thus maintaining the appropriate inner climatic environment for each organ. Thus the meridians regulate organ activ-ity and serve as pathways for information and substance to flow to and from the organs.
As an example of the external role of the meridian system, consider the response of the Tai Yang meridian to external cold. Tai Yang, the outermost yang channel, has the role of dispersing yang Qi and heat to the surface (i.e., wei- defensive Qi) in order to prevent invasion of excess cold into the body. It also controls the skin pores, which are opened or closed to prevent or induce sweating according to needs of warm-ing or cooling the surface. Using the warming yuan- source points (Wangu Small Intestine (SI) 4 and Jinggu Bladder (BL) 64) on this meridian can rapidly resolve symptoms of external cold such as runny nose, aversion to cold and wind, itchy throat, low grade fever and stiffness in the upper back and neck caused by cold stagnation in the upper part of the Tai Yang.
As an example of the inner role of the meridian system, consider the functions of the Tai Yin meridian. Among many other functions, Tai Yin is the receiver and balancer of damp-ness. Moisture that is needed for the proper
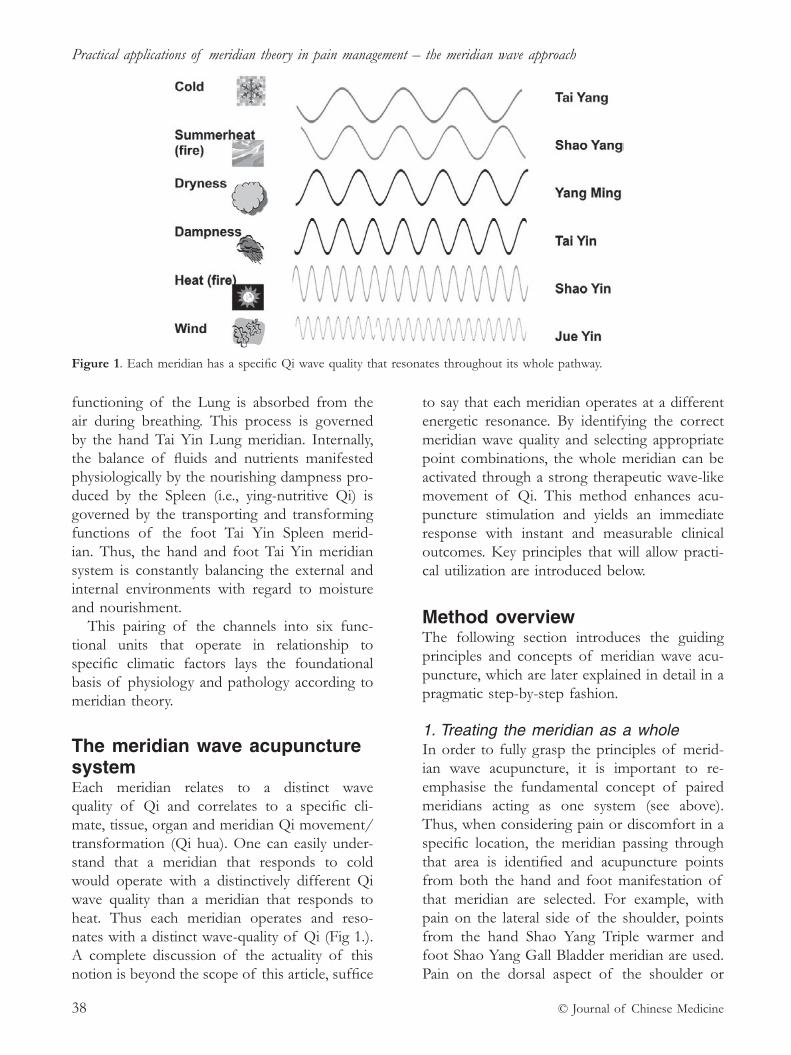
Practical applications of meridian theory in pain management – the meridian wave approach
© Journal of Chinese Medicine38
functioning of the Lung is absorbed from the air during breathing. This process is governed by the hand Tai Yin Lung meridian. Internally, the balance of fluids and nutrients manifested physiologically by the nourishing dampness pro-duced by the Spleen (i.e., ying- nutritive Qi) is governed by the transporting and transforming functions of the foot Tai Yin Spleen merid-ian. Thus, the hand and foot Tai Yin meridian system is constantly balancing the external and internal environments with regard to moisture and nourishment.
This pairing of the channels into six func-tional units that operate in relationship to specific climatic factors lays the foundational basis of physiology and pathology according to meridian theory.
The meridian wave acupuncture system Each meridian relates to a distinct wave quality of Qi and correlates to a specific cli-mate, tissue, organ and meridian Qi movement/ transformation (Qi hua). One can easily under-stand that a meridian that responds to cold would operate with a distinctively different Qi wave quality than a meridian that responds to heat. Thus each meridian operates and reso-nates with a distinct wave- quality of Qi (Fig 1.). A complete discussion of the actuality of this notion is beyond the scope of this article, suffice
to say that each meridian operates at a different energetic resonance. By identifying the correct meridian wave quality and selecting appropriate point combinations, the whole meridian can be activated through a strong therapeutic wave- like movement of Qi. This method enhances acu-puncture stimulation and yields an immediate response with instant and measurable clinical outcomes. Key principles that will allow practi-cal utilization are introduced below.
Method overviewThe following section introduces the guiding principles and concepts of meridian wave acu-puncture, which are later explained in detail in a pragmatic step- by- step fashion.
1. Treating the meridian as a wholeIn order to fully grasp the principles of merid-ian wave acupuncture, it is important to re- emphasise the fundamental concept of paired meridians acting as one system (see above). Thus, when considering pain or discomfort in a specific location, the meridian passing through that area is identified and acupuncture points from both the hand and foot manifestation of that meridian are selected. For example, with pain on the lateral side of the shoulder, points from the hand Shao Yang Triple warmer and foot Shao Yang Gall Bladder meridian are used. Pain on the dorsal aspect of the shoulder or
Figure 1. Each meridian has a specific Qi wave quality that resonates throughout its whole pathway.
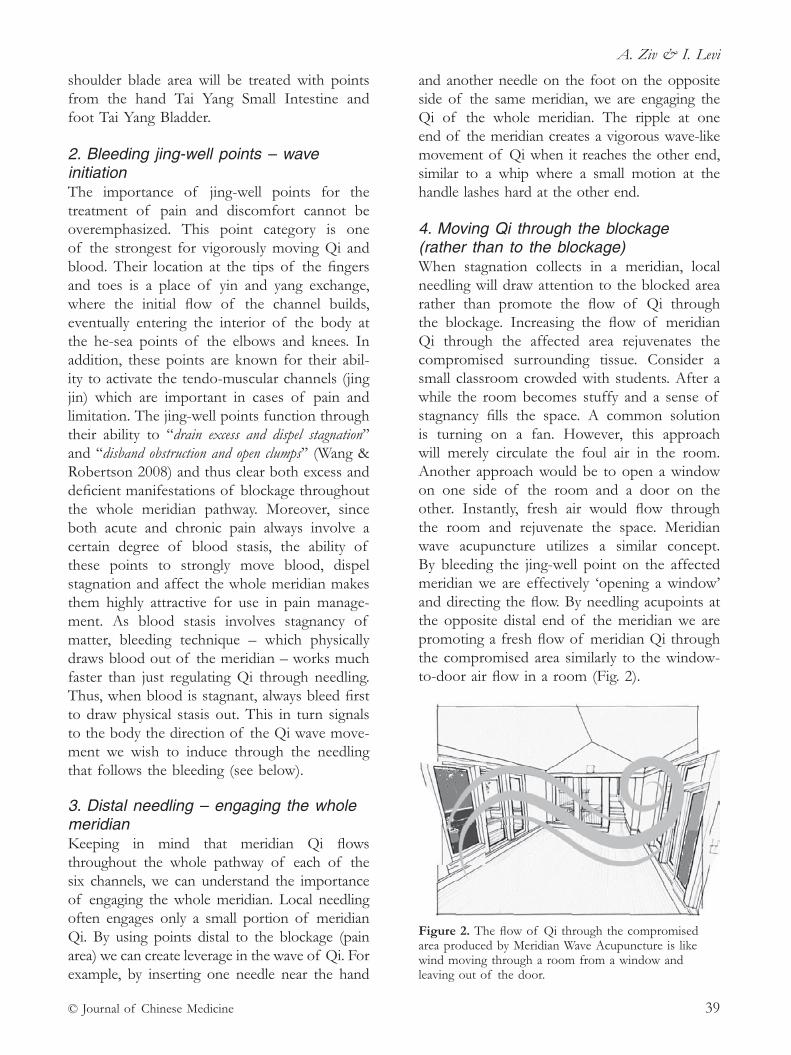
A. Ziv & I. Levi
© Journal of Chinese Medicine 39
shoulder blade area will be treated with points from the hand Tai Yang Small Intestine and foot Tai Yang Bladder.
2. Bleeding jing- well points – wave initiationThe importance of jing- well points for the treatment of pain and discomfort cannot be overemphasized. This point category is one of the strongest for vigorously moving Qi and blood. Their location at the tips of the fingers and toes is a place of yin and yang exchange, where the initial flow of the channel builds, eventually entering the interior of the body at the he- sea points of the elbows and knees. In addition, these points are known for their abil-ity to activate the tendo- muscular channels (jing jin) which are important in cases of pain and limitation. The jing- well points function through their ability to ‘‘drain excess and dispel stagnation’’ and ‘‘disband obstruction and open clumps’’ (Wang & Robertson 2008) and thus clear both excess and deficient manifestations of blockage throughout the whole meridian pathway. Moreover, since both acute and chronic pain always involve a certain degree of blood stasis, the ability of these points to strongly move blood, dispel stagnation and affect the whole meridian makes them highly attractive for use in pain manage-ment. As blood stasis involves stagnancy of matter, bleeding technique – which physically draws blood out of the meridian – works much faster than just regulating Qi through needling. Thus, when blood is stagnant, always bleed first to draw physical stasis out. This in turn signals to the body the direction of the Qi wave move-ment we wish to induce through the needling that follows the bleeding (see below).
3. Distal needling – engaging the whole meridianKeeping in mind that meridian Qi flows throughout the whole pathway of each of the six channels, we can understand the importance of engaging the whole meridian. Local needling often engages only a small portion of meridian Qi. By using points distal to the blockage (pain area) we can create leverage in the wave of Qi. For example, by inserting one needle near the hand
and another needle on the foot on the opposite side of the same meridian, we are engaging the Qi of the whole meridian. The ripple at one end of the meridian creates a vigorous wave- like movement of Qi when it reaches the other end, similar to a whip where a small motion at the handle lashes hard at the other end.
4. Moving Qi through the blockage (rather than to the blockage)When stagnation collects in a meridian, local needling will draw attention to the blocked area rather than promote the flow of Qi through the blockage. Increasing the flow of meridian Qi through the affected area rejuvenates the compromised surrounding tissue. Consider a small classroom crowded with students. After a while the room becomes stuffy and a sense of stagnancy fills the space. A common solution is turning on a fan. However, this approach will merely circulate the foul air in the room. Another approach would be to open a window on one side of the room and a door on the other. Instantly, fresh air would flow through the room and rejuvenate the space. Meridian wave acupuncture utilizes a similar concept. By bleeding the jing- well point on the affected meridian we are effectively ‘opening a window’ and directing the flow. By needling acupoints at the opposite distal end of the meridian we are promoting a fresh flow of meridian Qi through the compromised area similarly to the window- to- door air flow in a room (Fig. 2).
Figure 2. The flow of Qi through the compromised area produced by Meridian Wave Acupuncture is like wind moving through a room from a window and leaving out of the door.
Practical applications of meridian theory in pain management – the meridian wave approach
© Journal of Chinese Medicine40
5. Addressing the underlying conditionDifferential diagnosis is one of the jewels of Chinese medicine. A thorough understanding of the underlying imbalance involved in a problem is a key to clinical success. Apart from bleeding and needling to activate meridian Qi flow, we must always address any underlying imbalances. When using meridian wave acupuncture, we commonly experience that after the immediate improvement in pain and/or movement limita-tion after bleeding and needling to activate the meridian wave, we achieve additional instant improvement if we add one or two needles to address the underlying condition. It is almost as if the body ‘released’ Qi flow to the merid-ian wave as it felt secure that its underlying conditions are also being attended to by the treatment.
6. Repeatedly assessing the results of the treatment – wave effectAs discussed below, repeated assessment of the treatment effect is an integral part of this system, since results are expected immediately, during the treatment session.
Practical step- by- step meridian wave acupunctureIn the majority of the cases treated with this system, results are expected within minutes. In fact, if results are not achieved instantly, the steps conducted should be re- examined. This is not to say that we should expect immedi-ate results in 100% of patients. However, in most cases this is what we have seen. For over 15 years, this system has been used in our clin-ics and taught to hundreds of practitioners. The feedback received supports this notion. In addition, this system has been adopted as treatment of choice in a major hospital’s ortho-paedic emergency room (A&E) for acute pain after being validated in a randomized controlled study.
Step one: Establishing a pain/limitation scaleEstablishing an objective assessment of the degree of pain and/or limitation is a crucial
step. Since results of the treatment are assessed during the acupuncture session, and since an immediate improvement of 20 to 100% is expected, an accurate initial assessment is neces-sary to provide feedback on treatment efficacy. The assessment must actively engage the patient, and it is best to scale the limitation from 1 to 10. Whether the complaint is pain, discom-fort, numbness, tingling or decreased range of motion, a quantified measurement should be pursued. Initially simply ask the patient to gently show what movement or posture gener-ates the most discomfort and to quantify this on a scale of 1 to 10. The assessment should be used repeatedly throughout the treatment to identify which intervention (point combina-tion, meridian selection, etc.) yields the best therapeutic effect. Three approaches should be considered:(1) Palpation: the patient feels the pain as a
reaction to palpation at a specific location. (2) Range of motion: the pain arises during
specific movements (flexion, extension, rotation, etc.). This includes both passive range of movement (ROM) testing, where the pain arises when the practitioner initiates the movement, and active ROM testing, where pain arises when the patient initiates the movement.
(3) Resistance: the pain arises as a reaction to resistance to certain movements.
In addition, the nature of the patient’s problem is likely to provide important information about the type of stagnation that is blocking the meridian. This may be heat or cold sensations, aggravation due to specific factors, heaviness, weakness, moving pain, fixed pain, and so on. This information is crucial for selecting the cor-rect points on the meridian to activate the wave. For example, with pain associated with redness and a sensation of heat, ying- spring points are often selected due to their ability to clear heat.
Step two: Identifying the correct meridianAfter completing the assessment, identifying the correct meridian should be easy: simply ask the patient to point at the area of dis-comfort. Remember that the channel has two

A. Ziv & I. Levi
© Journal of Chinese Medicine 41
outputs, one on the hand and one on the foot. More than one meridian may be involved, in which case identify all the meridians involved. However, insist on isolating which meridian is compromised the most (i.e., most painful or limited in motion).
Step three: Wave initiation – bleeding the jing- well pointAfter identifying the correct meridian and quan-tifying the pain or limitation of ROM, the ini-tiation of the meridian Qi wave is achieved by bleeding the jing- well point. Since each meridian has two jing- well points, one on the hand and one on the foot, the selected point should be on the limb closest to the obstruction. For example, for right- sided anterior shoulder pain involving the Yang Ming meridian, bleeding is done at right Shangyang Large Intestine (LI) 1, for left- sided medial knee pain involving the Jue Yin meridian, bleeding is done at left Dadun Liver (LR) 1, or for lower back pain radiating to the back of the left thigh, bleeding is done at left Zhiyin BL 67. More complex examples require an understanding of the meridian sys-tem: for left- sided upper neck pain along the Shao Yang Gall Bladder meridian, bleeding is done at left- sided Guanchong San Jiao (SJ) 1, since this the end of the meridian closer to the obstruction. For right- sided upper back pain along the Tai Yang Bladder meridian, bleeding is done at right- sided Shaoze SI 1, again as this is the end of the meridian closer to the obstruction. As a general rule, pain below the navel is addressed by bleeding jing- well points on the feet, and pain above the navel, by bleed-ing those on the hands.
Before bleeding, massage the meridian downwards towards the jing- well point several times. It is best to wet the point area with an ethanol swab, as apart from sanitizing reasons, this expands the blood vessels and aids the bleeding process. Bleeding should be conducted swiftly, piercing with a lancet at a location two to three millimetres away from the corner of the nail. Eight to twelve drops of blood should be drawn (in cases of blood deficiency or post- menstruation this should be reduced to three to four drops). Normally, bleeding is only
performed in the first three or four treatments and substituted with needling with a small nee-dle in later treatments.
Step four: Reassessment of pain/limitation scale – wave effectSince bleeding is the first intervention to be conducted, its effect should be immediately assessed. A major improvement (30 to 60%) indicates that the degree of blood stasis in the meridian is high. This may help to decide how many bleeding sessions will be conducted dur-ing later treatments.
Step five: Wave propagation – oppositional distal needling After bleeding to initiate the meridian Qi wave, the ‘whip’ action of promoting and prop agating the wave is pursued. Points are selected to cre-ate the greatest leverage of meridian Qi. The more distal the points are, the greater ‘wave leverage’ can be achieved. Therefore, needling is conducted in a contralateral manner across the body. Points are selected to include the obstruction area in the wave. This is to say that the obstruction (pain) should be on the meridian between the two points selected. For example, when treating left sided ankle sprain along the foot Shao Yang Gall Bladder (GB) meridian (at Qiuxu GB 40), bleeding is done first at left Zuqiaoyin GB 44, and then needles can be inserted at right Zhongzhu SJ 3 and left Diwuhui GB 42. This will initiate a merid-ian Qi wave that includes the obstruction area near Qiuxu GB 40. In this example, needling left Yanglingquan GB 34 instead of Diwuhui GB 42 would create a shorter wave that would not cover the compromised area. After needle insertion, the best technique is to simultane-ously manipulate both needles (using the right and left hands simultaneously). If this cannot be achieved, then the needle most distal to the painful area is manipulated first, followed immediately by the paired needle.
Step six: Point selection according to meridian obstructionApart from the principle of point selection described above, points may also be selected
Practical applications of meridian theory in pain management – the meridian wave approach
© Journal of Chinese Medicine42
according to degree of sensitivity on palpation. Optimal point selection would involve point categories and functions according to the five shu- transporting or five phase theories. Other points such as xi- cleft points or any other point categories that add clinical value in relation to the nature of the obstruction in the meridian (damp, cold, heat, stasis etc.) may be selected. For example, a swollen right sided tennis elbow along the Yang Ming Large Intestine meridian could be treated by bleeding right Shang yang LI 1, followed by needling right Sanjian LI 3 and left Xiangu ST 43 to propagate the wave. These shu- stream points would further enhance the wave effect by addressing the dampness (swelling) obstructing the meridian.
Step seven: Reassessment of pain/limitation scale – wave effectAs in step four, another assessment is con-ducted. The importance of this principle cannot be over- emphasised. Good results indicate cor-rect meridian and point selection. Poor results, on the other hand, require reanalysis of the meridian and point selection. In addition, any positive change is normally reassuring for both the patient and practitioner.
Step eight: Enhancing wave Qi flow through physical movementTo further enhance the wave Qi flow through the obstructed area, physical movement is added. This is preferably done during needle manipulation. If simultaneous manipulation and movement are not feasible, movement should follow immediately after needle manipulation for wave propagation. If possible, the initial movement that was selected for assessing pain level (step one) is gently repeated during this phase. Movement of the compromised area enhances wave Qi flow and further rejuvenates the surrounding tissues with fresh flow of Qi and blood.
Step nine: Addressing the underlying conditionThe final acupuncture points needled during a treatment session are aimed at balancing
the underlying condition. A thorough intake, including pulse, tongue and meridian assess-ment are the essential tools for accurate dif-ferential diagnosis. As mentioned earlier, adding just one or two points to address the underlying condition according to differential diagnosis can profoundly increase results during treatment, and cumulative success during the treatment series. In fact, in cases of severe deficiency, progress is difficult to achieve without applying this principle.
Summary exampleTo summarize with an example, consider the case of a 42- year- old male with left- sided medial knee pain due to a medial meniscus tear. The pain is fixed, localized and often accompa-nied by a burning sensation. There is no local swelling. The pain is worse in the morning and slightly better after moving around. Other symptoms from the intake as well as pulse and tongue diagnosis indicate Liver Qi stagnation. Following the steps described above, the practi-tioner would first assess and quantify the degree of pain and limitation – in this case by asking the patient to bend the knee (knee flexion) to the point where pain arises. The degree of motion (knee angle) and pain score should be recorded. The second step would involve asking the patient to point to the exact area of discom-fort during the movement – in this case reveal-ing that the obstruction is on the foot Jue Yin Liver meridian. Step three would be to initiate a meridian Qi wave by bleeding left sided Dadun LR 1. Step four would involve reassessing pain and range of motion. Step five would involve wave propagation through opposite hand and foot meridian selection. For this patient this would mean selecting the right hand Jue Yin Pericardium (PC) meridian and the left foot Jue Yin Liver meridian. Step six would involve point selection following the principles of dis-tal needling to propagate a wave that includes the obstruction using points that address the nature of the obstruction. A good combina-tion in this case would thus be right- sided Neiguan PC 6 with left- sided Xingjian LR 2 (a ying- spring point to clear heat). Simultaneous needle stimulation would then be performed.

A. Ziv & I. Levi
© Journal of Chinese Medicine 43
Step seven would involve reassessment. Step eight would involve asking the patient to gently bend the knee several times (without reaching the pain threshold), preferably whilst the points are simultaneously stimulated. Step nine would involve adding one or two points to address the underlying condition. There are many options here, one possibility would be Yanglingquan GB 34 on the opposite side. This point not only treats stagnation in the Liver but also addresses the tissue damage (torn ligament) as it is the
command point of the sinews and tendons. An illustration of this process is outlined in Fig. 3.
referencesEllis A., Wiseman N. & Boss K. (1989) Grasping the
Wind. An Exploration into the Meaning of Chinese Acupuncture Point Names, pp. 375. Paradigm Publications, Brooklyn.
Wang J. Y. & Robertson J. D. (2008) Applied Channel Theory in Chinese Medicine. Eastland Press, Seattle.
Wang J. Y. (1999) Notes from teaching sessions, San Francisco, 1999.
Wang J. Y. (2000) Notes from internship, Beijing, 2000.Ziv A., Yoav M., Guy A., et al (2012) A randomized
controlled trial of an integrative approach utilising acupuncture for back and neck pain in an emergency department setting. European Journal of Integrative Medicine 4 (1), 23–24. A summary of this research was presented by Amos Ziv at the European Conference of Integrative Medicine in Florence (Italy) and at vari-ous orthopaedic conferences in Israel. In addition the study was presented by Dr Samuel Bar- Chaim, head of the Asaf Harofeh Medical Centre Emergency Services, at the MEMC Emergency Medicine conference in Marseille, France.
Amos Ziv MSc LAc is a researcher and an entre-preneur. He is the founder and former director of the clinical research unit of the Shiram Integrated Medicine Services in Asaf Harofeh Medical Center, Israel, where he headed the Acupuncture for Back and Neck Pain in the Emergency Room Clinical Trial (ABNP study). He is a graduate of the American College of TCM, San Francisco, California and an expert in TCM chan-nel theory applications in pain management and cardio-vascular conditions. Amos studied as a personal student of Professor Wang Ju Yi in California and China since 1999. He has published numerous articles in both TCM and scientific journals and is an invited speaker to international conferences. He has taught the meridian wave acupuncture system to hundreds of practitioners in Europe and Israel. Amos was a co- founder and chair-man of SIRF, the Sino- Israeli Research Foundation and is the founder and CEO of ReguRate Advanced Integrative Technologies in Cardiovascular Health. He is the owner and manager of Heaven and Earth TCM specialty clinic in Rehovot, Israel.
Idan Levi is a Chinese medicine practitioner who specialised extensively in meridian theory acupuncture, corrective exercise and lifestyle management. He has
Figure 3: Key steps of meridian wave acupuncture treatment in a left medial meniscus tear along the foot Jue Yin Liver meridian.1. Pain/limitation scale assessment2. Meridian selection 3. Wave initiation – bleed LHS Dadun LR 1 4. Reassessment 5. Wave initiation – point selection6. Point stimulation – RHS Neiguan PC 6 and LHS Xingjian LR 27. Reassessment 8. Knee movement 9. Addressing the underlying condition – RHS Yanglingquan GB 34LR=Liver; PC=Pericardium; GB=Gall Bladder; LHS=left hand side; RHS=right hand side

Practical applications of meridian theory in pain management – the meridian wave approach
© Journal of Chinese Medicine44
studied meridian wave acupuncture system with Amos Ziv and worked with him since 2009, and has served as an assistant teacher. He has presented his work and techniques in leading TCM conferences. Idan has gained vast clinical experience in leading physical therapy clinics in Israel and is currently the Head of the Chronic Pain and Orthopaedic Injury Department at Heaven and Earth TCM specialty clinic in Rehovot, Israel, and the Head of the Chinese Acupuncture unit at MedLeader Physiotherapy clinic in Raanana.
This article is reprinted with kind permission from the Journal of Chinese Medicine. Original publication: Ziv A. & Levi I. (2017) Practical applications of meridian theory in pain management – the meridian wave approach. Journal of Chinese Medicine (115), 5–12.
© 2016 Medical Association of Pharmacopuncture Institute 45
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 45–53
rESEArCh
Types of control in acupuncture clinical trials might affect the conclusion of the trials: a review of acupuncture on pain management
h. Chen School of Chinese Medicine, University of Hong Kong, Hong Kong, China and Department of Chinese Medicine, University of Hong Kong- Shenzhen Hospital, Shenzhen, China
Z. NingSchool of Chinese Medicine, University of Hong Kong, Hong Kong, China
w. l. lam School of Chinese Medicine, University of Hong Kong, Hong Kong, China
w.- Y. lam School of Chinese Medicine, University of Hong Kong, Hong Kong, China
Y. K. Zhao School of Chinese Medicine, University of Hong Kong, Hong Kong, China
J. w. F. Yeung School of Nursing, Hong Kong Polytechnic University, Hong Kong, China
B. F.- l. Ng Chinese Medicine Department, Hospital Authority, Hong Kong, China
E. T.- C. Ziea Chinese Medicine Department, Hospital Authority, Hong Kong, China
l. laoSchool of Chinese Medicine, University of Hong Kong, Hong Kong, China and Department of Chinese Medicine, University of Hong Kong- Shenzhen Hospital, Shenzhen, China
AbstractAnalgesic effects of acupuncture have been extensively studied in various clinical trials. However, the conclusion remains controversial, even among large scale randomized con-trolled trials. This study aimed to evaluate the association between the conclusion of the tri-als and the types of control used in those trials via systematic review. Published randomized controlled trials (RCTs) of acupuncture for pain were retrieved from electronic databases (Medline, AMED, Cochrane Libraries, EMBASE, PsycINFO, Clinicaltrials.gov, and CAB Abstracts) using a pre- specified search strategy. One hundred and thirty- nine studies leading to 166 pairs of acupuncture- control treatment effect comparisons (26 studies comprised of 53 intervention- control pairs) were analyzed based on the proportion of positive conclusions

A review of acupuncture on pain management
© 2016 Medical Association of Pharmacopuncture Institute46
in different control designs. We found that treatment effects of acupuncture compared with nontreatment controls had the highest tendency to yield a positive conclusion (84.3%), com-pared with nonneedle- insertion controls (53.3%). Whereas with needle- insertion controls, the lowest tendency of positive conclusions was observed (37.8%). Consistently, in studies reporting successful blinding, a higher tendency of positive findings on the treatment effect of acupuncture was found in the noninsertion sham controls compared with that in the insertion sham controls. We conclude that the type of control is likely to affect the conclu-sion in acupuncture analgesic trials. Appropriate control should be chosen according to the aims of studies.
Keywords: acupuncture, control, pain, randomized controlled trial.
IntroductionThe number of randomized controlled trials (RCTs) conducted on acupuncture have dra-matically increased over the past decade. The efficacy of acupuncture for pain is one of the most interesting outcomes in studies. Although many basic science studies have revealed the analgesia mechanisms of acupuncture (Lin & Chen 2008; Zhang et al. 2014), the effi-cacy of acupuncture remains controversial in clinical trials, e.g., in knee osteoarthritis (KOA) (Berman et al. 2004; Witt et al. 2005; Scharf et al. 2006; Witt et al. 2006; Lin & Chen 2008; Mavrommatis et al. 2012; Hinman et al. 2014; Zhang et al. 2014). The diverse mechanisms and complicated manual procedures involved in acupuncture treatment have contributed to the challenges of evaluating acupuncture trials (Chen & Lao 2014). For example, acupuncture produces a specific physiological effect and nonspecific needling effect (e.g., diffuse noxious inhibitory control) during the treatment (Le Bars et al. 1991). Patient expectations, acu-puncturist experience, number and specificity of acupoints, depth of needling, and dosage of acupuncture (duration, frequency and time) also affect the efficacy of acupuncture analgesia in RCTs (White et al. 2001). The benefits dur-ing the treatment are usually explained by: (1) treatment effects; (2) nonspecific effects; or (3) spontaneous remissions (Turner et al. 1994; Lao et al. 2001). A proper control or controls, e.g., waitlist, non- insertion sham acupuncture,
and insertion sham acupuncture, are utilized to evaluate the true effects in RCTs (Chen & Lao 2014). Arguments have been raised on the efficacy of acupuncture controls (Goddard et al. 2005; Irnich et al. 2011; Lee et al. 2011). Meng et al. (2011) reviewed acupuncture RCTs on pain published in 2006 to 2007 and found that trials using noninsertion shams yielded more positive outcomes (six of seven trials) than those using insertion shams (two of eight trials). Madsen et al. (2009) found that the type of placebo acu-puncture was not associated with the estimated analgesic effect of acupuncture. In this study, we aimed to examine whether positive conclusion is correlated with the type of controls in RCTs of acupuncture for pain. We systematically reviewed clinical trials of acupuncture for pain from 2004 to 2014. The association between the type of controls used in these studies and conclusion of acupuncture efficacy were further analyzed.
Materials and methods DatabaseA systematic search of RCTs with acupuncture was conducted to evaluate the proportion of positive conclusions in the different controls in RCTs. The search strategy was defined as below. Databases searched included Medline, AMED, Cochrane Libraries, EMBASE, PsycINFO, Clinicaltrials.gov, and CAB Abstracts.
Search strategyThe search keywords were as follows: “acupuncture*”, “acupoint*”, “acupress*”, “meridian*”, “needle*”, “sham acupuncture”,
Correspondence: L. Lao, School of Chinese Medicine, University of Hong Kong, 10 Sassoon Road, Pokfulam, Hong Kong, China. (email: [email protected]).

