Forensic Implications of Treating Traumatic Brain Injury ... Jacquin ACFP2018 Poster.pdfwarfare...
1
• INTRODUCTION Forensic Implications of Treating Traumatic Brain Injury in the Military Rachaell Dockery, Mark Kaminski, & Kristine M. Jacquin American College of Forensic Psychology 2018 The most common injuries in today’s warfare are Traumatic Brain Injuries (TBIs), with more than 360,000 military personnel and veterans (MPV) diagnosed between 2000 and 2016 6 : Army: 217,294 Marines: 52,715 Air Force: 50,391 Navy: 50,288 MPVs are more likely to acquire TBIs than civilian peers, due to the nature of their job, combat exposure, and military training. Although TBIs may result in physical impairment, more problematic consequences pertaining to forensic psychology involve MPV’s cognitive, emotional, and behavioral functioning. Dysfunction and dysregulation tendencies may negatively affect development and maintenance of interpersonal relationships and functioning in social settings, and reduce quality of life; these changes may result in criminality. The interrelated complexity of physical, cognitive, and emotional effects of TBIs often require the collaboration of neurologists, psychologists, psychiatrists, & occupational and physical therapists as a multi-disciplinary care team 9 . Better identification of TBIs and comorbid disorders in MPVs, along with military culturally sensitive treatment modalities and collaboration of specialty teams, may prevent problems that could result in criminal or civil litigation. TBIs may be primary, secondary, tertiary, or quaternary blast-induced injuries 6 . Blast injuries may result in poly-trauma injuries, neuropsychological impairments 9 as well as co-occurring mental health disorders. The uniqueness of “mission first” ideology and high operational tempos in military arenas makes it challenging for providers to identify and treat MPVs with TBIs. TBIs often impair functioning ability in family and social interactions, reflected in MPV behavioral or mood changes. TBIs frequently affect similar brain regions as posttraumatic stress disorder (PTSD); stress-associated maladaptive responses and dysfunctions are risks factors for arrest and incarceration. Studies show a correlation between frontal lobe dysfunction (a common blast impact area) and increased aggressive behavior 3 . Research further implies TBI patients with impulsive and aggressive behavioral tendencies may have elevated risks for verbal aggression and physical altercations 11 . IMPLICATIONS Scientific knowledge about the effects of TBIs is relativity new and limited. Unlike the private sector, MPVs face many treatment seeking barriers in military settings such as geographic access to specialized facilities 5 , limited specialty care providers 4 and inconsistent care due to multiple facility transitions 9 . Treatment delays may result in higher levels of disability, poorer outcomes and increased risks of developing comorbid disorders 2 . Interventions based on civilian population research may not be as effective or meet the needs of the military population due to warfare trauma and complex brain injuries 11 . Disorders such as depression and PTSD, and other traumas such as military sexual trauma may cloud diagnosis. Grief from blast circumstances (body mutilation and civilian casualties), survivor guilt, and loss of physical and mental abilities, may interfere with treatment outcomes 10 . As a result, numerous TBIs go underreported or undetected. MPV often require psychological treatment that may include pharmacotherapy, anger management, CBT, exposure therapy and psychoeducation 9,13 to prevent problems. Due to limited evidence-based clinical approaches and mental health stigmas, providing effective treatment may be difficult. Additionally, treatment conflicts may arise such as pharmacology used for PTSD symptoms may adversely affect TBI symptoms, and may lead to potential violence 15 . Moreover, research established MPVs are less likely to seek mental health care due to career repercussions and warrior culture 7;11;15 . With the increased propensity to suffer from psychological