Flis Henwood School of Applied Social Science University of Brighton.
25
Caring, sharing and service managing: The multiple realities of the primary care EPR Flis Henwood School of Applied Social Science University of Brighton
-
Upload
branden-campbell -
Category
Documents
-
view
215 -
download
1
Transcript of Flis Henwood School of Applied Social Science University of Brighton.
Caring, sharing and service managing: The multiple realities
of the primary care EPRFlis Henwood
School of Applied Social ScienceUniversity of Brighton
‘A lot of GP data is precisely and accurately recorded but not necessarily linked to diagnostic categories- you can’t necessarily look at all the data and identify everyone with heart disease. I’m not convinced that what is promised to us of open data is really what we can get’ (Dr Paul Cundy, IT spokesman on BMA’s GP Committee, writing about the care.data programme, in E-Health Insider October 2014)
‘Record quality is not an abstract concept but must be considered in relation to the fitness of information for a particular purpose. Careful recording and well-designed systems can help ensure that the record is fit for the range of purposes for which it might be used, but it may not possible to support all purposes equally and where compromise is necessary GPs should remember that the usual main purpose of their records is to support the care of individual patients’ (RCGP, 2009, p65, emphasis added)
‘GPs and their practice teams, are most likely to record information if they believe it to be important or relevant to a given context, which they have in mind at the time of recording (RCGP Health Informatics Task Force. Scope EPR Project report 1998.) This may include direct patient care, commissioning, sharing, Quality and Outcomes Framework, research or medico-legal factors. Relevance is therefore likely to be playing a key role in determining recording behaviour, raising the question of how individuals come to decide what is or is not important or relevant in a given context. This might be amenable to education and training’ (DH, RCGP and BMA, 2011 p76, emphasis added)
‘Seen as a site where multiple stories about patients and organisations are at stake, including the interoperability between these stories, the medical record becomes highly relevant both analytically and politically’ (Berg and Bowker, 1997, abstract)
‘Clinicians…saw the problem as one of how to reconcile the need to collect diagnostic data in the consultation in a way that makes it re-usable for other purposes, without damaging their relationships with their patients’ (Lusignan, 2003, p416, emphasis added).
Ford et al (2013) conclude: ‘doctors’ concerns are more centred on creating records that are useful to them and their team at the point of care, rather than on creating records that will be accessible for secondary uses’
Tensions in recording…
‘accept that coding is here to stay (and brings enormous benefits) but that primary care clinicians need to be enabled to see these benefits’ (Lusignan et al, 2003, p421) and
‘overcoming clinicians’ motivational problems and other socio-cultural reservations is needed in addition to technical training and system improvement’ (p421).
Solutions….?
Assumption that the benefits of a given technology can be, and are, given and known in advance of its implementation and use and that users simply need to work hard (through change management and training activities) to realise these in practice
Increasingly being challenged by those adopting a more sociotechnical approach to understanding EPRs (see for example, Greenhalgh et al (2009) in their systematic review of the ‘tensions and paradoxes’ in EPR research)
Beyond ‘benefits realisation’
Ontological and epistemological tensions:1. The EPR itself (‘container’ or ‘actor’?)2. The EPR user (‘information processor’ or
‘member of a socio-technical network’?)3. Organisational context (‘the setting within which
EPR is implemented’ or ‘the EPR in use?’)4. Clinical work (‘decision making’ or ‘situated
practice’)5. The process of change (‘the logic of determinism’ or
‘the logic of opposition’?)6. Implementation success (‘objectively defined’ or
‘socially negotiated’?)7. Complexity and scale (‘the bigger the better’ or ‘small
is beautiful’?).
Greenhalgh et al 2009: 7 key tensions in EPR research
Identify a tension experienced by clinicians as they construct the EPR during the PC consultation.
The EPR exhibits agency and may be thought of as ‘a collection of silent but consequential voices’ that present clinicians with a ‘dilemma of attention’ as they seek to deal with both the immediacy of the interpersonal interaction (the ‘here and now’) and the institutional demands (the ‘there and then’) of the EPR
This tension is sharpened by the use of computer templates which contain two different ‘framings of the patient’- as ‘individual’ or as ‘one of a population’.