H. Chen et al.
© 2016 Medical Association of Pharmacopuncture Institute 47
“placebo acupuncture”, “control acupuncture”, “acupuncture control”, and “pain”. Studies were limited to RCTs and journals in Science Citation Index (SCI). The search was conducted in March 2015.
ScreeningThe retrieved studies were imported into Endnote and any duplicates were removed. The abstracts of the studies were screened, followed by full- text screening according to the selection criteria below. The screening was performed by two individuals. Discrepancies were resolved by discussion with a third reviewer. Information on the type of controls and acupuncture efficacy conclusion from eligible studies were extracted according to the definition of outcomes.
Selection criteria1. Inclusion criteriaStudies: (1) were RCTs; (2) used pain score as an outcome; (3) used needling acupuncture (tra-ditional acupuncture, electro- acupuncture, and medical acupuncture) as the major intervention (not restricted to auricular acupuncture and scalp acupuncture as the secondary intervention); and (4) were published from 2004 to 2014.
2. Exclusion criteriaStudies: (1) used bee venom acupuncture as the intervention; (2) used acupoint injection as the intervention; (3) of poor quality design (unclear randomization method, incorrect concealment, and individual assessment), with low risk items less than five of seven (according to risk bias assessment tool in Cochrane review handbook); and (4) used active treatment of any acupunc-ture modalities (e.g., active acupuncture, auricu-lar acupuncture, etc.) as control(s).
Outcomes1. Type of acupuncture controlsWe classified acupuncture controls into several types according to the purpose of controls: (1) “nontreatment” control: patients usually received nontreatment, delayed treatment (waiting list), usual care, or/and rescue medication in consid-eration of medical ethics; (2) noninsertion sham: these do not penetrate the skin, but usually use
the blunt end of the acupuncture needles, non-insertion sham devices (e.g., Streitberger or Park sham devices), and other needle- resembling devices such as toothpicks and needling guid-ing tubes; (3) insertion sham: usually involves a superficial insertion of needles to acupoints or nonacupoints; (4) combined noninsertion and insertion sham; and (5) comparator (positive control): refers to active treatments, such as specific mediations and physiotherapies, some usual care, or standardized care, etc., which were thought to be effective.
Usual care refers to standardized patient care practices that have not been validated by rigorous clinical evidence, or uniform practices that have not been identified as the “best current therapy” in clinical practices while the individual-ized cares are available (Thompson et al. 2007). The role of usual care remains controversial (Thompson et al. 2007; Freedland et al. 2011). In pain trials, usual care commonly refers to standardized management that is not sufficient to kill pain but is routinely provided to patients (Thompson et al. 2007; Freedland et al. 2011). In this study, if both arms of intervention and control used usual care, we classified the type of control into no treatment control. Also participants in no treatment or waitlist control group have access to nonstudy healthcare services (Silverman & Miller 2004). There are other study designs where usual care serves as the comparator, and is only used in the control arm but not the intervention arm. In that case, we classified usual care as a positive control or comparator.
If a study contained two or more controls, information on each acupuncture- control comparison pair was extracted according to the control types.
2. Type of conclusions in clinical trialsPositive conclusion was defined as acupuncture showing statistically significant superiority to the control (p < 0.05) in the primary outcome of clinical studies. If no primary outcome was stated in the studies, the general conclusion of the study was judged as a positive conclusion when it indicated acupuncture was better than the control.
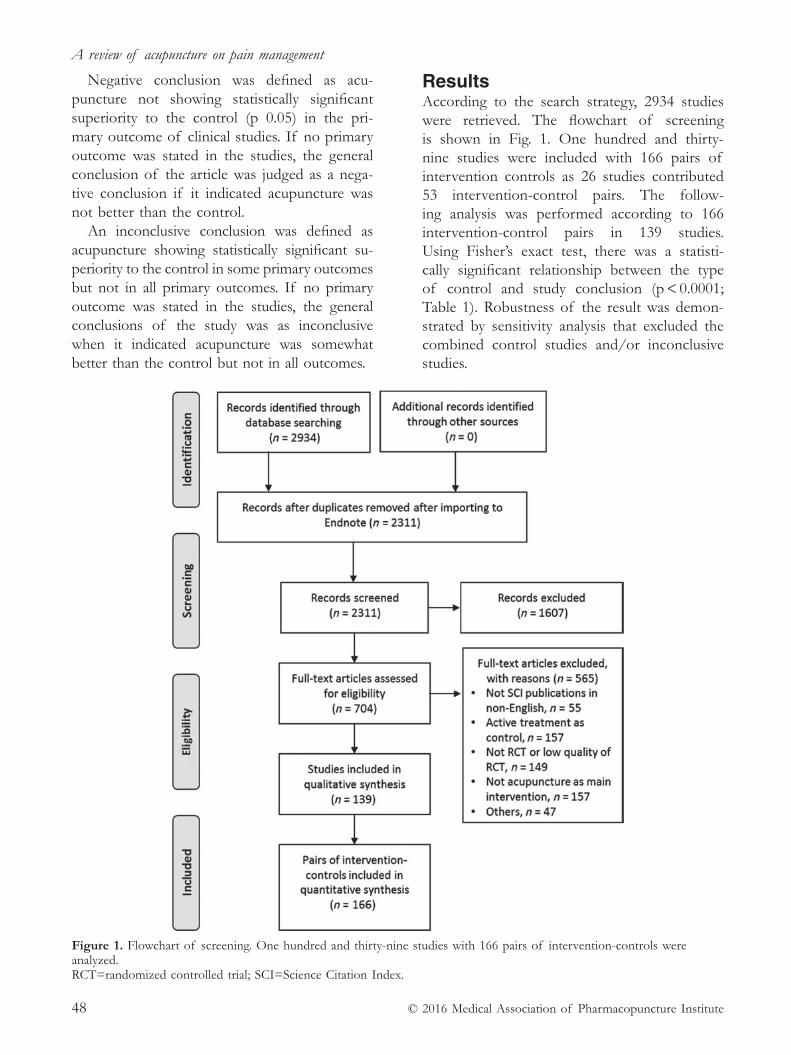
A review of acupuncture on pain management
© 2016 Medical Association of Pharmacopuncture Institute48
Negative conclusion was defined as acu-puncture not showing statistically significant superiority to the control (p 0.05) in the pri-mary outcome of clinical studies. If no primary outcome was stated in the studies, the general conclusion of the article was judged as a nega-tive conclusion if it indicated acupuncture was not better than the control.
An inconclusive conclusion was defined as acupuncture showing statistically significant su - periority to the control in some primary outcomes but not in all primary outcomes. If no primary outcome was stated in the studies, the general conclusions of the study was as inconclusive when it indicated acupuncture was somewhat better than the control but not in all outcomes.
resultsAccording to the search strategy, 2934 studies were retrieved. The flowchart of screening is shown in Fig. 1. One hundred and thirty- nine studies were included with 166 pairs of intervention controls as 26 studies contributed 53 intervention- control pairs. The follow-ing analysis was performed according to 166 intervention- control pairs in 139 studies. Using Fisher’s exact test, there was a statisti-cally significant relationship between the type of control and study conclusion (p < 0.0001; Table 1). Robustness of the result was demon-strated by sensitivity analysis that excluded the combined control studies and/or inconclusive studies.
Figure 1. Flowchart of screening. One hundred and thirty- nine studies with 166 pairs of intervention- controls were analyzed. RCT=randomized controlled trial; SCI=Science Citation Index.
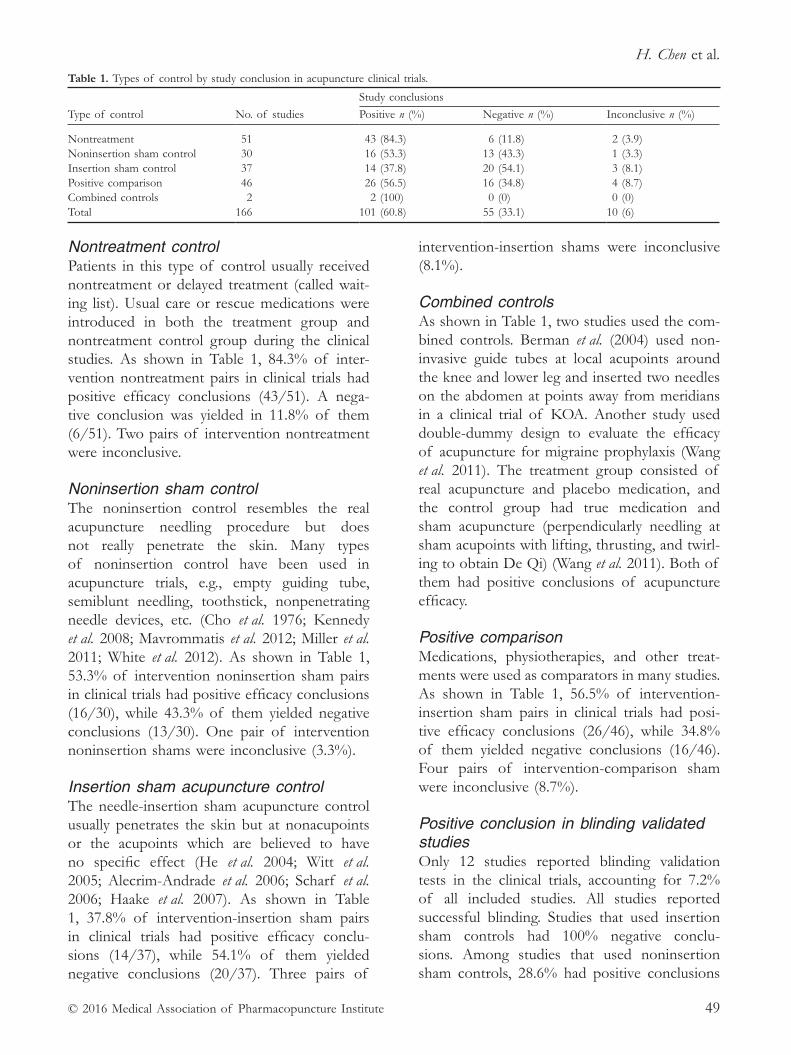
H. Chen et al.
© 2016 Medical Association of Pharmacopuncture Institute 49
Nontreatment controlPatients in this type of control usually received nontreatment or delayed treatment (called wait-ing list). Usual care or rescue medications were introduced in both the treatment group and nontreatment control group during the clinical studies. As shown in Table 1, 84.3% of inter-vention nontreatment pairs in clinical trials had positive efficacy conclusions (43/51). A nega-tive conclusion was yielded in 11.8% of them (6/51). Two pairs of intervention nontreatment were inconclusive.
Noninsertion sham controlThe noninsertion control resembles the real acupuncture needling procedure but does not really penetrate the skin. Many types of noninsertion control have been used in acupuncture trials, e.g., empty guiding tube, semiblunt needling, toothstick, nonpenetrating needle devices, etc. (Cho et al. 1976; Kennedy et al. 2008; Mavrommatis et al. 2012; Miller et al. 2011; White et al. 2012). As shown in Table 1, 53.3% of intervention noninsertion sham pairs in clinical trials had positive efficacy conclusions (16/30), while 43.3% of them yielded negative conclusions (13/30). One pair of intervention noninsertion shams were inconclusive (3.3%).
Insertion sham acupuncture controlThe needle- insertion sham acupuncture control usually penetrates the skin but at nonacupoints or the acupoints which are believed to have no specific effect (He et al. 2004; Witt et al. 2005; Alecrim- Andrade et al. 2006; Scharf et al. 2006; Haake et al. 2007). As shown in Table 1, 37.8% of intervention- insertion sham pairs in clinical trials had positive efficacy conclu-sions (14/37), while 54.1% of them yielded negative conclusions (20/37). Three pairs of
intervention- insertion shams were inconclusive (8.1%).
Combined controlsAs shown in Table 1, two studies used the com-bined controls. Berman et al. (2004) used non-invasive guide tubes at local acupoints around the knee and lower leg and inserted two needles on the abdomen at points away from meridians in a clinical trial of KOA. Another study used double- dummy design to evaluate the efficacy of acupuncture for migraine prophylaxis (Wang et al. 2011). The treatment group consisted of real acupuncture and placebo medication, and the control group had true medication and sham acupuncture (perpendicularly needling at sham acupoints with lifting, thrusting, and twirl-ing to obtain De Qi) (Wang et al. 2011). Both of them had positive conclusions of acupuncture efficacy.
Positive comparisonMedications, physiotherapies, and other treat-ments were used as comparators in many studies. As shown in Table 1, 56.5% of intervention- insertion sham pairs in clinical trials had posi-tive efficacy conclusions (26/46), while 34.8% of them yielded negative conclusions (16/46). Four pairs of intervention- comparison sham were inconclusive (8.7%).
Positive conclusion in blinding validated studiesOnly 12 studies reported blinding validation tests in the clinical trials, accounting for 7.2% of all included studies. All studies reported successful blinding. Studies that used insertion sham controls had 100% negative conclu-sions. Among studies that used noninsertion sham controls, 28.6% had positive conclusions
Table 1. Types of control by study conclusion in acupuncture clinical trials.
Type of control No. of studies
Study conclusions
Positive n (%) Negative n (%) Inconclusive n (%)
Nontreatment 51 43 (84.3) 6 (11.8) 2 (3.9)Noninsertion sham control 30 16 (53.3) 13 (43.3) 1 (3.3)Insertion sham control 37 14 (37.8) 20 (54.1) 3 (8.1)Positive comparison 46 26 (56.5) 16 (34.8) 4 (8.7)Combined controls 2 2 (100) 0 (0) 0 (0)Total 166 101 (60.8) 55 (33.1) 10 (6)

A review of acupuncture on pain management
© 2016 Medical Association of Pharmacopuncture Institute50
and 57.1% had negative conclusions (Table 2). However, the relationship between study control type and study conclusion in these studies was not significant (Fisher’s exact test, p = 0.47).
DiscussionIn this study, we systematically reviewed RCTs that studied the efficacy of acupuncture for pain. Potential association between the conclu-sions of acupuncture efficacy and the types of controls was analyzed. We found that studies had the highest tendency to yield positive con-clusions (84.3%) when nontreatment controls were used, compared with a lower tendency (53.3%) observed in the noninsertion controls, and lowest tendency (37.8%) in the insertion controls. Consistently, in studies reporting suc-cessful blinding, a higher tendency of positive conclusion was found in non- insertion sham controls compared with that in insertion sham controls.
In clinical practice, acupuncture analgesia may be explained by various effects, such as the specific therapeutic effect, nonspecific physiol-ogy effect, placebo effect, or disease spontane-ous remission. These effects are commonly distinguished by adopting specific controls or are excluded by appropriate trial design step by step.
The nontreatment control determines whether the disease has spontaneous remis-sion. It had the highest positive conclusion of acupuncture efficacy and the cost is lower than RCTs using other controls such as sham control. It is more feasible to conduct a clinical trial using nontreatment control compared with using other types of controls. With this advan-tage, nontreatment control is recommended to establish the adequate dose of acupuncture (e.g., number of acupoints, frequency, and
duration of acupuncture), optimize the duration of treatment, select proper measurements and measurement time points, or examine the safety in a pilot study or at the early stage of develop-ing a certain acupuncture treatment.
However, patients assigned to receive non-treatment usually prefer to get real treatment. Their feeling worse in the disease condition for not having the opportunity to receive the real treatment is called nocebo effect (Enck et al. 2008). The nocebo effect is regarded as negative placebo effect which has been raised from expectation and psychological condition-ing (Enck et al. 2008). Wait list control offers patients the same treatment as the treatment group after the patient completes treatment so that nocebo effect is minimized as much as possible. In fact, few studies restrict patients to take medications or other therapies if patients really need treatments. Taking into considera-tion the ethical issue and nocebo effect, usual care, medical education, or rescue medications are used as the “nontreatment” control (Cherkin et al. 2001; Cherkin et al. 2009).
Studies using the noninsertion controls have a higher tendency of positive conclusion com-pared with those using needle insertion controls in acupuncture for pain studies. It could be explained that needle insertion controls may produce more nonspecific physiological effects, e.g., the diffuse noxious inhibitory controls (Le Bars et al. 1991). The difference in pain scale between acupuncture treatment groups and nee-dle insertion controls is likely to be smaller than studies using noninsertion controls. However, noninsertion controls may reduce the success of blinding as patients with acupuncture experience are more likely to identify the sham treatment, which lowers patient expectancy and attendance. The noninsertion sham controls can be used for the short- term trials, e.g., acute pain study, or trials recruiting acupuncture naïve patients.
Table 2. Conclusions of studies with blinding credibility.
Type of control No. of studies
Study conclusions
Positive n (%) Negative n (%) Inconclusive n (%)
Noninsertion sham control 7 2 (28.6) 4 (57.1) 1 (14.3)Insertion sham control 5 0 (0) 5 (100) 0 (0)Total 12 2 (16.7) 9 (75) 1 (8.3)

H. Chen et al.
© 2016 Medical Association of Pharmacopuncture Institute 51
Insertion sham controls are more similar to real acupuncture. In the reviewed studies, most of the studies used superficial needling, and needle points were selected out of the meridians, distal acupoints, or acupoints with no effects (He et al. 2004; Linde et al. 2005; Witt et al. 2005; Alecrim- Andrade et al. 2006; Scharf et al. 2006; Haake et al. 2007; Molsberger et al. 2010). Needle manipulation should not be applied to partly reduce the nonspecific effect of insertion sham. However, this superficial, distal needling may also produce similar effects to real acupuncture. For example, Vas et al. (2012) used both needle insertion sham to study point specificity and noninsertion to control acupuncture technique. They found that all three treatments – real acupuncture, insertion sham and noninsertion sham – had better effects than conventional treatment, and there was no significant differ-ence among the three treatments (Vas et al. 2012). To achieve the advantages of both inser-tion and non- insertion sham controls, Berman et al. (2004) applied a combined control in a KOA trial. The acupuncture treatment consisted of real needling at five local points, four distal points, and tapping plastic guiding tube at two sham points (noninsertion sham control) at the abdomen, and the sham control consisted of inserting two needles at sham points (insertion sham control) and tapping at nine real points (noninsertion placebo control) (Lao et al. 2001; Berman et al. 2004).
The masking effectiveness or the blinding credibility should be measured for both real acupuncture and sham acupuncture treatments. Only 7.2% of studies assessed blinding success. No study with blinding credibility assessed indicated unsuccessful blinding. In the KOA study, the combined control produced accept-able masking effects (Berman et al. 2004), 25% and 33% of the patients were unsure of their assignment in the real acupuncture or sham acu-puncture group, and 67% and 58% believed that they were receiving true acupuncture (p = 0.06), respectively. In addition to the combined con-trol, to avoid the nonspecific effect of needling, the number of needling should be minimized.
In some studies, treatments with positive effects, such as conventional medications
or other active treatments (physiotherapies, radiotherapies, and chemotherapies, etc.) were introduced as the comparators, rather than controls, for acupuncture treatment. These comparators serve as “positive controls” so that the effectiveness of acupuncture can be meas-ured. The proportion of positive conclusions in such studies was 56.5%. It could be varied with the strength of therapeutic effects of the com-parator. If researchers choose strong positive comparators for acupuncture treatment, there would be less positive conclusions in the study. A double dummy design for acupuncture and comparator could enhance the blinding effect in clinical trials, e.g., introduce placebo medication in acupuncture and sham acupuncture in com-parison groups (Wang et al. 2011).
There are limitations in this study. Firstly, we only studied the association between the control type and study outcome. Although we had excluded the potential influence from the methodological quality, a few factors might affect the study outcome, e.g., the dose of acupuncture intervention, the severity of disease, the experience of acupuncturists, the effectiveness of controls, the success of blind-ing, etc. The potential effects should be fully considered in the clinical trial design. Secondly, as pain is a very common symptom, it mani-fests in various diseases. The search strategy we used in the study might not have retrieved all acupuncture clinical trials which were related to pain management. In the retrieved studies, pain was the major complaint. The findings from these studies should mainly reflect the trend of association in control type and study outcome. Lastly, given the difficulties to obtain the full text of many non- SCI publications, we limited the search in SCI publications. The restric-tion of studies in SCI publications may lead to bias.
Selection of controls in acupuncture trials is likely to affect the study conclusion. Studies using nontreatment controls have the highest tendency of positive conclusions, followed by noninsertion controls, and the lowest tendency in insertion sham controls. To improve the quality of acupuncture trials, the control needs to be appropriately selected.

A review of acupuncture on pain management
© 2016 Medical Association of Pharmacopuncture Institute52
Disclosure statementThe authors declare that they have no conflicts of interest and no financial interests related to the material of this manuscript.
AcknowledgementsThis project was supported by Hospital Authority, Hong Kong (HA105/48P T18).
referencesAlecrim- Andrade J., Maciel- Junior J. A., Cladellas X. C.,
et al. (2006) Acupuncture in migraine prophylaxis: a randomized sham- controlled trial. Cephalalgia 26 (5), 520–529.
Berman B. M., Lao L., Langenberg P., et al. (2004) Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Annals of Internal Medicine 141 (12), 901–910.
Chen H. Y. & Lao L. (2014) Challenges in evaluating acupuncture trials. In: Acupuncture in pain management (ed. C. Lucy), pp. 163–172. Nova Science Publishers, Hauppauge.
Cherkin D. C., Eisenberg D., Sherman K. J., et al. (2001) Randomized trial comparing traditional Chinese medi-cal acupuncture, therapeutic massage, and self- care education for chronic low back pain. Archives of Internal Medicine 161 (8), 1081–1088.
Cherkin D. C., Sherman K. J., Avins A. L., et al. (2009) A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Archives of Internal Medicine 169 (9), 858–866.
Cho Y. J., Song Y. K., Cha Y. Y., et al. (2013) Acupuncture for chronic low back pain: a multicenter, randomized, patient- assessor blind, sham- controlled clinical trial. Spine (Phila Pa 1976) 38 (7), 549–557.
Enck P., Benedetti F. & Schedlowski M. (2008) New insights into the placebo and nocebo responses. Neuron 59 (2), 195–206.
Freedland K. E., Mohr D. C., Davidson K. W. & Schwartz J. E. (2011) Usual and unusual care: existing practice control groups in randomized controlled trials of behavioral interventions. Psychosomatic Medicine 73 (4), 323–335.
Goddard G., Shen Y. S., Steele B. & Springer N (2005). A controlled trial of placebo versus real acupuncture. Journal of Pain 6 (4), 237–242.
Haake M., Muller H. H., Schade- Brittinger C., et al. (2007) German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel- group trial with 3 groups. Archives of Internal Medicine 167 (17), 1892–1898.
He D., Veiersted K. B., Høstmark A. T. & Medbø J. I. (2004) Effect of acupuncture treatment on chronic
neck and shoulder pain in sedentary female workers: a 6- month and 3- year follow- up study. Pain 109 (3), 299–307.
Hinman R. S., McCrory P., Pirotta M., et al. (2014) Acupuncture for chronic knee pain: a randomized clinical trial. JAMA 312 (13), 1313–1322.
Irnich D., Salih N., Offenbacher M. & Fleckenstein J. (2011) Is sham laser a valid control for acupuncture tri-als? Evidence- Based Complementary and Alternative Medicine Article ID: 485945.
Kennedy S., Baxter G. D., Kerr D. P., et al. (2008) Acupuncture for acute non- specific low back pain: a pilot randomised non- penetrating sham controlled trial. Complementary Therapies in Medicine 16 (3), 139–146.
Lao L., Ezzo J., Berman B. & Hammerschlag R. (2001) Assessing clinical efficacy of acupuncture: considera-tions for designing future acupuncture trials. In: Clinical acupuncture, pp. 187–209. Springer, Berlin.
Le Bars D., Villanueva L., Willer J. & Bouhassira D. (1991) Diffuse noxious inhibitory controls (DNIC) in animals and in man. Acupuncture in Medicine 9 (2), 47–56.
Lee H., Bang H., Kim Y. et al. (2011) Non- penetrating sham needle, is it an adequate sham control in acu-puncture research? Complementary Therapies in Medicine 19 (Suppl. 1), S41- S48.
Lin J. G. & Chen W. L. (2008) Acupuncture analgesia: a review of its mechanisms of actions. American Journal of Chinese Medicine 36 (4), 635–645.
Linde K., Streng A., Jurgens S., et al. (2005) Acupuncture for patients with migraine: a randomized controlled trial. JAMA 293 (17), 2118–2125.
Madsen M. V., Gøtzsche P. C. & Hróbjartsson A. (2009) Acupuncture treatment for pain: systematic review of randomized clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ 338, a3115.
Mavrommatis C. I., Argyra E., Vadalouka A. & Vasilakos D. G. (2012) Acupuncture as an adjunctive therapy to pharmacological treatment in patients with chronic pain due to osteoarthritis of the knee: a 3- armed, random-ized, placebo- controlled trial. Pain 153 (8), 1720–1726.
Meng X., Xu S. & Lao L. (2011) Clinical acupuncture research in the West. Frontiers of Medicine 5 (2), 134–140.
Miller E., Maimon Y., Rosenblatt Y. et al. (2011) Delayed effect of acupuncture treatment in OA of the knee: a blinded, randomized, controlled trial. Evidence- Based Complementary and Alternative Medicine Article ID: 792975.
Molsberger A. F., Schneider T., Gotthardt H. & Drabik A. (2010) German Randomized Acupuncture Trial for chronic shoulder pain (GRASP) – a pragmatic, controlled, patient- blinded, multi- centre trial in an outpatient care environment. Pain 151 (1), 146–154.
Scharf H. P., Mansmann U., Streitberger K., et al. (2006) Acupuncture and knee osteoarthritis: a three- armed randomized trial. Annals of Internal Medicine 145 (1), 12–20.

H. Chen et al.
© 2016 Medical Association of Pharmacopuncture Institute 53
Silverman H. J. & Miller F. G. (2004) Control group selection in critical care randomized controlled trials evaluating interventional strategies: an ethical assess-ment. Critical Care Medicine 32 (3), 852–857.
Thompson B. T. & Schoenfeld D. (2007) Usual care as the control group in clinical trials of nonpharmaco-logic interventions. Proceedings of the American Thoracic Society 4 (7), 577–582.
Turner J. A., Deyo R. A., Loeser J. D., et al. (1994) The importance of placebo effects in pain treatment and research. JAMA 271 (20), 1609–1614.
Vas J., Aranda J. M., Modesto M., et al. (2012) Acupuncture in patients with acute low back pain: a multicentre randomised controlled clinical trial. Pain 153 (9), 1883–1889.
Wang L. P., Zhang X. Z., Guo J., et al. (2011) Efficacy of acupuncture for migraine prophylaxis: a single- blinded, double- dummy, randomized controlled trial. Pain 152 (8), 1864–1871.
White A. R., Filshie J. & Cummings T. M. (2001) International Acupuncture Research Forum. Clinical trials of acupuncture: consensus recommendations for optimal treatment, sham controls and blinding. Complementary Therapies in Medicine 9 (4), 237–245.
White P., Bishop F. L., Prescott P., et al. (2012) Practice, practitioner, or placebo? A multifactorial, mixed- methods randomized controlled trial of acupuncture. Pain 153 (2), 455–462.
Witt C., Brinkhaus B., Jena S., et al. (2005) Acupuncture in patients with osteoarthritis of the knee: a randomized trial. Lancet 366 (9480), 136–143.
Witt C. M., Jena S., Brinkhaus B., et al. (2006) Acupuncture in patients with osteoarthritis of the knee or hip: a randomized, controlled trial with an additional non-randomized arm. Arthritis and Rheumatism 54 (11), 3485–3493.
Zhang R., Lao L., Ren K. & Berman B. M. (2014) Mechanisms of acupuncture- electroacupuncture on persistent pain. Anesthesiology 120 (2), 482–503.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/licenses/by- nc/4.0) which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published in the Journal of Acupuncture and Meridian Studies. Original publi-cation: Chen H., Ning Z., Lam W. L., et al. (2016) Types of control in acupuncture clinical trials might affect the conclusion of the trials: a review of acupunc-ture on pain management. Journal of Acupuncture and Meridian Studies, 9 (5), 227–233. https://www.science direct.com/science/article/pii/S2005290116301492


© 2018 Frontiers in Psychiatry 55
Correspondence: Younbyoung Chae, Department of Anatomy and Meridians, College of Korean Medicine, Gachon University, Seongnam, South Korea (email: [email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 55–66
rESEArCh
how placebo needles differ from placebo pills
Y. ChaeDepartment of Anatomy and Meridians, College of Korean Medicine, Gachon University, Seongnam, South Korea
Y.- S. leeDepartment of Anatomy and Meridians, College of Korean Medicine, Gachon University, Seongnam, South Korea
P. EnckDepartment of Internal Medicine, Psychosomatic Medicine and Psychotherapy, University of Tübingen, Tübingen, Germany
AbstractBecause acupuncture treatment is defined by the process of needles penetrating the body, placebo needles were originally developed with non- penetrating mechanisms. However, whether placebo needles are valid controls in acupuncture research is the subject of an ongoing debate. The present review provides an overview of the characteristics of placebo needles and how they differ from placebo pills in two aspects: (1) physiological response and (2) blinding efficacy. We argue that placebo needles elicit physiological responses similar to real acupuncture and therefore provide similar clinical efficacy. We also demonstrate that this efficacy is further supported by ineffective blinding (even in acupuncture- naïve patients) which may lead to opposite guesses that will further enhance efficacy, as compared to no- treatment, e.g., with waiting list controls. Additionally, the manner in which placebo needles can exhibit therapeutic effects relative to placebo pills include enhanced touch sensations, direct stimulation of the somatosensory system and activation of multiple brain systems. We finally discuss alternative control strategies for the placebo effects in acupuncture therapy.
Keywords: acupuncture, blinding, control, physiology, placebo.
IntroductionAcupuncture is a therapeutic intervention per-formed by “inserting one or more needles into specific sites on the body surface for therapeutic purposes” (Liu 2009). Placebo needles were developed and validated to evaluate the efficacy of acupunc-ture treatment in randomized controlled clinical
trials (RCTs) (Streitberger & Kleinhenz 1998; Park et al. 2002). Due to the indistinguishably inert nature of placebo controls compared with active treatments, placebo- controlled studies enable determination of the therapeutic effects of target treatments from unspecific treatment effects, such as medical context and consequent expectation. Similarly, placebo needles must be indistinguishable from real acupuncture needles and not produce any physiological therapeutic effects. To achieve this, non- penetrating needles with a similar appearance to real acupuncture

How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry56
needles, which retract telescopically into the needle handle when pressed on the skin, were developed because they provide patients with the visual illusion that their skin is being pen-etrated, much like a stage dagger in theatre performances.
Non- penetrating needles have been com-monly used as placebo controls for acupunc-ture research over several decades (Dincer & Linde 2003), and are often seen as standard when investigating the mechanisms under-lying the acupuncture effects (Hu et al. 2017). Interestingly, several studies have shown that the effectiveness of placebo acupuncture needles is similar to that of real acupuncture needles. A systematic review of clinical trials revealed only a small difference between real and placebo needles in terms of pain relief, whereas a mod-erate difference was found between placebo treatment and no treatment at all, e.g., during a waiting period (Madsen et al. 2009). RCTs have shown that real and placebo acupuncture treatments are equally effective and that both are superior to “treatments as usual” (TAU) for chronic pain (Schneider et al. 2006; Cherkin et al. 2009). Taken together, these findings imply that acupuncture treatment is equally effective as placebo acupuncture and therefore, that acu-puncture treatment effects are placebo effects (Solomon 2017). However, the adequacy of the controls being used in these studies remains to be determined (Enck et al. 2010). Many discussions of whether placebo needles are appropriate controls for acupuncture research have followed the development of these needles (Langevin et al. 2006), and there has been some criticism from a physiological perspective that placebo needles may not be proper controls for acupuncture studies (Lundeberg et al. 2008). In fact, placebo needles are neither fully indistin-guishable from regular needles nor physiologi-cally inert (Chae et al. 2011; Kang et al. 2011). Similarly, a recent meta- analysis suggested that neither the Streitberger device nor the Park Sham device is adequate inert controls for clini-cal studies (Zhang et al. 2015).
This issue pertains not only to acupuncture needles, but also to other treatment devices that involve physical contact with the patient, such as
injections, transcutaneous electrical nerve stimu-lation, manual therapy, and surgical interventions. Placebo devices, including placebo injections and placebo acupuncture needles, exhibit stronger effects than do oral placebo pills (Kaptchuk et al. 2000). Similarly, a meta- analysis showed that subcutaneous placebo administrations pro-duce greater effects than do oral placebos for the acute treatment of migraine (De Craen et al. 2000). A more recent meta- analysis of the effects of placebo interventions across all clinical con-ditions showed that physical placebo interven-tions, including acupuncture, have greater effects than do pill controls (Hróbjartsson & Gøtzsche 2010); sham acupuncture has been shown to have even greater effects than other physical pla-cebos (Linde et al. 2010). A clinical trial revealed that placebo needles have greater effects than placebo pills on self- reported pain and severity of symptoms in patients with persistent arm pain (Kaptchuk et al. 2006). Expectations on the potential benefit induced in the recipient, influenced by the magnitude of the invasiveness of the intervention, leads to therapeutic effects following a placebo treatment (Weimer & Enck 2014). The greater effect of placebo devices compared with placebo pills may be due to the additional physical contact or the tactile com-ponent of the intervention, which is minimally present with the use of pharmaceutical pills. Therefore, the contextual effects associated with the preparation of acupuncture treatment devices are multisensory and have a broader impact on the patient. The tactile context of treatment devices such as during acupuncture is essential for the establishment of therapeutic effects (Chae & Olausson 2017). In contrast to the use of oral placebo pills, this context has two components: physiological action and inef-fective blinding, which initially takes effect once the treatment is applied, and which, therefore, is different from the gradual unblinding due to experiences of adverse events during the drug applications.
Thus, the purpose of the present article was to review the two components of placebo devices, physiological action and effective blind-ing, and to discuss how these features result in stronger placebo effects relative to oral pills.

Y. Chae et al.
© 2018 Frontiers in Psychiatry 57
Physiological actions of placebo needlesThe “specific” effect of placebo needles due to tactile stimulation Pharmaceutical research involving a placebo requires a verum preparation with a specific drug and a placebo preparation without that drug, with the difference in the effects of these two preparations indicating the effectiveness of the target drug. The aims of this type of study design are to exclude any other possible factor that might influence the general effects of medical treatment, such as natural history, regression to the mean, and/or methodological biases, and to test the “true” therapeutic effects of the novel compound (Enck et al. 2013). Additionally, the non- specific effects of the treatment can be observed by comparing the response with placebo to a no- treatment con-trol condition, e.g., a waiting list; these effects are caused by the treatment preparation itself within a medical context, i.e., the attention the patient receives. The context provided by the medical setting may be referred to as the “specific” effect of the placebo (Wager & Atlas 2015). In fact, placebo effects are regarded as brain–body responses to contextual information that promote health and well- being (Wager & Atlas 2015).
In the case of placebo needles, tactile stimu-lation is an additional component that is associ-ated with the treatment context of acupuncture, which is absent in a pharmaceutical context. Due to this component, the expected difference in effect between placebo needle treatment and waiting list groups includes a tactile context that has been overlooked in previous studies. The tactile context provided by the placebo needles, much like the medical context under which a pill is given, cannot be physiologically inert, and this stimulation can even exert similar thera-peutic actions by enhancing touch sensations in the body (Kerr et al. 2011). Furthermore, the touch of the placebo needles experienced by the patient initiates a multisensory process and thereby activates bodily self- awareness. Overall, tactile stimulation provides a broader range of contexts that contribute to the effect and
improve the healing process relative to other placebo interventions (Lee & Chae 2018). The effect of the tactile component on the patient can be categorized accordingly into sensory- discriminative and affective- social aspects. These aspects of the tactile component play important roles in the therapeutic effect of acupuncture treatment in clinical practice (Chae & Olausson 2017), which is examined in the context of placebo needles in the following sections.
The sensory- discriminative aspect of the touch component of placebo needlesSeveral studies have examined in depth the sensory- discriminative aspect of acupuncture needles. The process of needle insertion and the types of needle manipulation (Seo et al. 2014) activate diverse touch perception pro-cesses and stimulate mechanically sensitive pain fibres (Zhao 2008). This tactile stimulation process produces what is known as the De Qi sensation (a combination of various sensations that include heaviness, numbness, soreness, and distention), which is fundamental for the therapeutic outcome of acupuncture treatment (Kong et al. 2005; Choi et al. 2013). Placebo nee-dles were first validated as a sufficient control in acupuncture studies under the assumption that a lesser degree of De Qi sensation would be evoked, thereby leading to less effective clini-cal outcomes (Streitberger & Kleinhenz 1998; Park et al. 2002). In the initial validation studies of placebo needles, participants were not able to distinguish the placebo needles from real needles, but they experienced a greater degree of De Qi sensation with real needles than with placebo needles (Streitberger & Kleinhenz 1998; Park et al. 2002; White et al. 2003) (Fig. 1).
On the other hand, a recent validation study of the Streitberger needle conducted with a large population showed no significant difference in De Qi sensation between patients treated with real and placebo needles, even though the pla-cebo needle does not penetrate the skin (Xie et al. 2013). Additionally, a study investigating Park Sham devices revealed that the De Qi sensation induced by real and placebo needles is not dis-tinguishable (Liang et al. 2013). De Qi sensation, a composite of unique sensations produced
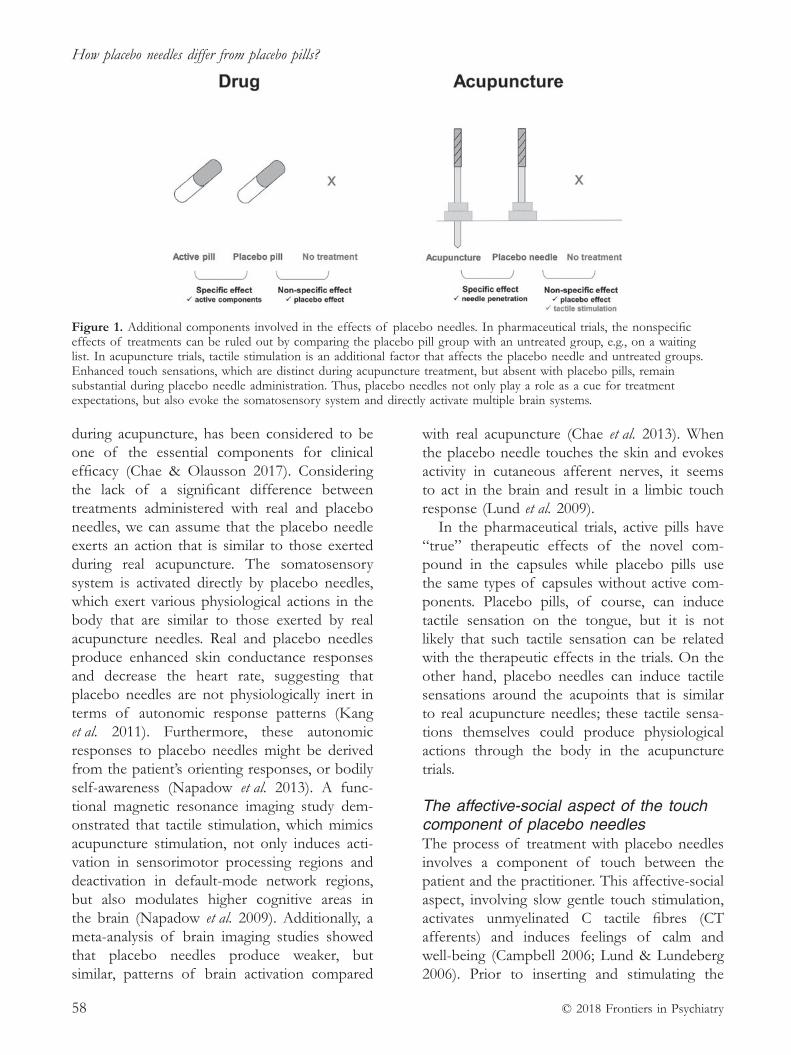
How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry58
during acupuncture, has been considered to be one of the essential components for clinical efficacy (Chae & Olausson 2017). Considering the lack of a significant difference between treatments administered with real and placebo needles, we can assume that the placebo needle exerts an action that is similar to those exerted during real acupuncture. The somatosensory system is activated directly by placebo needles, which exert various physiological actions in the body that are similar to those exerted by real acupuncture needles. Real and placebo needles produce enhanced skin conductance responses and decrease the heart rate, suggesting that placebo needles are not physiologically inert in terms of autonomic response patterns (Kang et al. 2011). Furthermore, these autonomic responses to placebo needles might be derived from the patient’s orienting responses, or bodily self- awareness (Napadow et al. 2013). A func-tional magnetic resonance imaging study dem-onstrated that tactile stimulation, which mimics acupuncture stimulation, not only induces acti-vation in sensorimotor processing regions and deactivation in default- mode network regions, but also modulates higher cognitive areas in the brain (Napadow et al. 2009). Additionally, a meta- analysis of brain imaging studies showed that placebo needles produce weaker, but similar, patterns of brain activation compared
with real acupuncture (Chae et al. 2013). When the placebo needle touches the skin and evokes activity in cutaneous afferent nerves, it seems to act in the brain and result in a limbic touch response (Lund et al. 2009).
In the pharmaceutical trials, active pills have “true” therapeutic effects of the novel com-pound in the capsules while placebo pills use the same types of capsules without active com-ponents. Placebo pills, of course, can induce tactile sensation on the tongue, but it is not likely that such tactile sensation can be related with the therapeutic effects in the trials. On the other hand, placebo needles can induce tactile sensations around the acupoints that is similar to real acupuncture needles; these tactile sensa-tions themselves could produce physiological actions through the body in the acupuncture trials.
The affective- social aspect of the touch component of placebo needlesThe process of treatment with placebo needles involves a component of touch between the patient and the practitioner. This affective- social aspect, involving slow gentle touch stimulation, activates unmyelinated C tactile fibres (CT afferents) and induces feelings of calm and well- being (Campbell 2006; Lund & Lundeberg 2006). Prior to inserting and stimulating the
Figure 1. Additional components involved in the effects of placebo needles. In pharmaceutical trials, the nonspecific effects of treatments can be ruled out by comparing the placebo pill group with an untreated group, e.g., on a waiting list. In acupuncture trials, tactile stimulation is an additional factor that affects the placebo needle and untreated groups. Enhanced touch sensations, which are distinct during acupuncture treatment, but absent with placebo pills, remain substantial during placebo needle administration. Thus, placebo needles not only play a role as a cue for treatment expectations, but also evoke the somatosensory system and directly activate multiple brain systems.