problems from TBIs, MPVs may be more prone to behavioral problems and substance abuse, identified as potential incarceration risks factors. These problems conflict with military standards of discipline and often result in a behavioral discharge. Unwanted or less than honorable discharges will likely result in litigation. MPVs continue to report long waitlists, processing delays, ongoing pain, addictive medication use, mental health treatment needs, and help with daily activities, which may require legal assistance. Research shows violent tendencies, substance abuse, domestic violence, and risky behaviors, are potential risk factors for altercations resulting in incarceration. Research links military service to higher divorce rates. Unnoticed or underreported mild-to-moderate TBIs may invalidate restrictive time frames and criteria to apply and receive VA Benefits, which increases the likelihood of civil litigation for treatment and services 9 . Adapt current approaches or develop novel interventions specifically geared towards MPVs with TBI and PTSD Using Complementary Alternative Medicine (CAM) therapies removes stigmas, limits side effects, and encourages involvement. CAM approaches are adaptable for physical disabilities and are available in military and private sectors. Refer MPVs to Vet Centers that offer diverse treatment options such as group and family therapy, and provide confidentially from commanders and veteran court judges. Consider legal alternatives similar to Veterans Courts and intervention referral programs such as Project NOVA 8 , that provide treatment options instead of incarceration, which may help decrease recidivism. Diagnosing comorbid disorders may reduce arrest or incarceration risk factors. Collaborate with multi-disciplinary care specialists to create a patient centered treatment plan, sensitive to the unique military culture and specialized needs of MPVs with TBIs. TBIs among MPVs present challenges for providers to meet the unique health care needs of MPVs, while reducing criminal and civil litigation risk factors. Proactively identifying TBIs and co-occurring disorders may reduce criminal behavior and legal involvement. Employing patient centered treatment programs instead of incarceration may decrease recidivism. Using interventions focused on reducing mood changes and risk-taking behaviors linked to hypervigilance, agitation, and aggressiveness may reduce criminal justice involvement. Therapeutic approaches that are culturally sensitive to the MPV population such as CAM and group therapies, will likely increase participation, improve emotional and cognitive functionality, and reduce criminality. Future research should specifically investigate MPV blast- related brain injuries to better identify impacted areas, long- term effects, and the relevance of symptoms and co- occurring disorders on criminology. New treatment approaches or adaptations to current approaches specifically geared toward MPVs with TBI/ PTSD may be more effective in reducing problems and risk factors that may result in criminal or civil litigation 16 . STATISTICS A recent VA study found 36% of MPVs suffering from a TBI comorbidly suffered with depression and an additional 35% were diagnosed with PTSD 13 : Other studies note correlations between MPVs diagnosed with PTSD and TBI, and increased incarceration, aggression, or violence from previous conflicts 17;7 . The Institute of Medicine reported that criminal justice involvement is one of the most significant issues faced by Iraq and Afghanistan war MPV 7 . CONCLUSIONS REFERENCES Symptoms Most Commonly Reported as Persisting Over Time MILITARY & VETERAN TBIs POTENTIAL LEGAL ISSUES 0 10 20 30 40 50 60 70 Memory Loss Inattention Poor Concentration Irritability Poor Sleep High Group Low Group Prior studies indicate MPVs described prolonged and persistent symptoms years after initial TBI injury, without patterns of predictability or uniformity (see figure above) 12 . Of those MPVs who reported a probable TBI while being deployed, 57% had not been evaluated by a physician for a brain injury that may lead to developing comorbid mental health issues 17 . 