Clinicians overcome this tension by ‘responding creatively to prompts within a dialogue constructed around the patient’s narrative’
This type of ‘creative work’ is required to avoid privileging ‘institution-centred’ care over ‘patient-centred’ care (Swinglehurst et al, 2010)
Recent example of ‘recursive’ approach: Swinglehurst et al
Logics as ‘modes of ordering’; different ways of thinking and acting that may co-exist in time and space (Law, 1994; Mol, 2008)
Actor networks – people and technologies enrolled into networks; networks achieve stability when all actors are aligned through process of translation involving 4 stages of ‘problematisation’ (defining prob/solution, getting acceptance, defining roles and practices, engaging others in fulfilling these roles…) (Callon, 1986)
Multiplicity- records create multiple bodies and ‘bodies politic’- a site where multiple stories about patients and orgs are at stake…(Berg and Bowker, 1997)
Logics, actor networks and multiplicity
Go back to record-making and observe, ask GPs to reflect on what they do to try and understand:◦ What is the purpose of the record and record
keeping? ◦ What do GPs record and how? Free text and coded
entries?◦ Who shares the record? Who’s it for?◦ What IS the EPR?
Our focus and questions
WHY RECORD? GOOD, SHARED, DEFENSIBLE PATIENT CARE ‘so someone else can carry on’ ‘to make sense to someone else’; ‘mostly to inform other clinicians’ ; ‘informing other people what’s going through your mind’ ‘a method of communicating’…. ‘it’s record keeping’ To defend ourselves’ ‘The records have to be fit for sharing and because so
many people come into the different practices now, everybody’s got to be able to carry on with, you know, from where you left off; it’s quite, you know, it’s quite frequent that (pause) they’ve got to be understandable for the next person’ (SE05, Lead Partner)
The logic of patient care?
WHO ELSE MIGHT LOOK AT THE RECORD: WHO IS IT FOR? ‘Other GPs, those doing audit; maybe practice
manager’ (MS01) ‘Others in practice’ (MS03) ‘The next doctor, if patient comes back…’ (MS04) ‘Fellow clinicians; receptionists -for example, if patient
lost the blood test (BT) form…’ (MS02). I wish we could communicate with other practices via
them, with all the, you know, the hospitals. We could get information from hospital records via our computer, the results, discharge summaries. I mean everything should really be done electronically at this stage …’(SE05, Lead Partner, Selbury Practice)
The network?
‘useful for looking back… you can see the story appear…it’s a useful short cut’. (MS01)
‘If I wanted to see all the blood pressures, I can do that and they’re all there you see? And if they’re not coded, you can’t find them that way. So it’s quite useful’ (SE05)
‘it structures the consultation; it’s useful to go back and find things; it’s organising isn’t it?’ (MS04, keen coder).
Overlap with args for use of free text- the ‘story’ again- this time the ‘details’ of that story: ◦ ‘It reminds me. So, ok, some of the details I can see it’s that
guy…it’s an important aspect of his history’ (MS03);◦ ‘It’s the story, if you like, the details, anything that can’t be
coded or if you can’t find the code (laughs)…it’s where the plan goes, what’s going to happen next, then if they go to someone else, s/he knows’ (MS01).
‘I would use “chat with patient” for anything that doesn’t fit with anything else…and I would use it for anything personal like problems at home’ (MS05)
Coding for patient care?
‘Both [codes and free text] have a role. Free text has the finer detail you never get from code. Coding is very useful, helps you look back more easily and see the thread and for audit as well…but I wouldn’t want to be without my free text (laughs)’ (MS01)
‘It’s the whole record that’s important
Frustration with the number of codes available ‘for the same thing’ (MS01)
‘confusing’ (MS01), ‘hard to find’ (MS02), ‘unduly complex’ (SE05)
‘the codes are very important for auditing purposes’, but there were simply ‘way too many’ that are ‘so precise’, citing the example of ‘accidently stung by a sea cucumber’ as the most absurd and useless she had come across (SE05, Lead GP)
Continuing tensions and resistances?
‘…they may look like symptoms but are intended to be diagnostic. There are semantic issues like ‘history of’ might refer to history of the complaint patient is presenting with today or might be interpreted as family history…it can be very hard to find rare or unfamiliar codes- especially with time available’ (MS02)
‘Coding is sort of dry…anyway. It’s difficult to code initially because, in General Practice, we don’t know what we’re dealing with’ (SE4).
Continuing tensions and resistances?
‘I’d like to code things as I go along…all this scrolling through and can’t find what you want…really hard.’ (MS03, Vision user who had used EMIS in the past).
In reflecting on why she uses so few codes, MS03 said: ‘it’s enough…with other system [EMIS], it codes as it goes along, so it’s much more useful but with this one, you have to search for it so it’s time consuming to do any more…so it’s enough, just enough to cover me [for medico-legal]’ (MS03, Vision user).