Y. Chae et al.
© 2018 Frontiers in Psychiatry 59
needle, the practitioner touches the patient to assess the skin tissue and identify the region to which the needle will be applied. This process of gently touching the patient’s skin activates CT afferents and alleviates unpleasantness. Furthermore, this type of pleasant touch re- establishes the patient’s sense of self- esteem and well- being by inducing a limbic touch response (Lund & Lundeberg 2006). A clinical study (Kaptchuk et al. 2008) supports the role of affective- social touch in treatments with acupuncture and placebo needles because the enhanced patient–doctor relationship produced greater improvements in patients with irritable bowel syndrome. Additionally, the entirety of the procedure, including warmth, empathy, and the communication of positive expectations, might influence clinical outcomes (Kaptchuk et al. 2008).
Gentle touch, which is always a component of acupuncture treatment, plays a crucial role in the overall outcome of the medical treatment. Gentle touch by a nurse before a surgical opera-tion decreases subjective and objective levels of stress in the patient (Whitcher & Fisher 1979). Furthermore, gentle touch plays a direct moderating role in the physiological responses of the patient such that it lowers blood pres-sure, enhances transient sympathetic reflexes, and increases pain thresholds (McGlone et al. 2014). The affective- social components of gentle touch also enhance the patient– doctor relationship, even when patients are treated with placebo needles (Kaptchuk et al. 2008). Although the gentle touch component prior to the application of real or placebo needles is not considered to be part of the active component of placebo treatment, it is nevertheless part of the placebo preparation in a clinical acupuncture trial. Thus, compared with the effects observed in a waiting list group or a group receiving another placebo intervention, this component generates a stronger doctor–patient relationship and enhances the placebo effect.
Although the placebo needle acts as a control due to its non- penetrating qualities, the tactile component is not completely removed; thus, its application in acupuncture trials may additionally produce crucial effects such as directly evoking
the somatosensory system, strengthening the doctor–patient relationship, and enhancing the patient’s general condition. The biophysical effects of placebo needles influence the patient’s expectations and contextualization, which likely also play roles in his or her cognitive percep-tion during the treatment process regarding the alleviation of symptoms.
Blinding of placebo needle applications The blinding components of placebo needlesPlacebo needles were developed based on a visual illusion that induces the belief that one’s skin has been penetrated (Streitberger & Kleinhenz 1998; Park et al. 2002). The tip of the placebo needle is blunt and retracts into the needle’s handle; thus, a placebo needle has a shape similar to that of a real needle, but is dissimilar in that it does not penetrate the skin. Because the placebo needle induces the sensation of pricking and appears to penetrate the skin, the patient is more likely to classify placebo needle treatment as active relative to placebo pills. Placebo pills are indistinguishable in appearance from the active drug, but the patient must be convinced that they are receiv-ing real treatment. The chance of determining whether a pill is a placebo or an active treatment is theoretically equal in pharmaceutical trials due to the indistinguishable appearance, smell, and taste of placebo pill compared to active drugs; in contrast, the chance of determining whether a needle is placebo or real is not completely equal, since the patient receiving the treatment while looking at and feeling the needle would be inclined to believe that the placebo treat-ment is active. Consequently, the probability of a patient determining placebo and real needle would be even more biased, if they have prior experience of acupuncture needling and have felt its therapeutic effects.
Blinding is another important issue that can minimize bias or the potential effect of context on the outcomes of RCTs (Wood et al. 2008). The blinding index (BI) was developed to assess the success of blinding in clinical trials (Baethge

How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry60
2013) and is interpreted as a “correct guess beyond chance.” For example, a BI of 1 indicates that all guesses are correct, a BI of −1 indicates that all guesses are incorrect, and a BI of 0 indicates that the probabilities of correct and incorrect guesses are equal (Bang et al. 2004). When clas-sifying the blinding results of trials, BI values > 0.2 are considered to indicate failed blinding because more participants guessed correctly, BI values < 0.2 and > −0.2 are considered to be random guesses, and BI values < −0.2 are also considered to indicate failed blinding because more participants guessed incorrectly (Bang et al. 2004). An assessment of blinding in tri-als involving pharmacological interventions for psychiatric disorders yielded average BI values of 0.18 and 0 in the active treatment and pla-cebo control groups, respectively (Freed et al. 2014). This finding implies that blinding was established successfully, which is an ideal result from a scientific perspective.
In contrast, people more often respond to placebo needles because they are more likely to believe that they are receiving active treat-ment, which is also known as an opposite guess (Zhang et al. 2015; Freed et al. 2014). Although a recent systematic review of the use of placebo needles for acupuncture in clinical trials with limited reporting of the credibility of blinding showed that participant blinding was successful in most cases (Zhang et al. 2015), participants were less likely than chance levels to believe that the needles were real, rather than placebos. When a BI calculation was applied to this review, the average BI values were 0.55 and −0.33 for the real and placebo needle groups, respectively (Zhang et al. 2015), indicating unsuccessful blinding. Additionally, based on the classifica-tion rules for blinding scenarios, 86% of studies have involved unblinded participants in the real acupuncture group (BI > 0.2) and participants making opposite guesses in the placebo group (BI< −0.2) (15).
A recent acupuncture study showed that 61 and 68% of patients administered real and placebo treatments, respectively, perceived treat-ment type correctly, which implies that blinding was unsuccessful (Vase et al. 2015). One pos-sible reason for this unsuccessful blinding is
the experience of the De Qi sensation, which could contribute to the correct identification of the treatment (Vase et al. 2015), even though placebo needling sessions produce substantial levels of this sensation. Another possible explanation is that smaller insertion and pullout forces are used during placebo needling (Chae et al. 2011). Differences in biomedical forces may be a crucial reason for the association of different somatosensory processes with the use of real and placebo needles (Schneider et al. 2006) (Figure 2).
Greater expectations during placebo needling produced greater placebo effectsAccording to systematic reviews of the BI in clinical trials, pharmacological placebo pills have an approximately 50% chance of being per-ceived as active, whereas this assumption is not necessarily true for placebo needles (Zhang et al. 2015; Freed et al. 2014). While in the aforemen-tioned studies the adverse events of drug trials indicate the risk of unblinding, the BI index seem to have been uncompromised, possibly due to the occurrence time and the frequency of such events.
The discussed BI patterns are often thought to indicate adequate blinding, but a greater prob-ability of believing that a placebo is real might be due to wishful thinking rather the well- known psychological preference toward real or better treatment (Bang 2016). The greater probability of opposite guesses in placebo needle groups may be related to greater expectations regard-ing symptom alleviation. Placebo effects, or any improvement in the symptoms or physiological condition of an individual receiving a placebo treatment (Enck et al. 2013), are based largely on the expectation of receiving actual treat-ment, cued and contextual conditioning, and/or observational and social learning (Colloca & Miller 2011). Thus, patients may have higher levels of expectation during placebo needling than when receiving placebo pills, which could contribute to treatment efficacy (Colloca et al. 2004). In this manner, placebo responses may be more frequent in placebo needles than in placebo pills because patients are more likely
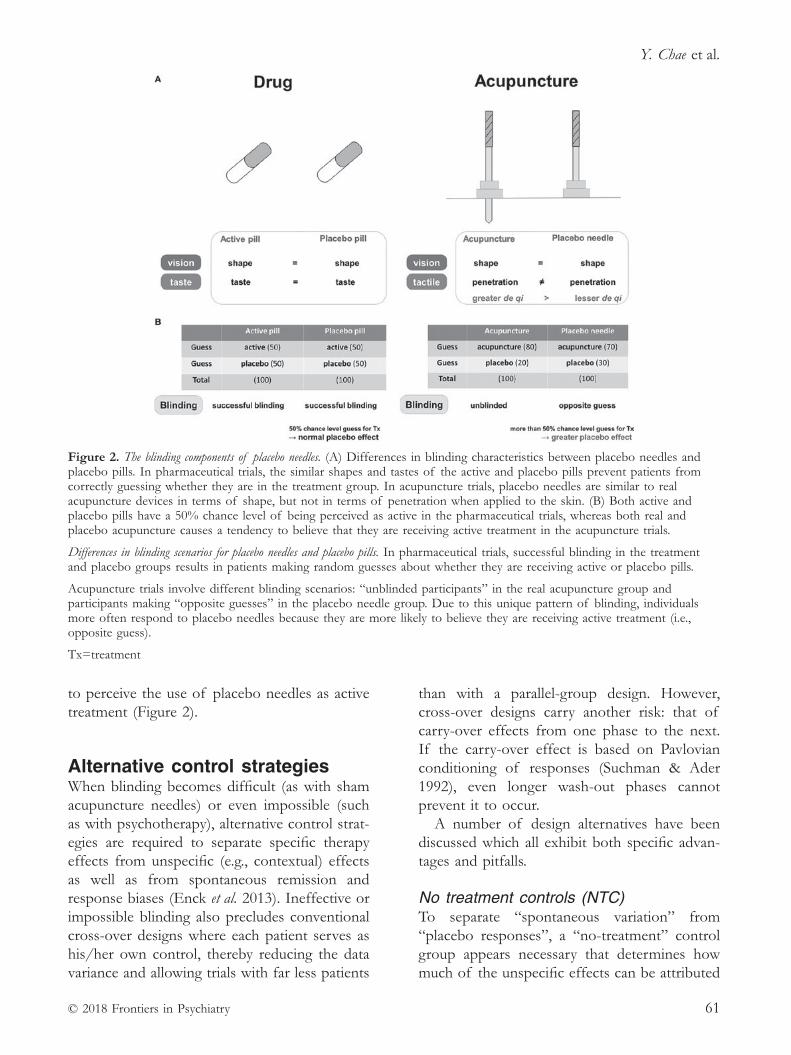
Y. Chae et al.
© 2018 Frontiers in Psychiatry 61
to perceive the use of placebo needles as active treatment (Figure 2).
Alternative control strategiesWhen blinding becomes difficult (as with sham acupuncture needles) or even impossible (such as with psychotherapy), alternative control strat-egies are required to separate specific therapy effects from unspecific (e.g., contextual) effects as well as from spontaneous remission and response biases (Enck et al. 2013). Ineffective or impossible blinding also precludes conventional cross- over designs where each patient serves as his/her own control, thereby reducing the data variance and allowing trials with far less patients
than with a parallel- group design. However, cross- over designs carry another risk: that of carry- over effects from one phase to the next. If the carry- over effect is based on Pavlovian conditioning of responses (Suchman & Ader 1992), even longer wash- out phases cannot prevent it to occur.
A number of design alternatives have been discussed which all exhibit both specific advan-tages and pitfalls.
No treatment controls (NTC)To separate “spontaneous variation” from “placebo responses”, a “no- treatment” control group appears necessary that determines how much of the unspecific effects can be attributed
Figure 2. The blinding components of placebo needles. (A) Differences in blinding characteristics between placebo needles and placebo pills. In pharmaceutical trials, the similar shapes and tastes of the active and placebo pills prevent patients from correctly guessing whether they are in the treatment group. In acupuncture trials, placebo needles are similar to real acupuncture devices in terms of shape, but not in terms of penetration when applied to the skin. (B) Both active and placebo pills have a 50% chance level of being perceived as active in the pharmaceutical trials, whereas both real and placebo acupuncture causes a tendency to believe that they are receiving active treatment in the acupuncture trials.
Differences in blinding scenarios for placebo needles and placebo pills. In pharmaceutical trials, successful blinding in the treatment and placebo groups results in patients making random guesses about whether they are receiving active or placebo pills.
Acupuncture trials involve different blinding scenarios: “unblinded participants” in the real acupuncture group and participants making “opposite guesses” in the placebo needle group. Due to this unique pattern of blinding, individuals more often respond to placebo needles because they are more likely to believe they are receiving active treatment (i.e., opposite guess).
Tx=treatment

How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry62
to spontaneous variation and recovery. Since this is rarely done, the exact size of the contri-bution of spontaneous variation to the placebo response is known only for minor and benign clinical conditions and may account here for approximately 50% of the placebo effect (Krogsboll et al. 2009). In experimental settings, “no treatment controls” may also serve to control for habituation and sensitization effects that may occur with repetitive stimulation, e.g., in pain and placebo analgesia experiments.
NTC are limited by ethical rules when patients with a severe clinical condition require treatment and cannot be offered trial participa-tion that would assign them to a NTC group, as set by the Declaration of Helsinki of the World Medical Association (World Medical Association 2013).
Waiting list control (WLC), treatment as usual (TAU)Assigning patients to a “no treatment” group may be ethically problematic, e.g., in case of severe diseases, or when for other reasons the patients require treatment; in such cases WLC and TAU are control strategies for non- drug testing when an inert “placebo” is not available, e.g., in psychotherapy, physical/manual therapy, surgery, and “instrumental” therapies (TENS, transcranial magnetic or direct current stimula-tion, laser or light therapy), including acupunc-ture (see above). While some of these therapies have “sham therapy techniques” that can serve as placebo controls, e.g., in acupuncture, others must rely on WLC and TAU as their only con-trol condition.
However, WLC and TAU face significant limitations: while patients expect to receive effective therapy, they are randomized to rou-tine treatment most of them have had in the past (TAU), or (in case of WLC) have to wait for the treatment they were recruited for, result-ing in disappointment and potentially nocebo effects (Weimer & Enck 2014). This affects only recruitment and compliance, and biases patient populations in such studies.
To avoid WLC and TAU and the associated disadvantages, studies in acute and chronic pain are often conducted comparing a novel drug
with another drug already available rather than with placebos (Saarto & Wiffen 2007; Quilici et al. 2009).
Comparative effectiveness research (CER)One approach to circumvent the placebo dilemma in RCT (for ethical as well as for meth-odological reasons) has recently been favoured by drug approval authorities, by boards of medi-cal societies, and by ethics committees, namely to avoid utilization of placebos in clinical trials. CER compares novel treatments to already approved therapies: to the best of our knowl-edge, this has never been done for acupuncture therapy, e.g., in chronic pain conditions.
However, as has been shown in a number of meta- analyses in depression, schizophrenia and other diseases, comparing a new therapy to a comparator increases the response solely driven by the higher likelihood of patients to receive active treatments (100%) as compared to placebo- controlled trials (Weimer et al. 2015). In such trials therefore, the placebo response is high but cannot be controlled anymore. Of specific interest is the fact that CER studies need to test for “non- inferiority” of the novel drug, resulting in higher patient numbers (Leon 2011).
Cohort multiple randomized controlled trial (CMRCT) designThe “cohort multiple randomized controlled trial” (CMRCT) (Relton et al. 2010) – formerly also known as the Zelen design (Zelen 1979) – splits the “no treatment” control arm of a drug trial (done for the purpose of mere observation of the natural course of the disease) from the drug trial itself, by recruiting a large cohort of patients for an “observational study” in which patients are followed under their TAU condition.
The observational cohort then serves as the basis for the recruitment of a subsample for the treatment study, either placebo- controlled or CER: patients are randomly approached, but can be selected based on a number of factors accounting for statistical representativeness.
A number of limitations apply, however: “the observational cohort needs to be monitored over time (a

Y. Chae et al.
© 2018 Frontiers in Psychiatry 63
cross- sectional sample analysis would not be sufficient to account for changes occurring over time), and it needs to be representative for complete patient cohort affected by the diseases, both in terms of disease features (e.g., symptom severity) as well as disease management (diag-nosis, TAU). Once such a cohort it established it may be used for more than one RCT ” (Weimer & Enck 2014).
Discussion and conclusionSimilar to other placebo types, placebo needles play an important contextual role in treatment expectations; however, they also directly evoke the somatosensory system and activate multiple brain systems. Placebo preparations are applied in studies to blind participants, and they enable the calculation of chance levels for patients’ guesses about whether interventions are thera-peutic or inert. However, the probability of making an opposite guess is greater for placebo needles than for placebo pills, which is often explained by patients’ greater expectations. Because patients are more likely to perceive placebos as active treatment in placebo needle trials, placebo responses may be observed more frequently to placebo needles than to placebo pills.
The tactile components of acupuncture needle use are crucial factors during treatment preparation and could not be fully controlled for as placebo needles were being developed. The distinctive touch sensations experienced during acupuncture treatment are substantial, even during the administration of placebo needles. Due to the physical contact necessary when applying placebo needles, the validity of these needles as controls has been in question from the perspectives of physiological inertness and blinding. These factors may result in placebo needles exerting stronger placebo effects than do other types of placebo preparation that do not include tactile components. Thus, the devel-opment of a technique to control for the tactile components of acupuncture interventions while participants are consciously receiving treatment is an important consideration. The studies reviewed here demonstrated that the De Qi sensation cannot be completely accounted for
when using placebo needles without control-ling for the tactile components, which suggests some level of clinical efficacy. Placebo needle administrations may inadvertently, albeit less robustly, activate the somatosensory system and induce regulatory mechanisms that are also trig-gered by acupuncture needling. Furthermore, placebo needles, or what we have considered to be control needles for experimental studies, may be a form of acupuncture treatment that is low dose or that provides weak stimulation.
In clinical trials, the placebo control should be indistinguishable from the active treatment (i.e., blinding success) and yet physiologically inert (less De Qi sensation in this case). In the case of acupuncture, however, it is difficult to meet these two criteria simultaneously (Chae 2017). Most importantly, our argument on the inadequacy of placebo needles as controls in acupuncture trials should not inhibit further acupuncture trials with randomized, controlled designs. Placebo needles indeed are more likely to induce placebo responses than placebo pills, which is largely due to the tactile component that cannot be separated from the components of the real acupuncture needles. In other words, conversely, our arguments imply that acupuncture needles contain a substantial level of placebo effect, which was not completely ruled out by controlling the penetration. It is also important to note that waiting lists do produce unspecific effects on their own (Gold et al. 2017). Furthermore, recent studies in acupuncture have employed study designs such as pragmatic trials, which compare acupuncture treatment with waiting lists and usual care (Witt et al. 2006; MacPherson et al. 2012; Chung et al. 2016), while other innovative control strategies still await validation with acupuncture. In the meantime, the discussion on the effect of the tactile components of placebo needles in its effectiveness as placebos, as well as effective blinding, needs to be continued.
Taken together, the placebo needles do have different characteristics from placebo pills in clinical trials. Our exploration does not imply that acupuncture may be more effective than placebo, but suggests that we have to consider these unique characteristics of placebo needles
How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry64
before we draw premature conclusions that acupuncture itself is just a placebo.
Author contributionsConceived and designed the paper: Y. C. and P. E.. Wrote the first draft of the paper: Y. C., Y.- S. L. and P. E.. Revised the paper and approved the final version: Y. C., Y.- S. L. and P. E.
AcknowledgementsThis research was supported by Basic Science Research Program through the National Re search Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2014K2A3A1000166 & 2015 R1D1A1A01058033 & 2015M3A9E3052338).
referencesBaethge C., Assall O. P. & Baldessarini R. J. (2013)
Systematic review of blinding assessment in random-ized controlled trials in schizophrenia and affective disorders 2000–2010. Psychotherapy and Psychosomatics 82 (3), 152–160.
Bang H., Ni L., & Davis C. E. (2004) Assessment of blinding in clinical trials. Controlled Clinical Trials 25 (2), 143–156.
Bang H. (2016) Random guess and wishful thinking are the best blinding scenarios. Contemporary Clinical Trials Communications 3, 117–121.
Campbell A. (2006) Role of C tactile fibres in touch and emotion–clinical and research relevance to acupunc-ture. Acupuncture in Medicine 24 (4), 169–171.
Chae Y., Um S. I., Yi S. H., et al. (2011) Comparison of biomechanical properties between acupuncture and non- penetrating sham needle. Complementary Therapies in Medicine 19 (Suppl. 1), S8–12.
Chae Y., Chang D. S., Lee S. H., et al. (2013) Inserting needles into the body: a meta- analysis of brain activity associated with acupuncture needle stimulation. Journal of Pain 14 (3), 215–222.
Chae Y. & Olausson H. (2017) The role of touch in acupuncture treatment. Acupuncture in Medicine 35 (2), 148–152.
Chae Y. (2017) The dilemma of placebo needles in acupuncture research. Acupuncture in Medicine 35 (5), 382–383.
Cherkin D. C., Sherman K. J., Avins A. L., et al. (2009) A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Archives of Internal Medicine 169 (9), 858–866.
Choi Y. J., Lee J. E., Moon W. K. & Cho S. H. (2013) Does the effect of acupuncture depend on needling
sensation and manipulation? Complementary Therapies in Medicine 21 (3), 207–214.
Chung V. C., Ho R. S., Liu S., et al. (2016) Electroacupuncture and splinting versus splinting alone to treat carpal tunnel syndrome: a randomized controlled trial. Canadian Medical Association Journal 188 (12), 867–875.
Colloca L., Lopiano L., Lanotte M. & Benedetti F. (2004) Overt versus covert treatment for pain, anxiety, and Parkinson’s disease. Lancet Neurology 3 (11), 679–684.
Colloca L. & Miller F. G. (2011) How placebo responses are formed: a learning perspective. Philosophical Transactions of the Royal Society of London, Series B Biological Sciences 366 (1572), 1859–1869.
De Craen A. J., Tijssen J. G., De Gans J. & Kleijnen J. (2000) Placebo effect in the acute treatment of migraine: subcutaneous placebos are better than oral placebos. Journal of Neurology 247 (3), 183–188.
Dincer F. & Linde K. (2003) Sham interventions in randomized clinical trials of acupuncture – a review. Complementary Therapies in Medicine 11 (4), 235–242.
Enck P., Klosterhalfen S. & Zipfel S. (2010) Acupuncture, psyche and the placebo response. Autonomic Neuroscience 157 (1–2), 68–73.
Enck P., Bingel U., Schedlowski M. & Rief W. (2013) The placebo response in medicine: minimize, maximize or personalize? Nature Reviews. Drug Discovery 12 (3), 191–204.
Freed B., Assall O. P., Panagiotakis G., et al. (2014) Assessing blinding in trials of psychiatric disorders: a meta- analysis based on blinding index. Psychiatry Research 219 (2), 241–247.
Gold S. M., Enck P., Hasselmann H., et al. (2017) Control conditions for randomized trials of behavioural inter-ventions in psychiatry: a decision framework. Lancet Psychiatry 4 (9), 725–732.
Hróbjartsson A. & Gøtzsche P. C. (2010) Placebo inter-ventions for all clinical conditions. Cochrane Database of Systematic Reviews Issue 1, Art. No.: CD003974.
Hu B., Bai F., Xiong L. & Wang Q. (2017) The endo-cannabinoid system, a novel and key participant in acupuncture’s multiple beneficial effects. Neuroscience and Biobehavioural Review 77, 340–357.
Kang O. S., Chang D. S., Lee M. H., et al. (2011) Autonomic and subjective responses to real and sham acupuncture stimulation. Autonomic Neuroscience 159 (1–2), 127–130.
Kaptchuk T. J., Goldman P., Stone D. A. & Stason W. B. (2000) Do medical devices have enhanced placebo effects? Journal of Clinical Epidemiology 53 (8), 786–792.
Kaptchuk T. J., Kelley J. M., Conboy L. A., et al. (2008) Components of placebo effect: randomized controlled trial in patients with irritable bowel syndrome. BMJ 336 (7651), 999–1003.
Kaptchuk T. J., Stason W. B., Davis R. B., et al. (2006) Sham device v inert pill: randomized controlled trial of two placebo treatments. BMJ 332 (7538), 391–397.

Y. Chae et al.
© 2018 Frontiers in Psychiatry 65
Kerr C. E., Shaw J. R., Conboy L. A., et al. (2011) Placebo acupuncture as a form of ritual touch healing: a neuro-phenomenological model. Consciousness and Cognition 20 (3), 784–791.
Kong J., Fufa D. T., Gerber A. J., et al. (2005) Psychophysical outcomes from a randomized pilot study of manual, electro, and sham acupuncture treat-ment on experimentally induced thermal pain. Journal of Pain 6 (1), 55–64.
Krogsbøll L. T., Hróbjartsson A. & Gøtzsche P. C. (2009) Spontaneous improvement in randomized clinical trials: meta- analysis of three- armed trials comparing no treat-ment, placebo and active intervention. BMC Medical Research Methodology 9 (1).
Langevin H. M., Hammerschlag R., Lao L., et al. (2006) Controversies in acupuncture research: selection of controls and outcome measures in acupuncture clinical trials. Journal of Alternative and Complementary Medicine 12 (10), 943–953.
Lee Y. S. & Chae Y. (2018) Powerful effects of placebo needles. Acupuncture in Medicine 36, 197–199.
Leon A. C. (2011) Evolution of psychopharmacology trial design and analysis: six decades in the making. Journal of Clinical Psychiatry 72 (3), 331–340.
Liang Z. H., Xie C. C., Li Z. P., et al. (2013) De Qi sensation in placebo acupuncture: a crossover study on Chinese medicine students. Evidence- Based Complementary and Alternative Medicine 2013, Article ID: 620671.
Linde K., Niemann K. & Meissner K. (2010) Are sham acupuncture interventions more effective than (other) placebos? A re- analysis of data from the Cochrane review on placebo effects. Forschende Komplementarmedizin 17 (5), 259–264.
Liu T. (2009) Acupuncture: what underlies needle admin-istration? Evidence- Based Complementary and Alternative Medicine 6 (2), 185–193.
Lund I. & Lundeberg T. (2006) Are minimal, superfi-cial or sham acupuncture procedures acceptable as inert placebo controls? Acupuncture in Medicine 24 (1), 13–15.
Lund I., Naslund J. & Lundeberg T. (2009) Minimal acupuncture is not a valid placebo control in random-ized controlled trials of acupuncture: a physiologist’s perspective. Chinese Medicine 4 (1).
Lundeberg T., Lund I., Naslund J. & Thomas M. (2008) The Emperors sham – wrong assumption that sham needling is sham. Acupuncture in Medicine 26 (4), 239– 242.
Madsen M. V., Gøtzsche P. C. & Hróbjartsson A. (2009) Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ 338, a3115.
MacPherson H., Tilbrook H., Bland J. M., et al. (2012) Acupuncture for irritable bowel syndrome: primary care based pragmatic randomised controlled trial. BMC Gastroenterology 12, 150.
McGlone F., Wessberg J. & Olausson H. (2014) Discriminative and affective touch: sensing and feeling. Neuron 82 (4), 737–755.
Napadow V., Dhond R. P., Kim J., et al. (2009) Brain encoding of acupuncture sensation–coupling on- line rating with fMRI. NeuroImage 47 (3), 1055–1065.
Napadow V., Lee J., Kim J., et al. (2013) Brain correlates of phasic autonomic response to acupuncture stimula-tion: an event- related fMRI study. Human Brain Mapping 34 (10), 2592–2606.
Park J., White A., Stevinson C., et al. (2002) Validating a new non- penetrating sham acupuncture device: two randomised controlled trials. Acupuncture in Medicine 20 (4), 168–174.
Quilici S., Chancellor J., Lothgren M., et al. (2009) Meta- analysis of duloxetine vs. pregabalin and gabapentin in the treatment of diabetic peripheral neuropathic pain. BMC Neurology 9 (6).
Relton C., Torgerson D., O’Cathain A. & Nicholl J. (2010) Rethinking pragmatic randomized controlled trials: introducing the “cohort multiple randomized controlled trial” design. BMJ 340:c1066.
Saarto T. & Wiffen P. J. (2007) Antidepressants for neuro-pathic pain. Cochrane Database of Systematic Reviews Issue 4, Article No.: CD005454.
Schneider A., Enck P., Streitberger K., et al. (2006) Acupuncture treatment in irritable bowel syndrome. Gut 55 (5), 649–654.
Seo Y., Lee I. S., Jung W. M., et al. (2014) Motion pat-terns in acupuncture needle manipulation. Acupuncture in Medicine 32 (5), 394–399.
Solomon S. (2017) Acupuncture for Headache. It’s Still All Placebo. Headache 57 (1), 143–146.
Streitberger K. & Kleinhenz J. (1998) Introducing a placebo needle into acupuncture research. Lancet 352 (9125), 364–365.
Suchman A. L. & Ader R. (1992) Classic condition-ing and placebo effects in crossover studies. Clinical Pharmacology and Therapeutics 52 (4), 372–377.
Vase L., Baram S., Takakura N., et al. (2015) Can acupunc-ture treatment be double- blinded? An evaluation of double- blind acupuncture treatment of postoperative pain. PLoS ONE 10 (3), e0119612.
Wager T. D. & Atlas L. Y. (2015) The neuroscience of placebo effects: connecting context, learning and health. Nature Reviews. Neuroscience 16 (7), 403–418.
Weimer K. & Enck P. (2014) Traditional and innova-tive experimental and clinical trial designs and their advantages and pitfalls. In: Handbook of Experimental Pharmacology (eds J. E Barrett, V. Flockerzi, M. A. Frohman et al.) pp. 237–272. Springer, Berlin.
Weimer K., Colloca L. & Enck P. (2015) Placebo effects in psychiatry: mediators and moderators. Lancet Psychiatry 2 (3), 246–257.
Whitcher S. J. & Fisher J. D. (1979) Multidimensional reaction to therapeutic touch in a hospital setting. Journal of Personality and Social Psychology 37 (1), 87–96.