1 Bogdanova, Y., & Verfaellie, M. (2012). Cognitive sequelae of blast-induced traumatic brain injury: Recovery and rehabilitation. Neuropsychology Review, 22(1), 4-20. doi:10.1007/s11065-012-9192-3 2 Brain Injury Association of America. (2009). Traumatic brain injury in the United States: A call for public/private cooperation. Retrieved from http://www.biausa.org 3 Brower, M. C., & Price, B. (2001). Neuropsychiatry of frontal lobe dysfunction in violent and criminal behaviour: A critical review. Journal of Neurology, Neurosurgery & Psychiatry, 71(6), 720-726. doi: 10.1136/jnnp.71.6.720 4 Connors, S. H., Gordon, W. A., Ashley, M. J., Trudel, T. M., & Braunling-McMorrow, D. (2007). Traumatic brain injury in the United States: A call for public/private cooperation. Brain Injury Association of America, 1-16. 5 Cote, M. J., Syam, S. S., Vogel, W. B., & Cowper, D. C. (2007). A mixed integer programming model to locate traumatic brain injury treatment units in the Department of Veterans Affairs: A case study. Health Care Management Science, 10(3), 253-267. doi:10.1007/s10729-007-9018-7 6 Defense and Veterans Brain Injury Center. (2017). DoD worldwide numbers for traumatic brain injury. Retrieved from http://dvbic.dcoe.mil/dod-worldwide-numbers-tbi 7 Elbogen, E. B., Johnson, S. C., Newton, V. M., Straits-Troster, K., Vasterling, J. J., Wagner, H. R., & Beckham, J. C. (2012). Criminal justice involvement, trauma, and negative affect in Iraq and Afghanistan war era veterans. Journal of Consulting and Clinical Psychology, 80(6), 1097-1102. doi:10.1037/ a0029967 8 Fossey, M., Cooper, L., Godier, L., & Cooper, A. (2017). A pilot study to support veterans in the criminal justice system: Final report. Retrieved from http://www.fim-trust.org/wp-content/uploads/ 2017/04/Project-Nova-Report.pdf 9 Jaffee, M. S., Helmick, K. M., Girard, P. D., Meyer, K. S., Dinegar, K., & George, K. (2009). Acute clinical care and care coordination for traumatic brain injury within Department of Defense. The Journal of Rehabilitation Research and Development, 46(6), 655-666. doi:10.1682/jrrd.2008.09.0114 10 Kerr, L. K. (2017, January 12). Responding to moral injury in veterans. Retrieved from https:// www.laurakkerr.com/2017/01/12/responding-to-moral-injury/ 11 King, P. R., & Wray, L. O. (2012). Managing behavioral health needs of veterans with traumatic brain injury (TBI) in primary care. Journal of Clinical Psychology in Medical Settings, 19(4), 376-392. doi: 10.1007/s10880-012-9345-9 12 Lange, R. T., Brickell, T. A., Ivins, B., Vanderploeg, R. D., & French, L. M. (2013). Variable, not always persistent, postconcussion symptoms after mild TBI in U.S. military service members: A five- year cross-sectional outcome study. Journal of Neurotrauma, 30(11), 958-969. doi:10.1089/neu. 2012.2743 13 National Institutes of Health. (2016). What are the treatments for TBI? Retrieved from https://www.nichd.nih.gov/health/topics/tbi/conditioninfo/Pages/treatment.aspx 14 Pine Tree Legal Assistance. (2010). A veteran’s guide to traumatic brain injury: Identifying and caring for TBI. Retrieved from https://statesidelegal.org/sites/default/files/Veterans%20guide%20to%20TBIs.pdf 15 Shrivastava, A., Bureau, Y., Rewari, N., & Johnston, M. (2013). Clinical risk of stigma and discrimination of mental illnesses: Need for objective assessment and quantification. Indian Journal of Psychiatry, 55(2), 178. doi:10.4103/0019-5545.111459 16 Strom, T. Q., Wolf, G. K., Crawford, E., Blahnik, M., & Kretzmer, T. (2016). Implementing prolonged exposure for veterans with comorbid PTSD and traumatic brain injury: Two case studies. Cognitive and Behavioral Practice, 23(2), 148-161. doi:10.1016/j.cbpra.2015.03.003 17 Tanielian, T., Jaycox, L. H., Schell, T., Marshall, G. N., Burnam, M. A., Eibner, C., . . . Vaiana, M. E. (2008, April 08). Invisible wounds: Mental health and cognitive care needs of America's returning veterans. Retrieved from https://www.rand.org/pubs/research_briefs/RB9336.html POSSIBLE SOLUTIONS STATISTICS
Transcript of Forensic Implications of Treating Traumatic Brain Injury ... Jacquin ACFP2018 Poster.pdfwarfare...