System differences, system affordances
‘we don’t always all use the same codes…sore throat or something like that, it doesn’t have huge implications if you chose whichever…but I think that with chronic disease conditions, we all try to sing from the same song sheet on that’ (SE01, Senior Partner, Selbury)
: ‘I don’t code any of the examination unless it’s something cardiac or something that might be useful for QOF, and the medications and the bloods’ (SE05)
‘that’s where coding becomes important because she becomes part of our chronic disease management programme; she’ll go onto disease modifying drugs and it’ll be important to follow up’ (MS02)
Coding for service management?
‘I’m feeling more and more cynical about data rich environments in which nobody seems to be able to draw out the right data to make the right conclusions’
On coding for QOF purposes: ‘I mean if someone pays me to record
“smokes with his right hand”, I’ll probably record it, which is very sad because it has no consequences to what I do’ (MS05)
Coding for service management?
Better understand what is happening on the ground- especially re coding and coded data
Devise a framework for understanding this that goes beyond ‘clinician resistance’ and needing them to ‘realise/see/understand the benefits’ of coding (realisation as recognition or appreciation?)
GPs already working to produce benefits but only when they see a good fit with logic of patient care (realisation as making happen or accomplish)
Information sharing?
◦ The patient care EPR◦ The service management EPR◦ The Research EPR
◦ Each with different ‘logics’ (modes of ordering’), made up of different networks of actors
◦ GPs at centre of all three but not equally engaged with all logics, enrolled into or aligned with all networks
The ‘multiple reality’ of Primary Care EPRs
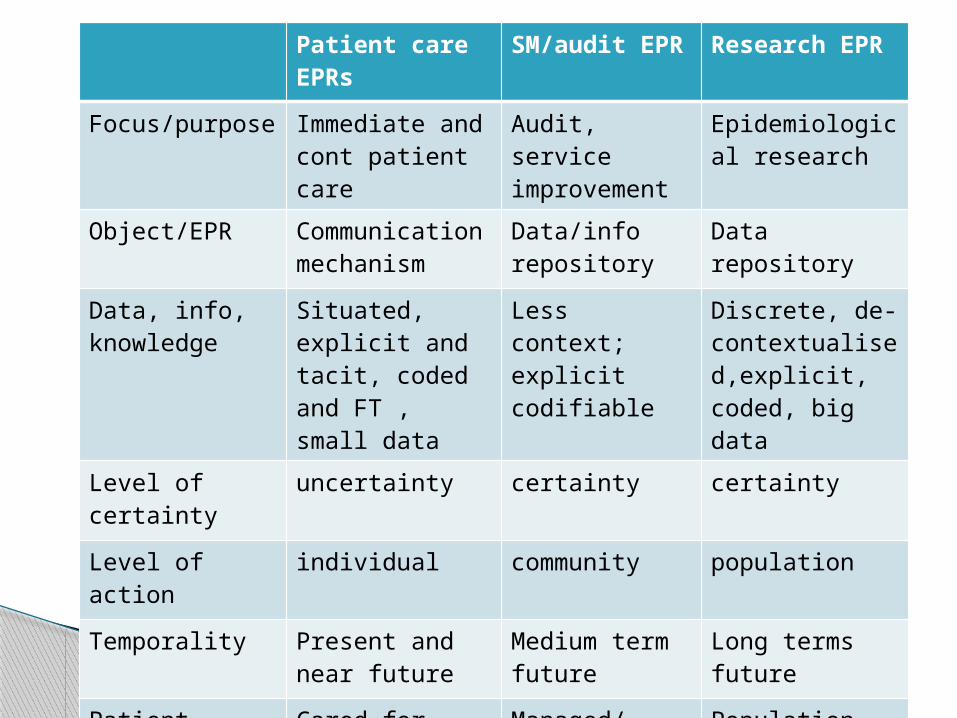
Patient care EPRs
SM/audit EPR Research EPR
Focus/purpose Immediate and cont patient care
Audit, service improvement
Epidemiological research
Object/EPR Communication mechanism
Data/info repository
Data repository
Data, info, knowledge
Situated, explicit and tacit, coded and FT , small data
Less context; explicit codifiable
Discrete, de-contextualised,explicit, coded, big data
Level of certainty
uncertainty certainty certainty
Level of action individual community population
Temporality Present and near future
Medium term future
Long terms future
Patient Cared for patient
Managed/audited patient
Population patient

Flis HenwoodSocial Science Policy and Research CentreSchool of Applied Social ScienceUniversity of [email protected]://www.brighton.ac.uk/ssparc/index.aspx
On Patient Record Enhancement Programme: http://prep.sussex.ac.uk/
Thanks!