How placebo needles differ from placebo pills?
© 2018 Frontiers in Psychiatry66
White P., Lewith G., Hopwood V. & Prescott P. (2003) The placebo needle, is it a valid and convincing placebo for use in acupuncture trials? A randomised, single- blind, cross- over pilot trial. Pain 106 (3), 401–409.
Witt C. M., Jena S., Selim D., et al. (2006) Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. American Journal of Epidemiology 164 (5), 487–496.
Wood L., Egger M., Gluud L., et al. (2008) Empirical evidence of bias in treatment effect estimates in con-trolled trials with different interventions and outcomes: meta- epidemiological study. BMJ 336 (7644), 601–605.
World Medical Association (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310 (20), 2191–2194.
Xie C. C., Wen X. Y., Jiang L., et al. (2013) Validity of the “Streitberger” needle in a Chinese population with acu-puncture: a randomized, single- blinded, and crossover pilot study. Evidence- Based Complementary and Alternative Medicine 2013, Article ID: 251603.
Zelen M. (1979) A new design for randomized clinical tri-als. New England Journal of Medicine 300 (22), 1242–1245.
Zhang C. S., Tan H. Y., Zhang G. S., et al. (2015) Placebo devices as effective control methods in acupuncture clinical trials: a systematic review. PLoS ONE 10 (11), e0140825.
Zhao Z. Q. (2008) Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology 85 (4), 355–375.
Conflict of Interest StatementThe authors declare that the research was con-ducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). The use, distribution or reproduction in other forums is per-mitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted aca-demic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
This article is reprinted from Frontiers in Psychiatry. Original publication: Chae Y., Lee Y.- S. & Enck P. (2018) Frontiers in Psychiatry 9, article 243. doi: 10.3389/fpsyt.2018.00 243

© 2018 Acupuncture Association of Chartered Physiotherapists 67
Correspondence: André Manso (email: [email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 67–75
CASE rEPOrTS
Acupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study
A. MansoNorth Hampshire Physiotherapy and Podiatry service, Basingstoke, UK
AbstractThis case study presents the inclusion of Western medical acupuncture in the treatment plan for greater trochanteric pain syndrome (GTPS). A patient with an 18- month history of lateral right hip pain was referred for physiotherapy due to its significant impact on her activities of daily living and sleep.
A physiotherapy plan including manual therapy, exercise, advice and three acupuncture/dry needling sessions was applied through six sessions, after which the patient reported sig-nificant improvement in the Numerical Pain Rating Scale (NPRS) and in the Hip Disability and Osteoarthritis Outcome Score (HOOS) at 2 weeks follow- up.
The detailed treatment plan and clinical reasoning is discussed, including the rationale for acupuncture and comparison with currently available literature but, as a case study, sensible generalization is advised.
Keywords: acupuncture, dry needling, greater trochanteric pain syndrome.
IntroductionGreater trochanteric pain syndrome (GTPS) is an expression that has been suggested to make terminology more accurate regarding localized lateral hip, thigh and buttock pain with focal point tenderness over the greater trochanter (GT) (Reid 2016; Brennan et al. 2017). Up until recently, clinicians and researchers would refer to this condition as trochanteric bursitis or gluteal tendinopathy, among others, but recent research shows that, often, inflammation is not involved (Brennan et al. 2017). According to Klauser et al. (2013) and Reid (2016), different conditions can be present in GTPS: degenerative tendinopathy/tears of gluteus minimus (glut-min) and medius (glutmed) (18% to 50%), along with muscle waste/dysfunction, calcification and fat degeneration; bursitis of one of the bursae around the GT (subgluteus minimus, medius,
maximus bursae and sometimes bursae between the iliotibial band and GT) (4% to 46%) and/or external coxa saltans. Understanding which of these is more relevant and in which phase they are, along with the mechanical analysis for each case, may get the physiotherapist more prepared to address the patient’s full presentation.
Currently, there is no defined treatment protocol and the first line of treatment often includes a range of conservative interventions, such as “physiotherapy, local corticosteroid injection (CSI), platelet- rich plasma injection, shockwave therapy (SWT), activity modification, pain- relief and anti- inflammatory medication and weight reduction” with success rates of over 90%. A few cases persist despite treatment and time, which “may require surgical intervention in the form of bursectomy, iliotibial band (ITB) lengthening techniques or gluteal tendon repair ” (Reid 2016, p.16).
Three studies were found that measure the effects of acupuncture (dry needling (DN)) on

Acupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study
© 2018 Acupuncture Association of Chartered Physiotherapists68
GTPS. Brennan et al. (2017) (N = 43, no control group) compared its effects with the ones of CSIs and found DN effects not to be inferior to CSI at 6 weeks follow- up, which supports the idea that the effects obtained with the CSI are due to the needling, rather than the sub-stance used as first suggested by Lewit (1979). Pavkovich (2015a) (N = 4, no control group) suggests that strengthening and stretching exer-cises combined with DN along the lateral thigh aspect leads to significant changes in pain and function at short- and long- term (12 months). A Pavkovich (2015b) case report shows signifi-cant changes in function and average pain levels post- 8 weeks of “DN only” treatment, but no changes in maximum pain level.
Considering the proposed mechanisms of action and principles of DN and acupuncture, one can justify their use to treat GTPS as: 1) it is a condition that mostly affects soft tissue, therefore there is reasoning for the use of trig-ger points (MTrPs) DN to improve the muscle tightness/dysfunction/fatigue and myofascial pain (Dommerholt & Fernandez- de- las- Peñas 2013); 2) the high levels of pain sometimes experienced often prevent a normal gait pat-tern and affect sleep and, consequently, rest and muscle recovery, which can be helped by the acupuncture effects on the pain pathways and opioid system, and by relaxation induction, through its central effects (White et al. 2008); 3) it can be a long- standing (months) condi-tion with the potential for central sensitization, which is believed to take place at central levels such as the dorsal horn, where acupuncture can stimulate the opioid peptide system to modulate this event (White et al. 2008); 4) by the trig-gering of local effects mediated by the release of neuropeptides which induce vasodilation, increasing local blood flow to surrounding tis-sues and promoting healing (White et al. 2008; Sandberg et al. 2003).
Case reportPatient profilePatient A is a 56- year- old female who works as a receptionist at a community hospital, which confines her to desk- based work for 8 h shifts.
Patient A enjoys being outside as she is a keen walker (2–4 h walks) and walks her large dog daily.
History of present condition18- month history with gradual onset of right lateral hip/thigh pain as detailed in Table 1.
No history of recent falls/trauma, road traf-fic accident or lower back pain. No red flags identified. Patient’s x- ray shows early degenera-tive changes with superior marginal acetabular osteophytes on the right hip joint.
Past medical historyNo previous right hip pain; one episode of acute severe lower back pain about 10 years ago, which resolved completely. No history of hip/lower back pain around her two pregnancies. Patient has had a coronary artery bypass graft-ing in 2006.
Drug historyCo- codamol, pro re nata (PRN) (stopped after the first appointment); aspirin (75 mg 1x day); Ramipril (2.5 mg 1x day), Bisoprolol (2.5 mg 1x day); Atorvastatin (40 mg 1x day).
Diagnosis and clinical reasoningPatient A was diagnosed with GTPS with significant component of gluteus minimus ten-dinopathy (possible tear) and possible bursitis, aggravated by lumbo- pelvic posture, poor spinal stability strategies and tight hip flexors/tensor fasciae latae (TFL). These changes are likely to have been aggravated by Patient A’s lifestyle (keen walker versus office- based job). For the patient, the main problem was the severity of Pain 1 (P1) and Pain 2 (P2) and the impact it was having on some of her activities of daily living (ADLs), such as walks, walking the dog, and the regular sleep disruption.
Acupuncture treatmentBefore considering acupuncture, Patient A had already undergone three physiotherapy treat-ments, focusing on:• education on the importance of work pos-
ture and daily activity modification regarding work and 2 to 4 h walks
• manual release of glutmin/TFL, active myo-fascial trigger points (MTrPs) and muscle energy techniques (MET)
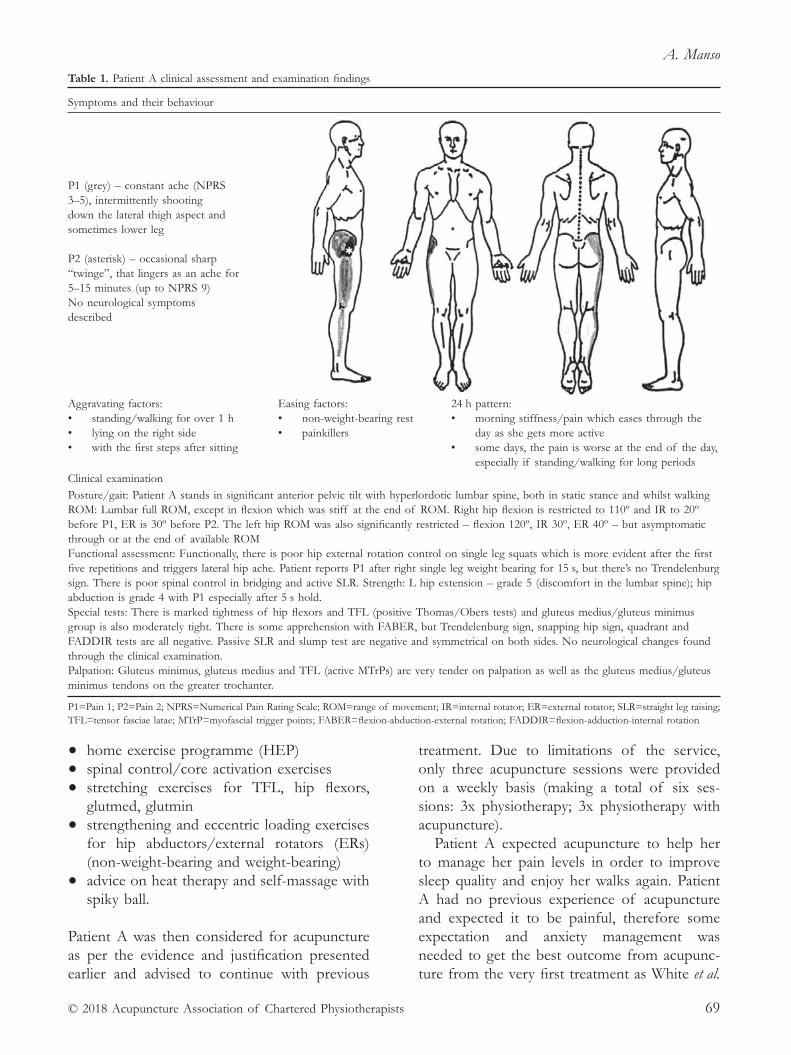
A. Manso
© 2018 Acupuncture Association of Chartered Physiotherapists 69
• home exercise programme (HEP)
• spinal control/core activation exercises
• stretching exercises for TFL, hip flexors, glutmed, glutmin
• strengthening and eccentric loading exercises for hip abductors/external rotators (ERs) (non- weight- bearing and weight- bearing)
• advice on heat therapy and self- massage with spiky ball.
Patient A was then considered for acupuncture as per the evidence and justification presented earlier and advised to continue with previous
treatment. Due to limitations of the service, only three acupuncture sessions were provided on a weekly basis (making a total of six ses-sions: 3x physiotherapy; 3x physiotherapy with acupuncture).
Patient A expected acupuncture to help her to manage her pain levels in order to improve sleep quality and enjoy her walks again. Patient A had no previous experience of acupuncture and expected it to be painful, therefore some expectation and anxiety management was needed to get the best outcome from acupunc-ture from the very first treatment as White et al.
Table 1. Patient A clinical assessment and examination findings
Symptoms and their behaviour
P1 (grey) – constant ache (NPRS 3–5), intermittently shooting down the lateral thigh aspect and sometimes lower leg
P2 (asterisk) – occasional sharp “twinge”, that lingers as an ache for 5–15 minutes (up to NPRS 9)No neurological symptoms described
Aggravating factors:• standing/walking for over 1 h• lying on the right side• with the first steps after sitting
Easing factors:• non- weight- bearing rest• painkillers
24 h pattern: • morning stiffness/pain which eases through the
day as she gets more active• some days, the pain is worse at the end of the day,
especially if standing/walking for long periodsClinical examinationPosture/gait: Patient A stands in significant anterior pelvic tilt with hyperlordotic lumbar spine, both in static stance and whilst walking ROM: Lumbar full ROM, except in flexion which was stiff at the end of ROM. Right hip flexion is restricted to 110º and IR to 20º before P1, ER is 30º before P2. The left hip ROM was also significantly restricted – flexion 120º, IR 30º, ER 40º – but asymptomatic through or at the end of available ROM Functional assessment: Functionally, there is poor hip external rotation control on single leg squats which is more evident after the first five repetitions and triggers lateral hip ache. Patient reports P1 after right single leg weight bearing for 15 s, but there’s no Trendelenburg sign. There is poor spinal control in bridging and active SLR. Strength: L hip extension – grade 5 (discomfort in the lumbar spine); hip abduction is grade 4 with P1 especially after 5 s hold. Special tests: There is marked tightness of hip flexors and TFL (positive Thomas/Obers tests) and gluteus medius/gluteus minimus group is also moderately tight. There is some apprehension with FABER, but Trendelenburg sign, snapping hip sign, quadrant and FADDIR tests are all negative. Passive SLR and slump test are negative and symmetrical on both sides. No neurological changes found through the clinical examination. Palpation: Gluteus minimus, gluteus medius and TFL (active MTrPs) are very tender on palpation as well as the gluteus medius/gluteus minimus tendons on the greater trochanter.
P1=Pain 1; P2=Pain 2; NPRS=Numerical Pain Rating Scale; ROM=range of movement; IR=internal rotator; ER=external rotator; SLR=straight leg raising; TFL=tensor fasciae latae; MTrP=myofascial trigger points; FABER=flexion- abduction- external rotation; FADDIR=flexion- adduction- internal rotation
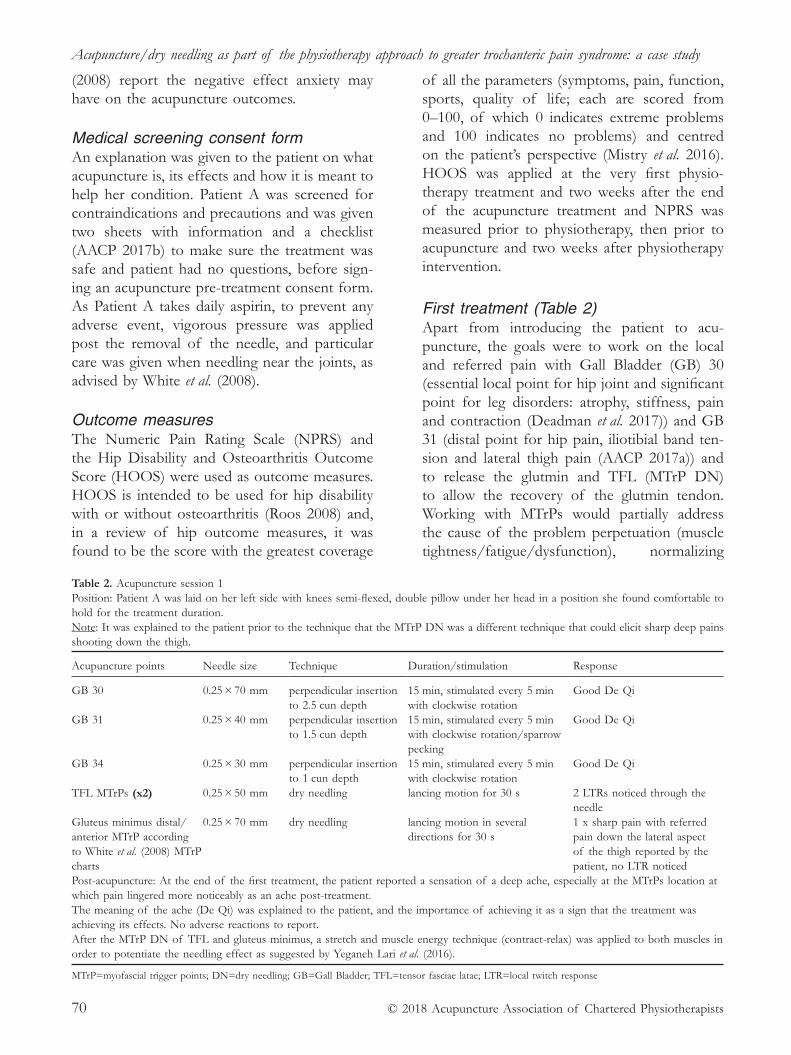
Acupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study
© 2018 Acupuncture Association of Chartered Physiotherapists70
(2008) report the negative effect anxiety may have on the acupuncture outcomes.
Medical screening consent formAn explanation was given to the patient on what acupuncture is, its effects and how it is meant to help her condition. Patient A was screened for contraindications and precautions and was given two sheets with information and a checklist (AACP 2017b) to make sure the treatment was safe and patient had no questions, before sign-ing an acupuncture pre- treatment consent form. As Patient A takes daily aspirin, to prevent any adverse event, vigorous pressure was applied post the removal of the needle, and particular care was given when needling near the joints, as advised by White et al. (2008).
Outcome measuresThe Numeric Pain Rating Scale (NPRS) and the Hip Disability and Osteoarthritis Outcome Score (HOOS) were used as outcome measures. HOOS is intended to be used for hip disability with or without osteoarthritis (Roos 2008) and, in a review of hip outcome measures, it was found to be the score with the greatest coverage
of all the parameters (symptoms, pain, function, sports, quality of life; each are scored from 0–100, of which 0 indicates extreme problems and 100 indicates no problems) and centred on the patient’s perspective (Mistry et al. 2016). HOOS was applied at the very first physio-therapy treatment and two weeks after the end of the acupuncture treatment and NPRS was measured prior to physiotherapy, then prior to acupuncture and two weeks after physiotherapy intervention.
First treatment (Table 2)Apart from introducing the patient to acu-puncture, the goals were to work on the local and referred pain with Gall Bladder (GB) 30 (essential local point for hip joint and significant point for leg disorders: atrophy, stiffness, pain and contraction (Deadman et al. 2017)) and GB 31 (distal point for hip pain, iliotibial band ten-sion and lateral thigh pain (AACP 2017a)) and to release the glutmin and TFL (MTrP DN) to allow the recovery of the glutmin tendon. Working with MTrPs would partially address the cause of the problem perpetuation (muscle tightness/fatigue/dysfunction), normalizing
Table 2. Acupuncture session 1Position: Patient A was laid on her left side with knees semi- flexed, double pillow under her head in a position she found comfortable to hold for the treatment duration.Note: It was explained to the patient prior to the technique that the MTrP DN was a different technique that could elicit sharp deep pains shooting down the thigh.
Acupuncture points Needle size Technique Duration/stimulation Response
GB 30 0.25 × 70 mm perpendicular insertion to 2.5 cun depth
15 min, stimulated every 5 min with clockwise rotation
Good De Qi
GB 31 0.25 × 40 mm perpendicular insertion to 1.5 cun depth
15 min, stimulated every 5 min with clockwise rotation/sparrow pecking
Good De Qi
GB 34 0.25 × 30 mm perpendicular insertion to 1 cun depth
15 min, stimulated every 5 min with clockwise rotation
Good De Qi
TFL MTrPs (x2) 0.25 × 50 mm dry needling lancing motion for 30 s 2 LTRs noticed through the needle
Gluteus minimus distal/anterior MTrP according to White et al. (2008) MTrP charts
0.25 × 70 mm dry needling lancing motion in several directions for 30 s
1 x sharp pain with referred pain down the lateral aspect of the thigh reported by the patient, no LTR noticed
Post- acupuncture: At the end of the first treatment, the patient reported a sensation of a deep ache, especially at the MTrPs location at which pain lingered more noticeably as an ache post- treatment. The meaning of the ache (De Qi) was explained to the patient, and the importance of achieving it as a sign that the treatment was achieving its effects. No adverse reactions to report. After the MTrP DN of TFL and gluteus minimus, a stretch and muscle energy technique (contract- relax) was applied to both muscles in order to potentiate the needling effect as suggested by Yeganeh Lari et al. (2016).
MTrP=myofascial trigger points; DN=dry needling; GB=Gall Bladder; TFL=tensor fasciae latae; LTR=local twitch response

A. Manso
© 2018 Acupuncture Association of Chartered Physiotherapists 71
muscle tone (Dommerholt & Fernandez- de- las- Peñas 2013) and facilitating the HEP.
Additionally, GB 34 was selected as it is a main point for stiffness of joints/muscles and a major point for lower limb disorders (Deadman et al. 2017). As it was Patient A’s first acupunc-ture experience, no more than six needles were used, of which only three were in place at the same time for a short period of 15 min.
Second treatment (Table 3)Patient A reported that after the first acupunc-ture treatment and with the HEP/self- massage she was feeling more relaxed and “less achy” when lying on her right at night, feeling she could achieve a deeper sleep. Patient A reported she was recently getting able to walk for periods of 1 h with ache onset just towards the end of it. Patient still reported P2 (NPRS 8). On examination, right hip ER improved to 40º, still with P2 at end of range, Obers’ test was better, but still showing a mild tightness. On palpation, the discomfort was more localised to the glut-min and at its insertion on the GT.
As there were no adverse reactions following the first treatment, the same points were used
and another “layer” (as proposed by Bradnam 2007) was added by working on the segments that provide motor supply to the glutmin (L4- S1) through Bladder (BL) 25–27, to increase the segmental effects (White et al. 2008). GB 29 was added for further local and segmental effects (White et al. 2008).
Third treatment (Table 4)At this stage, Patient A reported 80% overall improvement from the beginning of physiother-apy intervention and symptoms were as described on Table 5. On examination, P1 was quite local-ized on antero- superior aspect of the GT (not shooting even on deep palpation), Obers’ test was negative and hip abduction strength (pain- free) was Grade 5 which, in some way, added to a non- muscular source hypothesis, such as the bursae. Right hip had symmetrical range of movement (ROM) when compared with left hip, with similar end- feel, but P2 would still be trig-gered at the end of range of ER (NPRS 7).
Thus, on the third appointment the emphasis was given to local (bursae) and segmental effects by working with the “fencing the dragon” technique (White et al. 2008) and adding a
Table 3. Acupuncture session 2Position: as per previous sessionNote: As Patient A was sore after the dry needling on the first treatment and at the second treatment gluteus minimus was the main location of soreness (not TFL), only the gluteus minimus was needled.
Acupuncture points Needle size Technique Duration/stimulation Response
GB 30 0.25 × 70mm perpendicular insertion, 2,5 cun depth
15 min, stimulated every 5 min with clockwise rotation
strong De Qi
GB 31 0.25 × 40 mm perpendicular insertion, 1,5 cun depth
15 min, stimulated every 5 min with clockwise rotation/ sparrow pecking
mild De Qi
GB 34 0.25 × 30 mm perpendicular insertion, 1 cun depth
15 min, stimulated every 5 min with clockwise rotation
strong De Qi
BL 25 0.25 × 40 mm oblique towards spine, 1 cun depth
20 min, stimulated every 5 min with clockwise rotation
good De Qi
BL 26 0.25 × 40 mm oblique towards spine, 1 cun depth
20 min, stimulated every 5 min with clockwise rotation
good De Qi
BL 27 0.25 × 40 mm oblique towards spine, 1 cun depth
20 min, stimulated every 5 min with clockwise rotation
good De Qi
GB 29 0.25 × 60 mm oblique posteriorly insertion, 2,5 cun depth
20 min, stimulated every 5 min with clockwise rotation
good De Qi
Gluteus minimus MTrP as per last session
0.25 × 70 mm dry needling as per previous session and 5 min post stimulation
2 x LTR felt through the needle
Post- acupuncture: At the end of the second treatment, the patient reported she didn’t feel as sore as after the first treatment and that the Bladder points triggered a warmth sensation on the lower back. No adverse reactions to report As per last session, MET were applied to gluteus minimus after the removal of the needles.
TFL= tensor fasciae latae; GB=Gall Bladder; BL=Bladder; MTrP=myofascial trigger points; LTR= local twitch response; MET=muscle energy techniques
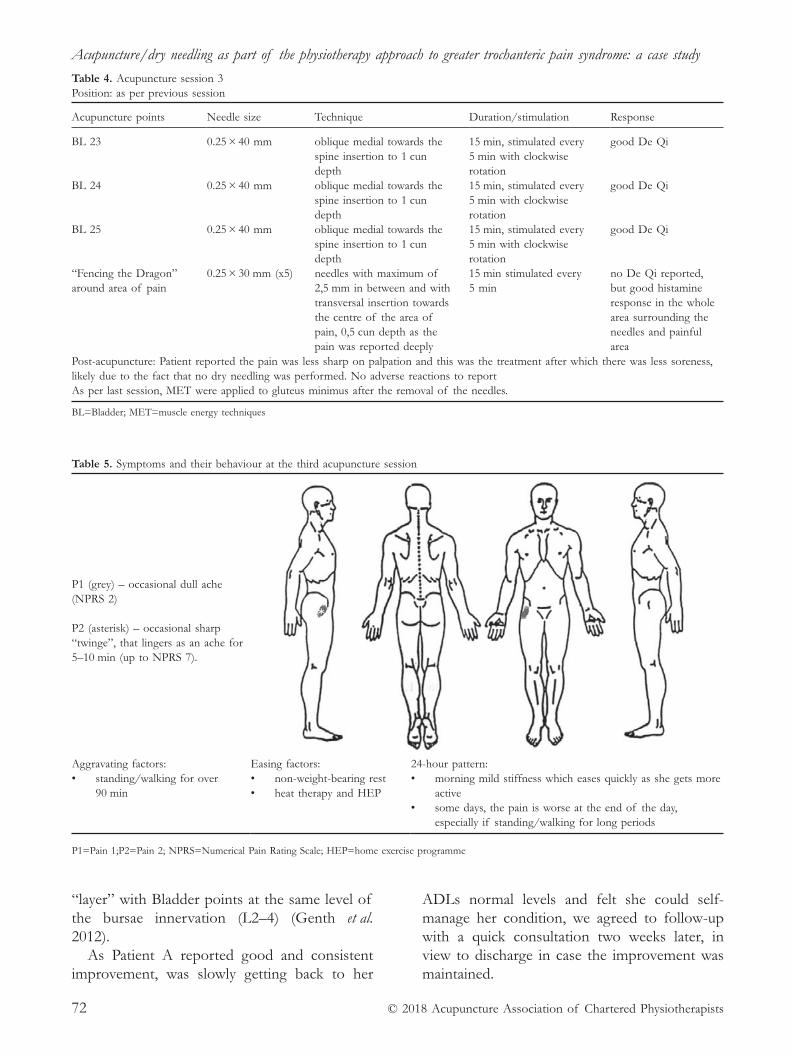
Acupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study
© 2018 Acupuncture Association of Chartered Physiotherapists72
“layer” with Bladder points at the same level of the bursae innervation (L2–4) (Genth et al. 2012).
As Patient A reported good and consistent improvement, was slowly getting back to her
ADLs normal levels and felt she could self- manage her condition, we agreed to follow- up with a quick consultation two weeks later, in view to discharge in case the improvement was maintained.
Table 4. Acupuncture session 3Position: as per previous session
Acupuncture points Needle size Technique Duration/stimulation Response
BL 23 0.25 × 40 mm oblique medial towards the spine insertion to 1 cun depth
15 min, stimulated every 5 min with clockwise rotation
good De Qi
BL 24 0.25 × 40 mm oblique medial towards the spine insertion to 1 cun depth
15 min, stimulated every 5 min with clockwise rotation
good De Qi
BL 25 0.25 × 40 mm oblique medial towards the spine insertion to 1 cun depth
15 min, stimulated every 5 min with clockwise rotation
good De Qi
“Fencing the Dragon” around area of pain
0.25 × 30 mm (x5) needles with maximum of 2,5 mm in between and with transversal insertion towards the centre of the area of pain, 0,5 cun depth as the pain was reported deeply
15 min stimulated every 5 min
no De Qi reported, but good histamine response in the whole area surrounding the needles and painful area
Post- acupuncture: Patient reported the pain was less sharp on palpation and this was the treatment after which there was less soreness, likely due to the fact that no dry needling was performed. No adverse reactions to report As per last session, MET were applied to gluteus minimus after the removal of the needles.
BL=Bladder; MET=muscle energy techniques
Table 5. Symptoms and their behaviour at the third acupuncture session
P1 (grey) – occasional dull ache (NPRS 2)
P2 (asterisk) – occasional sharp “twinge”, that lingers as an ache for 5–10 min (up to NPRS 7).
Aggravating factors:• standing/walking for over
90 min
Easing factors:• non- weight- bearing rest• heat therapy and HEP
24- hour pattern:• morning mild stiffness which eases quickly as she gets more
active• some days, the pain is worse at the end of the day,
especially if standing/walking for long periods
P1=Pain 1;P2=Pain 2; NPRS=Numerical Pain Rating Scale; HEP=home exercise programme
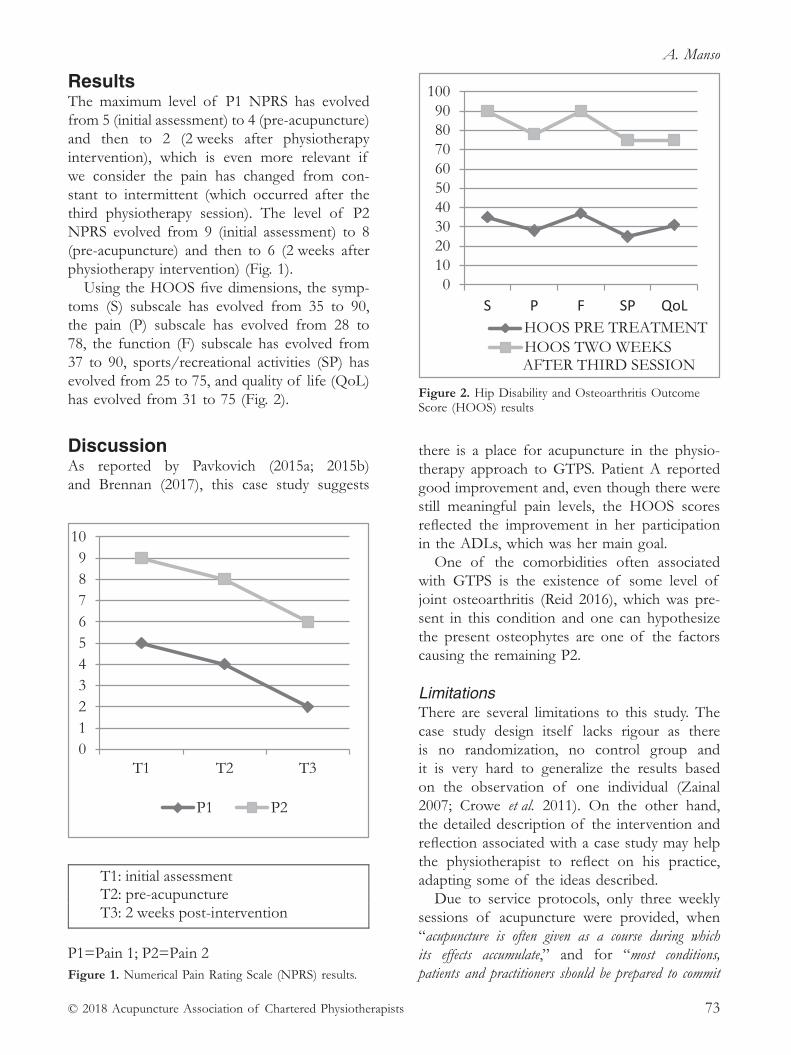
A. Manso
© 2018 Acupuncture Association of Chartered Physiotherapists 73
resultsThe maximum level of P1 NPRS has evolved from 5 (initial assessment) to 4 (pre- acupuncture) and then to 2 (2 weeks after physiotherapy intervention), which is even more relevant if we consider the pain has changed from con-stant to intermittent (which occurred after the third physiotherapy session). The level of P2 NPRS evolved from 9 (initial assessment) to 8 (pre- acupuncture) and then to 6 (2 weeks after physiotherapy intervention) (Fig. 1).
Using the HOOS five dimensions, the symp-toms (S) subscale has evolved from 35 to 90, the pain (P) subscale has evolved from 28 to 78, the function (F) subscale has evolved from 37 to 90, sports/recreational activities (SP) has evolved from 25 to 75, and quality of life (QoL) has evolved from 31 to 75 (Fig. 2).
Discussion As reported by Pavkovich (2015a; 2015b) and Brennan (2017), this case study suggests
there is a place for acupuncture in the physio-therapy approach to GTPS. Patient A reported good improvement and, even though there were still meaningful pain levels, the HOOS scores reflected the improvement in her participation in the ADLs, which was her main goal.
One of the comorbidities often associated with GTPS is the existence of some level of joint osteoarthritis (Reid 2016), which was pre-sent in this condition and one can hypothesize the present osteophytes are one of the factors causing the remaining P2.
LimitationsThere are several limitations to this study. The case study design itself lacks rigour as there is no randomization, no control group and it is very hard to generalize the results based on the observation of one individual (Zainal 2007; Crowe et al. 2011). On the other hand, the detailed description of the intervention and reflection associated with a case study may help the physiotherapist to reflect on his practice, adapting some of the ideas described.
Due to service protocols, only three weekly sessions of acupuncture were provided, when “acupuncture is often given as a course during which its effects accumulate,” and for “most conditions, patients and practitioners should be prepared to commit Figure 1. Numerical Pain Rating Scale (NPRS) results.
Figure 2. Hip Disability and Osteoarthritis Outcome Score (HOOS) results
Acupuncture/dry needling as part of the physiotherapy approach to greater trochanteric pain syndrome: a case study
© 2018 Acupuncture Association of Chartered Physiotherapists74
themselves to a course of about six to eight treatments”. However, “some MTrPs and other soft tissue injuries may respond after just one or two treatments” (White et al. 2008, p. 151).
The inclusion of acupuncture as part of a multi- faceted treatment plan may result in the inability to identify the contribution and merits of each of the parts but, as suggested by Wilson (2017), one can argue that the same multi- modal nature of the approach can be part of the reason for its success.
Alternative acupuncture approachesReflecting on the chosen intervention, the tech-nique known as “periosteal pecking” could have been used at the distal insertion of the glutmin and glutmed, as it has been showing promising results in clinical practice (Hanson et al. 2008) and suggested by a significant part of a group of 15 experts for the treatment of tendinopathy (Webster- Harrison et al. 2002).
Furthermore, additional Bladder points (BL 19- BL 23) could have been used to influence the sympathetic outflow to the lower limbs (Bradnam 2007) on the second treatment, in order to achieve normalization of the glutmin/glutmed tone, possibly facilitating gradual muscle/tendon loading and function recovery.
Future researchReflecting on this case and considering GTPS incidence, research focusing on the effects of dry needling versus acupuncture, needling techniques and physiotherapy versus needling alone, versus physiotherapy alone, would help understand the contribution of each of these parts and in planning how much of and which components to include in each specific case. Additionally, it would be interesting to better understand periosteal pecking in tendon pathol-ogy and its comparison with other modalities, such as SWT.
AcknowledgementsI’d like to acknowledge the patient for her com-pliance and availability throughout this process. I’d also like to acknowledge Andrew Oliver
for his inspiring and very approachable way of teaching. Finally, I’d like to thank my fiancée for her support and patience as I stuck needles into her in the name of professional development.
referencesAcupuncture Association of Chartered Physiotherapists
(AACP) (2017a) AACP Acupuncture Foundation Course Manual. AACP, Peterborough.
Acupuncture Association of Chartered Physiotherapists (AACP) (2017b), Safe Practice Guidelines for Acupuncture Physiotherapists, V3. AACP, Peterborough.
Bradnam L. (2007) A proposed clinical reasoning model for Western acupuncture. Journal of the Acupuncture Association of Chartered Physiotherapists Spring 2007, 21–30.
Brennan K. L., Allen, B. C. & Maldonado, Y. M. (2017) Dry needling versus cortisone injection in the treatment of greater trochanteric pain syndrome: a noninferiority randomized clinical trial. Journal of Orthopaedic and Sports Physical Therapy 47 (4), 232–239.
Crowe S., Cresswell K., Robertson A., et al. (2011) The case study approach. BMC Medical Research Methodology 11 (100).
Deadman P., Al- Khafaji M. & Baker K. (2017) A Manual of Acupuncture. [WWW document.] http://www.amanual ofacupuncture.com [Accessed October 2017–January 2018].
Dommerholt J. & Fernandez- de- las- Peñas C. (2013) Trigger Point Dry Needling. An Evidenced and Clinical- Based Approach, 1st edn. Churchill Livingstone/Elsevier, London.
Genth B., Von During M., Von Engelhardt L. V., et al. (2012) Analysis of the sensory innervation of the greater trochanter for innovating the treatment of the greater trochanteric pain syndrome. Clinical Anatomy 25 (8), 1080–1086.
Hanson Y., Carlsson C. & Olsson E. (2008) Intramuscular and periosteal acupuncture in patients suffering from chronic musculoskeletal pain – a controlled trial. Acupuncture in Medicine 26 (4), 214–223.
Klauser A. S., Martinoli C., Tagliafico A., et al. (2013) Greater trochanteric pain syndrome. Seminars in Musculoskeletal Radiology 17 (1), 43–48.
Lewit K. (1979) The needle effect in the relief of myo-fascial pain. Pain 6 (1), 83–90.
Mistry J. B., Jauregui J. J., Lerner A. L., et al. (2016) An assessment of the comprehensiveness of various hip outcome scores. Surgical Technology International 28, 267–274.
Pavkovich R. (2015a) Effectiveness of dry needling, stretching, and strengthening to reduce pain and improve function in subjects with chronic lateral hip and thigh pain: a retrospective case series. International Journal of Sports Physical Therapy 10 (4), 540–551.