•
INTRODUCTION
Forensic Implications of Treating Traumatic Brain Injury in the Military
Rachaell Dockery, Mark Kaminski, & Kristine M. Jacquin
American College of Forensic Psychology 2018
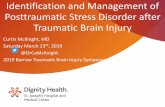
The most common injuries in today’s warfare are Traumatic Brain Injuries (TBIs), with more than 360,000 military personnel and veterans (MPV) diagnosed between 2000 and 2016 6 :
Army: 217,294 Marines: 52,715 Air Force: 50,391 Navy: 50,288
MPVs are more likely to acquire TBIs than civilian peers, due to the nature of their job, combat exposure, and military training.
Although TBIs may result in physical impairment, more problematic consequences pertaining to forensic psychology involve MPV’s cognitive, emotional, and behavioral functioning.
Dysfunction and dysregulation tendencies may negatively affect development and maintenance of interpersonal relationships and functioning in social settings, and reduce quality of life; these changes may result in criminality.
The interrelated complexity of physical, cognitive, and emotional effects of TBIs often require the collaboration of neurologists, psychologists, psychiatrists, & occupational and physical therapists as a multi-disciplinary care team 9.
Better identification of TBIs and comorbid disorders in MPVs, along with military culturally sensitive treatment modalities and collaboration of specialty teams, may prevent problems that could result in criminal or civil litigation.
TBIs may be primary, secondary, tertiary, or quaternary
blast-induced injuries 6. Blast injuries may result in poly-trauma injuries,
neuropsychological impairments 9 as well as co-occurring mental health disorders.
The uniqueness of “mission first” ideology and high operational tempos in military arenas makes it challenging for providers to identify and treat MPVs with TBIs.
TBIs often impair functioning ability in family and social interactions, reflected in MPV behavioral or mood changes.
TBIs frequently affect similar brain regions as posttraumatic stress disorder (PTSD); stress-associated maladaptive responses and dysfunctions are risks factors for arrest and incarceration.
Studies show a correlation between frontal lobe dysfunction (a common blast impact area) and increased aggressive behavior 3.
Research further implies TBI patients with impulsive and aggressive behavioral tendencies may have elevated risks for verbal aggression and physical altercations 11.
IMPLICATIONS Scientific knowledge about the effects of TBIs is relativity new
and limited. Unlike the private sector, MPVs face many treatment seeking
barriers in military settings such as geographic access to specialized facilities 5, limited specialty care providers 4 and inconsistent care due to multiple facility transitions 9.
Treatment delays may result in higher levels of disability, poorer outcomes and increased risks of developing comorbid disorders 2.
Interventions based on civilian population research may not be as effective or meet the needs of the military population due to warfare trauma and complex brain injuries 11.
Disorders such as depression and PTSD, and other traumas such as military sexual trauma may cloud diagnosis.
Grief from blast circumstances (body mutilation and civilian casualties), survivor guilt, and loss of physical and mental abilities, may interfere with treatment outcomes 10.
As a result, numerous TBIs go underreported or undetected. MPV often require psychological treatment that may include
pharmacotherapy, anger management, CBT, exposure therapy and psychoeducation 9,13 to prevent problems.
Due to limited evidence-based clinical approaches and mental health stigmas, providing effective treatment may be difficult.
Additionally, treatment conflicts may arise such as pharmacology used for PTSD symptoms may adversely affect TBI symptoms, and may lead to potential violence 15.
Moreover, research established MPVs are less likely to seek mental health care due to career repercussions and warrior culture7;11;15.
With the increased propensity to suffer from psychological problems from TBIs, MPVs may be more prone to behavioral problems and substance abuse, identified as potential incarceration risks factors.
These problems conflict with military standards of discipline and often result in a behavioral discharge. Unwanted or less than honorable discharges will likely result in litigation.
MPVs continue to report long waitlists, processing delays, ongoing pain, addictive medication use, mental health treatment needs, and help with daily activities, which may require legal assistance.