A. Manso
© 2018 Acupuncture Association of Chartered Physiotherapists 75
Pavkovich R. (2015b) The use of dry needling for a subject with chronic lateral hip and thigh pain: a case report. International Journal of Sports Physical Therapy 10 (2), 246–255.
Reid D. (2016) The management of greater trochanteric pain syndrome: a systematic literature review. Journal of Orthopaedics 13 (1), 15–28.
Roos E. (2008) HOOS User’s Guide 2003 (updated May 2008) Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark [WWW document.] www.koos.nu [Accessed November 2017- January 2018].
Sandberg M., Lundberg T., Lindberg L.- G. & Gerdle B. (2003) Effects of acupuncture on skin and muscle blood flow in healthy subjects. European Journal of Applied Physiology 90 (1–2), 114–119.
Shbeeb M. I. & Matteson E. L. (1996) Trochanteric bursitis (greater trochanter pain syndrome). Mayo Clinic Proceedings 71 (6), 565–569.
Webster- Harrison P., White A. & Rae J. (2002) Acupuncture for tennis elbow: an email consensus study to define a standardized treatment in a GP’s surgery. Acupuncture in Medicine 20 (4), 181–185.
White A., Cummings M. & Filshie J. (2008) An Introduction to Western Medical Acupuncture. Churchill Livingstone/Elsevier, Edinburgh.
Wilson J. (2017) Acupuncture for low back pain in a professional footballer. Acupuncture in Physiotherapy 29 (2), 59–64.
Yeganeh Lari, A., Okhovatian F., Naimi S. S. & Baghban, A. A. (2016) The effect of the combination of dry needling and MET on latent trigger point upper trape-zius in females. Manual Therapy, 21, 204–209.
Zainal Z. (2007) Case study as a research method. Jurnal Kemanusiaan 5 (1), 1–6.
André Manso graduated as a physiotherapist in Portugal and has worked in the UK over the last four years. He has always kept an enthusiastic interest in musculo-skeletal conditions as he worked in public, medico- legal, private and sports settings and, even though his practice is mostly clinical, he is keen to have permanent contact with the academic side of physiotherapy. André is a member of the Chartered Society of Physiotherapy and the Acupuncture Association of Chartered Physiotherapists, and currently works in Basingstoke in the local NHS musculoskeletal physiotherapy service.

© 2018 Acupuncture Association of Chartered Physiotherapists 77
Correspondence: Justin Walsh, Crystal Palace Physio Group, Jubilee Stand, Crystal Palace Park, London SE19 2BB, UK ([email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 77–82
CASE rEPOrTS
left elbow lateral epicondylalgia, treated successfully with acupuncture combined with typical physiotherapy intervention
J. walshCrystal Palace Physio Group, London, UK
AbstractThis case study documents the use of acupuncture in addition to typical physiotherapy modalities in the management of a 41- year- old manual worker with lateral epicondylalgia (tennis elbow). The patient responded well to the intervention, with subjective improve-ments on functional scales, as well as objective improvements in pain- free grip strength. Acupuncture appeared to provide a worthwhile reduction in pain within at least the short- to medium- terms, although the true effect of acupuncture cannot be fully understood from this case study as other modalities were also used. Nevertheless, the case presents a com-prehensive description of the successful management of a patient with lateral epicondylalgia where acupuncture was effectively included and was likely to have played a positive role.
Keywords: acupuncture, lateral epicondylalgia, physiotherapy, tennis elbow.
IntroductionLateral epicondylalgia is a musculoskeletal condi-tion affecting the lateral elbow, most commonly due to mechanical overload of the relevant tissues. The pathophysiology of the condition is characterized by tendinopathy at the com-mon extensor origin, where the tendons of the forearm extensors are affected, in particular the extensor carpi radialis brevis tendon. Fibre necrosis, abnormal blood vessel infiltration and matrix substance infiltration stimulate periten-dinous nociceptors, resulting in pain (Khan & Cook 2000).
Numerous treatments have been described in the literature for lateral epicondylalgia, includ-ing rest, nonsteroidal anti- inflammatory drugs (NSAIDs) (Green et al. 2001), corticosteroid injections (Coombes et al. 2010), strength-ening exercises (Tyler et al. 2010), forearm bracing (Calfee et al. 2008) and mobilization
with movement techniques (Vicenzino et al. 2007).
A systematic review (Trinh et. al. 2004) has described acupuncture as an effective modality for the short- term relief of lateral epicondyl algia pain. The relief of pain in the short term is an important consideration in the treatment of lat-eral epicondylalgia, as it is likely to assist in the patient’s compliance to physiotherapy appoint-ments and home exercise programmes. This can assist the therapist to introduce and progress an appropriate tendon loading programme, which is considered the mainstay of treatment for long- term relief of any tendinopathy (Cook & Purdam 2009).
There are numerous studies demonstrating this pain relieving effect of acupuncture in lat-eral epicondylalgia. Fink et al. (2002) compared acupuncture to sham acupuncture (5 cm away from true acupuncture points and avoiding Ah Shi and trigger points). They demonstrated greater reductions in pain within the acu-puncture group at 2 weeks, with both groups demonstrating pain reductions that were not
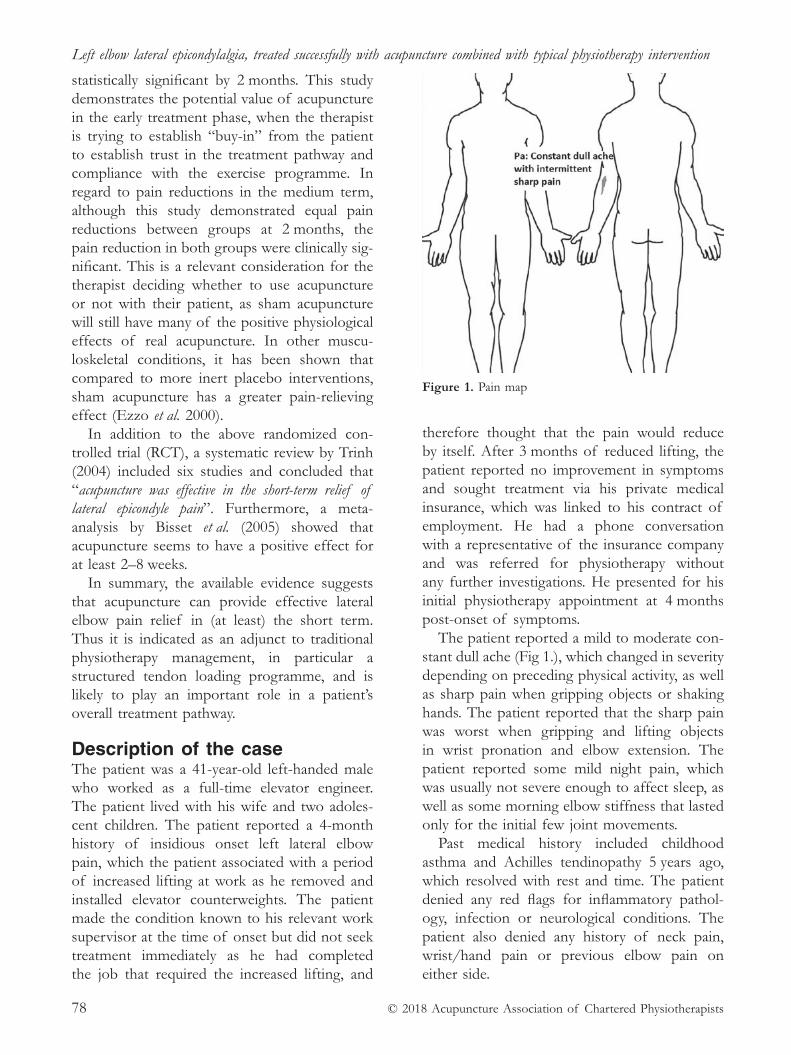
Left elbow lateral epicondylalgia, treated successfully with acupuncture combined with typical physiotherapy intervention
© 2018 Acupuncture Association of Chartered Physiotherapists78
statistically significant by 2 months. This study demonstrates the potential value of acupuncture in the early treatment phase, when the therapist is trying to establish “buy- in” from the patient to establish trust in the treatment pathway and compliance with the exercise programme. In regard to pain reductions in the medium term, although this study demonstrated equal pain reductions between groups at 2 months, the pain reduction in both groups were clinically sig-nificant. This is a relevant consideration for the therapist deciding whether to use acupuncture or not with their patient, as sham acupuncture will still have many of the positive physiological effects of real acupuncture. In other muscu-loskeletal conditions, it has been shown that compared to more inert placebo interventions, sham acupuncture has a greater pain- relieving effect (Ezzo et al. 2000).
In addition to the above randomized con-trolled trial (RCT), a systematic review by Trinh (2004) included six studies and concluded that “acupuncture was effective in the short- term relief of lateral epicondyle pain”. Furthermore, a meta- analysis by Bisset et al. (2005) showed that acupuncture seems to have a positive effect for at least 2–8 weeks.
In summary, the available evidence suggests that acupuncture can provide effective lateral elbow pain relief in (at least) the short term. Thus it is indicated as an adjunct to traditional physiotherapy management, in particular a structured tendon loading programme, and is likely to play an important role in a patient’s overall treatment pathway.
Description of the caseThe patient was a 41- year- old left- handed male who worked as a full- time elevator engineer. The patient lived with his wife and two adoles-cent children. The patient reported a 4- month history of insidious onset left lateral elbow pain, which the patient associated with a period of increased lifting at work as he removed and installed elevator counterweights. The patient made the condition known to his relevant work supervisor at the time of onset but did not seek treatment immediately as he had completed the job that required the increased lifting, and
therefore thought that the pain would reduce by itself. After 3 months of reduced lifting, the patient reported no improvement in symptoms and sought treatment via his private medical insurance, which was linked to his contract of employment. He had a phone conversation with a representative of the insurance company and was referred for physiotherapy without any further investigations. He presented for his initial physiotherapy appointment at 4 months post- onset of symptoms.
The patient reported a mild to moderate con-stant dull ache (Fig 1.), which changed in severity depending on preceding physical activity, as well as sharp pain when gripping objects or shaking hands. The patient reported that the sharp pain was worst when gripping and lifting objects in wrist pronation and elbow extension. The patient reported some mild night pain, which was usually not severe enough to affect sleep, as well as some morning elbow stiffness that lasted only for the initial few joint movements.
Past medical history included childhood asthma and Achilles tendinopathy 5 years ago, which resolved with rest and time. The patient denied any red flags for inflammatory pathol-ogy, infection or neurological conditions. The patient also denied any history of neck pain, wrist/hand pain or previous elbow pain on either side.
Figure 1. Pain map

J. Walsh
© 2018 Acupuncture Association of Chartered Physiotherapists 79
Physical examination revealed full range of motion of the hand, wrist, elbow, shoulder and cervical spine. Cervical quadrants and Spurling’s were negative. The patient had pain on palpation of the left lateral epicondyle and proximal 2 cm of the extensor tendons. Both stretching as well as loading of the extensor tendons reproduced the patient’s symptoms. Pain- free grip strength (PFGS) (grip strength to the first onset of pain) with the elbow flexed to 90º and the forearm in mid- prone was measured at 4.5 kg vs 48.2 kg for the left and right respectively. With the elbow extended and the forearm pronated, pain- free grip strength was 1.4 kg vs 51.2 kg for the left and right respectively. The patient had mild reproduction of pain on upper limb neural tension testing (radial nerve bias), but no reduc-tion in neural range of motion. The patient completed the patient specific functional scale questionnaire (PSFS), with an initial result of 3/10 (note: 0/10 = total impairment; 10/10 = no impairment).
As outlined in the table, a multimodal treat-ment approach was taken. This included educa-tion and advice regarding the presenting com-plaint and activity modification, prescription of a counterforce brace, mobilization, acupuncture and a home exercise programme of tendon loading exercises.
Treatment Treatment 1 (week 0)Rationale for prescription used in treatment 1: As this was the patient’s first experience with acupuncture, the number of points selected was limited to four and all were local to the injured area. This was to introduce the patient to acupuncture gently and gauge sensitivity. The local points were selected to stimulate A–δ and C fibres in order to encourage the release of calcitonin gene- related peptides (CGRP), substance P and neurokinin. Through these mechanisms, acupuncture can stimulate: 1) local vasodilation and increased vascular permeability (Sandberg et al. 2003), which may have a posi-tive effect on pain and healing due to increased blood flow to the treatment site; 2) peripheral opioid analgesia (Stein et al. 2001), which may
reduce the patient’s pain 2–3 days following treatment.
As well as the low number and localization of needles, the treatment duration was limited to 10 min, and 0.25 mm needles were used, which was also to ensure the treatment dose was low to begin with.
Treatment 2 (week 1)Subjective: After the initial treatment 1 week ago, the patient reported he had a mild increase in pain for 24 hours, followed by a modest reduction in pain.
Objective: When outcome measures were reas-sessed, PFGS with the elbow flexed to 90º and the forearm in mid- prone had increased to 15.1 kg for the left hand. With the elbow extended and the forearm pronated, PFGS had increased to 5.1 kg. PSFS remained at 3/10.
Rationale for prescription used in treatment 2: Due to the improvement in outcome measures and the lack of adverse reaction to treatment, it was decided to progress treatment, includ-ing acupuncture dose. Needling duration was increased to 15 min, with stimulation at 5 and 10 min. Large Intestine (LI) 4 was also added to increase distal stimulation, which has been suggested to activate supraspinal mechanisms and result in descending pain inhibition from the periaqueductal grey matter and the release of natural opioids (Bradnam 2003; Zhao 2008). This analgesic mechanism is also thought to be important for longer- term effects (Lundeberg 1998). Traditional Chinese medicine considers LI 4 to be a master point for pain and relaxa-tion because it is a distal point along the Large Intestine meridian (White et al. 2008).
Treatment 3 (week 2)Subjective: After the second treatment 1 week ago, the patient again reported a mild increase in pain for 24 hours before a proceeding reduction.
Objective: When outcome measures were re assessed, PFGS with the elbow flexed to 90º and the forearm in mid- prone had increased
Left elbow lateral epicondylalgia, treated successfully with acupuncture combined with typical physiotherapy intervention
© 2018 Acupuncture Association of Chartered Physiotherapists80
further to 22.4 kg for the left hand. With the elbow extended and the forearm pronated, PFGS had also further increased to 7.2 kg. PSFS began to demonstrate change, with an improvement to 5/10.
Rationale for prescription used in treatment 3: Due to further improvement and no adverse reaction, it was decided to progress treatment again, including acupuncture dose. Triple Energizer (TE) 5 was added to take the total number of needles to six. TE 5 was chosen to increase the stimulation along the same dermat-ome as the affected area. This had the intention of increasing dermatomal receptive input in the dorsal horn of the spinal cord and increase endogenous pain modulatory systems (Carlsson 2002; Bradnam 2003). To further progress dose, the needles were also stimulated twice rather than once, at 5 and 10 min.
Treatment 4 (week 4)Subjective: After the third treatment 2 weeks ago, the patient reported no post- treatment soreness and continued to report reductions in pain. The patient did report some mild, inter-mittent “tightness” developing in the region of the forearm extensor muscle bellies, possibly an effect of the loading exercise progressions.
Objective: When outcome measures were reas-sessed, PFGS with the elbow flexed to 90º and the forearm in mid- prone had increased further to 40.3 kg for the left hand. With the elbow extended and the forearm pronated, PFGS had also further increased to 17.3 kg. PSFS also improved to 7/10.
Rationale for prescription used in treatment 4: Due to further improvement and no adverse reaction, as well as a muscular type “tightness” reported by the patient, it was decided to add two needles to the belly of the extensor mus-cles. Two active trigger points were identified along the extensor muscle compartment and a needle was inserted into each, using a fanning technique of repeated penetration while chang-ing the direction of the needle until a twitch response was elicited. It has been proposed
that trigger point needling can reduce hyper-activity of the muscle spindle and therefore the stretch reflex, decreasing acetylcholine release and reducing unnecessary muscle contraction (Norris 2001), in turn reducing the ischaemia which can cause muscle pain.
In addition to the addition of trigger point therapy, the dose was also increased through the use of 0.30 mm needles for all the acupuncture points (with the exception of LI 4 and the new trigger point needles).
Treatment 5 (week 6)Subjective: After the fourth treatment 2 weeks ago, the patient reported no post- treatment soreness and continued to report reductions in pain and return to normal activities at home and work.
Objective: When outcome measures were reas-sessed, PFGS with the elbow flexed to 90º and the forearm in mid- prone was now pain free at 46.2 kg for the left hand. With the elbow extended and the forearm pronated, PFGS was now 40.1 kg, eliciting only very mild pain. PSFS was now 9/10.
Rationale for prescription used in treatment 5: The patient was keen to continue the home exercise programme and make this treatment his final appointment. Due to the positive response from the fourth treatment and the fact that the patient would not be followed- up after the fifth treatment, it was decided to repeat the same acupuncture intervention provided in the fourth treatment.
The patient will be followed- up via email in a further 4 weeks (after the submission of this case report) to ensure he is still on track for a full resolution of symptoms.
DiscussionThe patient responded well to the physiother-apy treatment provided, which included acu-puncture. Subjective improvements in function were demonstrated over the treatment period with a change in PSFS from 3/10 to 9/10. This was accompanied by objective improvements

J. Walsh
© 2018 Acupuncture Association of Chartered Physiotherapists 81
demonstrated by the change in pain- free grip strength from 1.4 kg to 40.1 kg with the elbow extended and wrist pronated.
Due to the multi- modal treatment applica-tion, it is hard to isolate the positive effect of the acupuncture from the other treatments applied. The patient received a structured and graded tendon loading programme in paral-lel with his acupuncture treatment. There is evidence for the effectiveness of loading pro-grammes in lateral epicondylalgia and therefore this may be the main reason for the patient’s improvement. In this evidence, however, treat-ment effects from loading programmes do not tend to occur until at least the 6–8 week mark and often not until 12–24 weeks. As described above, this patient received a modest pain relief as early as 24 h following the initial session and was reporting lasting pain relief within the first few weeks. This does seem to support the efficacy of acupuncture in this patient, however it must be mentioned that activity modification and prescription of the counterforce brace may have also contributed strongly to this effect.
Alternative acupuncture approachesThe acupuncture protocol used with this patient was chosen based on a combination of evidence from the literature, physiological rationale and patient response. Other methods have been described in the literature and could have been used with this patient. Molsberger & Hille (1994) describe an alternative treatment protocol that utilizes the pain- relieving effects of a non- segmental distal point (Gall Bladder 34) on the ipsilateral leg to the affected lateral epicondyle. The needle was inserted to 2 cm depth and stimulated until De Qi was elicited while the patient performed movements with the painful arm. This resulted in a 55% pain reduction for an average of 20 h in the inter-vention group. This method could have been used as an alternative if the patient tolerated the local acupuncture poorly or had other local contraindications to acupuncture in the area, such as skin scarring or cutaneous nerve compromise. Another technique that could have been used was periosteal pecking, whereby a needle is inserted into the area of the lateral
epicondyle and thrusted several times to touch the periosteum at the insertion of the extensor tendons. If the patient was unresponsive to the treatment described above and the acupuncture thus far was well tolerated, I would have consid-ered using this technique.
Future research considerationsWhen investigating the use of acupuncture with this patient, it was clear that the overall body of evidence for acupuncture in the management of lateral epicondylalgia is limited, with only a small number of good quality RCTs. Therefore, further trials would be of value to strengthen the understanding of this intervention. In addition, further research with longer term follow- ups would be valuable due to the high recurrence rates of lateral epicondylalgia. Research explor-ing this question would be worthwhile to assess whether acupuncture in combination with a tendon loading programme resulted in a lower recurrence rate than a loading programme alone, as well as compared to other interventions such as corticosteroid injection. As is the case with the use of acupuncture in other pathologies, much of the lateral epicondylalgia research is complicated by the lack of a true therapeutically inert placebo comparison. Further RCTs which utilize a truly passive placebo would be of value to further tease out the benefit of acupuncture as an intervention.
referencesBisset L., Paungmali A. & Vicenzino B., et al. (2005) A
systematic review and meta- analysis of clinical trials on physical interventions for lateral epicondylalgia. British Journal of Sports Medicine 39 (7), 411–422.
Bradnam L. (2003) A proposed clinical reasoning model for Western acupuncture. New Zealand Journal of Physiotherapy 31 (1), 40–45.
Calfee R. P., Patel A., DaSilva M. F. & Akelman E. (2008) Management of lateral epicondylitis: current concepts. Journal of the American Academy of Orthopaedic Surgeons 16 (1), 19–29.
Carlsson C. (2002) Acupuncture mechanisms for clini-cally relevant long- term effects- reconsideration and a hypothesis. Acupuncture in Medicine 20 (2–3), 82–99.
Cook J. L & Purdam C. R. (2009) Is tendon pathology a continuum? A pathology model to explain the clini-cal presentation of load- induced tendinopathy. British Journal of Sports Medicine 43 (6) 409–16.

Left elbow lateral epicondylalgia, treated successfully with acupuncture combined with typical physiotherapy intervention
© 2018 Acupuncture Association of Chartered Physiotherapists82
Coombes B. K., Bisset L. & Vicenzino B. (2010) Efficacy and safety of corticosteroid injections and other injec-tions for management of tendinopathy: a systematic review of randomized controlled trials. The Lancet 376 (9754), 1751–1767.
Ezzo J., Berman B., Hadhazy V. A., et al. (2000) Is acu-puncture effective for the treatment of chronic pain? A systematic review. Pain 86 (3), 217–225.
Fink M., Wolkenstein E., Karst M. & Gehrke A. (2002) Acupuncture in chronic epicondylitis: a randomized controlled trial. Rheumatology 41 (2), 205–209.
Green S., Buchbinder R., Barnsley L., et al. (2001) Nonsteroidal anti- inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database of Systematic Reviews, Issue 4. Art. No.: CD003686. DOI:10.1002/14651858.CD003686.
Khan K. M. & Cook J. L. (2000) Overuse tendon injuries: where does the pain come from? Sports Medicine and Arthroscopy Review 8 (1), 17–31.
Lundeberg T. (1998) The physiological basis of acupunc-ture. Conference presentation, MANZ/PAANZ Annual Conference, Christchurch, New Zealand, August 1998.
Molsberger A. & Hille E. (1994) The analgesic effect of acupuncture in chronic tennis elbow pain. British Journal of Rheumatology 33 (12), 1162–1165.
Norris C. M. (2001) Acupuncture: Treatment of Musculoskeletal Conditions. Butterworth- Heinemann, Oxford.
Sandberg M., Lundeberg T., Lindberg L. G. & Gerdle B. (2003) Effects of acupuncture on skin and muscle blood flow in healthy subjects. European Journal of Applied Physiology 90 (1–2), 114–119.
Stein C., Machelska H. & Schäfer M. (2001) Peripheral analgesic and anti- inflammatory effects of opioids. Zeitschrift fur Rheumatologie 60 (6), 416–24.
Trinh K. V., Phillips S. D., Ho E. & Damsma K. (2004) Acupuncture for the alleviation of lateral epicon-dyle pain: a systematic review. Rheumatology 43 (9), 1085–1090.
Tyler T. F., Thomas G. C., Nicholas S. J. & McHugh M. P. (2010) Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epi-condylosis: a prospective randomized trial. Journal of Shoulder and Elbow Surgery 19 (6), 917–922.
Vicenzino B., Cleland J. A. & Bisset L. (2007) Joint manipulation in the management of lateral epicon-dylalgia: a clinical commentary. Journal of Manual and Manipulative Therapy 15 (1), 50–56.
White A., Cummings M., Filshie J. (2008) An Introduction to Western Medical Acupuncture. Churchill Livingstone/Elsevier, Edinburgh.
Zhao Z.- Q. (2008) Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology 85 (4), 355–375.
Justin Walsh is a physiotherapist with experience of working in the public and private sectors of both the United Kingdom and Australia and is currently work-ing within the private sector in south east London. He has a particular interest in treating musculoskeletal injuries, including tendinopathy.

© 2018 Acupuncture Association of Chartered Physiotherapists 83
Correspondence: Diana Giura, Physiotherapy Department, Coalville Community Hospital, Broom Leys Road, Coalville, Leicester, LE67 4DE (email: [email protected])
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 83–86
CASE rEPOrTS
The use of Seirin Pyonex indwelling needles in the treatment of non- traumatic low back pain – a case study
D. GiuraPhysiotherapy Department, Coalville Community Hospital, Leicestershire, UK
AbstractMany people suffer at one time or another with lower back pain. Treatments used over the years have varied from advice to rest on the bed, medication, consultants and, eventually, a referral to our profession. Since the start of the NHS, 70 years ago, we have managed to gain respect as a profession and to be trusted in our assessments and treatments. We have been careful to keep in mind evidence- based practice (EBP) as we justify our reasoning. The AACP has fought and will continue to fight to keep acupuncture within the guidelines. We all know acupuncture works and, mostly, how, and yet commissioners find it expensive, time consuming and poorly supported by the research.
Lower back pain (LBP) has multiple causes. In the light of the National Institute for Health and Care Excellence (NICE) 2016 guideline on low back pain, acupuncture has been used less in its treatment, mostly in favour of more medication, although the experience of physiotherapists has shown this treatment method can be effective. This case study presents one of the cases the author has treated with Seirin Pyonex indwelling needles (SPIDN) over the last few years.
Keywords: AACP, acupuncture, indwelling needles, low back pain, Pyonex needles.
IntroductionThe most common use of indwelling needles is for auricular acupuncture. In 1999, Ernst and White published an article in the BMJ about reported side effects post- acupuncture. Indwelling needles were reported to be respon-sible for auricular perichondritis and cardiac tamponade. Since then, indwelling needles have been widely used to treat addictions and general pain, using the auricular points. Due to the sites of the needle insertion when using body points, the patients were thought to be more prone
to infection than with normal acupuncture. Auricular acupuncture was preferred on some occasions, due to the closer connection with the central nervous system.
Newton stated: “for every action, there is an equal and opposite reaction” (the third law of physics). Simplify this and then apply this to the nerv-ous system. As we now know, any skin surface stimulus will cause a reaction at the central nervous system level, which in turn will create a response at the level of stimulus. Of course, these connections are many and very fast due to the nature of the fibres that transfer the information between systems.
In 2013, Nitta published a review of indwell-ing Japanese needles in the AACP journal. The literature discussed in this review was of variable
The use of Seirin Pyonex indwelling needles in the treatment of non- traumatic low back pain
© 2018 Acupuncture Association of Chartered Physiotherapists84
quality and variable outcomes were reported. However, there does seem to be some reason-ably strong evidence to support the use of indwelling needles (IDNs) in the treatment of post- operative pain (Kotani et al. 2001) and post- operative nausea (Andrzejowski & Woodward 1996). There is also weak evidence to support the use of IDNs in breathlessness (Filshie et al. 1996; Davis et al. 2001), and some to suggest that IDNs can be used as a self- acupuncture treat-ment to prolong the effects of needling (Filshie et al. 1996; 2005) or as an independent treatment (Longbottom 2010). All of the authors reviewed agreed that IDNs are a convenient, practical, cost- effective and efficient method of applying acupuncture when used appropriately and with all aspects of safety considered.
Part of this therapist’s work was, and still is, based on the use of these needles in different situations. Since then, the SPIDN have been used for different problems such as labour and caesarean section, child constipation, etc.
There are only a few SPIDN sizes, from 0.6 mm to 1.5 mm needle length, on a 0.20 mm diameter. The ones this therapist usually uses are 0.20 mm x 0.6 mm, for the treatment of lower back pain, tennis and golfer’s elbow, whiplash, sprains etc. The following is a description of the treatment of a case of acute non- traumatic lower back pain.
Case studyPatient profileA 37- year- old male who was on the floor for a few hours playing with his son. He stood up and felt a twinge in the left side of his back.
He rested for 2 days, using a hot water bottle and hot baths. However, there was no improve-ment and his condition started to deteriorate. He did not attend his GP as there were no appointments for a few days. He took no medi-cation as he was fasting.
The patient was normally fit and well, and would go to the gym where he worked on his upper body using weights and ran on the treadmill.
He now found it difficult to sit, and was observed sitting very close to the edge of the
chair in reception. He asked if he could stand during the session due to his pain. He was due to fly out for pilgrimage to Mecca in 2 weeks. He had difficulty driving, so was brought to the first treatment session by his wife.
Examination was difficult due to his pain, therefore the therapist concentrated on his immediate goal that day, which was to be able to sit. The pain scale was 9–10/10 (where 10 is the highest pain and zero is no pain).
The patient was afraid of needles, however he consented to the Pyonex needles after dem-onstration and explanation.
A verbal consent was gained, and the acu-puncture consent form was signed before the treatment commenced.
First treatmentExtra points were used on the patient’s left hand: EX- UE- 7 (Yaotongdian). The patient was asked to move gently for 5 min. The pain score reported was 7–8/10. At this point, the thera-pist was able to assess his standing and sitting flexion. Positive standing flexion was discovered on his left side. The patient was asked if he could lie down so the therapist could release the tissue. He managed to do so for 10 min. After tissue release, the therapist reassessed standing flexion. The patient was still in pain and had difficulties sitting for more than 30 s. Pyonex needles were applied on the side of the pain reported by patient. The number of needles applied at the side was five. The patient was asked again to move gently. His reported pain was now 5/10. He was able to sit for 5 min but had discomfort on standing. He was sent home with gentle back stretchings taught by therapist and advised on Pyonex needle management.
Second treatmentThe second treatment followed four days after the first. The patient managed to drive himself to work and to the clinic. He reported he was doing the exercises as advised and that he felt the combination of the exercises and the indwelling needles helped, however he was still anxious as he was due to fly soon. Sitting and standing flexion were re- assessed, and both were found to be negative. The patient’s reported pain was

D. Giura
© 2018 Acupuncture Association of Chartered Physiotherapists 85
4–5/10 and he was able to sit down during the initial conversation. The second treatment con-sisted of tissue mobilization and re- application of the indwelling needles at the side of the pain reported by the patient, which was now around L2- L5 left side - 4 needles at EX- B- 2 (Hua Tuo Jiaji points). As he was able to move more, a core stability exercise was added.
Third treatmentThe third treatment took place three days before the patient’s flight. He reported an improvement to 2/10 on the pain scale, how-ever he felt stiffer. On examination, his skin was fine, with no change in the skin condi-tion noticed post- Pyonex needles. No redness nor any allergic reaction was reported by the patient. He managed to keep the needles in as advised (3–5 days). Treatment consisted of tis-sue mobilization and application of K- tape to the left lumbar area. The patient was advised to continue with the exercises and stretchings to maintain his mobility.
DiscussionI have been using this type of needle for a while now. I do believe they have changed my practice. I have found them very effective in the early stages of musculoskeletal problems, and I recently realized that they can also be effective in the chronic stages. I also advise my patients to use them, although this could be controver-sial. The disposal of the needles can be done in a normal bin as the needle is so small and unlikely to produce any needle stick injury. Best practice would be to dispose of them in a regu-lar sharps box. However, for the longer needles the practitioner and the patient should be aware of the possibility of an injury if not disposed of appropriately.
I have to say that the patient’s initial reaction to the application of the Pyonex needles was better than expected. I feel that these needles can be a good way of using acupuncture for people who are nervous of needles. The success of the treatment also depends on the patient’s commitment to get better.
The use of Pyonex indwelling needles has become more popular in the last few years. The
US armed services have used both indwelling ear needles and the more usual type in bat-tlefield medicine (mostly dealing with acute pain.) (Niemtzow et al. 2015). In Japan, they can be bought by the public. In the UK there are no restrictions as you can buy them even from Amazon. The needles are also sold at the AACP conferences. However, the AACP does not seem to encourage the use of this type of needle.
In my experience during and after the use of this type of needle in an outpatient and even in an inpatient setting, I have not encountered any side effects in relation to infections at the needle site, nor any reaction to the needle or plaster. However, if the needles are kept in situ longer than advised, or the patient’s skin is not clean, there is a danger of infection (Longbottom 2010; Campbell & Hopwood 2007). I do not use the needles on frail skin or if the skin is not intact.
Personally, I feel that the AACP should review the policy as I’m convinced that there could be a benefit from indwelling needles.
referencesAndrzejowski J. & Woodward D. (1996) Semi- permanent
acupuncture needles in the prevention of post- operative nausea and vomiting. Acupuncture in Medicine 14 (2), 68–70.
Campbell A. & Hopwood V. (2007) Debate – patients should be encouraged to treat themselves. Journal of the Acupuncture Association of Chartered Physiotherapists Autumn 2007, 57–61.
Davis C. L., Lewith G. T., Broomfield J. & Prescott P. (2001) A pilot project to assess the methodological issues involved in evaluating acupuncture as a treat-ment for disabling breathlessness. Journal of Alternative and Complementary Medicine 7 (6), 633–639.
Ernst E. & White A. R. (1999) Indwelling needles carry greater risks than acupuncture techniques. [Letter.] BMJ 318 (7182), 536.
Filshie J., Penn K., Ashley S. & Davis C. L. (1996) Acupuncture for the relief of cancer- related breath-lessness. Palliative Medicine 10 (2), 145–150.
Kotani N., Hashimoto H., Sato Y., et al. (2001) Preoperative intradermal acupuncture reduces postoperative pain, nausea and vomiting, analgesic requirement, and sym-pathoadrenal responses. Anesthesiology 95 (2), 349–356.
Longbottom J. (2010) Clinical use of long- duration press needles. Journal of the Acupuncture Association of Chartered Physiotherapists Spring 2010, 91–92.