Research shows violent tendencies, substance abuse, domestic violence, and risky behaviors, are potential risk factors for altercations resulting in incarceration.
Research links military service to higher divorce rates. Unnoticed or underreported mild-to-moderate TBIs may
invalidate restrictive time frames and criteria to apply and receive VA Benefits, which increases the likelihood of civil litigation for treatment and services 9.
Adapt current approaches or develop novel interventions specifically geared towards MPVs with TBI and PTSD
Using Complementary Alternative Medicine (CAM) therapies removes stigmas, limits side effects, and encourages involvement. CAM approaches are adaptable for physical disabilities and are available in military and private sectors.
Refer MPVs to Vet Centers that offer diverse treatment options such as group and family therapy, and provide confidentially from commanders and veteran court judges.
Consider legal alternatives similar to Veterans Courts and intervention referral programs such as Project NOVA 8, that provide treatment options instead of incarceration, which may help decrease recidivism.
Diagnosing comorbid disorders may reduce arrest or incarceration risk factors.
Collaborate with multi-disciplinary care specialists to create a patient centered treatment plan, sensitive to the unique military culture and specialized needs of MPVs with TBIs.
TBIs among MPVs present challenges for providers to meet the unique health care needs of MPVs, while reducing criminal and civil litigation risk factors.
Proactively identifying TBIs and co-occurring disorders may reduce criminal behavior and legal involvement.
Employing patient centered treatment programs instead of incarceration may decrease recidivism.
Using interventions focused on reducing mood changes and risk-taking behaviors linked to hypervigilance, agitation, and aggressiveness may reduce criminal justice involvement.
Therapeutic approaches that are culturally sensitive to the MPV population such as CAM and group therapies, will likely increase participation, improve emotional and cognitive functionality, and reduce criminality.
Future research should specifically investigate MPV blast-related brain injuries to better identify impacted areas, long-term effects, and the relevance of symptoms and co-occurring disorders on criminology.
New treatment approaches or adaptations to current approaches specifically geared toward MPVs with TBI/PTSD may be more effective in reducing problems and risk factors that may result in criminal or civil litigation 16.
STATISTICS A recent VA study found 36% of MPVs suffering from a TBI comorbidly suffered with depression and an additional 35% were diagnosed with PTSD 13: Other studies note correlations between MPVs diagnosed with PTSD and TBI, and increased incarceration, aggression, or violence from previous conflicts 17;7. The Institute of Medicine reported that criminal justice involvement is one of the most significant issues faced by Iraq and Afghanistan war MPV 7.
CONCLUSIONS
REFERENCES
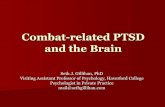
Symptoms Most Commonly Reported as Persisting Over Time
MILITARY & VETERAN TBIs
POTENTIAL LEGAL ISSUES
0 10 20 30 40 50 60 70
Memory Loss Inattention
Poor Concentration Irritability
Poor Sleep
High Group Low Group
Prior studies indicate MPVs described prolonged and persistent symptoms years after initial TBI injury, without patterns of predictability or uniformity (see figure above)12.
Of those MPVs who reported a probable TBI while being deployed, 57% had not been evaluated by a physician for a brain injury that may lead to developing comorbid mental health issues 17.
1 Bogdanova, Y., & Verfaellie, M. (2012). Cognitive sequelae of blast-induced traumatic brain injury: Recovery and rehabilitation. Neuropsychology Review, 22(1), 4-20. doi:10.1007/s11065-012-9192-3
2 Brain Injury Association of America. (2009). Traumatic brain injury in the United States: A call for public/private cooperation. Retrieved from http://www.biausa.org
3 Brower, M. C., & Price, B. (2001). Neuropsychiatry of frontal lobe dysfunction in violent and criminal behaviour: A critical review. Journal of Neurology, Neurosurgery & Psychiatry, 71(6), 720-726. doi:10.1136/jnnp.71.6.720
4 Connors, S. H., Gordon, W. A., Ashley, M. J., Trudel, T. M., & Braunling-McMorrow, D. (2007). Traumatic brain injury in the United States: A call for public/private cooperation. Brain Injury Association of America, 1-16.
5 Cote, M. J., Syam, S. S., Vogel, W. B., & Cowper, D. C. (2007). A mixed integer programming model to locate traumatic brain injury treatment units in the Department of Veterans Affairs: A case study. Health Care Management Science, 10(3), 253-267. doi:10.1007/s10729-007-9018-7
6 Defense and Veterans Brain Injury Center. (2017). DoD worldwide numbers for traumatic brain injury. Retrieved from http://dvbic.dcoe.mil/dod-worldwide-numbers-tbi
7 Elbogen, E. B., Johnson, S. C., Newton, V. M., Straits-Troster, K., Vasterling, J. J., Wagner, H. R., & Beckham, J. C. (2012). Criminal justice involvement, trauma, and negative affect in Iraq and Afghanistan war era veterans. Journal of Consulting and Clinical Psychology, 80(6), 1097-1102. doi:10.1037/a0029967
8 Fossey, M., Cooper, L., Godier, L., & Cooper, A. (2017). A pilot study to support veterans in the criminal justice system: Final report. Retrieved from http://www.fim-trust.org/wp-content/uploads/2017/04/Project-Nova-Report.pdf
9 Jaffee, M. S., Helmick, K. M., Girard, P. D., Meyer, K. S., Dinegar, K., & George, K. (2009). Acute clinical care and care coordination for traumatic brain injury within Department of Defense. The Journal of Rehabilitation Research and Development, 46(6), 655-666. doi:10.1682/jrrd.2008.09.0114
10 Kerr, L. K. (2017, January 12). Responding to moral injury in veterans. Retrieved from https://www.laurakkerr.com/2017/01/12/responding-to-moral-injury/
11 King, P. R., & Wray, L. O. (2012). Managing behavioral health needs of veterans with traumatic brain injury (TBI) in primary care. Journal of Clinical Psychology in Medical Settings, 19(4), 376-392. doi:10.1007/s10880-012-9345-9
12 Lange, R. T., Brickell, T. A., Ivins, B., Vanderploeg, R. D., & French, L. M. (2013). Variable, not always persistent, postconcussion symptoms after mild TBI in U.S. military service members: A five-year cross-sectional outcome study. Journal of Neurotrauma, 30(11), 958-969. doi:10.1089/neu.2012.2743
13 National Institutes of Health. (2016). What are the treatments for TBI? Retrieved from https://www.nichd.nih.gov/health/topics/tbi/conditioninfo/Pages/treatment.aspx
14 Pine Tree Legal Assistance. (2010). A veteran’s guide to traumatic brain injury: Identifying and caring for TBI. Retrieved from https://statesidelegal.org/sites/default/files/Veterans%20guide%20to%20TBIs.pdf
15 Shrivastava, A., Bureau, Y., Rewari, N., & Johnston, M. (2013). Clinical risk of stigma and discrimination of mental illnesses: Need for objective assessment and quantification. Indian Journal of Psychiatry, 55(2), 178. doi:10.4103/0019-5545.111459
16 Strom, T. Q., Wolf, G. K., Crawford, E., Blahnik, M., & Kretzmer, T. (2016). Implementing prolonged exposure for veterans with comorbid PTSD and traumatic brain injury: Two case studies. Cognitive and Behavioral Practice, 23(2), 148-161. doi:10.1016/j.cbpra.2015.03.003
17 Tanielian, T., Jaycox, L. H., Schell, T., Marshall, G. N., Burnam, M. A., Eibner, C., . . . Vaiana, M. E. (2008, April 08). Invisible wounds: Mental health and cognitive care needs of America's returning veterans. Retrieved from https://www.rand.org/pubs/research_briefs/RB9336.html
POSSIBLE SOLUTIONS
STATISTICS