The use of Seirin Pyonex indwelling needles in the treatment of non- traumatic low back pain
© 2018 Acupuncture Association of Chartered Physiotherapists86
National Institute for Health and Care Excellence (NICE) (2016) Low Back Pain and Sciatica in Over 16s: Assessment and Management. NICE Clinical Guideline 59. National Institute for Health and Clinical Excellence, London.
Niemtzow R. C., Belard J.- L & Nogier R. (2015) Battlefield acupuncture in the U. S. military: a pain- reduction model for NATO. Medical Acupuncture 27 (5), 344–348.
Nitta S. (2013) Is there a place for Japanese- style body indwelling needle acupuncture in physiotherapy prac-tice? Journal of the Acupuncture Association of Chartered Physiotherapists Spring 2013, 51–59.
Diana Giura graduated as a physiotherapist in 2002. She is a member of the Health and Care Professions Council, the Chartered Society of Physiotherapists, the
Association of Chartered Physiotherapists Interested in Neurology and the Acupuncture Association of Chartered Physiotherapists (AACP). Diana is a Member of the AACP Board and its regional repre-sentative for the East Midlands. She studied Chinese at Beijing Language and Culture University, Beijing, China from 1999 to 2000 and then acupuncture at Beijing University of Chinese Medicine from 2000 to 2001. She has been a clinical educator for students on neurological placement from Coventry, Leicester and other universities since 2005. Diana completed her Master’s degree in 2009 and gained a Preparing to Teach in the Lifelong Learning Sector qualification in 2013.
© 2018 Acupuncture Association of Chartered Physiotherapists 87
Correspondence: Dan Atkinson, Physiotherapist, Multi Sport, English Institute of Sport, EIS/L Boro. Performance centre, 1st Floor, Loughborough University LE11 3TU, UK (email: [email protected])
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 87–93
CASE rEPOrTS
Acupuncture for pain relief in a patient following hip arthroscopic surgery
D. Atkinson English Institute of Sport, Loughborough, UK
AbstractAcupuncture was used as an alternative modality for pain relief in a patient 8 weeks after hip arthroscopic surgery. Acupuncture was found to be effective in this case. Further qual-ity research is required to generalize the findings from this case study and apply it to the general population.
Keywords: Arthroscopy, hip OA, hip pain, pain relief, post-op
IntroductionThe management of the ‘young hip pain’ patient has seen many advances over the last 15 years, with better access to the specialism for the general population as well as advances in surgical techniques providing excellent outcomes, particularly with labral pathology (Stalzer et al. 2006). This is bolstered by good quality evidence supporting the intervention in the sporting field to maintain performance and assist in speedy return to play (RTP) that is then maintained up to 5 years post- surgery (Perets et al. 2018; Menge et al. 2017). While a reported 87% of athletes will RTP after surgery there can be complications, the presence of widespread osteoarthritis (OA) within the joint at the time of surgery being well documented (Casartelli et al. 2015a).
Hip arthroscopy is a procedure of choice where damage has been caused to the articular structures secondary to physiological changes apparent around the joint and, more importantly,
where this causes symptoms, as it shown that these physiological changes can be present in non- symptomatic patients (Abellan et al. 2011). These changes may be due to cam morphol-ogy, pincer morphology or instability, but are only considered part of the syndrome of femoro acetabular impingement (FAI) if a triad of factors exist as described in the Warwick agreement of FAI (Griffin et al. 2016). These include impingement symptoms (e.g. pain, loss of movement), clinical signs (on assessment) and diagnostic imaging to view morphology. Surgery can then be considered as an optional management strategy as well as conservative and physiotherapy- led rehabilitation.
Once surgery has taken place, effective post- operative care is vital to ensure opti-mal outcomes (Casartelli et al. 2015b) and will involve physiotherapy to guide a staged, goal- orientated process like that proposed by Bizzini et al. (2007). Initial stages are heavily influenced by the type of surgery completed in the arthroscopy. For example, where labral repair has occurred a patient may be partial weight- bearing for 4–6 weeks and will have limi-tations on their ability to actively and passively mobilize the operated joint. This is decided by

Acupuncture for pain relief in a patient following hip arthroscopic surgery
© 2018 Acupuncture Association of Chartered Physiotherapists88
the individual surgeon involved based on best practice models they have created with their team, in lieu of evidence- based practice, that is generally based around theory of biomechani-cal models (Grzybowski et al. 2015). This phase is described by Casartelli et al. (2015b) as the protective and early ambulation phase. Progress through this stage and onto later phases relies upon achieving goals (strength, neuromuscular control, range of movement) without the pres-ence of painful symptoms and is supported by numerous other authors (Wahoff & Ryan 2011). Controlling these symptoms is, therefore, of upmost importance to the physiotherapist aim-ing for optimal rehabilitation.
If pain is poorly controlled throughout rehabilitation it can delay the progress through the goal- orientated programme by reducing the ability to train the relevant muscle groups and mobilize the joint within patient comfort and allowing adequate tissue healing. Patients with FAI consistently display a weakness in all muscle groups around the hip and different activation patterns, particularly in the hip flexors (Casartelli et al. 2011), and again pain is considered a major factor in this inhibition. Kierkegaard et al. (2017) go a step further and report patients often describing a feeling of an inability to contract the muscle as well as the non- affected side, suggesting a central protective neural inhibition over just reduced cross- sectional area.
As a result, it is logical to investigate methods for reducing pain in this patient cohort, yet there is no research available looking into specific post- hip arthroscopic pain relief strategies. This author suggests parallels can be made with hip OA research, as FAI and OA are often linked and can present with similar symptoms. One such area of research investigates acupuncture as effective pain relief. Acupuncture has shown increasing use within the sports physiotherapy world with anecdotal evidence of the Western approach being widely discussed within OA- related pain. Kwon et al. (2006) performed a systematic review into the use of acupuncture in peripheral joint OA which included 18 random-ized controlled trials (RCTs) of varying quality. They were able to conclude that acupuncture did have favourable results over sham but only
in knee OA. The papers they reviewed with hip OA showed positive results, but there were too few patient numbers and too few accessible RCTs to provide a definitive answer. Witt et al. (2006) bolstered this opinion but also supported the use of acupuncture in hip OA with a RCT involving over 3500 patients with knee or hip OA. This study lacked blinding and statistical difference in a control group (waiting list con-trol for 3 months) but was able to demonstrate improved outcomes in the population. Haslam (2001) provides a better quality small RCT involving 32 patients. It compared acupuncture using mainly the Gall Bladder (GB) meridian, to advice and exercise for patients who were wait-ing for a hip arthroplasty. Statistically significant improvements in favour of the acupuncture group were found and led to the author advis-ing the use of acupuncture in this patient group.
Case reportThis case report documents the use of acu-puncture in a post- operative hip arthroscopy patient struggling to improve his function after an initial lack of effective physiotherapy.
Patient profile (Table 1) See Table 1 on opposite page.
Pain distribution diagram (Fig. 1)See Fig. 1 on p. 100.
Clinical opinionIneffective management strategies had led to fear avoidance to move a pre- operatively stiff and weak hip, worsening an already chronic pattern of pain. This was a complex picture of an acute- on- chronic scenario with aspects of pain associated to neurological sensitization as well as inflammation. Even though the patient’s surgery was more than 8 weeks prior to our appointment, the patient was still in phase I- II (Grzybowski et al. 2015) and to move forwards, symptoms needed to be addressed. Adequate tissue healing had occurred by this stage so no further restrictions on physiotherapy manage-ment remained.
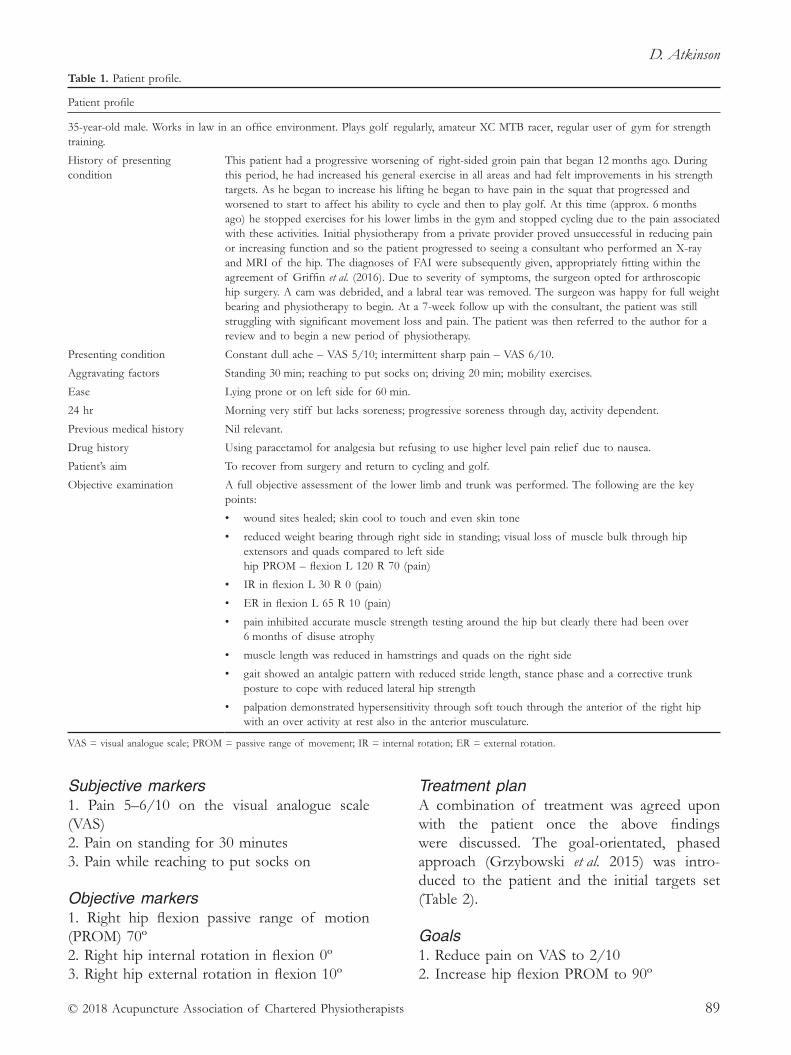
D. Atkinson
© 2018 Acupuncture Association of Chartered Physiotherapists 89
Subjective markers1. Pain 5–6/10 on the visual analogue scale (VAS)2. Pain on standing for 30 minutes3. Pain while reaching to put socks on
Objective markers1. Right hip flexion passive range of motion (PROM) 70º2. Right hip internal rotation in flexion 0º3. Right hip external rotation in flexion 10º
Treatment planA combination of treatment was agreed upon with the patient once the above findings were discussed. The goal- orientated, phased approach (Grzybowski et al. 2015) was intro-duced to the patient and the initial targets set (Table 2).
Goals1. Reduce pain on VAS to 2/102. Increase hip flexion PROM to 90º
Table 1. Patient profile.
Patient profile
35- year- old male. Works in law in an office environment. Plays golf regularly, amateur XC MTB racer, regular user of gym for strength training.
History of presenting condition
This patient had a progressive worsening of right- sided groin pain that began 12 months ago. During this period, he had increased his general exercise in all areas and had felt improvements in his strength targets. As he began to increase his lifting he began to have pain in the squat that progressed and worsened to start to affect his ability to cycle and then to play golf. At this time (approx. 6 months ago) he stopped exercises for his lower limbs in the gym and stopped cycling due to the pain associated with these activities. Initial physiotherapy from a private provider proved unsuccessful in reducing pain or increasing function and so the patient progressed to seeing a consultant who performed an X- ray and MRI of the hip. The diagnoses of FAI were subsequently given, appropriately fitting within the agreement of Griffin et al. (2016). Due to severity of symptoms, the surgeon opted for arthroscopic hip surgery. A cam was debrided, and a labral tear was removed. The surgeon was happy for full weight bearing and physiotherapy to begin. At a 7- week follow up with the consultant, the patient was still struggling with significant movement loss and pain. The patient was then referred to the author for a review and to begin a new period of physiotherapy.
Presenting condition Constant dull ache – VAS 5/10; intermittent sharp pain – VAS 6/10.
Aggravating factors Standing 30 min; reaching to put socks on; driving 20 min; mobility exercises.
Ease Lying prone or on left side for 60 min.
24 hr Morning very stiff but lacks soreness; progressive soreness through day, activity dependent.
Previous medical history Nil relevant.
Drug history Using paracetamol for analgesia but refusing to use higher level pain relief due to nausea.
Patient’s aim To recover from surgery and return to cycling and golf.
Objective examination
A full objective assessment of the lower limb and trunk was performed. The following are the key points:
• wound sites healed; skin cool to touch and even skin tone
• reduced weight bearing through right side in standing; visual loss of muscle bulk through hip extensors and quads compared to left side hip PROM – flexion L 120 R 70 (pain)
• IR in flexion L 30 R 0 (pain)
• ER in flexion L 65 R 10 (pain)
• pain inhibited accurate muscle strength testing around the hip but clearly there had been over 6 months of disuse atrophy
• muscle length was reduced in hamstrings and quads on the right side
• gait showed an antalgic pattern with reduced stride length, stance phase and a corrective trunk posture to cope with reduced lateral hip strength
• palpation demonstrated hypersensitivity through soft touch through the anterior of the right hip with an over activity at rest also in the anterior musculature.
VAS = visual analogue scale; PROM = passive range of movement; IR = internal rotation; ER = external rotation.

Acupuncture for pain relief in a patient following hip arthroscopic surgery
© 2018 Acupuncture Association of Chartered Physiotherapists90
Physiotherapy treatmentIn treating to obtain the initial goals a com-bination of manual therapy and exercise was
performed. Although successful in increasing PROM in the short term the patient would struggle with pain as an after effect. This created a need to view alternative treatment modalities.
Acupuncture The patient’s problem was painful symptoms distributed anteriorly and laterally in the right hip. These symptoms were not new and felt very sim-ilar to the symptoms the patient had pre- surgery. Evidently there were layers of both acute pain (8 weeks post- op) and chronic pain (14 months) and treatment therefore had to be considerate of these elements. The current evidence base for treatment of hip pain includes acupuncture (Haslam 2001; Witt et al. 2006; Kwon et al. 2006) and there is a growing body of evidence to sup-port practitioners in clinical reasoning in the use of Western acupuncture (Bradnam 2007; White et al. 2008a). These papers were used in conjunc-tion with the AACP Foundation Course manual
Figure 1. Pain distribution.
Table 2. Details of treatments.
Treatment number Selected points Needling technique Dose Treatment effect
1 GB 29GB 30GB 31GB 34GB 43ST 44 B/L
40 mm, p, 2–3 cm depth70 mm, p, 3–6 cm depth40 mm, p, 2–3 cm depth25 mm, o, 1–2 cm depth15 mm, p, 0.5 cm depth25 mm, p, 0.5 cm depth
10 min, gentle stimulation Generalized De QiVAS 3/10Hip flex PROM 80º
2 GB 29GB 30GB 31GB 34GB 43ST 44 B/L
40 mm, p, 2–3 cm depth70 mm, p, 3–6 cm depth40 mm, p, 2–3 cm depth25 mm, o, 1–2 cm depth15 mm, p, 0.5 cm depth25 mm, p, 0.5 cm depth
25 min, gentle stimulation Strong De QiVAS 3/10Hip flex PROM 83º
3 GB 29GB 30GB 31GB 34GB 43ST 44 B/LLI 4 B/L
40 mm, p, 2–3 cm depth70 mm, p, 3–6 cm depth40 mm, p, 2–3 cm depth25 mm, o, 1–2 cm depth15 mm, p, 0.5 cm depth25 mm, p, 0.5 cm depth25 mm, p, 1 cm depth
25 min, moderate stimulation Moderate De QiVAS 3/10Hip flex PROM 88º
4
GB 29 GB 30 GB 31 GB 34 GB 43 ST 44 B/L LI 4 B/L BL 26
40 mm, p, 2–3 cm depth 70 mm, p, 3–6 cm depth 40 mm, p, 2–3 cm depth 25 mm, o, 1–2 cm depth 15 mm, p, 0.5 cm depth 25 mm, p, 0.5 cm depth 25 mm, p, 1 cm depth 40 mm, o, 2 cm depth
25 min, moderate stimulation
Moderate De Qi VAS 3/10 Hip flex PROM 92º
GB = Gall Bladder; ST = Stomach; LI = Large Intestine; BL = Bladder; B/L = bilateral; p = perpendicular insertion; o = oblique insertion; PROM = passive range of movement

D. Atkinson
© 2018 Acupuncture Association of Chartered Physiotherapists 91
to guide the acupuncture points used and the appropriate dosage.
Informed consent was gained prior to acu-puncture treatment.
Rationale for point selectionKwon et al. (2006) identified RCTs that used a combination of acupuncture points to treat hip pain, and Haslam (2001) achieved the most positive results and was included in the system-atic review. They used a combination of GB points 29, 30, 34 and 43 along with four Ah Shi points placed in a north, south, east and west formation around the greater trochanter and then finally Large Intestine (LI) 4 and Stomach (ST) 44. The rationale for these points is not well explained other than the comment that the author wanted to choose points that passed over the hip, and that the GB meridian is said to have influence on muscles and tendons. The Ah Shi points were used to affect the muscles that stabilize the hip.
In this case, this author felt that to use the same dose on this patient would have been too high. The layering method described by Bradnam (2007) is consistent in advising care-ful treatment of new patients, and monitoring their response and tolerance to acupuncture. White et al. (2008a) support this and refer to the importance of considering a patient’s personal reactions when deciding upon the appropriate dose. As a result, only six needles were used for a short treatment time and minimal stimulation. They were placed close to the site of pain in the GB meridian to induce local tissue responses, which occur through modulation of the local immune system from neuropeptides released with stimulation of primary afferent nerve end-ings (Lundeberg et al. 1988b, cited in Bradnam 2007). This effect was increased through additional needles along a similar dermatomal pattern to stimulate segmental analgesia within the spinal cord, a process believed to act on the dorsal horn chemically through neural activation from Aδ nerve fibres (White et al. 2008b). Later in treatment, Bladder (BL) 26 was added to directly affect the nerve root at the dermatomal level of hip innervation which would logically also work via the same pathway.
As a De Qi response was achieved, this method proved adequate and allowed the thera-pist to continue with manual treatment modali-ties that created an increase in the patient’s PROM in the hip. De Qi, a sensation felt as result of needle insertion, is often desired anecdotally by therapists and thought of as nec-essary to create the segmental and supraspinal effects of acupuncture.
Notably, the patient’s impression of acu-puncture improved after the first session. This author believes the effect of acupuncture was enhanced via increased patient expectation. He believed it worked, and so it did – a theory sup-ported by Kong et al. (2009).
This patient’s pain was multi- factorial. Elements of acute and chronic pain were evi-dent. In such cases, multiple reasons for the maintenance of pain exist. This creates the need to ensure acupuncture treatment affects these multiple reasons through activation of several mechanisms, dependant on how greatly the central nervous system is sensitized (White et al. 2008a). This was considered in this case by increasing the dose of acupuncture over the four sessions by increasing the number of needles into extrasegmental regions that would also affect the hip region and pain. LI 4 is con-sidered to have strong pain- relieving qualities and was added to support ST 44. Additionally, points used within the hand and foot will create a stronger response thanks to the sensori motor homunculus and dense neural innervation, often activated through the idea of ‘big points’ in Western acupuncture.
As treatment advanced, the patient became more comfortable with acupuncture and an increase in the dosage through manipulation of number of needles, time and stimulation was achieved. This enabled greater use of manual therapy and a better compliance with a home exercise plan. As shown, PROM increased, and pain remained consistently low. Functionally, the patient improved and fewer symptoms were provoked in those provocative positions. Subjective markers all improved, pain on VAS was down to 3/10 and no longer constant, the patient was able to stand for longer periods, and he was finally able to put his socks and shoes

Acupuncture for pain relief in a patient following hip arthroscopic surgery
© 2018 Acupuncture Association of Chartered Physiotherapists92
on. The next phase of treatment involved an increase in strength work and a plan will be put in place to push strength targets and further improve the patient’s long- term picture.
Discussion This case has demonstrated the use of acu-puncture to assist in pain relief during the reha-bilitation of a patient following hip arthroscopy. It enabled the patient to tolerate the necessary physiotherapy to achieve the early phased approach now popularized in this area. This adds to the existing research that acupuncture is helpful in dealing with hip pain. To attribute all pain relief to acupuncture directly would be unscientific: the well- researched effects of appropriate movement, explanation of symp-toms and positive therapist/patient relationship all had a role in these improvements.
Since writing this paper, the author has become aware of a further two studies that are currently looking into what optimal rehabilita-tion should look like after hip arthroscopy. The details of these are not currently available but should shed further light on an under- reviewed area, but as often is the case, the research will be stimulated by appropriate questions being asked by clinicians.
Acupuncture was chosen as the modality for pain relief in this case due to available research supporting its use with hip OA. This case may not have been directly due to OA, but given the patient’s spread of symptoms, parallels were made appropriately. It would not be time- efficient to research all conditions and their treatment, however further research into post- operative Western acupuncture in the reha-bilitation stage would be helpful.
The acupuncture points used were effec-tive and chosen in conjunction with the best available research. Problematically, the research rarely explains why those points were chosen, so best practice models are selected. This cre-ated issues when describing to the patient why distal points were used. While best practice models are helpful, this author feels that all acupuncture research, particularly RCTs, should describe scientifically why points were used. In
this specific case, the best reaction was found when points proximal to pain were used and stimulated. Peripheral points had less effect. Due to this, more needles would be used around the site of pain in future cases, and could mean that with hip arthroscopies, local points are more effective.
Another important question to ask is how it worked. As identified through the work of Adrian White as referenced in this paper, pain science is advancing. To clinically reason how acupuncture is working requires this pain sci-ence to improve further still; testing done on rat populations needs to be advanced to make it adaptable to humans. Disappointingly, again there is very little explanation of the ‘how’ in the RCTs available. Discussion is normally directed at if there was a significant result, rather than how it came about. Future research needs to involve this element in discussion to assist therapists looking to bring the results into practice.
Limitations within this case study are notice-able. The available time to complete this case study was limited to a 4- week period due to work commitments. This undoubtedly will mean that research had to be very specific and did not allow for lateral thinking. It is possible that research exists for other conditions that would answer some of the questions this study has identified but will have been missed.
To summarize, this study presents a patient struggling with pain following ineffective physiotherapy management. Acupuncture was found to be an effective tool in managing pain which allowed physiotherapy to continue and increased its effectiveness.
referencesAbellan J., Esparza F., Blanco A., et al. (2011) Radiological
evidence of femoroacetabular impingement in asymp-tomatic athletes. British Journal of Sports Medicine 45 (4), 310–384.
Bizzini M., Notzli H. & Maffiuletti N. (2007) Femoroacetabular impingement in professional ice hockey players: a case series of 5 athletes after open surgical decompression of the hip. American Journal of Sports Medicine 35 (11), 1955–1959.
Bradnam L. (2007) A proposed clinical reasoning model for Western acupuncture. Journal of the Acupuncture
D. Atkinson
© 2018 Acupuncture Association of Chartered Physiotherapists 93
Association of Chartered Physiotherapists Spring 2007, 21–30.
Casartelli N. C., Maffiuletti N. A., Item- Glatthorn J. F. et al. (2011) Hip muscle weakness in patients with sympto-matic femoroacetabular impingement. Osteoarthritis and Cartilage 19 (7), 816–821.
Casartelli N. C., Leunig M., Maffiuletti N. A. & Bizzini M. (2015a) Return to sport after hip surgery for femoro-acetabular impingement: a systematic review. British Journal of Sports Medicine 49 (12), 819–824.
Casartelli N. C., Bizzini, M., Maffiuletti, N. A., et al. (2015b) Rehabilitation and return to sport after bilat-eral open surgery for femoroacetabular impingement in a professional ice hockey player: a case report. Physical Therapy in Sport 16 (2), 193–201.
Griffin D. R., Dickenson E. J., O’Donnell J., et al. (2016) The Warwick Agreement on femoroacetabular impinge-ment syndrome (FAI syndrome): an international consensus statement. British Journal of Sports Medicine 50 (19), 1169–1176.
Grzybowski J. S., Malloy P., Stegemann C., et al. (2015) Rehabilitation following hip arthroscopy – a systematic review. Frontiers in Surgery 2 (21).
Haslam R. (2001) A comparison of acupuncture with advice and exercises on the symptomatic treatment of osteoarthritis of the hip – a randomised controlled trial. Acupuncture in Medicine 19 (1), 19–26.
Kierkegarrd S., Mechlenburg I., Lund B., et al. (2017) Impaired hip muscle strength in patients with femoro-acetabular impingement syndrome. Journal of Science and Medicine in Sport 20 (12), 1062–1067.
Kong J., Kaptchuk T. J., Polich G., et al. (2009) An fMRI study on the interaction and dissociation between expectation of pain relief and acupuncture treatment. NeuroImage 47 (3), 1066–1076.
Kwon Y. D., Pittler M. H. & Ernst E. (2006) Acupuncture for peripheral joint osteoarthritis: a systematic review and meta- analysis. Rheumatology 45 (11), 1331–1337.
Menge T., Bhatia S., McNamara S., et al. (2017) Femoroacetabular impingement in professional football players, return to play and predictors of career length after hip arthroscopy. American Journal of Sports Medicine 45 (8), 1740–1744.
Perets I., Craig M. J., Mu B. H., et al. (2018) Midterm out-comes and return to sports among athletes undergoing hip arthroscopy. American Journal of Sports Medicine 46 (7), 1661–1667.
Stalzer S., Wahoff M. & Scalan M. (2006) Rehabilitation following hip arthroscopy. Clinics in Sports Medicine 25 (2), 337–357.
Wahoff M. & Ryan M. (2011) Rehabilitation after hip femoroacetabular impingement arthroscopy. Clinics in Sports Medicine 30 (2), 463–482.
White A., Cummings M., Barlas P., et al. (2008a) Defining an adequate dose of acupuncture using a neurophysio-logical approach – a narrative review of the literature. Acupuncture in Medicine 26 (2), 111–120.
White A., Cummings M. & Filshie J. (2008b) An Introduction to Western Medical Acupuncture. Churchill Livingstone/Elsevier, Edinburgh.
Witt C. M., Jena S., Brinkhaus B., et al. (2006) Acupuncture in patients with osteoarthritis of the knee or hip: a randomized, controlled trial with an additional non-randomized arm. Arthritis and Rheumatism 54 (11), 3485–3493.
Daniel Atkinson is a physiotherapist working with a sporting population within the English Institute of Sport and through physiokinetic at the University of Birmingham. He graduated with 1st class honours from Keele University in 2008 and has spent 10 years work-ing across elite sport and with the general population.


© 2018 Acupuncture Association of Chartered Physiotherapists 95
Correspondence: Suzanne Cronin, South Tees Foundation Trust, The James Cook University Hospital, Marton Road, Middlesbrough TS4 3BW, UK (email: suzannec [email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 95–103
CASE rEPOrTS
Acupuncture for the treatment of whiplash associated disorder
S. CroninSouth Tees Foundation Trust, The James Cook University Hospital, Middlesbrough, UK
AbstractThe objective of this case report is to discuss the acupuncture treatment of a 37- year- old female suffering from a case of whiplash associated disorder. The rationale for using acupuncture alongside other physiotherapy modalities is discussed with regard to recent evidence and guidelines. Acupuncture was chosen to alleviate pain and facilitate the use of other physiotherapy techniques to improve movement and function. Outcome measures implemented included the visual analogue scale for pain, the Oxford scale, neck disability index (NDI) and range of movement. The client completed six sessions of acupuncture on a weekly basis in a private physiotherapy setting. The client’s reported pain score fell from 7/10 to 0/10 from first to final assessment. There was also an improvement in the NDI score from 8/50 to 2/50. A proposed reasoning for this marked reduction in pain is discussed. Verbal and written informed consent was obtained from the client.
Keywords: acupuncture, physiotherapy, whiplash associated pain.
IntroductionWhiplash associated disorder (WAD) is a debili-tating condition that accounted for approxi-mately 300,000 insurance claims in 2003 (Burton 2003 in Mercer et al. 2007), a figure which has no doubt risen since 2003.
WAD results in soft tissues and/or bony injury following a rapid acceleration- deceleration movement of the head and neck and can affect other areas of the spine (Moore et al. 2005). WAD can be complicated and worsened by psy-chosocial factors. Chronic WAD is associated with the pain lasting more than six months, with research indicating around 14–42% of patients go on to develop chronic pain (Barnsley 1994) (Table 1).
Although acupuncture is commonly used in physiotherapy, there is limited strong evi-dence on the most effective physiotherapy management of WAD, with guidelines advising self- management strategies and highlighting any psychosocial factors (Verhagan et al. 2007; Williamson et al. 2009; NICE 2015a). In a systematic review conducted by Verhagen et al. (2007), the researchers concluded the current evidence does not provide support for the most effective treatment for WAD, suggesting active treatments are ‘probably’ more beneficial than a more ‘passive’ approach.
The Chartered Society of Physiotherapists (CSP) has developed guidelines which advise that patients suffering from a WAD should be provided with education on posture, use of heat and exercises to activate the deep neck flexor and improve range of motion (Moore et al. 2005). The guidelines report there is weak evidence for the use of acupuncture to treat this condition

Acupuncture for the treatment of whiplash associated disorder
© 2018 Acupuncture Association of Chartered Physiotherapists96
and therefore cannot support or refute its use. Additionally, researchers White and Ernst (1999) in an earlier review found no evidence for acu-puncture in the treatment of neck pain.
The NICE guidelines for the management of WAD conclude there is weak evidence for the long- term effectiveness of physiotherapy such as exercise and mobilization (NICE 2015a). They are not confident physiotherapy would benefit patients with WAD; however, this is in direct contradiction to the guidelines by the same organization which suggest acupuncture having a short- term benefit for sub- acute and chronic neck pain as detailed in the NICE guidelines for non- specific neck pain (NICE 2015b).
There is growing support of the use of acu-puncture for reducing neck pain (He et al. 2004; White et al. 2004; Vas et al. 2006; Willich et al. 2006; Witt et al. 2006; Fu et al. 2009; Trinh et al. 2009). It is proposed that acupuncture activates the body’s own pain- relieving responses locally, segmentally and by having a central effect on the nervous system (White et al. 2008).
It has been suggested that acupuncture can modulate inflammatory conditions through an inflammatory effect (White et al. 2008). Acupuncture has been shown to induce a phenotypic switch of muscle macrophages; this causes a reduction in pre- inflammatory cells and an increase in anti- inflammatory cells thus facilitating a healing response (da Silva et al. 2015). By treating with acupuncture, it is then hypothesized that promoting an inflammatory cascade will induce a healing response and improve the client’s rehabilitation. Omoigui
(2007) reports: “The origin of all pain is the inflam-mation and the inflammatory response”. In chronic conditions such as chronic whiplash, inflam-matory mediators such as bradykinin can add to the sensitization of tissues; this will lead to a smaller stimulus triggering a pain response (Chopade & Mulla 2010). It is important we as therapists recognize the importance of choosing the most effective treatments for WAD at the earliest stage possible to prevent the condition becoming chronic.
The evidence for the pain- relieving effect of acupuncture on these systems will be regarded in the rationale for the acupuncture selection later in this paper. The acupuncture treatment is justified in this case in order to attempt to alleviate pain and maximise potential for the client’s rehabilitation.
Description of the caseThe client was assessed in a private physiother-apy practice following authorization from the insurance company for six sessions of physio-therapy (Table 2). The client had not received any previous treatment for her neck pain. As all symptoms appeared consistent with whiplash associated injury (Ferrari et al. 2005), a diagnosis of QUEBEC grading 2b whiplash associated injury – ‘neck pain with point tenderness and reduced range of motion’ – was made (Hartling et al. 2001).
Acupuncture was discussed with the cli-ent and chosen to treat the client’s pain and facilitate other physiotherapy modalities. No
Table 1. Definition and grading of whiplash- associated disorder (WAD)
A definition and grading of WAD has been provided in guidelines by the Quebec Task Force:
‘Whiplash is an acceleration- deceleration mechanism of energy transfer to the neck. It may result from a rear- end or side- impact motor vehicle collision but can also occur during driving or other mishaps. The impact may result in bony or soft tissue injuries (whiplash injury) which in turn may lead to a variety of clinical manifestations called whiplash associated disorders.’ (Spitzer 1995)
0–No complaint about the neck and no physical sign(s)
1–Neck complaint of pain and no physical sign(s)
2a–Neck complaint and musculoskeletal sign(s). Normal range of motion (ROM)
2b–Neck complaint and musculoskeletal sign(s). Abnormal range of motion (ROM)
2–Neck complaint and neurological sign(s)
3–Neck complaint and fracture or dislocation
(Hartling et al. 2001)
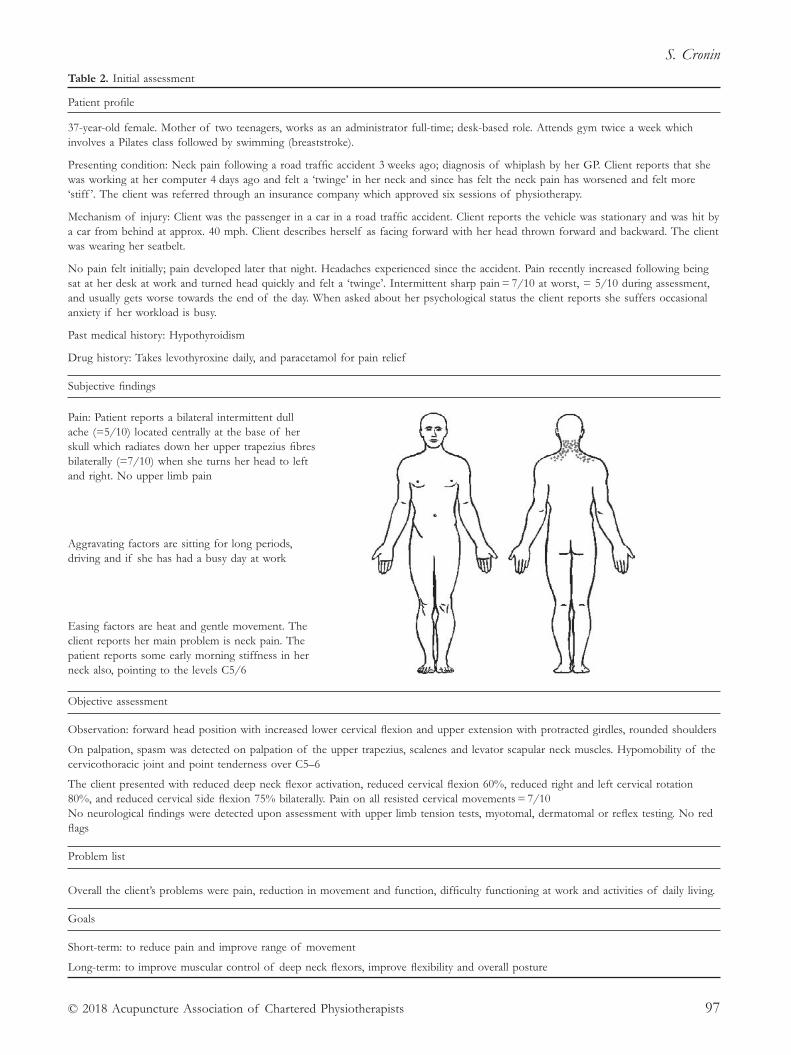
S. Cronin
© 2018 Acupuncture Association of Chartered Physiotherapists 97
Table 2. Initial assessment
Patient profile
37- year- old female. Mother of two teenagers, works as an administrator full- time; desk- based role. Attends gym twice a week which involves a Pilates class followed by swimming (breaststroke).
Presenting condition: Neck pain following a road traffic accident 3 weeks ago; diagnosis of whiplash by her GP. Client reports that she was working at her computer 4 days ago and felt a ‘twinge’ in her neck and since has felt the neck pain has worsened and felt more ‘stiff ’. The client was referred through an insurance company which approved six sessions of physiotherapy.
Mechanism of injury: Client was the passenger in a car in a road traffic accident. Client reports the vehicle was stationary and was hit by a car from behind at approx. 40 mph. Client describes herself as facing forward with her head thrown forward and backward. The client was wearing her seatbelt.
No pain felt initially; pain developed later that night. Headaches experienced since the accident. Pain recently increased following being sat at her desk at work and turned head quickly and felt a ‘twinge’. Intermittent sharp pain = 7/10 at worst, = 5/10 during assessment, and usually gets worse towards the end of the day. When asked about her psychological status the client reports she suffers occasional anxiety if her workload is busy.
Past medical history: Hypothyroidism
Drug history: Takes levothyroxine daily, and paracetamol for pain relief
Subjective findings
Pain: Patient reports a bilateral intermittent dull ache (=5/10) located centrally at the base of her skull which radiates down her upper trapezius fibres bilaterally (=7/10) when she turns her head to left and right. No upper limb pain
Aggravating factors are sitting for long periods, driving and if she has had a busy day at work
Easing factors are heat and gentle movement. The client reports her main problem is neck pain. The patient reports some early morning stiffness in her neck also, pointing to the levels C5/6
Objective assessment
Observation: forward head position with increased lower cervical flexion and upper extension with protracted girdles, rounded shoulders
On palpation, spasm was detected on palpation of the upper trapezius, scalenes and levator scapular neck muscles. Hypomobility of the cervicothoracic joint and point tenderness over C5–6
The client presented with reduced deep neck flexor activation, reduced cervical flexion 60%, reduced right and left cervical rotation 80%, and reduced cervical side flexion 75% bilaterally. Pain on all resisted cervical movements = 7/10No neurological findings were detected upon assessment with upper limb tension tests, myotomal, dermatomal or reflex testing. No red flags
Problem list
Overall the client’s problems were pain, reduction in movement and function, difficulty functioning at work and activities of daily living.
Goals
Short- term: to reduce pain and improve range of movement
Long- term: to improve muscular control of deep neck flexors, improve flexibility and overall posture
Acupuncture for the treatment of whiplash associated disorder
© 2018 Acupuncture Association of Chartered Physiotherapists98
contraindications were noted. Following advice on possible adverse effects, the client agreed, read the patient information leaflet and signed an informed consent form.
Treatment planInformed consent was obtained prior to each treatment.
• Acupuncture for pain management
• Education – posture, anatomy, pain, pac-ing, diagnosis. This included advice on posture throughout the day and while sat at her desk – a work station assessment was discussed.
• Exercises – given to improve range of motion, stability and control.
• Manual techniques and massage.
rationale for point selectionThree points were chosen during the first session as the client had not had acupuncture before, and the points were increased to seven during the second session. White et al. (2008) recommends using six points bilaterally to achieve the observed response.
It is proposed that acupuncture activates the body’s own pain- relieving responses. The inser-tion of these needles leads to local effects in the skin, segmental effects and extrasegmental effects in the body. It is due to these effects that acupuncture is used to treat pain in the short- and longer- term (Carlsson 2002).
Small Intestine (SI), Bladder meridian (BL) and Gall Bladder (GB) points were selected to allow for a segmental and local approach to the client’s pain (White et al. 2008). Additionally, Governor Vessel (GV) 14 was added during the second session as this point can help ease postural neck pain (White et al. 2004) (Table 3).
GB 20 was used bilaterally as it is deemed to ease occipital headache and relieve pain and stiffness in the neck (White et al. 2008). White et al. (2004) state GB 20 and GB 21 should be considered in a clinical setting for the treatment of neck pain.
The local effects of acupuncture lead to a release of a vasodilator calcitonin gene- related peptide (CGRP) which leads to the release of
inflammatory mediators which can promote healing and local pain relief (White et al. 2008).
For example, acupuncture needling activates the body’s Aδ and C fibres in skin and muscles, causing sensations described as “heaviness, tin-gling and soreness,” contributing to the sensa-tion of De Qi (White et al. 2008).
Supporting evidenceSystematic reviews have concluded the evidence for acupuncture and WAD is limited and fur-ther research is required (Moon et al. 2014). In a study of 80 participants with chronic WAD, Stirling et al. (2015) found some effectiveness of dry needling and exercise in a randomized controlled single blind placebo- controlled trial, but reported the results were not “clinically worthwhile”.
Acupuncture may result in pain relief and increased range of movement (Witt et al. 2006), and may be cost- effective in the management of chronic neck pain (Willich 2006). Furthermore, Ross et al. (1999) found in a large long- term study that patients in primary care respond well to acupuncture.
In a study by He et al. (2006), 24 participants with muscular neck pain were randomized into acupuncture and sham control groups. The acupuncture group received electroacupuncture over 16 body points, however participants self- administered auricular acupuncture over six points leading to clear flaws in the study’s statistical power. The control group had elec-troacupuncture applied with no power turned on. The intensity and frequency of pain was significantly lower in the acupuncture group, and these improvements were retained in this group for the following three years compared to the control group.
In a randomized controlled trial by Vas et al. (2006), the following points were used and standardized: GB 20/21, Liver (LR) 3, Large Intestine (LI) 4, GB 34, BL 10, GV 14, SI 3, BL 62 and GB 39. As in the study by White et al. (2004), the sham transcutaneous electrical nerve stimulation (TENS) was not turned on; and statistically significant improvements in
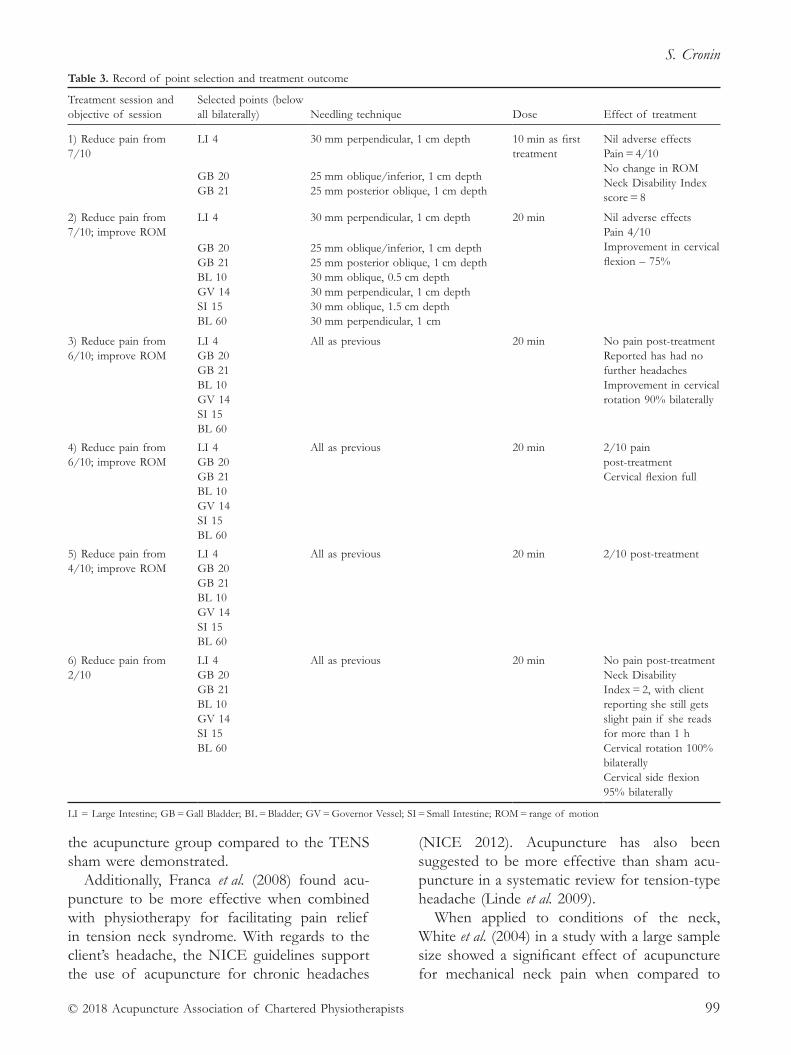
S. Cronin
© 2018 Acupuncture Association of Chartered Physiotherapists 99
the acupuncture group compared to the TENS sham were demonstrated.
Additionally, Franca et al. (2008) found acu-puncture to be more effective when combined with physiotherapy for facilitating pain relief in tension neck syndrome. With regards to the client’s headache, the NICE guidelines support the use of acupuncture for chronic headaches
(NICE 2012). Acupuncture has also been suggested to be more effective than sham acu-puncture in a systematic review for tension- type headache (Linde et al. 2009).
When applied to conditions of the neck, White et al. (2004) in a study with a large sample size showed a significant effect of acupuncture for mechanical neck pain when compared to
Table 3. Record of point selection and treatment outcome
Treatment session and objective of session
Selected points (below all bilaterally) Needling technique Dose Effect of treatment
1) Reduce pain from 7/10
LI 4 30 mm perpendicular, 1 cm depth 10 min as first treatment
Nil adverse effectsPain = 4/10No change in ROMNeck Disability Index score = 8
GB 20 25 mm oblique/inferior, 1 cm depthGB 21 25 mm posterior oblique, 1 cm depth
2) Reduce pain from 7/10; improve ROM
LI 4 30 mm perpendicular, 1 cm depth 20 min Nil adverse effects Pain 4/10Improvement in cervical flexion – 75%
GB 20 25 mm oblique/inferior, 1 cm depthGB 21 25 mm posterior oblique, 1 cm depthBL 10 30 mm oblique, 0.5 cm depthGV 14 30 mm perpendicular, 1 cm depthSI 15 30 mm oblique, 1.5 cm depthBL 60 30 mm perpendicular, 1 cm
3) Reduce pain from 6/10; improve ROM
LI 4GB 20GB 21BL 10GV 14SI 15BL 60
All as previous 20 min No pain post- treatmentReported has had no further headachesImprovement in cervical rotation 90% bilaterally
4) Reduce pain from 6/10; improve ROM
LI 4GB 20GB 21BL 10GV 14SI 15BL 60
All as previous 20 min 2/10 pain post- treatment Cervical flexion full
5) Reduce pain from 4/10; improve ROM
LI 4GB 20GB 21BL 10GV 14SI 15BL 60
All as previous 20 min 2/10 post- treatment
6) Reduce pain from 2/10
LI 4 GB 20 GB 21 BL 10 GV 14 SI 15 BL 60
All as previous
20 min
No pain post- treatment Neck Disability Index = 2, with client reporting she still gets slight pain if she reads for more than 1 h Cervical rotation 100% bilaterally Cervical side flexion 95% bilaterally
LI = Large Intestine; GB = Gall Bladder; BL = Bladder; GV = Governor Vessel; SI = Small Intestine; ROM = range of motion

Acupuncture for the treatment of whiplash associated disorder
© 2018 Acupuncture Association of Chartered Physiotherapists100
sham TENS which was not turned on over the same acupoints.
A large- scale German study (N = 3766) per-formed by Witt et al. (2006) found the use of acupuncture was associated with improvements in neck pain and disability when compared to routine care alone. In a Cochrane Review with a smaller number of participants (N = 661), Trinh et al. (2006) found moderate evidence that acu-puncture relieves pain better than some sham treatments in patients with neck pain.
With regards to WAD, the CSP guidelines conclude there is not enough clinical evidence to support or refute the use of acupuncture (Moore et al. 2005). However, it is still widely used in conjunction with other physiotherapy modalities. Researchers Fu et al. (2009) in a systematic review of 14 studies into the effec-tiveness of acupuncture for neck pain agreed that more long- term follow up in this area was required but reported a short- term benefit of acupuncture for neck pain.
Following a review of the literature, acupunc-ture seems to have a place in the treatment of pain conditions.
The evidence for the effectiveness of acu-puncture within physiotherapy is uncertain, with researchers reporting low quality evidence produced and using low sample sizes. The big-gest problem with the studies is that the place-bos used, i.e., the sham technique, provide no
real placebo, as the sham will have a treatment effect of its own and it has been demonstrated that the blunt needle can have profound effects on the limbic system (Pariente et al. 2005). Sham acupuncture involves needling non- acupuncture points or using a device whereby the guide tube is pressed against the skin but the needle either penetrates very slightly (superficial tissue) below the skin or not at all (Lund et al. 2009).
After reviewing the literature, the evidence suggests the effectiveness of acupuncture in the treatment of neck pain as part of a physiother-apy treatment plan
DiscussionThe client reported no pain following the sixth treatment session. The NDI score (Appendix 1) was 8 at initial assessment and reduced to 2 by the final session. The NDI is an outcome measure which is considered a valid and reliable tool for measuring neck pain (Vernon & Mior 1991; Stratford et al. 1999).
Improvements in range of motion were observed following the third session, and full rotation was achieved by the final session, but the client had some muscular tightness in side flexion and was advised to continue with the stretching exercises. Education on posture, use of heat, manual techniques and exercises to improve muscular control and improve range
Table 4. Clinical reasoning for points selected
Points selected Justification for points selected and supporting evidence
LI 4 bilaterally LI 4 covers dermatomes C6/C7 and is a “master point for pain.” It creates a calming response and was chosen also to create an extra segmental response (White et al. 2008).
Distal points LI 4 were used bilaterally to induce a strong supraspinal pain descending inhibitory effect (White et al. 2008). Additionally, Wu et al. (1999) found the acupoint LI 4 led to activity in the limbic area related to pain response and detected in the descending anti- nociceptive pathways.
Haker et al. (2000) found acupuncture to the LI 4 points and an ear point led to a sympathetic response in the related segment and resulted in pain relief.
GB 20 bilaterally “Master point” for pain and activating the sympathetic nervous system (Hecker et al. 2007)
GB 21 bilaterally GB 21 was chosen bilaterally to achieve a local, segmental and extra segmental effects and subsequently to target the client’s head and neck pain and stiffness (He et al. 2004; White et al. 2008).
BL 10 bilaterally Vas et al. (2006). Indicated for cervical pain (Hecker et al. 2007)
BL 60 bilaterally Distal point to facilitate the strength of the bladder meridian (White et al. 2004)
GV 14 bilaterally GV 14 during the second session as this point can help with postural neck pain (White et al. 2004)
SI 15 bilaterally (He et al. 2004)
LI = Large Intestine; GB = Gall Bladder; BL = Bladder; GV = Governor Vessel; SI = Small Intestine

S. Cronin
© 2018 Acupuncture Association of Chartered Physiotherapists 101
of motion were used as advised by Moore et al. (2005). The pain relief may be a result of the pain- relieving mechanisms of the acupuncture treatment in combination with the other physio-therapy modalities used, all of which may have combined to lead to favourable results.
Upon reflection, an alternative treatment would have been to use electroacupuncture for this case. In a randomized, double- blind study, Sator- Katzenschlager et al. (2004) found weekly auricular electroacupuncture reduced pain and therefore proved more effective than manual acupuncture in the treatment of chronic low back pain.
Another alternative treatment which could have been adopted was dry- needling trigger point acupuncture. Trigger point acupuncture over SI 15 may be used to manage myofascial trigger points common in the area and ease muscle spasm in upper trapezius (White et al. 2008). This is supported by Itoh et al. (2007) who found trigger point acupuncture treatment was more effective than manual acupuncture, resulting in lower intensity neck pain.
It has been proposed that mechanical dis-ruption of connective tissues in the body can have an effect on local and global anatomical tissues and lead to disturbances in the electri-cal response of tissues and cellular activity (Langevin & Yandow 2002). In addition to the pain- relieving responses of acupuncture docu-mented, a structural response has been observed following the manipulation of the acupuncture needle. In the subcutaneous tissue of a mouse, a gathering of collagen around the needle and altered fibroblast cellular activity several centi-metres away from the needle was demonstrated by Langevin et al. (2006). This mechanism could perhaps explain and have contributed to the improvement in the client’s range of motion.
The reduction in pain may have been caused by the segmental effects of acupuncture which stimulate Aδ and C fibres in skin and type 11 and type 111 fibres in muscles, activating the release of encephalin (White et al. 2008). Clement- Jones et al. (1980) showed that follow-ing acupuncture there was an increased level of B- endorphin detected in patients who received
acupuncture compared to those in the control. The segmental activation leads to a segmental analgesia which can last the duration of the session and days succeeding the initial treatment (White et al. 2008). This can explain how acu-puncture can have a cumulative effect on pain for the client.
Individuals with WAD have been shown to be hypersensitive to mechanical pressure which can lead to changes in the central processing of pain (Scott et al. 2005). In the brain, the cer-ebral cortex detects this sensation of needling and activates an area called the periaqueductal gray or ‘PAG’ which is the primary control centre for descending pain. The PAG has a high concentration of the cells which produce encephalin (White et al. 2008) and activation via the mechanism of acupuncture can lead to the release of noradrenaline and serotonin, leading to pain relief due to activation of descending pain inhibition (White et al. 2008). Furthermore, functional MRI (fMRI) have demonstrated the effect of acupuncture on the pain pathways of the brain (Napadow et al. 2009).
A pro- inflammatory effect of acupuncture may also be responsible for the reduction in the client’s pain. Wang et al. (2014) when treating rats with acupoint GB 30 showed that acupunc-ture regulates opioid- containing macrophages and anti- nociceptive mediators in inflammatory pain. These studies using animal models have limitations when generalizing the results to humans.
The client had not had acupuncture before. Additionally to the effect on pain, acupuncture has an effect on psychological aspects of pain and some researchers suggest that positive expectation of pain relief may amplify the effect of the treatment (Shi et al. 2012; Kong et al. 2009).
Additionally, the headache the client had experienced following the injury seemed to have benefited from treatment, however this may have been a result of an improvement in range of movement and function following the other physiotherapy modalities. Other researchers do however advocate acupuncture for tension headaches (Linde et al. 2009) and neurovascular headache (Zhao et al. 2011).
Acupuncture for the treatment of whiplash associated disorder
© 2018 Acupuncture Association of Chartered Physiotherapists102
Another problem with the studies is the small samples used, which leads to the risk of a type two error being made. Furthermore, a limitation of many of the studies included is that they do not investigate acute or sub- acute neck pain, which is commonly what a patient will present to physiotherapy with.
ConclusionIt appears that the segmental, extrasegmental and central effects proposed with acupuncture treatment had a good pain- relieving effect on the client in this case study. Due to its subjective nature, pain is difficult to study. It seems there is limited strong evidence for the effectiveness of acupuncture for the treatment of WAD, leading to contraindications in the guidelines and frustrations for acupuncturists who see on a daily basis the benefit this modality can have on the individual.
referencesBarnsley L., Lord S. & Bogduk N. (1994) Whiplash injury:
clinical review. Pain 58 (3), 283–307.Burton K. (2003). Treatment guidelines: Is there a
need? In: Proceedings of Whiplash Conference 2003, Bath, England, 6–8 May. Lyons Davidson Solicitors, Bristol, as cited in Mercer C., Jackson A. & Moore A. (2007) Developing clinical guidelines for the physiotherapy management of whiplash associated disorder (WAD). International Journal of Osteopathic Medicine 10, 50–54.
Carlsson C. (2002) Acupuncture mechanisms for clini-cally relevant long- term effects: reconsideration and a hypothesis. Acupuncture in Medicine 20 (2–3), 82–99.
Chopade A. R. & Mulla W. A. (2010) Novel strategies for the treatment of inflammatory hyperalgesia. European Journal of Clinical Pharmacology 66 (5), 429–444.
Clement- Jones V., Tomlin S., Rees L. H., et al. (1980) Increased ß- endorphin but not met- enkephalin levels in human cerebrospinal fluid after acupuncture for recurrent pain. Lancet 316 (8201), 946–949.
da Silva M. D., Bobinski F., Sato K. L., et al. (2015) IL- 10 cytokine released from M2 macrophages is crucial for analgesic and anti- inflammatory effects of acupuncture in a model of inflammatory muscle pain. Molecular Neurobiology 51 (1), 19–31.
Ferrari R., Russell A. S., Carroll L. J. & Cassidy J. D. (2005) A re- examination of the whiplash associated disorders (WAD) as a systemic illness. Annals of the Rheumatic Diseases 64 (9), 1337–1342.
Franca D. L., Senna- Fernandes V., Cortez C. M., et al. (2008) Tension neck syndrome treated by acupuncture combined with physiotherapy: a comparative clinical
trial (pilot study). Complementary Therapies in Medicine 16 (5), 268–277.
Fu L. M., Li J. T. & Wu W. S. (2009) Randomized con-trolled trials of acupuncture for neck pain: systematic review and meta- analysis. Journal of Alternative and Complementary Medicine 15 (2), 133–45.
Haker E., Egekvist H. & Bjerring P. (2000) Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. Journal of the Autonomic Nervous System 79 (1), 52–59.
Hartling L., Brison, R. J., Ardem C. & Pickett W. (2001) Prognostic value of the Quebec classification of whiplash- associated disorders. Spine 26 (1), 36–41.
He D., Veiersted K. B., Høstmark A. T. & Medbø J. I. (2004) Effect of acupuncture treatment on chronic neck and shoulder pain in sedentary female workers: a 6- month and 3- year follow- up study. Pain 109 (3), 299–307.
Hecker H.- U., Steveling A., Peuker E., et al. (2007) Colour Atlas of Acupuncture, 2nd edn. Thieme Publishing Group, Stuttgart.
Itoh K., Katsumi Y., Hirota S. & Kitakoji H. (2007) Randomized trial of trigger point acupuncture com-pared with other acupuncture for treatment of chronic neck pain. Complementary Therapies in Medicine 15 (3), 172–179.
Kong J., Kaptchuk T. J., Polich G., et al. (2009) An fMRI study on the interaction and dissociation between expectation of pain relief and acupuncture treatment. NeuroImage 47 (3), 1066–1076.
Langevin H. M. & Yandow J. A. (2002) Relationship of acupuncture points and meridians to connective tissue planes. Anatomical Record 269 (6), 257–265.
Langevin H. M., Bouffard N. A., Badger G. J., et al. (2006) Subcutaneous tissue fibroblast cytoskeletal remodeling induced by acupuncture: evidence for a mechanotransduction- based mechanism. Journal of Cellular Physiology 207 (3), 767–774.
Linde K., Allais G., Brinkhaus B., et al. (2009) Acupuncture for tension- type headache. Cochrane Database of Systematic Reviews 1: CD007587.
Lund I., Naslund J. & Lundeberg T. (2009) Minimal acupuncture is not a valid placebo control in random-ized controlled trials of acupuncture: a physiologist’s perspective. Chinese Medicine 4 (1).
Mercer C., Jackson A. & Moore A. (2007) Developing clinical guidelines for the physiotherapy management of whiplash associated disorders. International Journal of Osteopathic Medicine 10, 50–54.
Moon T.- W., Posadzki P., Choi T.- Y., et al. (2014) Acupuncture for treating whiplash associated dis order: a systematic review of randomized clinical trials. Evidence- based Complementary and Alternative Medicine 2014: 870271.
Moore A., Jackson A., Jordan J., et al. (2005) Clinical guide-lines for the physiotherapy management of whiplash- associated disorder. Chartered Society of Physiotherapy, London.
S. Cronin
© 2018 Acupuncture Association of Chartered Physiotherapists 103
Napadow V., Dhond R. P., Kim J., et al. (2009) Brain encoding of acupuncture sensation – coupling on- line rating with fMRI. NeuroImage 47, 1055–1065.
National Institute for Health and Clinical Excellence (NICE) (2012) Clinical guideline CG150. Headaches in over 12s: diagnosis and management. [WWW document.] http://www.nice.org.uk/guidance/cg150
National Institute for Health and Clinical Excellence (NICE) (2015a). Neck pain – whiplash injury. Available from http://cks.nice.org.uk/neck- pain- whiplash- injury (last accessed January 2016)
National Institute for Health and Clinical Excellence (NICE) (2015b) Clinical knowledge summary. Neck pain – non- specific. [WWW document.] http://cks.nice.org.uk/neck- pain- non- specific [Accessed January 2016].
Omoigui S. (2007) The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3 – inflammatory profile of pain syndromes. Medical Hypotheses 69 (6), 1169–1178.
Pariente J., White P., Frackowiak R. S. & Lewith G. (2005) Expectancy and belief modulate the neuronal substrates of pain treated by acupuncture. NeuroImage 25 (4), 1161–1167.
Ross J., White A. & Ernst E. (1999) Western, minimal acupuncture for neck pain: a cohort study. Acupuncture in Medicine 17 (1), 5–8.
Sator- Katzenschlager S. M., Scharbert G., Kozek- Langenecker S. A., et al. (2004) The short- and long- term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupuncture. Anesthesia and Analgesia 98 (5), 1359–1364.
Scott D., Jull G. & Sterling M. (2005) Widespread sensory hypersensitivity is a feature of chronic whiplash- associated disorder but not chronic idiopathic neck pain. Clinical Journal of Pain 21 (2), 175–181.
Shi G. X., Yang X. M., Liu C. Z. & Wang L. P. (2012) Factors contributing to therapeutic effects evaluated in acupuncture clinical trials. Trials 13:42.
Spitzer W. O., Skovron M. L., Salmi L. R., et al. (1995) Monograph of the Quebec Task Force on whiplash- associated disorders: redefining “whiplash” and its management. Spine 20 (8 Suppl), 1S- 73S.
Stirling M., Vicenzino B., Souvlis T. & Connelly L. B. (2015) Dry- needling and exercise for chronic whiplash- associated disorders: a randomized single- blind placebo- controlled trial. Pain 156 (4), 635–643.
Stratford P. W., Riddle D. L., Binkley J. M., et al. (1999) Using the Neck Disability Index to make decisions concerning individual patients. Physiotherapy Canada 51, 107–112, 119.
Trinh K. V., Graham N., Gross A. R., et al. (2006) Acupuncture for neck disorders. Cochrane Database of Systematic Reviews 3: CD004870.
Vas J., Perea- Milla E., Mendez C., et al. (2006) Efficacy and safety of acupuncture for chronic uncomplicated neck pain: a randomized controlled study. Pain 126 (1–3), 245–255.
Verhagen A. P., Scholten- Peeters G. G., van Wijngaarden S., et al. (2007) Conservative treatments for whiplash. Cochrane Database of Systematic Reviews 2: CD003338.
Vernon H. & Mior S. (1991) The Neck Disability Index: a study of reliability and validity. Journal of Manipulative and Physiological Therapeutics 14 (7), 409–415.
Wang Y., Gehringer R., Mousa S. A., et al. (2014). CXCL10 controls inflammatory pain via opioid peptide- containing macrophages in electroacupuncture. PLoS One 9 (4), e94696.
White A. R. & Ernst E. (1999) A systematic review of randomized controlled trials of acupuncture for neck pain. Rheumatology 38 (2), 143–147.
White A., Cummings M. & Filshie J. (2008) An Introduction to Western Medical Acupuncture, 1st edn. Churchill Livingstone/Elsevier, Edinburgh.
White P., Lewith G., Prescott P. & Conway J. (2004) Acupuncture versus placebo for the treatment of chronic mechanical neck pain. Annals of Internal Medicine 141 (12), 911–919.
Williamson E., Williams M., Hansen Z., et al. (2009). Development and delivery of a physiotherapy interven-tion for the early management of whiplash injuries: the Managing Injuries of the Neck Trail (MINT) interven-tion. Physiotherapy 95 (1), 15–23.
Willich S. N., Reinhold T., Selim D., et al. (2006) Cost- effectiveness of acupuncture treatment in patients with chronic neck pain. Pain 125 (1–2), 107–113.
Witt C. M., Jena S., Brinkhaus B., et al. (2006) Acupuncture for patients with chronic neck pain. Pain 125 (1–2), 98–106.
Wu M.- T., Hsieh J.- C., Xiong J., et al. (1999) Central nervous pathway for acupuncture stimulation: localiza-tion of processing with functional MRI imaging of the brain – preliminary experience. Radiology 212 (1), 133–141.
Zhao L., Guo Y., Wang W. & Yan L.- J. (2011) Systematic review on randomized controlled trials of acupuncture for neurovascular headache. Chinese Journal of Integrative Medicine 17 (8), 580–586.
Appendix 1Neck Disability Index https://www.aaos.org/uploadedFiles/NDI.pdfVernon H. (2008) The Neck Disability Index: state- of- the-
art, 1991–2008. Journal of Manipulative and Physiological Therapies 31 (7), 491–502.
Suzanne completed a Sports Therapy BSc in 2009 and then a Physiotherapy BSc in 2012, and currently works as a senior physiotherapist within pulmonary rehabilita-tion within the South Tees Foundation Trust. Having treated various spinal and peripheral conditions whilst working part- time within a private sports physiotherapy clinic, Suzanne felt acupuncture would be a suitable adjunct to complement her physiotherapy practice.

© 2018 Acupuncture Association of Chartered Physiotherapists 105
Correspondence: Lynn Pearce, The Courtyard Centre for Health and Wellbeing, Biggleswade, Bedfordshire SG18 0JA, UK ([email protected]).
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 105–107
OPINION
Electricity and electroacupuncture – a quick overview
l. PearcePrivate Practice, Biggleswade, UK
AbstractElectricity is good for the body. Attaching it to acupuncture needles can accelerate the effects we can have on tissue healing, relaxation of both mind and body through stimulating the release of neurotransmitters, and improving micro- circulation. This article takes a very brief look at some of the key parameters of electroacupuncture and suggests ways in which we can add it to our acupuncture- based toolbox.
Keywords: electroacupuncture, high frequency, low frequency.
IntroductionHistorically, there is an intimate link between electricity and health. Too much of it (like being struck by lightning) – well, that’s not very healthy at all, especially if you don’t survive; not enough of it and our biology cannot function as it should, which can lead to illness.
We live on a huge magnet which throws out electrical fields, we are affected by electricity in the atmosphere, and we are surrounded by and interact with many different wavelengths in the electromagnetic spectrum. Every cell is like a mini- magnet and generator, and there is a constant flux of electric current and physiology trying to keep some sort of homeostasis in our bodies.
Dan Keown’s enlightening book The Spark in the Machine (2014) provides an overview of how current may drive biological function and be linked to embryological development. There is an elegant correlation with the concept of the meridian network in here too – a must read.
Dr Tim Watson reiterates the need for the body to have current with this comment from Electrotherapy: Evidence Based Practice:
“ . . . there is a concept that biological tissues demonstrate electrical characteristics and that this bio- electrical activity is . . . integral to their form and function. It would appear that without this activity, characteristics, behaviour and response to adverse events, the body would not be able to deal with the environment as efficiently as it does.” (Watson 2008).
As physiotherapists, we are used to using elec-trotherapy and may have a vestigial memory of our theory from college as to what works on the tissues, and how. The main aim, with what-ever outside force we are using, is to stimulate physiology into a different state from the one in which we find it.
In terms of tissue healing, we know tissue needs blood flow and chemistry in order to heal. This precipitates a cascade of other events such as tissue laydown and remodelling. If we can stimulate this with our needles, how much more can we achieve with the addition of electro-acupuncture? And what kind of frequencies do

Electricity and electroacupuncture – a quick overview
© 2018 Acupuncture Association of Chartered Physiotherapists106
what kind of job? In short, is it worth adding current to the needle in order to gain a more enhanced effect?
In general terms, electricity applied to the tissues has one of three effects:
• chemical
• physical (or stimulatory)
• thermal.
These can influence the body at different levels:
• cellular
• tissue
• segmental
• systemic.
It is important to remember that two points connected together electrically in the lumbar spine, for example, will not just affect the local area. There will be segmental blocking, as per transcutaneous electrical nerve stimulation (TENS), and a global chemical effect which occurs after the treatment session and can con-tribute to increased endorphin production with an improvement in sleep and/or wellbeing (Han 2004; Lundburg 2005).
Likewise, certain tissues respond to certain fre-quencies and so if we can manipulate the internal environment more effectively by applying these frequencies, which we cannot do with manual acupuncture alone, then perhaps the treatment will be even more effective (Qi 2016) (Table 1).
Taking this as a baseline, we can see that the lower frequencies have greater effect on tissue healing – anything between 2–20 Hz seems to cover most of our patients’ needs!
When we compare the effect that electro-acupuncture has over manual acupuncture, we see we can achieve a lot more with the addition of electroacupuncture (Table 2).
In summary, the application of low frequency (between 2–15 Hz) is more useful in helping chronic pain, having a vascular effect due to an active muscle twitch. It has a longer lasting effect but may take longer to start having that effect. The physiology of endorphin produc-tion starts from 2–4 h post- treatment up to 48 h, with patients often reporting an increasing sense of tiredness and relaxation after this time as opposed to immediately after or during a treatment session (Duan 2016a; Duan 2016b). A 20–30 min stimulation is required.
Applying high frequency (between 80– 120 Hz) is more helpful in affecting acute pain or for more immediate relief, since relief is quicker but does not last as long. High frequen-cies tend to have a predominantly segmental and short- term effect (Mayor 2007). There is an associated release of dynorphin at the spinal cord level. A 10–20 min stimulation should give an anaesthetic effect.
Oschman (2000 p.179) claims that in general, “organisms are poised to respond to minute ‘whispers’ in the electromagnetic environment ”. What is significant about these results is the known relationship of using extremely low frequency (ELF) biomag-netic fields to promote healing. For example, in 1995 Siskin & Walker (Oschman 2000 p.87) noted that an ELF of 2 Hz stimulated nerve regeneration, and that a frequency of 7 Hz can
Table 1. Relationship between the range of ELF and the clini-cal results identified by Siskin & Walker (in Oschman 2000).
2 Hz Nerve regeneration7 Hz Bone regrowth10 Hz Ligament healing15, 20, 72 Hz Decreased skin death, stimulation of capillary
formation and fibroblast proliferation 25 and 50 Hz Enhances nerve growth factor activity
Table 2. Comparing manual acupuncture with electroacupuncture.
Manual acupuncture Electroacupuncture
Needle manipulation is brief and intermittent Only ‘low frequency’ is possible (twirling or lifting- thrusting) Strong manipulation risks tissue damage Mostly central mechanism with De Qi Local effects- trigger points e.g. some local tissue response
Stimulation is continued for the duration of treatment No limitation to frequency of stimulus (frequency- specific and tissue- specific effects can occur) Strength of stimulation only limited by patient tolerance More reaction around needle (2 Hz) – calcitonin gene- related peptide, vaso- intestinal peptide and noradrenaline, greater vasodilation, and increased segmental effects, alteration of sympathetic tone – segmental and visceral organs Best effect re- creates exercise = melatonin production = better sleep
L. Pearce
© 2018 Acupuncture Association of Chartered Physiotherapists 107
be used to stimulate bone growth. A frequency of 10 Hz promotes ligament healing, and 15, 20, and 72 Hz may be used to decrease skin necrosis and stimulate capillary formation (Table 1).
Key factors in getting the optimum dose are time, frequency and intensity (Fig 1). Establishing a correct dose is probably one of the most difficult things to do in acupuncture, as there are so many variables. However, that said, the time needs to be between 20–40 min for a low frequency effect to reach its optimum, and the intensity needs to be such that the patient is in charge of the current and that it is as high as they can stand without it being uncomfortable (Barlas 2006). Strong tapping is the order of the day. High frequency is faster acting, and actually does not need to be as strong – milder levels will bring segmental effects.
Certain conditions seem to respond particu-larly well – osteoarthritic (OA) knees, really tight chronically stiff spinal issues where the tissue is thick and blood flow is compromised, shoulder issues involving tension in the protective muscle splint, and many more. David Mayor’s book Electroacupuncture (2007) is the definitive text but applying the outline above for low and high frequency will give tissue and chemical specific effects that can dramatically speed up treatment for our clients.
So – is it worth applying current to the needles?
Absolutely – yes.
referencesBarlas P., Ting S. L., Chesterton L. S. et al. (2006) Effects
of intensity of electroacupuncture upon experimental pain in healthy human volunteers: a randomized, double- blind, placebo- controlled study. Pain 122 (1–2), 81–89.
Duan D., Tu Y., Yang X. & Liu P. (2016a) Electro-acupuncture restores 5- HT system deficit in chronic mild stress- induced depressed rats. Evidence- Based Complementary and Alternative Medicine 2016:7950635.
Duan D. M., Tu Y., Liu P. & Jiao S. (2016b) Antidepressant effect of electroacupuncture regulates signal targeting in the brain and increases brain- derived neurotrophic factor levels. Neural Regeneration Research 11 (10), 1595–1602.
Han J. S. (2004) Acupuncture and endorphins. Neuroscience Letters 361 (1–3), 258–61.
Keown D. (2014) The Spark in the Machine. Singing Dragon.Lundburg T. (2005) Conference presentation, BMAS
Electroacupuncture Study Day, 30 November 2005.Mayor D. (ed) (2007) Electroacupuncture: A practical manual
and resource. Churchill Livingstone, Edinburgh.Oschman J. L. (2000) Energy Medicine: The Scientific Basis.
Churchill Livingstone, Edinburgh.Qi L., Tang Y., You Y., et al. (2016) Comparing the effec-
tiveness of electroacupuncture with different grades of knee osteoarthritis: a prospective study. Cellular Physiology and Biochemistry 39 (6), 2331–2340.
Watson T. (ed) (2008) Electrotherapy: Evidence Based Practice, 12th edn. Churchill Livingstone, Edinburgh.
Lynn Pearce qualified from Addenbrookes School of Physiotherapy in 1982. She has worked clinically since that time within several fields and is now working in an outpatient private practice setting at the Courtyard Centre for Health and Wellbeing in Biggleswade, Bedfordshire. Her initial acupuncture training in 1989 was followed by a Traditional Chinese Medicine course in 1993 at the British College of Acupuncture, London. She regularly uses electroacupuncture alongside manual therapy and physiotherapy practice. She is also a tutor for the AACP and a qualified Clinical Canine Massage Practitioner and works at DogzAligned for our canine friends (www.dogzaligned.com).
Figure 1. The key components (after Mayor 2007).

© 2018 Acupuncture Association of Chartered Physiotherapists 109
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 109–110
reviews
The handy Cure S device – a brief personal reviewAlthough trained as a purist in ‘traditional’ acu-puncture, I have always had an interest in things electrical, and six years after completing my initial training began to use electroacupuncture in my clinical practice. As a side interest, I took courses in low intensity (low- level) laser therapy (LILT, or LLLT), but was always put off using it in practice by the relatively high price of the equipment. Over the years, however, I dab-bled with low- cost versions, such as Amcor’s Biobeam units from Israel (Mayor 1996) or the intriguing Chinese method of intranasal low- intensity laser therapy (iLILT) (Mayor 2014).
So Gudaro Med- Tech’s full- page colour advert for another such Israeli device, the ‘Handy Cure S,’ manufactured by Medical Quant, slap bang opposite the Editorial in the Spring 2018 edition of Acupuncture in Physiotherapy, caught my atten-tion. The advert was full of alluring references to acute or chronic musculoskeletal conditions that might respond to treatment using the device, with a number of ringing endorsements from practitioners (chiropractor, acupuncturist, massage and sports injury therapists). I was hooked!
The Handy Cure S has been available in Israel since at least 2009 (Friedmann et al. 2009). Although there is of course a voluminous lit-erature on LILT/LLLT and laser acupuncture (over 5,700 studies listed in PubMed currently), and at least one publication on a different device providing combinations of laser and LED light at different wavelengths and frequencies (Leal- Junior et al. 2014), I have not been able to locate other published studies that explicitly used the Handy Cure S. This is particularly surprising, given its low price and ready availability.
The device is comfortable to hold, not too heavy if rested on the area to be treated, and easy to use (additional probes/‘nozzles’ can be attached for acupuncture point and other
applications). Protective eyewear is supplied. Output combines 905 nm (‘Class 1M’) LILT, infrared (875 nm, 30–90 mW), visible red light (635 nm, 2–10 mW) and a static magnetic field (25–45 mT, although stated to be 25–45 MT in the Scientific Evidence printout supplied!). That’s an innovative and clever combination, with claimed synergistic effects (Friedmann et al. 2009) and a supposed penetration depth of up to 8–10 cm. The case studies included in the printout included some for non- musculoskeletal conditions such as thrombophlebitis, shingles and non- healing ulcers.
The user manual emphasizes the synergistic effects of the device on inflammation and tis-sue repair and describes the three programmes that can be used: variable frequency pulsation (1–250 Hz/sec) for initial treatment), 50 Hz (50 Hz/sec) for acute pain, and 5 Hz (5 Hz/sec) for chronic pain. Recommended treatment is for five minutes at each location (timed automatically), once or twice daily, for 21 days, with variable frequency applied during the first week and then either 5 or 50 Hz in subsequent weeks. For acute conditions this is somewhat puzzling, as the appropriate programme would not be used until the second week of treat-ment, when – hopefully – the condition would no longer be so acute. Also puzzling is the suggestion that penetration depth is greater at the lower frequency (i.e. for chronic condi-tions), whereas the textbooks – as well as other promotional material about the Handy Cure S – state that it is dependent on the wavelength of the light applied, not the frequency at which it is pulsed.
Feeling somewhat cautious when faced with these inconsistencies, and in the best traditions of ‘romantic’ (rather than hard- headed) science, I decided to have a go at ‘handy curing’ myself before trying it out on my patients. First off, my incipient bilateral Dupuytrens, with variable frequency twice daily for one week, followed by

Reviews
© 2018 Acupuncture Association of Chartered Physiotherapists110
5 Hz for the following two weeks. By the end of three weeks, I could possibly imagine some softening of the cords in my hands, although a critic might comment that such an improvement could as well be attributable to taking a break from work and endless keyboard bashing, and instead performing regular self- massage by rub-bing the device over my hands. The condition certainly got little better, and may have even got worse, during the subsequent very hot weather. I also tried it on a mild ankle sprain (with ice and elevation – improved by the next day), a stubbed toe (ditto), some venous eczema (pos-sible improvement – although I have noticed in the past that this may happen with hotter, drier weather and less sitting about), holiday heat rash and insect bites (possible slowing down of recovery compared to untreated areas?), and an inadvertent but uncomfortable self- injury from stupidly biting the inside of my own cheek (healing no quicker than usual).
I then ventured to try it in conjunction with acupuncture on a patient with longstanding groin pain (‘some improvement’ – but he always says this improves after acupuncture treatment), and on a close relative with chronic peroneal tendonitis (pain worsened and changed charac-ter, becoming more intrusive). Another patient has been using the device for a painful shoulder injury and does report benefit from using it consistently on a daily basis, in combination with regular but less frequent acupuncture treatment!
These few results from my own somewhat subjective and non- rigorous investigations are clearly inconclusive. A closer look at the testimonials supplied – in addition to those included in the Acupuncture in Physiotherapy advertisement – gave me the impression that the Handy Cure S is often recommended as an adjunctive rather than stand- alone treatment, which begs the question of which interven-tion is really responsible for the improvements experienced – as so often when more than one treatment is involved. I have to say that I would have felt more like continuing with my own experiments if I understood the justification for the frequencies used in the three different programmes offered by the Handy Cure S, and
if protocols did not require daily use for three weeks. As I wrote about LILT over 20 years ago in this journal: “From these rather rough and ready results, it is clear that a patient has to be well moti-vated to take on this particular form of ‘homework.’” (Mayor 1996).
Over the years I have seen many therapy devices come and go, and perhaps have become too sceptical, less open, as a result. As we all are, I am also well aware that expectation – positive or negative – can affect the results of treatment (Mayor et al. 2017). To really test the benefits or otherwise of equipment like the Handy Cure S will require some well conducted studies where practitioner bias can be reduced, or perhaps even counterbalanced, with both sceptics and enthusiasts involved. For now, though, my own Handy Cure S will probably join the other devices in my well- stocked cup-board of those currently out of favour, while I get on with using my hands and needles – and electro acupuncture, of course!
David MayorVisiting Fellow (Physiotherapy)
Department of Allied Health ProfessionsMidwifery and Social Work University of Hertfordshire
UK
referencesFriedmann H., Lipovsky A., Nitzan Y. & Lubart R. (2009)
Combined magnetic and pulsed laser fields produce synergistic acceleration of cellular electron transfer. Laser Therapy 18 (3), 137–141.
Leal- Junior E. C., Johnson D. S., Saltmarche A. & Demchak T. (2014) Adjunctive use of combination of super- pulsed laser and light- emitting diodes photo-therapy on nonspecific knee pain: double- blinded randomized placebo- controlled trial. Lasers in Medical Science 29 (6), 1839–1847.
Mayor D. (1996) Light, light . . . and more light: on LEDs, lasers and lunacy. Journal of the Acupuncture Association of Chartered Physiotherapists (March), 19–22.
Mayor D. (2014) Intranasal Low Intensity Laser Therapy [Book review]. Journal of the Acupuncture Association of Chartered Physiotherapists 26 (2), 113–116.
Mayor D. F., McClure L. S. & McClure J. H. C. (2017) Nonspecific feelings expected and experienced during or immediately after electroacupuncture: a pilot study in a teaching situation. Medicines 4 (2), 19.

© 2018 Acupuncture Association of Chartered Physiotherapists 111
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 111–114
Book reviews
Pocket Atlas of Acupuncture and Trigger PointsBy Hans- Ulrich Hecker, Angelika Steveling, Elmar T. Peuker and Kay LiebchenThieme Medical Publishers, 2017, 392 pages, paperback, £40ISBN 978–3132416031
The previous edition of this book, published in 2001, was one of my favourite points manuals for a number of years. I used it so much that it eventually fell apart and it sadly now resides in a small A3 folder. As a result of this, I was intrigued to see what improvements had been made in the updated version and was pleasantly surprised at the content. The newer version has increased by over 150 pages and the book appears to be well organized in terms of the
three informative parts: “Body Acupuncture Points,” “Ear Acupuncture Points” and “Trigger Points.” Part 4 contains the appendices. Although each section was colour- coded in the previous version, this has now been improved so that each section can be distinctly seen on the outer edges of the pages.
Part 1 is divided into 16 sections containing a formal introduction, information on the 12 main channels, information on the Conception Vessel and Governing Vessel, and ending with a short section on Extra points. Pleasingly, the nomenclature of the channels aligns with the World Health Organization advice, but the book contains only the important and use-ful points rather than every point along every channel. This may be considered a flaw by some professionals but, for the novice Western medical practitioner, this book contains ample information for effective practice. One of the positive aspects is that some point descriptions contain safety notes and practical anatomical tips which will be useful in the early stages of acupuncture practice. There is also reference to traditional Chinese medical concepts, with some points having been described classically, for example source points, connecting points, mu points, tonification/sedation points and open-ing points. This may, however, be confusing to some practitioners.
The second part, “Ear Acupuncture,” is divided into 22 short sections describing points mainly from the perspective of two different philosophies, Chinese and Nogier, although a short reference to Bahr is also included. It also contains practical hints and tips along with safety advice. There are plenty of other auricu-lar acupuncture books on the market but this will be sufficient for any novice practitioner.
By far the most expansive section is Part 3 relating to trigger points. The section begins with a short definition of trigger points with the references arranged in the Vancouver style.
Book reviews
© 2018 Acupuncture Association of Chartered Physiotherapists112
Oddly, this is different referencing to those in Part 1 in that only authors are mentioned. One example is Bischko, who has three different citations in the reference list contained in the appendices but it is unclear to which article the information is referring. There are 34 short chapters each discussing a separate muscle or group of muscles which is a big increase on the 19 chapters of the 2001 version. Again, these sections also contain hints and safety tips and also relate these points to local acupuncture points. This information, although not as in- depth as is in some other trigger point manuals available, still covers enough material, such as location and pain projection patterns, that it is likely to be of value to all physiotherapists and not just novice practitioners.
Overall, I was pleased with the range of content in the book and would recommend it as a study aid for trainees on Foundation Acupuncture courses as well as a handy aide- memoire for more experienced practitioners.
Lesley PattendenAACP Tutor and Board Director
The Fundamentals of AcupunctureBy Nigel ChingSinging Dragon, London, 2017, 752 pages, hardback, £60ISBN 978–1848193130
From the introduction, Nigel Ching appears to be a well- renowned acupuncturist and author of many acupuncture- related books, with this one being a translation of a book previously written in Danish. His hardback book was the third points manual to be reviewed by myself and was of a completely different style compared to Hecker et al. (2017) and Bouratinos and Jarmey (2018), with it being principally aimed at stu-dents of traditional Chinese medicine (TCM).
This large tome of over 700 pages is his cur-rent interpretation of TCM principles as well as a manual for acupuncture points, although much of the information is based on the work of other well- known authors such as Giovanni Maciocia, Larre and Rochat de la Vallée, and Peter Deadman. From a practical viewpoint,
the book does not adhere to World Health Organization nomenclature (although, oddly, the reference for this does appear in the reference list), and none of the tables/boxes are titled so it is not always easy to relate information in these to the relevant text.
There are six parts, with Parts 1–3 explain-ing “Basic Principles,” “The Vital Substances” and “The Internal Organs.” There were some interesting viewpoints within Part 1: the author describes yin and yang as relative and not abso-lute, and gives some useful examples of this particularly relating to physiological processes. He also describes the Five Phases not as ele-ments but as energies that are dynamic and are under constant change, and briefly describes the influences of the Ko and Shen cycles in terms which can be easily understood by the most novice of acupuncturists.
In the introduction to “Vital Substances,” the author tries to describe Qi as an overall concept with his definition being: “Qi is that which makes us alive whilst at the same time all matter is Qi” (p. 70), which is probably the most thought provoking one- line definition that I have

Book reviews
© 2018 Acupuncture Association of Chartered Physiotherapists 113
encountered. He then goes on to describe the different forms and functions of Qi, Jing (essence), Xue (blood), Jinye (fluids) and Shen (spirit/mind) in greater detail.
Part 3 (“The Internal Organs”) is divided into Zang Fu and Fu organs and then each organ is described in more detail in a manner similar to that of Maciocia (2006) but without the useful summary boxes and coloured highlighting con-tained within that book.
Interestingly, in Part 4, in addition to the information on the 12 regular channels, he includes a more expansive section on the Eight Extraordinary Vessels compared to other texts which was pleasing to read.
Part 5 introduces the reader to points along the channels starting with a general TCM clas-sification of points. He also provides a handy quick reference box depicting a list of points for each category including Ghost points and Heavenly Star points as well as the usual source and transporting points. The book then provides a list of actions and indications with a list of explanations for some of the terms used in later descriptions such as “expel, disperse, activate, anchor” before reviewing every point on every meridian which could be useful for physiother-apists wanting to understand more TCM.
It is always useful to select a commonly- used point and compare between texts to ascertain the level and quality of the information pro-vided to ascertain if the book will have some value to the reader. For Large Intestine (LI) 4, there were no practical safety hints, precautions or precise locations noted as the information given related to indications for use such as “stops pain,” “induces labour” and “headaches,” with some limited commentary on each of the indications.
The final section is on the use of needle techniques to affect Qi such as Xu ji (fast- slow insertion), Nian zhuan (rotation of the needle) and Hu xi (breathing), all of which were inter-esting to read and useful for effective practice.
In summary, this was not a manual for point locations even though every point was described, but an introduction to TCM theory related to some aspects of practice. It would be an interesting read for those wishing to gain a
basic understanding of TCM theories but there are other books on the market with similar information so this one did not stand out as a “must buy” book to have in your personal library.
Lesley PattendenAACP Tutor and Board Director
referencesHecker H.- U., Steveling A., Peuker E. T. & Liebchen
K. (2017) Pocket Atlas of Acupuncture and Trigger Points. Thieme Medical Publishers.
Bouratinos I. & Jarmey C. (2018) A Practical Guide to Acupoints, 2nd edn. Lotus Publishing.
Maciocia G. (2006) The Foundations of Chinese Medicine, 2nd edn. Churchill Livingstone, Edinburgh.
A Practical Guide to Acupoints, 2nd edn.By Ilaira Bouratinos and Chris JarmeyLotus Publishing, 2018, 416 pages, paperback, £29.99ISBN 978–1905367801
There have been a number of updated points manuals appearing on the market in recent months and this is another that fits the brief. The previous version appeared 10 years ago so it was interesting to see what additional information has been included in this version. Interestingly, the introduction notes that Chris Jarmey died suddenly in 2008 and therefore the update appears mainly to be the work of the other author and her associates.
The introduction to this updated book clari-fies the audiences at which this book is aimed, and there has been an effort to include infor-mation relevant to complementary health practi-tioners such as those practising Shiatsu, magnet therapy and Guasha. Consequently, some of the information is irrelevant to the majority of physiotherapists practising acupuncture and this new information accounts for most of the extra 50 pages of this version.
The book has already been reviewed by an eminent acupuncturist who extolled the quality of drawings, the depth of information pre-sented and other useful information. Personally,
Book reviews
© 2018 Acupuncture Association of Chartered Physiotherapists114
I found that the drawings lacked colour and definition; that some of the information was not useful; and that, as a resource, it was not as user- friendly as it could have been.
The first nine chapters review the process of needling safely with precautions and contrain-dications (colour- coded yellow and red respec-tively), but also include chapters on moxibustion and cupping. In terms of point selection, some general principles are given in Chapter 7, but the classification of points (Chapter 6) is purely from a traditional Chinese medical perspective which may be confusing to those familiar with a more Westernized approach, although interest-ing to read.
Chapters 10–24 cover each meridian individu-ally with the page corners coloured appropriately for each pairing of meridians. The light grey colour used for Large Intestine/Lung and the light purple for Governor/Conception Vessels
are difficult to distinguish quickly when trying to find a point location on these meridians.
One of the positive aspects of the book is that it now contains information on every point on every meridian rather than selected points only, although most of the expanded infor-mation pertains to other professionals rather than physiotherapists. On the negative side, the book does not use standard World Health Organization (WHO) nomenclature which is a shame.
In the meridian chapters, there are 43 Extra points described, and the addition of these changes the page layout compared to the first edition. As a result, there is a noticeable amount of “empty space” at the end of pages and chapters.
Given that the nomenclature for Extra points is confusing anyway, Chapter 24 describing these does not add any further clarity to the situation because it does not use WHO guidance. For example, it describes M- BW- 1A/1B which do not exist in WHO, and the authors have added three “new” points for lumbar pain (located near metacarpals 2/3/4) that I have not seen written in other texts.
At the beginning of the book there appears to be an opportunity to download supple-mentary information, however after a number of attempts via email to do this, no further information has been forthcoming. The author states that, overall, she wants the manual to be useful to the lay person as well as for health professionals, and it does align to this aspiration. Therefore, it is suitable as a points manual resource for physiotherapists practising acupuncture but it purposely does not include any evidence base and only gives a nod to the concept of Western medicine.
Lesley PattendenAACP Tutor and Board Director

© 2018 Acupuncture Association of Chartered Physiotherapists 115
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 115–116
News, views and interviews
Clinical efficacy of acupuncture on rheumatoid arthritis Chou and Chu (2018) have reviewed 43 stud-ies on the clinical efficacy of acupuncture on rheumatoid arthritis (RA) published between 1974 and 2018 – of which all but one reported positive benefits.
According to traditional Chinese medicine (TCM), RA is categorized as belonging to bi or impediment diseases. This is a group of diseases caused by the invasion of wind, cold, dampness or heat pathogen on the meridians, involving muscles, sinews, bones and joints, manifested by local pain, soreness, heaviness, hotness, and even articular swelling, stiffness and deformities.
An estimated 60–90% of arthritis patients are reported to use complementary and alter-native medicine, including acupuncture. When taking study design into consideration, TCM theory was adapted substantially in most of the investigations. The authors found an interesting fact that acupoint Zu San Li Stomach (ST 36) was used in almost every research, followed by Yang Ling Quan Gall Bladder (GB 34) and Hegu Large Intestine (LI 4).
Measurements of quality of life have gained more interest among RA patients than other disease- related parameters such as inflammatory biomarkers or joint counts. Some studies in this review have adopted related questionnaires. Acupuncture was found to be able to improve the quality of life in all but one of the studies reviewed.
An anti- inflammatory effect has been the most well- known mechanism of how acupuncture works for RA; many studies in this review used inflammatory biomarkers for comparison such as erythrocyte sedimentation rate, C- reactive protein, rheumatoid factor, interleukins, nuclear factor- κB, and tumor necrosis factor- α. Dong et al. indicated that a toll- like receptor (TLR) sig-nalling pathway contributed to the development and progression of RA and acupuncture could
reduce the expression of TLR4, thus leading to anti- inflammatory effects. Another possible mechanism could be attributed to the anti- oxidative effect (such as inducing the increased activities of super oxide dismutase and catalase in the serum of RA), alleviating oxidative stress and inflammation, and improving antioxidant and energy metabolic status.
Acupuncture has its root in TCM; tradition-ally, TCM does not seek the specific pathogen and pathological changes in a specific organ or individual, but seeks the disturbances among the self- controlled systems by analyzing all symp-toms and signs. The TCM therapeutics work by activating and improving system connection and enhancing human resistance. The mechanism in TCM is not like modern medicine that seeks the mechanism from cellular or molecular per-spectives. In light of this, to accomplish a well- designed randomized controlled trial (RCT) that has every possible variable controlled and takes TCM theory into account is extremely difficult
Each investigation, with the exception of one trial, found that any kind of acupuncture as the main treatment or adjuvant treatment tool could benefit clinical conditions of RA in human or animal subjects. There were no adverse effects of acupuncture reported. However, the authors note that there is still inconsistency regarding the clinical efficacy and lack of well- designed human/animal double- blinded RCTs. They suggest that future discussion for further agree-ment on taking TCM theory into consideration as much as possible is a top priority.
Rosemary LillieNews Editor
referenceChou P. - C. & Chu H. - Y. (2018) Clinical efficacy of acu-
puncture on rheumatoid arthritis and associated mech-anisms: a systemic review. Evidence- based Complementary and Alternative Medicine 2018, Article ID 8596918.

News, views and interviews
© 2018 Acupuncture Association of Chartered Physiotherapists116
helene langevin named as Director of the National Center for Complementary and Integrative health Dr Helene Langevin – familiar to many AACP members as AACP President – has been announced as the new Director of the National Center for Complementary and Integrative Health (NCCIH) in the US.
The NCCIH is the Federal government’s lead agency for scientific research on the diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine.
“Helene’s distinguished career and leadership in the integrative health community, along with her research on the role of non- pharmacological treatment for pain, makes her ideally suited to lead NCCIH,” said Dr. Francis Collins, National Institutes of Health (NIH) Director. “We are so pleased to have her join the NIH leadership team.”
Helene has published many influential papers on the physical and physiological effects of acu-puncture. She has lectured in the past at AACP annual conferences, and has a particular interest in the behaviour of fascia.
If you are interested in exploring her research, the feature article highlighted in the reference below will give a good overview, as well as providing further references to articles she has written.
Everyone at AACP congratulates Helene, and we wish her every success in this new role.
Rosemary LillieNews Editor
referenceLangevin, H (2013) The science of stretch. The Scientist
May 2013 [WWW document.] URL https://www.the- scientist.com/features/the- science- of- stretch- 39407

© 2018 Acupuncture Association of Chartered Physiotherapists 117
Acupuncture in Physiotherapy, Volume 30, Number 2, Autumn 2018, 117–119
Guidelines for authors
IntroductionAlways refer to a recent edition of Acupuncture in Physiotherapy. Please follow the style and layout of an article or item that is similar to your own contribution. If something is submitted for publication, then it is implied that it has not been simultaneously submitted to another journal or any other type of publication. Reprints may be considered, but these must be clearly identified as such and permission must be obtained from the original publisher.
Templates for clinical papers and case reports are available on the AACP website (www.aacp.org.uk), or by email on request. These templates should not be deviated from if used. Manuscripts may be returned to authors if they have not adhered to the guidelines. If necessary, the clini- cal editor should be consulted in the initial stages for clarification.
Authors may submit clinical papers, literature reviews, clinical commentaries, case reports, book reviews, course reports, news items, letters or photographs for consideration for inclu- sion in the journal. Academic and clinical papers are subject to review by the editorial committee and may require revision before being accepted.
A Portable Document Format (PDF) file of the final version of any academic article is available free of charge if notice is given to the clinical editor when the article is submitted.
All published material becomes the copyright of the Association.
All submissions should be sent directly to the clinical editor:
Dr Val Hopwood FCSP18 Woodlands CloseDibden PurlieuSouthampton SO45 4JGUK
Email: [email protected]
Preparation of manuscriptsAuthors should submit material by email or on CD-ROM. All articles must be typed with wide (3-cm) margins and the pages should be num-bered consecutively. Articles should be a maxi-mum of 7500 words (excluding the abstract, references and tables).
Papers should be arranged as follows:
TitleThe title of the article should be in sentence case, bold and ranged left, as in the main title above: note that there is no full stop and no underlining. The author’s name(s) and institutional affilia-tion(s) should run consecutively below the title. Again, there are no full stops.
Abstract A summary of not more than 250 words outlin-ing the purpose, scope and conclusions of the paper should be submitted. This should be followed by a minimum of three and a maximum of five keywords that best represent the contents.
Text The layout of the journal is that the main heading of each section is in sentence case and bold. Notice that, again, there are no full stops and no underlining.
The first paragraph is left-justified; subsequent paragraphs in the same section are indented, as is this part of the guidelines. When including dia- grams and photographs, these should be num-bered in the order in which they appear in the text, and should be submitted in separate files (do not embed images in the text). Any figure captions should be left-justified and run after the author’s biography at the end of the text. Any tables should come after the figure legends, if there are any. Please indicate placement in the text (e.g. “Fig. 1’’ and “Table 1’’). All figures and tables must be referred to in the text.

Guidelines for authors
© 2018 Acupuncture Association of Chartered Physiotherapists118
When using numbers in the text, these should be written out in words up to and including nine unless these are measurements, numbers in tables or units of time. Always use the Inter-national System of Units (SI).
Clinical papers: referencing All clinical papers must be fully referenced and the citations verified by the author. No excep-tions will be made. The reference list must be arranged alphabetically by the name of the first author or editor, following the Harvard style. In the text, give the author(s) and date of publica-tion in brackets [e.g. “(Smith 1998)’’], or if the main author’s name is part of a sentence, then only the year is in brackets [e.g. “as described by Smith (1998)’’]. For more than one author, reference can be made in the text to “Smith et al. (1998)’’ (note the italics). However, when writ- ing the reference list, the convention is as fol-lows: for up to five authors, write all the authors’ names; for six or more authors, write the first three authors’ names, followed by “et al.”
For journals, give the author’s surname and initials, the year of publication, the title of the paper, the full name of the journal, the volume number, the issue number in brackets, and the first and last page numbers of the article (note the correct use of italic, bold, commas and full stops):
Ceccherelli F., Rigoni M. T., Gagliardi G. & Ruzzante L. (2002) Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind randomized controlled study. Clinical Journal of Pain 18 (3), 149–153.
For books, give the author’s/editor’s surname and initials, the year of publication, the book title in italics, and the publisher and city of publication:
Williams P. L. & Warwick R. (eds) (1986) Gray’s Anatomy, 36th edn. Churchill Livingstone, Edinburgh.
For a chapter or section in a book by a named author (who may be one of several contributors), both chapter and book title should be given, along with the editor’s name(s), and the first and last page numbers of the chapter:
Bekkering R. & van Bussel R. (1998) Segmental acupunc-ture. In: Medical Acupuncture: A Western Scientific Approach (eds J. Filshie & A. White), pp. 105–135. Churchill Livingstone, Edinburgh.
For references to documents on the World Wide Web (WWW), give the author’s surname followed by all initials, the year of publication in brackets, the document title in italics, an indica-tion that it is a WWW document in square brackets and the complete Uniform Resource Locator (URL):
List D. (2004) Maximum Variation Sampling for Surveys and Consensus Groups. [WWW document.] URL http://www.audiencedialogue.net/maxvar.html
Please adhere strictly to this style of referencing in any contribution to the journal.
Acknowledgements Please state any funding sources, or companies providing technical or equipment support.
Photographs Photographs may be submitted in colour or black-and-white, but will be printed in mono-chrome. Images must be in sharp focus. Photo-graphs should be numbered and their placing indicated in the text. Digital photographs should be of high resolution (i.e. a minimum of 300 dots per inch).
Line illustrations These should follow the style used in the journal, i.e. any labelling text should be in sentence case (10-point, Arial font), graphs should be two-dimensional and all images must be mono-chrome. As with photographs, line illustrations should be numbered and their placement indi-cated in the text. All images should be of high resolution (i.e. a minimum of 1200 dots per inch).
Case reportsThe journal welcomes case reports of up to 3000 words. These should be structured as follows: title, abstract and keywords, a brief

Guidelines for authors
© 2018 Acupuncture Association of Chartered Physiotherapists 119
introduction, a concise description of the patient and condition, and an explanation of the assess-ment, treatment and progress, followed finally by a discussion and evaluation of the implications for practice. The study must be referenced throughout. Further guidance is available upon request.
Book reviewsAt the beginning of the review, give all details of the book including the title in bold, the author/editor’s full name(s), publisher, city and year of publication, price, whether hardback or paper-back, number of pages, and ISBN number. The reviewer’s name should appear at the end of the review in bold, right-justified, followed by their title and place of work in italics. Reviews of DVDs and DVD-ROMs should follow the same format. Book reviews and reports are normally
no more than 500 words in length; query for longer.
Please contact the book review editor before writing a review.
General points to notePlease enclose your home, work and email addresses, and telephone number.
It is the author’s responsibility to obtain and acknowledge permission to reproduce any material that has appeared in another journal or textbook.
A brief biographical note about the author(s) should be included at the end of a clinical paper in italics.
All notes and news should have clinical rel-evance to AACP. Please refer at all times to the style and layout of previous issues of the journal for whatever you are writing. Using these guide-lines will save the editorial team time.

Save The Date!DATE: Saturday 18th May 2019TIME: 9:00am - 5:00pm
DoubleTree by Hilton,London Docklands,London,SE16 5HW
4-for-3 GROUP DISCOUNTS
AACP ANNUAL CONFERENCE
2 0 1 9Celebrating our...
#AACP35
Join us in London for our biggest conference yet. We will also be celebrating our 35th anniversary on Friday 17th May with an evening of fun, food and festivities...with a few surprises! We are offering complimentary tickets to the anniversary celebrations for a limited number of conference delegates. Full speaker line-up to be announced soon. Join us on Facebook, Twitter and LinkedIn to make sure you don’t miss any announcements.
www.aacp.org.uk
Acupuncture in PhysiotherapyTM
Journal of the Acupuncture Associationof Chartered Physiotherapists
Autumn 2018 Volume 30, Number 2
ISSN 2058-3281
Acupuncture in Physiotherapy
TMVolum
e 30, Num
ber 2, Autum
n 2018
ACUPUNCTURE & MOXA TREATMENT ROOM
SPORTREHAB & EXERCISE
TAPING MASSAGE
SUPPORTS & BRACESCUPPING
© M
artin
mar
k | D
ream
stim
e
Sports & Physical Therapiesincluding Acupuncture, Moxibustion
Cupping, Magnetic and much more...
www.harmonymedical.co.ukt: +44 (0)208 5187337 e: [email protected]


















